Embed Size (px)
Citation preview

Classification of Pelvic Fractures: A Mechanistic Approach
Allison MoriartyDecember 16, 2006
Outline
Epidemiology Anatomy Imaging Classification Complications Treatment

Epidemiology
Only 2-3% of all skeletal fractures Most result from high energy trauma Severity of fracture depends on mechanism of injury
>Minor pelvic fractures (fractures of individual bones or single breaks in the pelvic ring; lower energy) – elderly patients after simple falls>Complex pelvic fractures (higher energy) – younger patients (50% <30yo, 77% <50yo), M:F = 3:1
Severe pelvic injury usually due to high-velocity MVA, industrial accidents, falls of a significant distance

Epidemiology
Complex Pelvic Fxs
Etiology % Patients Mortality RateMVA 43 26%Farm accident 18 0%Pedestrian accident 17 41%Motorcycle accident 8 38%Falls 6 17%Other 8 0%

Anatomy
Pelvic Ring Consists of 2 innominate
bones (ilium, ischium, pubis) and sacrum that are connected posteriorly at the SI joints and anteriorly at the symphysis pubis
The acetabulum is located where the ilium, ischium, and pubis meet laterally
Source: Berquist
Anatomy
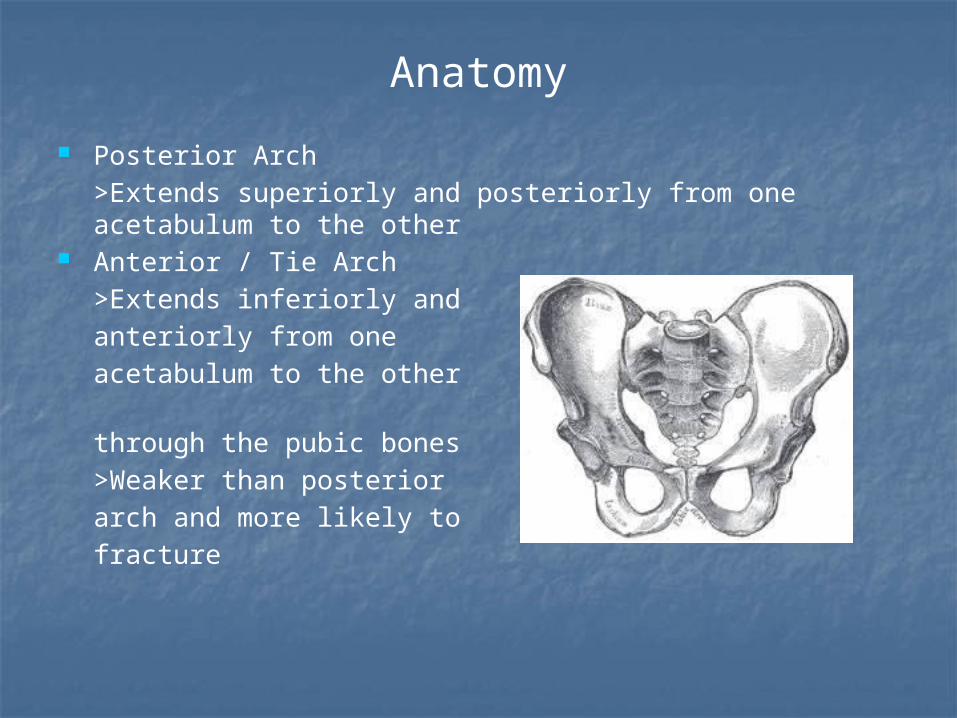
Posterior Arch >Extends superiorly and posteriorly from one acetabulum to the other
Anterior / Tie Arch>Extends inferiorly and anteriorly from one acetabulum to the other through the pubic bones>Weaker than posterior arch and more likely to fracture

Anatomy
Bony Pelvis
Source: Berquist
Composed of 2 innominate bones (ilium, ischium, pubis), sacrum, coccyx
SI joint – predominately amphiarthroidal (connected by fibrocartilage) and partially diarthroidal (synovial)
Pubic symphysis (articulation of bodies of pubic bones) – amphiarthroidal
Anatomy
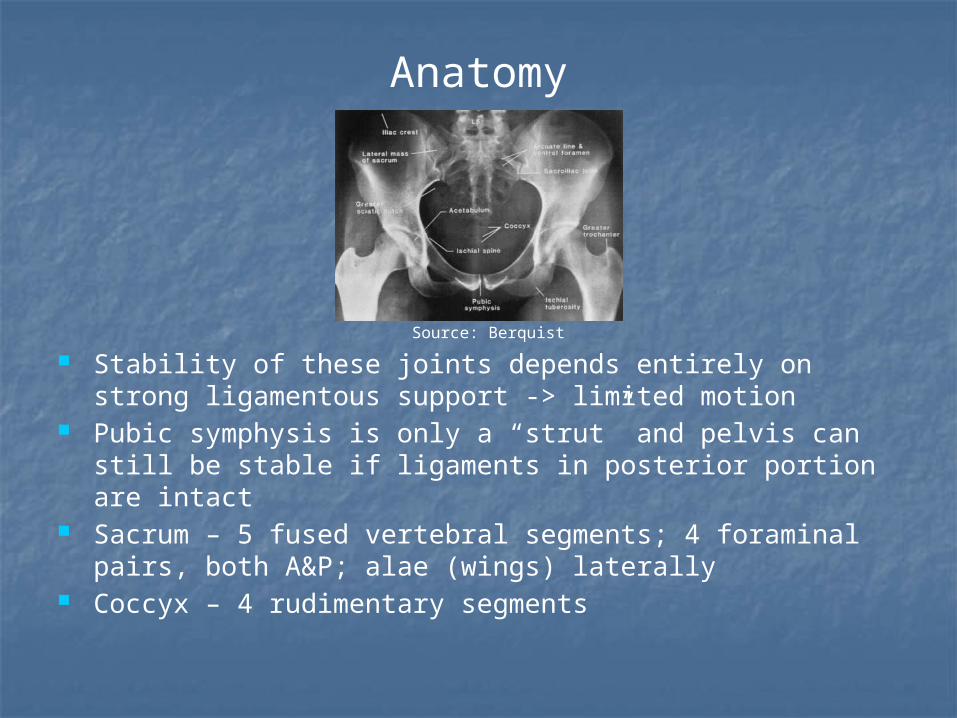
Source: Berquist
Stability of these joints depends entirely on strong ligamentous support -> limited motion
Pubic symphysis is only a “strut” and pelvis can still be stable if ligaments in posterior portion are intact
Sacrum – 5 fused vertebral segments; 4 foraminal pairs, both A&P; alae (wings) laterally
Coccyx – 4 rudimentary segments

Anatomy
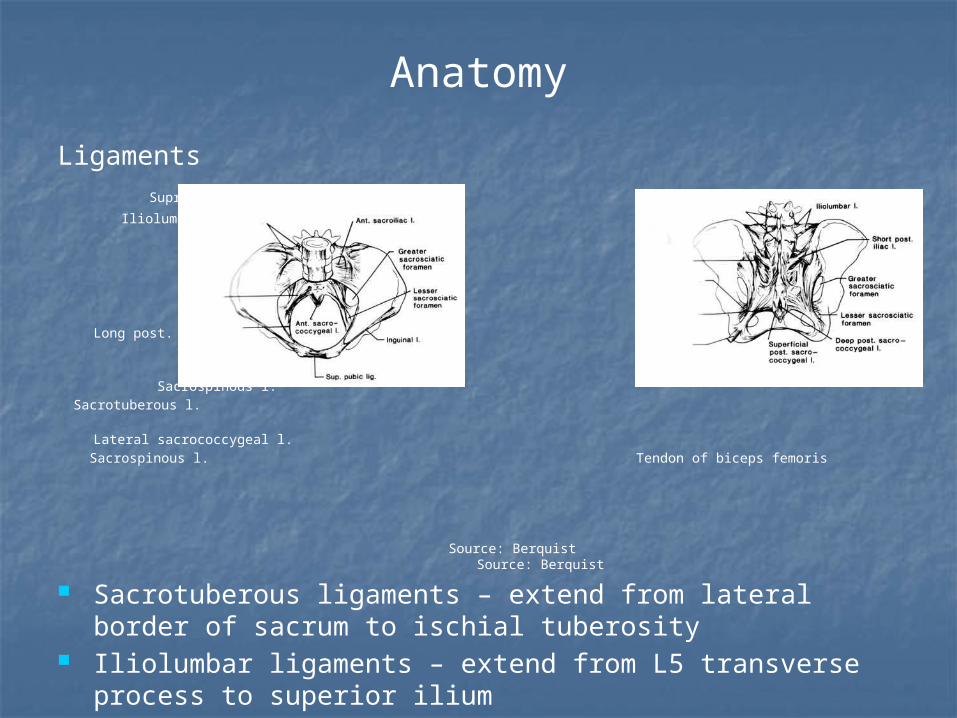
Ligaments Supraspinous l.
Iliolumbar l.
Long post. sacroiliac l.
Sacrospinous l. Sacrotuberous l. Lateral sacrococcygeal l. Sacrospinous l. Tendon of biceps femoris
Source: Berquist Source: Berquist
Anterior SI ligaments – extend from anterior sacrum to ilium Posterior SI ligaments (both originate from PSIS and PIIS) –
>Short – travels laterally to sacrum>Long – travels inferiorly to lateral portion of inferior sacrum
Interosseous SI ligaments – connect tuberosities of ilium and sacrum
Sacrospinous ligaments – extend from lateral border of sacrum to ischial spine
Anatomy
Ligaments Supraspinous l.
Iliolumbar l.
Long post. sacroiliac l.
Sacrospinous l. Sacrotuberous l. Lateral sacrococcygeal l. Sacrospinous l. Tendon of biceps femoris
Source: Berquist Source: Berquist
Sacrotuberous ligaments – extend from lateral border of sacrum to ischial tuberosity
Iliolumbar ligaments – extend from L5 transverse process to superior ilium
Lumbosacral ligaments – extend from L5 transverse process to superior sacrum
Anterior, superior, inferior pubic ligaments* Posterior SI ligaments stronger than anterior SI ligaments
Anatomy
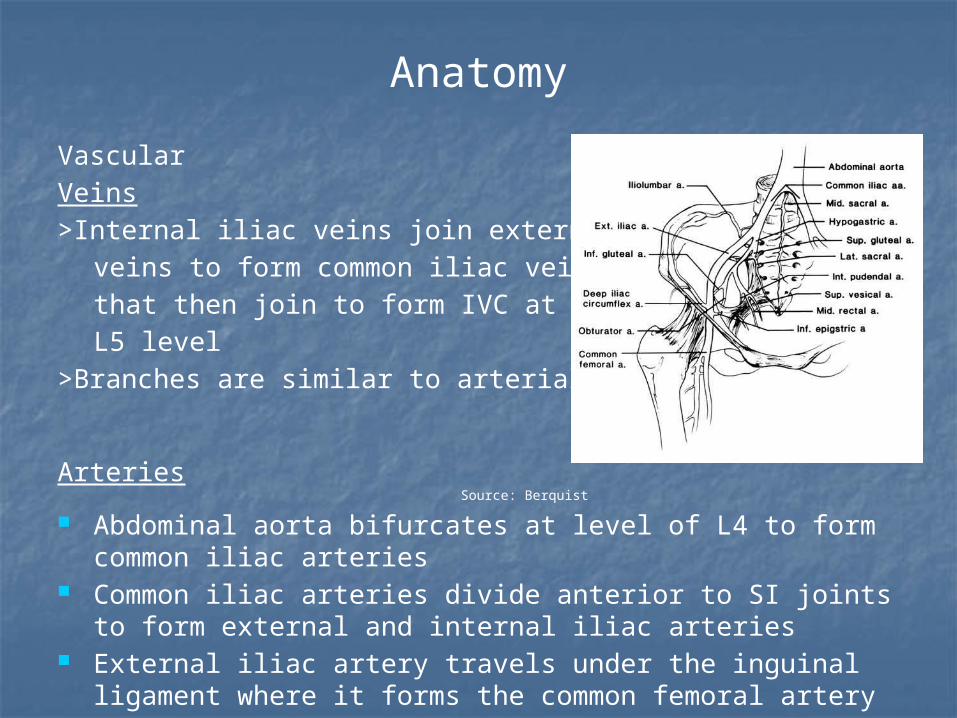
VascularVeins>Internal iliac veins join external iliac
veins to form common iliac veins that then join to form IVC at the L5 level
>Branches are similar to arterial branches
Arteries Source: Berquist
Abdominal aorta bifurcates at level of L4 to form common iliac arteries
Common iliac arteries divide anterior to SI joints to form external and internal iliac arteries
External iliac artery travels under the inguinal ligament where it forms the common femoral artery
Anatomy
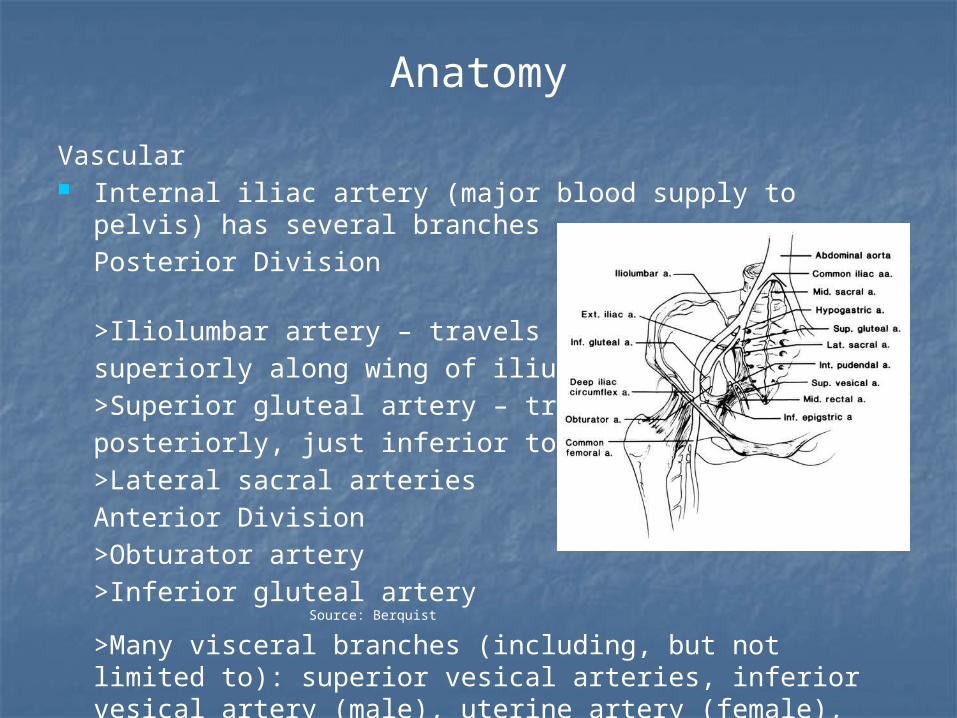
Vascular Internal iliac artery (major blood supply to pelvis) has
several branches Posterior Division >Iliolumbar artery – travelssuperiorly along wing of ilium >Superior gluteal artery – travels posteriorly, just inferior to the SI joint>Lateral sacral arteriesAnterior Division >Obturator artery>Inferior gluteal artery Source: Berquist
>Many visceral branches (including, but not limited to): superior vesical arteries, inferior vesical artery (male), uterine artery (female), internal pudendal artery, middle rectal artery
Anatomy
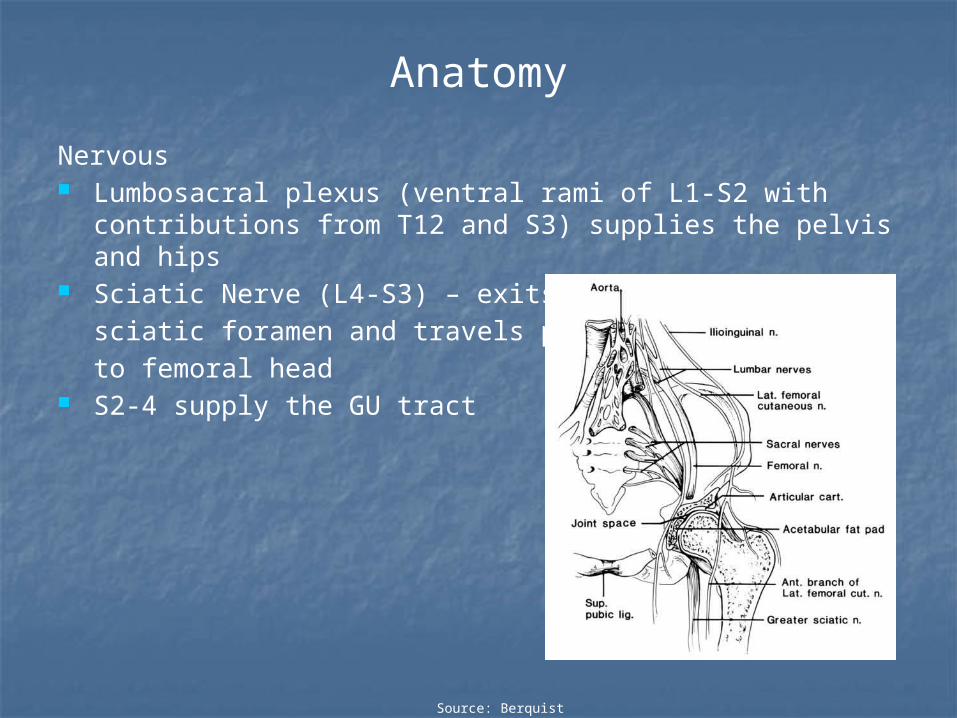
Nervous Lumbosacral plexus (ventral rami of L1-S2 with
contributions from T12 and S3) supplies the pelvis and hips Sciatic Nerve (L4-S3) – exits greater
sciatic foramen and travels posterior to femoral head
S2-4 supply the GU tract
Source: Berquist

Imaging
X-ray is the primary method of initial evaluation Standard view is the AP view; inlet and outlet views can be
obtained for clarification SI joint should be no more than 2-4mm wide; superior or
inferior offset of 1-2mm is normal Symphysis pubis should be no more than 5mm wide
Imaging
Source: Berquist
Source: Berquist
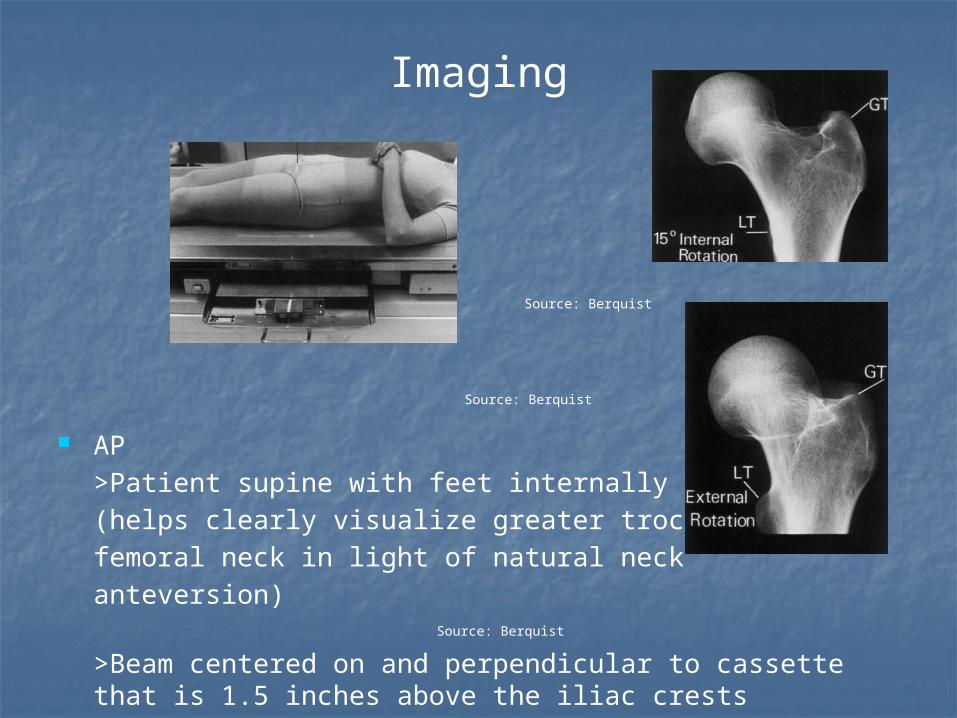
AP
>Patient supine with feet internally rotated 15˚ (helps clearly visualize greater trochanter and femoral neck in light of natural neck anteversion) Source: Berquist
>Beam centered on and perpendicular to cassette that is 1.5 inches above the iliac crests
Imaging
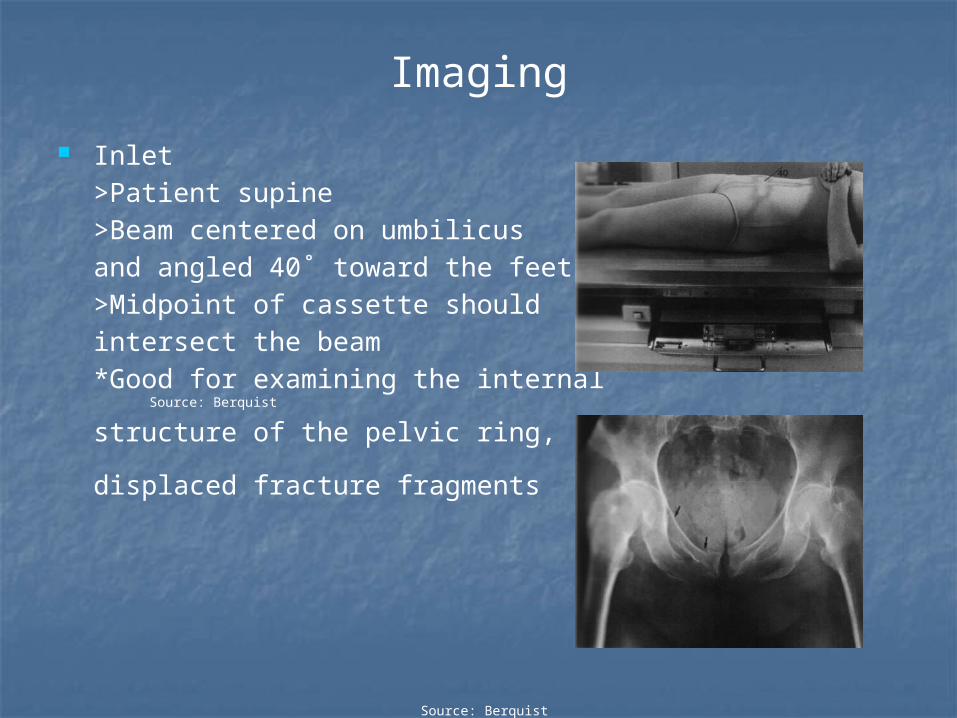
Inlet>Patient supine>Beam centered on umbilicus and angled 40˚ toward the feet>Midpoint of cassette should intersect the beam*Good for examining the internal Source: Berquist
structure of the pelvic ring,
displaced fracture fragments
Source: Berquist
Imaging
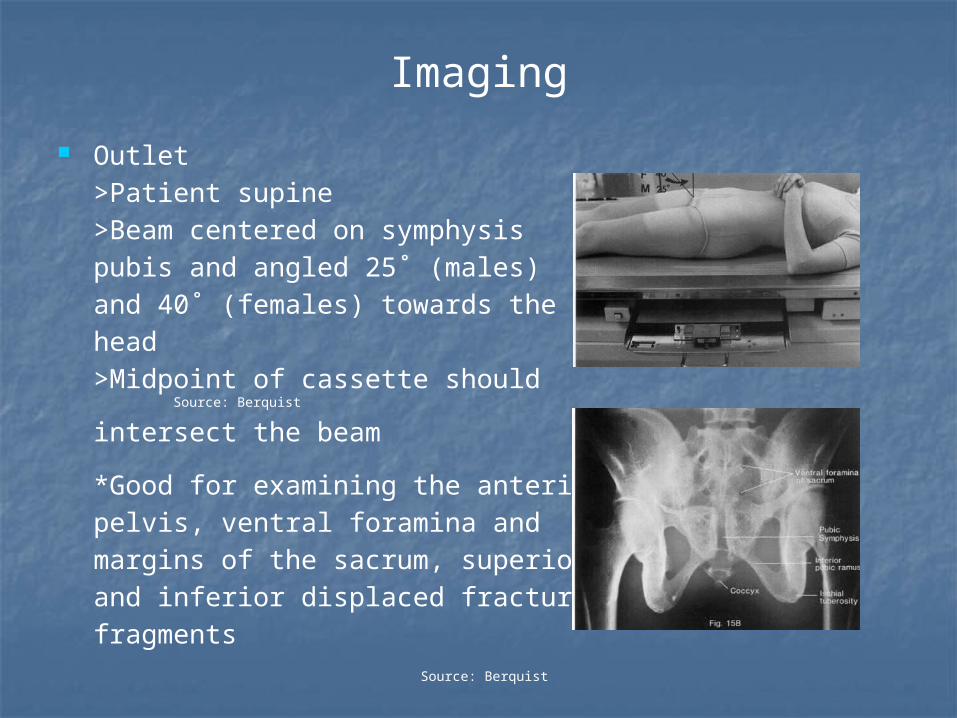
Outlet>Patient supine>Beam centered on symphysis pubis and angled 25˚ (males) and 40˚ (females) towards the head>Midpoint of cassette should Source: Berquist
intersect the beam
*Good for examining the anterior pelvis, ventral foramina and margins of the sacrum, superior and inferior displaced fracture fragments
Source: Berquist

Classification
The Young and Burgess system classifies pelvic fractures based on the direction of the applied force. This allows
recognition of likely associated injuries as well as assisting with planning of treatment.
Classification
Source: Pearson Source: Young
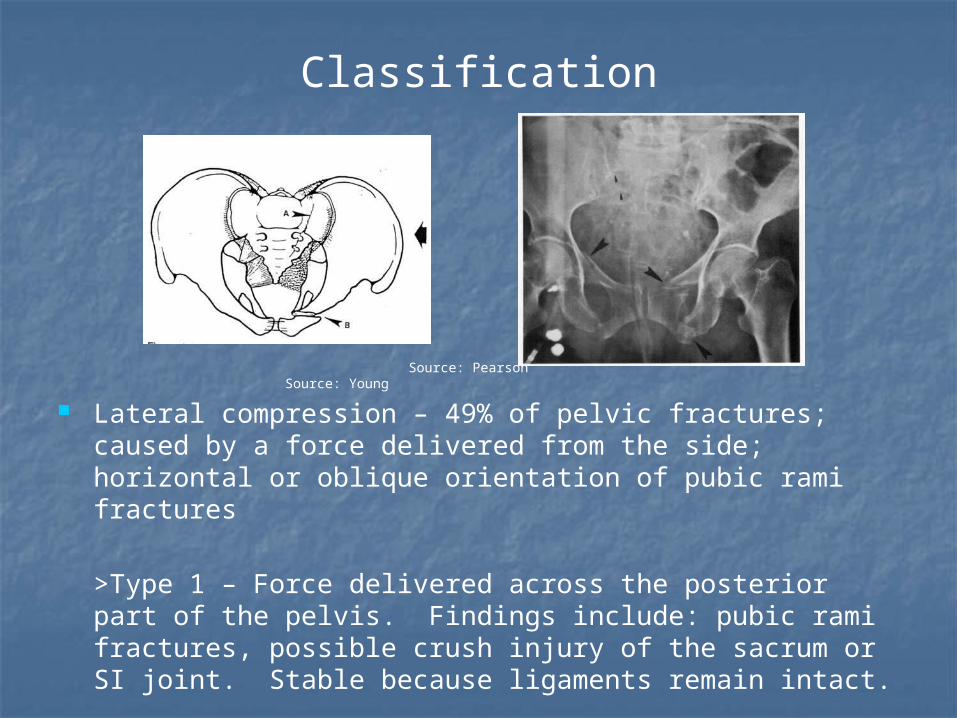
Lateral compression – 49% of pelvic fractures; caused by a force delivered from the side; horizontal or oblique orientation of pubic rami fractures
>Type 1 – Force delivered across the posterior part of the pelvis. Findings include: pubic rami fractures, possible crush injury of the sacrum or SI joint. Stable because ligaments remain intact.
Classification
Source: Pearson
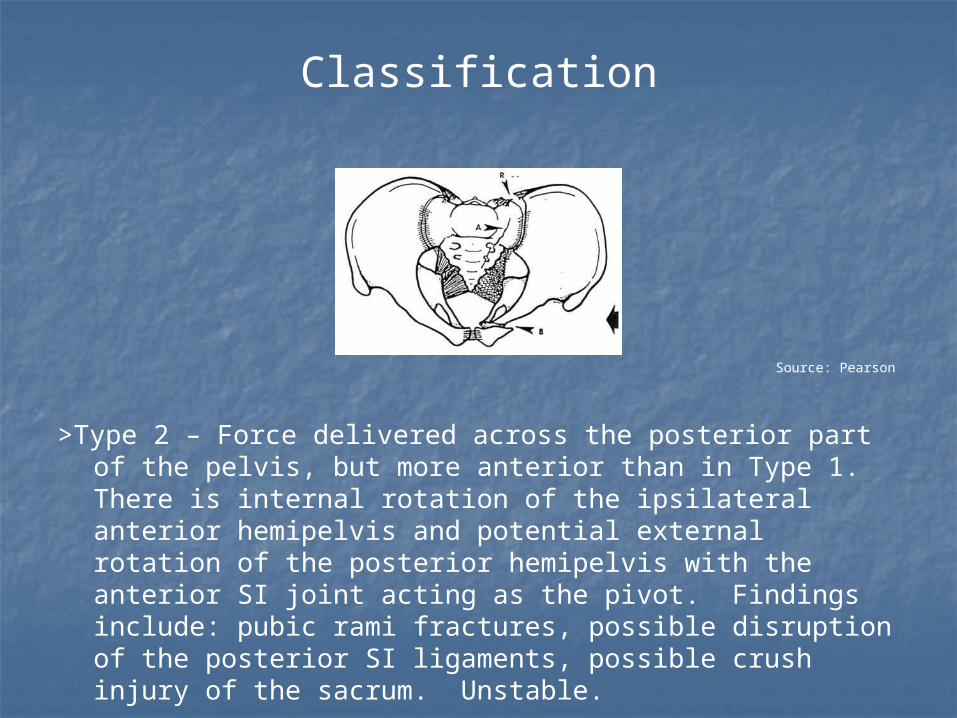
>Type 2 – Force delivered across the posterior part of the pelvis, but more anterior than in Type 1. There is internal rotation of the ipsilateral anterior hemipelvis and potential external rotation of the posterior hemipelvis with the anterior SI joint acting as the pivot. Findings include: pubic rami fractures, possible disruption of the posterior SI ligaments, possible crush injury of the sacrum. Unstable.

Classification
Source: Pearson
>Type 3 – Force delivered across the posterior part of the pelvis, but more anterior than in Type 1. It is so severe that there is external rotation of the contralateral hemipelvis as well as internal rotation of the ipsilateral hemipelvis (this pattern appears as lateral compression on the ipsilateral side and AP compression on the contralateral side). Findings include: pubic rami fractures; rupture of the ipsilateral posterior SI ligaments; rupture of the contralateral sacrospinous, sacrotuberous, and anterior SI ligaments; possible crush injury of the sacrum. Unstable.
Classification
Source: Pearson
Source: Young
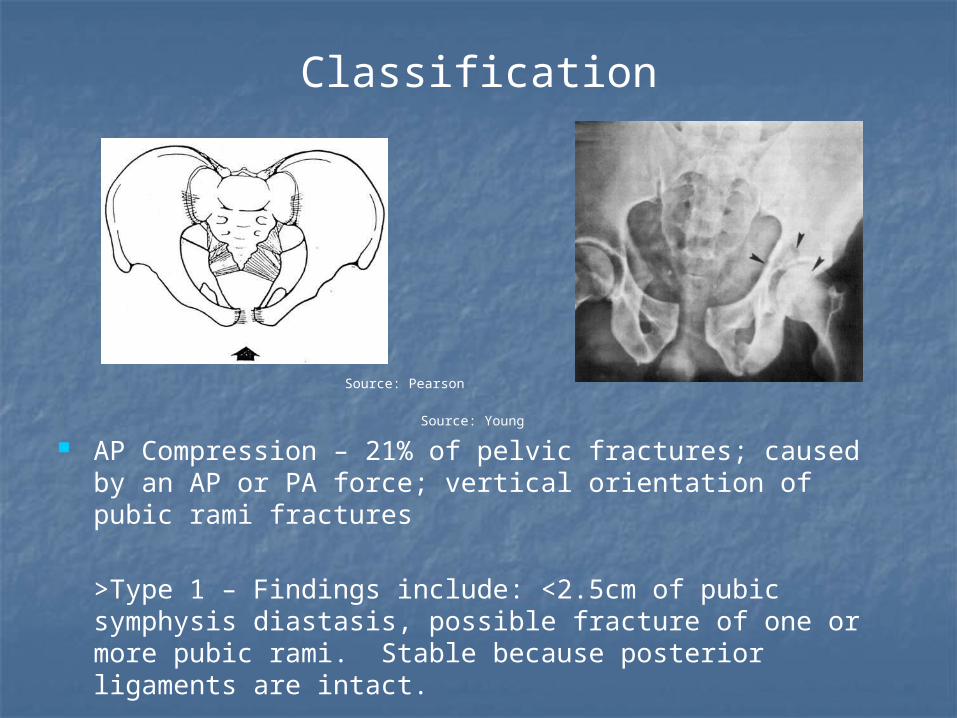
AP Compression – 21% of pelvic fractures; caused by an AP or PA force; vertical orientation of pubic rami fractures
>Type 1 – Findings include: <2.5cm of pubic symphysis diastasis, possible fracture of one or more pubic rami. Stable because posterior ligaments are intact.
Classification
Source: Pearson Source: Young
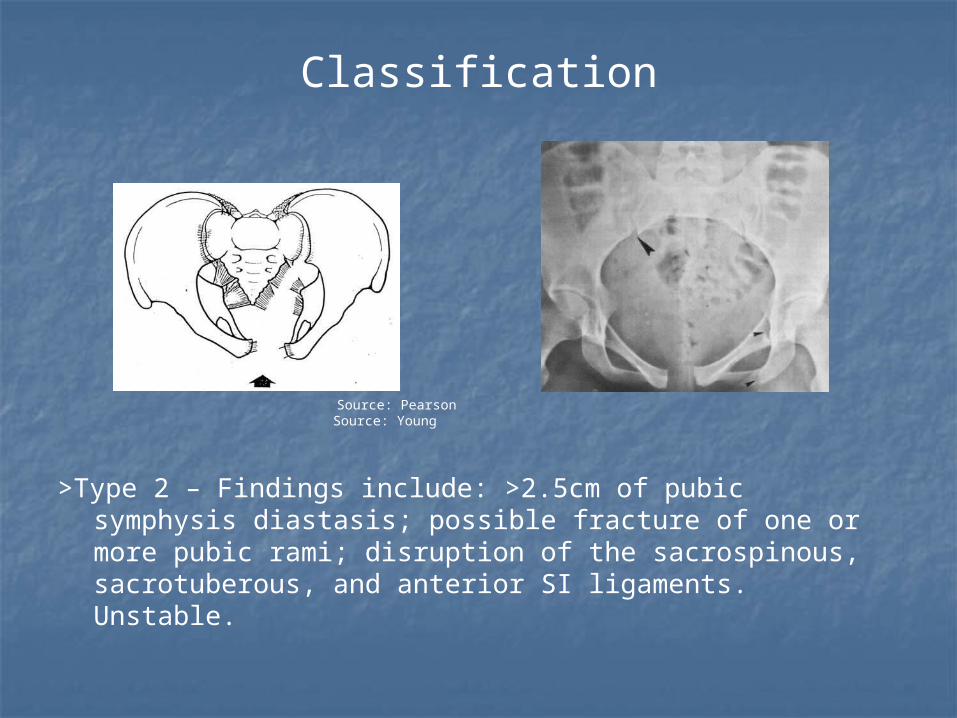
>Type 2 – Findings include: >2.5cm of pubic symphysis diastasis; possible fracture of one or more pubic rami; disruption of the sacrospinous, sacrotuberous, and anterior SI ligaments. Unstable.

Classification
Source: Pearson Source: Young
>Type 3 – Findings include: possible fracture of one or more pubic rami, total disruption of the pubic symphysis and SI joint. Unstable.
Classification
Source: Pearson Source: Young
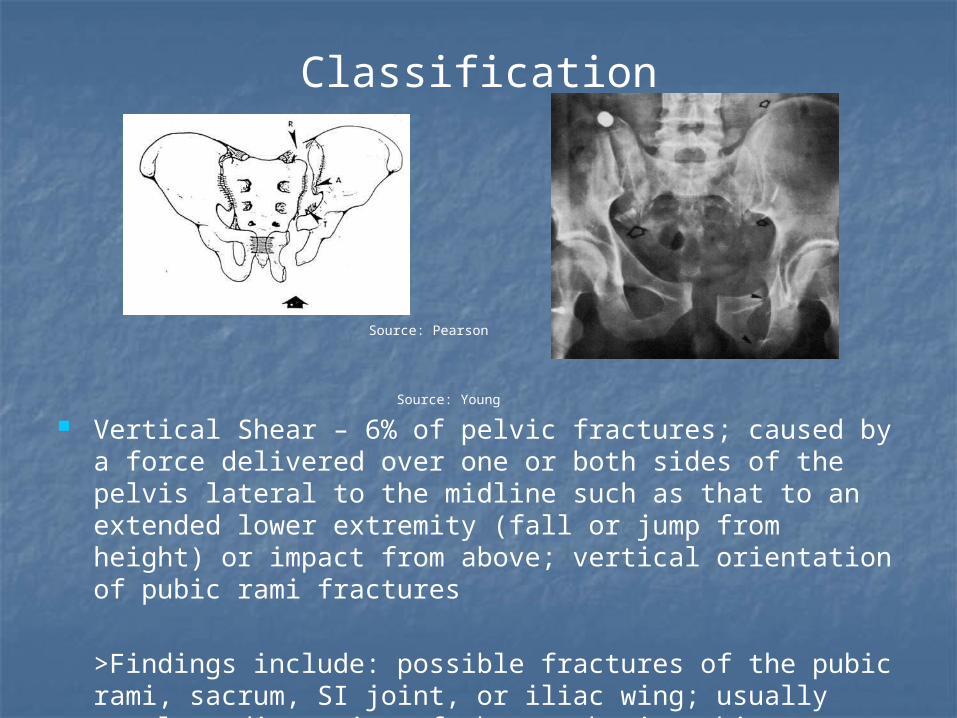
Vertical Shear – 6% of pelvic fractures; caused by a force delivered over one or both sides of the pelvis lateral to the midline such as that to an extended lower extremity (fall or jump from height) or impact from above; vertical orientation of pubic rami fractures
>Findings include: possible fractures of the pubic rami, sacrum, SI joint, or iliac wing; usually complete disruption of the symphysis pubis, anterior and posterior SI, sacrospinous, and sacrotuberous ligaments. Unstable.

Classification
Combination>Usually due to a crush mechanism. Source: Young
Most often vertical shear and lateral compression.

Complications
Hemorrhage / Vascular Injury>Usual source of retroperitoneal hemorrhage is venous plexus disruption in the posterior pelvis; can also be caused by large artery injury
GI / GU Injury>Perforation of the rectum or anus with bony fragments or entrapment of a portion of the bowel in the fracture site>Ureters (posterior pelvic fractures; infrequent); bladder, urethra (symphysis and pubic rami injury; urethra injured more often in males)
Neurologic Injury>Lumbosacral plexus and nerve root (especially with sacral fractures) injuries are the most common>Sciatic nerve at particular risk with posterior pelvic injury

Treatment
Initial treatment involves general trauma evaluation / resuscitation and hemorrhage control (can include angiography and embolization if bleeding persists)
Further treatment can involve external and/or internal fixation with particular attention paid to possible open fractures that involve associated injury to the GI or GU systems
Other postoperative measures include: aggressive pulmonary toilet, thromboembolic prophylaxis (heparin as allowed), slowly advancing weight-bearing status
Sources
1. Berquist TH, Coventry MB. Chapter 5: The Pelvis and Hips. Imaging of Orthopedic Trauma. 1992.
2. Koval KJ, Zuckerman JD. Handbook of Fractures. 2002.
3. Moore KL, Dalley AF. Clinically Oriented Anatomy. 1999.
4. Pearson, JM. “Pelvic Fractures” handout.
5. Young JWR, et al. Pelvic Fractures: Value of Plain Radiography in Early Assessment and Management. Radiology 1986;160:445-451.





























