Embed Size (px)
Citation preview
Informed Consent for Patient Transfers to a Veterans Affairs Medical Center
DANIEL F. JABLONSKI, MD, G. MICHAEL MOSLEY, MD, JAMES C. BYRD, MD, DEBORAH SCHWALLIE, RN, MS, ANN B. NATTINGER, MD
Objective: To evaluate whether informed consent was ob- tained pr ior to transfers o f patients f rom a community hospital to a Veterans Affairs medical center. Design: Cross-sectional study. Setting: A Department o f Veterap~ Affairs medical center. Participants: Eighty-six consecutive interhospital-trans- ferred patients. Nearly all were white men, with a median age o f 62.5 years. Fifty percent had three or more active medical problems and 17% had been transferred f rom in- tensive care unit& Measurements and ma in results: The authors defined in- formed consent as a discussion o f benefit& risks, and al- ternatives to transfer. Following transfer, patients and physicians were intertriewed using standardized parallel questionnaires. Physician-patient communication re- garding the benefits and risks o f transfer was infrequent. Informed consent was reported f o r none o f the transfers by patient interview, compared with 11% o f the transfers assessed by physician i ~ . Risks o f transfer were dis. cussed infrequently according to both physicians (17%) and patients (13%). Physicians perceived a risk to the pa- tient in 21% o f paMent transfers, and in 36% o f transfers defined by objective criteria as high-risk. Physicians re. called discussing benefits o f transfer more frequentiy thai* did p ~ t s (80% vs. 42%, t test, p < O. 001). Physicians also recalled discussing alternatives to transfer more fre- quently than did patients (61% v& 18%, t test p < 0.001). Conclusions: Verbal informed consent is obtained infre- quently pr ior to interhospital transfer o f patients. Risks o f transfer are seldom perceived and discussed with patients. Key words: veterans;patient transfers; informed consen~ risks. J GEN INTERN MED 1991; 6:229-232.
INTERHOSPITAL TRANSFERS place patients at risk. Patients may be transferred in unstable medical condition and may be exposed to four-to-six-hour treatment delays. 1, 2 Although no study has compared the mortality of trans- ferred patients with that of a disease-matched, non- transferred population, mistakes in stabilization prior to transfer and deterioration of clinical status en route have been documented. 3,~ In a review of 18,000
Received from the Division of General Internal Medicine, Clement J. Zablocki Veterans Affairs Medical Center and the Medical College of Wisconsin, Milwaukee, Wisconsin.
Presented at the 13th annual meeting of the Society of General Internal Medicine, Washington, DC, May 4, 1990, and the Primary Care Research and Development Conference, Michigan State Univer- sity, Lansing, Michigan, May 18, 1990.
Address correspondence and reprint requests to Dr. Jablonski: Division of General Internal Medicine, Clement J. Zablocki Veterans Affairs Medical Center, Milwaukee, WI 53295.
transfers to a county hospital, about 50 deaths were felt to have resulted from the transfers alone. 5
The benefits of transfer for the patient are less ap- parent. Universally accepted guidelines have promoted the transfer of patients for specialized care not available at the transferring facility. Specialized care following transfer, however, is a reason given for only 3% to 16% of interhospital transfers. In contrast, transfer studies cite lack of adequate insurance as the primary reason for 48% to 89% of patient transfers. TM
Governmental regulatory actions have been estab- lished in response to reports of inappropriate or unsafe patient transfers done solely for economic purposes, commonly referred to as "patient dumping." The Con- solidated Omnibus Reconciliation Act (COBRA) of 1986 was enacted as an amendment to the Medicare law to regulate patient transfers to publicly funded hospi- tals. 6 The 1986 COBRA mandated that patients are not to be transferred until stabilized, and then only when the medical benefits expected from treatment at an- other facility exceed the risks of transfer. An amend- ment to COBRA (OBRA 1989), effective July 1, 1990, listed several new provisions. These included the re- quirement that a physician or qualified health profes- sional sign a certification, including a list of risks versus benefits, stating the appropriateness of the transfer. Also, the transferring hospital must take all reasonable steps to inform a patient of the risks versus the benefits of a transfer prior to obtaining written informed con- sent or refusal.7, s
The penalties for failure to comply with the OBRA regulations include fines ($50,000) for physicians or hospitals guilty of illegal transfers. Physicians can also be prohibited from providing services under Medicare, and hospitals can be suspended or terminated from the Medicare program for any violation.7 In addition, medi- cal facilities that suffer financial losses following inap- propriate patient transfers may sue the transferring fa- cilities to cover the costs of care for these patients.
Transfer guidelines promulgated by professional groups such as the American Hospital Association 9 and the American College of Emergency Physicians 1° have called for written informed consent, but studies have shown that consent with documentation has been present in only O- 6% of patient transfers. 1, 2 The pur- pose of our study was to determine whether physicians obtained verbal informed consent from their patients prior to transfer.
229

230 Jablonski etal., INFORMED CONSENT FOR VAMC TRANSFERS
METHODS
Consecutive patient transfers to the Clement J. Zablocki Veterans Affairs Medical Center (VAMC) over a three-month period (October 26, 1989-January 31, 1990) were enrolled in the study. A "patient transfer" was defined as a patient who was sent to the VAMC
d i r ec t ly from a community hospital, either from the emergency department or from an inpatient service, and was admitted to the VAMC. We excluded transfers from other VA hospitals, community nursing homes, non-hospital detoxification facilities, free-standing am- bulatory care centers, and physicians' offices. Only acute care transfers were evaluated.
Following a phone call from a transferring physi- cian with an eligible patient transfer, demographic data (age, sex, insurance status, VA eligibility) and clinical information (diagnoses, hospital course, reason for transfer, medications, supportive measures, and ex- pected mode of transfer) were recorded by a clinical nurse expediter (DS) on a standardized form. The final decision to accept a patient for transfer, based on clini- cal stability, was made by an admitting staff internist or by a specialty service physician. Physicians collecting study information were not involved in accepting pa- tients for transfer. During the study period 98% of re- quested transfers were accepted, and an emergency de- partment logbook that listed all ambulance arrivals was used to insure the enrollment of all eligible patients.
Following transfer, we obtained the patient's consent to administer a Pfeiffer Mini-Mental Status Ex- amination to estimate his or her capacity to reliably answer the questionnaire, tl If the patient failed the Pfeiffer Mini-Mental Status Examination or if the patient was not alert and oriented prior to transfer, a family member or another decision maker was contacted. A standardized questionnaire was used to interview each patient or appropriate patient surrogate.
"Informed consent" was defined as a physician- patient or physician-surrogate discussion about the risks, benefits, and alternatives to transfer. Patients or surrogates were asked directlywhether these issues had been discussed prior to transfer. Terms were clarified by asking what benefits (advantages) or risks (disad- vantages or dangers) had been discussed, and whether they had felt they had any other alternatives (choices). Other questionnaire items determined who had ini- tially raised the possibility of transfer, when in the hos- pital course the transfer had been discussed, whether there had been understanding of the benefits and risks of transfer, and whether the patient had felt pressured into the transfer. The questions about understanding and pressure were asked using five-point Likert scales with responses ranging from "no understanding" to "complete understanding," and "felt no pressure" to "felt very pressured."
Transferring physicians were contacted by tele- phone as soon as practical after the transfer. Physicians
were informed that the information collected was to be used in a study of patient transfers and that the inter- viewer was in no way involved in the direct care of the patient. Agreement to participate in the interview was equated with implied consent. No physician refused to be interviewed. Physicians were interviewed using a parallel questionnaire, but were also asked whether they had perceived significant risk for the patient dur- ing the transfer process. Each transferring physician participated in the study only once to avoid the possi- bility that the study would alter physician practice.
Patients were divided into two groups: low-risk transfers and high-risk transfers. Criteria used to place a patient in the high-risk group 3 included a modification of the APACHE II system that has been prospectively validated to predict prognosis and mortality of criti- cally ill patients undergoing transfer. 12 Patients who had " 4 + " abnormal criteria or who had diagnoses that placed them at risk for either cardiovascular or respira- tory compromise (e.g., ventricular tachycardia, myo- cardial infarction in progress, airway compromise, se- vere GI bleeding) were included in the high-risk group. We also included patients transferred within 48 hours of a new diagnosis of intracerebral or subarach- noid bleeding, seizures, focal neurologic deficits, or mental status changes, as well as patients transferred directly from intensive care units. The mode of transfer was not considered when determining transfer risk.
Data were analyzed using the chi-square test for categorical data and Student's t-test for continuous data. The study was reviewed and approved by our human subjects research committee.
RESULTS
Demographics
Eighty-six patients met eligibility criteria for the study. Patient questionnaires were obtained in 90% (77/86) of the transfers, and physician questionnaires were obtained in 73% (63/86) of the transfers. Missing data were most often due to an inability to contact an appropriate patient surrogate or the transferring physi. cian. Complete data sets (demographics, patient and physician questionnaires) were obtained for 65% (56/86) of transfers.
Eighty-five of the transfers were male, and their mean age was 61.5 years; 41% were 65 years of age or older. Fifty percent had three or more active medical problems. Patients were reported to be alert and ori- ented in 80% (69/86) of transfers, while the remainder had poor or fluctuating mental status. Seventeen per- cent were transferred from an intensive care unit, 23% were from step-down units, 31% were from medical or surgical wards, and 2896were from community hospital emergency departments.
Fifty-two percent of the patients were uninsured, 40% had Medicare, 1% had Medicaid, and 2% had pri-
JOURNAL OF GENERAL INTERNAL MEDICINE, Volume 6 (May/June). 1991 231
vate insurance. Twenty-two percent of patients were transferred because they lacked insurance, and 45% of patients were transferred because they had previously received care at our VAMC. Of the latter group, 40% lacked insurance, and the remaining 60% had Medi- care. Only 16% of patients were transferred to receive special care unavailable in the community hospital.
Transfer Process
Ninety percent of the patients were transferred by ambulance; the remainder, by car, van, or cab. Of those transferred by ambulance, 17% of patients were accom- panied by a nurse or physician; all others were trans- ferred by emergency medical technicians alone. Pa- tients were transferred from more than 1 O0 miles away in 20% of cases; the remainder came from community hospitals within a 100-mile radius.
Informed Consent
Patients answered 74% (57/77) of the patient questionnaires and surrogates answered the remainder. Transferring physicians were interviewed for all of the physician questionnaires.
Table 1 compares the responses obtained from the parallel questionnaires given to patients and physi- cians. Comparisons were made only in the transfers where complete data sets were available for analysis (n----56). There were significant differences in the rates that physicians and patients recalled a discussion of the benefits and alternatives to transfer. Both physi- cians and patients answered that risks of transfer had been discussed infrequently. Physicians, however, stated that they had perceived a risk to the patient in only 21% (12/56; 95% CI 11-31%) of the transfers. Fifty percent (6/12) of the physicians who had per- ceived risk stated they had discussed it with their pa- tients. Patients or surrogates did not recall a discussion of risk in any of these transfers.
Because physicians frequently estimated transfer risks to be low, we analyzed the physician question- naires using a different definition for informed consent
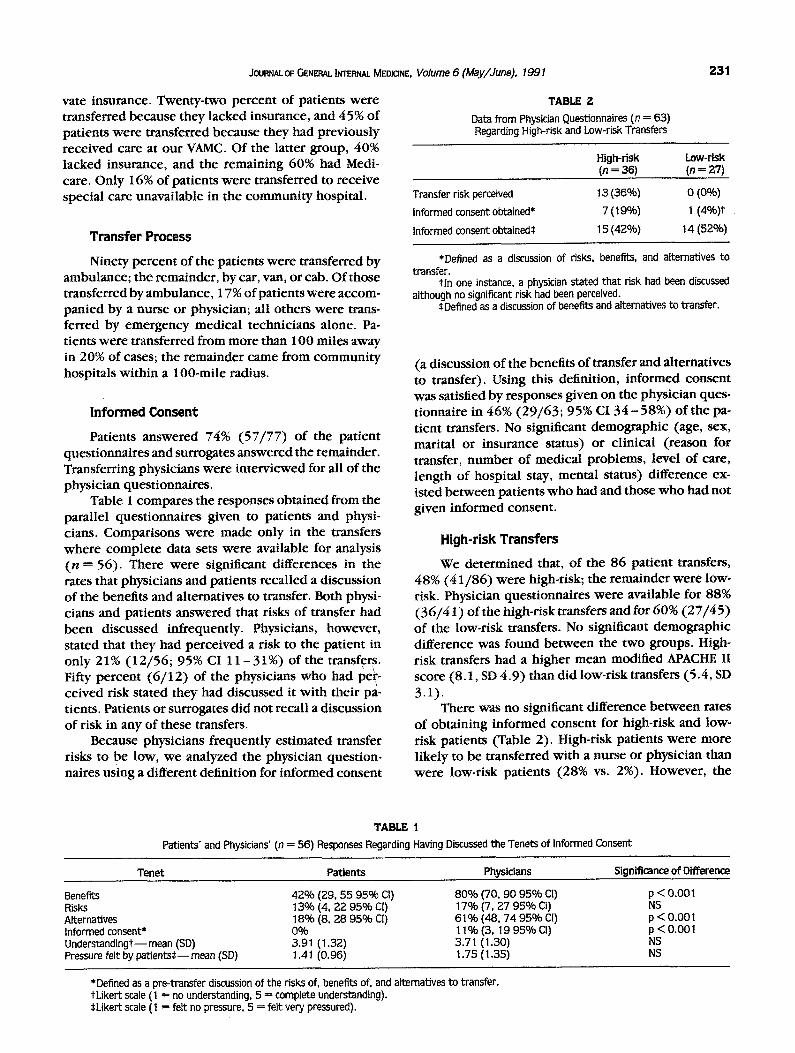
TABLE Z Data from Physician Questionnaires (n = 63) Regarding High-risk and Low-risk Transfers
High-risk Low-risk (n = 36) (n ---- 27)
Transfer risk perceived
Informed consent obtained*
Informed consent obtained*
13 (36%) 0 (0%) 7 (19%) 1 (4%)f
15 (42%) 14 (52%)
*Defined as a discussion of risks, benefits, and alternatives to transfer.
t ln one instance, a physician stated that risk had been discussed although no significant risk had been perceived.
*Defined as a discussion of benefits and alternatives to transfer.
(a discussion of the benefits of transfer and alternatives to transfer). Using this definition, informed consent was satisfied by responses given on the physician ques- tionnaire in 46% (29/63; 95% CI 34-58%) of the pa- tient transfers. No significant demographic (age, sex, marital or insurance status) or clinical (reason for transfer, number of medical problems, level of care, length of hospital stay, mental status) difference ex- isted between patients who had and those who had not given informed consent.
High-risk Transfers
We determined that, of the 86 patient transfers, 48% (41/86) were high-risk; the remainder were low- risk. Physician questionnaires were available for 88% (36/4 I) of the high-risk transfers and for 60% (27/45) of the low-risk transfers. No significant demographic difference was found between the two groups. High- risk transfers had a higher mean modified APACHE II score (8.1, SD 4.9) than did low-risk transfers (5.4, SD 3.1).
There was no significant difference between rates of obtaining informed consent for high-risk and low- risk patients (Table 2). High-risk patients were more likely to be transferred with a nurse or physician than were low-risk patients (28% vs. 2%). However, the
TABLE 1 Patients' and Physicians' (n ---- 56) Responses Regarding Having Discussed the Tenets of Informed Consent
Tenet Patients Physicians
Benefits 42% (29, 55 95% C1) 80% (70, 90 95% Ct) Risks 13% (4, 22 95% CI) 17% (7, 27 95% CI) Alternatives 18% (8, 28 95% CI) 61% (48, 74 95% CI) Informed consent* 0% 11% (3, t9 95% CI) Understandingt--mean (SD) 3.91 (1.32) 3.71 (1.30) Pressure felt by patients*--mean (SD) 1.41 (0.96) 1.75 (1.35)
Significance, of Difference
p < 0.001 NS p < 0.001 p < 0.001 NS NS
*Defined as a pre-transfer discussion of the risks of, benefits of, and alternatives to transfer. tLikert scale (1 = no understanding, 5 --- complete understanding). $Likert scale (1 = felt no pressure, 5 = felt very pressured).
P.3P. Jablonski eta/., INFORMED CONSENT FOR VAMC TRANSFERS
majority of both the high-risk (63%) and low-risk (84%) patients were transferred by emergency medical technicians who were not able to perform advanced cardiac life support (ACLS) or administer medications.
DISCUSSION
The case for informed consent for patient transfers is e loquent ly suppor ted by Kellermann and Acker- man. 13 They present four reasons why transfer patients are enti t led to informed consent: 1) patients have a right to emergency treatment that can be waived only with the patient 's informed consent; 2) the patient 's well-being is pro tec ted by informed consent; 3) physi- cian and institutional accountabil i ty for transfer deci- sions is raised by requiring informed consent; and 4) patients are assured of being adequately informed of their rights under existing state and federal laws. 13
While previous transfer studies t, 2, 4 have focused on patient transfers from hospital emergency depart- ments to publ ic or tertiary care referral hospitals, more than 70% of the patient transfers in our study originated from communi ty hospital inpatient services. Regard- less of transfer origin, patient risk has been docu- mented, 3 and the right to informed consent persists. Patients transferred from hospital inpatient services may have an even greater need for informed consent because of the nonemergent nature of many transfers (less potential patient benefit) and the loss of continu- ity of care incurred by the transfer.
The inf requency of informed consent found by this study is consistent with the findings of other studies 14 Physicians may have faced the common barriers to ob- taining informed consent from inpatients. 15 These in- c lude the attitudes held by both the physician and the patient, the complexi ty of the medical system, and the fact that medical decision making occurs as a process rather than an event.
Many factors may hinder informed consent in the setting of interhospital transfer, including economic pressures to transfer and lack of knowledge of the transfer process itself. Since most physicians transfer relatively few patients, they may be unaware of many of the details of transfer, including the support services available for the patient during transfer and those avail- able from the ambulance service. Without this informa- tion, transfer risks may be underestimated. Regardless of whether low risk was estimated subjectively (physi-
cian opinion) or objectively (modified APACHE II cri- teria), benefits and alternatives had been discussed be- fore only about half of the transfers in this study.
Infrequent verbal informed consent, as demon- strated in this study, may be a pre lude to difficulties in compliance with wri t ten informed consent. Further in- vestigation is indicated to examine why transfer risk is infrequently perceived and discussed. Enhancing phy- sicians' percept ions of potential transfer risks should improve the f requency of wri t ten consent required by the OBRA legislation and improve the quali ty of phys ic i an -pa t i en t discussion pr ior to transfer. Ulti- mately, the recognit ion of transfer risks and improved phys ic ian- patient communica t ion should prove bene- ficial to the care of the patient in transfer.
REFERENCES 1. Schiff RL, Ansell DA, SchlosserJE, IdrisAH, MorrisonA, Whitman
S. Transfers to public hospital: a prospective study of 467 pa- tients. N EnglJ Med. 1986;314:552-7.
2. Kellermann AL, Hackman BB. Emergency department patient 'dumping': an analysis of interhospital transfers to the Regional Medical Center at Memphis, Tennessee. Am J Public Health. 1988;78:1287-92.
3. Kerr HD, ByrdJC. Community hospital transfers to a VA medical center. JAMA. 1989;262:70-3.
4. Olson CM, Jastremski MS, Vilogi JP, Madden CM, Beney KM. Stabilization of patients prior to interhospital transfer. Am J Emerg Med. 1987;5:33-9.
5. Devise P. Cook County Hospital: bulwark of Chicago's apartheid health system. New Physician. 1971;20:394-8.
6. Frew SA, Roush WR, LaGreca K. COBRA: implications for emer- gency medicine. Ann Emerg Med. 1988;17:835-7.
7. Hudson T. New patient transfer amendments pose problems for hospitals. Hospitals. 1990;64:46-9.
8. Anonymous. New patient transfer laws take effect. ACEP News. 1990;9:13-9.
9. Anderson RJ, Cawley KA, Andrulis DP. The evolution of a public hospital transfer policy. Metropolitan Hospital. Chicago: Ameri- can Hospital Association, 1985;2(1).
10. American College of Emergency Physicians. Guidelines for trans- fer of patients. Ann Emerg Med. 1985;14:1221-2.
11. Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. 1975;23:433-41.
12. BionJF, Edlin SA, Ramsay G, McCabe S, Ledingham IM. Validation of a prognostic score in critically ill patients undergoing trans- port. Br MedJ. 1985;291:432-4.
13. Kellermann AL, Ackerman TF. Interhospital patient transfer: the case for informed consent. N EnglJ Med. 1988;319:643-6.
14. President's Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. Washington, DC: Government Printing Office, 1982;3:193-251.
15. Lidz CW, Meisel A, Osterweis M, HoldenJL, MarxJH, Munetz MR. Barriers to informed consent. Ann Intern Med. 1983;99:539-43.


















