Embed Size (px)
Citation preview

British Journal of Ophthalmology, 1980, 64, 206-210
Infantile cystoid maculopathyMICHAEL T. TRESE AND ROBERT Y. FOOSFrom the Department of Ophthalmology and the Department of Pathology,Jules Stein Eye Institute, UCLA School of Medicine, Los Angeles, USA
SUMMARY Three premature infants with no family history of eye disease showed bilateral cystoidmaculopathy on post-mortem examination. These macular lesions are indistinguishable macro-scopically from the macular lesions of sex-linked juvenile retinoschisis. Cystoid change was observedat various vertical retinal levels. The oldest child had a schisis cavity within the nerve fibre layer.All cases had reduced numbers of retinal ganglion cells and central nervous system (CNS) abnor-malities. The authors believe these are the first reported cases of a cystoid macular lesion presentat birth and the first description of the pathological features of a cystoid macular lesion in infants.
Cystoid macular change in infants is often a mani-festation of hereditary eye disease.' With a heredi-tary cause in mind it has been postulated thatthese macular lesions exist at birth, yet such anobservation has not been reported.2 At necropsywe have observed cystoid maculopathy in 3 pre-mature infants without a history of familial eyedisease. Similar macular changes have been notedclinically since at least 1898,3 yet the histopatho-logical features of this lesion in children havenever been described. This paper presents thesehistopathological features and reports the existenceof such a cystoid maculopathy at birth.
Materials and methods
The material for this study included both eyes from3 infants examined at necropsy either at the UCLACenter for the Health Sciences or at the Los AngelesCounty Harbor General Hospital over a 15-yearperiod. All eyes were taken within 2 to 6 hours ofdeath.
Preparation, gross sectioning, macroexamination,and recording of findings were performed accordingto our routine methods.' Microsections were pre-pared from celloidin-embedded eyes stained withhaematoxalin-eosin and peroidic acid Schiff tech-nique and alcian blue to determine the location andcontents of these spaces.
Correspondence to Robert Y. Foos, MD, Jules Stein EyeInstitute, UCLA School of Medicine, Los Angeles, Cali-fornia 90024, USA.
Case reports
CASE 1A black infant boy weighing 820 g was born to ahealthy 24-year-old woman. The pregnancy wasunremarkable. Fetal heart tones were present onadmission to hospital for delivery. Three generationsof family members were contacted by telephone andletter, and no history ofeye disease was found. Fatherand brother were examined and their eyes were foundto be normal. Delivery was complicated by prematurerupture of membranes. The child survived 11 daysbefore succumbing to respiratory distress syndrome.Supplemental oxygen therapy was necessary tomaintain a Po2 of between 21 and 177 mmHg.
Significant systemic necropsy findings wererestricted to immaturity of the white matter of thecentral nervous system.
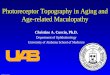
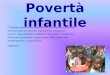
Ocular examination. The right eye measured14-2 mm (AP) X 14-8 mm (H) X 13-5 mm (V).The left eye measured 14-1 mm (AP) X 14-5 mm(H) X 13-6 mm (V). When incised, both eyesshowed cystoid changes in the maculae (Fig. 1).The peripheral retina and vitreous cavity wereunremarkable. On light-microscopical examinationnotable findings included bilateral cystoid changeconfined to the macula and involving predominantlythe outer nuclear layers. These cavities were out-lined by Muller cell pillars. The retinal ganglioncells were markedly reduced in number. Theperipheral retina was unremarkable (Fig. 2).
CASE 2This was a stillborn infant girl weighing 145 kg
206
on March 14, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.206 on 1 M
arch 1980. Dow
nloaded from

Infantile cystoid maculopathy
Fig. 1 Case 1. Macroscopicappearance of macular lesions.(A) Right eye showing multiplesmall cystoid change, radiallyarranged (x 18). (B) Left eyeshowing a more subtle similarlesion than (A) ( x 18).
born to a healthy 29-year-old Hispanic woman.
There was no family history of eye disease. Thedelivery was complicated by placental abruption.
Post-mortem examination revealed an anence-
phalic infant with a cervical meningomyelocele,who was otherwise appropriately developed forher birth weight.
Ocular examination. The right eye measured16-2 mm (AP) x 16-8 mm (H) X 16-6 mm (V);
the left eye 16-4 mm (AP) 16-8 mm (H) X 16-6 mm(V). The 2 eyes were unremarkable with the excep-
tion of cystoid lesions in the maculae. The peri-pheral retina and vitreous cavity were unremarkable.Except for the macular lesions both eyes were
unremarkable on microscopic examination. In themacula were moderately reduced numbers ofganglion cells and cystoid spaces that involved theinner nuclear layer. The Muller pillars were stretched
'limb.4-..O.- ~ ~~~~~~~~~~~~~~~~~~~~Va:; S..'
0A,
Fig. 2 Case 1. Microscopicappearance of macular lesions.(A) Right eye showing multiplecystoid spaces involving theouter nuclear layer (haematoxy-lin-eosin, x 142). (B) Left eye
showing less extensive cystoidmaculopathy (haematoxylin-eosin, x 142).
wEfhaUU:b:7jYl
,~J. . ... ....
2.lz.s ...<oOf. .k f: : . b
207
Sk
on March 14, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.206 on 1 M
arch 1980. Dow
nloaded from

Michael T. Trese and Robert Y. Foos
Fig. 3 Case 2. Macula showingextensive cystoid change in middleretinal layers with stretched andseemingly broken Muller pillars onleft. Note similarity to typical cystoiddegeneration ofperipheral retina(haematoxylin-eosin, x 146).
across these cavities (Fig. 3). The peripheral retinawas unremarkable.
CASE 3A white stillborn boy weighing 3-32 kg was bornto a healthy 25-year-old woman. There was nofamily history of eye disease. Fetal heart soundswere present when the mother arrived at the hospitalfor delivery. The pregnancy and delivery wereuncomplicated.The necropsy showed hydrocephalus, spina
bifida, and patent ductus arteriosus. The infant wasotherwise normal for his birth weight.
Ocular examination. Both eyes were large. Theright measured 21 2 mm (AP) x 19 0 mm (H) X19-9 mm (V); the left eye, 21-1 mm (AP) x 20-0 mm(H) X 18-8 mm (V). Both corneas measured 9-8mm (H) X 11 mm (V). When incised both eyesshowed large excavation of the optic nerve head.Central cystoid lesions and paracentral schisiscavities were observed within the macula in each
eye (Fig. 4). The peripheral retina and vitreouscavity were unremarkable.Both macular lesions in each eye were examined
microscopically. The more central lesion showedcystoid change within the nerve fibre layer. Asmall amount of haemorrhage was contained inone of these spaces (Fig. SA). The paracentrallesion was a large schisis cavity within the nervefibre layer, which had lost the radial support ofthe Muller pillars (Fig. 5B). The number of ganglioncells was moderately reduced. The anterior chamberangles were dysplastic. The peripheral retina andvitreous were unremarkable.
Discussion
These 3 cases show cystoid changes in the maculaeof both eyes. Cavitation was present at variousretinal levels and in the oldest infant large schisiscavities were within the nerve fibre layer. Macro-scopically these lesions are identical to the macular
Fig. 4 Case 3. Macula of lefteye showing central cystoidchange with Maller pillarsintact (white dots) andparacentral crescent-shapedarea of macular schisis withloss of Muller pillars ( x 17).
208
on March 14, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.206 on 1 M
arch 1980. Dow
nloaded from

Infantile cystoid maculopathy
Fig. 5 Case 3. Macula of lefteye. (A) Central lesion showingcystoid change within the nervefibre layer and Muller pillarsstretched across cavities. Notesimilarity to peripheral reticularcystoid degeneration (haema-toxylin-eosin, x 114). (B)Paracentral lesion showing lossof Muller pillars andformationof a large reticular-like(bullous) schisis cavity withinthe nerve fibre layer(haematoxylin-eosin, x 160).
lesions ofsex-X-linked retinoschisis, but in view of thenegative family history of eye diseases this diagnosisis unlikely. Since 50% of patients with sex-X-linkedretinoschisis have only macular lesions, however, thepossibility of a spontaneous genetic mutation mustbe considered., Some authors consider that cysticmacular change precedes peripheral retinoschisis.6Yanoff et al.7 postulated that the underlying
defect in sex-X-linked retinoschisis is in the innercytoplasm of Muller cells, which allows retino-schisis cavities to form. In our cases the Mullercells are stretched and broken across cystoid/schisiscavities, adding support to the hypothesis ofYanoff et al. As in hereditary juvenile retinoschisisthe retinal cavities in our cases contained no acid-mucopolysaccharide material. In all cases theperipheral retina was unremarkable.
It is well known that the peripheral retinoschisislesions of sex-X-linked retinoschisis tend to affectthe nerve fibre layer and cause large bullous thin-walled cavities extending into the vitreous.7-'0 Themacula of an affected child has never been described.Manschot1' has described the eyes of a 60-year-oldman who was a member of a family known tohave the gene for X-linked retinoschisis, andthese eyes showed wrinkling of the internal limiting
lamina and splitting of the nerve fibre layer withnormal underlying retinal tissue. Our eyes showedreduced ganglion cells seemingly related to thepatients' concomitant CNS changes.Von Sallman12 pointed out that generalised
retinal cystoid changes and even splitting of thenerve fibre layer can be produced by prepartumcompromise of the carotid jugular circulation inrhesus monkeys. These lesions, although extensive,did not involve the macula. In our cases there is noevidence, from the general necropsy data or fromthe ocular pathological findings to support anischaemic aetiology for the selective macularlesions seen in these 3 infants. In all cases retinalganglion cells were reduced in number. All childrenhad central nervous system abnormalities, whichmay relate to the poorly developed ganglion celllayer. One case had a patent ductus arteriosusseemingly unrelated to the ocular changes. Theauthors have been unable to determine if theseretinal and CNS lesions are meaningfully associatedor if the CNS lesions only allow the fortuitousnecropsy study of these eyes.This work was supported in part by Public Health ServiceGrants EY-00725 and EY-00331 from the National EyeInstitute, National Institutes of Health.
-20-9
SW
on March 14, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.206 on 1 M
arch 1980. Dow
nloaded from

Michael T. Trese and Robert Y. Foos
References
1Deutman AF. The Hereditary Dystrophies of the PosteriorPole of the Eye. Assen, The Netherlands: Royal Vangor-cum, 1971; 48-99.2Kraushar MF, Schepens CL, Kaplan JA. Congenitalretinoschisis. In: Tolentino Fl, Schepens CL, FreemanHM, eds. Vitreoretinal Disorders, Diagnosis, and Manage-ment. Philadelphia: Saunders, 1976; 249-59."Haas J. Ueber das Zusammenvorkommen von Vernd-derungen der Retina und Chorioidea. Arch Augenheilk1898; 37: 343-8.4Roth AM, Foos RY. A system for the macroexaminationof eyes in the laboratory. Am J Clin Pathol 1973; 59:674-83.'Krill AE. Hereditary Retinal and Choroidal Diseases.New York: Harper and Row, 1977; 2: 1044-62.
"Harris GS. Juvenile sex-linked retinoschisis. Mod ProbiOphthalmol 1969; 8: 363-70.7Yanoff M, Kertesz E, Zimmerman LE. Histopathologyof juvenile retinoschisis. Arch Ophthalmol 1968; 79: 49-53.8Yanoff M, Fine B. Ocular Pathology: A Text and Atlas.New York: Harper and Row, 1975; 416-32.9Hogan M, Zimmerman LE. Ophthalmic Pathology: AnAtlas and Textbook. Philadelphia: Saunders, 1962; 535-7.°0Zimmerman LE, Naumann G. The pathology of retino-schisis. In: New and Controversial Aspects of RetinalDetachment. McPherson A, ed. New York: Hoeber,1968; 400-23.uManschot WA. Pathology of hereditary juvenile retino-schisis. Arch Ophthalmol 1972; 88: 131-8.
12Von Sallman L. The effect of intrauterine surgical proce-dures on the development of the primate eye. InvestOphthalmol 1969; 8: 51-60.
210
on March 14, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.206 on 1 M
arch 1980. Dow
nloaded from





![Assessment report - ema.europa.eu › en › documents › variation... · (ie, cystoid ME [CME]). ME and cystoid macular oedema (CME) are common causes of poor visual outcome following](https://img.dokumen.tips/doc/110x75/5f1f96e2bf8ab064bd6ec5c9/assessment-report-ema-a-en-a-documents-a-variation-ie-cystoid-me.jpg)