Embed Size (px)
Citation preview

© 2018 The Council of State Governments Justice Center
Incorporating Gender-Responsive Services Into Specialty Courts
Adult and Juvenile Courts
June 1, 2018

Speakers• Jeannie Von Stultz, Ph.D., Deputy Chief - Mental
Health Services, Bexar County Juvenile Probation• Jamie Vaske, Ph.D., Associate Professor,
Department of Criminology & Criminal Justice, Western Carolina University
• Sarah Wurzburg, Deputy Program Director, Behavioral Health, The Council of State Governments Justice Center
2

Overview
• Gender-Responsive Services
• Survey of Adult Gender-Responsive Courts
• Girls and Boys Mental Health Courts in Bexar County, TX
3

4
National nonprofit, nonpartisan membership association of state government officials
Represents all three branches of state government
Provides practical advice informed by the best available evidence
4

5

Mission of the JPLI• The Judges’ and Psychiatrists’ Leadership Initiative (JPLI) aims to stimulate, support, and enhance
efforts by judges and psychiatrists to improve judicial, community, and systemic responses to people with behavioral health needs who are involved in the justice system.
6
Creating a community of judges and psychiatrists
Increasing the reach of trainings
Developing educational resources
Three Judges’ Guides
Subscribe to the JPLI Newsletter

Resources
7
https://csgjusticecenter.org/courts/judges-leadership-initiative/

Gender-Responsive Approach
Definition:
“Creating an environment through site selection, staff selection, program development, content and material that reflects an understanding of the realities of women’s lives, and is responsive to the issues of the clients.”
(Covington, S., 2007)
Council of State Governments Justice Center | 8
Covington, S. (2007) Women and addiction: A gender-responsive approach (the clinical innovators services). Center City, MN: Hazeldon.

Utilize a Multi-Faceted APPROACH
RelationalDevelop policies, practices, and programs that
are relational and promote healthy connections
Strengths-Based
Create an environment based on
safety, respect, and dignity
Trauma-Informed
Address substance abuse, trauma,
and mental health issues
Culturally CompetentProvide women with opportunities
to improve their socioeconomic conditions
HolisticEstablish a system of community supervision and
reentry with comprehensive, collaborative services
The Five CORE Practice Areas of Gender Responsiveness, CORE Associates
The National Resource Center for Justice Involved Women. Effective Strategies to Meet the Unique Needs of
Justice Involved Women. Developed February 2016.

Sex and Gender Differences • “Sex” and “gender” do not mean the same thing.
• Sex differences are related to biology.
• Gender is part of a person’s self-representation. It relates to culturally defined characteristics of masculinity and femininity.
• There are both sex and gender differences that relate to SUDs and SUD treatment for men and women.
• Slide 7
SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use Disorders Tool
Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.

Telescoping and Other Sex-related Differences
Telescoping, in this use of the term, refers to an effect whereby women “progress faster than men from initial use to alcohol- and drug-related problems, even when using a similar or lesser amount of substances.”
(Substance Abuse and Mental Health Services Administration [SAMHSA], 2009, p. 27; Piazza et al., 1989)
• Slide 8
SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use Disorders Tool
Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.

Gender Differences
• Factors such as culture, age, socioeconomic status, religion, disability, race/ethnicity, and sexual orientation all influence gender roles and expectations.
• Some gender traits are common, but none are absolute.
• Slide 9
SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use Disorders Tool
Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.

Sex and Gender Differences Related to SUDs
Women often differ from men in their:
• Pathways to substance use
• Risk factors for use
• Consequences of use
• Barriers to treatment/recovery
• Recovery support needs
• Slide 12
SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use Disorders Tool
Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.

Activity
Women and Men

Past Year Treatment for Depression Among Adolescents Aged 12–17 with Major Depressive Episode (MDE) in the United States, by Gender (2014)
15Source: SAMHSA, Center for Behavioral Health Statistics and Quality, National Survey on Drug Use and Health, 2014.

16
Source: SAMHSA, Center for Behavioral Health Statistics and Quality, National Survey on Drug Use and Health, 2014.

• Prisoners were 3 times more likely to have SPD than the total adult general population (GP).
• Jail inmates were 5 times more likely to have SPD than the total adult GP.
• Female prisoners and jail inmates were more likely than males to have an indicator of a mental health problem.
Bronson, J. Berzofsky, B. Indicators of Mental Health Problems Reported by Prisoners and Jail Inmates, 2011-12Bureau of Justice Statistics. June 2017. Retrieved from: https://www.bjs.gov/content/pub/pdf/imhprpji1112.pdf

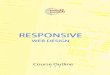
Substance Use: Women vs. MenWomen have lower rates of substance use and SUDs than men.
8.510.2
3.44.43.3
1.9
0
2
4
6
8
10
12
past yearalcohol
dependence
past monthheavy alcohol
use
past year illicitdrug
dependence orabuse
men
womenP
erce
nta
ge
Source: Substance Abuse and Mental Health Services Administration. (2015a). Behavioral health barometer: United States, 2015. HHS Publication No. SMA-16-Baro-2015. Rockville, MD: Substance Abuse and Mental Health Services Administration.
SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use Disorders Tool
Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.

www.bjs.gov
• 58% of state prisoners and 63% of sentenced jail inmates met the DSM-IV criteria for dependence or abuse. This compared to about 5% of the total general population.
• A larger percentage of females than males used drugs in the month before the offense.
19
Bronson, J. Stroop, J. Zimmer, S. Berzofksy, M. Illicit Drug Use, Dependence, and Abuse Among State Prisoners and Jail Inmates, 2007-09. June 2017. Retrieved from: https://www.bjs.gov/content/pub/pdf/dudaspji0709.pdf.

Protective Factors for Girls/Young Women
• Feeling connected to family, cared about, and supported; high parental warmth
• Parent disapproval of substance use
• Religious/spiritual practices
• Coping skills
SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use Disorders Tool
Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.

History of Women’s Services
Generic Treatment 1960s
1970s
Gender
Differences
Gender Specific
1980s
1990s-
2000s
Gender
Responsive
Council of State Governments Justice Center | 21
Grella, C. From Generic to Gender-Responsive Treatment: Changes in Social Policies, Treatment Services, and Outcomes of Women in Substance Abuse Treatment. Journal of Psychoactive Drugs. 5 November 2008.

Substance Use, Trauma, and Mental Health Cycle
© Institute for Health and RecoveryAdapted from: SAMHSA Addressing the Gender-specific Service Needs of Women with Substance Use
Disorders Tool Kit, MODULE 1 Women, Substance Use, and Substance Use Disorders (SUDs), 2017.
Criminal Justice

Women in the Justice System
• Increase in number of women incarcerated • While rest of the population is declining
• Women offenders are:• Low-income
• Undereducated
• Unskilled with sporadic employment
• Disproportionately women of color
• Less likely to have committed a violent crime
Council of State Governments Justice Center | 23
Bloom, B., Covington, S., Messina, N., Selvaggi, K., Owen, B. Gender-Responsive Policy and Practice Assessment Manual. February 18, 2014 for National Institute of Corrections.

Core Competencies: Women and Girls
• Sex and gender differences
• Relational approach in working with women and girls
• Understanding trauma in women and girls
• Family-centered needs of women and girls
• Special considerations during pregnancy
• Women’s health and healthcare
• Collaboration and interdisciplinary effectiveness
Council of State Governments Justice Center | 24
Substance Abuse and Mental Health Services Administration (2011). Addressing the Needs of Women and Girls: Developing Core Competencies for Mental Health and Substance Abuse Service Professionals. HHS Pub. No. (SMA) 11-4657. Rockville, MD: Substance Abuse and Mental Health Services Administration.

Council of State Governments Justice Center | 25
Co-Occurring Disorders Treatment
Trauma-informed
Culturally Competent
Integrated Care
Strengths-based
Gender-responsive
Recovery-oriented
Family-centered
Person-centered
Adapted from Wurzburg, S. Zentgraf, K. Russell, C. State Adolescent Substance Use Treatment Practice Guide. In review, 2014.

Overview
• Gender-Responsive Services
• Survey of Adult Gender-Responsive Courts
• Girls and Boys Mental Health Courts in Bexar County, TX
26

Introduction to Adult Gender-Responsive Courts
• Two approaches
– Female only docket or court
– Prostitution or human trafficking courts
• Greater attention to gender-responsive courts
– Legislation
– Outcome evaluations of female only DTCs
27

Despite Growing Attention…
• Do not know:
– Eligibility and screening criteria
– Requirements and procedures
– How can we improve upon these courts
28

Current Project
29

Female-Only Courts: Entry
30
Female-only courts
Eligibility Females onlyModerate to high riskNon-violentSUD
Identification Arraignment, probation, or treatment providers
Screening Treatment providerGender-neutral assessment

Female-Only Courts: Structure
31
Female-only courts
Length 18 months
Requirements Traditional problem solving court requirements (supervision, treatment, court appearances)
Mentors Available but not required by all

32
100%
100%
100%
100%
100%
100%
50%
50%
50%
0%
Mental health
Substance use
Trauma
Housing
Parenting skills
Physical health
Social support
Employment
Education
Family relations

Prostitution Diversion Courts
33
Prostitution diversion courts Female-only courts
Eligibility All gendersAll risk levelsNon-violentSUD or No SUDTraffic offenses
Females onlyModerate to high riskNon-violentSUD
Identification Initial appearance, booking, arraignment
Arraignment, probation, or treatment providers
Screening Treatment provider, Coordinator, Pretrial
Gender-neutral assessments
Treatment provider
Gender-neutral assessment

34
Prostitution diversion courts Female-only courts
Length 3 - 12 months 18 months
Requirements Varies Traditional problem solving court requirements
(supervision, treatment,court appearances)
Mentors Available but not required Available but not required

Other Observations
• Tracking program dropout
• Incentives
• Sanctions
35

Benefits• Increased collaboration between
judicial services and treatment providers
• Increased supervision and treatment of high-risk, transient clients
• Reductions in recidivism and increased reunification of parents with children
• Clients experience significant increases in perceived procedural justice
Challenges• Stable funding mechanisms and
reductions in key staff members
• Identifying gender-responsive, culturally-sensitive treatment providers
• Disproportionate minority contact in program participation and termination
•• Disagreement in treatment goals
between clients and treatment team
36

Recommendations
• Sustainability of programs and clients’ needs
• Conduct a needs assessment of community programs prior to implementation
• Ground policies and procedures in NADCP’s Best Practice Standards and gender-responsive principles
37

Treatment Courts Best Practice Inventory
38

Overview
• Gender-Responsive Services
• Survey of Adult Gender-Responsive Courts
• Girls and Boys Mental Health Courts in Bexar County, TX
39

Gender Specific Court Models
• Crossroads Court
– Girls Mental Health Court
– Pre-Adjudication Specialty Court
– First-time non-violent offenders
– Ages: 12-16
– History of Mental Health issues and Trauma
40

Gender Specific Court Models
• MIND (Males in Need of Direction) Court
– Boys Mental Health Court
– Pre-Adjudication Specialty Court
– First-time non-violent offenders
– Ages: 12-16
– History of Mental Health issues
41

Program Comparisons
42
DIFFERENCES MIND Court (Males) Crossroads Court (Females)
Presenting Problem Physically aggressive behavior Risky behaviors
Bullying (Bullied and Bullier) Running away, older peer associates
Underlying Issues Low emotional maturity Pseudo-emotional maturity
Reactive Strategic
Hypervigilant of school/home behavior Hypervigilant regarding social relationships & activities
Parental enmeshment Parental disengagement
Program Structure Less structured program increases accountability More structured program increases accountability
Supervision Issues More often at home or at friend’s home More often out in community – location unknown
Substance use – minimal to moderate testing Substance use – minimal to moderate testing
Individual Treatment Focus Emotional Regulation Emotional Attachment
Anger management Trauma-focused treatment
Impulse control Risk behavior reduction
Culture of males
Skills Training Focus Personal and social relationships (maintaining friendships) Personal & social relationships (healthy relationships)
Emotional Regulation Health & safety
Problem-solving Independent living skills
Stress management Life decisions and responsibilities
“Joven Noble”
Family Treatment Focus Strengthen family structure Strengthen family attachment
Strengthen boundaries Strength-focused communication
Equine Therapy Focus “Running with Mustangs” “Girls Rule”
Self-regulation Assertiveness
Internal and external triggers Boundaries
Observation and Environmental Cues Problem Solving Styles and Communication
Awareness of Thoughts and Internal Dialogue Positive Body Image
Problem Solving Obstacles and Distractions
Changing negative thought patterns Family Roles
Objective Perspective of Others and Empathy Leadership and Empowerment

Program ComparisonsDIFFERENCES (continued) MIND Court (Males) Crossroads Court (Females)
Program Strategies Monitor group dynamics - alpha male Monitor group dynamics – alliances/cliques
Male probation officer fosters role modeling Female probation officer fosters role modeling
Male case manager fosters open discussions Female treatment providers foster open discussions
Pregnancy Prevention Efforts Empower to accept limits (OK to go slow) Empower to set limits (Ok to say no)
Healthy relationships Healthy relationships
Long acting reversible contraceptives
Incentives Focused on graduation not phases Focused on phase advancement
Dress shirt/tie – Viewed as rite of passage Symbolic graduation blanket
Prefers gift cards Phase One watch
Pillows
Activities Minor league baseball games Amusement park
Hockey games Water park
Bowling College tours
Structured art therapy Process art therapy
Creative writing
SIMILARITIES
Need help with basic needs such as food/utilities/transportation/housing (more so for males)
Need help connecting to community treatment services
Parent/child benefit from psychoeducation regarding mental health diagnoses and treatment
Benefit from advocacy and support during ARD (Assessment, Review and Dismissal) Process
Child and Parent benefits from communication and interpersonal skills training
Child and Parent benefits from time and money management training
Child benefits from vocational readiness training
43

Presenting Problem
• MIND Court (Boys)
– Physically aggressive
– Bullied or bullying
• Crossroads (Girls)
– Risky behaviors
– Running away
– Older peer associates
44

Underlying Issues
• MIND (Boys)
– Low emotional maturity
– Reactive
– Hypervigilant of school/home behavior
– Parental enmeshment
• Crossroads (Girls)
– Pseudo-emotional maturity
– Strategic
– Hypervigilant of social relationships/activities
– Parental disengagement
45

Program Structure
• MIND (Boys)
– Less structured program increases accountability
• Crossroads (Girls)
– More structured program increases accountability
46

Supervision Issues
• MIND (Boys)
– More often at home or at friend’s home
– Substance Use: minimal - moderate testing
• Crossroads (Girls)
– More often out in community
– Location unknown
– Substance Use: minimal – moderate testing
47

Individual Treatment Focus
• MIND (Boys)
– Emotional Regulation
– Anger Management
– Impulse Control
– Culture of Males
• Crossroads (Girls)
– Emotional Attachment
– Trauma-focused Treatment
– Risk Behavior Reduction
48

Skills Training Focus
• MIND (Boys)– Personal/social
relationships (maintain friendships)
– Emotional regulation
– Problem-solving
– Stress management
– Joven Noble
• Crossroads (Girls)– Personal/social
relationships (healthy relationships)
– Health and safety
– Independent living skills
– Life decisions and responsibilities
49

Family Treatment Focus
• MIND (Boys)
– Strengthen family structure
– Strengthen boundaries
• Crossroads (Girls)
– Strengthen family attachment
– Strength-focused communication
50

Equine Therapy Focus
• MIND (Boys)
– “Running with Mustangs”
– Self-regulation
– Internal/external triggers
– Observation and
environmental cues
• Crossroads (Girls)
– “Girls Rule”
– Assertiveness
– Boundaries
– Problem solving styles and communication
– Positive body image
51

Equine Therapy Focus
• MIND (Boys)– Awareness of thought
and internal dialogue
– Problem solving
– Changing negative thought patterns
– Objective perspective
of others and empathy
• Crossroads (Girls)– Obstacles and
distractions
– Family roles
– Leadership and empowerment
52

Program Strategies
• MIND (Boys)
– Monitor group dynamics (alpha male)
– Male probation officer fosters role modeling
– Male case manager fosters open discussions
• Crossroads (Girls)
– Monitor group dynamics (alliances/cliques)
– Female probation officer fosters role modeling
– Female treatment providers fosters open discussions
53

Pregnancy Prevention Efforts
• MIND (Boys)
– Empower to accept limits (OK to go slow)
– Healthy relationships
• Crossroads (Girls)
– Empower to set limits (OK to say no)
– Healthy relationships
– Long acting reversible contraceptives
54

Incentives
• MIND (Boys)
– Focused on graduation not phases
– Dress shirt/tie (Rites of Passage)
– Prefers gift cards
• Crossroads (Girls)
– Focused on phase advancement
– Symbolic graduation blanket
– Phase I watch
– Pillows
55

Activities
• MIND (Boys)
– Minor League Bball
– Hockey games
– Bowling
– Structure art therapy
• Crossroads (Girls)
– Amusement park
– Water park
– College tours
– Process art therapy
– Creative writing
56

Similarities
• Assistance with basic needs (food, utilities, transportation, housing)
• Connecting to community-based treatment services
• Psychoeducation re: mental health
diagnoses and treatment (parent & child)
57

Similarities
• Advocacy and support during ARDs
• Communication and interpersonal training (parent and child)
• Time and money management training (parent and child)
• Vocational readiness training (child)
58

Questions and Answers
59

Key Resources: Gender-Responsive Services
• Addressing the Needs of Women and Girls: Developing Core Competencies for Mental Health and Substance Abuse Service Professionals: https://store.samhsa.gov/shin/content/SMA11-4657/SMA11-4657.pdf
• Bloom, B., Covington, S., Messina, N., Selvaggi, K., Owen, B. Gender-Responsive Policy and Practice Assessment Manual. February 18, 2014 for National Institute of Corrections.
• Ten Truths That Matter When Working With Justice Involved Women: http://cjinvolvedwomen.org/wp-content/uploads/2015/09/Ten_Truths.pdf
• Mandell, Kara, and Werner, Deborah, “Guidance to States: Treatment Standards for Women with Substance Use Disorders,” National Association of State Alcohol and Drug Abuse Directors, 2008. http://nasadad.org/wp-content/uploads/2010/12/Guidance-to-States-Treatment-Standards-for-Women1.pdf
• SAMHSA TIP 56: Addressing the Specific Behavioral Health Needs of Men: https://store.samhsa.gov/shin/content/SMA14-4882/SMA14-4882.pdf
60

Key Resources: TraumaWebsites
• National Center for Trauma Informed Care: http://www.nasmhpd.org/TA/nctic.aspx• National Institute of Corrections, Women Offenders: http://nicic.gov/womenoffenders• The National Resource Center on Justice Involved Women: http://www.cjinvolvedwomen.org• SAMHSA, Trauma and Justice Initiative: http://www.samhsa.gov/traumajustice/Publications
• SAMHSA TIP 57: Trauma-Informed Care in Behavioral Health Services: http://store.samhsa.gov/product/TIP-57-Trauma-Informed-Care-in-Behavioral-Health-Services/SMA14-4816
• SAMHSA Creating a Trauma Informed Criminal Justice System for Women: http://www.nasmhpd.org/docs/NCTIC/Women%20in%20Corrections%20TIC%20SR.pdf
• Blanch, A. Filson, B. Penney, D. Engaging Women in Trauma-Informed Peer Support: A Guidebook: http://www.nasmhpd.org/publications/engagingwomen.aspx
• Braude, L. & Miller, N. RSAT Training Tool: Understanding Co-occurring Disorders and Applying Integrated Treatment Strategies for Adult Correctional Populations: http://www.rsat-tta.com/Training-Curricula/Curricula
Council of State Governments Justice Center | 61

learning.csgjusticecenter.org
Developing a Mental Health Court is a free multimedia curriculum for individuals and teams seeking to start, maintain, or just learn about mental health courts or other criminal justice/mental health collaborations.
Developing a Mental Health Court: An Interdisciplinary Curriculum
CSG
Ju
stic
e C
ente
r

https://csgjusticecenter.org/mental-health/learning-sites/
Criminal Justice/Mental Health Learning Sites

Contact Information Jamie Vaske, Ph.D., Associate Professor, Department of Criminology & Criminal Justice, Western Carolina University [email protected]
Jeannie Von Stultz, Ph.D., Deputy Chief -Mental Health Services, Bexar County Juvenile Probation [email protected]
Sarah Wurzburg, Deputy Program Director, Behavioral Health, The Council of State Governments Justice Center
64

The presentation was developed by members of The Council of State Governments Justice Center staff. The statements made reflect the views of the authors, and should not be considered the official position of The Council of State Governments Justice Center, the members of The Council of State Governments, or the funding agency supporting the work.
Join our distribution list to receive CSG Justice Center updates and announcements!
www.csgjusticecenter.org/subscribe

© 2018 The Council of State Governments Justice Center
Behavioral Health Diversion Interventions
Moving from On-Off Programs to a System-Wide Strategy
June 1, 2018

Speakers
• Honorable Stephen GossDOUGHERTY JUDICIAL CIRCUIT SUPERIOR COURT, GEORGIA
• Sarah Wurzburg, Deputy Program Director, Behavioral Health THE COUNCIL OF STATE GOVERNMENTS JUSTICE CENTER
2

Overview
• Challenges in the Field
• What is Diversion?
• Moving from One-Off Program to a Systems Strategy
3

4
National nonprofit, nonpartisan membership association of state government officials
Represents all three branches of state government
Provides practical advice informed by the best available evidence
4

Behavioral Health at the CSG Justice Center
Council of State Governments Justice Center | 5
Criminal Justice / Mental Health
Consensus Project
police chiefs | consumers | pretrial service
administrators | probation officials | state legislators |
substance abuse providers | state corrections directors |
judges | district attorneys | families | parole board
members | county executives | public defenders | crime
victims | state corrections directors | prosecutors | mental health
advocates | court administrators | mental health providers | researchers
| jail administrators | sheriffs | correctional mental health providers |
state mental health directors | victim advocates | parole officials
Criminal Justice/Mental Health
Learning Sites Program

Mission of the JPLI• The Judges’ and Psychiatrists’ Leadership Initiative (JPLI) aims to stimulate, support, and enhance
efforts by judges and psychiatrists to improve judicial, community, and systemic responses to people with behavioral health needs who are involved in the justice system.
6
Creating a community of judges and psychiatrists
Increasing the reach of trainings
Developing educational resources
Three Judges’ Guides
Subscribe to the JPLI Newsletter

Resources
7
https://csgjusticecenter.org/courts/judges-leadership-initiative/

Addressing a National Crisis of Too Many People with Mental Illnesses in Jails

An Unprecedented Response
More than 430 counties across 43 states, representing 40% of the U.S. population, have resolved to reduce the
number of people with mental illnesses in jails.
Council of State Governments Justice Center | 9

The Stepping Up Initiative’s Data-Driven Approach to Systems Change
1. Is your leadership committed?2. Do you have timely screening and assessment?3. Do you have baseline data?4. Have you conducted a comprehensive process analysis and
service inventory?5. Have you prioritized policy, practice, and funding?6. Do you track progress?
The number of people with SMI booked into jail
Reduce
1
ShortenThe average length of stay for people SMI in jails
2
IncreaseThe percentage of connection to care for people with SMI in jail
3
LowerRates of recidivism
4
Six Questions County Leaders Need to Ask
Strategies Should Focus on Four Key Measures
Council of State Governments Justice Center | 10

Framework for Police-Mental
Health Collaborations
Is our leadership committed to the police-mental health collaboration (PMHC)?
Are we following clear protocols to respond to people who have mental illnesses?
Are we providing staff with quality mental health and de-escalation training?
Do we have the resources and service connections for people who have mental illnesses?
Do we collect and analyze data?
Do we have a process for reviewing and improving performance?
Council of State Governments Justice Center | 11

Primary Practice-Level Challenges
• Targeting Interventions Based on BH Needs and Criminogenic Risk
• Assessing serious mental illnesses, substance use disorders, and criminogenic risk factors in courts and correctional facilities
• Targeting and tailoring appropriate services and supervision based on level of needs and risk
• Incorporating Assessment Information into Case Plans
• Utilizing the assessment information for BOTH behavioral health criminogenic risk in case plans
• Defining lead case planner at an agency and outlining case conferencing procedures
• Knowing When to Refer to Which Intervention
• Taking the assessment information to guide program referral such as cognitive behavioral intervention
Council of State Governments Justice Center | 12

Primary Systems-Level Challenges
• Quantification of Needs Using Data
• Systematic identification of people with behavioral health needs by courts and corrections, using validated tools and standard definitions of mental illness and SUDs
• Accurate data collection and reporting on prevalence, entries, length of stay, and connections to treatment
• Identifying System Improvements and Treatment Gaps Using Data
• Selecting strategies and designing programs based on projected impact on key outcome measures
• Specifying gaps in community-based services and treatment based on data on connections to care
Council of State Governments Justice Center | 13

Use of data to identify and prioritize systems improvements
14
Jurisdiction Metric Finding Action Taken
Bexar County, Texas
The number of people with mental illnesses in jail
County does not know how many people with mental illnesses are in the jail.
Bexar County established universal screening for mental illnesses.
New York City, New York
Length of stay
People with mental illnesses stayed in jail 112 days on average as compared to 61 days for those without mental illnesses.
New York City implemented early pretrial diversion options to move people with mental illnesses out of jail in a timely way.
Franklin County, Ohio
Connection to care post- release
More than one in three of people who had contact with the behavioral health care system in the year prior to their incarceration did not have contact with the behavioral health care system in the year following their release from jail.
The local Alcohol Drug And Mental Health (ADAMH) board establisheda jail liaison team to provide in-reach service to get follow-up appointments within two weeks of release.
Salt Lake County, Utah
Recidivism rate
One out of three people on pretrial supervision and one out of two people on county probation did not fulfill the requirements of their supervision.
Salt Lake County recommendations included establishing intensive supervision caseloads for people who are assessed as being moderate to high risk of reoffending and who are also assessed as having an SMI.

What does the term diversion mean to you?

Behavioral Health Diversion Terms
• Diversion
• Jail Diversion
• Deflection
• Early Intervention

What is Behavioral Health Diversion?
• Jail diversion is a community-based, collaborative criminal justice–mental health response for justice-involved people with mental illnesses where jail time is reduced or avoided, and the individual is linked to comprehensive and appropriate services.
– Judges’ Criminal Justice/Mental Health Leadership Initiative. (2010). Judges’ guide to mental health diversion: A reference for justice system practitioners. Delmar, NY: Policy Research Associates, CMHS National GAINS Center.

Behavioral Health Diversion Intervention• This term includes common name brand programs (like
LEAD) and local practices (e.g., court processes that lead to a diversion-related outcome). These programs and practices share the following diversion-related goals: (1) connecting people who have behavioral health needs to treatment and support services, and (2) reducing or eliminating jail time by exploring alternatives to traditional case processing.
18

Behavioral Health Diversion Strategy
• Diversion strategies that address systems enhancements
• Opportunities for diversion at multiple intercept points– Ability to divert eligible individuals at different points in the criminal
justice system
• For those not eligible for diversion providing providing reentry services that include connection to behavioral health services in the community

Discussion Questions
• Do you consider your specialty court diversion?
• Do you know about other diversion interventions in the court system?
• Is there a larger strategy across agencies in the criminal justice system for people with BH needs?
20

Challenges to Developing Continuum of Diversion Responses
• No clear “common” language standards for diversion related terminology
• Diversion programs and practices constantly evolving
• No clear strategies on how to build diversion opportunities throughout the criminal justice system

Key Questions• What is behavioral health diversion?
– Providing definition for diversion
• How is a system of diversion developed? – Key components needed for strategic development
• What are options for behavioral health diversion? – Describing common BH diversion interventions,
programs/practices
• How do you develop multiple diversion options for your systems?– Key components tailored for each subpart of system (LE,
pretrial, courts, jails)

Overview
• Challenges in the Field
• What is Diversion?
• Moving from One-Off Program to a Systems Strategy
23

Agency-Specific Diversion Interventions
• Programs and practices that are designed to divert people at specific process-oriented phases (i.e., pre-arrest, pre/post-booking, and pre-trial) and implemented by the main agency that has the best opportunity and resources.
24

Continuum of BH Diversion Interventions
• A range of behavioral health diversion programs and practices that span a community’s criminal justice system—starting from first contact with law enforcement (arrest) through incarceration.
25

Behavioral Health Diversion Decision Points

Behavioral Health Diversion Options

Multiple Behavioral Health Diversion OptionsLaw Enforcement Considerations Pretrial Considerations Court Considerations Jail Considerations
Is our leadership committed to the police-mental health collaboration (PMHC)?
Are we following clear protocols to respond to people who have mental illnesses?
Are we providing staff with quality mental health and de-escalation training?
Do we have the resources and service connections for people who have mental illnesses?
Do we collect and analyze data?
Do we have a process for reviewing and improving performance?
Engage stakeholders
Identify target population
Conduct a comprehensive process analysis and inventory of services
Identify and leverage funding streams
Information sharing
Track progress
Engage stakeholders
Identify target population
Conduct a comprehensive process analysis and inventory of services
Identify and leverage funding streams
Information sharing
Track progress
Is our leadership committed?
Do we conduct timely screening and assessments?
Do we have baseline data?
Have we conducted a comprehensive process analysis and inventory of services?
Have we prioritized policy, practice, and funding improvements?
Do we track progress?
Specific questions are in development

Behavioral Health Diversion Continuum Components
• Engage stakeholders
• Identify target population
• Conduct a comprehensive process analysis and inventory of services
• Identify and leverage funding streams
• Information sharing
• Track progress

A Framework for Prioritizing Resources
30
Subgrouping B
High criminogenic risk/ some significant BH treatment needs
Prioritize for intensive supervision (in lieu of incarceration or as condition of release) coordinated with appropriate treatment and supports
Subgrouping A
Low criminogenic risk/ some significant BH treatment needs
Divert from criminal justice system without intensive community supervision if connected to appropriate treatment and supports

Collaborative Case Planning1. Interagency Collaboration and Information-Sharing
2. Staff Training
3. Screening and Assessment
4. Case Conference Procedures
5. Participant Engagement
6. Prioritized Needs and Goals
7. Responsivity
8. Legal Information
9. Participant Strengths
10. Gender Considerations
31
https://csgjusticecenter.org/nrrc/collaborative-comprehensive-case-plans/

Goal of BH Diversion Resources• Provide information on diversion • Agency-specific information on possible interventions
– Law enforcement– Courts– Pretrial – Jails
• Assist jurisdictions to develop, or modify, a continuum of diversion responses for people with behavioral health disorders in the criminal justice system – identification of BH issues, – alternatives to traditional case processing, – reduction or avoidance of jail time, and – linkage to comprehensive and appropriate community-based services.

Questions and Answers
33

Resources
34

learning.csgjusticecenter.org
Developing a Mental Health Court is a free multimedia curriculum for individuals and teams seeking to start, maintain, or just learn about mental health courts or other criminal justice/mental health collaborations.
Developing a Mental Health Court: An Interdisciplinary Curriculum
CSG
Ju
stic
e C
ente
r

https://csgjusticecenter.org/mental-health/learning-sites/
Criminal Justice/Mental Health Learning Sites

Contact Information Judge Stephen Goss,Dougherty Judicial Circuit Superior Court, Georgia [email protected]
Sarah WurzburgDeputy Program Director, Behavioral Health The Council of State Governments Justice [email protected]
37

The presentation was developed by members of The Council of State Governments Justice Center staff. The statements made reflect the views of the authors, and should not be considered the official position of The Council of State Governments Justice Center, the members of The Council of State Governments, or the funding agency supporting the work.
Join our distribution list to receive CSG Justice Center updates and announcements!
www.csgjusticecenter.org/subscribe