Embed Size (px)
Citation preview
INCIDENT REPORTING AND
MANAGEMENT POLICY

2
Policy Title:
Incident Reporting and Management Policy
Executive Summary:
East Cheshire NHS trust is committed, through its Health and Safety and Risk Management Policies, to the maintenance of safe working practices and the provision of an environment, which is safe for staff, patients and others; in accordance with good clinical practice and the requirements of Health and Safety, Fire Safety, Security and Environmental Legislation. This policy applies to all staff employed by East Cheshire NHS trust. This policy relates to the requirement of all personnel employed in all areas of the trust to report all untoward events, including near misses, regardless of whether they involve patients, visitors, staff or contractors. The reporting of untoward events is an integral part of the trust’s risk management strategy, which has a goal of identifying and then removing, or reducing to an acceptable level all risks across the organisation. The reporting and subsequent management of the incidents reported will allow the trust to put measures in place to reduce or eliminate the likelihood of recurrence and allow the organisation to learn from previous incidents and experiences.
Supersedes: Policy for the Management and Investigation of Incidents Including the Analysis of Data
Description of Amendment(s):
Rewritten policy using new trust board template Guidance on reporting removed from policy and in a supporting document. Process for serious incident reporting and investigation removed from policy and in a supporting document.
This policy will impact on: All staff working within the trust.
Financial Implications: None
Policy Area: Trust Wide Document Reference:
ECT002967
Version Number: 4.0 Effective Date: May 2018
Issued By: Director of Corporate Affairs and Governance
Review Date: May 2021
Author: Head of Safety and Risk Impact Assessment Date:
14th May 2018
APPROVAL RECORD
Committees / Group Date
Consultation: Risk Management Sub-committee 15th May 2018
Approved by Director: Director of Corporate Affairs and Governance
15th May 2018
Ratified by: Risk Management subcommittee 15th May 2018
Received for information Action
Clinical Directors, Deputy Directors and Heads of Service
5th June 2018

3
Incident Reporting and Management Policy
Table of Contents
XXXXX
Page x
1. Introduction
Page 4
2. Objective
Page 4
3. Scope of Policy
Page 4
4. Roles & Responsibility
Page 5
5. Implementation
Page 6
6. Associated Documentation & References
Page 10
7. Training & Resources 8. Monitoring & Audit
Page 10
Page 11
9. Equality & Diversity Page 11
Appendix 1 Procedure for the Reporting of incidents Appendix 2 Flowchart for the Reporting of Serious Incidents Requiring Investigation (including Never Events) Appendix 3 Incident red flags Appendix 4 Assessment of quality in terms of investigation reports Appendix 5

4
1 Introduction
East Cheshire NHS trust is committed, through its Health and Safety and Risk Management Policies, to the maintenance of safe working practices and the provision of an environment, which is safe for staff, patients and others; in accordance with good clinical practice and the requirements of Health and Safety, Fire Safety, Security and Environmental Legislation. This policy applies to all staff employed by East Cheshire NHS trust. This policy relates to the requirement of all personnel employed in all areas of the Trust to report all untoward events, including near misses, regardless of whether they involve patients, visitors, staff or contractors. The reporting of untoward events is an integral part of the trust’s Risk Management Strategy, which has a goal of identifying and then removing, or reducing to an acceptable level all risks across the organisation. As an organisation we can also transfer the risk to another stakeholder or accept the risk as it is. The reporting and subsequent management of the incidents reported will allow the trust to put measures in place to reduce or eliminate the likelihood of recurrence and allow the organisation to learn from previous incidents and experiences. The trust is committed to ensuring an organisational just culture in which front-line operators and others are not punished for actions, omissions or decisions taken by them which are commensurate with their experience and training.
2 Objective
This policy and associated standard operating procedures sets out the process for reporting and management of clinical and non-clinical incidents, accidents and near miss events reported via the electronic Datix integrated risk management system. This includes the reporting of incidents, accidents, and ‘near miss’ events related to patients, staff, volunteers, contractor, visitors and assets and including the investigation of serious incidents.
This policy is supported by related documents, policies and procedures as listed in section 7.
3 Scope of Policy
All staff, including agency staff, student learners, volunteers and contracted staff are required to report incidents, accidents and near misses (hereafter referred to collectively as incidents) in line with this policy and procedure.

5
4 Roles & Responsibilities
4.1 Chief Executive Has overall accountability for trust wide legislative compliance and management of risk. 4.2 Director of Corporate Affairs and Governance Has delegated accountability for ensuring the trust has robust risk management arrangements in place, including processes for reporting, responding and commencing investigations into clinical and non-clinical incidents. This person also has responsibility for keeping the Trust Board fully informed about serious incidents requiring investigation as well as general trends. They are also the trust’s Executive Lead for Speaking Up and as such staff may directly raise with them any concerns they have in relation to the trust’s response and management of specific patient safety incidents. 4.3 All Executive Directors Have operational responsibility for the implementation and monitoring of the risk management systems in place in the trust. This includes provision of specialist advice and support, implementation of independent scrutiny process and representing the trust at relevant Clinical Commissioning Group serious incident review meetings. Acts as the designated Liaison Officer for patients and families in relation to serious incidents as required. 4.4 Deputy Director of Corporate Affairs and Governance The Deputy Director of Corporate Affairs and Governance will provide specialist advice across the organisation in relation to incidents and risk management for a range of functions at all levels in the organisation to support the effective management of clinical and non-clinical incidents. This person has responsibility to ensure that robust processes are in place to ensure the trust reports and reviews incidents and that appropriate investigations are undertaken. They are also the Freedom to Speak Up Guardian with whom staff can discuss concerns regarding patient safety incidents they have become aware of, witnessed or been directly involved in. 4.5 Head of Safety and Risk The Head of Safety and Risk has operational responsibility for the implementation and monitoring of the incident reporting and management systems in place in the trust, including ensuring that the trust fulfils its statutory and contractual duties through the Serious Incident Framework to report incidents externally via the Strategic Executive Information System and the National Reporting and Learning System. Provides specialist advice to operational teams to support effective clinical and non-clinical risk issues associated with incidents, including analysing and reporting on learning from trends and serious incidents. This post holder is the Information Asset Owner for the Datix integrated risk management system and has overall responsibility for the management of the system. 4.6 Specialist Advisers eg Fire Safety, Health & Safety, Manual Handling, Safeguarding Team, Falls Coordinator etc. The specialist advisors within East Cheshire NHS trust will have oversight of incidents within their scope of practice. Each specialist advisor will receive an email notification from Datix when an incident within their speciality is reported. 4.7 Risk Management Team and Governance Heads of Service The Risk Management Team has responsibility to review and approve each incident reported and assign each incident to the appropriate person. Each member of the team can review any incident that is reported but each has their own specialist area in which they can provide advice to the incident handler. The risk management team will support the organisation and will produce appropriate reports, analysis and training where required. 4.8 Clinical Directors

6
Clinical Directors have the responsibility to ensure that incidents are reviewed at service line Safety, Quality Standards meetings on a monthly basis and receive assurance that actions are implemented and this can be evidenced. 4.9 Associate Directors The Associate Directors in each Directorate have operational responsibility for ensuring staff within their respective service line adheres to this policy and associated procedures. The Associate Directors are responsible for embedding individual and system learning as a result of incidents reported within the trust. Each Associate Director is responsible for all incidents being investigated appropriately and any actions arising from an investigation and implemented within timescales and evidence of completion forwarded to the risk management team to upload to Datix. 4.10 Service and Departmental Managers/Matrons Have a responsibility to review incident forms pertaining to their area and to ensure that accidents/incidents within their area of responsibility are investigated and managed effectively. They must escalate any concerns up to the Associate Director immediately. 4.11 Managers/ Team Leaders Have a responsibility to review incident forms pertaining to their area and to ensure that accidents/incidents within their area of responsibility are investigated and managed effectively and within timescales. They must escalate any concerns up to their Manager immediately. 4.12 All staff All staff employed by the trust have a legal, professional and moral duty to report accidents/incidents and near misses as soon as reasonably practical. They have a duty to assist with any accident/incident or near miss incident investigation that they have been involved in or have knowledge of. Staff must report any hazards they identify to their manager/the appropriate person to be resolved before any accidents or incidents occur. They must also take all reasonable steps to minimise risks to patients, colleagues and others. They have a duty to follow any changes in any policy, procedure or practice that has been identified as a result of an incident review or of lessons learnt. Where death or serious injury occurs as a result of an incident or there is a significant impact on the delivery of services, this must be reported immediately to a senior manager and the risk management team in hours or to the senior manager on call, out of hours.
5.0 Implementation
5.1 Recording Incidents (All must be entered on DATIX)
All incidents must be reported via the Datix Risk Management System. This is accessible via East Cheshire NHS trust Infonet and the application launcher.
All staff must be encouraged to report incidents appropriately and should refer to the relevant standard operating procedure and guidance entitled: “Incident Reporting Guide” which can be found on the Trust Infonet in the Datix and Patient Safety section. Training and guidance are available via the Risk Management Team.

7
5.2 Definitions Accident/incident – an unplanned and uncontrolled event that has led to or could lead to injury, ill health, harm to persons, damage to property, equipment or loss. Patient safety incident – anything associated with the patient and their clinical treatment or care which has or could lead to ill health or harm. Non patient safety incident (non-clinical) – an accident/incident involving anyone (staff, patient relative or visitor, contractor or visitor to the trust) or item or equipment, property or premise that is not directly associated with patient treatment or care. Serious Incident Requiring Investigation. A serious incident requiring investigation (SIRI, formally a serious untoward incident, SUI) is any incident on an NHS site or elsewhere whilst in NHS funded or NHS regulated care involving patients, relatives, visitors, staff, contractors, building, equipment or property and which may or has:
Caused death (including suicide) or serious injury or was life threatening
Contributed to reduced standards of care
Involved a hazard to public health
Involved an absconded patient detained under the Mental Health Act, Deprivation of Liberty standards and/or where a patient poses a significant risk to themselves or others
Caused serious disruption to services
Caused significant damage to NHS assets
Caused significant damage to the reputation of an NHS organisation or its staff
Involved fraud or suspected fraud
Given rise to a significant claim for damages
Involved the suspension of a member of staff or a student on care/clinical, professional or managerial issues
Raised concerns following an inquest
Caused a serious breach in confidentiality
Involved an attack on a member of staff, visitor or patient Near Miss – any event which had the potential to cause injury, ill health, damage, harm or loss but did not due to staff intervention or circumstance. Never Event – are defined as serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented by healthcare providers. They are reportable in the trust as a SIRI and managed as such. The list at present is as follows (Never Events list, January 2018, https://improvement.nhs.uk/resources/never-events-policy-and-framework/ ):
1. Wrong site surgery 2. Wrong implant/prosthesis 3. Retained foreign object post-procedure 4. Mis-selection of a strong potassium containing solution 5. Administration of medication by the wrong route 6. Overdose of Insulin due to abbreviations or incorrect device 7. Overdose of methotrexate for non-cancer treatment 8. Mis-selection of high strength midazolam during conscious sedation 9. Failure to install functional collapsible shower or curtain rails 10. Falls from poorly restricted windows 11. Chest or neck entrapment in bedrails 12. Transfusion or transplantation of ABO-incompatible blood components or organs 13. Misplaced naso or oro-gastric tubes 14. Scalding of patients 15. Unintentional connection of a patient requiring oxygen to an air flowmeter

8
5.3 Incident Response and Management Immediate Action The immediate safety or well-being of the patient, staff member or visitor affected or involved in an incident is paramount. Any remedial first aid or emergency treatment must be given and in the event of patient safety incidents and the patient’s medical team must be informed. Any environmental incident where must be resolved if there is a risk that someone could be harmed. The member of staff in charge of an area is responsible for ensuring that appropriate action has been taken to make the area safe following any incident and to ensure that the risk of the incident occurring again is reduced and that the incident is reported at the earliest opportunity. Incident Management The response to an incident must be proportionate to the severity of impact or harm. The most serious events will be rated as having a consequence that is severe harm or death (or a risk that is high in the case of near miss events). These must be reported, escalated and responded to immediately by the senior clinician involved in the patient’s care, Associate Director and Matron. This must also be reported to the Risk Management Team as soon as reasonably practical. The Risk Management Team will review each incident. Any incident which is graded no harm, low harm or a near miss will be assigned to the appropriate handler and closed on Datix. The handler will receive an email from Datix informing them that they are the handler. The link in the email will allow the handler to access the incident and review the information provided by the reporter. If the handler considers that further information is required on the incident (I.E further action has been taken to resolve the incident) then the incident record can still be updated even though it is closed. There are some incidents that even if graded no harm, low harm or a near miss still require an investigation. These are termed as incident red flags and have been agreed with Directorates (listed in Appendix 3). These incidents will be assigned to the appropriate handler for investigation.
Any equipment involved in the accident / incident must be made safe and retained for the purposes of any further investigation by Medical Devices Safety Officer who investigates and notifies The Medicines and Healthcare products Regulatory Agency (MHRA).
Incident occurs
Person involved made safe and remedial action taken
Report to Manager and on Datix
Report to Manager/Matron/Associate
Director/Doctor as appropriate. Out of Hours notify Site Manager.
For Serious Incidents
Report incident to Risk Management
Serious Incident Flowchart Appendix 2

9
If a patient receives a radiation dose “much greater than intended” then this is reportable to the Care Quality Commission. IRMER incident reporting guidance can be found at http://www.cqc.org.uk/content/reporting-irmer-incidents. Any incidents that involve blood transfusions could be reportable to SHOT (Serious Hazards of Transfusion). All blood transfusion incidents are notified to East Cheshire NHS trust Blood Transfusion Practitioner who is responsible for reporting to SHOT. Information on SHOT can be found at http://www.shotuk.org/reporting/sabre/ In line with professional bodies such as Nursing and Midwifery Council and the General Medical Council and the Health and Care Professionals Council, health professionals must be open and candid with patients. Any incident involving a patient should be discussed with the patient and/or carers and should be documented on Datix when reporting an incident. For any incident graded moderate and above that has occurred to a patient under the care of East Cheshire NHS trust then, in line with Duty of Candour Policy which must be complied with, a letter must be offered to explain the incident to the patient and/or carers. Following investigation of this incident then the outcome of the investigation should be discussed with the patient and/or carers and a letter offered to detail the outcome. This is detailed in the Duty of Candour Policy. When an incident is closed an automated email will be sent back to the reporter of the incident to inform them of any lessons learned. The “Lessons Learned and Feedback to Reporter” field from within Datix is included in the email and this informs them of personalise feedback from the investigator. 5.4 INVESTIGATION If an incident is requiring investigation then the incident will be assigned to the appropriate person. Datix should be used as part of the clinical care for the patient and incidents reviewed in a timely manner so any action required can be implemented and discussions with the patient/carers held. For low harm, no harm or near miss incidents that require a local investigation this will completed by the Consultant, Department Manager, Senior Sister or Team Leader. The outcome of the investigation will be documented on Datix, training is provided to new managers and support is ongoing via the Risk Management Team. Investigating and closing an incident on Datix SOP is also available on the Infonet. All moderate harm incidents will be investigated locally and are monitored by the Risk Management Team to ensure appropriate investigation has taken place and duty of candour applied. Where severe harm or death has occurred as a result of an incident, the incident is a potential, near miss or actual Never Event or there is a potential for serious harm if the incident reoccurs then a more comprehensive investigation will be required. The incident will be reviewed by the Risk Management Team and initial information will be gathered. The incident will then be discussed with the Director of Corporate Affairs and Governance with the view to reporting as a serious incident to East Cheshire CCG and the CQC via StEIS. The serious incident flowchart will then be followed [Appendix 2]. If an incident does not meet the criteria from reporting as a serious incident but is deemed to require further investigation it will be logged as an incident requiring investigation and the serious incident process will still be followed. The investigation will be completed using the root cause analysis investigation method. Information can be found on NHS Improvement website and via the Risk Management Team. Tools and Templates can be found on the trust Infonet under forms and templates.

10
Human factors should be taken into consideration when investigating an incident, further information on human factors can be found in Appendix 6. 5.5 CHECK AND CHALLENGE Once an RCA report has been completed by the investigator and before executive approval at Serious Incident Requiring Investigation Subcommittee a check and challenge meeting is held. The investigator will present the report to the check and challenge group (comprising of the Medical Director, Director of Nursing, Quality and Performance, Director of Corporate Affairs and Governance, Deputy Director of Corporate Affairs and Governance and Head of Safety and Risk). The report is then scrutinised to ensure the contributory factors, root cause and learning has been extrapolated from the investigation to reduce the risk of the incident occurring again.
6 Associated Documentation & References
Datix and Patient Safety pages, Trust Infonet: Standard operating procedure: “How to report an incident” Standard operating procedure: “Investigating and closing an incident on Datix” Standard operating procedure: “Approving and Grading Incidents” Standard operating procedure: “The management of medication incidents” Policies, Trust Infonet: Duty of Candour policy Duty of Candour standard operating procedure Risk Management Strategy Freedom to speak up: Raising Concerns NHS Improvement website: NHS England Serious Incident Framework: Supporting learning to prevent recurrence. NHS England Serious Incident Framework 2015/2016 – Frequently asked questions. NHS England Revised Never Events Policy and Framework. (2018) This document: Flowchart for the Reporting of Serious Incidents Requiring Investigation (including Never Events). [Appendix 2] Maternity Serious Incidents which require reporting to the CCG [Appendix 5]
7 Training & Resources

11
The Risk Management Team can provide training and advice on request in any aspect of risk management. A short video guide to entering information into a patient-related incident report on Datix can be found on the trust infonet. When a new manager commences employment at East Cheshire NHS trust it is the responsibility of their manager to request appropriate access to Datix by email to [email protected] in order to investigate any incidents in their area. The Risk Management Team will contact the new manager with a username and password for the system and provide training on using the Datix system. Tools and templates for investigation of serious incidents can be found at the Forms and templates section on the Infonet.
8 Monitoring & Audit
The effectiveness of the implementation of this policy will be monitored by the Head of Safety, Risk and Resilience and assurance provided on the following indicators via the Quarterly Complaints Incidents Claims and Patient Experience Report to the Risk Management Sub-committee and Safety Quality and Standards Committee in line with terms of reference:
Key performance indicators:
Percentage of SIRIs reported to the clinical commissioning group within 48 hours of identifying the incident.
Percentage of SIRIs 72 hour SBAR sent to clinical commissioning group within timescales
Percentage of SIRI Root Cause Analysis reports sent to clinical commissioning group within 60 day timescale.
Number of patient safety incidents reported. The standard of Root Cause Analysis are explained in Appendix 4 as set out in the Mazar’s Independent Review (Dec 2015)
9 Equality & Diversity
The trust is committed to an environment that promotes equality and embraces diversity in its performance as an employer and service provider. It will adhere to legal and performance requirements and will mainstream equality and diversity principles through its policies, procedures and processes. This policy should be implemented with due regard to this commitment. The Equality Analysis for this policy is available on request from the author.
12
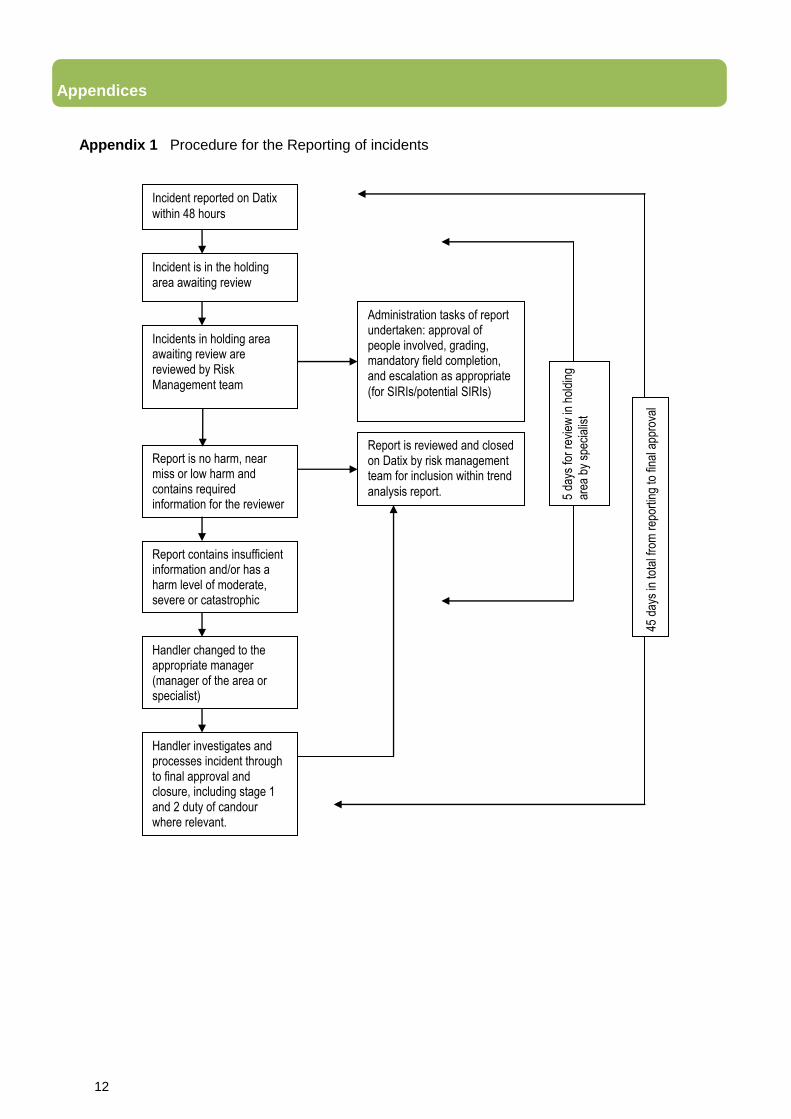
Appendices Appendix 1 Procedure for the Reporting of incidents
Incident reported on Datix
within 48 hours
Incident is in the holding area awaiting review
Report contains insufficient information and/or has a harm level of moderate, severe or catastrophic
Incidents in holding area awaiting review are reviewed by Risk Management team
Report is reviewed and closed on Datix by risk management team for inclusion within trend
analysis report.
Report is no harm, near miss or low harm and contains required information for the reviewer
Handler changed to the appropriate manager (manager of the area or specialist)
Handler investigates and processes incident through to final approval and closure, including stage 1 and 2 duty of candour where relevant.
Administration tasks of report undertaken: approval of people involved, grading, mandatory field completion, and escalation as appropriate
(for SIRIs/potential SIRIs)
5 da
ys fo
r re
view
in h
oldi
ng
area
by
spec
ialis
t
45 d
ays
in to
tal f
rom
rep
ortin
g to
fina
l app
rova
l

Appendix 2: Serious Incident Flowchart

14
Head of Service/ Service Manager /Head
of Safety and Risk informed
Ward/Department: Completes an incident report
immediately on Datix
Staff member to report immediately to: Service Manager (or deputy) Head of Service (or deputy)
Risk Management Department
Incident review/RCA planned/takes place. If
root cause lies with third party, then inform
Director of Corporate
Affairs and Governance
Report and action
plan developed
Draft report approved by the Service Line
SQS group and made “final”
TOR added to RCA template: SBAR
produced providing update to the CCG within 72 hours of reporting on StEIS
Leads review patient’s notes/statements/evidence
gathered Head of Service: Identifies Lead Consultant and Lead Investigator (in discussion with RM
department as appropriate) Risk Management Department informs:
CCG via StEIS within 48 hours and arranges check & Challenge date informing all concerned.
Final report sent to
Solicitors for legal review if agreed with Deputy Director of Corporate Affairs & Governance
Approved report sent to CCG within 60
working days
Head of Service: Discusses incident with
Director of Corporate Affairs and Governance (or deputy) Director of Nursing (or deputy)
and confirms incident as an SIRI with the risk manager and that it should be reported on StEIS
within 48 hours
When reporting an SIRI please ensure you use the following
statement: “My name is…..I am calling from…..
and I need to report a serious incident requiring investigation”
If the individual is not available ensure that a message is left
requesting an immediate call back as soon as available
Director of Corporate Affairs and Governance (or
deputy) informs: Chief Executive, Director of
Nursing Performance and
Quality, Medical Director
Definition of a SIRI: An accident or incident when a patient, member of staff, or a member of the public suffers: o Serious injury, o Major permanent harm o Unexpected death o Where the actions of health service staff are likely to cause significant public concern or press coverage o Where there is serious damage and/or loss of health care property. o Grade 3 or 4 pressure sore
o Serious falls
Progress against action plan monitored via SIRI Tracker by Governance Department Business Manager
All actions complete? Closed by service line
SIRI SC approves report and agrees action plan with service
line
Service Line SQS monitors
implementation of action plan
Corporate Affairs and Governance Team requests
StEIS reassignment via CCG
Final report sent to RM Department for
quality assurance/check &
challenge
Incident occurs – does it meet the definition of an SIRI (see definition below)
Audit completed – post action plan implementation

15
Appendix 3 Incident red flags (Incidents which need to be investigated by the appropriate handler)
One patient who has had numerous incidents reported
Paediatric incidents
Controlled drug, insulin, anticoagulant, methotrexate, midazolam incidents to be assigned as normal and left open for the handler to investigate
Omissions/lapses in care which have altered the patient’s journey
H&S (RIDDOR) incidents where a member of staff is injured (David will pick up on these)
VTE (any patient developing a DVT or PE)
C.Diff and MRSA bacteraemia
Externally reportable incidents such as blood transfusions or medical device failures
Any incident where abuse/neglect to a patient is suspected
Moderate and severe incidents and death all require investigation (and duty of candour stage 2)
Mortuary incidents which include: o Accidental damage to a body o Discovery of an additional organ(s) in a body on evisceration for a second
post-mortem examination, or during the repatriation or embalming process o Discovery of an organ or tissue following post-mortem examination and
release of body o Loss, disposal or retention of a whole fetus or fetal tissue (gestational age
greater than 24 weeks) against the express wishes of the family o Loss, disposal or retention of a whole fetus or fetal tissue (gestational age
less than 24 weeks) against the express wishes of the family o Inadvertent disposal or retention of an organ against the express wishes of
the family o Incident leading to the temporary unplanned closure of a mortuary resulting
in an inability to deliver services o Loss of an organ (Post mortem) o Major equipment failure in the mortuary o Post-mortem examination conducted was not in line with the consent given
or the PM examination proceeded with inadequate consent o Post-mortem examination of the wrong body o Release of the wrong body
Babies born at term (≥37 completed weeks of gestation), following labour, with a severe brain injury diagnosed in the first seven days of life, namely babies that have one or more of the following: This must be highlighted to Andy (or covering manager) for legal services to be informed and discussion on reporting to the NHSLA.
o Diagnosed with grade III hypoxic ischaemic encephalopathy (HIE); o Actively therapeutically cooled; o Have all three of the following signs: decreased central tone; comatose;
seizures of any kind.

16
Appendix 4 Assessment of quality in terms of investigation reports ref. Mazar’s Independent Review (Dec 2015) Excellent/good – no typographical; grammar; date; naming errors – report was easy to read, followed a logical flow and the evidence gathered clearly linked to recommendations and to action plans. The report could be shared with families as a robust piece of independent writing and with professionalism. Adequate – showed most of the information needed was available but was presented in a manner that made understanding the issues difficult; often these had grammar; date; naming and typing errors. Could have caused distress to families if shared by showing a lack of respect and attention to detail. Probably had not been quality reviewed at any level or detail. Poor/inadequate – these varied between having typographical errors to an unacceptable standard; naming the service user incorrectly; wrong dates; no flow and were either cursory or provided insufficient information to form good recommendations or action plans. These reports lacked challenge or effort in securing learning. Likely to cause distress to a family due to its cursory nature or lack of professionalism; and had most likely not been read properly during any phase of quality review by the Head of Safety and Risk. The Trust has a quality assurance proforma which is completed prior to the final draft being submitted for check and challenge.

17
Appendix 5: Maternity Serious Incidents which require reporting to the CCG There is regional agreement that the following serious incidents will be reported via StEIS to the Clinical Commissioning Group:
Postpartum haemorrhage where the Trust Major Haemorrhage Protocol is initiated
Unplanned maternal transfers to ICU
Hysterectomy (not for previously diagnosed cancer or placenta accrete)
Babies at or over 36 weeks gestation at birth, admitted to a Neonatal Intensive Care
Unit for cooling (the reporting organisation will be the place where the woman is
booked/received antenatal care, not the place of delivery)
Screening incidents
Screening incidents will be managed in line with the guidance provided by the
Population screening committee which can be accessed via
https://www.gov.uk/guidance/nhs-population-screening-explained Duty of Candour The Head of Midwifery and the Clinical Lead Consultant for Obstetrics and Gynaecology hold responsibility for quality and risk management within the maternity department and must be notified of incidents which come under the duty of candour policy. A duty of candour lead will be appointed for individual cases and will be responsible for ensuring that the patient is provided with information in line with the Trust’s Duty of Candour policy. Involvement of patients and their families in the investigation process Parents will be offered the opportunity to contribute to the investigation of stillbirths and other incidents where an adverse outcome has occurred. A meeting with the service leads will be offered or they can contribute with a written statement or pose questions they wish the RCA to address if this is more acceptable to them. Feedback following such investigations will be in line with the Trust Duty of Candour policy.

18
Maternal Fetal/Neonatal Organisation
Antepartum haemorrhage requiring resuscitation Postpartum haemorrhage >1000mls Return to theatre/laparotomy Eclamptic seizure Maternal collapse/cardiac/respiratory arrest Hysterectomy HDU admission 3rd and 4th degree tears Delay in perineal suturing > 1 hour Failed instrumental delivery Uterine rupture Shoulder dystocia Sepsis Postnatal readmission Thromboembolism Epidural delay for > 1 hour & anaesthetic complications (eg. > 4 attempts to site epidural) Duration of active labour – primips > 3 hours, multips > 2 hours Duration established labour > 18 hours Home birth not achieved due to staffing levels Intraoperative problems (eg. Bladder trauma) Undiagnosed major fetal abnormality Transfer of care from another hospital/care provider
APGAR <7 at 5 minutes Transfer to another unit Cord pH <7.2 Birth trauma Failure/incorrect baby labelling Cord prolapse Unanticipated admission to NNU (in the absence of risk factors) Undiagnosed congenital abnormality Diagnosis of HIE/baby required cooling/seizures Sepsis Temperature <36°C on admission to NNU Ventilation problems Meconium aspiration Born without midwifery assistance
Medication errors Any untoward incident that could potentially cause harm/loss/damage Delay in responding to attend to patient Near miss safety incidents affecting patients, visitors, staff Tissue viability incident Slips, trips, falls Delay in Drug errors Failure to follow antenatal and newborn screening guidelines Filing errors Lack of equipment/resources Inadequate staffing levels Verbal complaint Serious Incidents Requiring Immediate escalation Maternal Death Neonatal Death (up to 28 days age) Intrapartum stillbirth Serious birth trauma to baby Baby Abduction Retention of swabs/instruments Closure of maternity/neonatal unit Post partum haemorrhage initiating massive haemorrhage protocol Unplanned hysterectomy Unplanned admission to ICU Babies requiring cooling from 36/40

Appendix 6: HUMAN FACTORS All staff involved in an incident, irrespective of whether they are reporting or investigating or being investigated, should consider the following aspects of Human factors which may have contributed to the incident. This is important as there are usually multiple causes in serious clinical incident, and often present in minor incidents too. The acronym in Human Factors of "IM SAFE" applies across incidents in any industry: Illness, Medication, Stress, Alcohol, Fatigue, Eat (hungry). Within each of these there are many considerations including, but not limited to:- 1. Illness-was the service provider unwell with a pyrexia for example, or returned to work too soon after a period of illness, or do they have a long term condition which needs re-evaluating. 2. Medication-unlike some other industries health care does not prohibit staff from working while on some frequently prescribed medications which may affect performance and contribute to error e.g. opiate analgesia, sedating anti-histamines 3. Stress-while stress within the workplace may be readily considered e.g. understaffed, excess patient demand; domestic stress that a staff member brings into the workplace should also be considered 4. A for alcohol should also read hung over. Again NHS healthcare does not yet do random drug alcohol screening on its staff, in contrast to some industries where staff are legally prohibited from consuming alcohol within 8hr of shift start time; and staff colleagues should be open and honest if there is a suspicion of alcohol abuse, or alcohol related incident. 5. Fatigue: while being tired is part of being human, fatigue (which is not resolved by a good sleep) may be insidious and dangerous. Staff should consider whether they are adequately fresh when arriving for their work, adequate break period during a shift, adequate awake prior to leaving the workplace en route home or to another workplace. It is recognised that human performance is lowest between 3-5am and 3-5pm. 6. Eat: while there are considerable inter-individual variations in eating habits, if we are inadequately fuelled for work our performance is likely to be compromised and we lose insight to our performance /underperformance when inadequately nourished. In particular we may also lose insight to how communication within the team may be adversely affected by being hungry. It is a "false economy" to just see another patient before we have a break when we know we need nourishment. So while it is the employers duty to provide sufficient breaks, staff have a duty to take in sufficient nourishment during the breaks.