Embed Size (px)
Citation preview

REVIEW ARTICLE
Sports Medicine 14 (2): 82-99, 19920112-1642/92/0008-0082/$09.00/0© Adis International Limited. All rights reserved.
SP01156
Incidence, Severity, Aetiology and Preventionof Sports InjuriesA Review of Concepts
Willem van Meche/en, Hynek H/obil and Han CG. KemperDepartment of Health Science, Faculty of Human Movement Sciences, Vrije Universiteit enUniversity of Amsterdam, Amsterdam, The Netherlands
Contents82 Summary84 I. Sports Injury Incidence: Theoretical Considerations84 l.l The Definition of Sports Injury85 1.2 Sports Injury Incidence86 1.3 Research Design87 2. Sports Injury Data87 2.1 Sports Injury Incidence: The Netherlands as an Example87 2.2 Other Comparisons88 3. Severity of Sports Injuries88 3.1 Nature of Sports Injuries89 3.2 Duration and Nature of Treatment89 3.3 Sports Time Lost90 3.4 Working Time Lost90 3.5 Permanent Damage91 3.6 Costs of Sports Injuries92 4. Aetiology and Prevention of Sports Injuries97 4.1 Sport-Specificity of Sports Injuries97 5. Conclusions
Summary Notwithstanding the healthy influence of sporting activities on risk factors, in particular thoseof cardiovascular disease, it is becoming increasingly apparent that sports can present a dangerto health in the form of sports injuries. The extent of the sports injury problem calls for preventative action based on the results of epidemiological research. For the interpretation of thesefacts uniform definitions are needed and limitations of research designs should be known. Measures to prevent sports injuries form part of what is called the 'sequence of prevention'. Firstlythe extent of the sports injury problem must be identified and described. Secondly the factorsand mechanisms which playa part in the occurrence of sports injuries have to be identified. Thethird step is to introduce measures that are likely to reduce the future risk and/or severity ofsports injuries. This measure should be based on the aetiological factors and the mechanism asidentified in the second step. Finally the effect of the measures must be evaluated by repeatingthe first step.
REVIEW ARTICLE
Sports Medicine 14 (2): 82-99, 19920112-1642/92/0008-0082/$09.00/0© Adis International Limited. All rights reserved.
SP01156
Incidence, Severity, Aetiology and Preventionof Sports InjuriesA Review of Concepts
Willem van Meche/en, Hynek H/obil and Han CG. KemperDepartment of Health Science, Faculty of Human Movement Sciences, Vrije Universiteit enUniversity of Amsterdam, Amsterdam, The Netherlands
Contents82 Summary84 I. Sports Injury Incidence: Theoretical Considerations84 l.l The Definition of Sports Injury85 1.2 Sports Injury Incidence86 1.3 Research Design87 2. Sports Injury Data87 2.1 Sports Injury Incidence: The Netherlands as an Example87 2.2 Other Comparisons88 3. Severity of Sports Injuries88 3.1 Nature of Sports Injuries89 3.2 Duration and Nature of Treatment89 3.3 Sports Time Lost90 3.4 Working Time Lost90 3.5 Permanent Damage91 3.6 Costs of Sports Injuries92 4. Aetiology and Prevention of Sports Injuries97 4.1 Sport-Specificity of Sports Injuries97 5. Conclusions
Summary Notwithstanding the healthy influence of sporting activities on risk factors, in particular thoseof cardiovascular disease, it is becoming increasingly apparent that sports can present a dangerto health in the form of sports injuries. The extent of the sports injury problem calls for preventative action based on the results of epidemiological research. For the interpretation of thesefacts uniform definitions are needed and limitations of research designs should be known. Measures to prevent sports injuries form part of what is called the 'sequence of prevention'. Firstlythe extent of the sports injury problem must be identified and described. Secondly the factorsand mechanisms which playa part in the occurrence of sports injuries have to be identified. Thethird step is to introduce measures that are likely to reduce the future risk and/or severity ofsports injuries. This measure should be based on the aetiological factors and the mechanism asidentified in the second step. Finally the effect of the measures must be evaluated by repeatingthe first step.

Sports Injury Research Terminology 83
In this review some aspects of the first and second step of the sequence of prevention arediscussed.
The extent ofthe sports injury problem is often described by injury incidence and by indicatorsof the severity of sports injuries. Sports injury incidence should preferably be expressed as thenumber of sports injuries per exposure time (e.g. per 1000 hours of sports participation) in orderto facilitate the comparability of research results. However, one should realise that the outcomeof research applying this definition of sports injury incidence is highly dependent on the definitions of 'sports injury' and 'sports participation'.
The outcome of such research also depends on the applied research design and research methodology. The incidence of sports injuries depends on: the method used to count injuries (e.g.prospective vs retrospective); the method used to establish the population at risk; and on therepresentativeness of the sample.
Severity of sports injuries can be described on the basis of 6 criteria: the nature of the sportsinjury; the duration and nature of treatment; sporting time lost; working time lost; permanentdamage; and cost. Here also uniform definitions are important and necessary in order to enhancethe comparability of research data. In the second step of the 'sequence of prevention' the aetiological factors that playa role in the occurrence of a sports injury have to be identified by epidemiological studies. Epidemiological research on the aetiology of sports injuries requires a conceptual model. The most commonly applied model is a stress/capacity model in which internal(personal) and external (environmental) aetiological factors are identified. In this model stressand capacity must be in balance and preventative measures must be designed to achieve ormaintain this balance. However, merely to establish the aetiological factors is not enough; themechanism by which sports injuries occur must also be identified. Athletes are in constant interaction with their environment and aetiological factors must be approached from this point ofview. In a second, more dynamic, conceptual model on the aetiology of sports injuries, the importance of the determinants of sports behaviour, as well as the interaction between the variousaetiological factors, is discussed. Whether or not a sports injury results from sports behaviourlargely depends on the extent to which 'prevention' is incorporated in the determinants of sportsbehaviour. The drawback of both conceptual models is the fact that neither of them incorporatea time perspective. They can therefore not be applied to research on the aetiology of overuseinjuries. In this perspective the application of a stress/strain/capacity model can be useful. Thisis a more dynamic and time-based 3-phase sequential model in which behaviour, amongst otheraetiological factors, plays an important role. In this model an athlete is seen as an active manipulator of stress by whom the amount of strain evoked by sports participation can be altered,thereby influencing the capacity to perform in a certain sports situation, but also influencing therisk to sustain a sports injury, either acute or long term.
Finally, despite the importance of the model of choice in studying the aetiology of sportsinjuries one should realise that again the choice of research design influences the outcome ofsuch research. Case series usually give no information on the underlying population at risk, sothey are of no value in drawing valid conclusions on the risk factors of injuries. Only by relatingthe injuries to corresponding population denominators can one estimate injury rates and identifyimportant risk factors and high risk sportspeople. As in research on sports injury incidence; research on risk factors should be undertaken on groups that are homogeneous with regard to age,sex, level of competition and type of sport.
During recent decades both the government andsports organisations in the Netherlands have encouraged sporting activities, as exemplified by the'Trim U Fit' (1968), 'Sportreal' (1976). 'NederlandOke' (1980) and 'Sport, zelfs ik doe het' (1986)
campaigns. The Netherlands was not alone in this:witness the 'Sport for All' campaign of the BritishSports Council and, again in Britain, the 'Exercisefor Health' campaign (Hutson 1983), as well as Fitness Canada (Shephard 1985). Underlying these ef-
Sports Injury Research Terminology 83
In this review some aspects of the first and second step of the sequence of prevention arediscussed.
The extent ofthe sports injury problem is often described by injury incidence and by indicatorsof the severity of sports injuries. Sports injury incidence should preferably be expressed as thenumber of sports injuries per exposure time (e.g. per 1000 hours of sports participation) in orderto facilitate the comparability of research results. However, one should realise that the outcomeof research applying this definition of sports injury incidence is highly dependent on the definitions of 'sports injury' and 'sports participation'.
The outcome of such research also depends on the applied research design and research methodology. The incidence of sports injuries depends on: the method used to count injuries (e.g.prospective vs retrospective); the method used to establish the population at risk; and on therepresentativeness of the sample.
Severity of sports injuries can be described on the basis of 6 criteria: the nature of the sportsinjury; the duration and nature of treatment; sporting time lost; working time lost; permanentdamage; and cost. Here also uniform definitions are important and necessary in order to enhancethe comparability of research data. In the second step of the 'sequence of prevention' the aetiological factors that playa role in the occurrence of a sports injury have to be identified by epidemiological studies. Epidemiological research on the aetiology of sports injuries requires a conceptual model. The most commonly applied model is a stress/capacity model in which internal(personal) and external (environmental) aetiological factors are identified. In this model stressand capacity must be in balance and preventative measures must be designed to achieve ormaintain this balance. However, merely to establish the aetiological factors is not enough; themechanism by which sports injuries occur must also be identified. Athletes are in constant interaction with their environment and aetiological factors must be approached from this point ofview. In a second, more dynamic, conceptual model on the aetiology of sports injuries, the importance of the determinants of sports behaviour, as well as the interaction between the variousaetiological factors, is discussed. Whether or not a sports injury results from sports behaviourlargely depends on the extent to which 'prevention' is incorporated in the determinants of sportsbehaviour. The drawback of both conceptual models is the fact that neither of them incorporatea time perspective. They can therefore not be applied to research on the aetiology of overuseinjuries. In this perspective the application of a stress/strain/capacity model can be useful. Thisis a more dynamic and time-based 3-phase sequential model in which behaviour, amongst otheraetiological factors, plays an important role. In this model an athlete is seen as an active manipulator of stress by whom the amount of strain evoked by sports participation can be altered,thereby influencing the capacity to perform in a certain sports situation, but also influencing therisk to sustain a sports injury, either acute or long term.
Finally, despite the importance of the model of choice in studying the aetiology of sportsinjuries one should realise that again the choice of research design influences the outcome ofsuch research. Case series usually give no information on the underlying population at risk, sothey are of no value in drawing valid conclusions on the risk factors of injuries. Only by relatingthe injuries to corresponding population denominators can one estimate injury rates and identifyimportant risk factors and high risk sportspeople. As in research on sports injury incidence; research on risk factors should be undertaken on groups that are homogeneous with regard to age,sex, level of competition and type of sport.
During recent decades both the government andsports organisations in the Netherlands have encouraged sporting activities, as exemplified by the'Trim U Fit' (1968), 'Sportreal' (1976). 'NederlandOke' (1980) and 'Sport, zelfs ik doe het' (1986)
campaigns. The Netherlands was not alone in this:witness the 'Sport for All' campaign of the BritishSports Council and, again in Britain, the 'Exercisefor Health' campaign (Hutson 1983), as well as Fitness Canada (Shephard 1985). Underlying these ef-

84
1. Establishing the 2. Establishingextent of the sports aetiology andinjury problem .... mechanism ot• incidence
... injuries
• severity
r ~4. Assessing their .... 3. Introducing
effectiveness by"'"
preventiverepeating step 1 measures
Fig. 1. The 'sequence of prevention' of sports injuries (vanMechelen et al. 1987).
forts was the supposedly healthy influence of sporting activities on risk factors, in particular those ofcardiovascular diseases.
Reasons for participating in sport are many andvaried but 2 relatively common ones are health/fitness and pleasure/relaxation (Manders & Kropman 1979).
It is becoming increasingly apparent that as wellas having a health-giving aspect, sport can presenta danger to health in the form of accidents andinjuries. An individual who has to give up or cutdown his or her sporting activities as a result ofinjury is unable to pursue some or all of his or hergoals. If the injury is serious enough the athleteswill also have recourse to the medical services tohave it treated. Injuries can also result in absencefrom school or work.
Given these unwanted side effects of sports participation it was recognised in Europe and elsewhere that a preventative approach towards the reduction of sports injuries should have high priority.It was for that reason that, within the 'health forall by the year 2000' policy of the World HealthOrganization, the Council of Europe launched aEuropean coordinated research project 'Sport ForAll: Sports Injuries and Their Prevention' in orderto improve the understanding of sports injuries andto develop a scientifically based prevention strategy. Measures to prevent sports injuries do notstand by themselves. They form part ofwhat mightbe called a 'sequence of prevention' (fig. 1; vanMechelen et al. 1987).
Sports Medicine 14 (2) 1992
First, the problem must be identified and described in terms of incidence and severity of sportsinjuries. Then the factors and mechanisms whichplaya part in the occurrence of sports injuries haveto be identified. The third step is to introducemeasures that are likely to reduce the future riskand/or severity of sports injuries. This measureshould be based on the aetiological factors and themechanisms as identified in the second step. Finally the effect of the measures must be evaluatedby repeating the first step. In this review some aspects of the first and the second step of the sequence of prevention will be discussed.
1. Sports Injury Incidence: TheoreticalConsiderations1.1 The Definition of Sports Injury
In general 'sports injury' is a collective name forall types of damage that can occur in relation tosporting activities. Various studies of incidence define the term sports injury in different ways(Boersma-Slutter et al. 1979; Franke & Franke 1980;Groh & Groh 1975; Hunter & Torgan 1983; LaCava1978; Lysens & Ostlyn 1984; McLatchie 1979;Mueller & Blyth 1974). In some studies a sportsinjury is defined as one sustained during sportingactivities for which an insurance claim is submitted (Brandt Corstius 1983). In other studies thedefinition is confined to injuries treated at a hospital casualty or other medical department(Boersma-Slutter et al. 1979; Clement & Taunton1981; Edixhoven et al. 1980; Hitchcock & Karmi1982; Jaflin 1981; Janka & Daxecker 1984; Jost etal. 1981; Kvidera & Frankel 1983; Maehlum &Daljord 1984; Maehlum 1984; Oh & Schmid 1982;Schurmeyer et al. 1983; Sedlin et al. 1984; Steinbruck & Rieden 1984; Steinbruck & Cotta 1983).The different definitions partly explain the differing incidences found. The results of these varioussurveys are therefore not comparable (Kranenborg1982). If sports injuries are recorded through themedical channels, a fairly large percentage of serious, predominantly acute injuries will be observed and less serious and/or overuse injuries willnot be recorded. If such a limited definition is used,
84
1. Establishing the 2. Establishingextent of the sports aetiology andinjury problem .... mechanism ot• incidence
... injuries
• severity
r ~4. Assessing their .... 3. Introducing
effectiveness by"'"
preventiverepeating step 1 measures
Fig. 1. The 'sequence of prevention' of sports injuries (vanMechelen et al. 1987).
forts was the supposedly healthy influence of sporting activities on risk factors, in particular those ofcardiovascular diseases.
Reasons for participating in sport are many andvaried but 2 relatively common ones are health/fitness and pleasure/relaxation (Manders & Kropman 1979).
It is becoming increasingly apparent that as wellas having a health-giving aspect, sport can presenta danger to health in the form of accidents andinjuries. An individual who has to give up or cutdown his or her sporting activities as a result ofinjury is unable to pursue some or all of his or hergoals. If the injury is serious enough the athleteswill also have recourse to the medical services tohave it treated. Injuries can also result in absencefrom school or work.
Given these unwanted side effects of sports participation it was recognised in Europe and elsewhere that a preventative approach towards the reduction of sports injuries should have high priority.It was for that reason that, within the 'health forall by the year 2000' policy of the World HealthOrganization, the Council of Europe launched aEuropean coordinated research project 'Sport ForAll: Sports Injuries and Their Prevention' in orderto improve the understanding of sports injuries andto develop a scientifically based prevention strategy. Measures to prevent sports injuries do notstand by themselves. They form part ofwhat mightbe called a 'sequence of prevention' (fig. 1; vanMechelen et al. 1987).
Sports Medicine 14 (2) 1992
First, the problem must be identified and described in terms of incidence and severity of sportsinjuries. Then the factors and mechanisms whichplaya part in the occurrence of sports injuries haveto be identified. The third step is to introducemeasures that are likely to reduce the future riskand/or severity of sports injuries. This measureshould be based on the aetiological factors and themechanisms as identified in the second step. Finally the effect of the measures must be evaluatedby repeating the first step. In this review some aspects of the first and the second step of the sequence of prevention will be discussed.
1. Sports Injury Incidence: TheoreticalConsiderations1.1 The Definition of Sports Injury
In general 'sports injury' is a collective name forall types of damage that can occur in relation tosporting activities. Various studies of incidence define the term sports injury in different ways(Boersma-Slutter et al. 1979; Franke & Franke 1980;Groh & Groh 1975; Hunter & Torgan 1983; LaCava1978; Lysens & Ostlyn 1984; McLatchie 1979;Mueller & Blyth 1974). In some studies a sportsinjury is defined as one sustained during sportingactivities for which an insurance claim is submitted (Brandt Corstius 1983). In other studies thedefinition is confined to injuries treated at a hospital casualty or other medical department(Boersma-Slutter et al. 1979; Clement & Taunton1981; Edixhoven et al. 1980; Hitchcock & Karmi1982; Jaflin 1981; Janka & Daxecker 1984; Jost etal. 1981; Kvidera & Frankel 1983; Maehlum &Daljord 1984; Maehlum 1984; Oh & Schmid 1982;Schurmeyer et al. 1983; Sedlin et al. 1984; Steinbruck & Rieden 1984; Steinbruck & Cotta 1983).The different definitions partly explain the differing incidences found. The results of these varioussurveys are therefore not comparable (Kranenborg1982). If sports injuries are recorded through themedical channels, a fairly large percentage of serious, predominantly acute injuries will be observed and less serious and/or overuse injuries willnot be recorded. If such a limited definition is used,

Sports Injury Research Terminology
only part of the total sports injury problem is revealed: this 'tip-of-the-iceberg' phenomenon iscommonly described in epidemiological research(Walter et a1. 1985). This can be illustrated by theresults of van Galen and Diederiks (1990); using abroad definition of sports injuries (any self-reported sports injury) in a national survey on sportsinjuries, 43% of all injuries were found to be medically treated.
To make sports injury surveys comparable andto avoid the 'tip-of-the-iceberg' phenomenon as faras possible, an unambiguous, universally applicable definition of 'sports injury' is the first prerequisite. This definition should be based on a concept of health other than that customary in standardmedicine. In everyday life individuals are regardedas healthy if they are able to do their daily work.Athletes, on the other hand, are not fully recoveredunless they can take part in their sport (trainingsession or match). One of the definitions based onthis premise is that used by the National AthleticInjury Registration System (NAIRS) in the US.'The reportable injury is one that limits athleticparticipation for at least the day after the day ofonset' (Vinger 1981). NAIRS classifies injuries, according to the length of incapacitation, into 'minor' (1 to 7 days), 'moderately serious' (8 to 21days) and 'serious' (over 21 days or permanentdamage). An example of an even more extensivedefinition that takes these considerations into account is the one proposed by the Council of Europe, in which a sports injury is defined as any injury as a result of participation in sport with oneor more of the following consequences: (a) a reduction in the amount or level of sports activity;(b) a need for (medical) advice or treatment; and(c) adverse social or economic effects (van Vulpen1989).
Even if one uniform definition of 'sports injury'is applied, the need remains for uniform agreementon other issues such as the way in which sportsinjury incidence is expressed, the ways in whch reliable estimates are made of both the number ofpeople engaging in sports and the number of injured sportspersons, etc.
85
1.2 Sports Injury Incidence
A common indication of disease in the population or a section of the population is incidence.If we substitute 'sports injury or sports accident'for 'disease', incidence can be defined as the number of new sports injuries or accidents during a particular period divided by the total number of sportspersons at the start of the period (= population atrisk). Incidence also gives an estimate of risk. If wemultiply the figure obtained by 100 we have thepercentage rate (Sturmans 1984). Expressed in thisway sports injury incidence provides a yardstickfor the extent of the sports injury problem.
Incidence rate of sports injuries is usually defined as a number of new sports injuries during aparticular period (e.g. 1 year) divided by the totalnumber of sportsmen at the start of the period(population at risk). Here again, it should be realised that it is important when interpreting andcomparing the various incidence rates to knowwhich definition of 'sports injury' was used andhow comparable were the samples.
Another problem lies in the way incidence ratesare expressed. In some cases the number of injuriesin a particular category of sportspersons per seasonor per year is taken, or the number of injuries perplayer per match. In both cases no allowance ismade for any differences in exposure (the numberof hours during which the person actually runs therisk of being injured), despite the fact that this factor certainly influences the risk of injury. Incidencefigures that take no account of exposure are therefore, according to Kranenborg (1982), not a goodindication of the true extent of the problem, norcan incidence rates for different sports be properlycompared. It would be better to calculate the incidence of sports injuries in relation to exposure indays, hours or sports event. This would enable different sports and different sportspersons to becompared more fairly in this respect (Eriksson 1983;Kennedy et a1. 1977; Wallace 1988; Zemper 1984).For this purpose injury incidence is expressed bymany researchers as the number ofinjuries per 1000hours of sports participation (e.g. Backx et a1. 1990;Ekstrand 1982; Lysholm & Wiklander 1987; van
Sports Injury Research Terminology
only part of the total sports injury problem is revealed: this 'tip-of-the-iceberg' phenomenon iscommonly described in epidemiological research(Walter et a1. 1985). This can be illustrated by theresults of van Galen and Diederiks (1990); using abroad definition of sports injuries (any self-reported sports injury) in a national survey on sportsinjuries, 43% of all injuries were found to be medically treated.
To make sports injury surveys comparable andto avoid the 'tip-of-the-iceberg' phenomenon as faras possible, an unambiguous, universally applicable definition of 'sports injury' is the first prerequisite. This definition should be based on a concept of health other than that customary in standardmedicine. In everyday life individuals are regardedas healthy if they are able to do their daily work.Athletes, on the other hand, are not fully recoveredunless they can take part in their sport (trainingsession or match). One of the definitions based onthis premise is that used by the National AthleticInjury Registration System (NAIRS) in the US.'The reportable injury is one that limits athleticparticipation for at least the day after the day ofonset' (Vinger 1981). NAIRS classifies injuries, according to the length of incapacitation, into 'minor' (1 to 7 days), 'moderately serious' (8 to 21days) and 'serious' (over 21 days or permanentdamage). An example of an even more extensivedefinition that takes these considerations into account is the one proposed by the Council of Europe, in which a sports injury is defined as any injury as a result of participation in sport with oneor more of the following consequences: (a) a reduction in the amount or level of sports activity;(b) a need for (medical) advice or treatment; and(c) adverse social or economic effects (van Vulpen1989).
Even if one uniform definition of 'sports injury'is applied, the need remains for uniform agreementon other issues such as the way in which sportsinjury incidence is expressed, the ways in whch reliable estimates are made of both the number ofpeople engaging in sports and the number of injured sportspersons, etc.
85
1.2 Sports Injury Incidence
A common indication of disease in the population or a section of the population is incidence.If we substitute 'sports injury or sports accident'for 'disease', incidence can be defined as the number of new sports injuries or accidents during a particular period divided by the total number of sportspersons at the start of the period (= population atrisk). Incidence also gives an estimate of risk. If wemultiply the figure obtained by 100 we have thepercentage rate (Sturmans 1984). Expressed in thisway sports injury incidence provides a yardstickfor the extent of the sports injury problem.
Incidence rate of sports injuries is usually defined as a number of new sports injuries during aparticular period (e.g. 1 year) divided by the totalnumber of sportsmen at the start of the period(population at risk). Here again, it should be realised that it is important when interpreting andcomparing the various incidence rates to knowwhich definition of 'sports injury' was used andhow comparable were the samples.
Another problem lies in the way incidence ratesare expressed. In some cases the number of injuriesin a particular category of sportspersons per seasonor per year is taken, or the number of injuries perplayer per match. In both cases no allowance ismade for any differences in exposure (the numberof hours during which the person actually runs therisk of being injured), despite the fact that this factor certainly influences the risk of injury. Incidencefigures that take no account of exposure are therefore, according to Kranenborg (1982), not a goodindication of the true extent of the problem, norcan incidence rates for different sports be properlycompared. It would be better to calculate the incidence of sports injuries in relation to exposure indays, hours or sports event. This would enable different sports and different sportspersons to becompared more fairly in this respect (Eriksson 1983;Kennedy et a1. 1977; Wallace 1988; Zemper 1984).For this purpose injury incidence is expressed bymany researchers as the number ofinjuries per 1000hours of sports participation (e.g. Backx et a1. 1990;Ekstrand 1982; Lysholm & Wiklander 1987; van

Injury incidence =
86
Mechelen 1991). The equation of Chambers (1979)recently adapted by de Loes and Goldie (1988) canbe used to calculate injury incidence taking exposure into account.
(No. of sports injuries/year) x 104
(No. of participants) x (hours ofsports participation/week) x (weeks
of season/year)
De Loes and Goldie (1988) demonstrated veryclearly that a league table of 'injury sports' basedon the calculation of incidence without taking exposure into consideration differs from one that doescorrect incidence for exposure time. The importance of calculating incidence taking exposure timeinto account was also clearly demonstrated by vanGalen and Diederiks (1990), who identified majordifferences in incidence per 1000 hours of sportsparticipation depending on age, gender and sports.Lindenfeld et al. (1988) proposed that the definition of incidence of sports injuries should be further sharpened by using actual exposure time atrisk, rather then overall time spent on sports participation. For reasons of practicality actual exposure time at risk is not very often used in research.
As can be seen from the above-mentioned injury incidence equation, not only the definition ofsports injury will affect the outcome of the equation but also the definition of sports participation.One should be aware of differences between recreational and competitive sports, organised andnonorganised sports (van Galen & Diederiks 1990)and training and competition (van Mechelen et al.1987), and one should decide whether to includeor exclude some of these categories in the definition of sports participation.
1.3 Research Design
The extent to which sports injury incidence canbe assessed depends on: the definition ofsports injury; the way in which incidence is expressed; themethod used to count injuries; the method to establish the population at risk; and the representativeness of the sample (Kranenborg 1982). Injuriescan be counted retrospectively or prospectively, us-
Sports Medicine 14 (2) 1992
ing questionnaires or person-to-person interviews.Prospective studies can, by quantifying exposuretime, accurately estimate the risk and incidence ofinjury according to the level and type of exposureof an athlete, while retrospective studies can alsoidentify some risk factors depending on choice ofresearch design, e.g. case-control studies (Walter etal. 1985). Depending on the methods used the researcher will be confronted to a greater or lesserextent with phenomena such as recall bias, overestimation of the hours of sports participation(Klesges et al. 1990), incomplete response, nomesponse, invalid injury description, and problems related to the duration and cost of research. Theseaspects are not further discussed here in depth.
Despite these problems special attention has tobe paid to the method of assessing the populationat risk and to the representativeness ofthe sample.If the population at risk is not clearly identified itis not possible to calculate reliable incidence data.With regard to the representativeness of the sampleit has to be taken into consideration that the performance of sports, and therefore the incidence ofsports injuries, is highly determined by selection.Bol et al. (1991) recognised 4 kinds of selection (a)self-selection (personal preferences) and/or selection by social environment (parents, friends, school,etc.); (b) selection by sports environment (trainer,coach, etc.); (c) selection by sports organisations(organisation ofcompetition by age and gender, thesetting of participation standards, etc.); and (d) selection by social, medical and biological factors(socioeconomic background, mortality, age, aging,gender, etc.). For examples: within a certain sportcompeting at a high level increases sports injuryincidence (Caine et al. 1989; Jorgensen 1988; Pettrone & Ricardelli 1987); in contrast to individualsports and team sports more injuries are sustainedduring matches than during training (Ekstrand &Nigg 1989; Fintelman et al. 1989); in contact sportsmore injuries are sustained than in noncontactsports (Chambers 1979; de Loes & Goldie 1988);during and shortly after the growth spurt boys sustain more injuries (Backous et al. 1988; Caine etal. 1989; Stanitski 1989).
Differences in injury incidence between various
Injury incidence =
86
Mechelen 1991). The equation of Chambers (1979)recently adapted by de Loes and Goldie (1988) canbe used to calculate injury incidence taking exposure into account.
(No. of sports injuries/year) x 104
(No. of participants) x (hours ofsports participation/week) x (weeks
of season/year)
De Loes and Goldie (1988) demonstrated veryclearly that a league table of 'injury sports' basedon the calculation of incidence without taking exposure into consideration differs from one that doescorrect incidence for exposure time. The importance of calculating incidence taking exposure timeinto account was also clearly demonstrated by vanGalen and Diederiks (1990), who identified majordifferences in incidence per 1000 hours of sportsparticipation depending on age, gender and sports.Lindenfeld et al. (1988) proposed that the definition of incidence of sports injuries should be further sharpened by using actual exposure time atrisk, rather then overall time spent on sports participation. For reasons of practicality actual exposure time at risk is not very often used in research.
As can be seen from the above-mentioned injury incidence equation, not only the definition ofsports injury will affect the outcome of the equation but also the definition of sports participation.One should be aware of differences between recreational and competitive sports, organised andnonorganised sports (van Galen & Diederiks 1990)and training and competition (van Mechelen et al.1987), and one should decide whether to includeor exclude some of these categories in the definition of sports participation.
1.3 Research Design
The extent to which sports injury incidence canbe assessed depends on: the definition ofsports injury; the way in which incidence is expressed; themethod used to count injuries; the method to establish the population at risk; and the representativeness of the sample (Kranenborg 1982). Injuriescan be counted retrospectively or prospectively, us-
Sports Medicine 14 (2) 1992
ing questionnaires or person-to-person interviews.Prospective studies can, by quantifying exposuretime, accurately estimate the risk and incidence ofinjury according to the level and type of exposureof an athlete, while retrospective studies can alsoidentify some risk factors depending on choice ofresearch design, e.g. case-control studies (Walter etal. 1985). Depending on the methods used the researcher will be confronted to a greater or lesserextent with phenomena such as recall bias, overestimation of the hours of sports participation(Klesges et al. 1990), incomplete response, nomesponse, invalid injury description, and problems related to the duration and cost of research. Theseaspects are not further discussed here in depth.
Despite these problems special attention has tobe paid to the method of assessing the populationat risk and to the representativeness ofthe sample.If the population at risk is not clearly identified itis not possible to calculate reliable incidence data.With regard to the representativeness of the sampleit has to be taken into consideration that the performance of sports, and therefore the incidence ofsports injuries, is highly determined by selection.Bol et al. (1991) recognised 4 kinds of selection (a)self-selection (personal preferences) and/or selection by social environment (parents, friends, school,etc.); (b) selection by sports environment (trainer,coach, etc.); (c) selection by sports organisations(organisation ofcompetition by age and gender, thesetting of participation standards, etc.); and (d) selection by social, medical and biological factors(socioeconomic background, mortality, age, aging,gender, etc.). For examples: within a certain sportcompeting at a high level increases sports injuryincidence (Caine et al. 1989; Jorgensen 1988; Pettrone & Ricardelli 1987); in contrast to individualsports and team sports more injuries are sustainedduring matches than during training (Ekstrand &Nigg 1989; Fintelman et al. 1989); in contact sportsmore injuries are sustained than in noncontactsports (Chambers 1979; de Loes & Goldie 1988);during and shortly after the growth spurt boys sustain more injuries (Backous et al. 1988; Caine etal. 1989; Stanitski 1989).
Differences in injury incidence between various

Sports Injury Research Terminology
specific types of sports are discussed below (seesection 2.2).
The outcome of research on the extent of thesports injury problem is highly dependent on definitions of 'sports injury', 'sports injury incidence'and 'sports participation', and that allowanceshould be made for exposure time when calculatingincidence. It should be borne in mind that the outcome of such research also depends on the appliedresearch design and research methodology, as wellas on the representativeness of the sample.
2. Sports Injury Data2.1 Sports Injury Incidence: The Netherlandsas an Example
Boersma-Sliitter et al. (1979) and Kranenborg(1980), using different methods, reach annual totalsof 560 000 (medically treated) and 1.2 million(medically and nonmedically treated) injuries, respectively, corresponding to yearly rates of 20 and46.5%. These figures are not directly comparable,since the 2 surveys differed, in particular with regard to sample, research method and definition of'sports injury'. Obviously this affects the interpretation of the figures.
Rogmans and Weerman (1982) calculated in asurvey of home and leisure time accidents that 21%of all accidents took place at sports and recreational locations; Verbeek et al. (1984) in a surveyof the frequency of and background to sports injuries among schoolchildren, arrived at a rate of10% a month; Inklaar (1985), using data from anongoing survey of morbidity in the Netherlands,calculated an average rate of 2.4% over a period of4 years.
Recently a representative nationwide telephonesurvey in the Netherlands revealed, in a totalpopulation of some 15 million, an overall sportsinjury incidence 00.3 (95% confidence limits: 3.1to 3.5) injuries per 1000 hours spent on sports; 1.4injuries per 1000 hours spent on sports were medically treated (van Galen & Diederiks 1990). In thisstudy an absolute number of 2.7 million sports injuries was calculated of which 1.7 million weremedically treated. Major sports injury incidence
87
differences per 1000 hours spent on sports werediscerned with regard to age, sex, specific sport,recreational vs competitive sport and number ofweekly hours spent on sports.
2.2 Other Comparisons
One way of indicating the relative extent of thesports injury problem is to compare the number ofsports injuries with, for instance, the number ofroad accidents or accidents at work.
Through the Home Accidents Surveillance System (PORS), for instance, a total of 32 276 accidents were recorded by the casualty departmentsof the hospitals participating in the scheme duringthe second 6 months of 1983. Of these, 28.6% related to sport, 14.9% to leisure-time games, 0.7%to occupational activities and 9.1% to road accidents (Stichting Consument en Veiligheid 1985).Clearly, sport and games account for the majority.
Davies (1981) noted that more consultationstook place at the casualty departments of Glasgowhospitals in 1979 for sports accidents than for roadaccidents. Williams (1975) estimated, without indicating how, that 5% of injuries treated at casualtydepartments in Great Britain related to sports accidents. Guyer and Ellers (1990) calculated thenumber of treatments of all unintentional childhood injuries (ages 0 to 19 years) in emergencywards of hospitals in 1985 in the US. Reasons fortreatment were: 48.5% not specified, 23.0% falls,16.3% sports and 7.1% traffic-related injuries.
In West Germany, Steinbriick and Cotta (1983)estimated that sports accidents made up 10 to 15%of total accidents and Von Schiirmeyer et al. (1983),on the basis of data from other sources, gives theproportion of sports accidents among total inpatient and outpatient cases as 5 to 10%.
In a I-year prospective study on acute sportsinjuries in a total population of a Swedish municipality with 31 620 inhabitants de Loes (1990) registered all emergency visits to the Public HealthCare. 571 sports injuries were registered; they madeup 17% of all acute injury visits, whereas acutehome injuries, acute work injuries and acute trafficinjuries made up 26, 19 and 7%, respectively (31 %
Sports Injury Research Terminology
specific types of sports are discussed below (seesection 2.2).
The outcome of research on the extent of thesports injury problem is highly dependent on definitions of 'sports injury', 'sports injury incidence'and 'sports participation', and that allowanceshould be made for exposure time when calculatingincidence. It should be borne in mind that the outcome of such research also depends on the appliedresearch design and research methodology, as wellas on the representativeness of the sample.
2. Sports Injury Data2.1 Sports Injury Incidence: The Netherlandsas an Example
Boersma-Sliitter et al. (1979) and Kranenborg(1980), using different methods, reach annual totalsof 560 000 (medically treated) and 1.2 million(medically and nonmedically treated) injuries, respectively, corresponding to yearly rates of 20 and46.5%. These figures are not directly comparable,since the 2 surveys differed, in particular with regard to sample, research method and definition of'sports injury'. Obviously this affects the interpretation of the figures.
Rogmans and Weerman (1982) calculated in asurvey of home and leisure time accidents that 21%of all accidents took place at sports and recreational locations; Verbeek et al. (1984) in a surveyof the frequency of and background to sports injuries among schoolchildren, arrived at a rate of10% a month; Inklaar (1985), using data from anongoing survey of morbidity in the Netherlands,calculated an average rate of 2.4% over a period of4 years.
Recently a representative nationwide telephonesurvey in the Netherlands revealed, in a totalpopulation of some 15 million, an overall sportsinjury incidence 00.3 (95% confidence limits: 3.1to 3.5) injuries per 1000 hours spent on sports; 1.4injuries per 1000 hours spent on sports were medically treated (van Galen & Diederiks 1990). In thisstudy an absolute number of 2.7 million sports injuries was calculated of which 1.7 million weremedically treated. Major sports injury incidence
87
differences per 1000 hours spent on sports werediscerned with regard to age, sex, specific sport,recreational vs competitive sport and number ofweekly hours spent on sports.
2.2 Other Comparisons
One way of indicating the relative extent of thesports injury problem is to compare the number ofsports injuries with, for instance, the number ofroad accidents or accidents at work.
Through the Home Accidents Surveillance System (PORS), for instance, a total of 32 276 accidents were recorded by the casualty departmentsof the hospitals participating in the scheme duringthe second 6 months of 1983. Of these, 28.6% related to sport, 14.9% to leisure-time games, 0.7%to occupational activities and 9.1% to road accidents (Stichting Consument en Veiligheid 1985).Clearly, sport and games account for the majority.
Davies (1981) noted that more consultationstook place at the casualty departments of Glasgowhospitals in 1979 for sports accidents than for roadaccidents. Williams (1975) estimated, without indicating how, that 5% of injuries treated at casualtydepartments in Great Britain related to sports accidents. Guyer and Ellers (1990) calculated thenumber of treatments of all unintentional childhood injuries (ages 0 to 19 years) in emergencywards of hospitals in 1985 in the US. Reasons fortreatment were: 48.5% not specified, 23.0% falls,16.3% sports and 7.1% traffic-related injuries.
In West Germany, Steinbriick and Cotta (1983)estimated that sports accidents made up 10 to 15%of total accidents and Von Schiirmeyer et al. (1983),on the basis of data from other sources, gives theproportion of sports accidents among total inpatient and outpatient cases as 5 to 10%.
In a I-year prospective study on acute sportsinjuries in a total population of a Swedish municipality with 31 620 inhabitants de Loes (1990) registered all emergency visits to the Public HealthCare. 571 sports injuries were registered; they madeup 17% of all acute injury visits, whereas acutehome injuries, acute work injuries and acute trafficinjuries made up 26, 19 and 7%, respectively (31 %

88
not defined). In a similar study, Sandelin et al.(1987) estimated that in the adult population inFinland about 1.5 million acute medically treatedinjuries occurred in 1980. Work-related injuriesmade up 17%, sports injuries 14% and traffic injuries 12%.
However, these studies record only relativelyserious accidents requiring medical attention andignore chronic injuries and less serious accidents.In addition, reliable incidence rates can not be calculated from data of this kind, since there are noprecise data on the population from which the injured are taken. Information on exposure time isalso lacking and in many cases the sample is notrepresentative (Walter et al. 1985).
A report by the Dutch Ministry of Health, Welfare and Cultural AtTairs (WVC 1985) gives a 'league table' based on inpatient and outpatient treatment records. This expresses the risk of sportsinjuries in terms of the number of injuries per 100practitioners ofeach sport. The highest risk is foundin soccer (4.2%), the lowest in skating and tabletennis (0.1 %). Unfortunately no allowance is madefor the fact that the amount of time spent on thevarious sports can ditTer, which in itself can atTectthe risk of receiving an injury. The orthopaedicclinic of the University of Heidelberg treated 8974injuries to 8204 spOrtspersons from 1972 to 1981.Steinbruck and Cotta (1983) analysed these injuries, calculating a risk factor for each sport fromthe number of recorded injuries and the total number of organised spOrtspersons in the region concerned. Each sport had a ditTerent risk factor, butagain no allowance was made for the ditTerentlengths of time spent on each sport. Van Galen andDiederiks (1990) made a similar 'league table' taking into account time spent on each sport, indoorsoccer was ranked number 1 with 8.7 injuries per1000 hours, basketball number 10 with 4.4 injuriesper 1000 hours and swimming number 20 with 1.2injuries per 1000 hours.
3. Severity of Sports Injuries
Severity can be described on the basis of 6 criteria:
• Nature of sports injury
Sports Medicine 14 (2) 1992
• Duration and nature of treatment• Sporting time lost• Working time lost• Permanent damage• Cost
3.1 Nature of Sports Injuries
Lysens and Ostyn (1984) give the followingcategories of medical diagnosis: sprain (of jointcapsule and ligaments), strain (of muscle or tendon), contusion (bruising), dislocation or subluxation, fracture (of bone), abrasion (graze), laceration (open wound), infection or inflammation, andconcussion.
In order to scale the severity of sports injuriesby medical diagnosis in some studies the AIS (Abbreviated Injury Scale) is used in which injuries aregraded 1 to 6, where 6 is the code for the mostsevere, virtually unsurvivable, injury (de Loes &Goldie 1988).
It is the nature of the injury that determineswhether assistance (medical or otherwise) is sought.It is known, for instance (Kranenborg 1981), thatapproximately 50% of injured kortball players seekmedical assistance by consulting their GP, takingphysiotherapy or attending a hospital casualty department. It is understandable that the other halfdoes not consider medical treatment necessary sincethe most common injuries in indoor korfball areabrasions and other injuries not requiring medicaltreatment (van GetTen et al. 1990).
In general the most common sports injuries arecontusions and sprains predominantly located onthe lower extremity (Beek & Murphy 1983; de Loes1990; Hensley & Paup 1979; Jungst et al. 1983;Krahl & von Steinbmck 1980; Kristiansen 1983;Maehlum 1984; Maehlum & Daljord 1984; Pfbrringer & Keyl 1978; Sandelin et al. 1987; Shively& Grana 1981; van Galen & Diederiks 1990; vanRens 1982; von Steinbmck & Cotta 1983, vonSteinbruck & Reiden 1984).
This is not true in every sport: fractures are themost common type of injury in horse-riding (Edixhoven et al. 1980; von Steinbmck 1980), hang-gliding (Penschuck 1980), parachute jumping (Stein-
88
not defined). In a similar study, Sandelin et al.(1987) estimated that in the adult population inFinland about 1.5 million acute medically treatedinjuries occurred in 1980. Work-related injuriesmade up 17%, sports injuries 14% and traffic injuries 12%.
However, these studies record only relativelyserious accidents requiring medical attention andignore chronic injuries and less serious accidents.In addition, reliable incidence rates can not be calculated from data of this kind, since there are noprecise data on the population from which the injured are taken. Information on exposure time isalso lacking and in many cases the sample is notrepresentative (Walter et al. 1985).
A report by the Dutch Ministry of Health, Welfare and Cultural AtTairs (WVC 1985) gives a 'league table' based on inpatient and outpatient treatment records. This expresses the risk of sportsinjuries in terms of the number of injuries per 100practitioners ofeach sport. The highest risk is foundin soccer (4.2%), the lowest in skating and tabletennis (0.1 %). Unfortunately no allowance is madefor the fact that the amount of time spent on thevarious sports can ditTer, which in itself can atTectthe risk of receiving an injury. The orthopaedicclinic of the University of Heidelberg treated 8974injuries to 8204 spOrtspersons from 1972 to 1981.Steinbruck and Cotta (1983) analysed these injuries, calculating a risk factor for each sport fromthe number of recorded injuries and the total number of organised spOrtspersons in the region concerned. Each sport had a ditTerent risk factor, butagain no allowance was made for the ditTerentlengths of time spent on each sport. Van Galen andDiederiks (1990) made a similar 'league table' taking into account time spent on each sport, indoorsoccer was ranked number 1 with 8.7 injuries per1000 hours, basketball number 10 with 4.4 injuriesper 1000 hours and swimming number 20 with 1.2injuries per 1000 hours.
3. Severity of Sports Injuries
Severity can be described on the basis of 6 criteria:
• Nature of sports injury
Sports Medicine 14 (2) 1992
• Duration and nature of treatment• Sporting time lost• Working time lost• Permanent damage• Cost
3.1 Nature of Sports Injuries
Lysens and Ostyn (1984) give the followingcategories of medical diagnosis: sprain (of jointcapsule and ligaments), strain (of muscle or tendon), contusion (bruising), dislocation or subluxation, fracture (of bone), abrasion (graze), laceration (open wound), infection or inflammation, andconcussion.
In order to scale the severity of sports injuriesby medical diagnosis in some studies the AIS (Abbreviated Injury Scale) is used in which injuries aregraded 1 to 6, where 6 is the code for the mostsevere, virtually unsurvivable, injury (de Loes &Goldie 1988).
It is the nature of the injury that determineswhether assistance (medical or otherwise) is sought.It is known, for instance (Kranenborg 1981), thatapproximately 50% of injured kortball players seekmedical assistance by consulting their GP, takingphysiotherapy or attending a hospital casualty department. It is understandable that the other halfdoes not consider medical treatment necessary sincethe most common injuries in indoor korfball areabrasions and other injuries not requiring medicaltreatment (van GetTen et al. 1990).
In general the most common sports injuries arecontusions and sprains predominantly located onthe lower extremity (Beek & Murphy 1983; de Loes1990; Hensley & Paup 1979; Jungst et al. 1983;Krahl & von Steinbmck 1980; Kristiansen 1983;Maehlum 1984; Maehlum & Daljord 1984; Pfbrringer & Keyl 1978; Sandelin et al. 1987; Shively& Grana 1981; van Galen & Diederiks 1990; vanRens 1982; von Steinbmck & Cotta 1983, vonSteinbruck & Reiden 1984).
This is not true in every sport: fractures are themost common type of injury in horse-riding (Edixhoven et al. 1980; von Steinbmck 1980), hang-gliding (Penschuck 1980), parachute jumping (Stein-

Sports Injury Research Terminology
berg 1988), roller skating (Horner & McCabe 1984;Jost et al. 1981; Kvidera & Franke11983) and skiing(Menke & Muller 1982). When assessing literaturewhich takes diagnosis as the yardstick for the severity of injuries one needs to know where and bywhom the injuries are examined. In the case of injuries treated at casualty departments there has already been a kind ofpreselection: these injuries areofa more serious kind. This could give the impression that sport produces only relatively serious,acute injuries. Overuse injuries (Kowal 1980; Orava et al. 1985) which have become much morecommon recently with the increasing popularity ofrecreational sports such as running and fitnesstraining, are not included in casualty departmentrecords.
Recording of the nature of sports injuries enables the sports with relatively serious injuries tobe identified. The need to prevent serious injuriesin a particular sport need not coincide with a highoverall incidence of injuries in that sport.
3.2 Duration and Nature of Treatment
Data on the duration and nature of treatmentcan be used to determine the severity of an injurymore precisely, especially ifit is a question ofwhatmedical bodies are involved in the treatment andwhat therapies used. The cost of medical treatmentcan be estimated (Tolpin et al. 1981), and the effectiveness of different therapies for similar injuries can be compared.
For example, in the municipality study of deLoes (1990) during 1 year, 571 acute injuries treatedin Public Health Care Clinics were registered. Those571 injuries led to a total of989 visits to the PublicHealth Clinics, being 4% of all visits (includingsports injury and nonsports injury visits). The average number of visits per sports injury was 1.9;fractures required 3.3 visits per injury, whilewounds required only 1.1 visits per injury. Eightpercent of the acutely injured sportspersons werehospitalised, with an average stay of 3.7 days perpatient: 4.8 days per patient for fractures and 2.0days per patient for contusions. In this study it was
89
clear that the nature ofa sports injury and the duration and nature of treatment are strongly related.
In a survey of 66 804 persons, any sports injurynoted as such by the interviewed persons was takendown by van Galen and Diederiks (1990): 945 injuries were registered retrospectively over a 4-weekrecall period. With regard to these injuries firsttreatment following injury, subsequent emergencytreatment and follow-up treatment were registered(table I).
Average number of subsequent treatments perinjury was also calculated: 4.9 for physiotherapy,3.9 for sports first-aid attendant, 2.6 for medicalspecialist, 2.3 for first-aid ward and 1.8 for GP.
3.3 Sports Time Lost
It is important for a sportsperson to be able totake up his or her sport again as soon as possibleafter an injury. Sport and exercise play an essentialpart in people's free time and thus influence theirmental well-being. The loss of sporting time is animportant psychosocial factor (Tsongas 1981). Thelength of sporting time lost gives the most preciseindication of the consequences of an injury to anindividual.
Schlattmann et at. (1986) classify the seriousness of injuries in accordance with NAIRS, into'minor' (1 to 7 days lost), 'moderately serious' (8to 21 days) and 'serious' (over 21 days or permanent damage).
Sandelin et at. (1987) classified 71% of injuriesas minor (absence from sport < 1 week), 20% asmoderate (absence from sport 1 to 3 weeks) and9% as severe, while de Loes and Goldie (1988)classified 20% as minor (absence from sport < 1week), 50% as moderate (absence from sport 1 to4 weeks) and 30% as severe.
Van Galen and Diederiks (1990) did not adoptthe NAIRS classification of seriousness. They usedthe cessation or reduction of training as an indication ofseriousness. In this study 56% ofall medically treated injuries led to the cessation or reduction of training as did 40% of all nonmedicallytreated injuries. There appeared to be a strong relationship between sporting time lost and: (a) the
Sports Injury Research Terminology
berg 1988), roller skating (Horner & McCabe 1984;Jost et al. 1981; Kvidera & Franke11983) and skiing(Menke & Muller 1982). When assessing literaturewhich takes diagnosis as the yardstick for the severity of injuries one needs to know where and bywhom the injuries are examined. In the case of injuries treated at casualty departments there has already been a kind ofpreselection: these injuries areofa more serious kind. This could give the impression that sport produces only relatively serious,acute injuries. Overuse injuries (Kowal 1980; Orava et al. 1985) which have become much morecommon recently with the increasing popularity ofrecreational sports such as running and fitnesstraining, are not included in casualty departmentrecords.
Recording of the nature of sports injuries enables the sports with relatively serious injuries tobe identified. The need to prevent serious injuriesin a particular sport need not coincide with a highoverall incidence of injuries in that sport.
3.2 Duration and Nature of Treatment
Data on the duration and nature of treatmentcan be used to determine the severity of an injurymore precisely, especially ifit is a question ofwhatmedical bodies are involved in the treatment andwhat therapies used. The cost of medical treatmentcan be estimated (Tolpin et al. 1981), and the effectiveness of different therapies for similar injuries can be compared.
For example, in the municipality study of deLoes (1990) during 1 year, 571 acute injuries treatedin Public Health Care Clinics were registered. Those571 injuries led to a total of989 visits to the PublicHealth Clinics, being 4% of all visits (includingsports injury and nonsports injury visits). The average number of visits per sports injury was 1.9;fractures required 3.3 visits per injury, whilewounds required only 1.1 visits per injury. Eightpercent of the acutely injured sportspersons werehospitalised, with an average stay of 3.7 days perpatient: 4.8 days per patient for fractures and 2.0days per patient for contusions. In this study it was
89
clear that the nature ofa sports injury and the duration and nature of treatment are strongly related.
In a survey of 66 804 persons, any sports injurynoted as such by the interviewed persons was takendown by van Galen and Diederiks (1990): 945 injuries were registered retrospectively over a 4-weekrecall period. With regard to these injuries firsttreatment following injury, subsequent emergencytreatment and follow-up treatment were registered(table I).
Average number of subsequent treatments perinjury was also calculated: 4.9 for physiotherapy,3.9 for sports first-aid attendant, 2.6 for medicalspecialist, 2.3 for first-aid ward and 1.8 for GP.
3.3 Sports Time Lost
It is important for a sportsperson to be able totake up his or her sport again as soon as possibleafter an injury. Sport and exercise play an essentialpart in people's free time and thus influence theirmental well-being. The loss of sporting time is animportant psychosocial factor (Tsongas 1981). Thelength of sporting time lost gives the most preciseindication of the consequences of an injury to anindividual.
Schlattmann et at. (1986) classify the seriousness of injuries in accordance with NAIRS, into'minor' (1 to 7 days lost), 'moderately serious' (8to 21 days) and 'serious' (over 21 days or permanent damage).
Sandelin et at. (1987) classified 71% of injuriesas minor (absence from sport < 1 week), 20% asmoderate (absence from sport 1 to 3 weeks) and9% as severe, while de Loes and Goldie (1988)classified 20% as minor (absence from sport < 1week), 50% as moderate (absence from sport 1 to4 weeks) and 30% as severe.
Van Galen and Diederiks (1990) did not adoptthe NAIRS classification of seriousness. They usedthe cessation or reduction of training as an indication ofseriousness. In this study 56% ofall medically treated injuries led to the cessation or reduction of training as did 40% of all nonmedicallytreated injuries. There appeared to be a strong relationship between sporting time lost and: (a) the

90 Sports Medicine 14 (2) 1992
Table I. Percentage of patients receiving various forms of treatment for sports injuries (van Galen & Diederiks 1990)
Treatment given by
Self-treated
Sports first-aid attendant
General practitioner
Hospital first-aid ward
Physiotherapist
Medical specialist
Sports masseur
First treatment following injury
(n = 692)
3024
29970.415
Subsequent emergencytreatment (n =119)
13182631na
7
6
Follow-up treatment
(n =263)
92612282
11
12
Abbreviation: na = not applicable.
number of treatments; (b) injury site; and (c) medical diagnosis.
From these 3 population studies it can be concluded that 50 to 60% of all sports injuries do notlead to a substantial loss of sporting time.
3.4 Working Time Lost
Like the cost of medical treatment, the lengthof working time lost gives an indication of the financial consequences of sports injuries to society.If official statistics are used, e.g. data from the Industrial Insurance Administration Office and Industrial Insurance Boards, many people, includingstudents, old age pensioners, the disabled, the unemployed, the self-employed, housewives and civilservants, are excluded (Vermeer 1982). Data of thiskind can be used to compare the cost to society ofsports injuries with that of other situations involving risks, such as work and traffic (Kranenborg1982). The comparison is of particular importanceto official bodies wanting to have the consequencesof sports injuries covered by a separate insurancescheme. Sandelin et al. (1987), in a municipalitystudy, registered medically treated acute sports injuries; 29% resulted in sick leave, ofwhich 50% didnot exceed I week.
In a I-year municipality study de Loes (1990)recorded that compensated work-related sick leavewas taken for 162 (29%) of those injuries, with anaverage length of sick-leave of 21.5 days. Van Galenand Diederiks (1990) found that of 945 injured
sportspersons II % lost work time (average duration 8.8 days), 7% lost study time (average duration 5.6 days) and 3% lost other daily activity time(average duration 5.9 days).
However, sporting activities may reduce theamount of sick leave taken by improving employees' general physical and mental condition. A costbenefit analysis of the positive and negative effectsof sporting activities on loss of working time isneeded (Shephard 1985). According to Sorensen andSonne-Holm (1980), the adverse socioeconomic effects of sports injuries are negligible in comparisonwith the positive effect of sporting activities. Aneconomic analysis of the effect of sports participation on working time (van Puffelen et al. 1989)revealed a loss of working time as a result of sportsparticipation in the age groups 18 to 34 and 55+years rather than a gain. Only in the 35- to 54-yearold age group could a positive effect on workingtime be found. Even in this study, however, theoverall effect on working time lost was calculatedto be negative.
3.5 Permanent Damage
The vast majority of sports injuries heal without permanent disability. Serious injuries (according to the NAIRS classification) such as fractures,ligament, tendon and intra-articular injuries (Kent1982), spinal injuries (Torg et al. 1979) and eyeinjuries (Vinger 1981) can leave permanent damage (residual symptoms). Excessive delay between
90 Sports Medicine 14 (2) 1992
Table I. Percentage of patients receiving various forms of treatment for sports injuries (van Galen & Diederiks 1990)
Treatment given by
Self-treated
Sports first-aid attendant
General practitioner
Hospital first-aid ward
Physiotherapist
Medical specialist
Sports masseur
First treatment following injury
(n = 692)
3024
29970.415
Subsequent emergencytreatment (n =119)
13182631na
7
6
Follow-up treatment
(n =263)
92612282
11
12
Abbreviation: na = not applicable.
number of treatments; (b) injury site; and (c) medical diagnosis.
From these 3 population studies it can be concluded that 50 to 60% of all sports injuries do notlead to a substantial loss of sporting time.
3.4 Working Time Lost
Like the cost of medical treatment, the lengthof working time lost gives an indication of the financial consequences of sports injuries to society.If official statistics are used, e.g. data from the Industrial Insurance Administration Office and Industrial Insurance Boards, many people, includingstudents, old age pensioners, the disabled, the unemployed, the self-employed, housewives and civilservants, are excluded (Vermeer 1982). Data of thiskind can be used to compare the cost to society ofsports injuries with that of other situations involving risks, such as work and traffic (Kranenborg1982). The comparison is of particular importanceto official bodies wanting to have the consequencesof sports injuries covered by a separate insurancescheme. Sandelin et al. (1987), in a municipalitystudy, registered medically treated acute sports injuries; 29% resulted in sick leave, ofwhich 50% didnot exceed I week.
In a I-year municipality study de Loes (1990)recorded that compensated work-related sick leavewas taken for 162 (29%) of those injuries, with anaverage length of sick-leave of 21.5 days. Van Galenand Diederiks (1990) found that of 945 injured
sportspersons II % lost work time (average duration 8.8 days), 7% lost study time (average duration 5.6 days) and 3% lost other daily activity time(average duration 5.9 days).
However, sporting activities may reduce theamount of sick leave taken by improving employees' general physical and mental condition. A costbenefit analysis of the positive and negative effectsof sporting activities on loss of working time isneeded (Shephard 1985). According to Sorensen andSonne-Holm (1980), the adverse socioeconomic effects of sports injuries are negligible in comparisonwith the positive effect of sporting activities. Aneconomic analysis of the effect of sports participation on working time (van Puffelen et al. 1989)revealed a loss of working time as a result of sportsparticipation in the age groups 18 to 34 and 55+years rather than a gain. Only in the 35- to 54-yearold age group could a positive effect on workingtime be found. Even in this study, however, theoverall effect on working time lost was calculatedto be negative.
3.5 Permanent Damage
The vast majority of sports injuries heal without permanent disability. Serious injuries (according to the NAIRS classification) such as fractures,ligament, tendon and intra-articular injuries (Kent1982), spinal injuries (Torg et al. 1979) and eyeinjuries (Vinger 1981) can leave permanent damage (residual symptoms). Excessive delay between
Sports Injury Research Terminology
the occurrence of an injury and the medical assistance can aggravate the injury (Kent 1982). Ifthe residual symptoms are slight, they may causethe individual to modify his or her level of sportingactivity. In some cases, however, he or she mayhave to choose another sport or give up sport altogether. Serious physical damage can cause permanent disability or death (Dolmans 1985; Koplan1970), thus reducing or eliminating the individual's capacity for work. When taking precautions,then, priority should be given to measures in sportswhere such injuries are common, even though theparticular sport itself is characterised by a low incidence of sports injuries and/or a low absolutenumber of participants. The government could playa major part here (Tsongas 1981). In a study bySandelin et al. (1987) II % of the patients complained of some late sequelae from their initialtrauma 2 years after injury. In the majority ofcasesthe initial trauma was a sprain type.
3.6 Costs of Sports Injuries
The calculation of the costs of sports injuriesessentially involves the expression of the abovementioned 5 categories of seriousness of sports injuries in economic terms. A general classificationof the economic costs of sports injuries is set outby Tolpin et al. (1981). The economic costs are divided into:
1. Direct costs, i.e. the cost of medical treatment (diagnostic expenses such as x-rays, doctor's fee, cost of medicines, admission costs, etc.)2. Indirect costs, i.e. expenditure incurred inconnection with the loss of productivity due toincreased morbidity and mortality levels (lossof working time and expertise due to death orhandicap).Social costs can be classified as quantifiable and
unquantifiable. Quantifiable costs include insurance and legal expenses. Unquantifiable costs arethe harmful effects of a sports injury on the psychosocial life of the individual or his family, e.g.owing to economic dependence, loss of social statusor position or social isolation. These costs are
91
quantifiable only to the extent that the quality oflife is quantifiable (Miles 1979).
In the view of Tolpin et al. (1981) an adequateinjury registration system is essential to any assessment of the total cost associated with sportsinjuries. The system must be reliable and continuous. Any cost analysis must identify the sportswhich are most 'expensive' for the community (Sorensen & Sonne-Holm 1980), so that the first interventions can be taken there.
The social consequences can to some extent beexpressed in figures, and would seem to be of nosmall extent. Vermeer (1982), for instance, calculated that compulsorily insured persons alone lost1 073 000 working days as a result of sports injuries in 1979. This corresponds to sickness benefitpaid out under the compulsory insurance schemeof over $US50 million. Vermeer explicitly notesthat school children, students, civil servants, members of the armed forces, old age pensioners, widows and self-employed persons were not includedin this calculation.
The direct and indirect costs in the Netherlandsassociated with medically treated sports injurieshave been estimated to run up to $US225 million(Den Toom & Schuurman 1988).
Steinbriick and Cotta (1983) estimated the annual cost of sports injuries in West Germany atover $US2500 million. Matter et al. (1982) usedinsurance company data to estimate the direct andindirect cost of skiiing accidents in Switzerlandfrom 1978 to 1980 at $USI2 900000. Tolpin et al.(1981) calculated that some $US6 million werespent on medical treatment of eye injuries receivedin the course of sporting activities in the US in1980. The total cost of roller saking accidents inthe US has been estimated at $US100 million perannum (Kvidera & Frankel 1983). In the US manybaseball and softball injuries are incurred in basesliding. The average medical cost per base slidinginjury was estimated to be $USI223, and it wascalculated that the installation of break-away basesacross the US would save $US2 billion in medicalcosts per year (Janda et al. 1990). Guyer and Ellers(1990) estimated the total cost of hospital inpatientand emergency department treatment of children
Sports Injury Research Terminology
the occurrence of an injury and the medical assistance can aggravate the injury (Kent 1982). Ifthe residual symptoms are slight, they may causethe individual to modify his or her level of sportingactivity. In some cases, however, he or she mayhave to choose another sport or give up sport altogether. Serious physical damage can cause permanent disability or death (Dolmans 1985; Koplan1970), thus reducing or eliminating the individual's capacity for work. When taking precautions,then, priority should be given to measures in sportswhere such injuries are common, even though theparticular sport itself is characterised by a low incidence of sports injuries and/or a low absolutenumber of participants. The government could playa major part here (Tsongas 1981). In a study bySandelin et al. (1987) II % of the patients complained of some late sequelae from their initialtrauma 2 years after injury. In the majority ofcasesthe initial trauma was a sprain type.
3.6 Costs of Sports Injuries
The calculation of the costs of sports injuriesessentially involves the expression of the abovementioned 5 categories of seriousness of sports injuries in economic terms. A general classificationof the economic costs of sports injuries is set outby Tolpin et al. (1981). The economic costs are divided into:
1. Direct costs, i.e. the cost of medical treatment (diagnostic expenses such as x-rays, doctor's fee, cost of medicines, admission costs, etc.)2. Indirect costs, i.e. expenditure incurred inconnection with the loss of productivity due toincreased morbidity and mortality levels (lossof working time and expertise due to death orhandicap).Social costs can be classified as quantifiable and
unquantifiable. Quantifiable costs include insurance and legal expenses. Unquantifiable costs arethe harmful effects of a sports injury on the psychosocial life of the individual or his family, e.g.owing to economic dependence, loss of social statusor position or social isolation. These costs are
91
quantifiable only to the extent that the quality oflife is quantifiable (Miles 1979).
In the view of Tolpin et al. (1981) an adequateinjury registration system is essential to any assessment of the total cost associated with sportsinjuries. The system must be reliable and continuous. Any cost analysis must identify the sportswhich are most 'expensive' for the community (Sorensen & Sonne-Holm 1980), so that the first interventions can be taken there.
The social consequences can to some extent beexpressed in figures, and would seem to be of nosmall extent. Vermeer (1982), for instance, calculated that compulsorily insured persons alone lost1 073 000 working days as a result of sports injuries in 1979. This corresponds to sickness benefitpaid out under the compulsory insurance schemeof over $US50 million. Vermeer explicitly notesthat school children, students, civil servants, members of the armed forces, old age pensioners, widows and self-employed persons were not includedin this calculation.
The direct and indirect costs in the Netherlandsassociated with medically treated sports injurieshave been estimated to run up to $US225 million(Den Toom & Schuurman 1988).
Steinbriick and Cotta (1983) estimated the annual cost of sports injuries in West Germany atover $US2500 million. Matter et al. (1982) usedinsurance company data to estimate the direct andindirect cost of skiiing accidents in Switzerlandfrom 1978 to 1980 at $USI2 900000. Tolpin et al.(1981) calculated that some $US6 million werespent on medical treatment of eye injuries receivedin the course of sporting activities in the US in1980. The total cost of roller saking accidents inthe US has been estimated at $US100 million perannum (Kvidera & Frankel 1983). In the US manybaseball and softball injuries are incurred in basesliding. The average medical cost per base slidinginjury was estimated to be $USI223, and it wascalculated that the installation of break-away basesacross the US would save $US2 billion in medicalcosts per year (Janda et al. 1990). Guyer and Ellers(1990) estimated the total cost of hospital inpatientand emergency department treatment of children

92 Sports Medicine 14 (2) 1992
are different from health promotional exercise andfitness programmes.
4. Aetiology and Prevention ofSports Injuries
Table II. Internal (personal) and external (environmental) risk
factors which may play a part in sports injuries (van Mechelenet al. 1987)
Risk factors can be divided into 2 main categories (Backx et al. 1990; Medved et al. 1973; Miles1979; Rozendal et al. 1979; Schlatmann et al. 1986;Segesser 1983; van Enst 1982; van Vulpen 1989).
The first category comprises the internal personal factors, the second the external, environmental factors. Data from the literature (vanMechelen et al. 1987) enable the factors to be classified into these 2 types, internal and external (tableII).
This division is based on partly proven, partlysupposed causal relationships between the risk factors and the injury. However, it may well be that
External factorsSports-related factors
type of sportexposurenature of eventrole of opponentsand team mates
Venuestate of floor or groundlightingsafety measures
Equipment
tools. e.g. stick or racket
risk acceptance
protective equipment
other equipment (shoes.clothing etc.)
Weather conditions
temperaturerelative humidity
windTrainer
conduct of matchrules
referee's application of
rules
Internal factorsPhysical defectPhysical fitness
aerobic endurancestrengthspeed
sporting skill/coordinationflexibility of muscles
Previous injuryPsychological factors
self-concept
risk acceptance
type A and type Cpersonality
locus of control
Physical build
height
weight
joint stability
body fatAge
Sex
(0 to 19 years) in the US in 1982 as a result ofsports injuries was $US580.8 million of a total of$US7544.9 million, ranking third after traffic-related injuries $US2785.2 million and injuries as aresult of a fall $US809.6 million. Davison and Ryan(1988) estimate the total cost of treatment by anoutpatient sports injury clinic in the UK to be£89.25 per injury. De Loes (1990) calculated anoverall mean of direct and indirect cost of $US335per acute medically treated sports injury, identifying motorcycling, downhill skiing and equinesports as the most expensive sports, respectively$US618, $US400 and $US393.
It should be noted, however, that due to differences in healthcare systems and wage compensation systems international comparisons may behampered. Even at a national level similar injuriesmay produce different costs in different states, asdemonstrated by Pritchett (1980) with regard to thecost of high school football injuries in the 6 western states of the US.
Van Puffelen et al. (1989) calculated that sportsparticipation resulted in an overall positive balance of 155 million Dutch guilders per annum forThe Netherlands. However, a closer look at the 4subcategories of costs analysed presented a diversepicture; there was a 23.3 million guilders positivebalance with regard to GP consultation, a 22.1 million guilders negative balance as a result of the consultation of medical specialists, a 286.1 millionguilders positive balance for inpatient treatment anda 130.2 million guilders negative balance due toworking time lost.
In a review on 'the economics of fitness andsport with particular reference to worksite programmes' which was not specifically aimed at thedescription of the costs of sports injuries but at anoverall cost-benefit analysis of fitness and sportsShephard (1989) concluded that, worksite exerciseand fitness programmes 'appear to be both cost effective and cost beneficial' and that 'a return in therange of $US2 to $US5 for every dollar investedwith a total package of health promotion is achievable'. It should be noted, however, that competitive sports, in which most injuries are sustained,
92 Sports Medicine 14 (2) 1992
are different from health promotional exercise andfitness programmes.
4. Aetiology and Prevention ofSports Injuries
Table II. Internal (personal) and external (environmental) risk
factors which may play a part in sports injuries (van Mechelenet al. 1987)
Risk factors can be divided into 2 main categories (Backx et al. 1990; Medved et al. 1973; Miles1979; Rozendal et al. 1979; Schlatmann et al. 1986;Segesser 1983; van Enst 1982; van Vulpen 1989).
The first category comprises the internal personal factors, the second the external, environmental factors. Data from the literature (vanMechelen et al. 1987) enable the factors to be classified into these 2 types, internal and external (tableII).
This division is based on partly proven, partlysupposed causal relationships between the risk factors and the injury. However, it may well be that
External factorsSports-related factors
type of sportexposurenature of eventrole of opponentsand team mates
Venuestate of floor or groundlightingsafety measures
Equipment
tools. e.g. stick or racket
risk acceptance
protective equipment
other equipment (shoes.clothing etc.)
Weather conditions
temperaturerelative humidity
windTrainer
conduct of matchrules
referee's application of
rules
Internal factorsPhysical defectPhysical fitness
aerobic endurancestrengthspeed
sporting skill/coordinationflexibility of muscles
Previous injuryPsychological factors
self-concept
risk acceptance
type A and type Cpersonality
locus of control
Physical build
height
weight
joint stability
body fatAge
Sex
(0 to 19 years) in the US in 1982 as a result ofsports injuries was $US580.8 million of a total of$US7544.9 million, ranking third after traffic-related injuries $US2785.2 million and injuries as aresult of a fall $US809.6 million. Davison and Ryan(1988) estimate the total cost of treatment by anoutpatient sports injury clinic in the UK to be£89.25 per injury. De Loes (1990) calculated anoverall mean of direct and indirect cost of $US335per acute medically treated sports injury, identifying motorcycling, downhill skiing and equinesports as the most expensive sports, respectively$US618, $US400 and $US393.
It should be noted, however, that due to differences in healthcare systems and wage compensation systems international comparisons may behampered. Even at a national level similar injuriesmay produce different costs in different states, asdemonstrated by Pritchett (1980) with regard to thecost of high school football injuries in the 6 western states of the US.
Van Puffelen et al. (1989) calculated that sportsparticipation resulted in an overall positive balance of 155 million Dutch guilders per annum forThe Netherlands. However, a closer look at the 4subcategories of costs analysed presented a diversepicture; there was a 23.3 million guilders positivebalance with regard to GP consultation, a 22.1 million guilders negative balance as a result of the consultation of medical specialists, a 286.1 millionguilders positive balance for inpatient treatment anda 130.2 million guilders negative balance due toworking time lost.
In a review on 'the economics of fitness andsport with particular reference to worksite programmes' which was not specifically aimed at thedescription of the costs of sports injuries but at anoverall cost-benefit analysis of fitness and sportsShephard (1989) concluded that, worksite exerciseand fitness programmes 'appear to be both cost effective and cost beneficial' and that 'a return in therange of $US2 to $US5 for every dollar investedwith a total package of health promotion is achievable'. It should be noted, however, that competitive sports, in which most injuries are sustained,

Sports Injury Research Terminology 93
Fig. 2. Two examples of possible causal relationships between a known risk factor and a sports injury (adapted fromLast 1988). F represents an unknown third factor.
both risk factor and injury are dependent on thesame third factor in different ways (fig. 2; Last1988). Thus, lowering the factor 'F reduces the riskof injury in figure 2a but not in figure 2b.
The classification into internal and external factors can be approached on the basis of the stress/capacity model, which was used in its classical formin The Netherlands in the field of social and preventative medicine to describe the interaction beteween humans and their environment (Ettema1973). It can also be applied in sports medicine,especially to the prevention of injuries. In thismodel the stress is determined by the sportsperson's environment, i.e. external factors. His or hercapacity is determined by the state of the internal,personal factors. Stress and capacity must be inbalance (Segesser 1983); preventative measuresmust therefore be designed to achieve or maintainthis balance, either by raising the capacity or reducing the stress or both. As the sportsman's capacity increases, proneness to injuries decreases. Inpractice this was seen mainly as a question of improving physical fitness. It is known that fatiguereduces movement coordination, thus increasingthe risk of injury. The incidence of injuries is higherthan 'average' in the preseason (Ekstrand 1982) andduring lengthy tournaments (Kersey & Rowan1983), perhaps owing to insufficient aerobic endurance resulting in fatigue setting in sooner. Poortechnique and lack ofexperience can also influencecapacity. Inexperienced squash players, for instance, cause more injuries than experienced onesboth to themselves and to others (Pforringer & Keyl1978).
1-----1.~ Risk factor
F
1-----1.~ Sports injury
(a)
(b)
F --..,~~ Risk factor --~.~ Sports injury According to the stress/capacity model, stresscan be reduced by changing the external, environmental factors. For instance, the introduction ofeye guards in squash reduced eye injury (Easterbrook 1982), the use of high top basketball shoesin combination with taping reduced the incidenceof ankle sprains in basketball (Garrick & Requa1973) and the introduction of mouthguards in fieldhockey reduced dental injuries (Bolhuis 1987).
Merely to establish the causes of sports injuries,i.e. the internal and external factors, is not enough;the mechanism by which they occur must also beidentified. Athletes are in constant interaction withtheir environment, and the risk factors must be approached from this angle. Miles (1977) formulateda 'sports injury equation', according to which theoccurrence of sports injuries is determined by 'luck,environment, attitude to risks, individual susceptibility to injuries, training factors, safety precautions, personal factors, etc.'.
It is now becoming clear that sports injuries result from a complex interaction of identifiable riskfactors, of which only a fraction seem to be identified (Lysens et al. 1984). The knowledge of riskfactors relevant for all sports or groups of sportsseems to be limited.
It should be stressed that the area of intrinsicrisk factors is highly conjectural and that manyplausible hypotheses lack substantiating evidenceat the present (Lorentzen 1988). In a report by theCouncil of Europe (van Vulpen 1989) it was concluded that most of the epidemiological studieshave concentrated on internal and external riskfactors from a medical, rather monocausal, pointof view and that little is known about the psychological and behavioural aspects of the occurrenceof sports injuries. Taerck's (1977) statement that'the multifaceted problem of what causes athleticinjuries has only rarely been studied from a psycho-social point of view' still holds in 1991. Crossman (1985) remarked that 'further in depth research investigating the psycho-social factorsinfluencing the incidence of injury is needed ... '
One of the few studies on psychosocial risk factors was performed by Lysens et al. (1986), whofound a relationship between psychosocial factors,
Sports Injury Research Terminology 93
Fig. 2. Two examples of possible causal relationships between a known risk factor and a sports injury (adapted fromLast 1988). F represents an unknown third factor.
both risk factor and injury are dependent on thesame third factor in different ways (fig. 2; Last1988). Thus, lowering the factor 'F reduces the riskof injury in figure 2a but not in figure 2b.
The classification into internal and external factors can be approached on the basis of the stress/capacity model, which was used in its classical formin The Netherlands in the field of social and preventative medicine to describe the interaction beteween humans and their environment (Ettema1973). It can also be applied in sports medicine,especially to the prevention of injuries. In thismodel the stress is determined by the sportsperson's environment, i.e. external factors. His or hercapacity is determined by the state of the internal,personal factors. Stress and capacity must be inbalance (Segesser 1983); preventative measuresmust therefore be designed to achieve or maintainthis balance, either by raising the capacity or reducing the stress or both. As the sportsman's capacity increases, proneness to injuries decreases. Inpractice this was seen mainly as a question of improving physical fitness. It is known that fatiguereduces movement coordination, thus increasingthe risk of injury. The incidence of injuries is higherthan 'average' in the preseason (Ekstrand 1982) andduring lengthy tournaments (Kersey & Rowan1983), perhaps owing to insufficient aerobic endurance resulting in fatigue setting in sooner. Poortechnique and lack ofexperience can also influencecapacity. Inexperienced squash players, for instance, cause more injuries than experienced onesboth to themselves and to others (Pforringer & Keyl1978).
1-----1.~ Risk factor
F
1-----1.~ Sports injury
(a)
(b)
F --..,~~ Risk factor --~.~ Sports injury According to the stress/capacity model, stresscan be reduced by changing the external, environmental factors. For instance, the introduction ofeye guards in squash reduced eye injury (Easterbrook 1982), the use of high top basketball shoesin combination with taping reduced the incidenceof ankle sprains in basketball (Garrick & Requa1973) and the introduction of mouthguards in fieldhockey reduced dental injuries (Bolhuis 1987).
Merely to establish the causes of sports injuries,i.e. the internal and external factors, is not enough;the mechanism by which they occur must also beidentified. Athletes are in constant interaction withtheir environment, and the risk factors must be approached from this angle. Miles (1977) formulateda 'sports injury equation', according to which theoccurrence of sports injuries is determined by 'luck,environment, attitude to risks, individual susceptibility to injuries, training factors, safety precautions, personal factors, etc.'.
It is now becoming clear that sports injuries result from a complex interaction of identifiable riskfactors, of which only a fraction seem to be identified (Lysens et al. 1984). The knowledge of riskfactors relevant for all sports or groups of sportsseems to be limited.
It should be stressed that the area of intrinsicrisk factors is highly conjectural and that manyplausible hypotheses lack substantiating evidenceat the present (Lorentzen 1988). In a report by theCouncil of Europe (van Vulpen 1989) it was concluded that most of the epidemiological studieshave concentrated on internal and external riskfactors from a medical, rather monocausal, pointof view and that little is known about the psychological and behavioural aspects of the occurrenceof sports injuries. Taerck's (1977) statement that'the multifaceted problem of what causes athleticinjuries has only rarely been studied from a psycho-social point of view' still holds in 1991. Crossman (1985) remarked that 'further in depth research investigating the psycho-social factorsinfluencing the incidence of injury is needed ... '
One of the few studies on psychosocial risk factors was performed by Lysens et al. (1986), whofound a relationship between psychosocial factors,

94
such as high level of life change and stress coping,and the occurrence of sports injuries. In a reviewby Kelley (1990) of psychological risk factors andsports injuries 11 psychological risk factors arementioned including high levels of positive or negative life change; high levels of tyPe A behaviour(people who are often seen as aggressive, harddriving, ruled by the clock and obsessed with accomplishing more than time will allow) and typeC behaviour (people who are classified as dependent, sweet, passive, gentle and nice, but also resentful, unforgiving, worried, anxious, bored, frustrated and apathetic); high levels of trait anxiety,poor reaction and movement times due to poorattentional focus; high or low tolerance ofpain; highlevels of extraverted or introverted behaviour; behaviour associated with insecurity, overprotectionand dependency; behaviour which reflects that theathlete feels little control over the athletic situation; behaviour which reflects poor self-concept andpoor self-esteem; experience of conflict betweenpassivity and aggression; and high levels ofdepression. The research of Lysens et al. (1986) and theabove-mentioned shift in approach towards thepsychosocial aspects of the occurrence of sports injuries draws attention to the fact that the injuryrisk is primarily dependent on the interaction between athletes and their personal characteristics,either physical or psychological, and the sports environment. This requires a more dynamic model(modified after Backx et al. 1990; Bol et al. 1991;Kok & Bouter 1990), as presented in figure 3, onthe interrelation between the various risk factorsand the occurrence of a sports injury and subsequent preventative measures, rather than the scalebalance approach of the classical stress/capacitymodel.
This model focuses on 'sports behaviour' whichmay lead to an injury. Risk factors, such as thoserelating to the athlete, the sports environment, personal equipment and load are seen as external variables, all (causally) involved in the activity andpossibly leading to an injury. When such behaviour is identified with acceptable certainty the determinants of behaviour must be clarified (Kok &Bouter 1990).
Sports Medicine 14 (2) 1992
Three factors are distinguished as determinantsof behaviour: (a) attitude; (b) social influence; and(c) self-efficacy-cum-barriers. Kok and Bouter(1990) describe these determinants as follows:
1. 'Attitude refers to the knowledge and beliefsof a person concerning the specific consequences of a certain form of behaviour. An attitude is the weighing of all consequences of theperformance of the behaviour, as seen by theindividual. Health is only seen as one of theconsiderations, and is often an unimportant one.When health is part of attitude one may suppose that healthy motivation is a combinationof the perceived severity of the health risk, theperceived susceptibility to the health risk, andthe effectiveness of the preventive behaviour.'2. 'Social influence is the influence by others;directly by what others expect, indirectly by whatothers do (modeling).' 'Social influence is oftenunderestimated as a determinant of behaviour.It can lead to behaviour that conflicts with previous attitudes. Most sports situations are socialsituations.'3. 'Self-efficacy-cum-barriers stands for the determinant whether one is able to perform the(desired) behaviour. It involves an estimationof ability, taking into account possible internal(e.g. insufficient skiU, knowledge, endurance) orexternal barriers (e.g. resistance from others,time and money not available, etc.). Self-efficacy is the people's perception of their abilityto perform the behaviour, and barriers are thereal problems they face in actually performingthe behaviour.'Whether or not an injury results from sports be
haviour largely depends on the extent to which'prevention' is incorporated in the determinants ofbehaviour.
Regardless of whether the aetiology and prevention of sports injuries are approached from abalance-scale or behaviour-oriented, more complex perspective at least 1 problem remains. Neither approach adequately accounts for the aetiology of overuse injuries, which constitute about 10%ofall sports injuries (van Galen & Diederiks 1990).Overuse injuries develop over long periods and are
94
such as high level of life change and stress coping,and the occurrence of sports injuries. In a reviewby Kelley (1990) of psychological risk factors andsports injuries 11 psychological risk factors arementioned including high levels of positive or negative life change; high levels of tyPe A behaviour(people who are often seen as aggressive, harddriving, ruled by the clock and obsessed with accomplishing more than time will allow) and typeC behaviour (people who are classified as dependent, sweet, passive, gentle and nice, but also resentful, unforgiving, worried, anxious, bored, frustrated and apathetic); high levels of trait anxiety,poor reaction and movement times due to poorattentional focus; high or low tolerance ofpain; highlevels of extraverted or introverted behaviour; behaviour associated with insecurity, overprotectionand dependency; behaviour which reflects that theathlete feels little control over the athletic situation; behaviour which reflects poor self-concept andpoor self-esteem; experience of conflict betweenpassivity and aggression; and high levels ofdepression. The research of Lysens et al. (1986) and theabove-mentioned shift in approach towards thepsychosocial aspects of the occurrence of sports injuries draws attention to the fact that the injuryrisk is primarily dependent on the interaction between athletes and their personal characteristics,either physical or psychological, and the sports environment. This requires a more dynamic model(modified after Backx et al. 1990; Bol et al. 1991;Kok & Bouter 1990), as presented in figure 3, onthe interrelation between the various risk factorsand the occurrence of a sports injury and subsequent preventative measures, rather than the scalebalance approach of the classical stress/capacitymodel.
This model focuses on 'sports behaviour' whichmay lead to an injury. Risk factors, such as thoserelating to the athlete, the sports environment, personal equipment and load are seen as external variables, all (causally) involved in the activity andpossibly leading to an injury. When such behaviour is identified with acceptable certainty the determinants of behaviour must be clarified (Kok &Bouter 1990).
Sports Medicine 14 (2) 1992
Three factors are distinguished as determinantsof behaviour: (a) attitude; (b) social influence; and(c) self-efficacy-cum-barriers. Kok and Bouter(1990) describe these determinants as follows:
1. 'Attitude refers to the knowledge and beliefsof a person concerning the specific consequences of a certain form of behaviour. An attitude is the weighing of all consequences of theperformance of the behaviour, as seen by theindividual. Health is only seen as one of theconsiderations, and is often an unimportant one.When health is part of attitude one may suppose that healthy motivation is a combinationof the perceived severity of the health risk, theperceived susceptibility to the health risk, andthe effectiveness of the preventive behaviour.'2. 'Social influence is the influence by others;directly by what others expect, indirectly by whatothers do (modeling).' 'Social influence is oftenunderestimated as a determinant of behaviour.It can lead to behaviour that conflicts with previous attitudes. Most sports situations are socialsituations.'3. 'Self-efficacy-cum-barriers stands for the determinant whether one is able to perform the(desired) behaviour. It involves an estimationof ability, taking into account possible internal(e.g. insufficient skiU, knowledge, endurance) orexternal barriers (e.g. resistance from others,time and money not available, etc.). Self-efficacy is the people's perception of their abilityto perform the behaviour, and barriers are thereal problems they face in actually performingthe behaviour.'Whether or not an injury results from sports be
haviour largely depends on the extent to which'prevention' is incorporated in the determinants ofbehaviour.
Regardless of whether the aetiology and prevention of sports injuries are approached from abalance-scale or behaviour-oriented, more complex perspective at least 1 problem remains. Neither approach adequately accounts for the aetiology of overuse injuries, which constitute about 10%ofall sports injuries (van Galen & Diederiks 1990).Overuse injuries develop over long periods and are

Sports Injury Research Terminology
Physical factors• body composition• health• physical fitness• skills
Load• type of sport• gamelpractice• recreation!
competition
Psychosocial factors• aims• risk taking• stress coping• motivation
Personal equipment• protective materials(shin guards, braces)
• instrumental materials(racket. stick, club)
• other materials(shoes. clothing)
95
Physical factors• acoommodation• weather• objects of handling• equipment (of others)
Human factors• team mates• opponent• referee• coach• spectators
Fig. 3. Determinants of sports behaviour (modified from Backx et aI. 1990; Bol et aI. 1991).
difficult to diagnose and to treat (Peterson & Renstrom 1986). The abovementioned models do notincorporate a time perspective.
For this reason a third approach (fig. 4) basedon a recent update of the stress/capacity model, asapplied in the field of occupational medicine, willbe discussed (van Dijk et al. 1990). This modeltakes into account the effects of training and overload over an extended period and behavioural aspects. It can therefore be useful in describing theaetiology of acute injuries, as well as overuse injuries.
The 'stress-strain-capacity model' is a time-based3-phase sequential model. In this model stress andcapacity are regarded as dynamic values in contrast to the classifical stress/capacity balance scalemodel in which stress and capacity were seen asmore or less static entities.
In the stress-strain-capacity model 'stress' is defined as external load, i.e. all external environmental factors affecting sports activity. 'Strain' isdefined as all processes by which responses in thebody are evoked as the result of stress and personalcontrol. 'Personal control' is defined as the ability
Sports Injury Research Terminology
Physical factors• body composition• health• physical fitness• skills
Load• type of sport• gamelpractice• recreation!
competition
Psychosocial factors• aims• risk taking• stress coping• motivation
Personal equipment• protective materials(shin guards, braces)
• instrumental materials(racket. stick, club)
• other materials(shoes. clothing)
95
Physical factors• acoommodation• weather• objects of handling• equipment (of others)
Human factors• team mates• opponent• referee• coach• spectators
Fig. 3. Determinants of sports behaviour (modified from Backx et aI. 1990; Bol et aI. 1991).
difficult to diagnose and to treat (Peterson & Renstrom 1986). The abovementioned models do notincorporate a time perspective.
For this reason a third approach (fig. 4) basedon a recent update of the stress/capacity model, asapplied in the field of occupational medicine, willbe discussed (van Dijk et al. 1990). This modeltakes into account the effects of training and overload over an extended period and behavioural aspects. It can therefore be useful in describing theaetiology of acute injuries, as well as overuse injuries.
The 'stress-strain-capacity model' is a time-based3-phase sequential model. In this model stress andcapacity are regarded as dynamic values in contrast to the classifical stress/capacity balance scalemodel in which stress and capacity were seen asmore or less static entities.
In the stress-strain-capacity model 'stress' is defined as external load, i.e. all external environmental factors affecting sports activity. 'Strain' isdefined as all processes by which responses in thebody are evoked as the result of stress and personalcontrol. 'Personal control' is defined as the ability
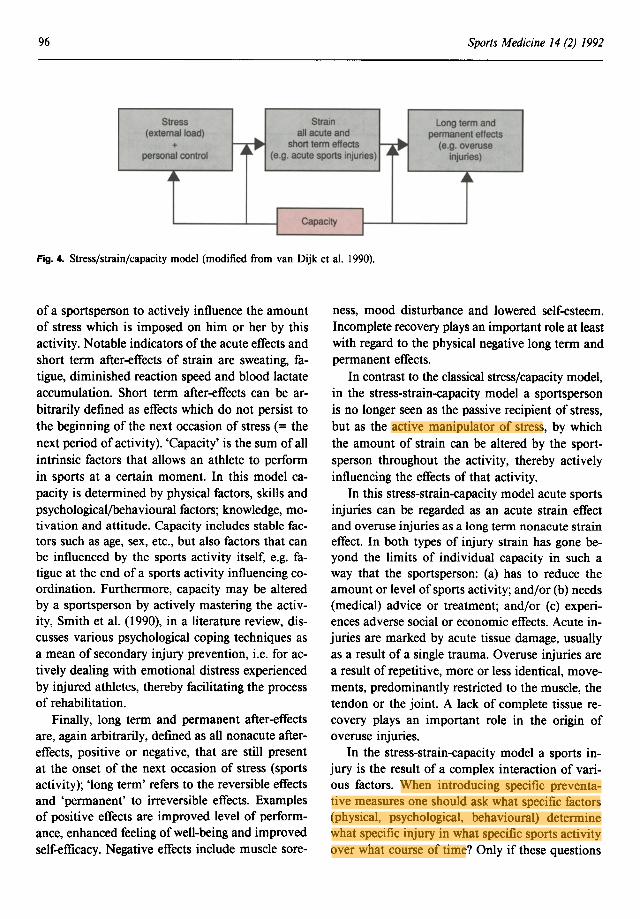
96 Sports Medicine 14 (2) 1992
Stress Strain Long term and(external load)
~~all acute and
~~permanent effects
+ short term effects (e.g. overusepersonal control (e.g. acute sports injuries) injuries)
o4~ .A"
I Capacity II
Fig. 4. Stress/strain/capacity model (modified from van Dijk et at. 1990).
of a sportsperson to actively influence the amountof stress which is imposed on him or her by thisactivity. Notable indicators of the acute effects andshort term after-effects of strain are sweating, fatigue, diminished reaction speed and blood lactateaccumulation. Short term after-effects can be arbitrarily defined as effects which do not persist tothe beginning of the next occasion of stress (= thenext period of activity). 'Capacity' is the sum of allintrinsic factors that allows an athlete to performin sports at a certain moment. In this model capacity is determined by physical factors, skills andpsychological/behavioural factors; knowledge, motivation and attitude. Capacity includes stable factors such as age, sex, etc., but also factors that canbe influenced by the sports activity itself, e.g. fatigue at the end of a sports activity influencing coordination. Furthermore, capacity may be alteredby a sportsperson by actively mastering the activity, Smith et at. (1990), in a literature review, discusses various psychological coping techniques asa mean of secondary injury prevention, i.e. for actively dealing with emotional distress experiencedby injured athletes, thereby facilitating the processof rehabilitation.
Finally, long term and permanent after-effectsare, again arbitrarily, defined as all nonacute aftereffects, positive or negative, that are still presentat the onset of the next occasion of stress (sportsactivity); 'long term' refers to the reversible effectsand 'permanent' to irreversible effects. Examplesof positive effects are improved level of performance, enhanced feeling of well-being and improvedself-efficacy. Negative effects include muscle sore-
ness, mood disturbance and lowered self-esteem.Incomplete recovery plays an important role at leastwith regard to the physical negative long term andpermanent effects.
In contrast to the classical stress/capacity model,in the stress-strain-eapacity model a sportspersonis no longer seen as the passive recipient of stress,but as the active manipulator of stress, by whichthe amount of strain can be altered by the sportsperson throughout the activity, thereby activelyinfluencing the effects of that activity.
In this stress-strain-eapacity model acute sportsinjuries can be regarded as an acute strain effectand overuse injuries as a long term nonacute straineffect. In both types of injury strain has gone beyond the limits of individual capacity in such away that the sportsperson: (a) has to reduce theamount or level of sports activity; and/or (b) needs(medical) advice or treatment; and/or (c) experiences adverse social or economic effects. Acute injuries are marked by acute tissue damage, usuallyas a result of a single trauma. Overuse injuries area result of repetitive, more or less identical, movements, predominantly restricted to the muscle, thetendon or the joint. A lack of complete tissue recovery plays an important role in the origin ofoveruse injuries.
In the stress-strain-eapacity model a sports injury is the result of a complex interaction of various factors. When introducing specific preventative measures one should ask what specific factors(physical, psychological, behavioural) determinewhat specific injury in what specific sports activityover what course of time? Only if these questions
96 Sports Medicine 14 (2) 1992
Stress Strain Long term and(external load)
~~all acute and
~~permanent effects
+ short term effects (e.g. overusepersonal control (e.g. acute sports injuries) injuries)
o4~ .A"
I Capacity II
Fig. 4. Stress/strain/capacity model (modified from van Dijk et at. 1990).
of a sportsperson to actively influence the amountof stress which is imposed on him or her by thisactivity. Notable indicators of the acute effects andshort term after-effects of strain are sweating, fatigue, diminished reaction speed and blood lactateaccumulation. Short term after-effects can be arbitrarily defined as effects which do not persist tothe beginning of the next occasion of stress (= thenext period of activity). 'Capacity' is the sum of allintrinsic factors that allows an athlete to performin sports at a certain moment. In this model capacity is determined by physical factors, skills andpsychological/behavioural factors; knowledge, motivation and attitude. Capacity includes stable factors such as age, sex, etc., but also factors that canbe influenced by the sports activity itself, e.g. fatigue at the end of a sports activity influencing coordination. Furthermore, capacity may be alteredby a sportsperson by actively mastering the activity, Smith et at. (1990), in a literature review, discusses various psychological coping techniques asa mean of secondary injury prevention, i.e. for actively dealing with emotional distress experiencedby injured athletes, thereby facilitating the processof rehabilitation.
Finally, long term and permanent after-effectsare, again arbitrarily, defined as all nonacute aftereffects, positive or negative, that are still presentat the onset of the next occasion of stress (sportsactivity); 'long term' refers to the reversible effectsand 'permanent' to irreversible effects. Examplesof positive effects are improved level of performance, enhanced feeling of well-being and improvedself-efficacy. Negative effects include muscle sore-
ness, mood disturbance and lowered self-esteem.Incomplete recovery plays an important role at leastwith regard to the physical negative long term andpermanent effects.
In contrast to the classical stress/capacity model,in the stress-strain-eapacity model a sportspersonis no longer seen as the passive recipient of stress,but as the active manipulator of stress, by whichthe amount of strain can be altered by the sportsperson throughout the activity, thereby activelyinfluencing the effects of that activity.
In this stress-strain-eapacity model acute sportsinjuries can be regarded as an acute strain effectand overuse injuries as a long term nonacute straineffect. In both types of injury strain has gone beyond the limits of individual capacity in such away that the sportsperson: (a) has to reduce theamount or level of sports activity; and/or (b) needs(medical) advice or treatment; and/or (c) experiences adverse social or economic effects. Acute injuries are marked by acute tissue damage, usuallyas a result of a single trauma. Overuse injuries area result of repetitive, more or less identical, movements, predominantly restricted to the muscle, thetendon or the joint. A lack of complete tissue recovery plays an important role in the origin ofoveruse injuries.
In the stress-strain-eapacity model a sports injury is the result of a complex interaction of various factors. When introducing specific preventative measures one should ask what specific factors(physical, psychological, behavioural) determinewhat specific injury in what specific sports activityover what course of time? Only if these questions

Sports Injury Research Terminology
are answered are all aetiological factors taken intoconsideration and effective prevention is possible.
Despite the importance of the model of choicein studying the risk factors of sports injuries, thechoice of research design is also important. Caseseries usually give no information on the underlying population at risk, so they are of no value indrawing valid conclusions on the risk factors of injuries. Only by relating the injuries to corresponding population denominators one can estimate injury rates and identify important risk factors andhigh risk sportspersons (Walter et al. 1985). As inresearch on sports injury incidence, research on riskfactors should be undertaken on groups homogeneous with regard to age, sex, level of competitionand type of sport (Bol et al. 1991).
4.1 Sport-Specificity of Sports Injuries
Many sports injuries are highly sports specificwhich is in accordance with the various aetiological models. The locations and types of injuriesfound in the studies ofparticular sports clearly showthat the type of sport determines both in manycases. Different injuries occur in wrestling (Snook1980, 1982) than in soccer (Ekstrand 1982; Kristiansen 1983; Maehlum 1984; ), running (Jacobs etal. 1986; Koplan et al. 1982; Macera et al. 1989;Marti et al. 1988; Walter et al. 1989), squash (Easterbrook 1982; Pforringer & Keyl 1978) or tennis(Kulund et al. 1979). Nomenclature such as 'tenniselbow', 'golfer's elbow' and 'jumper's knee' suggestthat particular injuries are sport-specific (Travers1980), and consequently that precautions againstinjuries should be sport-specific. On the other hand,sports where similar injuries occur could be groupedtogether, and similar measures could be taken forthese groups.
5. Conclusions
Incidence and severity provide a yardstick forthe first step of prevention of sports injuries. However, in order to get reliable and comparable data,uniform definitions and adequate research designsand methodology are needed. Various internal and
97
external risk factors for sports injuries have to beidentified. It should be kept in mind, however, thatsports injuries may have several causes, includingthe behaviour of the sportsperson, and that manyinjuries evolve over time. Conceptual models ofthe aetiology of sports injuries should therefore takebehaviour into account and should be time-based.The stress-strain-capacity model as presented is anexample of such a model.
Acknowledgement
This study was partly supported with a research grantof the Dutch Ministry of Welfare, Health and CulturalAffairs as a contribution to the Council of Europe research project 'Sport for All: Sports Injuries and TheirPrevention'.
References
Backous DD, Friedl KE, Smith NJ, Parr TJ, Csarpine Jr WD.Soccer injuries and their relation to physical maturity. American Journal of Diseases of Children 142 (8): 839-842,1988
Backx FJG, Inklaar H, Koornneef M, van Mechelen W. DraftFIMS position statement on the prevention of sports injuries.Geneeskunde en Sport, Special Issue, May, 1990
Backx FJG. Sports injuries in youth, etiology and prevention.Thesis, University of Utrecht, 1991
Murphy P, van Beek PA. Letsel bij volleybal. Geneeskunde enSport 16: 59-65, 1983
Boersma-Slutter, W, Brookman A, Lagra HM, Minderaa PH. Sport,een riskante zaak. Geneeskunde en Sport 12; 41-49, 1979
Bol E, Schmickli SL, Backx FJG, van Mechelen W. Sportblessures onder de knie, Nationaal Instituut voor SportGezonheidsZorg publication 38, Papendal, The Netherlands,1991
Bolhuis JHA. Tandletsel in de hockeysport. Thesis, University ofUtrecht, 1987
Brandt Cortstius JJ. Het voorkomen van sportblessures - prevoentie is meer dan vaststellen van incidentie. Masters thesis,Inter Faculteit der Lichamelijke Opvooding, Amsterdam, 1983
Caine D, Cockrane B, Cain C, Zemper E. An epidemiologic investigation of injuiries affecting young competitive femalegymnasts. American Journal of Sports Medicine 17: 811-820,1989
Chambers RB. Orthopedic injuries in athletes (ages 6 to 17): comparison of injuries occumng in six sports. American Journalof Sports Medicine 7: 195-197, 1979
Clement DB, Taunton JE. A guide to the prevention of runninginjuries. Australian Family Physician 10: 156-174, 1981
Crossman J. Psychosocial factors and athletic injury. Journal ofSports Medicine 25: 151-154, 1985
Davies JE. Sports injuries and society. British Journal of SportsMedicine 15: 80-83, 1981
Davison J, Ryan MP. A Sports Medicine clinic in the community. British Journal of Sports Medicine 22 (2): 75-77,1988
de Loes M, Goldi K. Incidence rate of injuries during sport activity and physical exercise in a rural Swedish municipality:incidence rates in 17 sports. International Journal of SportsMedicine 9: 461-467, 1988
van Dijk FJH, van Dormolen M, Kompier MAJ, Meijman TF.Herwaardering model belasting-belastbaarheid 68: 3-10, 1990
Dolmans I, Pool J, Erdman-Trip JF, Smit B. Plotse dood bij sport.Geneeskunde en S~rt 18: 95-99, 1985
Easterbrook M. Eye mjuries in squash and racquetball players:an update. Physician and Sports Medicine 10 (3): 47-56, 1982
Sports Injury Research Terminology
are answered are all aetiological factors taken intoconsideration and effective prevention is possible.
Despite the importance of the model of choicein studying the risk factors of sports injuries, thechoice of research design is also important. Caseseries usually give no information on the underlying population at risk, so they are of no value indrawing valid conclusions on the risk factors of injuries. Only by relating the injuries to corresponding population denominators one can estimate injury rates and identify important risk factors andhigh risk sportspersons (Walter et al. 1985). As inresearch on sports injury incidence, research on riskfactors should be undertaken on groups homogeneous with regard to age, sex, level of competitionand type of sport (Bol et al. 1991).
4.1 Sport-Specificity of Sports Injuries
Many sports injuries are highly sports specificwhich is in accordance with the various aetiological models. The locations and types of injuriesfound in the studies ofparticular sports clearly showthat the type of sport determines both in manycases. Different injuries occur in wrestling (Snook1980, 1982) than in soccer (Ekstrand 1982; Kristiansen 1983; Maehlum 1984; ), running (Jacobs etal. 1986; Koplan et al. 1982; Macera et al. 1989;Marti et al. 1988; Walter et al. 1989), squash (Easterbrook 1982; Pforringer & Keyl 1978) or tennis(Kulund et al. 1979). Nomenclature such as 'tenniselbow', 'golfer's elbow' and 'jumper's knee' suggestthat particular injuries are sport-specific (Travers1980), and consequently that precautions againstinjuries should be sport-specific. On the other hand,sports where similar injuries occur could be groupedtogether, and similar measures could be taken forthese groups.
5. Conclusions
Incidence and severity provide a yardstick forthe first step of prevention of sports injuries. However, in order to get reliable and comparable data,uniform definitions and adequate research designsand methodology are needed. Various internal and
97
external risk factors for sports injuries have to beidentified. It should be kept in mind, however, thatsports injuries may have several causes, includingthe behaviour of the sportsperson, and that manyinjuries evolve over time. Conceptual models ofthe aetiology of sports injuries should therefore takebehaviour into account and should be time-based.The stress-strain-capacity model as presented is anexample of such a model.
Acknowledgement
This study was partly supported with a research grantof the Dutch Ministry of Welfare, Health and CulturalAffairs as a contribution to the Council of Europe research project 'Sport for All: Sports Injuries and TheirPrevention'.
References
Backous DD, Friedl KE, Smith NJ, Parr TJ, Csarpine Jr WD.Soccer injuries and their relation to physical maturity. American Journal of Diseases of Children 142 (8): 839-842,1988
Backx FJG, Inklaar H, Koornneef M, van Mechelen W. DraftFIMS position statement on the prevention of sports injuries.Geneeskunde en Sport, Special Issue, May, 1990
Backx FJG. Sports injuries in youth, etiology and prevention.Thesis, University of Utrecht, 1991
Murphy P, van Beek PA. Letsel bij volleybal. Geneeskunde enSport 16: 59-65, 1983
Boersma-Slutter, W, Brookman A, Lagra HM, Minderaa PH. Sport,een riskante zaak. Geneeskunde en Sport 12; 41-49, 1979
Bol E, Schmickli SL, Backx FJG, van Mechelen W. Sportblessures onder de knie, Nationaal Instituut voor SportGezonheidsZorg publication 38, Papendal, The Netherlands,1991
Bolhuis JHA. Tandletsel in de hockeysport. Thesis, University ofUtrecht, 1987
Brandt Cortstius JJ. Het voorkomen van sportblessures - prevoentie is meer dan vaststellen van incidentie. Masters thesis,Inter Faculteit der Lichamelijke Opvooding, Amsterdam, 1983
Caine D, Cockrane B, Cain C, Zemper E. An epidemiologic investigation of injuiries affecting young competitive femalegymnasts. American Journal of Sports Medicine 17: 811-820,1989
Chambers RB. Orthopedic injuries in athletes (ages 6 to 17): comparison of injuries occumng in six sports. American Journalof Sports Medicine 7: 195-197, 1979
Clement DB, Taunton JE. A guide to the prevention of runninginjuries. Australian Family Physician 10: 156-174, 1981
Crossman J. Psychosocial factors and athletic injury. Journal ofSports Medicine 25: 151-154, 1985
Davies JE. Sports injuries and society. British Journal of SportsMedicine 15: 80-83, 1981
Davison J, Ryan MP. A Sports Medicine clinic in the community. British Journal of Sports Medicine 22 (2): 75-77,1988
de Loes M, Goldi K. Incidence rate of injuries during sport activity and physical exercise in a rural Swedish municipality:incidence rates in 17 sports. International Journal of SportsMedicine 9: 461-467, 1988
van Dijk FJH, van Dormolen M, Kompier MAJ, Meijman TF.Herwaardering model belasting-belastbaarheid 68: 3-10, 1990
Dolmans I, Pool J, Erdman-Trip JF, Smit B. Plotse dood bij sport.Geneeskunde en S~rt 18: 95-99, 1985
Easterbrook M. Eye mjuries in squash and racquetball players:an update. Physician and Sports Medicine 10 (3): 47-56, 1982

98
Edixhoven P, Sinha SC, Dandy J. Horse injuries. Injury 12 (4):279-282, 1980
Ekstrand J. Soccer injuries and their prevention. Linkoping University Medical Dissertations no. 130, Linkoping, 1982
Ekstrand J, Nigg BM. Surface-related injuries in soccer. SportsMedicine 8: 56-62, 1989
van Enst GC. Gezondheid en physical fitness. Medisch Contact40: 1288-1290, 1982
Eriksson EKG. Sports accidents. Presented at Symposium on Accidents in Europe; Newcastie-upon-Tyne, September, 1983
Ettema JH. Het model belasting en belast baanheid. Tijdschriftvoor Sociale Geneeskunde 51: 44-54, 1973
Fintelman LFJ, Rijks GS, Hildebrandt VH. Sportblessures bij ervaren competiue-basketballers (English summary), TNO Institute for Preventive Health Care, Leiden, 1989
Franke A, Franke K. Epidemiolo~e von Unfallen und Fehlbelandungsfolgen beim Sport. MedlZin und Sport 6: 184-189, 1980
van Galen W, Diederisk J. Sportblessures breed uitgemeten, Uitg.De Vrieseborch, Haarlem, 1990
Garrick JG, Requa RK. Role of external support in the prevention of ankle sprain. Medicine and Science in Sports 5: 200203, 1973
van Geffen Y, Bach FJG, van Mechelen W, Beijer HJM. Zaalkorfbalblessures bij 30-plussers: analyse van blessures en toepassing van preventieve maatregelen. Geneeskunde en Sport23 (4): 137-145, 1990
Groh H, Groh P. Sportverletzungen und Sportschaken, LeutpoldWerk, Munich, 1975
Guyer B, Ellers B,. Childhood injuries in the United States: mortality, morbidity and cost. American Journal of Diseases inChildhood 144: 649-652, 1990
Hensley LD, Paup DC. A survey of badminton injuries. BritishJournal of Sports Medicine 13: 156-160, 1979
Hitchcock ER, Karmi MZ. Sports injuries to the central nervoussystem. Journal of the Royal College ofSurgeons of Edinburgh27 (I): 46-49, 1982
Horner C, McCabe MJ. Ice-skating and roller disco injuries inDublin. British Journal of Sports Medicine 18: 207-211,1984
Hunter LY, Torgan C. Dismounts in gymnastics: should scordingbe reevaluated? American Journal of Sports Medicine II: 208210, 1983
Hutson M. Community health, exercise and injury risk. NursingTimes August: 22-25, 1983
Inklaar H. De epidemiologie van sportletsels; Publicatie NationalInstituut voor SportGezonheidsZorg no. 16, 1985
Jacobs 51, Berson BL. Injuries to runners: a study of entrants toa 10 000 meter race. American Journal of Sports Medicine 14(2): 151-155, 1986
Jaflin B. An epidemiologic study of ski injuries: Vail, Colorado;Mount Sinai. Journal of Medicine 48: 353-359, 1981
Janda DH, Wojtys EM, Hankin FM, Benedict ME, HensingerRN. A three-phase analysis of the prevention of recreationalsoftball injuries. American Journal of Sports Medicine 18: 632635, 1990
Janka C. Daxecker F. Augenverletzungen durch Wintersport.Fortschritte der Ophtalmologie 81: 71-72, 1984
Jost 0, von Ruland 0, Heger RA. Rollschuhfahrersdverletzungen; Deutsche Zeitschrift fiir Sportsmedizin 10: 268-274, 1981
Jorgensen U. The incidence and prevalence of injuries in badminton. In Proceedings of the Council of Europe 2nd meeting1987, National Institute for Sports Health Care, Oosterbeek,1988
Jiingst BK, Keth RK, Stopfkuchen H, Schranz D. Verletzungenim Handballsport, Ergebnisse einer Befragung, MiinchenerMedizinische Wochenschrift 125: 531-533, 1983
Kelly Jr MJ. Psychological risk factors and sports injuries. Journal of Sports Medicine and Physical Fitness 30: 1990
Kennedy MC, Vanderfield GK, Kennedy JR. Sport: assessing therisk. Medical Journal of Australia 2: 253-254, 1977
Kent F. Athletes wait too long to report injuries. Physician andSportsmedicine 10 (4): 127-129, 1982
Kersey RD, Rowan L. Injury account during the 1980 NCAAwrestling championships. American Journal ofSportsmedicineII: 147-151 1983
KIesges RC, Eck LH, Mellon MW, Fulliton W, Somes GW, et al.The accuracy of self-reports of physical activity. Medicine andScience in Sport and Exercise 22 (5): 690-697, 1990
Kok G, Bouter LM. On the importance of planned health edu-
Sports Medicine 14 (2) 1992
cation: prevention of ski injury as an example. American Journal of Sports Medicine 18 (6): 600-605, 1990
Koplan JP. Cardiovascular death while running. Journal of theAmerican Medical Association 242: 2578-2579, 1979
Koplan JP, Powell KE, Sikes RK, Shirley RW, Campbell Gc. Anepidemiological study of the benefits and risks of running.Journal of the American Medical Association 248 (32): 31183121, 1982
Kowal DM. Nature and causes of injuries in women resultingfrom an endurance training program. American Journal ofSports Medicine 8: 265-269, 1980
Krahl H, Steinbruck K. Traumatologie des Sports. In Cotta H(Ed.) Belastungs-toleranz des Bewegungsapparates, Gerg ThieneVerlag, Stuttgart, 1980
Kranenborg N. Blessures bij micro-korfballers. Geneeskunde enSport 14: 36-40, 1981
Kranenborg N. Sportbeoefening en blessures. Geneeskunde enSport 13: 89-93, 1980
Kranenborg N. Sportbeoefening en blessures. Tijdschrift voor Sociale Geneeskunde . 60, 9: 224-227, 1982
Kristiansen B. Association football injuries in school boys. Scandinavian Journal of Sports Science 5: 102, 1983
Kulund DN, McCue FC, Rockwell DA, Gieck JH. Tennis injuries: prevention and treatment, a review. American Journal ofSports Medicine 7: 249-253, 1979
Kvidera D, Frankel VH. Trauma on eight wheels: a study ofrollerskating injuries in Seattle. American Journal of Sports Medicine II: 38-41, 1983
La Cava G. Environment, equipment and prevention of sport'sinjuries. Journal of Sports Medicine and Physical Fitness 18:1-2, 1978
Last JM. A dictionary of epidemiology 2nd ed. Oxford UniversityPress, New York, 1988
Lindenfield TN, Noyes ER, Marshall MT. Components of injuryreporting systems. American Journal of Sports Medicine 16(Suppl. I): 69-81, 1988
de Loes M. Medical treatment and costs of sports-related injuriesin a total population. International Journal of Sports MedicineII: 66-72, 1990
Lorentzen R. Causes of injuries: intrinsic factors. In Disix et al.(Eds) The Olympic book of sportsmedicine Vol. I, pp. 376390, Blackwell Scientific Publisher, Carlton, 1988
Lysens R, Lefevre J, Ostyn M. The predictability of sports injuries: a preliminary report. International Journal of SportsMedicine 5 (Suppl.): 153-155, 1984
Lysens R, Ostyn M. Prolegomena bij de preventie van sport letsels. Hermes 17: 85-94, 1984
Lysens RJJ, van de Auweele Y, Ostyn MS. The relationship between psychosocial factors and sports injuries. Journal ofSportsMedicine and Physical Fitness 26: 77-84, 1986
Lysholm J, Wiklander J. Injuries in runners. American Journalof Sports Medicine 15 (2): 168-171, 1987
Macera CA, Pate RR, Powell KE, Jackson KL, Kendrick JS, etal. Predicting lower-extremity injuries among habitual runners.Archives of Internal Medicine 149: 2565-2568, 1989
Maehlum S, Daljord OA. Acute sports injuries in Oslo: a oneyear study. British Journal of Sports Medicine 18: 181-185,1984
Maehlum S. Football injuries in Oslo: a one-year study. BritishJournal of Sports Medicine 18: 186-190, 1984
Manders T, Kropman J. Sportdeelname: wat weten wij er van?Institut voor Toegepaste Sociologie, Nijmegen, 1979
Marti B, Vader JP, Minder CE, Abelin T. On the epidemiologyof running injuries. American Journal of Sports Medicine 16(3): 285-294, 1988
Matter P, Spinas GA, Ott G. Risiko- und Schweregradentwicklung der aplinen Skiunfaelle und deren soziale Bedeutung. Sozial- und Praeventivmedizin 27: 19-22, 1982
McLatchie GR. Equestrian injuries, a one-year prospective study.British Journal of Sports Medicine 13: 29-32, 1979
Medved R, Pavisic V, Medved V. Causes of injuries during thepractical classes on physical education in schools. Journal ofSports Medicine 13: 32-41, 1973
Menke W, Muller EK. Sicherheitsskibindung. Miinchener Medizinische Wochenschrift 8: 183-184, 1982
Miles S. Fit, for anything? British Journal of Sports Medicine 12:173-175, 1977
Mueller Fa, Blyth CS. North Carolina high school football injury
98
Edixhoven P, Sinha SC, Dandy J. Horse injuries. Injury 12 (4):279-282, 1980
Ekstrand J. Soccer injuries and their prevention. Linkoping University Medical Dissertations no. 130, Linkoping, 1982
Ekstrand J, Nigg BM. Surface-related injuries in soccer. SportsMedicine 8: 56-62, 1989
van Enst GC. Gezondheid en physical fitness. Medisch Contact40: 1288-1290, 1982
Eriksson EKG. Sports accidents. Presented at Symposium on Accidents in Europe; Newcastie-upon-Tyne, September, 1983
Ettema JH. Het model belasting en belast baanheid. Tijdschriftvoor Sociale Geneeskunde 51: 44-54, 1973
Fintelman LFJ, Rijks GS, Hildebrandt VH. Sportblessures bij ervaren competiue-basketballers (English summary), TNO Institute for Preventive Health Care, Leiden, 1989
Franke A, Franke K. Epidemiolo~e von Unfallen und Fehlbelandungsfolgen beim Sport. MedlZin und Sport 6: 184-189, 1980
van Galen W, Diederisk J. Sportblessures breed uitgemeten, Uitg.De Vrieseborch, Haarlem, 1990
Garrick JG, Requa RK. Role of external support in the prevention of ankle sprain. Medicine and Science in Sports 5: 200203, 1973
van Geffen Y, Bach FJG, van Mechelen W, Beijer HJM. Zaalkorfbalblessures bij 30-plussers: analyse van blessures en toepassing van preventieve maatregelen. Geneeskunde en Sport23 (4): 137-145, 1990
Groh H, Groh P. Sportverletzungen und Sportschaken, LeutpoldWerk, Munich, 1975
Guyer B, Ellers B,. Childhood injuries in the United States: mortality, morbidity and cost. American Journal of Diseases inChildhood 144: 649-652, 1990
Hensley LD, Paup DC. A survey of badminton injuries. BritishJournal of Sports Medicine 13: 156-160, 1979
Hitchcock ER, Karmi MZ. Sports injuries to the central nervoussystem. Journal of the Royal College ofSurgeons of Edinburgh27 (I): 46-49, 1982
Horner C, McCabe MJ. Ice-skating and roller disco injuries inDublin. British Journal of Sports Medicine 18: 207-211,1984
Hunter LY, Torgan C. Dismounts in gymnastics: should scordingbe reevaluated? American Journal of Sports Medicine II: 208210, 1983
Hutson M. Community health, exercise and injury risk. NursingTimes August: 22-25, 1983
Inklaar H. De epidemiologie van sportletsels; Publicatie NationalInstituut voor SportGezonheidsZorg no. 16, 1985
Jacobs 51, Berson BL. Injuries to runners: a study of entrants toa 10 000 meter race. American Journal of Sports Medicine 14(2): 151-155, 1986
Jaflin B. An epidemiologic study of ski injuries: Vail, Colorado;Mount Sinai. Journal of Medicine 48: 353-359, 1981
Janda DH, Wojtys EM, Hankin FM, Benedict ME, HensingerRN. A three-phase analysis of the prevention of recreationalsoftball injuries. American Journal of Sports Medicine 18: 632635, 1990
Janka C. Daxecker F. Augenverletzungen durch Wintersport.Fortschritte der Ophtalmologie 81: 71-72, 1984
Jost 0, von Ruland 0, Heger RA. Rollschuhfahrersdverletzungen; Deutsche Zeitschrift fiir Sportsmedizin 10: 268-274, 1981
Jorgensen U. The incidence and prevalence of injuries in badminton. In Proceedings of the Council of Europe 2nd meeting1987, National Institute for Sports Health Care, Oosterbeek,1988
Jiingst BK, Keth RK, Stopfkuchen H, Schranz D. Verletzungenim Handballsport, Ergebnisse einer Befragung, MiinchenerMedizinische Wochenschrift 125: 531-533, 1983
Kelly Jr MJ. Psychological risk factors and sports injuries. Journal of Sports Medicine and Physical Fitness 30: 1990
Kennedy MC, Vanderfield GK, Kennedy JR. Sport: assessing therisk. Medical Journal of Australia 2: 253-254, 1977
Kent F. Athletes wait too long to report injuries. Physician andSportsmedicine 10 (4): 127-129, 1982
Kersey RD, Rowan L. Injury account during the 1980 NCAAwrestling championships. American Journal ofSportsmedicineII: 147-151 1983
KIesges RC, Eck LH, Mellon MW, Fulliton W, Somes GW, et al.The accuracy of self-reports of physical activity. Medicine andScience in Sport and Exercise 22 (5): 690-697, 1990
Kok G, Bouter LM. On the importance of planned health edu-
Sports Medicine 14 (2) 1992
cation: prevention of ski injury as an example. American Journal of Sports Medicine 18 (6): 600-605, 1990
Koplan JP. Cardiovascular death while running. Journal of theAmerican Medical Association 242: 2578-2579, 1979
Koplan JP, Powell KE, Sikes RK, Shirley RW, Campbell Gc. Anepidemiological study of the benefits and risks of running.Journal of the American Medical Association 248 (32): 31183121, 1982
Kowal DM. Nature and causes of injuries in women resultingfrom an endurance training program. American Journal ofSports Medicine 8: 265-269, 1980
Krahl H, Steinbruck K. Traumatologie des Sports. In Cotta H(Ed.) Belastungs-toleranz des Bewegungsapparates, Gerg ThieneVerlag, Stuttgart, 1980
Kranenborg N. Blessures bij micro-korfballers. Geneeskunde enSport 14: 36-40, 1981
Kranenborg N. Sportbeoefening en blessures. Geneeskunde enSport 13: 89-93, 1980
Kranenborg N. Sportbeoefening en blessures. Tijdschrift voor Sociale Geneeskunde . 60, 9: 224-227, 1982
Kristiansen B. Association football injuries in school boys. Scandinavian Journal of Sports Science 5: 102, 1983
Kulund DN, McCue FC, Rockwell DA, Gieck JH. Tennis injuries: prevention and treatment, a review. American Journal ofSports Medicine 7: 249-253, 1979
Kvidera D, Frankel VH. Trauma on eight wheels: a study ofrollerskating injuries in Seattle. American Journal of Sports Medicine II: 38-41, 1983
La Cava G. Environment, equipment and prevention of sport'sinjuries. Journal of Sports Medicine and Physical Fitness 18:1-2, 1978
Last JM. A dictionary of epidemiology 2nd ed. Oxford UniversityPress, New York, 1988
Lindenfield TN, Noyes ER, Marshall MT. Components of injuryreporting systems. American Journal of Sports Medicine 16(Suppl. I): 69-81, 1988
de Loes M. Medical treatment and costs of sports-related injuriesin a total population. International Journal of Sports MedicineII: 66-72, 1990
Lorentzen R. Causes of injuries: intrinsic factors. In Disix et al.(Eds) The Olympic book of sportsmedicine Vol. I, pp. 376390, Blackwell Scientific Publisher, Carlton, 1988
Lysens R, Lefevre J, Ostyn M. The predictability of sports injuries: a preliminary report. International Journal of SportsMedicine 5 (Suppl.): 153-155, 1984
Lysens R, Ostyn M. Prolegomena bij de preventie van sport letsels. Hermes 17: 85-94, 1984
Lysens RJJ, van de Auweele Y, Ostyn MS. The relationship between psychosocial factors and sports injuries. Journal ofSportsMedicine and Physical Fitness 26: 77-84, 1986
Lysholm J, Wiklander J. Injuries in runners. American Journalof Sports Medicine 15 (2): 168-171, 1987
Macera CA, Pate RR, Powell KE, Jackson KL, Kendrick JS, etal. Predicting lower-extremity injuries among habitual runners.Archives of Internal Medicine 149: 2565-2568, 1989
Maehlum S, Daljord OA. Acute sports injuries in Oslo: a oneyear study. British Journal of Sports Medicine 18: 181-185,1984
Maehlum S. Football injuries in Oslo: a one-year study. BritishJournal of Sports Medicine 18: 186-190, 1984
Manders T, Kropman J. Sportdeelname: wat weten wij er van?Institut voor Toegepaste Sociologie, Nijmegen, 1979
Marti B, Vader JP, Minder CE, Abelin T. On the epidemiologyof running injuries. American Journal of Sports Medicine 16(3): 285-294, 1988
Matter P, Spinas GA, Ott G. Risiko- und Schweregradentwicklung der aplinen Skiunfaelle und deren soziale Bedeutung. Sozial- und Praeventivmedizin 27: 19-22, 1982
McLatchie GR. Equestrian injuries, a one-year prospective study.British Journal of Sports Medicine 13: 29-32, 1979
Medved R, Pavisic V, Medved V. Causes of injuries during thepractical classes on physical education in schools. Journal ofSports Medicine 13: 32-41, 1973
Menke W, Muller EK. Sicherheitsskibindung. Miinchener Medizinische Wochenschrift 8: 183-184, 1982
Miles S. Fit, for anything? British Journal of Sports Medicine 12:173-175, 1977
Mueller Fa, Blyth CS. North Carolina high school football injury

Sports Injury Research Terminology
study: equipment and prevention. Journal of Sports Medicine2: 1-10. 1974
Oh S, Schmid UD. Kindliche Kopfverletzungen beim Shifahrenund ihre optimale Prophylaxe. Zeitschrift fUr Kinderchirurgie30: 66-72, 1983
Orava S, Jaroma H, Hulkko A. Overuse injuries in cross-countryskiing. British Journal of Sports Medicine 19 (3): 158-160, 1985
Penschuck C. Verletzungsursachten beim Drachenfliegen. DerChirurgie 51: 336-340, 1980
Peterson L, Renstrom P. Sports injuries, their prevention andtreatment. Martin Dunitz Ltd, London, 1986
Pettrone FA, Riccardelli E. Gymnastic injuries: the VilJinia experience 1982-1983. American Journal ofSports MedIcine 15:59-62, 1987
Pforringer W, Keyl W. Sportverletzungen beim Squash, Eidemiologie und Prevention. Miinchener Medizinische Wochenschrift 120: 1163-1166, 1978
Pritchett JW. High cost of high school football injuries. AmericanJournal of Sports Medicine 8 (3): 197-199, 1980
van Rens TJG. Sport en gezondheid, orthopaedische aspecten.Medisch Contact 40: 1283-1288, 1982
Rogmans WHJ, Weerman A. Registratie van ongevalspatientenop de eerste hulpafdeling; Stichting Consument en Veiligheid,1982
Rozendal RH, Bakker CJ, Lamur K. Risikofactoren bij recreatiesport. Sportcahiers 12, Nederlands Katholeike Sportfederatie,1979
Sandelin J, Santavirta S, Lattilii R, Sarna S. Sports injuries in alarge urban population: occurrence and epidemiological aspects. International Journal of Sports Medicine 8: 61-66, 1987
Schlatmann HFPM, Hlobil H, van Mechelen W, Kemper HCG.Naar een Registratiesysteem van Sportblessures in Nederland,National Institut voor SportGezondheidZorg, Oosterbeek,Netherlands, 1986
Sedlin ED, Zitner DT, McGinnis G. Roller skating accidents andinjuries. Journal of Trauma 24: 136-139, 1984
Segesser B. Aetiologie von Reversiblen und Irreversiblen Sportschaden. Schweizerische Zeitschrift fiir Sportmedizin 31: 8186, 1983
Shephard RJ. Current perspectives on the economics of fitnessand sport with particular reference to worksite programmes.Sports Medicine 7: 286-309, 1989
Shephard RJ. The impact of exercise upon medical costs. SportsMedicine 2: 133-143, 1985
Shively RA, Grana WA. High school sports injuries. Physicianand Sportsmedicine 9: 46-50, 1981
Smith AM, Scott SG, Wiese DM. The psychological effects ofsports injuries: coping. Sports Medicine 9 (6): 352-369, 1990
Snook GA. A survey of wrestling injuries. American Journal ofSports Medicine 8: 450-453, 1980
Snook GA. Injuries in intercollegiate wrestling. American Journalof Sports Medicine 10: 142-144, 1982
Sorensen CH, Sonne-Holm S. Social costs of sports injuries. British Journal of Sports Medicine 14: 24-25, 1980
Stanitski CL. Common injuries in preadolescent and adolescentchildren. Recommendations for intervention. Sports Medicine7: 32-41, 1989
Steinberg PJ. Injuries to Dutch sport parachutists. British Journalof Sports Medicine 22 (I): 25-30, 1988
Stichting Consumet and Veiligheid. Jaaroverzicht 1984. Prive ongevallen en registratie systeem. PORS - Ongevallen 84; Uitgave Stichtinl! Consument en Veiligheid, 1985
Sturmans F. Epldemiologie, Dekker & van de Vegt, Nijmegen1984
99
Taerk GS. The injury-prone athlete: a psychological approach.Journal of Sports Medicine 17: 187-194, 1977
Tolpin HG, Yinger PF, Tolpin DW. Economic considerations.International Ophthalmology Clinics 21: 179-201, 1981
den Toom PJ, Schuurman MIM. Een model voor berekeningvankosten van ongevallen in de prive-sfeer. Stichting Consument en Veiligheid 40, 1988
To~ JS, Truex TG, Quendenfeld TG, Burstein A, et al. The natIOnal football head and neck injury registration: report andconclusions 1978. Journal of the American Medical Association 241: 1477-1479, 1979
Travers PRo Sports injuries. Physiotherapy 66: 215-216, 1980Tsongas PE. The role of government in injury prevention. Inter
national Ophthalmology Clinics 21: 171-177, 1981van Mechelen W, Hlobil H, Kemper HCG. How can sports in
juries be prevented? Nationaal Instituut voor SportGezondheidsZorg publicatie nr 25E, Papendal, 1987
van Mechelen W. 25 jaar schade door sport. Geneeskunde enSport 23: 196-198, 1991
van Puffelen F, Reyman JON, Vellhuysen JW. Sport en gezondheid, economisch beziem, SEO, Amsterdam, 1989
van Vulpen AV. Sport for all: sports injuries and their prevention.Council of Europe, National Institut voor SportGezondheidsZorg, Oosterbeek, 1989
Veerbeek ALM, Postma MA, Bach FJG. De epidemiologie vansportblessures bi) de schoolgaande jeugd. National Instituut voorSportGezondheldsZorg Osterberbeek, 1984
Vermeer JP. Sport en sociale verzekering. Tijdschrift Sociale Geneeskunde 60: 222-223, 1982
Yinger PF. Eye and face protection for United States hockey players: a chronology. International Ophthalmology Clinic 21: 8386, 1981
Yinger PF. Principles of protection. International OphthalmologyClinics 21: 149-161, 1981
Von Schiirmeyer T, Hiddig J, Herter T. Die Bedeutung des Schaedel-Him-Traumas im Sport. Deutsche Zeitschrift fiir Sportmedizin 3: 86-89, 1983
von Steinbriick K. Wirbelsaulen veilelzungen beim Reiden. TeilI. Unfallheilkunde 83: 366-372, 1980
Wallace RB. Application of epidemiologic principles to sports injury research. American Journal ofSports Medicine 16 (Suppl.I): 22-25, 1988
Walter SD, Sutton JR, McIntosh JM, Connolly C. The aetiologyof sports injuries: a review of methodologies. Sports Medicine2: 47-58, 1985
Walter SD, Hart LE, McIntosh JM, Sutton JR. The Ontario cohort study of running - related injuries. Archives of InternalMedicine 149: 2561-2564, 1989
Williams JPG. Sports injuries - the case for specialised clinics inthe United Kingdom. British Journal of Sports Medicine 9:22-24, 1975
Zemper ED, NCAA injury surveillance system: initial results.Presented at Olympic Scientific Congress, Los Angeles, 1984
Correspondence and reprints: Willem van Mechelen. Departmentof Health Science, Faculty of Human Movement Sciences, VrijeUniversiteit en University of Amsterdam, Meibergdreef 15, 1105AZ Amsterdam, The Netherlands.
Sports Injury Research Terminology
study: equipment and prevention. Journal of Sports Medicine2: 1-10. 1974
Oh S, Schmid UD. Kindliche Kopfverletzungen beim Shifahrenund ihre optimale Prophylaxe. Zeitschrift fUr Kinderchirurgie30: 66-72, 1983
Orava S, Jaroma H, Hulkko A. Overuse injuries in cross-countryskiing. British Journal of Sports Medicine 19 (3): 158-160, 1985
Penschuck C. Verletzungsursachten beim Drachenfliegen. DerChirurgie 51: 336-340, 1980
Peterson L, Renstrom P. Sports injuries, their prevention andtreatment. Martin Dunitz Ltd, London, 1986
Pettrone FA, Riccardelli E. Gymnastic injuries: the VilJinia experience 1982-1983. American Journal ofSports MedIcine 15:59-62, 1987
Pforringer W, Keyl W. Sportverletzungen beim Squash, Eidemiologie und Prevention. Miinchener Medizinische Wochenschrift 120: 1163-1166, 1978
Pritchett JW. High cost of high school football injuries. AmericanJournal of Sports Medicine 8 (3): 197-199, 1980
van Rens TJG. Sport en gezondheid, orthopaedische aspecten.Medisch Contact 40: 1283-1288, 1982
Rogmans WHJ, Weerman A. Registratie van ongevalspatientenop de eerste hulpafdeling; Stichting Consument en Veiligheid,1982
Rozendal RH, Bakker CJ, Lamur K. Risikofactoren bij recreatiesport. Sportcahiers 12, Nederlands Katholeike Sportfederatie,1979
Sandelin J, Santavirta S, Lattilii R, Sarna S. Sports injuries in alarge urban population: occurrence and epidemiological aspects. International Journal of Sports Medicine 8: 61-66, 1987
Schlatmann HFPM, Hlobil H, van Mechelen W, Kemper HCG.Naar een Registratiesysteem van Sportblessures in Nederland,National Institut voor SportGezondheidZorg, Oosterbeek,Netherlands, 1986
Sedlin ED, Zitner DT, McGinnis G. Roller skating accidents andinjuries. Journal of Trauma 24: 136-139, 1984
Segesser B. Aetiologie von Reversiblen und Irreversiblen Sportschaden. Schweizerische Zeitschrift fiir Sportmedizin 31: 8186, 1983
Shephard RJ. Current perspectives on the economics of fitnessand sport with particular reference to worksite programmes.Sports Medicine 7: 286-309, 1989
Shephard RJ. The impact of exercise upon medical costs. SportsMedicine 2: 133-143, 1985
Shively RA, Grana WA. High school sports injuries. Physicianand Sportsmedicine 9: 46-50, 1981
Smith AM, Scott SG, Wiese DM. The psychological effects ofsports injuries: coping. Sports Medicine 9 (6): 352-369, 1990
Snook GA. A survey of wrestling injuries. American Journal ofSports Medicine 8: 450-453, 1980
Snook GA. Injuries in intercollegiate wrestling. American Journalof Sports Medicine 10: 142-144, 1982
Sorensen CH, Sonne-Holm S. Social costs of sports injuries. British Journal of Sports Medicine 14: 24-25, 1980
Stanitski CL. Common injuries in preadolescent and adolescentchildren. Recommendations for intervention. Sports Medicine7: 32-41, 1989
Steinberg PJ. Injuries to Dutch sport parachutists. British Journalof Sports Medicine 22 (I): 25-30, 1988
Stichting Consumet and Veiligheid. Jaaroverzicht 1984. Prive ongevallen en registratie systeem. PORS - Ongevallen 84; Uitgave Stichtinl! Consument en Veiligheid, 1985
Sturmans F. Epldemiologie, Dekker & van de Vegt, Nijmegen1984
99
Taerk GS. The injury-prone athlete: a psychological approach.Journal of Sports Medicine 17: 187-194, 1977
Tolpin HG, Yinger PF, Tolpin DW. Economic considerations.International Ophthalmology Clinics 21: 179-201, 1981
den Toom PJ, Schuurman MIM. Een model voor berekeningvankosten van ongevallen in de prive-sfeer. Stichting Consument en Veiligheid 40, 1988
To~ JS, Truex TG, Quendenfeld TG, Burstein A, et al. The natIOnal football head and neck injury registration: report andconclusions 1978. Journal of the American Medical Association 241: 1477-1479, 1979
Travers PRo Sports injuries. Physiotherapy 66: 215-216, 1980Tsongas PE. The role of government in injury prevention. Inter
national Ophthalmology Clinics 21: 171-177, 1981van Mechelen W, Hlobil H, Kemper HCG. How can sports in
juries be prevented? Nationaal Instituut voor SportGezondheidsZorg publicatie nr 25E, Papendal, 1987
van Mechelen W. 25 jaar schade door sport. Geneeskunde enSport 23: 196-198, 1991
van Puffelen F, Reyman JON, Vellhuysen JW. Sport en gezondheid, economisch beziem, SEO, Amsterdam, 1989
van Vulpen AV. Sport for all: sports injuries and their prevention.Council of Europe, National Institut voor SportGezondheidsZorg, Oosterbeek, 1989
Veerbeek ALM, Postma MA, Bach FJG. De epidemiologie vansportblessures bi) de schoolgaande jeugd. National Instituut voorSportGezondheldsZorg Osterberbeek, 1984
Vermeer JP. Sport en sociale verzekering. Tijdschrift Sociale Geneeskunde 60: 222-223, 1982
Yinger PF. Eye and face protection for United States hockey players: a chronology. International Ophthalmology Clinic 21: 8386, 1981
Yinger PF. Principles of protection. International OphthalmologyClinics 21: 149-161, 1981
Von Schiirmeyer T, Hiddig J, Herter T. Die Bedeutung des Schaedel-Him-Traumas im Sport. Deutsche Zeitschrift fiir Sportmedizin 3: 86-89, 1983
von Steinbriick K. Wirbelsaulen veilelzungen beim Reiden. TeilI. Unfallheilkunde 83: 366-372, 1980
Wallace RB. Application of epidemiologic principles to sports injury research. American Journal ofSports Medicine 16 (Suppl.I): 22-25, 1988
Walter SD, Sutton JR, McIntosh JM, Connolly C. The aetiologyof sports injuries: a review of methodologies. Sports Medicine2: 47-58, 1985
Walter SD, Hart LE, McIntosh JM, Sutton JR. The Ontario cohort study of running - related injuries. Archives of InternalMedicine 149: 2561-2564, 1989
Williams JPG. Sports injuries - the case for specialised clinics inthe United Kingdom. British Journal of Sports Medicine 9:22-24, 1975
Zemper ED, NCAA injury surveillance system: initial results.Presented at Olympic Scientific Congress, Los Angeles, 1984
Correspondence and reprints: Willem van Mechelen. Departmentof Health Science, Faculty of Human Movement Sciences, VrijeUniversiteit en University of Amsterdam, Meibergdreef 15, 1105AZ Amsterdam, The Netherlands.





























