Embed Size (px)
DESCRIPTION
incertitudinea de masurare
Citation preview

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
COURSE NOTESA model for calculating measurement uncertainty in
medical laboratories
Model pentru calcularea incertitudinii de măsurare în laboratoarele medicale
Irina L. Dumitriu1, Bogdan Gurzu1, Simona M. Slǎtineanu1, Liliana Foia2, Traian Mutiu3, Corina Şchiriac4, Mioara Achirecesei4, Maria Enea4
1. Department of Functional Sciences, Faculty of Medicine, “Gr. T. Popa” University of Medicine andPharmacy, Iasi
2. Department of Semiology and Prevention, Faculty of Dental Medicine, “Gr. T. Popa” University ofMedicine and Pharmacy, Iasi
3. “Politehnica” University of Timisoara4. Medical Investigations PRAXIS Iaşi.
Abstract
Introduction: All medical laboratories that require recognition for competency assessment have to es-timate the uncertainty of measurement of assay test results “where relevant and possible” (ISO 15189:2007Medical laboratories - Particular requirements for quality and competence). The repeated quantitative examina-tion of an analyte with the same method will offer more or less different results. This is happening because theoutcome of an assay depends not only upon the analyte itself, but also upon few error factors that could yielddoubts about the obtained result. The mathematical, quantitative expression of this doubt is known as uncertaintyof measurement (UM). Methods: It is the responsibility of each medical laboratory to identify all error sourcesthat can be quantified and converted in standard deviations that could be used to estimate the type A or B of un-certainty. In the case of Romanian medical laboratories, the European Accreditation (EA) accepted as referencedocuments for UM estimation the Guide to the Expression of Uncertainty in Measurement (GUM) and RomanianStandard SR ENV 13005. Discussion and conclusion: In this paper, authors present and discuss the modalitiesof UM estimation in two different situations: when the used reference materials (calibrators) are or are nottraceable to certified reference materials (CRM). Complete and informative UM reporting can only lead to betterdecisions in healthcare.
Keywords: precision, accuracy, uncertainty of measurement, calibrator.
Rezumat
Introducere. Toate laboratoarele medicale care doresc recunoaştere de competenţă trebuie să-şi esti-meze incertitudinea de măsurare acolo unde este “relevant şi posibil” (SR EN ISO 15189, Standard Român, La-boratoare medicale, Cerinţe particulare pentru calitate şi competenţă, 2007). În cazul unor măsurari repetateale unui analit obţinem rezultate diferite, mai mult sau mai puţin apropiate între ele, deşi valoarea analitului
65

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
este aceeaşi. Valoarea unui rezultat măsurat nu depinde numai de valoarea însăşi, ci şi de o serie de factori deeroare, care aduc o neîncredere, un dubiu asupra rezultatului obţinut. Exprimarea matematică, cantitativă aacestei neîncrederi se numeşte incertitudine de măsurare (UM). Material şi metodă. Este responsabilitatea fie-cărui laborator să-şi indentifice toate sursele de eroare care pot fi cuantificate şi convertite în deviaţii standardpe baza cărora să-şi estimeze UM de tip A şi de tip B. Pentru laboratoarele medicale din România, EuropeanAcreditation (EA) recunoaşte ca documente de bază pentru estimarea UM, Guide to the Expression of Uncer-tainty in Measurement (GUM) şi Standardul Român SR ENV 13005 (Ghid pentru exprimarea incertitudinii demăsurare). Discuţii şi concluzii. Autorii prezintă modalităţile de estimare a UM în laboratoarele medicale dinţara noastră când calibratorii utilizaţi sunt trasabili sau nu la materiale de referinţă certificate (MRC). Raporta-rea corectă şi completă a UM influenţează decizia terapeutică.
Cuvinte-cheie: precizie, acurateţe, incertitudine de măsurare, calibrator.
All medical laboratories that require re-cognition for competency assessment have to es-timate the uncertainty of measurement of assaytest results “where relevant and possible” (1).
The term “uncertainty” means a doubtand “uncertainty of measurement” (UM) is adoubt on the validity of outcome measurements.UM is only applicable to results of numericalquantitative measurement.
According to GUM “the result of ameasurement is only an approximation or estim-
ate of the value of the measurand and thus iscomplete only when accompanied by a state-ment of the uncertainty of that estimate” (2). In-deed, due to measurement uncertainty, a ‘truevalue’ of measurement can never be known.
There are several definitions of the UM:● “estimation of the range of values within which
the true value of a measurand lies” (2);● “parameter characterizing the dispersion of the
quantity values being attributed to a measur-and, based on the information used” (3).
From daily practice it is wellknown that when a measurement is re-peated n times we obtain n differentresults, although the analyte is thesame. This happens because the resultsof a measurement are depending notonly upon the analyte itself, but alsoupon a number of error factors thatcould yield doubts about the estimate.
It is important not to confusethe terms „error of measurement” and“uncertainty of measurement” (2, 3).An error of measurement is the differ-ence between the measured value andthe “true value” of the analyte beingmeasured. As such, the error is asingle value that can be applied as acorrection to the result. The UM is arange of values and this range cannotbe used to correct a measurement’sresult (4).
66
Figure 1. Precision and accuracy of measurements (modified afterMark Martinec http://www.ijs.si/time/).

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
The UM is the number after “±” signand it is expressed as “standard deviation (or agiven multiple of it), or the half-width of an in-terval having a stated level of confidence” (2).
Uncertainty of measurement comprises,in general, many components grouped in 2 types(A and B) derived from method for estimationof their numerical value (2, 5, 6).
Type A uncertainty is obtained by cal-culation from a series of repeated measure-ments, using statistical methods. Type A uncer-tainty comprises random errors which arisefrom random effects. Random errors cannot beeliminated but the uncertainty due to their effectmay be reduced by increasing the number ofmeasurements and applying statistical analysis.
Type B uncertainty appears by meansother than those used for a Type A evaluation.For example, by using data from outsidesources: calibration certificates, manufacturers’specifications, previous measurement data, ex-perience with the behavior of the instruments,intercomparison scheme and all other relevant
information. Type B uncertainty encompassessystematic errors.
Each component of uncertainty is rep-resented by an estimated standard deviationnamed standard uncertainty (Ui) equal to thepositive square root of the estimated variance.
The performance of quantitative testsfrom medical laboratory is attested by two com-ponents: precision and accuracy of measurements(Figure 1) (7). These two components should betaken into account for a reasonable estimation ofmeasurement uncertainty in medical laboratories.
Precision is characterized by the dis-persion of values obtained by repeated measure-ments of an analyte and it is expressed by stand-ard deviation (SD) and coefficient of variation(CV) (Figure 2).
Precision of measurements is evaluatedby type A uncertainty (8).
Type A uncertainty is based on a statist-ical analysis of n different values obtained fromrepeated measurements of an analyte using thesame method.
67
n
xX
n
xi∑
= =1
( )1n
1
2XXi
SD−
=−
=∑
n
i
100•=X
SDCV , where
X = average of measured valuesXi = individual measured valuesSD = standard deviation CV = coefficient of variation n = number of measurements
Figure 2. Precision of measurements on control serum. Results obtained by repeated measurements on a control material have a Gaussian distribution.
Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
The mean is determined by adding agroup of measured values, then dividing thetotal by the number of measurements in thegroup as equation [1]:
n
n
1i ix
n
nx...ix...2x1xX
∑==
+++++= [1],
where:
X = mean of the measured values,Xi = individual measurements,n = number of the values Xi in the group.
Then the standard deviation is determ-ined by equation [2].
This standard deviation (SD) representedby a statistically estimate (experimental standarddeviation) constitutes type A uncertainty.
There are many possibilities for assessingtype A uncertainty. Type A uncertainty is based onrepeated measurements of the same analyte over a
long period of time. For that reason,medical laboratories estimate type Ameasurement uncertainty by usingcontrol material (in which the analytesare stable for a long period of time).Control material is homologue to pa-tient sample. Control material is meas-ured by the same measurement sys-tem, with the same calibrator and re-agents as patient sample. Therefore, byextrapolation, the precision of meas-urements using the control material isidentical with the precision of meas-urements using patient sample inwhich the analytes have only short-term stability.
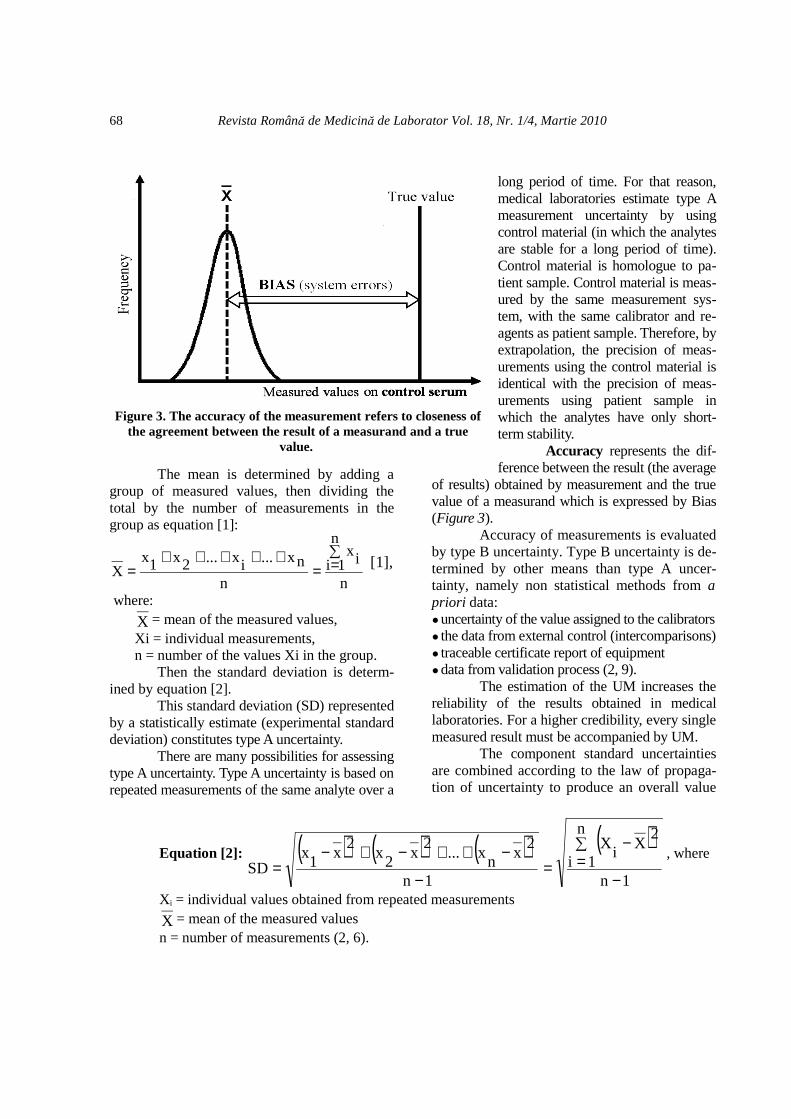
Accuracy represents the dif-ference between the result (the average
of results) obtained by measurement and the truevalue of a measurand which is expressed by Bias(Figure 3).
Accuracy of measurements is evaluatedby type B uncertainty. Type B uncertainty is de-termined by other means than type A uncer-tainty, namely non statistical methods from apriori data:●uncertainty of the value assigned to the calibrators● the data from external control (intercomparisons)● traceable certificate report of equipment ●data from validation process (2, 9).
The estimation of the UM increases thereliability of the results obtained in medicallaboratories. For a higher credibility, every singlemeasured result must be accompanied by UM.
The component standard uncertaintiesare combined according to the law of propaga-tion of uncertainty to produce an overall value
68
Equation [2]: ( ) ( ) ( ) ( )1n
n
1i
2X
iX
1n
2x
nx...
2x
2x
2x
1x
SD−
∑
=−
=−
−++−+−=
, where
X i = individual values obtained from repeated measurements
X = mean of the measured valuesn = number of measurements (2, 6).
Figure 3. The accuracy of the measurement refers to closeness ofthe agreement between the result of a measurand and a true
value.

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
of uncertainty, known as the combined stand-ard uncertainty (UMc) . UMc is given by thesquare root of the sum of the squares:
U2BU2
AcUM +±= [3].
Expanded uncertainty (U) is calcu-lated by multiplying the standard uncertaintyUMc with an appropriate coverage factor k:
U = k • UMc [4], for a desired levelof confidence of 95%, k is approximately 2.
Uncertainty reported with the result isexpanded uncertainty and is then convenientlyexpressed as:
Y ± U [5], where:
Y = measured result,U = expanded uncertainty.
The Guide to the expression of uncer-tainty in measurement (GUM) (2) was de-veloped for estimating UM in all laboratoriestypes. In non-medical laboratories the potentialsources of uncertainty are usually readily identi-fiable, quantifiable and converted in standarddeviations in fields such as physical and chem-ical measurements (e.g. electrical, materials, op-tics, etc). These standard deviations are used forcalculation of UMc.
The Working Group for the MedicalTesting Laboratory recognizes that the imple-mentation of the uncertainty of measurement re-quirement offers opportunities for pathologylaboratories to add value to their diagnostic ser-vices, particularly in educating users to betterunderstand the limitations of tests, and in recog-nizing when clinically significant changes in pa-tient results have or have not occurred. ISO15189 also recognizes that the rigor of estimat-ing uncertainty of measurement may be basedon the needs of the client.
In medical testing there are many poten-tial “uncertainties” that can significantly affecttest results (for example: poor specimen collec-tion or transport, patient related factors such as
biological variation and the presence of drugs,clerical and reporting errors etc). Not all thesefactors can be quantified in standard deviationsand therefore such factors are excluded from theestimation of uncertainty of measurement (7). Itis important to identify such factors and keepthem under an adequate management. In medic-al laboratories is difficult to strictly respectGUM regulations. However, medical laboratorymeasurements are strictly monitored by an in-ternal and external control system, and thereforethe data generated can be used to estimate UM.
A basic requirement of GUM is to es-tablish a mathematical expression which has toinclude all the input quantities that signific-antly influences the test result. In medicallaboratories rigorously implementation ofGUM is difficult, but the above requirement ofGUM must be respected.
Whatever approach is used, estimationof UM should consider the basic requirementsof GUM and the following steps (2, 4):
1. complete definition (or specification) ofthe measurand;
2. careful consideration and understanding ofeach phase of the measurement process;
3. mathematical expression of the equationrelating measurand (Y) and input quantities (Xi)using a functional relationship in the formY = f ( X1, X2, X3...Xn). Functional relationship fshould enclose all input quantities that contributeto the final result;
4. estimation of a certain value for all inputquantities in functional relationship f using stat-istical methods or other means;
5. evaluation of standard uncertainty forevery quantity Xi;
6. calculation of combined standard uncer-tainty;
7. calculation of expanded standard uncer-tainty with a chosen coverage factor;
8. reporting uncertainty of measurement.
1. Defining the measurand as fully as possiblein terms of designation, matrix, unit of measure,because lack of measurand definition brings a
69

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
major uncertainty to the final test result. Thiswill yield major discrepancies between themeasurement results in different laboratories forthe same analyte.
Analyte is a term used to identify thesubstance or constituent of interest (e.g. creatin-ine) that is the subject of measurement. How-ever, a substance can have a number of proper-ties (e.g. concentration, different matrix, differ-ent unit of measure, different measurementmethods), some or all of which can be utilizedto quantify the substance in an appropriatemeasuring system. The particular quantifiableproperty of the analyte used in the measuringsystem is called the measurand (7).
For example, the analyte is creatinineand the measurand is creatinine concentration inserum, plasma or urine expressed in mg/dl orµmol/l. Therefore it is essential to define ascompletely as possible the quantity that is meas-ured (i.e. the measurand) by a given procedure.
2. Establishing the measurement principle ofthe specified technical procedure for performinga test concerning of all reaction phases is exem-plified by the principle of measurement of creat-inine in a biological sample. Picric acid reacts inalkaline conditions with creatinine from analysedbiological sample to form picramic acid. This is acolored product with a color intensity which ismeasured at a certain wave length (510 nm) asoptic density directly proportional with creatinineconcentration from analysed biological sample.
3. Establishing a mathematical formula thatdetermines the functional relationship betweenmeasured quantity Y and measured quantities(Xi, input quantities upon which final test resultdepends). In order to convert optical densityinto a test result a reference material (calibrator)with a known value of creatinine (measurand) isused. The calibrator is measured in the sameconditions as the analyzed biological sample. Atthe end of the reaction, optical density (OD)read by the equipment for reference material hasthe same value as the value assigned to the cal-
ibrator from the specifications of the manufac-turer. This process it is called calibration andrepresents a “set of operations that establish, un-der specified conditions, the relationshipbetween values of quantities indicated by ameasuring instrument or measuring system, orvalues represented by a material measure or areference material, and the corresponding valuesrealized by standards” (3). Therefore, the resulty of creatinine from patient sample could be cal-culated by rule of three:
2500 OD................. 3.6 (calibrator value)1800 OD.................. y
calibratorcalibrator
sample valueOD
ODy •= [6],
where OD is optical density (of calibrat-or, respectively to patient sample).
Figure 4 represents the calibrationcurve for creatinine in 2 points, respectively 0and 3.6 mg/dl. If the calibrator value of 3.6mg/dl includes UM expressed as range value(see the dotted lines of Figure 4), the opticaldensity of final product reaction of patientsample, 1800, will lead to different results ac-cording to the calibration curve used.
Since the reference materials (calibrat-ors, etalons and standards) are very homogen-ous it is admitted that value distribution is rect-angular (9). Thus, calibration curve can be situ-ated anywhere in the range marked with dottedlines, not necessarily in the middle of the range.
The constructed calibration curve couldbe validated and used for carrying out the meas-urements on the patient’s samples only after isverified using the control materials of knownvalues because a lot of error sources from usedequipment used, reagents, medium conditions,laboratory technicians etc. may appear. Themeasurement system (equipment, reagents, cal-ibration curve and analyst) is verified in termsof correctness by testing control materials ondifferent levels. These control materials havepredetermined values and could alert the analystregarding the errors of measurement system.
70

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
The results obtained by measuring con-trol materials are analyzed considering West-gard rules and the acceptance / rejection criteriaof each laboratory. Internal control tests withcontrol materials are similar to diagnostic testsof patient samples. Similarly with diagnostictests in patients, which identify the health prob-lems of the patient, the tests of internal controlidentify the “health problems” (errors) of themeasurement system (10). Rapid detection andadequate treatment is depending upon preciseand quick identification of the “healthproblem”.
The reference materials (calibrators, et-alons, standards) are considered Xi quantitiesupon which final test result depends, while con-trol material is used for verifying and validatingthe correctness of calibration but does not havea direct influence on final result.
4. Estimation of a value for all input quantitiesThe result of a quantitative measure-
ment Y is a functional relationship f (X i), whereX i represents all the factors upon which themeasurement depends (X1, X2, X3 ... Xn) (4, 7).All relevant sources of uncertainties that could
influence the test result should be identified.Consideration should be given to all relevantfactors that may contribute to the overall uncer-tainty of a measurement and could influence thetest result. Some examples are given below:
X1 = factors affecting pre-analytical phasecannot be usually quantified, but must becontrolled by an adequate management;
X2 = measurement procedure (method, re-agents, measuring instruments, laboratoryhardware etc);
X3 = reference material (calibrator);X4 = factors affecting post-analytical phase; ....Xn = others factors.
In medical laboratories, after identifica-tion of all input quantities Xi, it could be ob-served that the measurement procedure used(method, reagents, instruments, laboratory stuffetc.) and the reference materials (calibrators) arethe only quantifiable factors that could be con-verted in standard deviations.
The best estimation for the measurementprocedure used is the average of the measuredvalues obtained in n repeated measurements (theprecision) between-day and within-day measur-ing technique (from data of internal control).
The estimation of the value of referencematerial (calibrator) is offered by the manufacturer.
5. Estimation of standard uncertainty foreach quantity Xi
At least 30 values of control serum onat least 30 different consecutive days were usedin the measurement procedure. In this case theXi input estimate is usually the average value.All values from the internal control have Gaus-sian (normal) distribution. Standard uncertaintyU(xi) is the estimated standard deviation of themean calculated by formula [2]. This standarduncertainty is estimated by statistical calculationof measurement values and therefore it is namedType A uncertainty.
When the medical laboratory uses refer-ence materials which are not traceable to CRM,the laboratory does not know the UM of the cal-
71
Figure 4. Calibration curve in 2 points.

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
ibrator although this is a measured value and isaccompanied by UM. When used calibrators aretraceable to certified reference materials(CRM), their values are accompanied by exten-ded uncertainty. Uncertainty of the values as-signed to the calibrator can be obtained by re-quest from the manufacturer usually as extendeduncertainty (for 95% confidence interval of thecalibrator assigned value, k=2) (Figure 5).Combined uncertainty of the values assigned tothe calibrator is used in medical laboratories, soUextended should be divided by 2.
Uncertainty of the values assigned tothe calibrator indicates the accuracy measure-ment as type B uncertainty because it is takenfrom the manufacturer’s specifications and it isnot a result of statistical calculations performedby the medical laboratory (11, 12).
6. Calculation of combined standarduncertainty (UMc)
Calculation of combined standarduncertainty is done following equation[5], in which the medical laboratory hasthe responsibility to choose many UBi:
U2
nB
...U2
1BU2
AUMc +++±= [7]
where:UA = U measurement procedure (from internal
quality control),UB1 = Ucalibrator (from manufacturer spe-
cifications),UB2 = UBias (from external quality con-
trol),Uother factors (from speciality literature
data) (4).Under these conditions, equation
[5] becomes equation [8].
7. Calculation of expanded standard un-certainty (UM expanded) with a chosen cover-age factor
Expanded uncertainty, usually shownby the symbol U, is obtained by multiplying theUMc by a coverage factor, denoted by symbolk = 2, for a level of confidence of approximately95% (2).
UM expanded = U = UMc · k [9].
8. Reporting uncertainty of measurementMost laboratories have chosen until
now not to state measurement uncertainty intheir test reports. Instead, such information hasbeen given only when the physicians have spe-cifically required it. It is important for laborator-ies to understand the clinical implications of theresults of the measurements they report and tobe aware of those where UM could affect clinic-al interpretations and patient management.
72
Equation [8]:
U2
factorsother ...U2
control) nalBias(exterU2calibratorU
2cUM +++±=
tproceduremeasuremen.
Figure 5. UM of used reference material (calibrator)represents type B uncertainty (UB) because it is taken from
manufacturer specifications (X = average values measured).

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
Uncertainty reported with the result isexpanded uncertainty and is then convenientlyexpressed as:
Y ± U [10], where:Y = measured result,U = expanded uncertainty.
The laboratory should offer detaileddata to users (physician, patient) about the pat-tern estimation used for UM.
Each laboratory has the responsibility toidentify all quantifiable error sources, which can
be converted in standard deviations used for es-timating type A and type B standard uncertainty.
Type A standard uncertainty is assessedfrom internal quality control data (statistical cal-culation on at least 30 values of control serumfrom at least 30 different consecutive days).Type A standard uncertainty illustrates the pre-cision of laboratory measurements.
When the laboratory uses traceable cal-ibrators to certified reference materials (CRM)with attributed UM, this can be treated as type Bstandard uncertainty. Type B standard uncer-tainty shows the accuracy of measurements.
73
Figure 6. Combined standard uncertainty comprises type A standard uncertainty (UA, precision ofmeasurements) and type B standard uncertainty (UB, accuracy of measurements).
UA is statistically calculated from values of independent measurements with Gaussian distribution. Regarding
type B uncertainty, there are many kinds of UB according to literature specifications: UB1, UB2, ….. ,UBn. When amedical laboratory chooses to estimate its accuracy of measurements from Bias intercomparisons, the standarddeviation of Bias (Bias values from many participations to external control have rectangular distribution) has to
be calculated following the formula 3
SDBias
a= , where a = Bias (adapted after SR ENV 13005:2005).
Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 201074
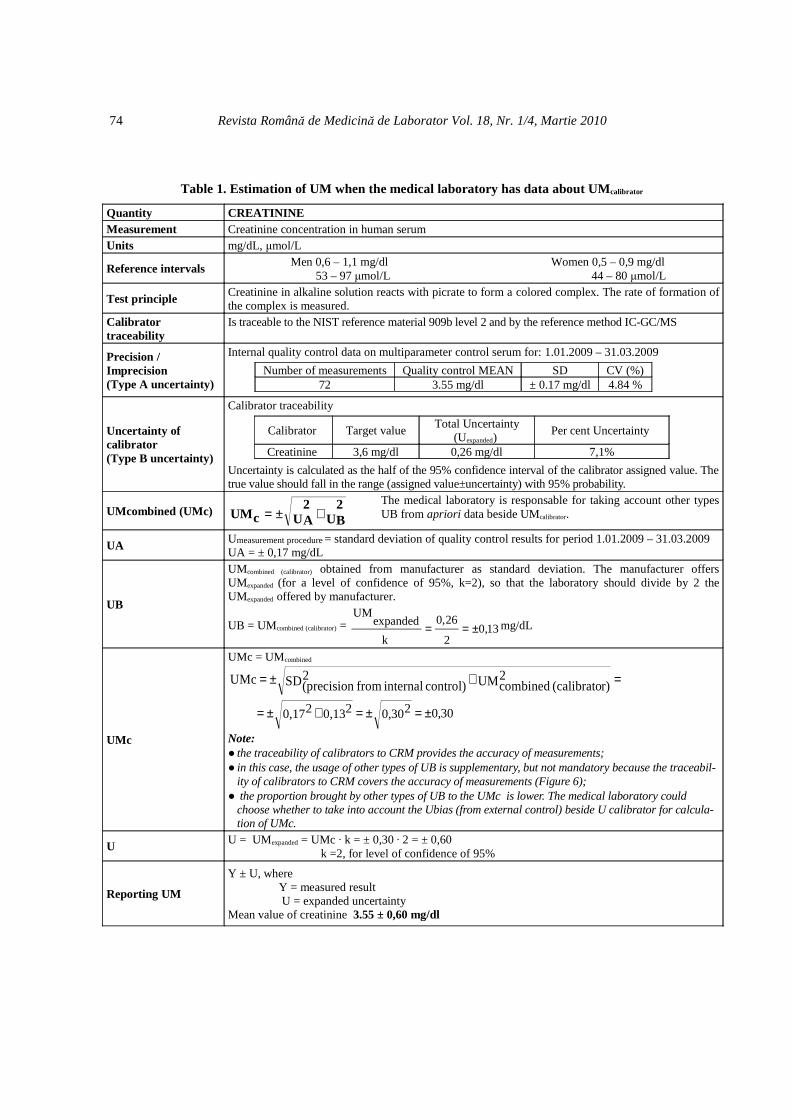
Table 1. Estimation of UM when the medical laboratory has data about UMcalibrator
Quantity CREATININEMeasurement Creatinine concentration in human serumUnits mg/dL, µmol/L
Reference intervals Men 0,6 – 1,1 mg/dl 53 – 97 µmol/L
Women 0,5 – 0,9 mg/dl 44 – 80 µmol/L
Test principle Creatinine in alkaline solution reacts with picrate to form a colored complex. The rate of formation ofthe complex is measured.
Calibratortraceability
Is traceable to the NIST reference material 909b level 2 and by the reference method IC-GC/MS
Precision /Imprecision(Type A uncertainty)
Internal quality control data on multiparameter control serum for: 1.01.2009 – 31.03.2009
Number of measurements Quality control MEAN SD CV (%)72 3.55 mg/dl ± 0.17 mg/dl 4.84 %
Uncertainty ofcalibrator(Type B uncertainty)
Calibrator traceability
Calibrator Target valueTotal Uncertainty
(Uexpanded) Per cent Uncertainty
Creatinine 3,6 mg/dl 0,26 mg/dl 7,1%
Uncertainty is calculated as the half of the 95% confidence interval of the calibrator assigned value. Thetrue value should fall in the range (assigned value±uncertainty) with 95% probability.
UMcombined (UMc)U
2BU
2AcUM +±=
The medical laboratory is responsable for taking account other typesUB from apriori data beside UMcalibrator.
UA Umeasurement procedure = standard deviation of quality control results for period 1.01.2009 – 31.03.2009UA = ± 0,17 mg/dL
UB
UMcombined (calibrator) obtained from manufacturer as standard deviation. The manufacturer offersUMexpanded (for a level of confidence of 95%, k=2), so that the laboratory should divide by 2 theUMexpanded offered by manufacturer.
UB = UMcombined (calibrator) = 13,02
26,0
k
expandedUM
±== mg/dL
UMc
UMc = UMcombined
=+±= UM2r)(calibrato combinedSD2
control) internal from (precisionUMc
30,00,3020,1320,172 ±=±=+±=
Note:● the traceability of calibrators to CRM provides the accuracy of measurements;● in this case, the usage of other types of UB is supplementary, but not mandatory because the traceabil-
ity of calibrators to CRM covers the accuracy of measurements (Figure 6);● the proportion brought by other types of UB to the UMc is lower. The medical laboratory could
choose whether to take into account the Ubias (from external control) beside U calibrator for calcula-tion of UMc.
U U = UMexpanded = UMc · k = ± 0,30 · 2 = ± 0,60 k =2, for level of confidence of 95%
Reporting UM
Y ± U, where Y = measured result U = expanded uncertainty Mean value of creatinine 3.55 ± 0,60 mg/dl

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
Unfortunately, in most medical laborat-ories from our country calibrators without trace-able values are used. If an appropriate referencematerial or reference procedure is unavailable,then alternative approaches may be used, e.g.external quality assessment data or inter-labor-atory comparisons (13).
In this case, accuracy of measurementsis estimated by type B uncertainty calculated asstandard deviation of Bias values from externalcontrol. Bias is the difference between meas-ured result and average results of participantmedical laboratories based on an intercomparis-ons scheme (external control). Bias values frommany external control participations have a rect-angular distribution (variance) given by:
( ) ( )12
24a
12
22a
12
2minmax)i(x2U ==−= [11] (6).
For this reason, standard deviation ofBias is calculated by formula:
3
a
32
2a
34
24a
12
24aSD U ==
•=== [12],
(Figure 6).
In this paper the authors summarize theestimation of UM in two situations: when theassigned values of traceable calibrators to CRMare or not accompanied by UM as shown inTables 1 and 2.
The assigned values of traceable calib-rators to CRM are accompanied by UM asshown in Table 1.
Manufacturers do not always providethe uncertainty of the values assigned to calib-rators. In this case UM is estimated by follow-ing the model shown in Table 2.
Conclusions
1. Uncertainty Measurement of a measuredresult increases its reliability.2. A reasonable estimation of UM includes pre-cision (UA) and accuracy of measurements (UB):
a. Precision is expressed as standarddeviation of the values obtained in in-ternal quality control using a large num-ber of measurements on at least 30 daysperiod. b. Measurements results in medicallaboratories are used for clinical de-cisions, and therefore it is very importantto include accuracy of measurement inUMcombined. Each medical laboratory hasthe responsibility to guarantee the accur-acy of measurements by using referencematerials (calibrators) with traceability toCRM and / or participations of the labor-atory to intercomparison schemes.
3. The laboratories should request data aboutthe traceability of calibrators from the manufac-turers. Uncertainty of the value assigned to thecalibrator has a major importance in assessingmeasurement accuracy. 4. When the medical laboratory does not havedata about the calibrator values’ UM, the accur-acy of measurements could be estimated bystandard deviation of Bias from external qualitycontrol (intercomparison schemes).5. It is important for laboratories to understandthe clinical implications of the results of the meas-urements they report and to be aware of those res-ults where UM could affect clinical interpretationsand patient management. The clinician needs to beaware of the UM together with the result to makea correct diagnosis. The uncertainty of the result isimportant, e.g. when looking at the limits of refer-ence interval or cut off. It is necessary to estimatethe UM when comparing results to allowable val-ues, e.g. tolerance limits or allowable (legal) con-centrations (doping control).6. Where uncertainty of measurement inform-ation, if reported, could significantly affect clin-ical interpretations and patient management(e.g. tumor marker monitoring), such informa-tion should be readily available on request andcomprehensive about the laboratory’s method ofassessment.
75

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
7. Assessing and reporting measurement un-certainty will help reduce the differencesbetween laboratories’ results, which translatesinto prompt clinical decision, low costs, higherefficiency and highest confidence of cliniciansand patients in testing results.
Acknowledgements
This study was supported by MedicalInvestigations Praxis S.R.L., Iasi, Romania. andthe National University Research Council –CNCSIS, grant PN_2_ID_PCE_2670/2008.
76
Table 2. Estimation of UM when the medical laboratory does not have data about UMcalibrator
Quantity Tyroid stimulating hormone (TSH)Measurement TSH concentration in human serum.
Units µUI/mL
Reference intervals 0,4 – 6,0 µUI/mL
Test principleThe TSH ELISA test is based on the principle of a solid phase enzyme-linked immunosorbent as-say. The assay system utilizes a unique mouse monoclonal antibody directed against a distinct an-tigenic determinant on the intact TSH molecule.
Calibratortraceability
6 calibrators (included in kit): 0; 0,5; 2; 5; 10; 25 µUI/ml is not traceable to CRM
Precision /Imprecision(Type A uncertainty)
internal QC data on multiparameter control serum for: 1.01.2009 – 31.03.2009Number of measurements QC Mean SD CV (%)
48 4.03 µUI/ml ± 0.32 µUI/ml 7.94%
Type B uncertainty
Standard deviation of Bias from external quality control (intercomparisons schemes) Bias = measured result – intercomparison average The Bias values from the same period for Umeasurement procedure have a rectangular distribution, so
3BiasSDa
= (Figure 6)
BIAS1 (Cycle 6/Sample 8) = 2.98 – 3.02 = - 0,04BIAS2 (Cycle 6/ Sample 10) = 3.64 – 3.81 = - 0,17BIAS3 (Cycle 6/ Sample 11) = 4,26 – 4,20 = +0,06
09,03
17,0
3
.max
3BiasSD =−
===BIASa
µUI/ml
UMc
UMc = UMcombined
U2BU
2AcUM +±=
=+±=control) (externalSD
2BiasSD
2control) internal from (precisionUMc
= 0,330,092
0.322
±=+± µUI/ml
Note: The medical laboratory is responsible for taking into account other UB types from aprioridata beside UMBias (from external control)
U U = UMexpanded = UMc · k = ± 0,33 · 2 = ± 0,66 µUI/ml k =2, for level of confidence of 95%
Reporting UM
Y ± U, where Y = measured result U = expanded uncertaintyMean value of TSH 4.03 ± 0,66 µµµµUI/ml

Revista Română de Medicină de Laborator Vol. 18, Nr. 1/4, Martie 2010
Abbreviations list
CRM certified reference materialsCV coefficient of variationEA European AccreditationGUM Guide to the expression of
uncertainty in measurementOD optical densitySD standard deviationUM uncertainty of measurementUMc combined standard uncertaintyUMexpanded, U expanded standard uncertainty
References
1. International Organization of Standardization, ISO/TC212. ISO 15189:2007, Medical laboratories - Particular re-quirements for quality and competence, 2nd Edition.Geneva, 2007: p372. ISO/IEC Guide 98-3:2008. Uncertainty of measurement- Part 3: Guide to the expression of uncertainty in measure-ment (GUM:1995). International Organization for Standard-ization (ISO)/ International Electrotechnical Commission(IEC): Geneva, 2008: p 3-583. BIPM, IEC, IFCC, ILAC, ISO, IUPAC, IUPAP, OIML,The International Vocabulary of Metrology, Basic and Gen-eral Concepts and Associated Terms - VIM, Joint Committeefor Guides in Metrology- JCGM 200:2008 [ISO/IEC Guide
99]: p 22-284. Eurachem / Citac Guide CG4, Quantifying Uncertaintyin Analytical Measurement, Second Edition, 2001: p16-305. Technical Report EA- 4/16 (rev00). Guidelines on theexpression of uncertainty in quantitative testing. EuropeanCo-operation for Accreditation (EA), 2003: p 6-166. SR ENV 13005:2005. Romanian Standard for estima-tion of measurement uncertainty, Third Edition; 2005: p 8-187. White GH, Farrance I. Uncertainty of measurement inquantitative medical testing: a laboratory implementationguide. Clin Biochem Rev. 2004;25(4):S1-S248. Hibbert B. Quality assurance for the analytical chem-istry laboratory. Oxford University Press US, 2007: p 2559. Taylor BN, Kuyatt KE. Guidelines for Evaluating andExpressing the Uncertainty of NIST Measurement Result -National Institute of Standards and Technology TechnicalNote 1297. U.S. Government Printing Office, WashingtonDC, 1994: p 2-610. Are there similar performance characteristics for QCand diagnostic tests? "Westgard Rules" and Multirules.Westgard QC (n.d.) Retrieved November 01, 2009 fromhttp://www.westgard.com/mltirule.htm#performance11. European Diagnostic Manufactures Association(EDMA). Estimation of uncertainty of measurement in med-ical laboratories, 2006: p 2-512. The Romanian Accreditation Association (RENAR).Instruction for validation of methods used in medical labor-atories, RENAR Code: I-12, First Edition, 2007: p 1-913. White GH. Basics of estimating measurement uncer-tainty. Clin Biochem Rev. 2008 Aug;29 Suppl 1:S53-60
77





























