Embed Size (px)
Citation preview
150
Clinical significanceWe succeeded in developing a system of measurement for deciding what prosthodontic treatment modality should be selected for preservation of the abutment teeth from the standpoint of vibratory characteristics by application of in-vivo modal analysis to the maxil-lary dentition of the maxillectomy patient.
AbstarctPurpose: The purpose of this study was to apply in-vivo modal analysis to the maxillary dentition of the maxillectomy patient using obturator prostheses which were different in lateral wall height of the bulb: specifi-cally a high type (H type), middle type (M type), and low type (L type).Methods: The left central incisor was struck with an impact hammer, and the response at each measure-ment point was detected using a Laser-Doppler vibrom-eter. The transfer function was then obtained from each measurement point using a fast Fourier transform ana-lyzer. Finally, a computer analysis and simulation were performed based on the measured transfer functions to obtain the natural frequency, modal shape decay rate (DR), and maximum displacement (MDP).Results: The results showed that the natural frequen-cy was different between with and without obturator prostheses, that the modal shapes with M and L type obturator prostheses are more suitable than that with H type. The DR of the maxillary dentition with the L type was significantly higher than that with the H or M types, and the MDP of the maxillary dentition with an obturator prosthesis was significantly lower than with-out an obturator prosthesis.Conclusion: From the standpoint of vibratory charac-teristics, the L type obturator prosthesis is the most suitable bulb design for the patient of the three types obturator prostheses. This is the first report to apply
in-vivo modal analysis to the maxillary dentition of the maxillectomy patient using obturator prostheses and clarify the vibratory characteristics of the dentition.
Key words: in-vivo modal analysis, obturator prosthe-sis, maxillectomy patient, maxillofacial prosthetics, bulb designs
IntroductionSurgical resection of the maxilla due to malignant tumor causes the loss of supporting structures, creates an interconnection between the oral and nasal cavity,1 and results in many types of oral functional disorders. A maxillary surgical defect can be compensated for by the use of an obturator prosthesis2 that enables maxillectomy patients to recover a number of functions, such as mastica-tion, deglutition, speech, and appearance.3 The bulb of an obturator prosthesis extends into the nasal cavity, ensuring oronasal separation, the re-tention and stability of the obturator prosthesis, and restoring the natural shape of the cheeks. However, in partially edentulous cases with large maxillary defects, the lack of support and the weight of the bulb of an obturator prosthesis can cause dislodging and rotational forces, that is a cantilever effect, on the abutment teeth, especially during mastication.1, 2, 4
With regard to nasal extension, Brown5 report-ed that increasing the lateral wall height of an ob-turator prosthesis above the scar band can prevent vertical displacement geometrically. Desjardins6 recommended the medial wall should not be as high as the lateral wall, and that the anterior as-pect should be higher than the posterior aspect to encourage mucous drainage in the medial and posterior direction into the nasopharynx. Sharry7 reported that it was not necessary to fill the entire defect, since filling the cavity with a mass of acryl-ic not only adds unwanted weight to the prosthe-
J Jpn Prosthodont Soc 52:150-159, 2008
Corresponding to: Dr Itsuki MuraseDepartment of Maxillofacial Prosthetics, Graduate School, Tokyo Medical and Dental University1-5-45 Yushima, Bunkyou-ku, Tokyo 113-8549, JapanTel: +81-3-5803-5556, Fax: +81-3-5803-5556E-mail: [email protected]
Received on April 24, 2007/Accepted on August 1, 2007
ORIGINAL ARTICLE
In-Vivo Modal Analysis of Maxillary Dentition in a Maxillectomy Patient Wearing Buccal Flange Obturator Prostheses with Different Bulb Height DesignsItsuki Murase, DDS
Department of Maxillofacial Prosthetics, Graduate School, Tokyo Medical and Dental University, Tokyo, Japan
07_01_Murase.indd 150 08.5.2 8:19:14 PM

In-Vivo Modal Analysis of Maxillary Dentition 151
sis, but will impair speech quality.On the other hand, based on scientific analysis,
some studies8-12 have recently used modal analysis to investigate the effect of bulb design on the vi-bratory characteristics of obturator prostheses. Modal analysis13 is one method of revealing the dynamic characteristics of a structure with mass by investigating how each component vibrates at its own natural frequency. Modal shape can be ob-served at the natural frequency, and the transient response simulation of this system can calculate the maximum displacement (MDP) and decay rate (DR) of each component for any selected intensity, direction, and location of the impact force.
Concerning the application of modal analysis to maxillofacial prosthetics, Piyawat et al 14 evaluated the vibratory characteristics of metal framewoks of obturator prostheses with different designs. Oki et al 8 compared the vibratory characteristics among solid, buccal flange and hollow obturator prosthe-ses. Orapin et al 9 evaluated the effect of the bulb relined with a soft lining material on the vibratory characteristics of obturator prostheses. Kobayashi et al 10, 11 compared the vibratory characteristics among designs of different lateral bulb heights in both hollow10 and buccal flange11 obturator pros-theses. Oki et al 12 evaluated the vibratory charac-teristics of eight obturator prostheses with differ-ent lateral and medial bulb heights and hollow and buccal flange bulb forms.
However, these studies were not directly applied to living human maxillary dentition. It appears to be necessary to analyze the vibratory characteris-tics of living human maxillary dentition with the obturator prostheses from the viewpoint of preser-vation of abutment teeth. Since the vibratory char-acteristics of a structure depend on numerous fac-tors, including its shape, mass and stiffness,15 it is not evident whether the vibratory characteristics of obturator prostheses in vitro reflect those of the living dentition with the obturator prosthesis in place.
Modal analysis is normally applied to rigid sub-stances, so there have been many difficulties with the direct application of modal analysis to living human maxillary dentition due to the highly damping effect of the periodontal ligament. Du et al 16 were the first to apply modal analysis to the living human maxillary dentition of normal and cleft lip and palate (CLP) subjects. Iida et al 17 re-ported the effect of bone grafting in CLP patients on the vibratory characteristics of maxillary den-
tition from the standpoint of modal shape, DR, and MDP. Both studies16, 17 used an acceleration sensor which was 5.8 mm in diameter and estab-lished only a single measurement point per mea-sured tooth, which made it possible to observe the two-dimensional modal shape of the maxillary dentition. Matsui et al 18 applied a Laser-Doppler vibrometer, which employs an extremely small la-ser spot, less than 100 µm in diameter, as a sensor, making it possible to establish two measurement points per measured tooth and to observe the three-dimensional modal shape of the maxillary dentition. They reported the vibratory character-istics of the maxillary dentition in normal subjects with and without a mouthguard from the stand-point of modal shape, DR, and MDP.
The purpose of this study was to apply in-vivo modal analysis to the maxillary dentition of a maxillectomy patient with and without an obtura-tor prosthesis and to determine the most suitable bulb design from the viewpoint of preservation of abutment teeth. For this purpose, we used a La-ser-Doppler vibrometer to establish two measure-ment points per measured tooth and analyzed the three-dimensional modal shape of the maxillary dentition. We then evaluated the effect of differ-ence in lateral wall height of the bulb on the max-illary residual dentition from the standpoint of the natural frequency, DR, and MDP.
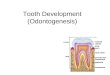
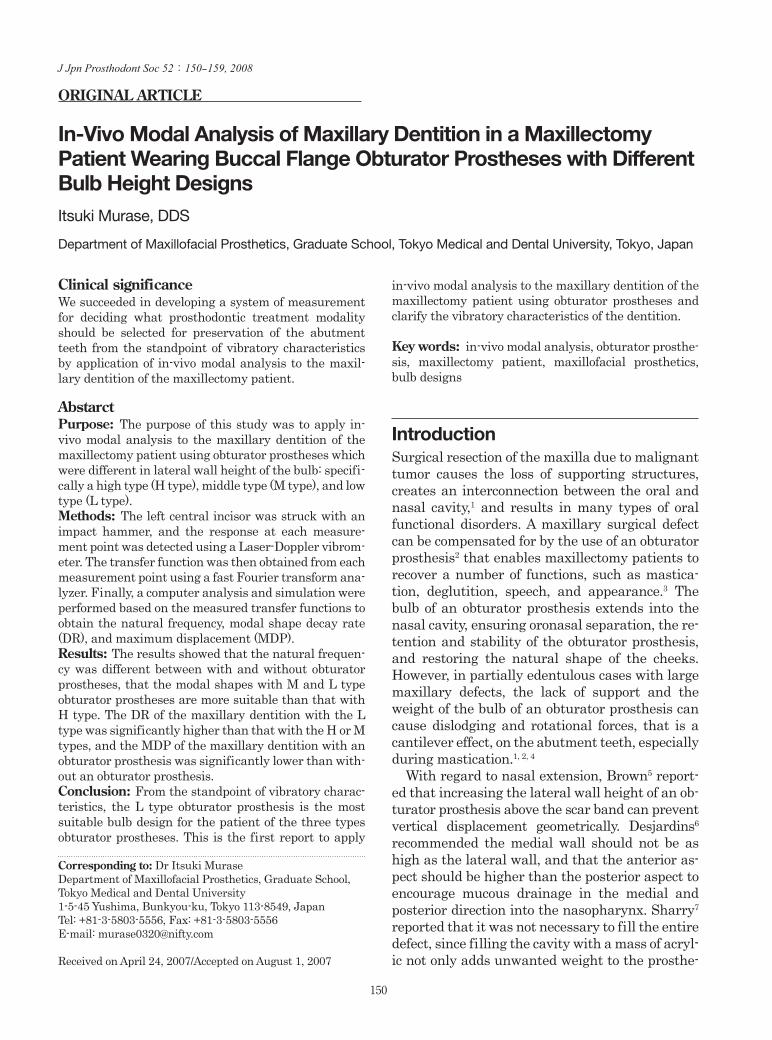
Materials and Methods1. Test subjectA 62-year-old male patient participated in this study. The patient had undergone right maxillary resection for tumor and immediate reconstruction with the rectus abdominis flap to inside the buccal region. The maxillary dentition of the patient re-mained from the right lateral incisor to the left second molar, and showed no periodontal dis-ease (Fig. 1a,b). Before this experiment was car-ried out, the approval of Tokyo Medical and Dental University’s ethics committee was obtained for the experiment (registered number: 184). In-formed consent was obtained from the patient prior to the experiment.
2. Obturator prosthesisTo fabricate an obturator prosthesis, a final im-pression was taken with compound and silicon im-pression material (Exafine, GC Co., Tokyo, Japan)
07_01_Murase.indd 151 08.5.2 8:19:14 PM
Murase et al., J Jpn Prosthodont Soc 52 : 150-159, 2008152
using an individual resin tray. The working plaster model was made of dental stone. The defect size in the model was 19 mm medial-distally, 50 mm buc-cal-palatally, and 26 mm in height (Fig. 2).
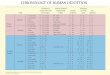
The maxillary and mandibular models were mounted on an articulator with a jaw relation re-cord by the bite plate. Then, the artificial teeth (Enduea Anterio and Enduea Posterio, Shofu Co., Tokyo, Japan) were provisionally arranged accord-ing to the mandibular model to determine the gen-eral form of the palate and the alveolar ridge on the defect side. After confirming that the wax den-ture was suited to the patient, a metal framework was fabricated of chrome-cobalt alloy (Biosil-f, DeguDent Co., Hanau, Germany) by referring to the wax denture. The framework had two em-brasure clasps on the first molar and second pre-molar and on the first premolar and canine tooth, a circumferential clasp on the second molar and a wire clasp (Sun-Cobalt Clasp-Wire, Dentsply-Sankin Co., Tokyo, Japan) with the cast rest on the right lateral incisor. Registration of interocclu-sal relations was then taken by means of a frame-work with a wax rim, and the artificial teeth were again arranged. A buccal flange-type obturator prosthesis with a bulb wall thickness of approxi-mately 2 mm was fabricated in the standard man-ner using heat-polymerizing acrylic resin (Acron, GC Co., Tokyo, Japan). The obturator prosthesis was adjusted until the subject was able to wear it easily and painlessly. The edge of the lateral wall of the bulb was about 20 mm above the lateral scar band (Fig. 3a,b). The obturator prosthesis in this study was of the H type.
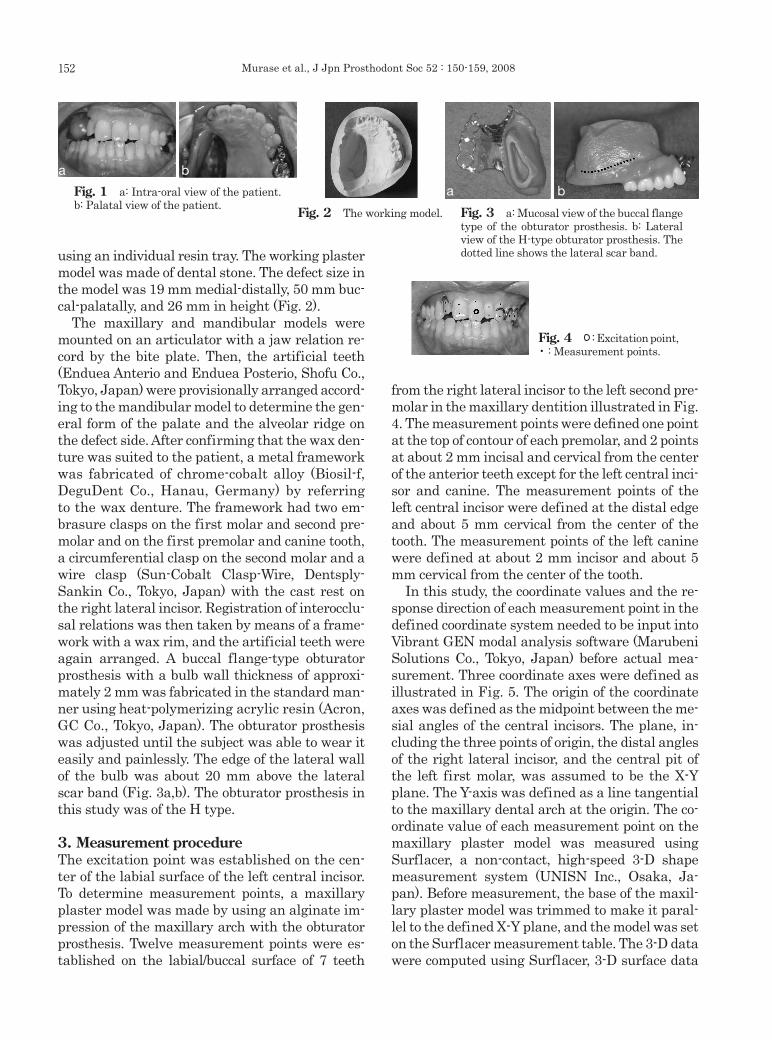
3. Measurement procedureThe excitation point was established on the cen-ter of the labial surface of the left central incisor. To determine measurement points, a maxillary plaster model was made by using an alginate im-pression of the maxillary arch with the obturator prosthesis. Twelve measurement points were es-tablished on the labial/buccal surface of 7 teeth
from the right lateral incisor to the left second pre-molar in the maxillary dentition illustrated in Fig. 4. The measurement points were defined one point at the top of contour of each premolar, and 2 points at about 2 mm incisal and cervical from the center of the anterior teeth except for the left central inci-sor and canine. The measurement points of the left central incisor were defined at the distal edge and about 5 mm cervical from the center of the tooth. The measurement points of the left canine were defined at about 2 mm incisor and about 5 mm cervical from the center of the tooth.
In this study, the coordinate values and the re-sponse direction of each measurement point in the defined coordinate system needed to be input into Vibrant GEN modal analysis software (Marubeni Solutions Co., Tokyo, Japan) before actual mea-surement. Three coordinate axes were defined as illustrated in Fig. 5. The origin of the coordinate axes was defined as the midpoint between the me-sial angles of the central incisors. The plane, in-cluding the three points of origin, the distal angles of the right lateral incisor, and the central pit of the left first molar, was assumed to be the X-Y plane. The Y-axis was defined as a line tangential to the maxillary dental arch at the origin. The co-ordinate value of each measurement point on the maxillary plaster model was measured using Surflacer, a non-contact, high-speed 3-D shape measurement system (UNISN Inc., Osaka, Ja-pan). Before measurement, the base of the maxil-lary plaster model was trimmed to make it paral-lel to the defined X-Y plane, and the model was set on the Surflacer measurement table. The 3-D data were computed using Surflacer, 3-D surface data
Fig. 2 The working model.
Fig. 4 : Excitation point, • : Measurement points.
Fig. 1 a: Intra-oral view of the patient. b: Palatal view of the patient.
ba
Fig. 3 a: Mucosal view of the buccal flange type of the obturator prosthesis. b: Lateral view of the H-type obturator prosthesis. The dotted line shows the lateral scar band.
ba
07_01_Murase.indd 152 08.5.2 8:19:15 PM
In-Vivo Modal Analysis of Maxillary Dentition 153
management-convert-analysis software (Image-ware Inc., Ann Arbor, MI, USA). The coordinate values of each measurement point were input into Vibrant GEN to draw the wire frame shape.
The response direction of each measurement point was defined by the value of angles formed by the X-axis and perpendicular lines tangential to the maxillary dental arch at each measure-ment point (Fig. 6). These angles were geometri-cally calculated from the projection of measure-ment points onto the X-Y plane using the maxillary plaster model.
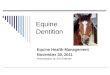
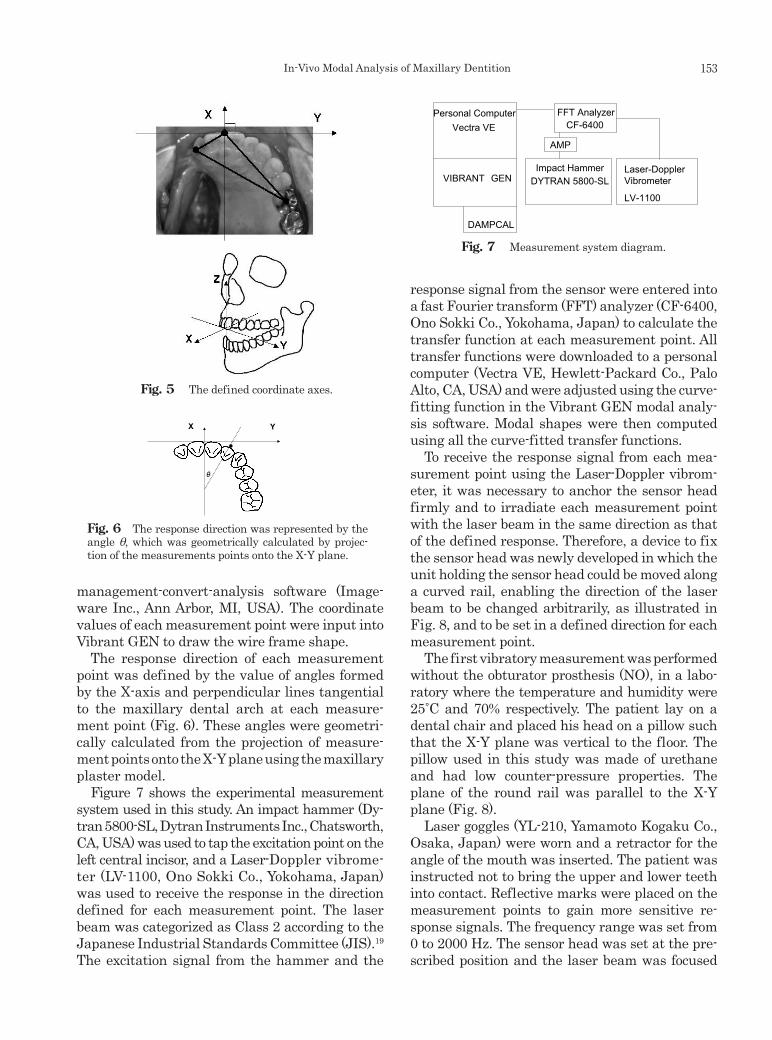
Figure 7 shows the experimental measurement system used in this study. An impact hammer (Dy-tran 5800-SL, Dytran Instruments Inc., Chatsworth, CA, USA) was used to tap the excitation point on the left central incisor, and a Laser-Doppler vibrome-ter (LV-1100, Ono Sokki Co., Yokohama, Japan) was used to receive the response in the direction defined for each measurement point. The laser beam was categorized as Class 2 according to the Japanese Industrial Standards Committee (JIS).19 The excitation signal from the hammer and the
response signal from the sensor were entered into a fast Fourier transform (FFT) analyzer (CF-6400, Ono Sokki Co., Yokohama, Japan) to calculate the transfer function at each measurement point. All transfer functions were downloaded to a personal computer (Vectra VE, Hewlett-Packard Co., Palo Alto, CA, USA) and were adjusted using the curve-fitting function in the Vibrant GEN modal analy-sis software. Modal shapes were then computed using all the curve-fitted transfer functions.
To receive the response signal from each mea-surement point using the Laser-Doppler vibrom-eter, it was necessary to anchor the sensor head firmly and to irradiate each measurement point with the laser beam in the same direction as that of the defined response. Therefore, a device to fix the sensor head was newly developed in which the unit holding the sensor head could be moved along a curved rail, enabling the direction of the laser beam to be changed arbitrarily, as illustrated in Fig. 8, and to be set in a defined direction for each measurement point.
The first vibratory measurement was performed without the obturator prosthesis (NO), in a labo-ratory where the temperature and humidity were 25˚C and 70% respectively. The patient lay on a dental chair and placed his head on a pillow such that the X-Y plane was vertical to the floor. The pillow used in this study was made of urethane and had low counter-pressure properties. The plane of the round rail was parallel to the X-Y plane (Fig. 8).
Laser goggles (YL-210, Yamamoto Kogaku Co., Osaka, Japan) were worn and a retractor for the angle of the mouth was inserted. The patient was instructed not to bring the upper and lower teeth into contact. Reflective marks were placed on the measurement points to gain more sensitive re-sponse signals. The frequency range was set from 0 to 2000 Hz. The sensor head was set at the pre-scribed position and the laser beam was focused
Fig. 5 The defined coordinate axes.
Fig. 6 The response direction was represented by the angle θ, which was geometrically calculated by projec-tion of the measurements points onto the X-Y plane.
YX
Fig. 7 Measurement system diagram.
FFT AnalyzerCF-6400
Impact Hammer DYTRAN 5800-SL
Personal Computer Vectra VE
Laser-DopplerVibrometer
LV-1100
DAMPCAL
VIBRANT GEN
AMP
07_01_Murase.indd 153 08.5.2 8:19:16 PM
Murase et al., J Jpn Prosthodont Soc 52 : 150-159, 2008154
on the measurement point to gain the maximum response. The left central incisor was tapped 5 times for each measurement point in the direction parallel to the X-axis, while the sensor head was moved and adjusted to irradiate each measure-ment point with the laser beam one by one. The transfer function of each measurement point was obtained using the FFT analyzer from the summed average of 5 separate measurements. All transfer functions were transferred to Vibrant GEN. Using the technique reported by Iida et al 17 and Matsui et al 18, the curve-fitting frequency range was set at 400 Hz, which included the resonance peak in the middle, after which the curve-fitted transfer functions were calculated. The natural frequency was then obtained and modal shapes in the buc-colingual direction were computed.
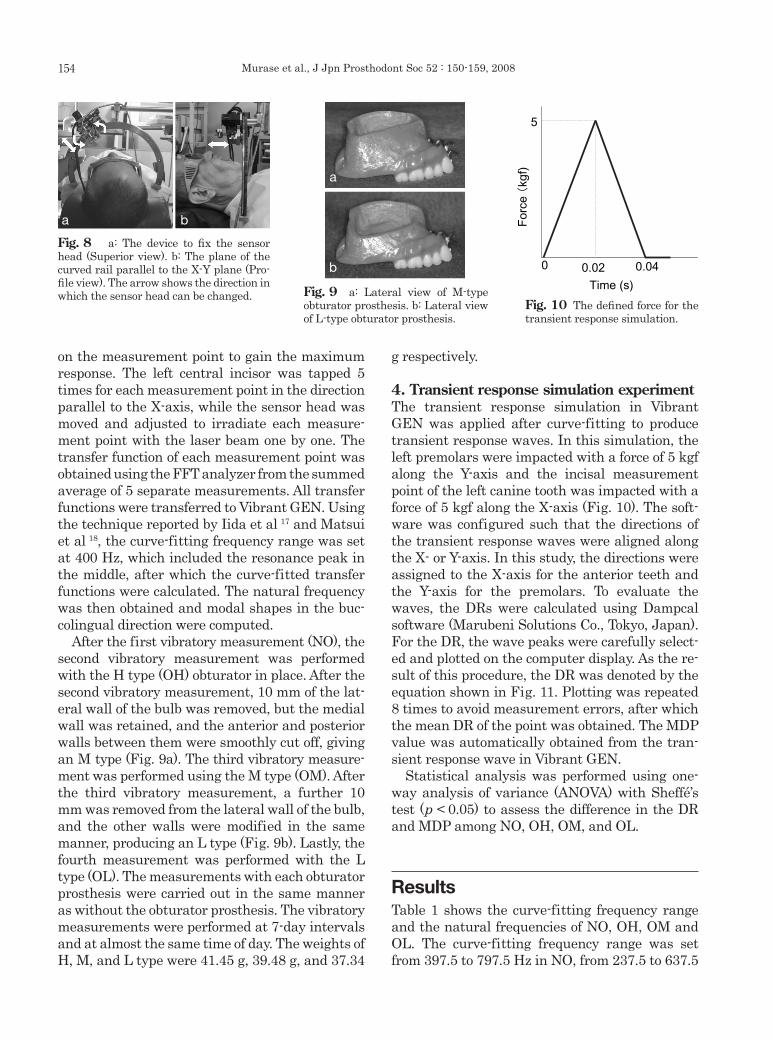
After the first vibratory measurement (NO), the second vibratory measurement was performed with the H type (OH) obturator in place. After the second vibratory measurement, 10 mm of the lat-eral wall of the bulb was removed, but the medial wall was retained, and the anterior and posterior walls between them were smoothly cut off, giving an M type (Fig. 9a). The third vibratory measure-ment was performed using the M type (OM). After the third vibratory measurement, a further 10 mm was removed from the lateral wall of the bulb, and the other walls were modified in the same manner, producing an L type (Fig. 9b). Lastly, the fourth measurement was performed with the L type (OL). The measurements with each obturator prosthesis were carried out in the same manner as without the obturator prosthesis. The vibratory measurements were performed at 7-day intervals and at almost the same time of day. The weights of H, M, and L type were 41.45 g, 39.48 g, and 37.34
g respectively.
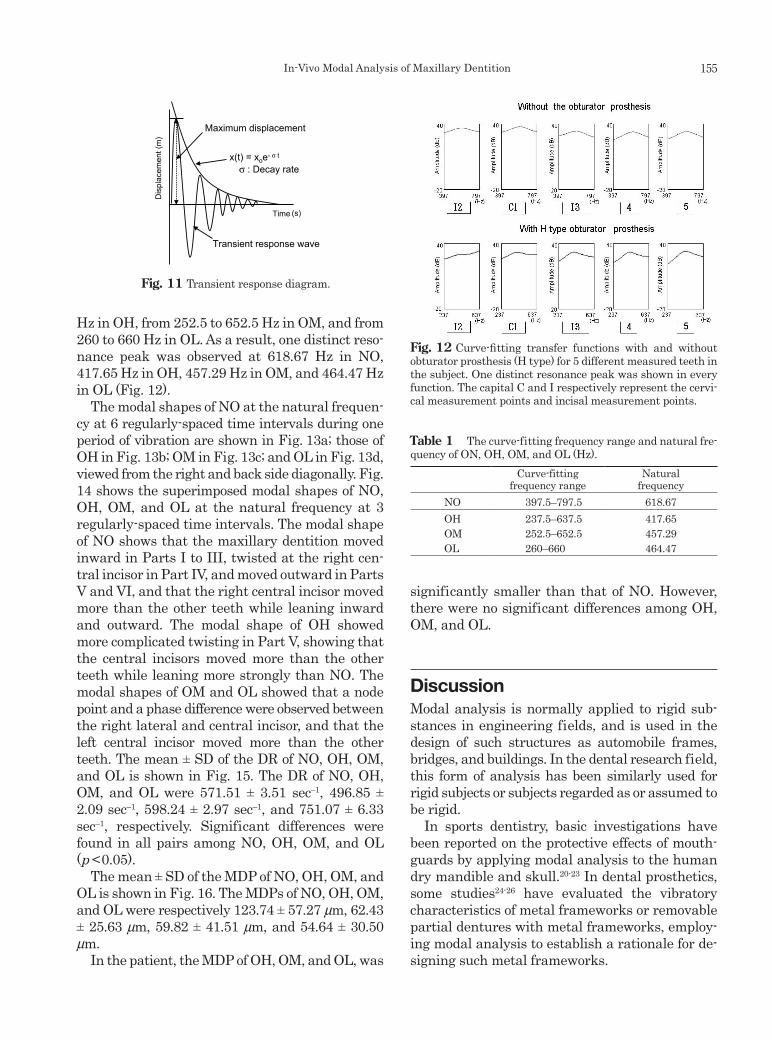
4. Transient response simulation experimentThe transient response simulation in Vibrant GEN was applied after curve-fitting to produce transient response waves. In this simulation, the left premolars were impacted with a force of 5 kgf along the Y-axis and the incisal measurement point of the left canine tooth was impacted with a force of 5 kgf along the X-axis (Fig. 10). The soft-ware was configured such that the directions of the transient response waves were aligned along the X- or Y-axis. In this study, the directions were assigned to the X-axis for the anterior teeth and the Y-axis for the premolars. To evaluate the waves, the DRs were calculated using Dampcal software (Marubeni Solutions Co., Tokyo, Japan). For the DR, the wave peaks were carefully select-ed and plotted on the computer display. As the re-sult of this procedure, the DR was denoted by the equation shown in Fig. 11. Plotting was repeated 8 times to avoid measurement errors, after which the mean DR of the point was obtained. The MDP value was automatically obtained from the tran-sient response wave in Vibrant GEN.
Statistical analysis was performed using one-way analysis of variance (ANOVA) with Sheffé’s test (p < 0.05) to assess the difference in the DR and MDP among NO, OH, OM, and OL.
ResultsTable 1 shows the curve-fitting frequency range and the natural frequencies of NO, OH, OM and OL. The curve-fitting frequency range was set from 397.5 to 797.5 Hz in NO, from 237.5 to 637.5
Fig. 10 The defined force for the transient response simulation.
0 0.04
5
Time (s)
Fig. 10
0.02
For
ce(kg
f)
Fig. 9 a: Lateral view of M-type obturator prosthesis. b: Lateral view of L-type obturator prosthesis.
a
b
Fig. 8 a: The device to fix the sensor head (Superior view). b: The plane of the curved rail parallel to the X-Y plane (Pro-file view). The arrow shows the direction in which the sensor head can be changed.
ba
07_01_Murase.indd 154 08.5.2 8:19:16 PM
In-Vivo Modal Analysis of Maxillary Dentition 155
Hz in OH, from 252.5 to 652.5 Hz in OM, and from 260 to 660 Hz in OL. As a result, one distinct reso-nance peak was observed at 618.67 Hz in NO, 417.65 Hz in OH, 457.29 Hz in OM, and 464.47 Hz in OL (Fig. 12).
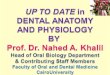
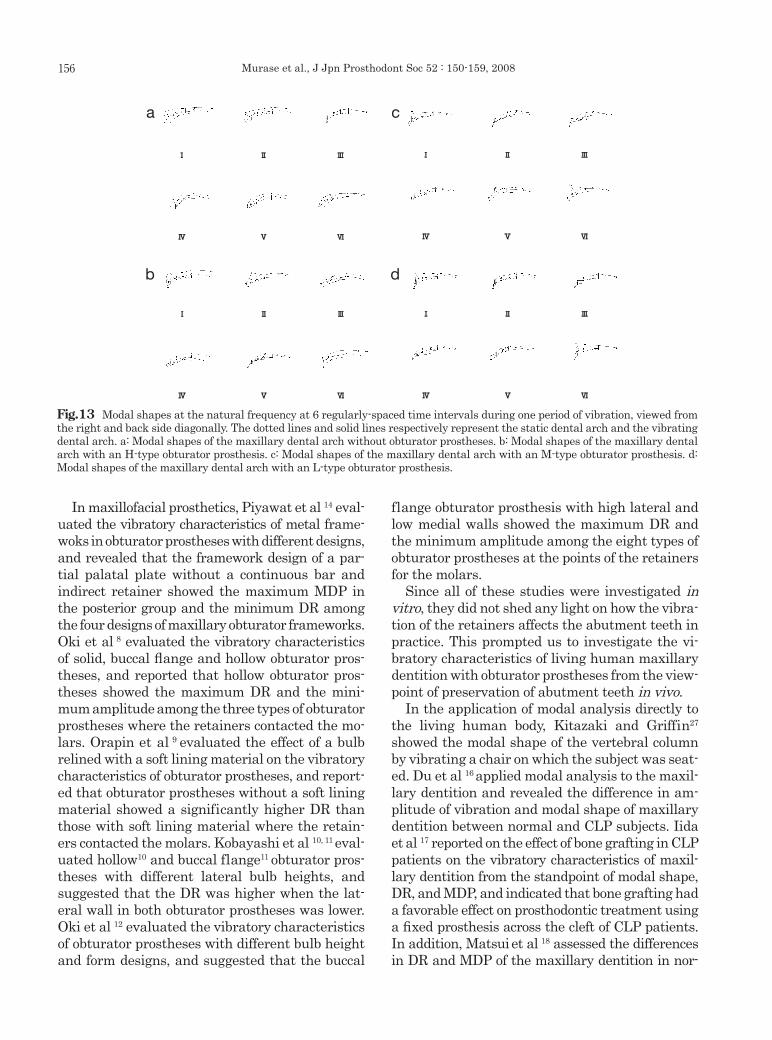
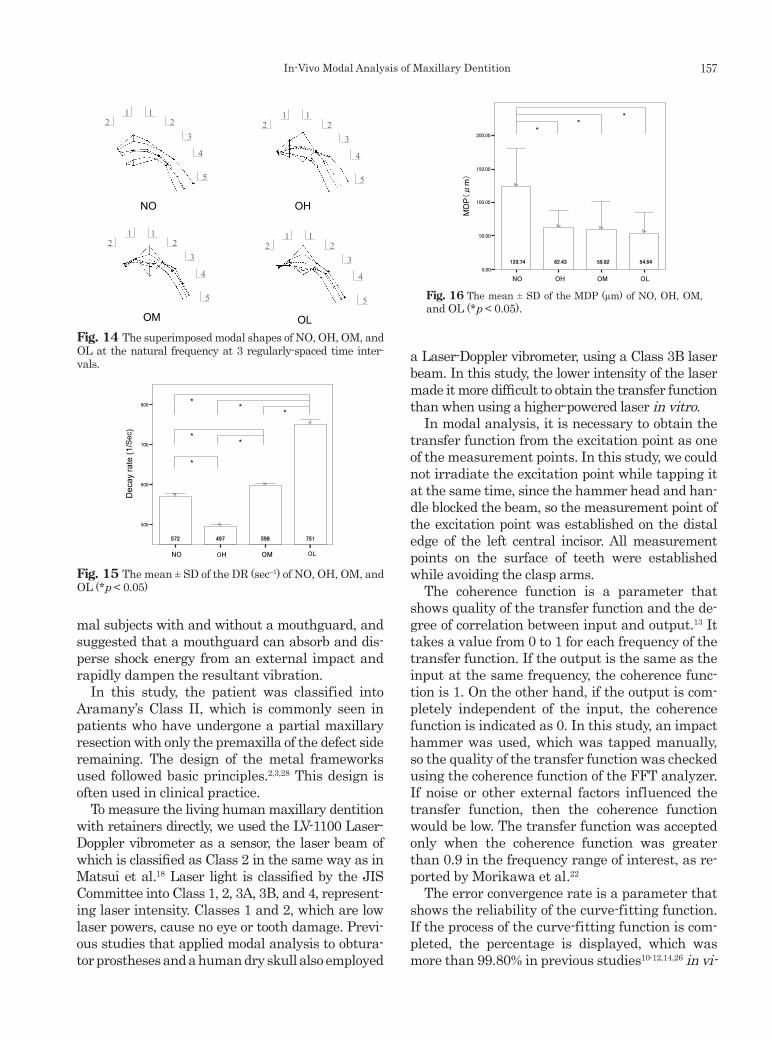
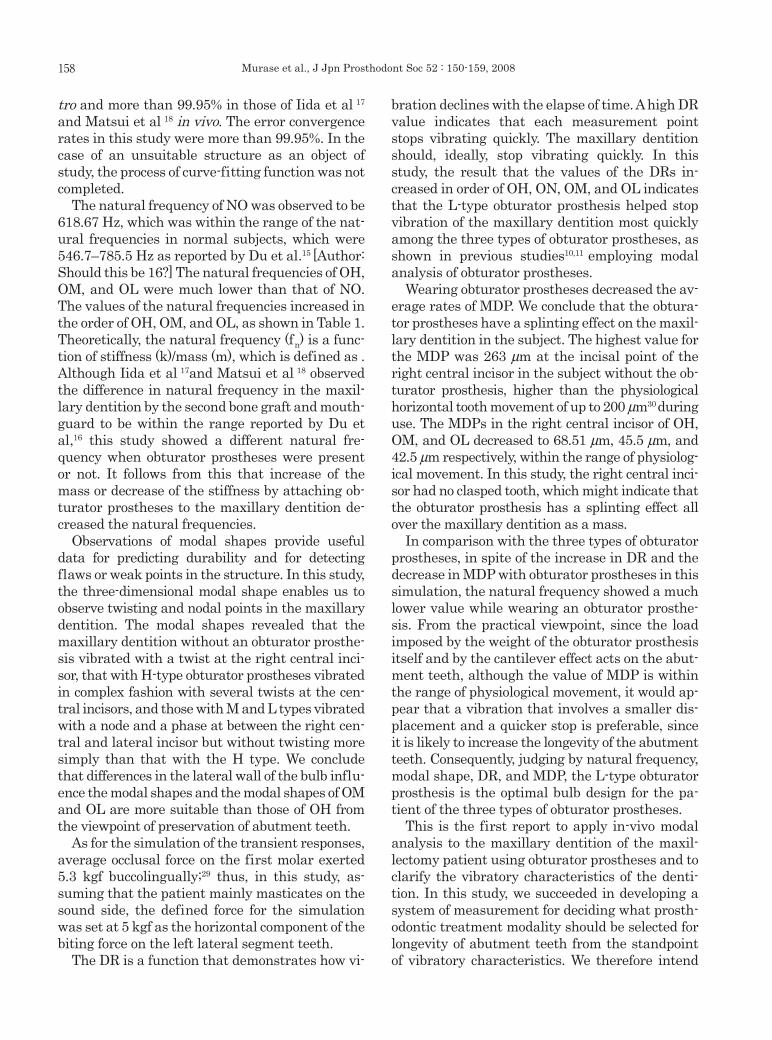
The modal shapes of NO at the natural frequen-cy at 6 regularly-spaced time intervals during one period of vibration are shown in Fig. 13a; those of OH in Fig. 13b; OM in Fig. 13c; and OL in Fig. 13d, viewed from the right and back side diagonally. Fig. 14 shows the superimposed modal shapes of NO, OH, OM, and OL at the natural frequency at 3 regularly-spaced time intervals. The modal shape of NO shows that the maxillary dentition moved inward in Parts I to III, twisted at the right cen-tral incisor in Part IV, and moved outward in Parts V and VI, and that the right central incisor moved more than the other teeth while leaning inward and outward. The modal shape of OH showed more complicated twisting in Part V, showing that the central incisors moved more than the other teeth while leaning more strongly than NO. The modal shapes of OM and OL showed that a node point and a phase difference were observed between the right lateral and central incisor, and that the left central incisor moved more than the other teeth. The mean ± SD of the DR of NO, OH, OM, and OL is shown in Fig. 15. The DR of NO, OH, OM, and OL were 571.51 ± 3.51 sec–1, 496.85 ± 2.09 sec–1, 598.24 ± 2.97 sec–1, and 751.07 ± 6.33 sec–1, respectively. Significant differences were found in all pairs among NO, OH, OM, and OL (p < 0.05).
The mean ± SD of the MDP of NO, OH, OM, and OL is shown in Fig. 16. The MDPs of NO, OH, OM, and OL were respectively 123.74 ± 57.27 µm, 62.43 ± 25.63 µm, 59.82 ± 41.51 µm, and 54.64 ± 30.50 µm.
In the patient, the MDP of OH, OM, and OL, was
significantly smaller than that of NO. However, there were no significant differences among OH, OM, and OL.
DiscussionModal analysis is normally applied to rigid sub-stances in engineering fields, and is used in the design of such structures as automobile frames, bridges, and buildings. In the dental research field, this form of analysis has been similarly used for rigid subjects or subjects regarded as or assumed to be rigid.
In sports dentistry, basic investigations have been reported on the protective effects of mouth-guards by applying modal analysis to the human dry mandible and skull.20-23 In dental prosthetics, some studies24-26 have evaluated the vibratory characteristics of metal frameworks or removable partial dentures with metal frameworks, employ-ing modal analysis to establish a rationale for de-signing such metal frameworks.
Fig. 11 Transient response diagram.
Time (s)
Maximum displacement
Dis
plac
emen
t (m
)
Transient response wave
x(t) = xoe- σ t
σ : Decay rate
Fig. 12 Curve-fitting transfer functions with and without obturator prosthesis (H type) for 5 different measured teeth in the subject. One distinct resonance peak was shown in every function. The capital C and I respectively represent the cervi-cal measurement points and incisal measurement points.
Table 1 The curve-fitting frequency range and natural fre-quency of ON, OH, OM, and OL (Hz).
Curve-fitting frequency range
Natural frequency
NO 397.5–797.5 618.67OH 237.5–637.5 417.65OM 252.5–652.5 457.29OL 260–660 464.47
07_01_Murase.indd 155 08.5.2 8:19:17 PM
Murase et al., J Jpn Prosthodont Soc 52 : 150-159, 2008156
In maxillofacial prosthetics, Piyawat et al 14 eval-uated the vibratory characteristics of metal frame-woks in obturator prostheses with different designs, and revealed that the framework design of a par-tial palatal plate without a continuous bar and indirect retainer showed the maximum MDP in the posterior group and the minimum DR among the four designs of maxillary obturator frameworks. Oki et al 8 evaluated the vibratory characteristics of solid, buccal flange and hollow obturator pros-theses, and reported that hollow obturator pros-theses showed the maximum DR and the mini-mum amplitude among the three types of obturator prostheses where the retainers contacted the mo-lars. Orapin et al 9 evaluated the effect of a bulb relined with a soft lining material on the vibratory characteristics of obturator prostheses, and report-ed that obturator prostheses without a soft lining material showed a significantly higher DR than those with soft lining material where the retain-ers contacted the molars. Kobayashi et al 10, 11 eval-uated hollow10 and buccal flange11 obturator pros-theses with different lateral bulb heights, and suggested that the DR was higher when the lat-eral wall in both obturator prostheses was lower. Oki et al 12 evaluated the vibratory characteristics of obturator prostheses with different bulb height and form designs, and suggested that the buccal
flange obturator prosthesis with high lateral and low medial walls showed the maximum DR and the minimum amplitude among the eight types of obturator prostheses at the points of the retainers for the molars.
Since all of these studies were investigated in vitro, they did not shed any light on how the vibra-tion of the retainers affects the abutment teeth in practice. This prompted us to investigate the vi-bratory characteristics of living human maxillary dentition with obturator prostheses from the view-point of preservation of abutment teeth in vivo.
In the application of modal analysis directly to the living human body, Kitazaki and Griffin27
showed the modal shape of the vertebral column by vibrating a chair on which the subject was seat-ed. Du et al 16 applied modal analysis to the maxil-lary dentition and revealed the difference in am-plitude of vibration and modal shape of maxillary dentition between normal and CLP subjects. Iida et al 17 reported on the effect of bone grafting in CLP patients on the vibratory characteristics of maxil-lary dentition from the standpoint of modal shape, DR, and MDP, and indicated that bone grafting had a favorable effect on prosthodontic treatment using a fixed prosthesis across the cleft of CLP patients. In addition, Matsui et al 18 assessed the differences in DR and MDP of the maxillary dentition in nor-
Fig.13 Modal shapes at the natural frequency at 6 regularly-spaced time intervals during one period of vibration, viewed from the right and back side diagonally. The dotted lines and solid lines respectively represent the static dental arch and the vibrating dental arch. a: Modal shapes of the maxillary dental arch without obturator prostheses. b: Modal shapes of the maxillary dental arch with an H-type obturator prosthesis. c: Modal shapes of the maxillary dental arch with an M-type obturator prosthesis. d: Modal shapes of the maxillary dental arch with an L-type obturator prosthesis.
Fig.13b
b
Fig.13c
c
Fig.13d
d
Fig.13a
a
07_01_Murase.indd 156 08.5.2 8:19:18 PM
In-Vivo Modal Analysis of Maxillary Dentition 157
mal subjects with and without a mouthguard, and suggested that a mouthguard can absorb and dis-perse shock energy from an external impact and rapidly dampen the resultant vibration.
In this study, the patient was classified into Aramany’s Class II, which is commonly seen in patients who have undergone a partial maxillary resection with only the premaxilla of the defect side remaining. The design of the metal frameworks used followed basic principles.2,3,28 This design is often used in clinical practice.
To measure the living human maxillary dentition with retainers directly, we used the LV-1100 Laser-Doppler vibrometer as a sensor, the laser beam of which is classified as Class 2 in the same way as in Matsui et al.18 Laser light is classified by the JIS Committee into Class 1, 2, 3A, 3B, and 4, represent-ing laser intensity. Classes 1 and 2, which are low laser powers, cause no eye or tooth damage. Previ-ous studies that applied modal analysis to obtura-tor prostheses and a human dry skull also employed
a Laser-Doppler vibrometer, using a Class 3B laser beam. In this study, the lower intensity of the laser made it more difficult to obtain the transfer function than when using a higher-powered laser in vitro.
In modal analysis, it is necessary to obtain the transfer function from the excitation point as one of the measurement points. In this study, we could not irradiate the excitation point while tapping it at the same time, since the hammer head and han-dle blocked the beam, so the measurement point of the excitation point was established on the distal edge of the left central incisor. All measurement points on the surface of teeth were established while avoiding the clasp arms.
The coherence function is a parameter that shows quality of the transfer function and the de-gree of correlation between input and output.13 It takes a value from 0 to 1 for each frequency of the transfer function. If the output is the same as the input at the same frequency, the coherence func-tion is 1. On the other hand, if the output is com-pletely independent of the input, the coherence function is indicated as 0. In this study, an impact hammer was used, which was tapped manually, so the quality of the transfer function was checked using the coherence function of the FFT analyzer. If noise or other external factors influenced the transfer function, then the coherence function would be low. The transfer function was accepted only when the coherence function was greater than 0.9 in the frequency range of interest, as re-ported by Morikawa et al.22
The error convergence rate is a parameter that shows the reliability of the curve-fitting function. If the process of the curve-fitting function is com-pleted, the percentage is displayed, which was more than 99.80% in previous studies10-12,14,26 in vi-
Fig. 14 The superimposed modal shapes of NO, OH, OM, and OL at the natural frequency at 3 regularly-spaced time inter-vals.
21 1
23
4
5
21 1
23
4
5
21 1
23
4
5
21 1
23
4
5
Fig.14
NO OH
OM OL
NO OH OM OL
500
600
700
800
572 497 598 751
*
**
*
*
*
Dec
ay r
ate
(1/S
ec)
Fig. 15
Fig. 15 The mean ± SD of the DR (sec–1) of NO, OH, OM, and OL (*p < 0.05)
Fig. 16
**
*
LOHOON
0.00
50.00
100.00
150.00
200.00
123.74 62.43 59.82 54.64
MD
P(μ
m)
OM
Fig. 16 The mean ± SD of the MDP (µm) of NO, OH, OM, and OL (*p < 0.05).
07_01_Murase.indd 157 08.5.2 8:19:19 PM
Murase et al., J Jpn Prosthodont Soc 52 : 150-159, 2008158
tro and more than 99.95% in those of Iida et al 17 and Matsui et al 18 in vivo. The error convergence rates in this study were more than 99.95%. In the case of an unsuitable structure as an object of study, the process of curve-fitting function was not completed.
The natural frequency of NO was observed to be 618.67 Hz, which was within the range of the nat-ural frequencies in normal subjects, which were 546.7–785.5 Hz as reported by Du et al.15 [Author: Should this be 16?] The natural frequencies of OH, OM, and OL were much lower than that of NO. The values of the natural frequencies increased in the order of OH, OM, and OL, as shown in Table 1. Theoretically, the natural frequency (fn) is a func-tion of stiffness (k)/mass (m), which is defined as . Although Iida et al 17and Matsui et al 18 observed the difference in natural frequency in the maxil-lary dentition by the second bone graft and mouth-guard to be within the range reported by Du et al,16 this study showed a different natural fre-quency when obturator prostheses were present or not. It follows from this that increase of the mass or decrease of the stiffness by attaching ob-turator prostheses to the maxillary dentition de-creased the natural frequencies.
Observations of modal shapes provide useful data for predicting durability and for detecting flaws or weak points in the structure. In this study, the three-dimensional modal shape enables us to observe twisting and nodal points in the maxillary dentition. The modal shapes revealed that the maxillary dentition without an obturator prosthe-sis vibrated with a twist at the right central inci-sor, that with H-type obturator prostheses vibrated in complex fashion with several twists at the cen-tral incisors, and those with M and L types vibrated with a node and a phase at between the right cen-tral and lateral incisor but without twisting more simply than that with the H type. We conclude that differences in the lateral wall of the bulb influ-ence the modal shapes and the modal shapes of OM and OL are more suitable than those of OH from the viewpoint of preservation of abutment teeth.
As for the simulation of the transient responses, average occlusal force on the first molar exerted 5.3 kgf buccolingually;29 thus, in this study, as-suming that the patient mainly masticates on the sound side, the defined force for the simulation was set at 5 kgf as the horizontal component of the biting force on the left lateral segment teeth.
The DR is a function that demonstrates how vi-
bration declines with the elapse of time. A high DR value indicates that each measurement point stops vibrating quickly. The maxillary dentition should, ideally, stop vibrating quickly. In this study, the result that the values of the DRs in-creased in order of OH, ON, OM, and OL indicates that the L-type obturator prosthesis helped stop vibration of the maxillary dentition most quickly among the three types of obturator prostheses, as shown in previous studies10,11 employing modal analysis of obturator prostheses.
Wearing obturator prostheses decreased the av-erage rates of MDP. We conclude that the obtura-tor prostheses have a splinting effect on the maxil-lary dentition in the subject. The highest value for the MDP was 263 µm at the incisal point of the right central incisor in the subject without the ob-turator prosthesis, higher than the physiological horizontal tooth movement of up to 200 µm30 during use. The MDPs in the right central incisor of OH, OM, and OL decreased to 68.51 µm, 45.5 µm, and 42.5 µm respectively, within the range of physiolog-ical movement. In this study, the right central inci-sor had no clasped tooth, which might indicate that the obturator prosthesis has a splinting effect all over the maxillary dentition as a mass.
In comparison with the three types of obturator prostheses, in spite of the increase in DR and the decrease in MDP with obturator prostheses in this simulation, the natural frequency showed a much lower value while wearing an obturator prosthe-sis. From the practical viewpoint, since the load imposed by the weight of the obturator prosthesis itself and by the cantilever effect acts on the abut-ment teeth, although the value of MDP is within the range of physiological movement, it would ap-pear that a vibration that involves a smaller dis-placement and a quicker stop is preferable, since it is likely to increase the longevity of the abutment teeth. Consequently, judging by natural frequency, modal shape, DR, and MDP, the L-type obturator prosthesis is the optimal bulb design for the pa-tient of the three types of obturator prostheses.
This is the first report to apply in-vivo modal analysis to the maxillary dentition of the maxil-lectomy patient using obturator prostheses and to clarify the vibratory characteristics of the denti-tion. In this study, we succeeded in developing a system of measurement for deciding what prosth-odontic treatment modality should be selected for longevity of abutment teeth from the standpoint of vibratory characteristics. We therefore intend
07_01_Murase.indd 158 08.5.2 8:19:19 PM

In-Vivo Modal Analysis of Maxillary Dentition 159
to carry out further investigations and establish a universal rule for the fabrication of obturator pros-theses and removable partial dentures.
Conclusion It is concluded that the L-type obturator prosthe-sis is the preferable bulb design for the maxillec-tomy patient of the three types of obturatar pros-theses that are different in lateral wall height of the bulb by direct application of modal analysis to the living maxillary dentition of the patient.
References 1. Coffin F. Cancer and the dental surgeon. Br Dent J
1964; 116: 243-253. 2. Beumer J, Curtis TA, Firtell DN. Maxillofacial reha-
bilitation, prosthodontic and surgical considerations. Author: Location?:CV Mosby; 1979, p.188-243.
3. Aramany MA. Basic principles of obturator design for partially edentulous patients. Part II: Design principles. J Prosthet Dent 1978; 40: 656-662.
4. Brown KE. Clinical considerations improving obtu-rator treatment. J Prosthet Dent 1970; 24: 461-466.
5. Brown KE. Peripheral consideration in improving obturator retention. J Prosthet Dent 1968; 20: 176-181.
6. Desjardins RP. Obturator prosthesis design for ac-quired maxillary defects. J Prosthet Dent 1978; 39: 424-435.
7. Sharry JJ. Extensions of partial denture treatment. Dent Clin North Am 1962; 821-835.
8. Oki M, Taniguchi H, Ohyama T. Evaluation of ob-turator prostheses using vibration analysis. J Med Dent Sci 1999; 46: 21-30.
9. Orapin K, Oki M, Taniguchi H. The vibratory prop-erties of an obturator prosthesis with a soft lining material. J Med Dent Sci 2000; 47: 1-10.
10. Kobayashi M, Oki M, Ozawa S et al. Vibration analysis of obturator prostheses with different bulb height designs. J Med Dent Sci 2002; 49: 121-128.
11. Kobayashi M, Iida T, Taniguchi H. Vibration analy-sis of buccal flange obturator prostheses with dif-ferent bulb height designs. J Jpn Maxillofacial Pros-thet 2003; 26: 12-19. (in Japanese, English abstract)
12. Oki M, Iida T, Mukohyama H et al. The vibratory characteristics of obturators with different bulb height and form designs. J Oral Rehabilitaiton 2006; 33: 43–51.
13. Nagamatsu A. Introduction to modal analysis,. [Author: Location?]Corona, Inc; 1993, p. 95. (in Japanese)
14. Piyawat P, Taniguchi H, Ohyama T. The vibration
analysis of obturator framework designs. J Med Dent Sci 2000; 47: 221-231.
15. Inman DJ. Engineering vibration. [Author: Location?]: Prentice Hall International, Inc.; 1996, p.364–393.
16. Du L, Suzuki R, Taniguchi H et al. Application of modal analysis to human subjects: comparison of healthy subjects and cleft lip and palate subjects. J Med Dent Sci 1998; 45: 39-49.
17. Iida T, Mukoyama H, Suzuki R et al. Modal analysis of maxillary dentition in cleft lip and palate patients before and after bone grafting. J Med Dent Sci 2001; 48: 87-94.
18. Matsui R, Yamanaka T, Iida T et al. Modal analysis of maxillary dentition in human subjects with and without a mouthguard. J Sports Dent 2006; 10: 6-15.
19. Japanese Industrial Standards Committee hand-book safety-I, [Author: Location?]: Japanese Stan-dards Association; 2005, p.16-17. (in Japanese)
20. Hasegawa Y. Fundamental study on effects of dif-ferent forms of mouthguards on modal shape and damping ratio of human dry mandible. J Stomatol Soc Jpn 1994; 61: 309-328. (in Japanese, English abstract)
21. Ou M, Taniguchi H, Ohyama T. Analysis on decay rate of vibration following impact to human dry skull with and without mouthguards. Bull Tokyo Med Dent Univ 1996; 43: 13-24.
22. Morikawa M, Taniguchi H, Ohyama T. Evaluation of athletic mouthguard through vibration test on maxillary teeth of human dry skull. J Med Dent Sci 1998; 45: 9-18.
23. Yamanaka T, Ueno T, Oki M et al. Study on the effects of shortening the distal end of a mouthguard using modal analysis. J Med Dent Sci 2002; 49: 129-133.
24. Arkdornnukit M, Taniguchi H, Ohyama T. Rigidity of three different types of mandibular major con-nector through vibratory observations. Int J Prosth-odont 2001; 14: 510–516.
25. Inoue T, Oki M, Phankosol P, Ohyama T et al. Vibra-tion analysis of maxillary removable partial den-ture frameworks. J Oral Rehabil 2002; 29: 341-349.
26. Matsumoto N, Taniguchi H, Ohyama T. Vibration analysis of maxillary removable denture using three types of major connectors. J Stomatol Soc Jpn 2003; 70: 104-113. (in Japanese, English abstract)
27. Kitazaki S, Griffin MJ. Resonance behavior of the seated human body and effects of posture. J Bio-mech 1998; 31: 143-149.
28. Parr GR, Tharp GE, Rahn AO. Prosthodontic prin-ciples in the framework design of maxillary obtura-tor prostheses. J Prosthet Dent 1989; 62: 201-212.
29. Morikawa A. Investigation of occlusal force on low-er first molar in function. J Stomatol Soc Jpn 1994; 61: 54-78. (in Japanese, English abstract)
30. Grant DA, Stern IB, Listgarter MA. Periodontics, 6 th ed., Saint Louis: Mosby Co; 1988, p.551.
07_01_Murase.indd 159 08.5.2 8:19:19 PM