Embed Size (px)
Citation preview

Improving Frequency and Proficiency of Breast Self-Examination:Effectiveness of an Education Program
JOYCE A. MAMON, PHD, AND JANE G. ZAPKA, SCD
Abstract: A randomized trial to improve breast self-examination(BSE) performance among college-age women was developed andresults evaluated at a large public university. The major interventionwas a BSE group education session conducted in classroom andworkshop settings. The pre-intervention and six-months-after ex-perimental-control comparisons show that: current performance ofBSE increased by 26 per cent, bi-monthly or more often BSEperformance increased by 29 per cent, and performance proficiencyimproved by 22 per cent. A change index, adjusting for each group'slevel on these three measures at pre-intervention, showed higherlevels of change; 57 per cent, 36 per cent, and 28 per cent,respectively. A significantly larger proportion of women in the
Introduction
Breast cancer is a major health concern, as it remainsthe most common type of cancer among women, accountingfor 26 per cent of all cancers in women.' Breast self-examination (BSE) has been widely promoted as a methodfor early breast cancer detection; the National Cancer Insti-tute (NCI) and the American Cancer Society (ACS) haveconsistently recommended that women perform monthlyBSE in addition to utilizing other detection methods.2 Al-though the controversy continues regarding the efficacy ofBSE in early diagnosis,3 it is particularly attractive from acost perspective for community-wide application. Despitepromotion of BSE as an appropriate supplement to routineclinical palpation, current data indicate that BSE perform-ance is low. Only 35 per cent of a random national sample ofwomen perform BSE on a routine basis4 and even fewerperform BSE competently, with proficiency estimates rang-ing from 9 per cent to 57 per cent.5-'3
To improve BSE performance and overcome many ofthe problems in previous BSE education research, a BSEprogram was developed, implemented, and evaluated forwomen in the college community. College women wereselected as a target population for a randomized trial becauseof the commitment of schools to help achieve the long-termhealth goals of the nation, because the college settingrepresents access to a large number of women,* and becauseone-quarter of cancers are found in women younger than age50.15
*There are approximately six million women enrolled in junior and four-year institutions of higher education, 45 per cent are women 18-19 years old,30 per cent are 20-21 years old, 15 per cent are 22-24 years old, and 16 percent are between 25 and 34 years of age.'4
Address reprint requests to Joyce A. Mamon, PhD, Senior ResearchAssociate, Health Services Research and Development Center, Johns Hop-kins University, School of Hygiene and Public Health, 624 N. Broadway,Baltimore, MD 21205. Dr. Mamon is also Assistant Professor, Department ofBehavioral Science and Health Education; Dr. Zapka is Associate Professor,Health Administration Program, Division of Public Health, University ofMassachusetts, Amherst, and Faculty Associate, JHUSHPH. This paper,submitted to the Journal June 18, 1984, was revised and accepted forpublication January 8, 1985.
C 1985 American Journal of Public Health 0090-0036/85$1.50
experimental group discussed BSE with others than women in thecontrol groups. The "talked to" mothers, compared to the "nottalked to" mothers performed BSE more regularly, in more posi-tions, and spent more time on the examination.
The results from this study suggest that properly targetededucational programs can significantly improve early detectionbehaviors in women. In addition, the evaluation protocol definedproficiency measures and validated measurement tools. Subsequentstudies need to examine the relation of proficiency measures todetection of abnormality and subsequent effect on morbidity andmortality, so that the debate about BSE efficacy can be scientificallyaddressed. (Am J Public Health 1985; 75:618-624.)
Program DescriptionStudy Subjects
The target population was the 12,500 undergraduate andgraduate females attending a large public east coast universi-ty during academic years 1980-81 and 1981-82. A total of1,682 women participated in the randomized trial. Themedian age of the participants was 21 years, 86 per cent wereWhite, and 93 per cent were never married. Average lengthof enrollment at the university was 1.5 years.Needs Assessment, Program Objectives, Educational Strategies
An education needs assessment survey of a stratifiedrandom sample of 600 females at this university was con-ducted six months prior to the intervention program.'6l'7 Thebehavioral and educational objectives of the program weredefined using the findings from this survey, along withreview of previous application of relevant theories andconceptual models, and basic practice principles.
The behavioral objectives were to:* increase the number of women initiating and continu-
ing correct and regular practice of BSE;* increase the proficiency of BSE performance amongwomen who practice BSE regularly;
* increase the regular and correct practice of BSEamong women who sporadically practice BSE;
* promote active discussion about BSE wih significantothers, particularly mothers, so as to promote BSEpractice in that population; and
* promote appropriate utilization of professional serv-ices (periodic screening, report of suspicious breastchanges).
The educational objectives were to:* provide information to participants about risk factors
for breast cancer, the diagnostic procedures and treat-ment modalities for breast cancer, and the importanceof BSE for the early detection of breast cancer;
* teach the BSE skill, with special attention to posi-tions, motions and techniques, frequency and timing,and recognition of symptoms; and
* explore psychosocial factors and barriers related tothe subject of breast cancer and the performance ofbreast self-examination, such as fears, denial, embar-rassment, perceptions of risk, and confidence in thetechnique and in one's ability to perform it correctly.
AJPH June 1985, Vol. 75, No. 6618

IMPROVING BSE FREQUENCY, PROFICIENCY
Specification of the behavioral and educational objec-tives determined the strategies, content areas, and teachingmethods to be emphasized in the BSE program.'6"7 Theprimary intervention was a group educational session con-ducted by trained peer educators.** The group session,lasting 1 to 1½/2 hours, was selected as the main strategybecause it permitted access to large numbers of women withenough time to emphasize skill development via multipleteaching techniques, as well as deal with the cognitive andaffective components known to be related to breast cancerdetection behaviors. Group sessions also promoted discus-sion between peers, an important vehicle for enhancingsocial support for BSE performance.
The group sessions were conducted in two settings:classrooms and workshops for organized groups. The latterincluded sororities, dormitories, and women's organizationswhich requested a BSE program. Sessions in classes reacheda more captive audience, one for which a control group wasfeasible. Women from randomly selected classes were ex-pected to be different from those who were motivated tovoluntarily attend a workshop, thus providing an opportuni-ty to investigate selection bias. Although men were in theclasses and therefore exposed to the intervention, the pro-ject evaluation scheme did not include them.
To enhance frequency/regularity of performance, skilldevelopment included a discussion with the participants ofthe need for routine performance of BSE and strategies forreminding oneself to perform BSE monthly. For improve-ment in proficiency of BSE performance, skill developmentincluded an explanation of the specific steps necessary forperforming a competent breast self-examination, viewing asegment of a cancer film on how to perform BSE (to enhanceidentification, the film chosen had a woman about the sameage as that of the target population), a demonstration by thepeer facilitator to review the technique, and opportunitiesfor participants to practice/demonstrate techniques (e.g., onbreast models, press back of hand to be able to exemplifytactile skills). These strategies were a blend of didactic andparticipatory approaches; modeling (via a peer facilitator)and group sessions are known to be effective in developingbehaviors and enhancing motivations, whereas films andmore passive strategies (e.g., flip charts, pamphlets) arehelpful in reinforcing the participatory learning. To permitadditional learning and review for conducting a proficientexamination, two cancer pamphlets were distributed as wellas a specially developed wallet-sized peel-back sticker thatoutlined the BSE steps to be conducted in each of the threepositions and the appropriate time of the month to performBSE. The sticker was designed not only for improving recallof the correct BSE technique but as a cue-to-action since itcould be positioned permanently in a place where the womanwas likely to perform her self-examination.
The objective of increasing discussion regarding BSEwith significant others was addressed by peer group discus-sion during the workshop so that the female participantswould become comfortable talking with other women aboutBSE, particularly women in their support network. Also,known risk factors were presented and discussed; this partof the session was designed not only to provide cognitiveinformation on risk factors but also to encourage participantsto talk with older women, particularly mothers, who are athigher risk of breast cancer. Participants were given two
**Educational protocol available from authors.
peel-back stickers and encouraged to pass one on to arelative or friend.
Appropriate utilization of professional services waspromoted by noting that "normalcy" of breast tissue neededto be established by an initial clinical examination. If awoman had not had a clinical breast examination in theprevious year or was unsure of normalcy, it was recom-mended that she obtain a clinical palpation to establish anappropriate baseline for herself. Then, whenever a changewas noticed use of services was recommended for medicalconfirmation. To avoid unnecessary stress, the fact that 80per cent of all lumps are not cancerous was emphasized.
Flip charts were developed to reinforce cognitive infor-mation (risk factors, methods of diagnosis and treatment,reasons for a baseline clinical examination), skill develop-ment (steps for proficiency), and psychological issues (fears,attitudes, perceptions of risk, social support). A summaryhandout reinforced key points and assisted with recall andpractice after the session.
In addition to the group education sessions, a universi-ty-wide information campaign was designed and implement-ed to increase awareness and to provide reinforcement. Thecampaign consisted of newspaper ads and articles, radiospots, and extensive use of posters for information andadvertising of workshops.
Evaluation Research DesignTarget Groups, Research Schedule, Response Rates
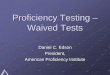
Figure 1 delineates the target groups, the interventionand observation schedule, final sample sizes, and the re-sponse rates at six-month follow-up. The classroom inter-vention groups were randomly assigned*** to one of foursubgroups. Experimental Groups E1 and E2 received theeducational program; in addition, Experimental Group E1completed a written pretest questionnaire similar in contentto the baseline diagnostic survey.'6 The two control groupsdid not receive the educational program; Control Group C1completed a written pretest questionnaire. Since the womenattending workshops WI and W2 were self-selected, theywere not randomized into experimental and control groups:however, women in Group W, completed a pretest question-naire and received the intervention program, women inGroup W2 received the educational program without com-pleting the pretest. All workshop participants received thesix-month post-test questionnaire.
Since one of the objectives of this project was topromote active discussion about BSE with significant others(particularly mothers) so as to improve BSE practice in thatpopulation, a convenience sample of mothers whose daugh-ters were exposed to the educational program was inter-viewed by telephone regarding their BSE practices.
Each student participant was mailed a post-test ques-tionnaire six months after the initial participation date. Afterone letter and a telephone follow-up, the response rate was79.4 per cent. Given the high mobility of a student popula-
***To achieve comparability between the four classroom subgroups,disciplines were put into clusters (e.g., for history classes, History 101comprised one cluster, a set of second-year history classes comprised anothercluster.) Once a cluster had been defined, professors were contacted forparticipation in the study. When professors of four classes in the cluster hadagreed to participate, the classes in that cluster were then randomly assignedto one of the four classroom groups. In all, there were 20 clusters, coveringthe spectrum of disciplines (e.g., social sciences, natural sciences, health,physical education, etc.) and class levels.
AJPH June 1985, Vol. 75, No. 6619

MAMON AND ZAPKA
FIGURE 1-Study Design, Intervention and Observation Schedules, Sample Sizes and Foilow-up Response RatesIntervention and Control Groups
Group
Experimental Group I (E,)
Experimental Group 2 (E2)
Control Group I (C,)
Control Group 2 (C2)
BaselinePretest
Written Survey
0
6 MonthPost-Intake
Intervention Written Survey
x
x
0
0
0
0
0
Numberof
SubjectsAccrued
Follow-UpResponseRate %
342 83
328 78
342 76
340 80
Experimental Group 3 (W,)
Experimental Group 4 (W2)
0 x
x
Experimental Group(daughters reported discussion)
Control Group(daughters did not reportdiscussion)
0
0
0
0
181 76
149 91
96 NA*
101 NA
tion, this response rate was considered good. There was novariation between classrooms and workshops significant inthese response rates; respondent/non-respondent analysis ofbaseline data showed no variations in sociodemographiccharacteristics or performance of the BSE behavioral mea-sures.
Measurement and AnalysisThe structured written questionnaire included items
related to the program's behavioral objectives. Measures ofnumerous antecedent factors including knowledge, atti-tudes, and health history variables were also collected.
Proficiency of BSE performance was measured bywhether a woman performs BSE in more than one positionand by a 19-item proficiency index score derived from NCIand ACS recommended criteria regarded the correct tech-nique for BSE. Items on BSE performance were structuredopen-ended questions with standardized probes for positionand arm placement. These structured questions were adapt-ed from the 1979 National Survey on Breast Cancer.t Eachof these proficiency criteria was scored as being done (1) ornot done (0). Each criterion step was weighted according tothe level of sensitivity and specificity found in the experi-mentals and controls who participated in a validation sub-study. This involved a subsample of study participantsdemonstrating their usual BSE to a trained observer whoscored the individual according to the same criteria used toscore the self-reported written responses.'8
Comparison of study groups for each of these behaviorswithin the pre-intervention and six-month follow-up timeperiods were analyzed as well as changes over time in each
tThe structured items in the National Cancer Institute survey were asfollows: 1) "Please tell me specifically, what steps you use when you examineyour breasts"; 2) "Is there any special position you assume?"; 3) "Is thereanything else you do?". Based upon pilot testing this last question wasmodified to "Are your arms in any special position?"
major dependent variable. An effectiveness index (EI)tt wasused to assess the degree of change between two timeperiods adjusted according to the group's potential forchange. '9
ResultsBaseline
Comparison at baseline between the two classroomstudy groups El and Cl, showed no differences in age, race,marital status, or family income. For breast cancer detectionbehavior among those currently performing BSE, a higherproportion of the controls (68 per cent) had performed BSEthan experimentals (56 per cent). Since the direction of thisdiscrepancy is in favor of the control group, differencesbetween experimentals and controls observed at follow-upfor this measure will be a conservative estimate of the effectof the program.
There were no differences between the workshop groupWI and experimental classroom group El in baseline levels ofperformance proficiency, number of positions, or havingobtained a clinical breast examination in the past year.However, a lower proportion of the participants in theworkshops as compared to the classroom population werefound to practice BSE currently as well as routinely (definedas bimonthly to monthly practice). Also, the workshopparticipants tended to be younger, had a higher socioeco-nomic status, and included more unmarried and Whitewomen. Given that women living in dormitories and soror-ities are more likely to be younger and never married, thesefindings are not surprising. Based upon these results theworkshop groups were analyzed separately from the class-room groups.
ttEI = (P2 - P)/100 - PI x 100: the numerator represents actual changebetween pre- and post-intervention; the denominator represents potential forchange at pre-intervention. P, = baseline, P2 = 6 month follow-up pastintervention.
AJPH June 1985, Vol. 75, No. 6
Group SessionCLASSROOMSpring, 1981
RandomizedClasses
RandomizedWorkshops
Group SessionWORKSHOPSFall-Spring,1980-1981
ParticipantMothersFollow-up(Mothers ofExperimentalGroups 1-4)Spring, 1982
Convenience
*Not applicable
620

IMPROVING BSE FREQUENCY, PROFICIENCY
PretestAnalyses were conducted to measure the effect of the
pretest on the behavioral outcome measures at six monthspost-intake. No differences were found in the two experi-mental classroom groups (El and E2), indicating that thepretest instrument did not affect the outcome behaviors ofthe experimental classroom group El. In contrast, compari-sons between the two classroom control groups (Cl and C2)on the outcome measures suggest that the pretest may haveincreased regularity of BSE performance and promptedsome discussion with others regarding BSE. However, thepretest does not appear to have had any effect on perform-ance proficiency, care-seeking behavior, or discussion ofBSE with a relative. The pretest appears also to have had noeffect on the workshop group (WI), with the possible excep-tion of discussion of BSE with others.ttt
Given that the pretest had no significant effect whengiven in conjunction with the educational program interven-tion, the El and E2 experimental classroom groups werecombined in subsequent analyses, and the WI and W2workshop groups were also combined. Since the pretestappears to have influenced frequency of performance in theabsence of an intervention program, classroom controlgroups (C, and C2) were analyzed separately. Based on thesedata, the C2 group is viewed as the reference control group.All other study groups were compared to the C2 group.Program Effectiveness
Table 1 presents frequency of BSE performance at sixmonth follow-up. Both classroom- and workshop experimen-tal groups were more likely to have performed BSE withinthe past six months and bimonthly than the control group(without pretest). Differences in monthly BSE performancewere less marked.
The proficiency of study participants reporting doingBSE in all experimental groups was superior to that of thecontrol group C2 (Table 2), in terms of the number ofpositions (two or more) and the average BSE proficiencyscore. An alternative analysis, where the proficiency scorewas dichotomized at the median (.9), indicated the samepattern as the comparison of mean scores (last column Table2).
To determine the full impact of the educational programon each of the study groups, comparisons were made ofBSEproficiency for all individuals who responded to the six-month follow-up (Table 3). In other words, people who
reported never performing BSE were also included andassigned a score of zero. The same pattern of substantialprogram effect was observed.
Table 4 indicates that both experimental groups (El andWI) and the control group (C1) participants who received thepretest were more apt to report discussion with others thancontrol group participants who did not receive the pretest. Alarger proportion of the experimental workshop participantsreported such discussions with their mothers. The "talkedto" mothers, compared to the "not talked to" mothersperformed BSE more regularly, in more positions, and spentmore time on the examination.Changes Between Pre- and Post-Intervention
Table 5 reports the per cent change between pre-intervention and six-month post-intervention as well as theeffectiveness index (EI). Data on absolute change, as well asdata adjusted by potential for change, indicate that BSEperformance by the experimental groups, as measured by allfrequency and proficiency measures, were better than that ofeither control group.
Class and workshop experimental group participantsachieved over 50 per cent of the potential change (as definedby the denominator of the effectiveness index, 100-PI), intheir current performance of BSE. The relative change overtime in bimonthly to monthly performance was also sizablefor the experimental study groups (28 per cent and 22 percent, respectively for classroom and workshop participants).
BSE proficiency was also improved in the experimentalgroups. For number of positions, there is over a four-folddifference between the experimental groups and the refer-ence control group (C2) and a 13-fold difference betweenthese two groups in the relative proportional change overtime for performing BSE above the median proficiencyscore.
DiscussionThis study represents an effort to advance the study of
the effectiveness of BSE programs and efficacy of BSE inearly detection through the application of robust planningand evaluation methodology. Characteristics of this demon-stration project included:
* an extensive preliminary needs assessment study of arepresentative sample of the target population;'6
* application of educational planning principles to the
tttData available on request to authors.
TABLE 1-Frequency of BSE by Study Group at Six-Month Follow-up
Per Cent Per CentPerforming Performing Per Cent
Within Past 6 Bimonthly- PerformingStudy Group Na Months Monthly Monthly
Control-without pretest (C2) 268 64.2 27.2 7.8Difference: (E1 and E2)b - C2 (95% Cl)C 530 16.7 (+ .06) 20.5 (± .07) 3.9 (+ .04)Difference: (WI and W2)d - C2 (95% Cl) 270 10.2 (+ .08) 10.1 (± .08) -.4 (± .05)Difference: C1I - C2 (95% Cl) 255 10.3 (± .08) 10.1 (± .08) .4 (+ .05)
rThe Ns represents the number of individuals according to the study group who responded to the six-month follow-up interview.bExperimental Classes (with and without pretest).CCI = Confidence Interval.dExperimental Workshops (with and without pretest).*Control with Pretest.
AJPH June 1985, Vol. 75, No. 6 621

MAMON AND ZAPKA
TABLE 2-BSE Proficiency by Study Group Performes at Six-month Follow-up
Per Cent Proficiency Proficiency2 or 3 Index Score Index Score,
Study Group Na Positions (mean, s.d.) % .9
X S.D.Control-without pretest (C2) 182 30.2 2.7 7.0 2.7 19.8Difference: (E1 and E2)b - C2 (95% CI)c 437 24.7 (± .09) 1.8 (+ .51) 24.8 (+ .08)Difference: (W, and W2)d - C2 (95% Cl) 208 22.7 (+ .10) 1.2 (+ .57) 15.8 (+ .09)Difference: (Cl' - C2 (95% CI) 204 4.1 (± .09) .3 (± .54) 6.7 (± .08)
aThe Ns represent the number of individuals according to study group who responded to six-month follow-up and reported everperforming BSE.
bExperimental Classes (with and without pretest).CCI = Confidence Interval.dExperimental Workshops (with and without pretest).'Control with Pretest.
intervention design, including use of several educa-tional methods; and
* a rigorous evaluation design which-focused on multiple behavioral outcome measures
(i.e., frequency, proficiency, care-seeking),-was tailored to different subgroups of the population
(classroom and workshops),included randomized comparison groups,
-accounted for the effects of testing,included follow-up data collection for six months postintervention,
-included intensive follow-up to achieve high follow-upresponse rate (79 per cent),incorporated explicit criteria for measuring BSE,15and
-measured competency using tools and data based on avalidation substudy.'8
The results of this study demonstrated that targetededucational interventions have significant impact in increas-ing the proportion of women who are currently performingBSE or are performing BSE on a reasonably routine basis.The intervention had less impact on increasing the propor-tion of women who practice monthly. However, frequencyof performance in this study was measured using the mostconservative approach; women were asked the number oftimes BSE was performed over a six-month period. Reviewof survey items on BSE frequency in a national surveyindicates that use of such an open-ended format yields lowerestimates of monthly performance than a forced choice
format (e.g., weekly, monthly, bimonthly, etc.); as much asa 12 per cent variability in reporting of monthly performancehas been observed.20 In this study, "reasonably" routinepractice (i.e., bimonthly as well as monthly performance)was of interest because studies based on estimates of detec-tion lead time, lifetime risk, and mathematical modelingindicate that performance of BSE three to four times peryear may be an adequate interval of BSE performance fordetecting breast abnormalities.21-25
Results also indicated that proficiency of performancewas significantly improved as a result of the educationalprogram. Since proficiency was found not to be highlycorrelated with frequency or regularity ofBSE performance,this separate dimension should be separately measured inresearch.
It was assumed during program planning that the popu-lation of the classes would be fundamentally different fromthose in the workshops who self-selected to attend. Whilethe workshop groups had lower levels of performance atbaseline with respect to all behavioral dimensions, theeffectiveness index results were similar to that of the class-room groups. This suggests that the program was equally butnot more effective in the self-selected group of women whoattended workshops than it was for the random classroomgroup.
No changes in care-seeking were observed, which maynot be surprising considering the age of the study populationand expected frequency of detecting problems. These find-ings suggest that there is not a negative psychological effectfrom performing BSE that induces women to inappropriately
TABLE 3-BSE Proficiency Performance by Study Group at Six-month Follow-up (All Subjects)
ProficiencyProficiency Index Index Score %
Study Group N' Score (mean, s.d.) .9
X S.D. %Control (without pretest) (C2) 265 4.8 3.9 13.6Difference: (El and E2)b - C2 (95% CI)c 511 2.7 (+ .61) 21.6 (+ .07)Difference: (W, and W2)d - C2 (95% Cl) 268 1.7 (± .70) 14.5 ( .07)Difference: Cl@ - C2 (95% Cl) 252 1.1 (+ .66) 7.9 (+ .07)
aThe Ns represent the number of individuals according to suy group who responded to six-month follow-up. People neverperforming BSE included as Os. Those who did not report specific stepa of BSE performance are excluded (2% of the respondents at six-month follow-up).
bExperimental Classes (with and without pretest).cCI = Confidence IntervaldExpedmental Workshops (with and without pretest).'Control with Pretest.
AJPH June 1985, Vol. 75, No. 6622

IMPROVING BSE FREQUENCY, PROFICIENCY
TABLE 4-Discussion of BSE with Secondary Target Groups by Study Group at Six-month Follow-up
% Discussed % DiscussedStudy Group Na With Others With Mothers
Control (without pretest) (C2) 182 41.2 18.0Difference: (El and E2)b - C2 (95% Cl)C 444 12.0 (+ .09) 3.0 (+ .07)Difference: (W1 and W2)d - C2 (95% Cl) 215 14.1 (+ .10) 8.0 (+ .08)Difference: Cl' - C2 (95% Cl) 209 2.3 (+ .10) -3.0 ( .07)
aThe Ns represent the number of Individuals according to study group who responded to six-month follow-up. People neverperforming BSE included as Os. Those who did not report specific steps of BSE performance are excluded (2%h of the respondents at six-month follow-up).
bExpermental Classes (with and without pretest).CI = Confidence Interval.dExperimental Workshops (with and without pretest).'Control with Pretest.
utilize the health care system. Post-intervention analyses of The data on discussion ofBSE with significant others byattitudes'7 also substantiated this finding; women were study participants suggest that the explicit urging of programfound to have less fear and a more realistic perception of the participants to speak with other women may be an effectiveincidence and prevalence of breast cancer. strategy for reaching secondary target groups.26
TABLE 5-Changes in BSE Performance Outcome Measures Over Time by Study Group
% Change BetweenPre- and Post- Effectiveness
Baseline Index
Frequency of BSE Performance% Currently within Past 6 MonthsControl (without pretest) (C2) -3.1 -9.5
Difference: (El + E2)a - C2 (95% CI)b 28.7 (± .06) 66.8 (± .07)Difference: (W1 + W2M - C2 (95% Cl) 32.2 (+ .07) 62.7 (+ .08)Difference: C1d - C2 (95% Cl) 10.3 (+ .04) 31.5 (+ .06)
% Monthly-BimonthlyControl (without pretest) (C2) 6.3 8.0
Difference: (E1 + E2) - C2 (95% Cl) 23.1 (± .06) 28.0 (± .06)Difference: (W1 + W2) - C2 (95% Cl) 20.4 (+ .06) 21.9 (+ .07)Difference: C, - C2 (95% Cl) 10.1 (+ .05) 12.7 (± .06)
% MonthlyControl (without pretest) (C2) .2 .2
Difference: (El + E2) - C2 (95% Cl) 4.2 (± .02) 4.5 (± .03)Difference: (W1 + W2) - C2 (95% Cl) 4.8 (+ .03) 5.3 ( .03)Difference: C, - C2 (95% Cl) .4 (± .01) .4 (+ .01)
Proficiency of BSE Performance% Performing in 2 or 3 PositionsControl (without pretest) (C2) 5.2 6.9
Difference: (El + E2) - C2 (95% Cl) 22.3 (± .07) 31.0 (± .08)Difference: (Wl + W2) - C2 (95% Cl) 28.0 (± .08) 34.4 (+ .09)Difference: C, - C2 (95% Cl) 4.1 (± .05) 5.5 (+ .06)
% Performing Above MedianProficiency ScoreControl (without pretest) (C2) 1.7 2.1
Difference: (El + E2) - C2 (95% Cl) 19.9 (+ .06) 26.0 (+ .07)Difference: (Wl + W2) - C2 (95% Cl) 18.1 (± .06) 21.4 (± .07)Difference: C, - C2 (95% Cl) 6.7 (± .04) 8.2 (± .05)
aEl between baseline (PI) and 6 month post-intervention (P2) where El = P2- Pl x 100.bExperimental Classes (with and without pretest). 100 - P1CCI = Confidence Interval.dExperimental Workshops (with and without pretest).'Control with Pretest.
AJPH June 1985, Vol. 75, No. 6623

MAMON AND ZAPKA
Although college women represent a select subgroup ofthe female population, comparison of study data on knowl-edge and BSE behaviors to that of older women suggeststhat there may be some common factors across ages, as wellas factors specific to particular age groups. 17 Even so,similar rigorous educational program planning and evalua-tion needs to be replicated with diverse subsamples ofwomen. Due to feasibility considerations, a six-month fol-low-up period was used. A longer follow-up time periodwould provide even more insight into maintenance of BSEproficiency.
BSE studies will always depend on indirect assessmentof actual performance since it cannot be observed as itnaturally occurs. While this study made advances in deter-mining accuracy of reporting for one of the major methods ofobtaining BSE information (i.e., via self-report), this tooneeds replication and expansion. Measures validating obser-vation, written survey, telephone and in-person reportingneed cross-validation on diverse subgroups of women. Sub-sequently, studies need to examine the relationship of profi-cient performance to lump/abnormality detection, then to itseffect on disease detection, and to subsequent morbidity(staging) and mortality. Only then will the debate about BSEefficacy be scientifically addressed.
REFERENCES1. American Cancer Society: Cancer Facts and Findings: 1983. New York:
American Cancer Society, 1983.2. US Department of Health and Human Services: Recommendations of the
National Cancer Institute and the American Cancer Society on Screeningfor Breast Cancer of Asymptomatic Women. (memorandum) Bethesda,MD: July 1982, National Institutes of Health, Public Health Services.
3. Cole P, Austin H: Breast self-examination: an adjuvant to early cancerdetection. (editorial) Am J Public Health 1981; 71:572-574.
4. National Cancer Institute: National Survey on Breast Cancer: A Measureof Progress in Public Understanding. NIH Pub. No. 81-2306. WashingtonDC: Govt Printing Office, 1980.
5. Huguley CM, Brown RL: The value of breast self-examination. Cancer1981; 47:989-995.
6. Crosson KE, Nessel AE, Engstrom PF, Grover PL: Health educationresearch in preventive oncology: A study of factors influencing thepractice of breast self-examination. Philadelphia, PA: The Fox ChaseCancer Center: Grant NOI-CN45055, NCI, DHEW, 1978.
7. Lynch J, Lynch H, Guirgis H, et al: Mobile cancer screening: epidemolo-gic and cancer control model. In: Nieburgs H (ed): Prevention andDetection of Cancer: Part II, Vol I, 1978.
8. Grady KE, Kegeles SS, Lund AK: Experimental studies to increase BSE:preliminary findings. In: Mettlin C, Murphy GP (eds): Progress in Clinicaland Biological Research, Vol 83: Issues in Cancer Screening and Commu-nications. New York: Alan R. Liss, 1982; 91-105.
9. Trotta P: Breast self-examination: factors influencing compliance. OncolNurs Forum 1980; 7:13-17.
10. Laughter D, Kean TJ, Drean KD, et al: The breast self-examinationpractices of high risk women: implications for patient education. PatientCounseling Health Educ 1981; 3:103-107.
11. Hall DC, Adams CK, Stein GH, et al: Improved detection of humanbreast lesions following experimental training. Cancer 1980; 46:408-414.
12. Howe HL: Proficiency in performing breast self-examination. PatientCounseling Health Educ 1980; 4:151-153.
13. Celentano DD, Holtzman D: Breast self-examination competency: ananalysis of self-reported practice and associated characteristics. Am JPublic Health 1983; 73:1321-1323.
14. Digest of Education Statistics; 1982 National Center for EducationStatistics, US DOE. Washington, DC: Govt Printing Office, 1982.
15. US Department of Health and Human Services: Surveillance, Epidemiol-ogy, and End Results: Incidence and Mortality Data, 1973-77. NIH Pub.No. 81-2330. Bethesda, MD: National Cancer Institute, 1981.
16. Zapka JG, Mamon J: Integration of theory, practitioner standards,literature findings, and baseline data: a case study in planning breast self-examination education. Health Educ Q 1982; 9:330-356.
17. Mamon J, Zapka JG, Ciperson J, Docie KC: Breast Self-Examination(BSE) Educational Program in a University Setting. Final Report ofDesign and Evaluation of Cancer Programs and Protocols. Submitted tothe National Cancer Institute, Contract NOI-CN-95439, Bethesda, Mary-land, September 1982.
18. Mamon J, Zapka JG: Measuring the proficiency of breast self-examina-tion: Validity of self-report compared with demonstration. Evaluation andthe Health Professions 1985; 8 (in press).
19. Green LW: Toward cost benefit evaluation of health education: someconcepts, methods, and examples. Health Education Monogr 1974;2(Suppl):34-64.
20. Gallup Organization: A Survey Concerning: Cigarette Smoking, HealthCheck-ups, Cancer Detection Tests. New York: American Cancer Soci-ety, 1977.
21. Kirsh R, Klein M: Examination schedules for breast cancer. Cancer 1974,33:1444-1450.
22. Schwartz M: An analysis of the benefits of serial screening for breastcancer based upon a mathematical model of the disease. Cancer 1978:41:1550-1564.
23. Shapiro S, Goldberg JD, Hutchinson GB: Lead time in breast cancerdetection and implications for periodicity of screening. Am J Epidemiol1974; 100:357-366.
24. Thiessen EU: Breast self-examination in proper perspective. Cancer1971; 23:1537-1545.
25. Smith EM, Francis AM, Polissar L: The effect of breast self-exampractices and physician examinations on extent of disease at diagnosis.Prev Med 1980; 9:409-417.
26. Gravell J, Zapka JG, Mamon J: Impact of breast self-examination plannededucational messages on social network communications: an exploratorystudy. Health Educ Q 1985 (in press).
ACKNOWLEDGMENTSThe authors gratefully acknowledge the helpful comments and sugges-
tions on earlier drafts of this manuscript by Sam Shapiro, Donald M.Steinwachs, and Ellen MacKenzie of the Health Services Research andDevelopment Center, School of Hygiene and Public Health; Pamela Fischerof the School of Medicine, Johns Hopkins University; and JoAnne Cipersonof University Health Services, University of Maryland/College Park. Thisresearch was supported by the National Cancer Institute, Contract No. NOI-CN-95439.
4HOJ?ES OF THIE IFUTIU}E:W4 E already have enioughl kniowledge wlicih, if brought
togrethier, comlipared anid sorted. wvould give us someapproachl to the nlormtial clhild. The crux of the problem is asquickly' as possible to brinig wihat kiowledge we have inlto theopeln. broadcast it. anid miiake it famiiiliar to tile average busv,but deeply concernied, parent.
"\\Te await fromii the scientific world that formula whicilNvill eniable all those \vlho care for chiildreni, whlo seek a betterera. to miol(d the boys and girls of todlay iinto stalwarts to whomwe entruist outr lhopes of the fuittire.' -Hcrbert Hoover.-From The American Public Health News, August 1931.
624 AJPH June 1985, Vol. 75, No. 6