Embed Size (px)
Citation preview

Implementing A Case Management Comprehensive Care Coordination
Model To Achieve Outcomes
April 28, 2015Sandy McFolling, MS, RN, ACMSenior Clinical Advisor, ACMA/Compare
Amir K Jaffer, MD, MBA, SFHMProfessor of Medicine, Associate Chief Medical OfficerVice Chair, Quality and Patient Safety, Division Chief, Hospital MedicineMedical Director, Case Management

Objectives
• Present CM Comprehensive Care Model structure and goals
• Define roles and responsibilities
• Demonstrate effectiveness and share outcomes
• Provide Medical Director insights and tools for physicians
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Plan – Vision & Goals
To provide a comprehensive patient centered
experience throughout the continuum to manage
patient resources, coordinate sustainable care
transitions, exceed patient expectations and achieve
quality outcomes.
- Patient/Family Focus
- Proactive Standardized Approach
- Risk Screening with Targeted Interventions
- Technology to Enhance Efficiency
- IP/OP System/Service Integration
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
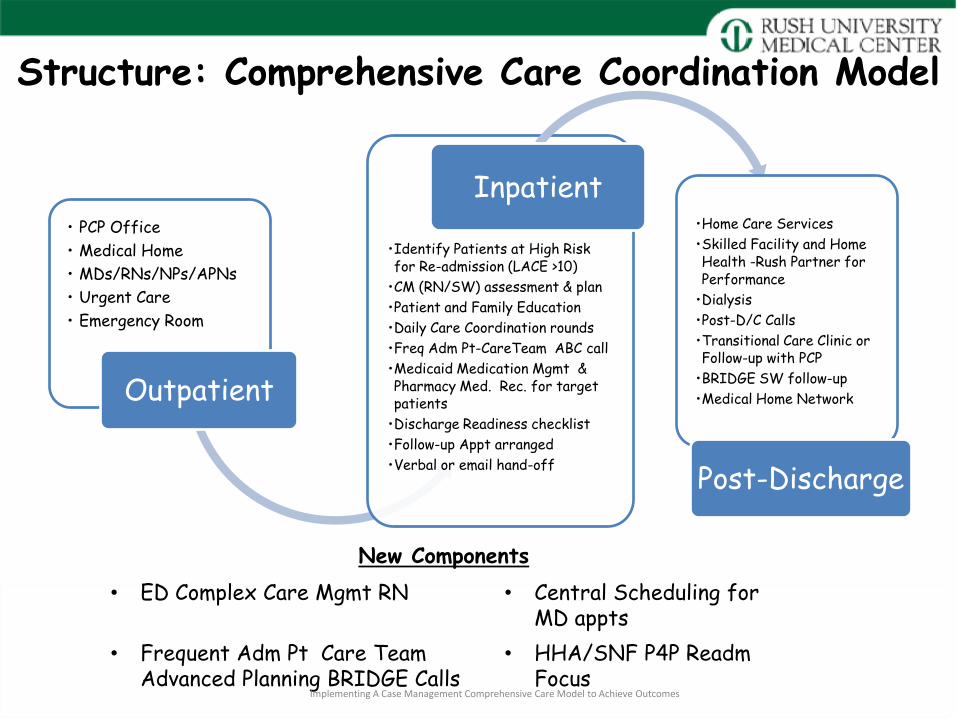
Structure: Comprehensive Care Coordination Model
• PCP Office
• Medical Home
• MDs/RNs/NPs/APNs
• Urgent Care
• Emergency Room
Outpatient
•Identify Patients at High Risk for Re-admission (LACE >10)
•CM (RN/SW) assessment & plan
•Patient and Family Education
•Daily Care Coordination rounds
•Freq Adm Pt-CareTeam ABC call
•Medicaid Medication Mgmt & Pharmacy Med. Rec. for target patients
•Discharge Readiness checklist
•Follow-up Appt arranged
•Verbal or email hand-off
Inpatient•Home Care Services
•Skilled Facility and Home Health -Rush Partner for Performance
•Dialysis
•Post-D/C Calls
•Transitional Care Clinic or Follow-up with PCP
•BRIDGE SW follow-up
•Medical Home Network
Post-Discharge
New Components
• ED Complex Care Mgmt RN • Central Scheduling for MD appts
• Frequent Adm Pt Care Team Advanced Planning BRIDGE Calls
• HHA/SNF P4P ReadmFocus
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Opportunities and Potential Strategies to ImproveCare Coordination
Opportunities Potential Strategies
Anticipate patient and family needs
- Daily Care Coordination rounds - EPIC communication and access (My Chart, Medical Home Report, Individual Care Plan)
Identify high risk patients - Implement risk stratification and interventions (LACE)- Complete proactive assessment at access points(ED, inpatient admission)
Promote Medication Safety - Pharmacist med reconciliation- Pharmacy follow-up calls post d/c - Discharge medication program- Medicaid Medication Coordination
Provide IP/OP Coordination and “Safety Net” to avoid readmissions
- CM-BRIDGE SW IP/OP Communication- Transitional Care Clinic Appts- Case Mgmt Model (ED & Inpatient)- Rush-Skilled Facility Care Coordination ( Rush MD and APN) - Rush Partner for Performance with Home Health agencies- Medical Home Network MD Follow-up Appt coordination - Palliative Care and Hospice End of Life Planning
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Case Management Action Steps
Opportunities Strategies/Actions
Anticipate patient and family needs
- Begin RN Care Coordination Role in ED
- Complete checklists and preplan discharges
-Create EPIC individualized care plan
Identify high risk patients
And
Provide IP/OP Coordination
- Implement LACE screening tool, perform 100% screening in EPIC
- Expand RN & SW CM roles to: provide targeted intervention, andenhance communication with internal and external providers
- Implement ABC interdisciplinary calls for frequent admit patients
- Enhance SNF and Home Health Partner for Performance collaboration and commitment to outcomes
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Case Management Inpatient Care Coordination
Roles Focus Caseload
Complex Care Coordinator RN
- At risk/readm pts LACE > 10- Clinically complex pts- Person centered plan & safety net- Initial screen and triage
12
SW Care Coordinator - Discharge planning- Complex psychosocial
20
CM Liaison - Routine screening and discharge planning- Medicare Important Message Notice- Medication Assistance
Unit Medical Director and Senior Case Manager
- Care Coordination- Outlier/LOS Management- Readmissions
- Throughput- Pt Satisfaction- LOC Mgmt
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
Modified LACE Tool
Attribute Value Points
Length of Stay Less 1 day 0
1 day 1
2 days 2
3 days 3
4-6 days 4
7-13 days 5
14 or more days 6
Acute Admission Inpatient-ED Admit 3
Observation or Direct Admit 0
Comorbidity No prior history 0
(Comorbidity points are cumulative to maximum of 6 points)
DM no complications, Cerebrovascular disease, Hx of MI, PVD, PUD 1
Mild liver disease, DM with end organ damage, CHF, COPD, Cancer, Leukemia, lymphoma, any tumor, cancer, moderate to
severe renal dz 2
Dementia or connective tissue disease 3
Moderate or severe liver disease or HIV infection 4
Metastatic cancer 6
Emergency Room visits during previous 6 months 0 visits 0
1 visits 1
2 visits 2
3 visits 3
4 or more visits 4

Risk Screen-Targeted Interventions-IP/OP Settings
Basic-All Patients Pt/Caregiver education on Dx, Meds, Diet, Activity, and Anticipatory Problems (Alert Sheet)
High Risk Med Teaching (polypharmacy =/or high risk med)
Daily Care Coordination Rounds
CM resource folder/Contact info/2-CARE Line
CM/SW interview for financial and psychosocial at risk patients
CM/SW assessment and plan
D/C Readiness Checklist
High Risk CM/SW patient/family interdisciplinary meeting including community providersCM/SW assessment, plan, and follow-up
CM patient readmission screening interview and person centered plan
Interdisciplinary Team Advanced Planning BRIDGE Call-ABC (PCP, CM, BRIDGE SW and community provider)Pharmacy medication reconciliationCM/RN/Pharmacy home going meds arranged
MD-MD discussion (hand-off)
Post Discharge follow-up call (CM or BRIDGE SW)
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Complex Care Coordinator RN Assessment and Person Centered Plan
Problems Interventions
Health Literacy
Disease Management
Dehydration, ↓ fluid intake. Concern about frequency during evening.
Recurrent SOB, HF “doubles up on meds to manage HF symptoms”
CCC RN Teaching and review of After Visit Summary. Refer to pharmacy & RN for reinforcement
Medication Management
Confusion tid vs bid
Cannot afford inhaler
Ran out of meds & cannot afford refill.
Conference with HHA, MD office, pt/family.
Obtain payer/family approval for med reimbursementFill scripts at Rush OP Pharmacy
Access to Care Complex wound care, pt noncompliance requests LTAC in ED
Chronic renal insuff, back pain, Substance abuse. Missed MD appts likes to be seen in ED when problem arises
ED Adm AvoidanceED CCC RN arranges LTAC adm
Person Centered PlanControl & flexibility with MD appt. Call office & seen next day (TCC, ED, Home MD)
Access/Pt Support
Misses dialysis w/o help to climb 8 stairs for curbside transport
Person Centered PlanHHA, Dialysis & Support person to coordinate transport schedule
Palliative Care Colon CA, Liver Mets, GI Bleed. Refusing hospice, lives home with daughter.
Person Centered PlanPatients wishes understood Med adjust to manage symptoms, create plan with HHA to manage care with Home PC when ready.
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

ABC Call for Frequently Admitted Patients
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
Duration: 10 minutes
Date:_______________ Patient: __________________ Admit Date: ____________
(2 minute) We are holding this call in regards to _______________’s admissions so that we can connect providers and
collect input to improve the continuity based plan for this patient.
On the call is: _______________ _______________ _______________ _______________
The goal of the call is to discuss things that are driving the requirements for ___________________’s admissions and
then interventions for any modifiable factors.
(1 minute) Based on our current research, we (Bridge) see Dr. _________________ is highly influential in the patient’s
care. Could you please start us off with what you see as the primary drivers in this patient’s admissions?
Admission Drivers
_______ Symptom Relief _________________________________________________________
_______ Unclear goals of care or End of life ___________________________________________
_______ Access to medication or usage education _____________________________________
_______ Access to follow-up care providers ___________________________________________
_______ Mental health issues ______________________________________________________
_______ Psychosocial ____________________________________________________________
_______ (Other) _________________________________________________________________
(3 minutes) Open the discussion to the other participants for drivers
(4 minutes) Intervention plan based on modifiable drivers. Owner ______________________
Patient is expected to follow up with: ___________________________ By When: ________________
Other Notes:

• MD Appt at Transitional Care Clinic
• Rush BRIDGE Social Work Follow-up Calls and Coordination
• Skilled Facilities with Rush MDs and Nurse Practitioners
• Partnership for Performance with Home Health Agencies
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
Post Discharge

Performance Outcomes
• Case Management Staff Satisfaction
• Post Discharge Care Coordination and Sustainable Care
• General Medicine Pilot Performance
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

CM Staff Survey – Impact ( 1-5 Scale)
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
Enhanced team collaboration & effectiveness 4.17
Improved patient satisfaction 3.83
Improved discharge coordination 3.83
Reduced readmissions 3.50
CM Staff Satisfaction
Role
Able to make a difference 4.67
Clear expectations 4.17
Satisfied with role 4.17
Have tools I need 3.50

July – June 2013, 2014 and July- Dec 2015
FY2013# Readms/Total
%
FY2014# Readms/Total
%
YTD 2015# Readms/Total
%
Home 12.8% 12.6% 11.2%
HHA 21.3% 21.6% 17.2%
SNF 14.3% 17.4% 14.6%
IP Hospice 1.7% 1.3% 0.9%
Home Hospice 4.5% 7.8% 3.9%
Rehab 1.9% 2.8% 2.8%
LTAC 13.1% 14.7% 8.3%
Post Discharge CoordinationReadmission Rates by Discharge Disposition
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Home Health Readmissions Within 30 Days All Cause (Total vs. Partner for Performance )
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
20.8%
17.2%
21.5%
18.0%
14.4%15.9% 16.4% 17.1%
9.8%8.8%
9.9% 9.4%
13.0%
8.4%6.6% 6.6%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
FY14 FY15-YTD Jul Aug Sept Oct Nov Dec
Rush Total HHA Partner for Performance HHA
FY14 9.1

Readm Variance by Inpt Unit :Pilot Units=Greatest Reduction
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

CM Model Outcomes-General Medicine Floors
2013 2014 FYTD 2015 (Dec)
Rush TotalAll Cause Readm-
15.1% 14.6% 14.6%
Medicine Pilot Units All Cause Readm
Phase I-2 Med Floors
Pre Pilot(July-Dec)
18.8%
Pilot(Jan-May) 18.1%
Phase II (Added2 floors-Med/Onc)
23% 19.9%
Patient Satisfaction
84.5% 85.7% 83.1%
Patient Screened w/in 24hrs
82.7% 90.4%
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Medical Director –CM System Director Partnership
• Care model and leadership team development
• Weekly touch base meetings
• Case facilitation support and physician education
• Care planning meeting/rounds support and leadership
• Strategic planning and performance improvement projects
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Physician Leadership and Support
• Associate Medical Director
• ED Physician Advisors
• Unit Medical Director and Observation Team Physician Officer Role Development
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Process Improvement-Level of Care Management
Goal:
Design ED to Floor process to assign appropriate LOC, obtain supporting physician order/documentation, provide hand-offs and efficiently place patients in Medical floor observation unit beds
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Process Redesign
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Process Redesign- EPIC Smart Text
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

• A smart phrase has been developed to cue physicians to include their clinical reasoning for either initial placement in observation or inpatient status or subsequent conversion to inpatient status.
• A certification check box (which does not replace the full certification done using the smart phrase) is generated for any inpatient order.
• Any unsigned „Admit to Inpatient‟ order fires a delinquency in the Attending‟s in basket which pops up every time they enter Epic.
• All Medicare Observation cases placed on a shared list, our „Preadmission list‟
– Another Epic list was created that captures all Observation patients
• All cases reviewed several times daily by the Armstrong/Observation Attending, Physician Advisor or Unit Medical Director, and CM Preadmission Nurse.
Process Redesign: LOC Status Change
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes
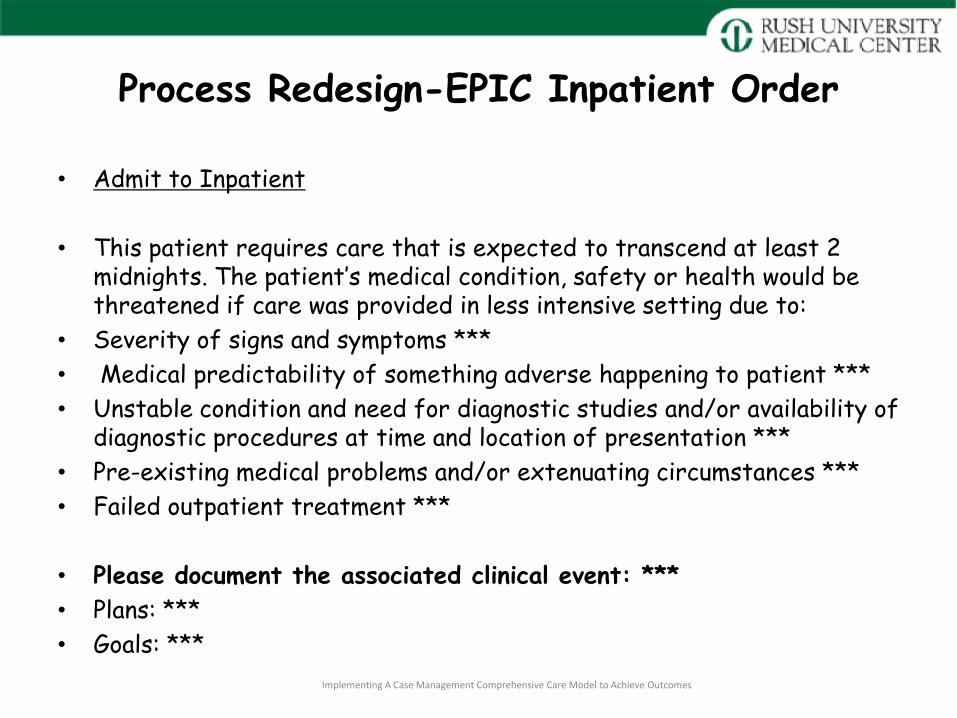
Process Redesign-EPIC Inpatient Order
• Admit to Inpatient
• This patient requires care that is expected to transcend at least 2 midnights. The patient‟s medical condition, safety or health would be threatened if care was provided in less intensive setting due to:
• Severity of signs and symptoms ***
• Medical predictability of something adverse happening to patient ***
• Unstable condition and need for diagnostic studies and/or availability of diagnostic procedures at time and location of presentation ***
• Pre-existing medical problems and/or extenuating circumstances ***
• Failed outpatient treatment ***
• Please document the associated clinical event: ***
• Plans: ***
• Goals: ***
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Process Redesign- EPIC Certification Checkbox
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

Process Redesign-EPIC deficiency notice
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes

ConclusionCare Coordination Implementation Requires:
• Partnership with Medical Director and CM Director
• Staff involvement and engagement
• Understanding the culture
• Risk stratification of routine and complex patients
• Outcome tracking and adjustments
• Holding community partners accountable
• Leveraging tools and technology
• Commitment to sustaining gains
• Flexibility and willingness to change
• Team support throughout changesImplementing A Case Management
Comprehensive Care Model to Achieve Outcomes

Thank-you!
Questions?

Tools
• LACE Screening
• Daily Risk Report
• Process Flow
• Patient Education Material
• Discharge Checklist
• SNF Coordinated Care Program
• Home Health Agency Transitions In Care
Implementing A Case Management Comprehensive Care Model to Achieve Outcomes









![Comprehensive ESRD Care Initiative LDO Model€¦ · Comprehensive ESRD Care Initiative LDO Model . July [15], 2015 . ... Comprehensive ESRD Care Initiative Participation Agreement](https://img.dokumen.tips/doc/110x75/5af2cc657f8b9a95468ba91b/comprehensive-esrd-care-initiative-ldo-model-comprehensive-esrd-care-initiative.jpg)



















