Embed Size (px)
Citation preview

Background
❑ Increased Transitions: Surgical patients are vulnerable to handoff errors due to the number of transitions in the perioperative setting.
❑ Framework: A lack of framework leads to inconsistent and variable quality handoffs. The Joint Commission reports miscommunication contributes to 50 to 80% of sentinel events.
❑ Evidenced Based Checklist: To reduce omission of information and improve the quality of the handoff process, an evidenced based checklist was created to use during handoff.
PurposeProvide a standardized tool to reduce omission of patient information, increase information accuracy and improve communication during patient handoff.
Conclusions & Further StudyWith the addition of the checklist, a consistent process for handoff was created which ultimately decreased the variability of information given during handoff of care. Also, the omission of information decreased in every category. The categories with the most improvement decreased the rate of omission of information, on average, by 37%. The handoff time also improved from an average of 2 minutes to 1.5 minutes. The handoff time improvement was a positive, unexpected finding.
Some limitations of the project include the size of the audit group and a lack of the attending anesthesia and postop nurse buy-in. A lack of buy-in contributed to a decrease in use of the checklist. The charge nurse was responsible for completing the audit in real time. In some instances, the audit was not completed due to the unit’s high patient flow or census. There were also multiple nurses performing the audits which led to variability in the evaluations.
Discussion❑ The checklist can be utilized during other anesthesia handoffs including provider
to provider, provider to ICU team, as well as implementation in the adult PACU.
❑ Studies have shown that implementation of a structured handoff checklist during transfer of care increases communication, improves employee satisfaction, lowers the number of questions and callbacks to the physician teams, does not increase handoff time at bedside, increases information accuracy and decreases omissions.
References1. Halterman, R. S., Gaber, M., Janjua, M. S. T., Hogan, G. T., & Cartwright, S. M. I. (2019). Use of a
Checklist for the Postanesthesia Care Unit Patient Handoff. Journal of Perianesthesia Nursing, 34(4), 834–841. https://doi.org/10.1016/j.jopan.2018.10.007
2. Muralidharan, M., Clapp, J. T., Pulos, B. P., Diraviam, S. P., Baranov, D. Y., Gordon, E. K. B., & Lane-Fall, M. B. (2018). How does training in anesthesia residency shape residents' approaches to patient care handoffs? A single-center qualitative interview study. BMC Medical Education, 18, 271–277. https://doi.org/10.1186/s12909-018-1387-8
3. Inadequate Handoff Communication. (2017). Sentinel Event Alert, (58), 1–6. Retrieved from www.jointcommission.org
4. Funk, E., Taicher, B., Thompson, J., Iannello, K., Morgan, B., & Hawks, S. (2016). Structured Handover in the Pediatric Postanesthesia Care Unit. Journal of Perianesthesia Nursing, 31(1), 63–72. http://dx.doi.org/10.1016/j.jopan.2014.07.015
5. Bruno, G. M., & Guimond, M. E. “B. (2017). Patient Care Handoff in the Postanesthesia Care Unit: A Quality Improvement Project. Journal of PeriAnesthesia Nursing, 32(2), 125–133. doi:10.1016/j.jopan.2015.10.002
6. Robins, H.-M., & Dai, F. (2015). Handoffs in the Postoperative Anesthesia Care Unit: Use of a Checklist for Transfer of Care. AANA Journal, 83(4), 264–268. Retrieved from www.aana.com/aanajournalonline
7. Boat, A. C., & Spaeth, J. P. (2013). Handoff checklists improve the reliability of patient handoffs in the operating room and postanesthesia care unit. Pediatric Anesthesia, 23(7), 647–654. doi:10.1111/pan.12199
8. Nagpal, K., Abboudi, M., Manchanda, C., Vats, A., Sevdalis, N., Bicknell, C., … Moorthy, K. (2013). Improving postoperative handover: a prospective observational study. The American Journal of Surgery, 206(4), 494–501. doi: 10.1016/j.amjsurg.2013.03.005
AcknowledgementsDr. Craig Belon PhD, MD
Assistant Clinical Professor of Anesthesiology and Pain Medicine
Design & Methods
❑ Handoff: After receiving anesthesia, it is critical for patients to be closely monitored. Handoff occurs from the surgical team, OR nurse and anesthesia team to the assuming PACU nurse.
❑ Lack of Consistency: Attending physicians lack a consistent process for modeling a complete handoff. The variability of handoff from anesthesia providers as well as turnover time pressures contributes to a disorganized transfer of care and leads to omission of information.
❑ Evidenced Based Checklist: With the help of an attending anesthesiologist, the PACU nurses created a standardized evidenced-based tool to use during handoff.
❑ Education: Given to the nurses and anesthesia providers before implementation of the tool. A laminated copy of the checklist was supplied at each bedside as well as laminated badge buddies for the anesthesiologists.
❑ Effectiveness of Tool: The charge nurse conducted observational audits of anesthesia handoff before and after use of the checklist.
Implementation Plan
Implementation of an Anesthesia Handoff Checklist ToolChildren’s Surgery Center
Cheryl Ditter BSN, RN, CPAN
Melody Hillstrom BSN, RN, CCRN
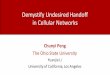
Performance Data
Pre checklist n=22 audits conductedPost checklist n=66 audits conducted
Average time of handoff improved from 2.05 minutes prior to use of checklist to 1.46 minutes after implementation of the checklist.
Anesthesia Handoff Checklist❑ Stable airway + Vital signs❑ Are you ready for report?❑ Name, weight, age, allergies❑ Procedure❑ Medical history ❑ Airway management ❑ Access/fluids❑ Medications given❑ Intraoperative complications or concerns❑ Postoperative: Labs, pain control, PONV plan❑ Bladder status ❑ Family/Disposition plan❑ Contact/pager for anesthesia provider/orders in❑ Any questions?
81%
54%
59%
54%
41%
64%
86%
73%
86%
32% 33%
26%
22%
18%
27%
36%
27%
47%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Are you readyfor report?
Patient's name Weight and Ageof patient
Allergies Intra-operativeconcerns
Post-op plan Bladder Status Family anddischarge plan
Contact/pagernumber
Categories with Greatest % of Omission
Pre Checklist Post Checklist