Embed Size (px)
Citation preview

Elucidating the risk factors for chronic obstructive pulmonary
disease: an umbrella review of meta-analyses
Vanesa Bellou1,2, Lazaros Belbasis1, Athanasios K Konstantinidis2, Evangelos Evangelou1,3
1Department of Hygiene and Epidemiology, University of Ioannina Medical School, Ioannina,
Greece
2Department of Respiratory Medicine, University of Ioannina Medical School, Ioannina, Greece
3Department of Epidemiology and Biostatistics, School of Public Health, Imperial College
London, London, UK
Conflict of interest:
None
Running head:
Risk factors for COPD
Word count of the summary: 238 words
Word count of the manuscript: 2779 words
Number of references: 48
Number of tables: 2
Number of figures: 1
Corresponding author:
Dr Evangelos Evangelou
1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20

Assistant Professor, [email protected]
Department of Hygiene and Epidemiology, University of Ioannina Medical School, Ioannina,
Greece
Acknowledgements:
Author contributions: VB, LB and EE designed the study. VB and LB performed the
literature search, the study selection and the data extraction. VB and LB performed the
statistical analyses. VB and LB wrote the first draft of the manuscript, whereas AK and
EE critically reviewed the manuscript. All authors approved the final version of the
manuscript.
Guarantor: EE is the guarantor of the content of the manuscript, including the data and
analysis.
Role of sponsors: Not applicable
Conflicts of interest: None
2
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36

Summary
Chronic obstructive pulmonary disease (COPD) is commonly attributed to smoking,
ignoring neglecting other potential risk factors. We aim to critically appraise the
epidemiological credibility of the risk factors examined for COPD in published meta-
analyses. We performed a systematic search to capture systematic reviews and meta-
analyses of observational studies on risk factors and biomarkers for COPD. We applied a
set of standardized methodological criteria based on level of statistical significance,
sample size, between-study heterogeneity, and statistical biases. Our search yielded 11
eligible papers including a meta-analysis for 18 risk factors or biomarkers for COPD, and
8 eligible papers performing only a systematic review. Eleven associations achieved
statistical significance at P <0.001 and 6 associations at P <10-6. Thirteen associations
presented an I2 ≥50%, while 6 associations had evidence for small-study effects and/or
excess significance bias. The associations that had high epidemiological credibility for an
increased risk for COPD were history History of tuberculosis and rheumatoid arthritis,
exposure to biomass fuels, tobacco smoking, and second-hand smoking were supported
by high epidemiological credibility for an increased risk for COPD. Furthermore, robust
highly suggestive evidence was found for elevated levels of serum CRP, and serum
fibrinogen in COPD patients compared to healthy controls. Our approach indicates that,
despite thatwhilst a proportion of COPD patients are non-smokers, only a narrow range
of risk factors not related to smoking have been studied for an association with COPD.
There is also a need to decipher possible protective factors in COPD pathogenesis given
that more than a half of ever smokers do not develop COPD.
Keywords: epidemiology; epidemiologic credibility; risk factor; biomarker; bias
3
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59

Abbreviation list: CI, confidence interval; COPD, chronic obstructive pulmonary
disease; IQR, interquartile range; MR, Mendelian randomization; OR, odds ratio; RA,
rheumatoid arthritis; RR, risk ratio; SE, standard error
4
60
61
62

Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by progressive
airflow obstruction, due to narrowing of small airways, and destruction of alveolar walls
1,2. The global prevalence of COPD is estimated to be 10.7% in individuals aged 30 years
or more 3. In the USA, COPD is the third leading cause of death 4,5, and it is associated
with a large economic burden 6.
COPD results from an interplay of genetic and environmental risk factors 7. The most
recent meta-analysis of genome-wide association studies found 22 loci associated with
COPD 8. Smoking is considered the main and causal environmental risk factor for COPD
9. However, it is not the only risk factor since about 30% of COPD patients have never
smoked 10. Another fact that should not be neglected is that the attributable fraction for
smoking is lower in developing countries compared with developed countries. 9 This
observation indicates the importance to identify additional risk factors in order to tackle
the prevalence of COPD, especially in low and middle-income countries. For this reason,
a number of other environmental risk factors have been examined for an association with
COPD, including indoor and outdoor air pollution and occupational exposures 9.
Several environmental factors and biomarkers have been considered in systematic
reviews and meta-analyses for risk for COPD. However, there has been no effort to
systematically summarize and critically appraise these associations. We performed an
umbrella review to map the range and validity of current evidence on environmental
factors and biomarkers for affecting the risk for COPD, and to examine their
epidemiological credibility and the presence of statistical biases in these associations.
5
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84

Methods
We conducted an umbrella review, which is a systematic collection and evaluation of
multiple systematic reviews and meta-analyses on a specific research topic 11. Identified
risk factors from the umbrella review were assessed using standardized, state-of-the-art
methods.12–14
Search strategy and eligibility criteria
We systematically searched PubMed from inception to December 31, 2017 to
identify systematic reviews and meta-analyses of observational studies examining the
association of environmental factors or serum biomarkers and risk for COPD. We used
the following search algorithm: (“chronic obstructive pulmonary disease” OR “chronic
bronchitis” OR emphysema OR COPD) AND (“systematic review*” OR meta-analys*).
We did not apply any language restrictions. When more than one meta-analysis on the
same research question was available, the meta-analysis with the largest number of
prospective cohort studies was retained for our analysis. We excluded meta-analyses
limited in a specific geographic location. Literature search and selection of eligible
studies were performed independently by two investigators (VB, LB), and in case of
discrepancies the final decision was that of a third investigator (EE).
We additionally searched for Mendelian randomization (MR) studies examining the
potential causal association between risk factors and COPD. In this search, the following
search algorithm was used: (“mendelian randomization” OR “mendelian randomisation”)
AND “obstructive pulmonary disease”. We complemented the search strategy by
6
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106

reference screening of eligible MR studies. An MR study is an approach that uses
measured variation in genes of known function to make causal inference of the effect of
an exposure on an outcome. It is an application of the technique of instrumental variables
with genotype acting as an instrument for the exposure of interest. 15
Data extraction
Data extraction was performed independently by two investigators (VB, LB), and in
case of discrepancies the final decision was that of a third investigator (EE). From each
eligible article, we recorded the first author, the year of publication, the examined risk
factors and the number of studies considered. For From each eligible article including a
systematic reviews without a quantitative synthesis, we recorded the justification for not
conducting meta-analysis and the main conclusion.
For From each eligible article including a meta-analysesanalysis, we extracted the
study-specific risk estimates (i.e., standardized mean difference, risk ratio, odds ratio, and
hazard ratio) along with the corresponding 95% confidence interval (CI) and the number
of cases and controls in each study for each risk factor. We screened the component
studies to ensure that none of the eligible meta-analyses included studies with shared
population.
From each MR study, we extracted the first author and year of publication, the risk
factor considered, the level of comparison for exposure, the genetic instrument used, the
applied statistical approach, the sample size, the causal odds ratio and its 95% CI, the P-
value for the association, and whether the authors claimed that a causal relationship
exists.
7
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128

Statistical analysis
For each meta-analysis, we estimated the summary effect size estimate and its 95%
CI using fixed-effect and random-effects models. In the case of meta-analyses with
continuous data, the standardized mean difference was transformed to an odds ratio. We
also estimated the 95% prediction interval (PI), which further accounts for between-study
heterogeneity and evaluates the uncertainty for the effect that would be expected in a new
study addressing that the same association. For the largest study of each meta-analysis,
we estimated the SE of the effect size estimate and we examined whether the SE was less
than 0.10.
Between-study heterogeneity was assessed by the I2 metric. I2 ranges between 0%
and 100% and is the ratio of between-study variance over the sum of within-study and
between-study variances. Values exceeding 50% or 75% are usually judged to represent
large or very large heterogeneity, respectively.
We assessed whether there was evidence for small-study effects (i.e., whether
smaller studies tend to give substantially larger estimates of effect size compared with
larger studies) with the Egger’s regression asymmetry test 16. A P <0.10 combined with a
more conservative effect in the largest study than in random-effects meta-analysis was
judged to provide evidence for small-study effects.
We further applied the excess statistical significance test, which evaluates whether
there is a relative excess of formally significant findings in the published literature due to
any reason (e.g., publication bias, selective reporting of outcomes or analyses) 17. This
test assesses whether the observed number of studies with nominally significant results is
8
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150

larger than their expected number. Excess statistical significance was claimed at two-
sided P <0.10.
Assessment of epidemiological credibility
We identified associations that had the strongest evidence and no signals of large
between-study heterogeneity or, small-study effects or excess significance bias.
Specifically, we considered as convincing the associations that fulfilled all the following
criteria: statistical significance per random-effects model at P <1 × 10-6, based on >1000
cases, without large between-study heterogeneity (I2 <50%), 95% PI excluding the null
value, and no evidence of small-study effects and excess significance bias. The
associations with >1000 cases, P <1 × 10-6 in random-effects meta-analysis, and largest
study presenting a statistically significant effect (P <0.05) were graded as highly
suggestive. The associations supported by >1000 cases and a statistically significant
effect at P < 1 × 10-3 were considered as suggestive. The remaining nominally significant
associations were considered as having weak evidence. For associations with convincing
and highly suggestive evidence, we performed a sensitivity analysis including only
prospective cohort studies and nested case-control studies, and we examined whether
there was a change in the level of epidemiological credibility.
The statistical analyses and the power calculations were done with STATA, version
12.0.
Ethics approval statement
Our study does not involve human subjects. Thus, ethics approval is not required.
9
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172

Results
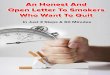
Our literature search resulted in 1801 papers, and nineteen articles were deemed
eligible (Figure 1). Eight articles performed a systematic review without quantitative
synthesis of the available evidence, and eleven articles performed a meta-analysis as well.
Thirteen articles were excluded after full-text screening, because another more recently
published meta-analysis with more component studies was available. These meta-
analysesarticles pertained to biomass fuels, history of tuberculosis, history of psoriasis,
serum vitamin D, tobacco smoking, second-hand smoking, and occupational exposures.
Five meta-analysespapers were excluded after full-text screening, because they included
meta-analyses due towith fundamental errors in statistical synthesis. Specifically, in these
five papers, we identified errors in the extraction or the calculation of effect size, or
inclusion of multiple component studies with overlapping samples.
Meta-analyses of risk factors and biomarkers for COPD
The 11 eligible articles included 18 unique meta-analyses. The median number of
studies per meta-analysis was 5 (IQR, 4 – 11) and the median number of cases was 2732
(IQR, 2108 – 3359). Nine of 18 meta-analyses examined exposures to various noxious
particles, 4 meta-analyses focused on medical conditions as risk factors for developing
COPD, and 5 meta-analyses examined the levels of serum inflammatory biomarkers in
COPD patients compared with healthy controls.
Thirteen associations were nominally significant (P <0.05), and eleven of them
remained statistically significant at P <0.001. Only six of them were statistically
significant at P <1 × 10-6 (Table 1). These associations pertained to exposure to biomass
10
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194

fuels, history of tuberculosis, history of rheumatoid arthritis (RA), tobacco smoking,
second-hand smoking, serum C-reactive protein (CRP), and serum fibrinogen. Only three
associations had 95% PI that excluded the null value (Table 1). These associations
focused on history of tuberculosis, tobacco smoking, and second-hand smoking. In fifteen
meta-analyses, the result in the largest study was more conservative than the summary
result under in the random-effects model. Also, in 10 meta-analyses, the standard error of
the largest study was less than 0.10 in a log OR scale.
Five associations (biological dust, second-hand smoking, serum TNFα, traffic
intensity on nearest road, and traffic load on major roads within 100 meters) had small or
moderate between-study heterogeneity (I2 <50%). Three associations (gases or fumes,
mineral dust, and serum CRP) had large heterogeneity (I2 ≥50% and I2 ≤75%). Ten
associations (history of tuberculosis, exposure to biomass fuels, tobacco smoking, history
of psoriasis, history of RA, waterpipe smoking, serum vitamin D, vitamin D deficiency,
and serum fibrinogen) presented very large heterogeneity (I2 >75%).
In 5 associations, there was evidence for small-study effects (Table 1). These
associations pertained to history of tuberculosis, exposure to biomass fuels, history of
psoriasis, second-hand smoking, and serum vitamin D. In 4 associations, there was
evidence for excess statistical significance and these associations pertained to exposure to
biomass fuels, second-hand smoking, serum vitamin D, and vitamin D deficiency (Table
1). In four meta-analyses, pertaining to history of RA and psoriasis, traffic intensity on
nearest road, and traffic load on major roads within 100 meters, excess significance test
could not be performed because sample sizes of component studies were not available.
Assessment of epidemiological credibility
11
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217

Seven associations (history of tuberculosis, history of RA, exposure to biomass fuels,
tobacco smoking, second-hand smoking, serum CRP, and serum fibrinogen) were graded
as highly suggestive (P <1 × 10-6 in random-effects meta-analysis and largest study with a
statistically significant effect at P <0.05). Five of them (history of tuberculosis, exposure
to biomass fuels, tobacco smoking, serum CRP, and serum fibrinogen) with highly
suggestive evidence also presented a large effect size (i.e., OR >2.00).
Three associations (history of psoriasis, serum vitamin D, and serum leukocytes)
presented suggestive evidence (more than 1000 cases, and P <0.001 but P >1 × 10-6).
Three associations (waterpipe smoking, vitamin D deficiency, and serum TNFα) were
supported by weak evidence. Five associations (exposure to biological dust, gases or
fumes, mineral dust, traffic intensity on nearest road, and traffic load on major roads
within 100 meters) were not statistically significant (P >0.05 under the random-effects
model).
From the associations that were supported by highly suggestive evidence, exposure
to biomass fuels 18, history of tuberculosis 19 and history of RA 20 were examined in case-
control studies, cross sectional studies and retrospective cohort studies. In contrast, the
associations on active smoking and second-hand smoking were mainly examined in
prospective cohort studies. In the sensitivity analysis, the association for active tobacco
smoking remained highly suggestive, but the association for second-hand smoking
presented weak evidence due to small number of COPD cases (Table 2). In the meta-
analyses on serum CRP and serum fibrinogen 21, only one prospective cohort study was
included.
Mendelian randomization studies for COPD
12
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240

Overall, we captured 4 MR studies for risk of developing COPD 22–25. Three MR
studies 22,23,25 examined the causal effect of genetically elevated levels of serum CRP on
COPD risk. These MR studies constructed haplotypes of polymorphisms in CRP gene as
instrumental variable. An additional MR study examined the causal effect of genetically
elevated levels of serum interleukin-6 on COPD risk and used 8 single nucleotide
polymorphisms as instrumental variables 24. All MR studies used individual-level data.
The findings from the MR studies indicated that a genetically elevated serum CRP and
serum interleukin-6 was not associated with increased risk for developing COPD.
Systematic reviews without a meta-analysis
The eight eligible systematic reviews that did not perform quantitative synthesis
focused on n-3 fatty acids intake 26,27, exposure to pesticides 28, dietary fiber intake 27,
menopause 29, agricultural work 30, construction work 31, and socioeconomic status 32. The
systematic reviews avoided quantitative synthesis due to large methodological
heterogeneity of observational studies. The authors of the systematic reviews concluded
that low socioeconomic status 32, higher intake of dietary fibers 27, exposure to
agricultural and construction workplaces 30,31, and exposure to pesticides 28 may increase
the risk for COPD, but they argued that the evidence for n-3 fatty acids, and menopause
was inconsistent 26,27,29.
Discussion
In this umbrella review, we summarized and critically appraised the evidence on 18
risk factors and serum biomarkers for COPD. Overall, three toxic exposures (i.e., active
13
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262

and passive tobacco smoking, and biomass fuels exposure), and two medical conditions
(i.e., history of tuberculosis, and RA) presented robust evidencehigh epidemiological
credibility for an elevated COPD risk. Additionally, highly suggestive evidence indicated
that serum levels of two biomarkers (i.e. CRP, fibrinogen) were higher in COPD patients
than healthy controls.
Smoking is the foremost risk factor for developing COPD. There is a vast amount of
observational studies supporting an association with COPD. Despite the very large
between-study heterogeneity, the 95% PI excluded the null value, indicating a robust
credible association between smoking and risk for COPD. Smokers presented a 4-fold
increased risk compared to never smokers. Additionally, passive smoking was also
strongly associated with risk for COPD, increasing the lung’s total burden of inhaled
particles and gases 33. Higher smoking intensity, commonly measured by the number of
pack-years, is related to COPD severity 7. Only 40% to 50% of lifetime smokers develop
COPD 34, indicating that unknown protective factors and potential gene-environment
interactions attenuate the risk in smokers 33.
About 30% of COPD patients are never-smokers, indicating that there are additional
factors modifying the risk for COPD. Our umbrella review indicated that exposure to
biomass fuel was also associated with risk for developing COPD. In developing
countries, exposure to indoor air pollution is considered the main risk factor for COPD
and it contributes to the pathogenesis of COPD through deposition of noxious particles
on the airways 33. Although the largest exposure burden is reported in low-income
countries, biomass fuels, primarily wood, are also used in developed countries, mainly for
14
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284

heating 9. Combustion of biomass fuel produces a variety of air pollutants especially
particulate matter, which is inhaled into the small airways and alveolar spaces. 35
Moreover, our results depicted a highly suggestive relationship between history of
tuberculosis and COPD, indicating that COPD could be a long-term complication of
tuberculosis 36. The 95% PI for this association excluded the null value, but evidence for
small-study effects was found, indicating that the effect size could be inflated. Also, this
association was examined only in case-control studies and cross-sectional studies. The
underlying mechanism explaining this association could be fibrosis and inflammation of
the airways induced directly by the mycobacterium or by the immune response of the
host. 2 In developing countries, epidemiological studies indicated that history of
tuberculosis exerted a much larger risk for COPD compared with exposure to biomass
fuels or tobacco smoking. 2,37 It is disputed that smoking could be the underlying link
between tuberculosis and COPD, because A meta-analysis of observational studies
showed that smokers have an elevated risk of tuberculosis, and this observation could
indicate that the association between tuberculosis and risk for COPD could be partly
explained through smoking 34. However, there are studies showing that the association
remains statistically significant even after adjusting for tobacco smoking and biomass
fuels. This evidence supports an association of history of tuberculosis with COPD,
independent of smoking. is independent of smoking 2,37 Tobacco smoking and biomass
fuels may also contribute in the airflow obstruction caused by tuberculosis, resulting in
COPD
Furthermore, our study showed that highly suggestive evidence exists for an
increased risk of developing COPD in RA patients., but tIn the respective meta-analysis,
15
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307

this association was examined exclusively in retrospective cohort studies, and a temporal
association could not be established. Smoking is a risk factor for both RA and COPD;
hence, this association is commonly attributed to the effect of smoking.38–40 The first
prospective cohort study was recently published and was based on the population of
Nurses’ Health Study.41 In this study, a statistically significant association was found
between RA and risk for COPD, whereas the association remained significant after
adjusting for confounding and mediation by smoking and other exposures through
marginal structural models. Under the light of this observation, RA could be considered
to increase the risk for COPD independently of smoking. This association could be
explained by the fact that smoking is a shared risk factor for both conditions 38–40. We
should also note that current evidence from genome-wide association studies do not
support the presence of shared genetic polymorphisms between RA and COPD.8,42 A
previous study showed that RA, besides increasing the risk for COPD, also facilitates a
shortening of time course for developing COPD.
COPD is associated with systemic oxidative stress, activation of circulating
inflammatory cells and increased plasma levels of proinflammatory cytokines, which
include CRP, interleukin-6, fibrinogen, white blood cells and TNF-α 21,43. The findings of
our umbrella review indicated that there is highly suggestive evidence for increased
levels of two markers of systemic inflammation in COPD patients, serum levels of CRP
and fibrinogen in COPD patients. Only suggestive and weak evidence was found for
elevated levels of serum leukocytes and serum TNF-α in COPD patients, respectively.
However, genetically elevated serum CRP and serum interleukin-6 were not associated
with risk for COPD based on the findings from MR studies 22–25. The findings of MR
16
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330

studies indicate that either clinical manifestations of COPD lead to an elevation of serum
CRP or the observation association is caused by confounders. 23 For the association of
fibrinogen and risk for COPD, we did not identify any MR study. This observation
indicates that inflammatory markers do not modify the risk for COPD, and probably the
elevated levels of these markers in COPD patients areis attributed to the physical course
of disease. The absence of a causal association between serum inflammatory markers and
risk for COPD does not preclude their clinical significance. These markers are useful as
prognostic indicators, as well as surrogate markers to monitor response to treatment,
rather than diagnostic tools. 23
Our umbrella review has some strengths and introduces some innovations in the field
of COPD epidemiology. First, we summarized all previously published meta-analyses of
observational studies on risk environmental factors and biomarkers affecting the risk for
COPD. Second, we applied a set of additional statistical tools (i.e., level of significance,
95% PI, and excess significance test) and methodological criteria to further examine the
robustness credibility of the associations. However, our umbrella review also has some
limitations. First, we considered only risk factors that were examined in published
systematic reviews and meta-analyses. There might be additional risk factors with
adequate number of observational studies that have not yet been considered in a meta-
analysis. Also, Egger’s test should be interpreted with caution in presence of large
between-study heterogeneity. However, it is unlikely that the credibility assessment
would be different if we did not consider the hints for small-study effects.
Conclusions
17
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352

In this umbrella review, we showed that active and passive smoking, exposure to
biomass fuels, history of tuberculosis and history of RA are associated with an increased
risk for developing COPD and these associations are supported by highly suggestive
evidence. Smokers had a 4-fold increase in the risk of developing COPD, whereas
individuals exposed to the rest of the risk factors had an at least 2-fold increase in the risk
for COPD. Also, we found that serum CRP and serum fibrinogen are increased in patients
with COPD. From the perspective of public health, the prevention of exposure to noxious
particles through tobacco control, and avoidance of indoor air pollution through exposure
to biomass fuels is the most appropriate strategy for the prevention of COPD. Also, in
developing countries, population-wide public health interventions to control tuberculosis
could be an additional approach towards the prevention of COPD. There is a need for
more research on protective factors that might prevent or delay the ons et of COPD in
high-risk populations. Given the chronic course and the debilitating property of COPD,
the identification of risk factors and biomarkers could help define a high-risk population
to target for screening.
18
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368

References
1. Barnes PJ, Shapiro SD, Pauwels RA. Chronic obstructive pulmonary disease:
molecular and cellular mechanisms. Eur Respir J [Internet]. 2003 Oct;22(4):672–
88. Available from: http://www.ncbi.nlm.nih.gov/pubmed/14582923
2. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers.
Lancet (London, England) [Internet]. 2009 Aug 29;374(9691):733–43. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/19716966
3. Adeloye D, Chua S, Lee C, Basquill C, Papana A, Theodoratou E, et al. Global
and regional estimates of COPD prevalence: Systematic review and meta-analysis.
J Glob Health [Internet]. 2015 Dec;5(2):20415. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/26755942
4. Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD
surveillance--United States, 1999-2011. Chest [Internet]. 2013 Jul;144(1):284–
305. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23619732
5. Kochanek KD, Murphy SL, Xu J, Arias E. Mortality in the United States 2013.
Hyattsville, MD, MD; 2014.
6. Ford ES, Murphy LB, Khavjou O, Giles WH, Holt JB, Croft JB. Total and state-
specific medical and absenteeism costs of COPD among adults aged ≥ 18 years in
the United States for 2010 and projections through 2020. Chest [Internet]. 2015
Jan;147(1):31–45. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/25058738
19
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389

7. Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease.
Lancet (London, England) [Internet]. 2012 Apr 7;379(9823):1341–51. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/22314182
8. Hobbs BD, de Jong K, Lamontagne M, Bossé Y, Shrine N, Artigas MS, et al.
Genetic loci associated with chronic obstructive pulmonary disease overlap with
loci for lung function and pulmonary fibrosis. Nat Genet [Internet]. 2017
Mar;49(3):426–32. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/28166215
9. Eisner MD, Anthonisen N, Coultas D, Kuenzli N, Perez-Padilla R, Postma D, et al.
An official American Thoracic Society public policy statement: Novel risk factors
and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit
Care Med [Internet]. 2010 Sep 1;182(5):693–718. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/20802169
10. Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic
obstructive pulmonary disease. Lancet (London, England) [Internet]. 2015 Mar
7;385(9971):899–909. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/25123778
11. Ioannidis JPA. Integration of evidence from multiple meta-analyses: a primer on
umbrella reviews, treatment networks and multiple treatments meta-analyses.
CMAJ. 2009 Oct;181(8):488–93.
12. Bellou V, Belbasis L, Tzoulaki I, Evangelou E, Ioannidis JPA. Environmental risk
factors and Parkinson’s disease: An umbrella review of meta-analyses.
20
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411

Parkinsonism Relat Disord [Internet]. 2016 Feb;23:1–9. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/26739246
13. Bellou V, Belbasis L, Tzoulaki I, Middleton LT, Ioannidis JPA, Evangelou E.
Systematic evaluation of the associations between environmental risk factors and
dementia: An umbrella review of systematic reviews and meta-analyses.
Alzheimers Dement [Internet]. 2017 Apr 4;13(4):406–18. Available from:
http://linkinghub.elsevier.com/retrieve/pii/S1552526016328539
14. Bellou V, Belbasis L, Tzoulaki I, Evangelou E. Risk factors for type 2 diabetes
mellitus: An exposure-wide umbrella review of meta-analyses. PLoS One
[Internet]. 2018;13(3):e0194127. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/29558518
15. Lawlor DA, Tilling K, Davey Smith G. Triangulation in aetiological
epidemiology. Int J Epidemiol [Internet]. 2017 Jan 20;dyw314. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/28108528
16. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected
by a simple, graphical test. BMJ. 1997 Sep;315(7109):629–34.
17. Ioannidis JPA, Trikalinos TA. An exploratory test for an excess of significant
findings. Clin Trials. 2007 Jan;4(3):245–53.
18. Hu G, Zhou Y, Tian J, Yao W, Li J, Li B, et al. Risk of COPD from exposure to
biomass smoke: a metaanalysis. Chest [Internet]. 2010 Jul;138(1):20–31.
Available from: http://www.ncbi.nlm.nih.gov/pubmed/20139228
21
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432

19. Byrne AL, Marais BJ, Mitnick CD, Lecca L, Marks GB. Tuberculosis and chronic
respiratory disease: a systematic review. Int J Infect Dis [Internet]. 2015
Mar;32:138–46. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25809770
20. Ungprasert P, Srivali N, Cheungpasitporn W, Davis Iii JM. Risk of incident
chronic obstructive pulmonary disease in patients with rheumatoid arthritis: A
systematic review and meta-analysis. Joint Bone Spine [Internet]. 2016
May;83(3):290–4. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/26709254
21. Gan WQ, Man SFP, Senthilselvan A, Sin DD. Association between chronic
obstructive pulmonary disease and systemic inflammation: a systematic review
and a meta-analysis. Thorax [Internet]. 2004 Jul;59(7):574–80. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/15223864
22. van Durme YMTA, Verhamme KMC, Aarnoudse A-JLHJ, Van Pottelberge GR,
Hofman A, Witteman JCM, et al. C-reactive protein levels, haplotypes, and the
risk of incident chronic obstructive pulmonary disease. Am J Respir Crit Care Med
[Internet]. 2009 Mar 1;179(5):375–82. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/19096002
23. Dahl M, Vestbo J, Zacho J, Lange P, Tybjærg-Hansen A, Nordestgaard BG. C
reactive protein and chronic obstructive pulmonary disease: a Mendelian
randomisation approach. Thorax [Internet]. 2011 Mar;66(3):197–204. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/21059738
24. van Durme YMTA, Lahousse L, Verhamme KMC, Stolk L, Eijgelsheim M, Loth
22
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454

DW, et al. Mendelian randomization study of interleukin-6 in chronic obstructive
pulmonary disease. Respiration [Internet]. 2011;82(6):530–8. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/21997388
25. Wium-Andersen MK, Orsted DD, Nordestgaard BG. Elevated C-reactive protein,
depression, somatic diseases, and all-cause mortality: a mendelian randomization
study. Biol Psychiatry [Internet]. 2014 Aug 1;76(3):249–57. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24246360
26. Fulton AS, Hill AM, Williams MT, Howe PRC, Coates AM. Paucity of evidence
for a relationship between long-chain omega-3 fatty acid intake and chronic
obstructive pulmonary disease: a systematic review. Nutr Rev [Internet]. 2015
Sep;73(9):612–23. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/26185126
27. Fonseca Wald ELA, van den Borst B, Gosker HR, Schols AMWJ. Dietary fibre
and fatty acids in chronic obstructive pulmonary disease risk and progression: a
systematic review. Respirology [Internet]. 2014 Feb;19(2):176–84. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/24372903
28. Doust E, Ayres JG, Devereux G, Dick F, Crawford JO, Cowie H, et al. Is pesticide
exposure a cause of obstructive airways disease? Eur Respir Rev [Internet]. 2014
Jun;23(132):180–92. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24881073
29. Campbell B, Davis SR, Abramson MJ, Mishra G, Handelsman DJ, Perret JL, et al.
Menopause, lung function and obstructive lung disease outcomes: a systematic
23
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476

review. Climacteric [Internet]. 2018 Feb;21(1):3–12. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/29106307
30. Fontana L, Lee S-J, Capitanelli I, Re A, Maniscalco M, Mauriello MC, et al.
Chronic Obstructive Pulmonary Disease in Farmers: A Systematic Review. J
Occup Environ Med [Internet]. 2017 Aug;59(8):775–88. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/28594705
31. Borup H, Kirkeskov L, Hanskov DJA, Brauer C. Systematic review: chronic
obstructive pulmonary disease and construction workers. Occup Med (Lond)
[Internet]. 2017 Apr 1;67(3):199–204. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/28204712
32. Gershon AS, Dolmage TE, Stephenson A, Jackson B. Chronic obstructive
pulmonary disease and socioeconomic status: a systematic review. COPD
[Internet]. 2012 Jun;9(3):216–26. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/22497534
33. From the Global Strategy for the Diagnosis, Management and Prevention of
COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017
[Internet]. 2017. Available from: http://goldcopd.org
34. Jayes L, Haslam PL, Gratziou CG, Powell P, Britton J, Vardavas C, et al.
SmokeHaz: Systematic Reviews and Meta-analyses of the Effects of Smoking on
Respiratory Health. Chest [Internet]. 2016 Jul;150(1):164–79. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/27102185
35. Assad NA, Kapoor V, Sood A. Biomass smoke exposure and chronic lung disease.
24
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498

Curr Opin Pulm Med [Internet]. 2016 Mar;22(2):150–7. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/26814722
36. Chakrabarti B, Calverley PMA, Davies PDO. Tuberculosis and its incidence,
special nature, and relationship with chronic obstructive pulmonary disease. Int J
Chron Obstruct Pulmon Dis [Internet]. 2007;2(3):263–72. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/18229564
37. Menezes AMB, Hallal PC, Perez-Padilla R, Jardim JRB, Muiño A, Lopez M V, et
al. Tuberculosis and airflow obstruction: evidence from the PLATINO study in
Latin America. Eur Respir J [Internet]. 2007 Dec;30(6):1180–5. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/17804445
38. Shen T-C, Lin C-L, Chen C-H, Tu C-Y, Hsia T-C, Shih C-M, et al. Increased risk
of chronic obstructive pulmonary disease in patients with rheumatoid arthritis: a
population-based cohort study. QJM [Internet]. 2014 Jul;107(7):537–43. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/24497528
39. Di Giuseppe D, Discacciati A, Orsini N, Wolk A. Cigarette smoking and risk of
rheumatoid arthritis: a dose-response meta-analysis. Arthritis Res Ther [Internet].
2014 Mar 5;16(2):R61. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24594022
40. Sugiyama D, Nishimura K, Tamaki K, Tsuji G, Nakazawa T, Morinobu A, et al.
Impact of smoking as a risk factor for developing rheumatoid arthritis: a meta-
analysis of observational studies. Ann Rheum Dis [Internet]. 2010 Jan;69(1):70–
81. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19174392
25
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520

41. Sparks JA, Lin T-C, Camargo CA, Barbhaiya M, Tedeschi SK, Costenbader KH,
et al. Rheumatoid arthritis and risk of chronic obstructive pulmonary disease or
asthma among women: A marginal structural model analysis in the Nurses’ Health
Study. Semin Arthritis Rheum [Internet]. 2018 Apr;47(5):639–48. Available from:
http://linkinghub.elsevier.com/retrieve/pii/S0049017217303827
42. Okada Y, Wu D, Trynka G, Raj T, Terao C, Ikari K, et al. Genetics of rheumatoid
arthritis contributes to biology and drug discovery. Nature [Internet]. 2014 Feb
20;506(7488):376–81. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24390342
43. Sinden NJ, Stockley RA. Systemic inflammation and comorbidity in COPD: a
result of “overspill” of inflammatory mediators from the lungs? Review of the
evidence. Thorax [Internet]. 2010 Oct;65(10):930–6. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/20627907
44. Alif SM, Dharmage SC, Bowatte G, Karahalios A, Benke G, Dennekamp M, et al.
Occupational exposure and risk of chronic obstructive pulmonary disease: a
systematic review and meta-analysis. Expert Rev Respir Med [Internet]. 2016
Aug;10(8):861–72. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/27187563
45. Schikowski T, Adam M, Marcon A, Cai Y, Vierkötter A, Carsin AE, et al.
Association of ambient air pollution with the prevalence and incidence of COPD.
Eur Respir J [Internet]. 2014 Sep;44(3):614–26. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24488569
26
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542

46. Zhu B, Zhu B, Xiao C, Zheng Z. Vitamin D deficiency is associated with the
severity of COPD: a systematic review and meta-analysis. Int J Chron Obstruct
Pulmon Dis [Internet]. 2015;10:1907–16. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/26392765
47. Waziry R, Jawad M, Ballout RA, Al Akel M, Akl EA. The effects of waterpipe
tobacco smoking on health outcomes: an updated systematic review and meta-
analysis. Int J Epidemiol [Internet]. 2016 Apr 13;dyw021. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/27075769
48. Zhu M, Wang T, Wang C, Ji Y. The association between vitamin D and COPD
risk, severity, and exacerbation: an updated systematic review and meta-analysis.
Int J Chron Obstruct Pulmon Dis [Internet]. 2016;11:2597–607. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/27799758
27
543
544
545
546
547
548
549
550
551
552
553
554
555
556

Figure. Flow chart of literature search
28
20 articles were excluded
13 were not the largest meta-analysis5 were meta-analyses with fundamental statistical errors1 was meta-analysis focused in limited geographic location1 was meta-analysis not adequately presenting the effect estimates
173 articles were excluded
22 were diagnostic, prognostic or screening studies 122 had outcomes other than risk for COPD15 were treatment studies 6 were incidence or prevalence studies8 were observational studies
1589 articles were excluded
866 were treatment studies 312 had outcomes other than risk for COPD 138 were editorials or narrative reviews 130 were articles about genetic epidemiology 40 were articles about health economics and quality of life47 were diagnostic, prognostic or screening studies31 were methodological papers22 were incidence or prevalence studies3 were observational studies
39 articles reviewed by full text screening
19 eligible articles published until December 31, 2017
212 articles reviewed by abstract screening
1801 articles reviewed by title screening
557
558
559
560
561

Table 1. Characteristics of 18 associations of risk factors for chronic obstructive pulmonary disease.
Reference Risk factor Level of comparison
N cases/ N controls
N studies
Effect size
metric
RE summary effect size (95%
CI)P random
95% prediction
intervalI2
Small-study effects/Excess significance
bias
Credibility
Alif, 2016 44 Biological dust High vs. low exposure 2732/19,367 5 OR 0.99 (0.75 – 1.31) 0.935 0.48 – 2.04 31 No/No NS
Alif, 2016 44 Gases or fumes
High vs. low exposure 2732/19,367 5 OR 1.03 (0.73 – 1.45) 0.886 0.36 – 2.95 59.
6 No/No NS
Alif, 2016 44 Mineral dust High vs. low exposure 2732/19,367 5 OR 0.97 (0.68 – 1.39) 0.874 0.32 – 2.96 61.
1 No/No NS
Byrne, 2015 19 History of tuberculosis Yes vs. no 3682/52,140 8 OR 3.10 (2.24 – 4.31) 1.22 × 10-11 1.10 – 8.75 76 Yes/No Highly
suggestive
Eisner, 2010 9 Second-hand smoking Yes vs. no 3206/88,952 12 OR 1.56 (1.40 – 1.74) 3.48 × 10-16 1.23 – 1.99 27.
2 Yes/Yes Highly suggestive
Gan, 2004 21 Serum CRP High vs. low levels 2877/8885 5 OR 2.33 (1.73 – 3.14) 2.17 × 10-8 0.96 – 5.67 63.
4 No/No Highly suggestive
Gan, 2004 21 Serum leukocytes
High vs. low levels 2715/8795 3 OR 2.23 (1.44 – 3.44) 3.01 × 10-4 0.02 – 322.54 83 No/No Suggestive
Gan, 2004 21 Serum TNFα High vs. low levels 116/71 4 OR 2.96 (1.71 – 5.12) 1.00 × 10-4 0.89 – 9.85 0 No/No Weak
Gan, 2004 21 Serum fibrinogen
High vs. low levels 4279/4752 4 OR 2.42 (1.78 – 3.28) 1.33 × 10-8 0.64 – 9.21 89.
1 No/No Highly suggestive
Hu, 2010 18 Biomass fuels smoking Yes vs. no 3501/36,295 15 OR 2.37 (1.72 – 3.26) 1.25 × 10-7 0.72 – 7.75 83.
6 Yes/Yes Highly suggestive
Jayes, 2016 34 Tobacco smoking
Ever vs. never smokers
6238/105,517 22 OR 3.90 (3.08 – 4.94) 1.52 × 10-29 1.40 – 10.86 89.5 No/No Highly
suggestive
Schikowski, 2014 45
Traffic intensity on nearest road
Per 5,000 vehicles/day increase
100/3378 4 OR 1.30 (0.92 – 1.82) 0.135 0.61 – 2.73 0 No/NA NS
Schikowski, 2014 45
Traffic load on major roads within 100 m
Per 500,000 vehicles/day increase
100/3378 4 OR 1.26 (0.95 – 1.70) 0.103 0.68 – 2.33 0 No/NA NS
Ungprasert, 2016 46
History of psoriasis Yes vs. no NA/NA 7 OR 1.45 (1.21 – 1.73) 4.40 × 10-5 0.80 – 2.61 91 Yes/NA Suggestive
29
562
563

Reference Risk factor Level of comparison
N cases/ N controls
N studies
Effect size
metric
RE summary effect size (95%
CI)P random
95% prediction
intervalI2
Small-study effects/Excess significance
bias
Credibility
Ungprasert, 2016 20
History of rheumatoid arthritis
Yes vs. no NA/NA 4 OR 1.99 (1.61 – 2.45) 1.67 × 10-10 0.80 – 4.92 80.5 No/NA Highly
suggestive
Waziry, 2016 47 Waterpipe smoking
Ever vs. never 2150/63,628 4 OR 3.18 (1.25 – 8.09) 0.015 0.04 – 241.36 95.
2 No/No Weak
Zhu, 2015 48 Serum vitamin D
High vs. low levels 1981/1283 13 OR 0.29 (0.16 – 0.51) 1.65 × 10-5 0.03 – 2.80 94 Yes/Yes Suggestive
Zhu, 2015 48 Vitamin D deficiency Yes vs. no 3312/6918 12 OR 1.77 (1.18 – 2.64) 0.006 0.47 – 6.65 83.
1 No/Yes Weak
CI: confidence interval, CRP: C-reactive protein, OR: odds ratio, NS: not significant, P random: P value under random-effects model, TNF: Tumor necrosis factor
30
564565
566
567

Table 2: Sensitivity analysis of prospective cohort studies for associations with convincing or highly suggestive evidence
Reference Risk factor Level of comparison
N cases/ N controls
N studies
Effect size
metric
RE summary effect size (95%
CI)P random
95% prediction
intervalI2 Credibility
Jayes, 2016 34 Tobacco smoking
Ever vs. never smokers
6238/105,517 18 OR 4.28 (3.09 – 5.92) 1.77 × 10-18 1.11 – 16.57 90.1 Highly suggestive
Eisner, 2010 9 Second-hand smoking Yes vs. no 732/5363 3 OR 1.43 (1.24 – 1.65) 1.01 × 10-6 0.53 – 3.87 4 Weak
CI: confidence interval, OR: odds ratio, P random: P value under random-effects model
31
568
569
570
571
572