Embed Size (px)
Citation preview

Immunologic ToleranceImmunologic Tolerance
ContentsContents
• Part Part Ⅰ IntroductionⅠ Introduction• Part Ⅱ Development of Immunologic Part Ⅱ Development of Immunologic
ToleranceTolerance• Part Part Ⅲ Mechanism of Ⅲ Mechanism of Immunologic Immunologic
ToleranceTolerance• Part Ⅳ Part Ⅳ Immunologic Tolerance and Clinic Immunologic Tolerance and Clinic
MedicineMedicine
• Definition: A type of specific unresponsiveness to an antigen induced by the exposure of specific lymphocytes to that antigen, but response to other antigens normally.
• Tolerogens: antigens that induce tolerance
Part Part Ⅰ IntroductionⅠ Introduction
General features of Immunologic tolerance
• Tolerance is antigenic specific and results from the recognition of antigens by specific lymphocytes.
• Normal individuals are tolerant of their own antigens(self antigen)----- Self-tolerance.
• Foreign antigens may be administered in ways that preferentially inhibit immune response by inducing tolerance in specific lymphocytes---antigen induction.
Immunologic features of toleranceImmunologic features of tolerance
It is an antigen-induced, active process Like immunologic memory, it is antigen specific Like immunologic memory, it can exist in B cells,
T cells or both Like immunologic memory, its easier to induce
and lasts longer in T cells than in B cell
It is an antigen-induced, active process Like immunologic memory, it is antigen specific Like immunologic memory, it can exist in B cells,
T cells or both Like immunologic memory, its easier to induce
and lasts longer in T cells than in B cell

Difference of Immuologic tolerance & immunodeficiency, immu
nosuppressionImmunodeficiency: any condition in which there
is deficiency in the production of humoral and /or cell-mediated immunity---non-specificity to Ag
Immunosuppression: The suppression of immune responses to antigens. This can be achieved by various means, including physical, chemical----non-specificity to Ag

Part Ⅱ Development of Part Ⅱ Development of Immunologic ToleranceImmunologic Tolerance
• Owen first observed immunologic tolerance to allogenic antigen in fetal period in 1945
1. Induction of immunologic tolerance to antigen in fetal period and neonate period
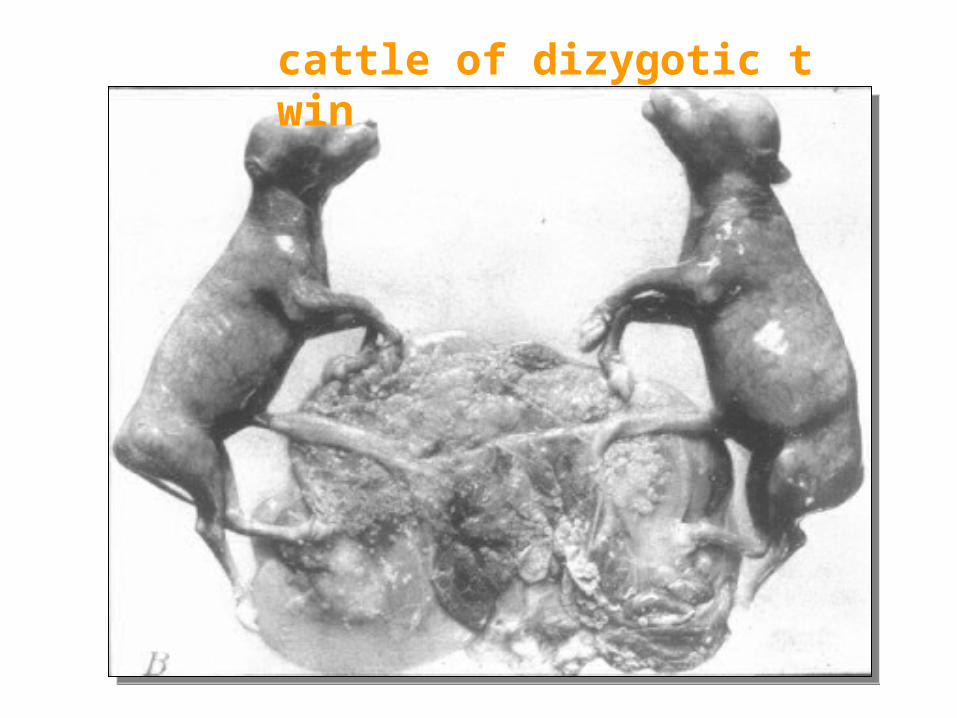
cattle of dizygotic twin
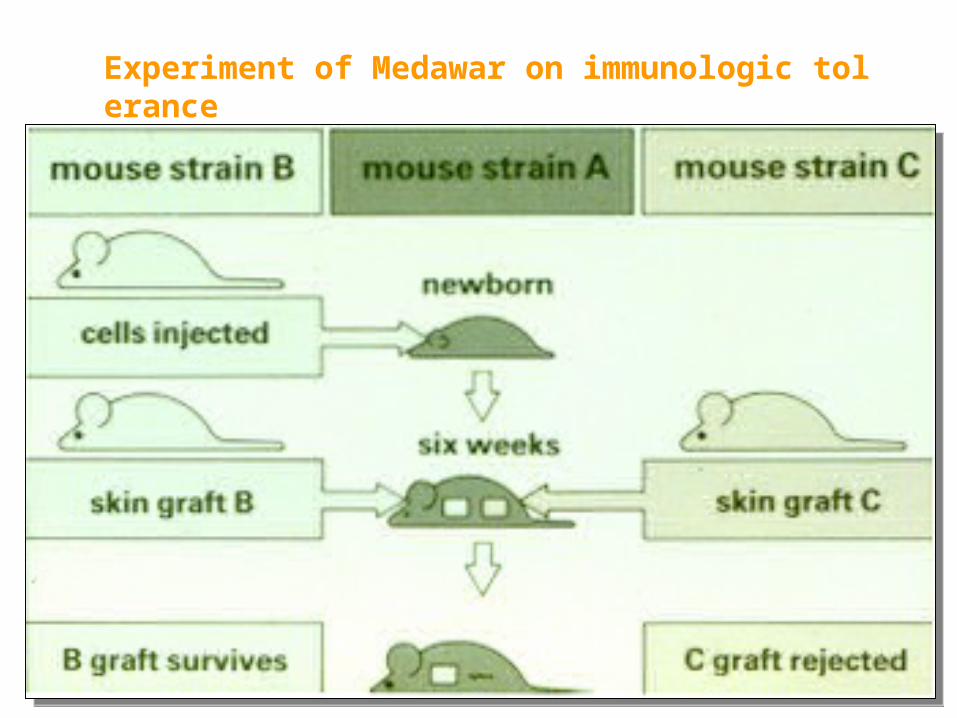
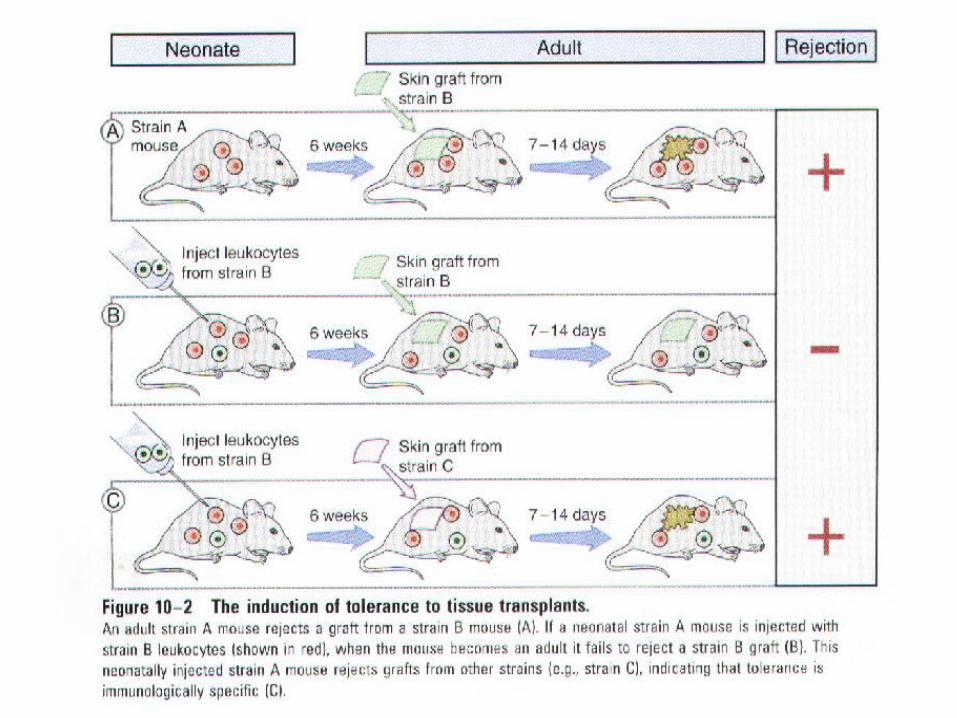
Experiment of Medawar on immunologic tolerance
2. Induction of immunologic tolerance to
antigen in adult
Antigen and immunologic tolerance:
• Concentration of antigens
• Type of antigen: monomer, aggregates
• Pathway of antigen entering body
• Features of determinant: tolerogenic epitope
• Variation of antigen
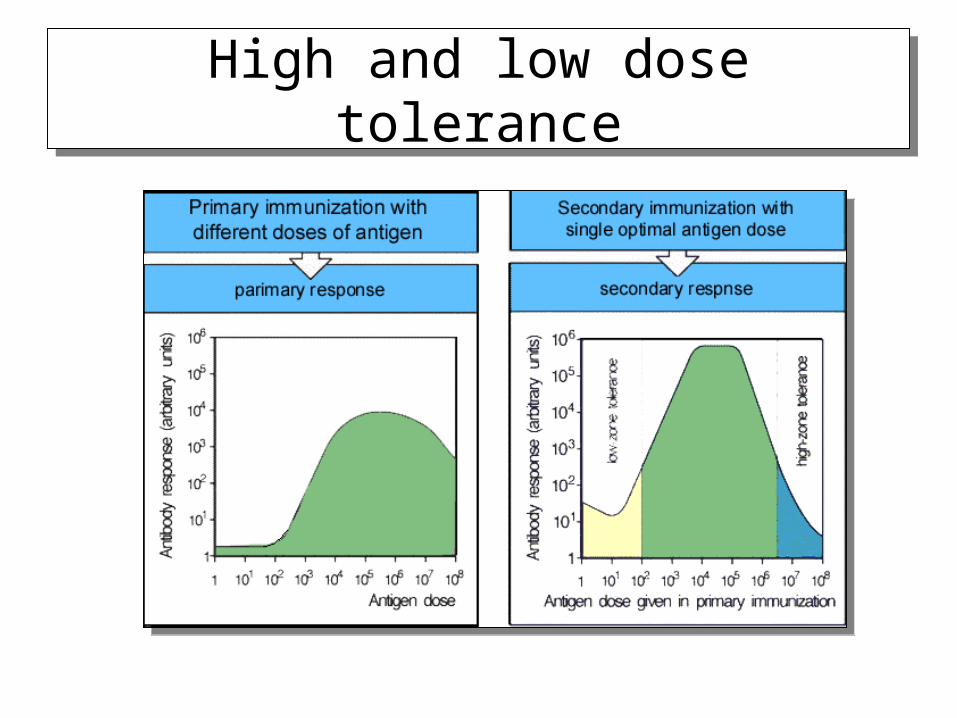
High and low dose toleranceHigh and low dose tolerance
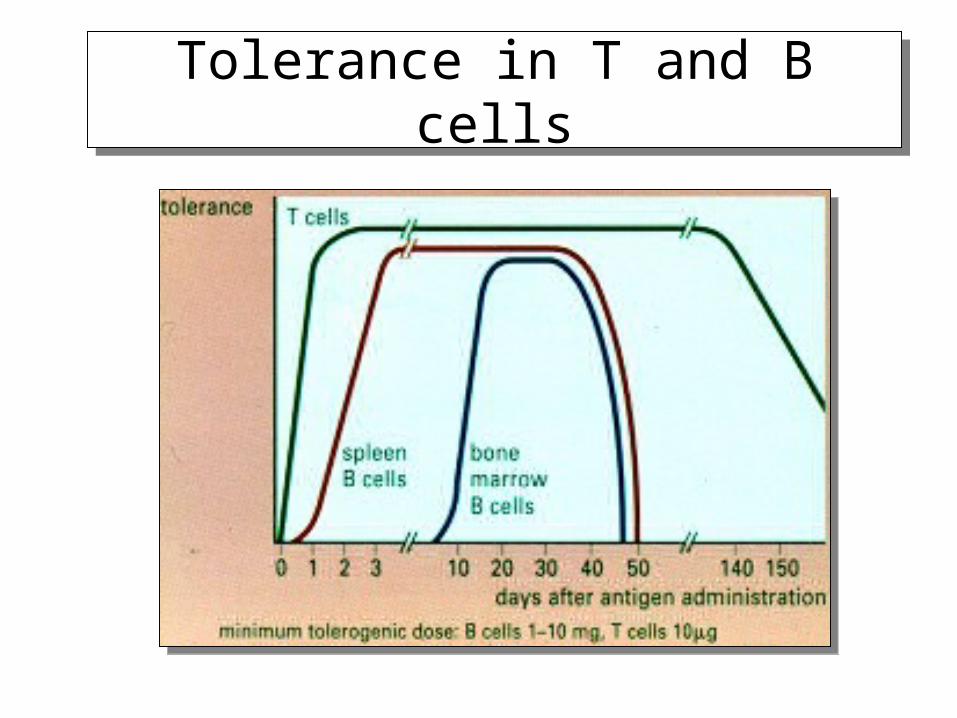
Tolerance in T and B cellsTolerance in T and B cells
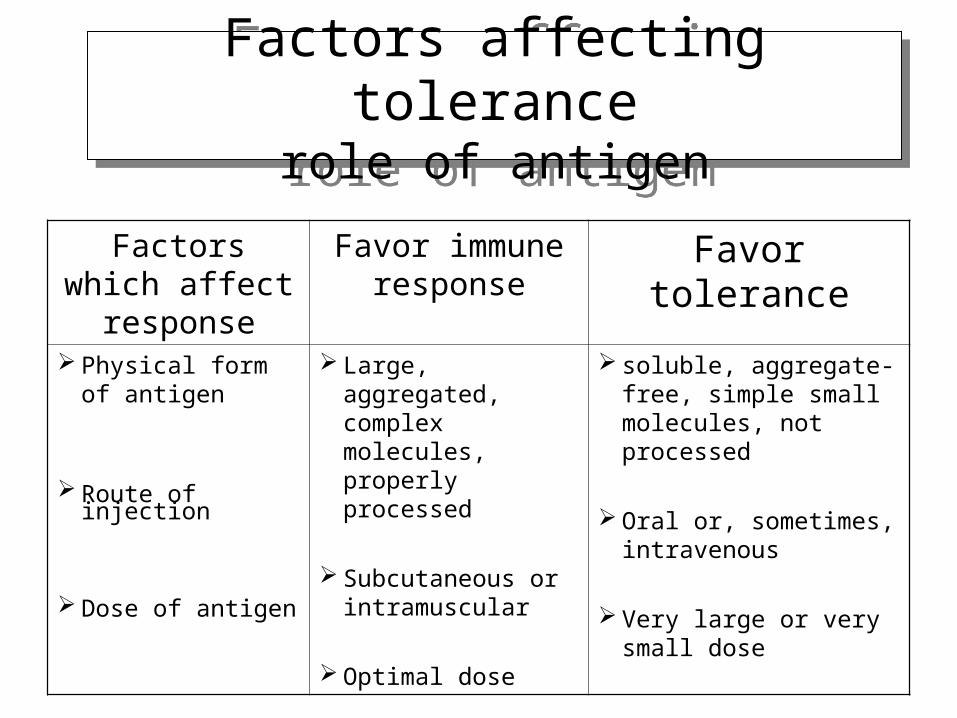
Factors affecting tolerancerole of antigen
Factors affecting tolerancerole of antigen
Factors which affect response
Favor immune response
Favor tolerance
Physical form of antigen
Route of injection
Dose of antigen
Large, aggregated, complex molecules, properly processed
Subcutaneous or intramuscular
Optimal dose
soluble, aggregate-free, simple small molecules, not processed
Oral or, sometimes, intravenous
Very large or very small dose
Individual and immunologic tolerance:
Heredity, Age, Gender, Health
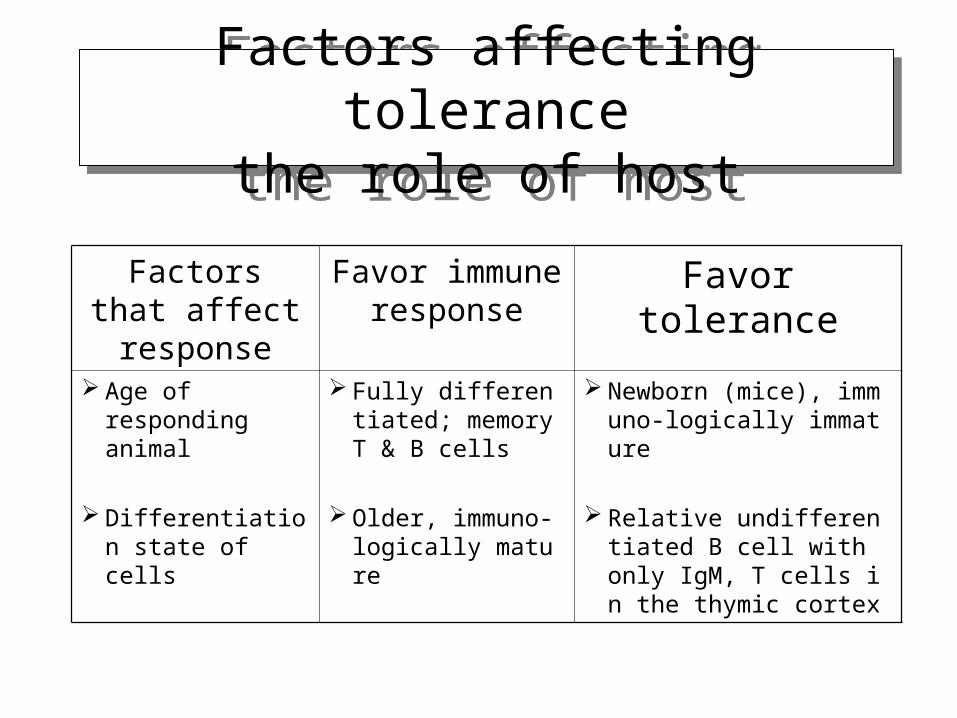
Factors affecting tolerancethe role of host
Factors affecting tolerancethe role of host
Factors that affect response
Favor immune response
Favor tolerance
Age of responding animal
Differentiation state of cells
Fully differentiated; memory T & B cells
Older, immuno-logically mature
Newborn (mice), immuno-logically immature
Relative undifferentiated B cell with only IgM, T cells in the thymic cortex
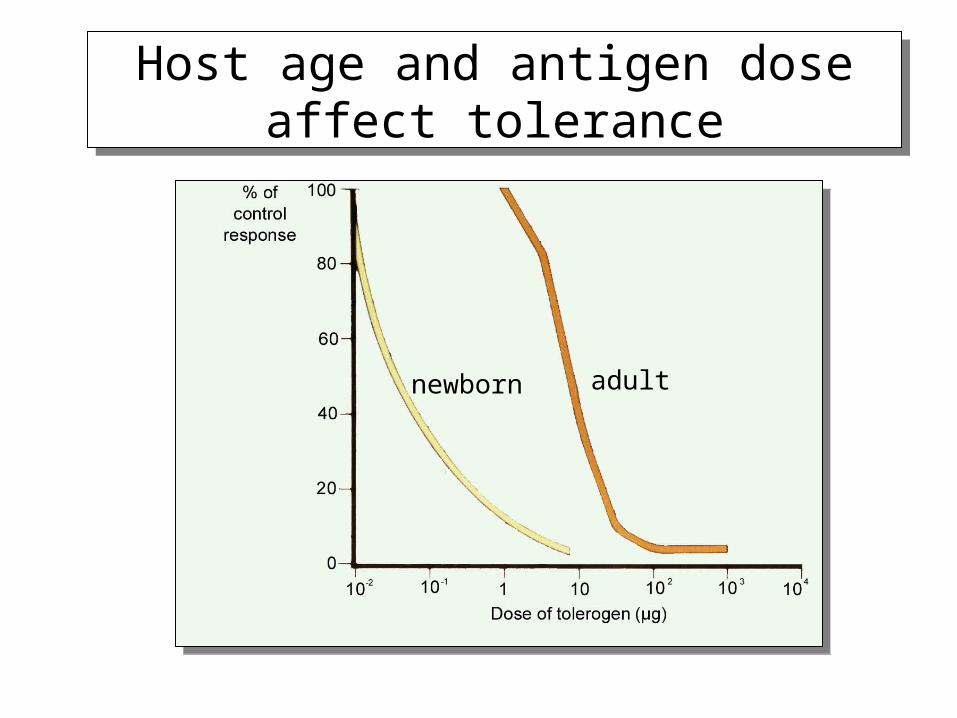
Host age and antigen dose affect tolerance
Host age and antigen dose affect tolerance
newborn adult

Part Part Ⅲ Mechanism of Ⅲ Mechanism of Immunologic ToleranceImmunologic Tolerance
1. Central tolerance: Central tolerance occurs in the central
lymphoid organs as a consequence of immature self-reactive lymphocytes recognizing ubiquitous self-antigen.
2. Peripheral tolerance: tolerance was induced in peripheral organs
as a result of mature self-reactive lymphocytes encountering tissue-specific self antigens under particular conditions

1. Central tolerance
Clonal deletion (apoptotic cell death)
During maturation of lymphocytes in the thymus for T cell or in the bone marrow for B maturation, immature lymphocytes that recognize ubiquitous self-antigen with high affinity are deleted by negative selection

Clonal deletion:negative selection of T cells in the thymus
Clonal deletion:negative selection of T cells in the thymus
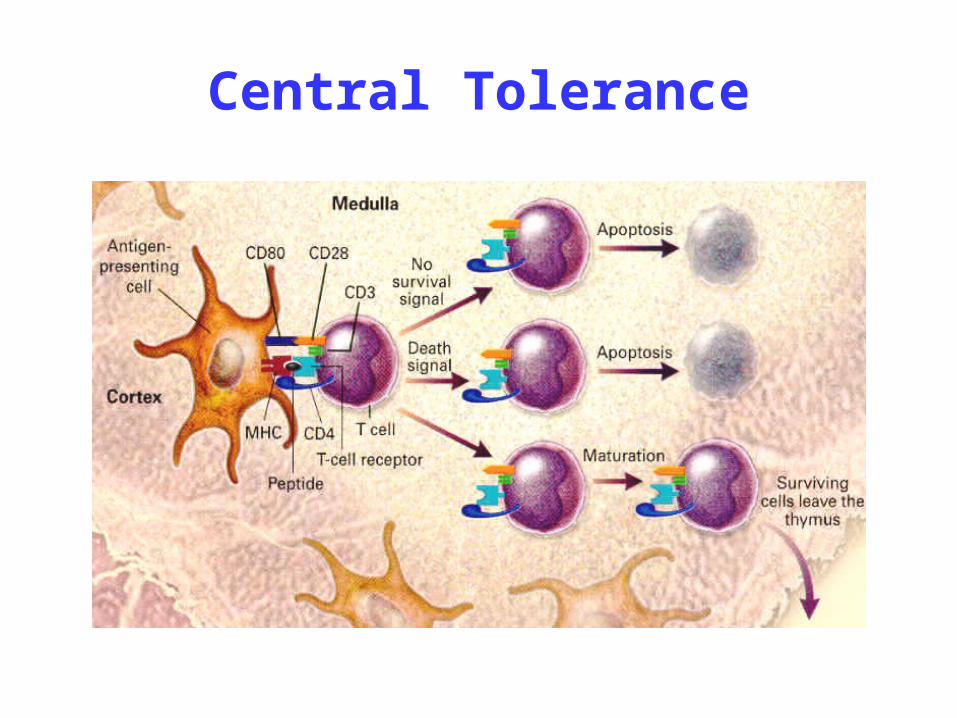
Central Tolerance
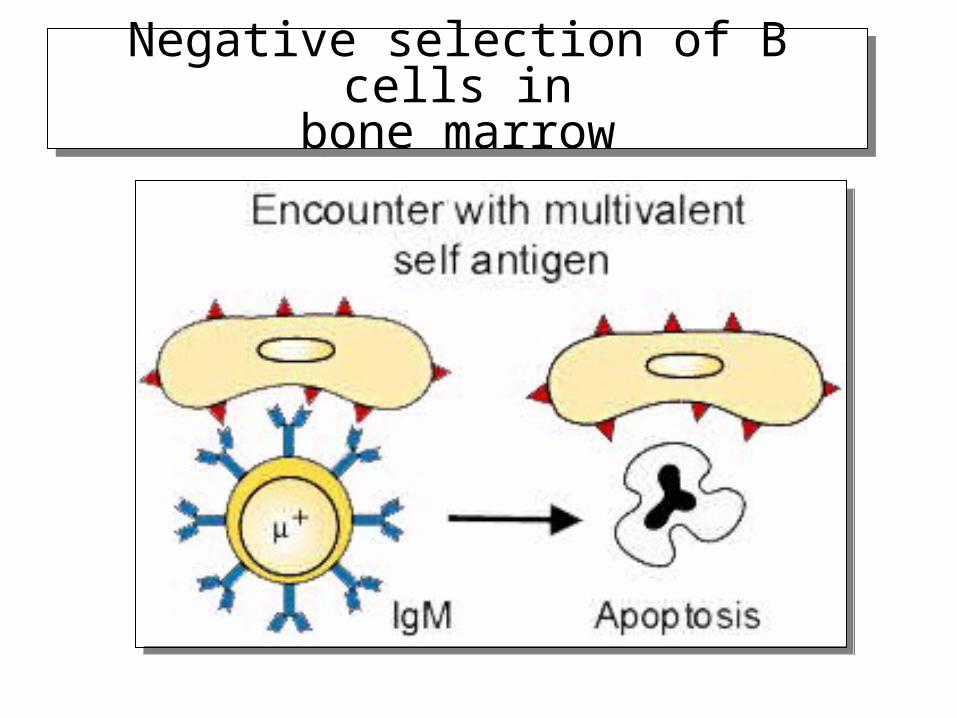
Negative selection of B cells inbone marrow
Negative selection of B cells inbone marrow
2. Peripheral tolerance
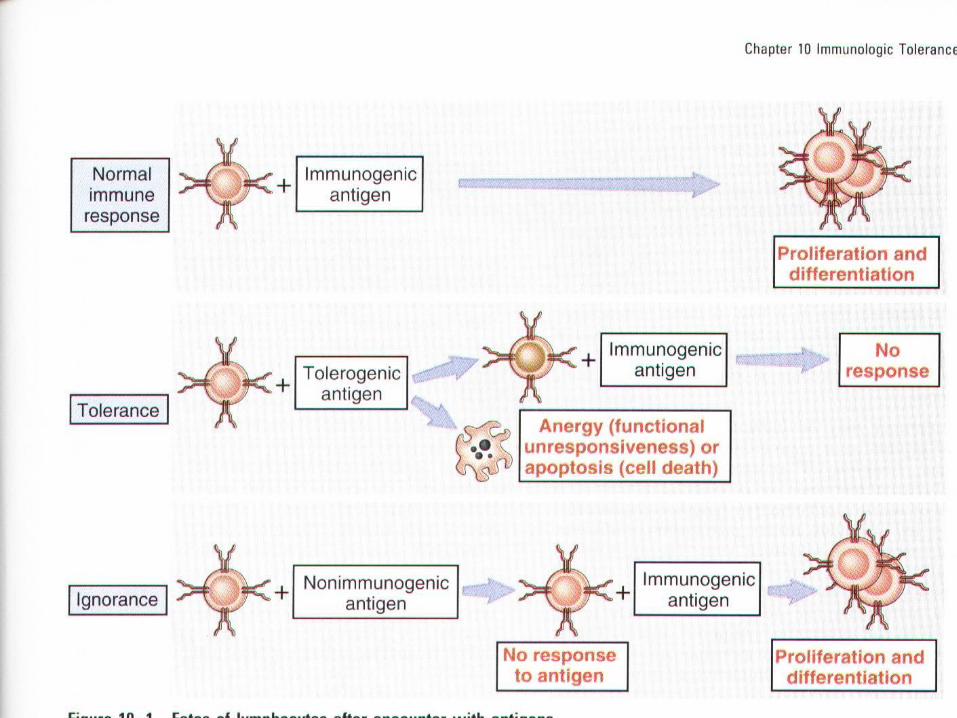
① clonal deletion and clonal ignorance:
large tissue specific antigen delete specific T cells.
self-reactive lymphocytes remain viable and functional but do not react to the self antigens in any detectable way.
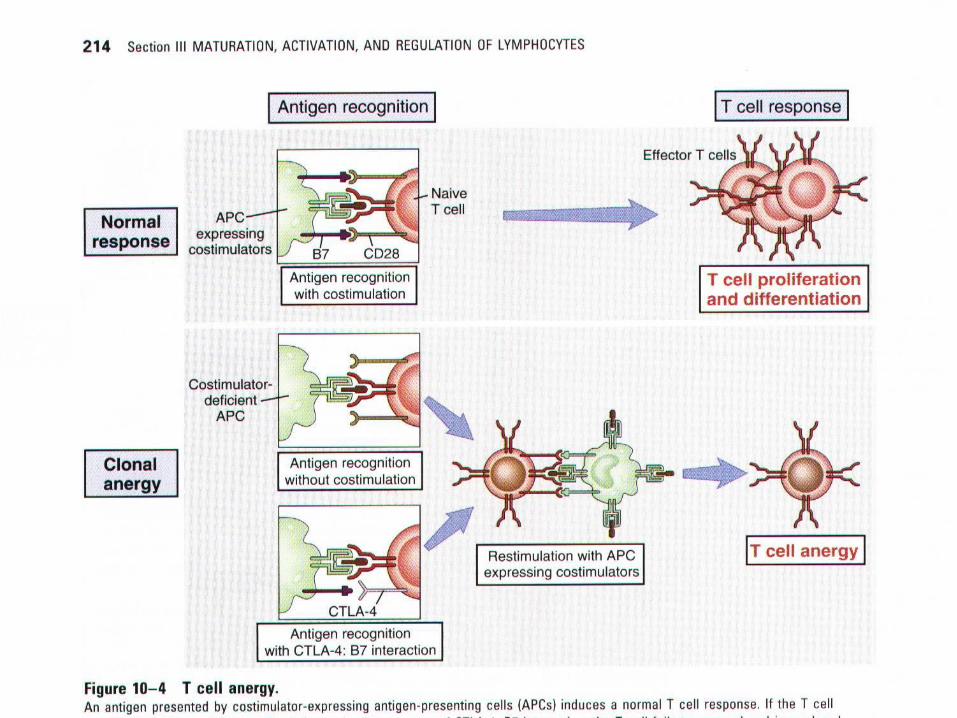
② Clonal anergy and inactivation:
functional inactivation without cell death: lack co-stimulatory signal

Clonal anergy in T cellsClonal anergy in T cells

Clonal anergy in B cellsClonal anergy in B cells

③ Action of Suppressor lymphocyte (Ts)
④ Action of cytokines: TGF- , IL-10
⑤ Holdback in signal tranduction
⑥ Immunologically privileged sites
anatomic barrier: clonal ignorance
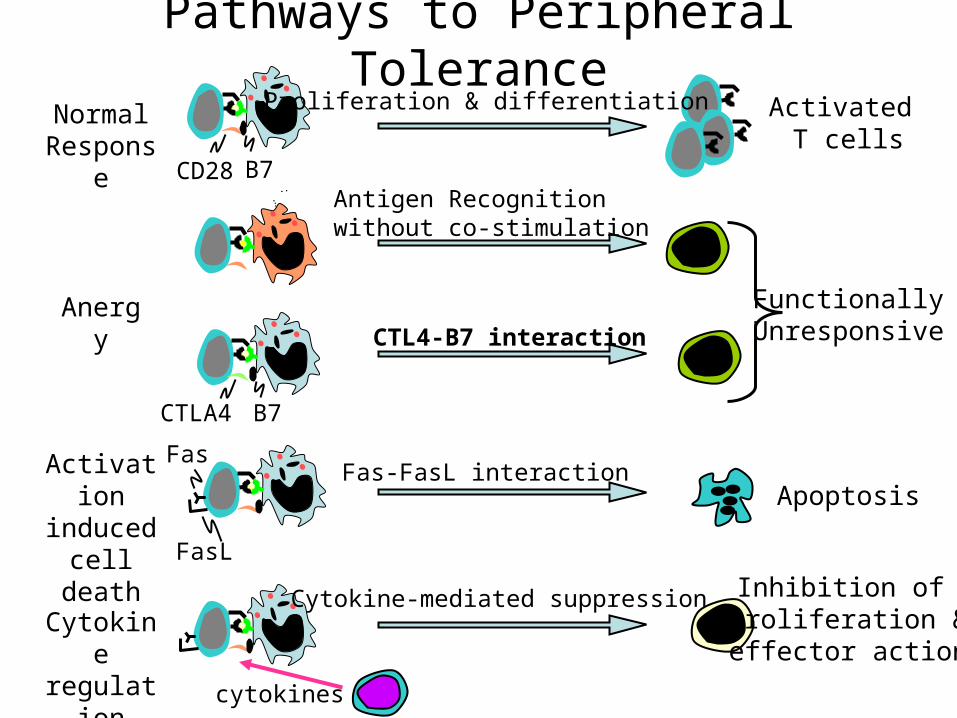
Fas
FasL
cytokines
Apoptosis
Inhibition of proliferation &effector action
Activated T cells
NormalResponse
CD28 B7
Proliferation & differentiation
Antigen Recognitionwithout co-stimulation
Anergy
CTLA4 B7
FunctionallyUnresponsiveCTL4-B7 interaction
Fas-FasL interaction
Cytokine-mediated suppression
Activation induced
cell death
Cytokine regulation
Pathways to Peripheral Tolerance
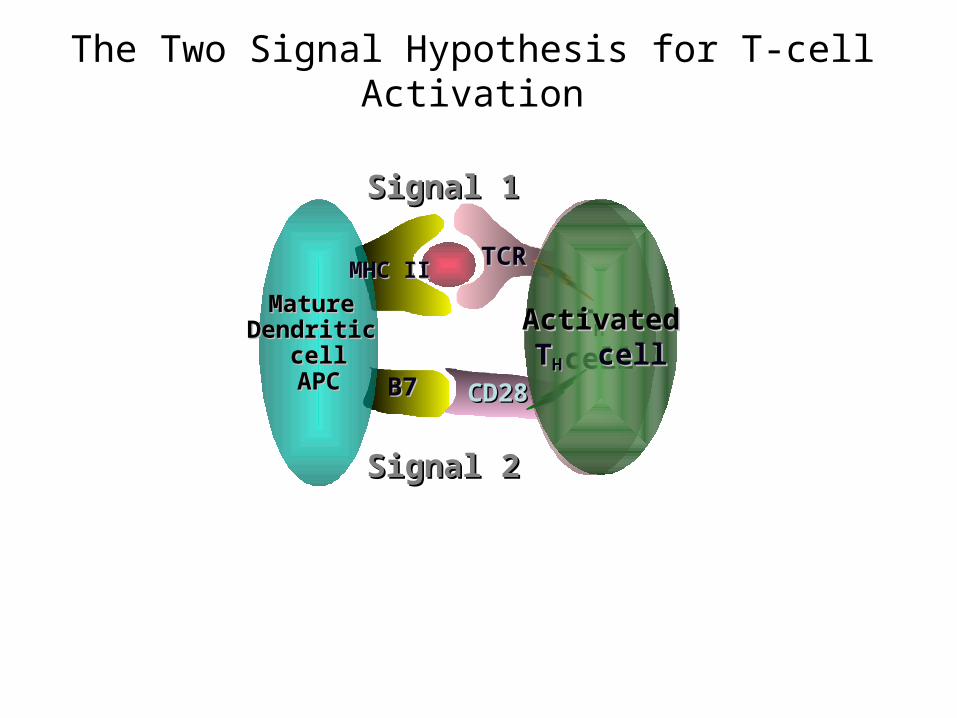
The Two Signal Hypothesis for T-cell Activation
Mature Mature Dendritic Dendritic
cellcellAPCAPC
TTHH cellcell
CD28CD28B7 B7
MHC IIMHC II TCR TCR
Signal 2Signal 2
Signal 1Signal 1
Activated Activated TTHH cell cell
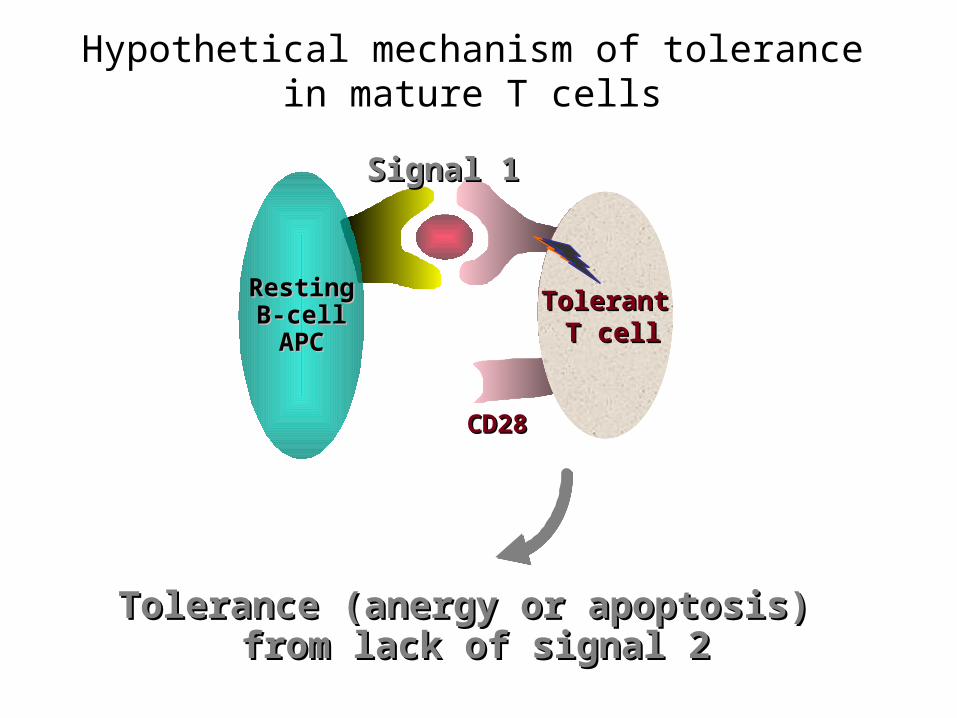
Hypothetical mechanism of tolerance in mature T cells
CD28CD28
RestingRestingB-cellB-cellAPCAPC
TTH0H0 cell cell
Tolerance (anergy or apoptosis) Tolerance (anergy or apoptosis) from lack of signal 2from lack of signal 2
Signal 1Signal 1
TolerantTolerant T cellT cell
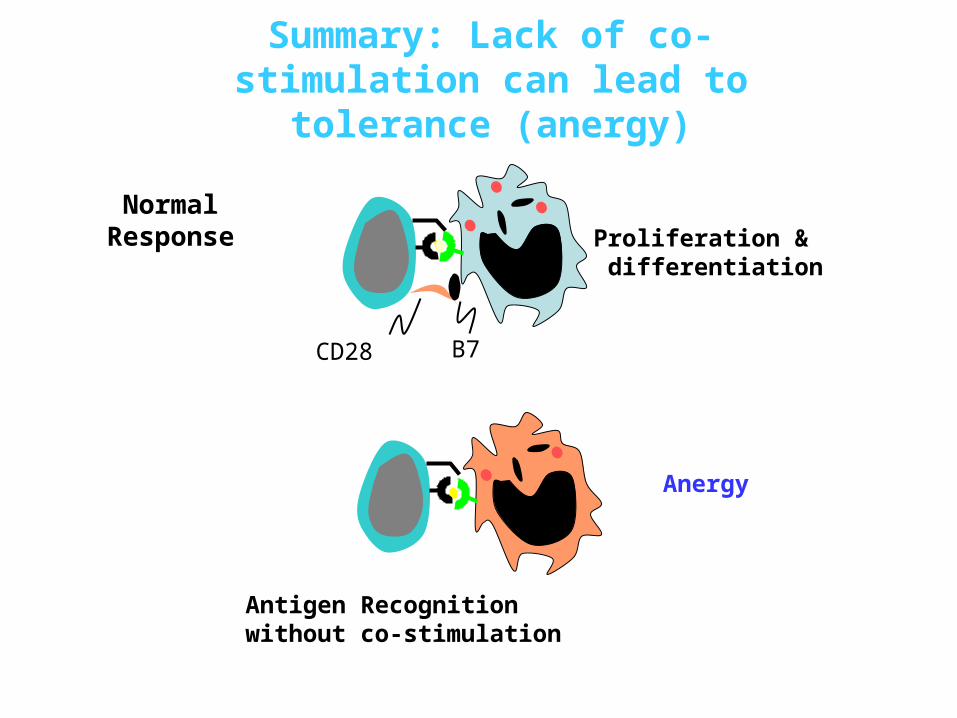
NormalResponse
CD28 B7
Proliferation & differentiation
Summary: Lack of co-stimulation can lead to tolerance (anergy)
Antigen Recognitionwithout co-stimulation
Anergy
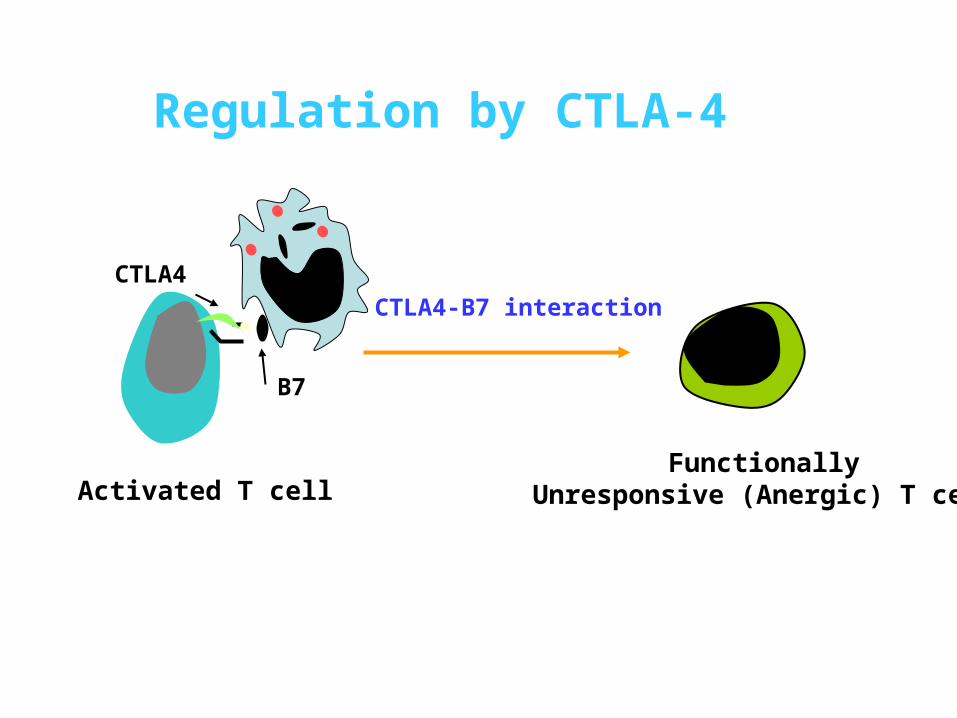
Regulation by CTLA-4
CTLA4
B7
FunctionallyUnresponsive (Anergic) T cell
CTLA4-B7 interaction
Activated T cell
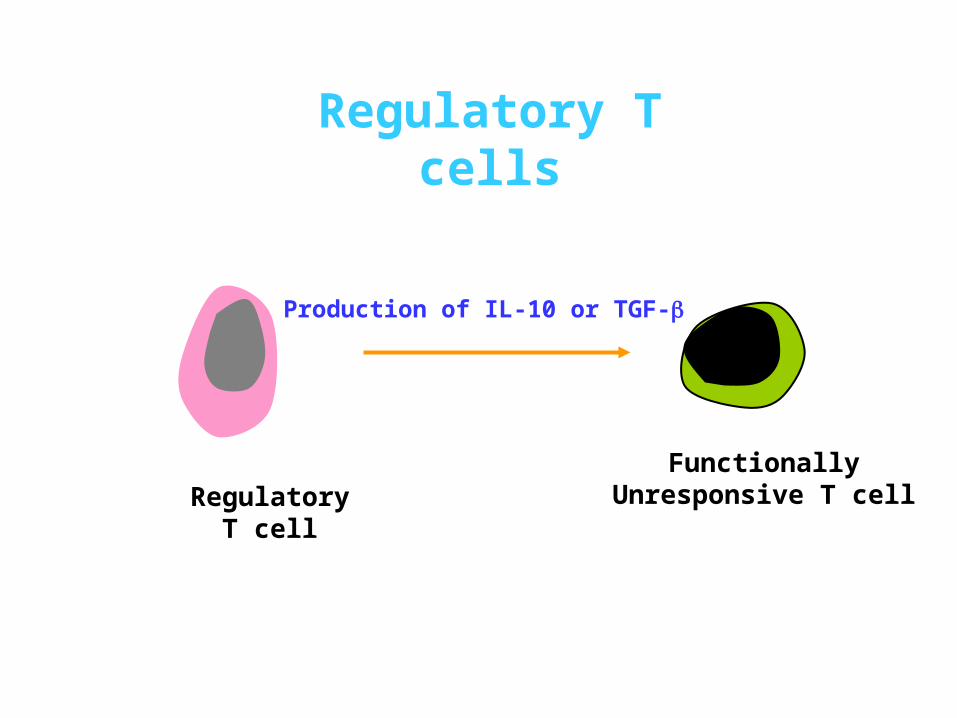
Regulatory T cells
FunctionallyUnresponsive T cell
Production of IL-10 or TGF-
RegulatoryT cell
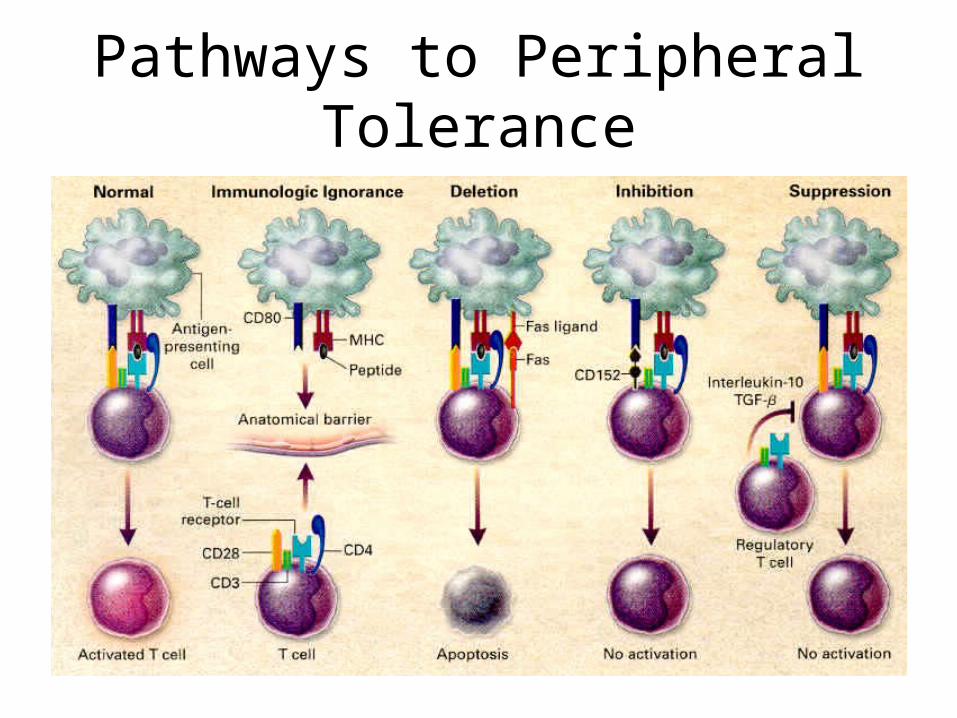
Pathways to Peripheral Tolerance
Inhibition by Antibody Feedback
• Passively administered antibody can prevent an antibody response
• Antibody produced during an immune responses leads to elimination of antigen (stimulus)–Less antigen available to stimulate specific cells–Immune complexes can bind to inhibitory receptors
Application: RhoGam for Erythroblastosis Fetalis
Major Immune Inhibitory Receptors
• B cells– FcRII
• T cells– CTLA4
• NK cells– KIR (killer cell Ig-like receptors),
Anti-Idiotypes and Immune Regulation
• Definition
– anti-idiotype response-antibody produced against immunoglobulin or TCR idiotypes that serve to down-regulate immune response
– The epitope for an responsive anti-idiotype molecule (antibody, BCR, or TCR) is the internal image formed by the CDR region of the respective epitopes antigen receptor
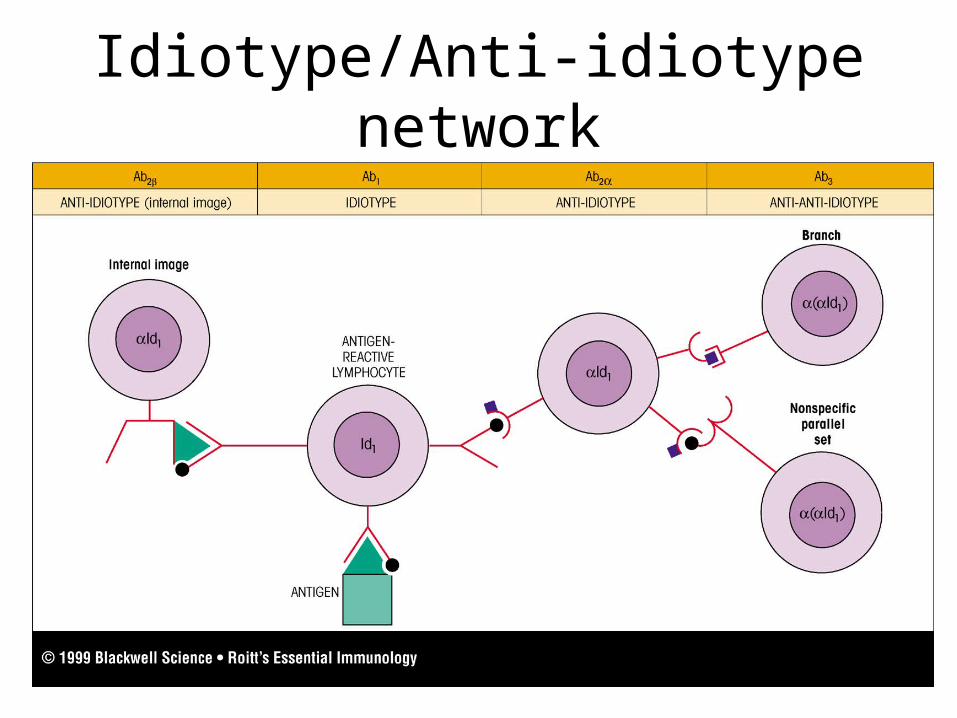
Idiotype/Anti-idiotype network
Part Ⅳ Part Ⅳ Immunologic Immunologic Tolerance and Clinic Tolerance and Clinic
MedicineMedicine
• Prevent the rejection of organ allografts and xenografts
• Treat autoimmune diseases
• Treat allergic diseases
1. To induce immunologic tolerance
2. To terminate immunologic tolerance
• To treat tumor:
enhance first signal or second signal
• To treat infection diseases
And now for a clinical case….

• 6 year old male, ER with unexplained bruising associated with minor trauma
• Patient has minimal clotting activity• FVIII levels <1% of normal
• Patient given i.v. FVIII concentrate i.v. and released but returns in two weeks with same problem• Repeated FVIII treatment
• However, FVIII is ineffective.
Patient Presentation

Issues• Coagulation factor inhibitors (anti-FVIII
activity)• Basis?
•Lack of tolerance. Why?• Prevalence/impact
•20-30% FVIII, less FIX• Treatment/problems
•FVIII concentrate or rFVIII• Inhibitors develop that neutralize FVIII• Therapy?
• Porcine FVIII with less cross-reactivity • Tolerance (high dose)• Gene therapy
What are Inhibitors?
• IgG; commonly subclass 4, mixed 1 & 4• Occur in
• Congenital factor deficiency = alloimmune
• Previously unaffected = autoimmune • Associated with pregnancy, autoimmunity,
malignancy, multi-transfusion, advanced age etc.

SummarySummary
Definition of immunologic tolerance
Features of immunologic tolerance
Induction of immunologic tolerance
Mechanism of immunologic tolerance
Clinical application of immunologic tolerance
![민사법사례연습 Ⅱ - hermesbook.ipdisk.co.krhermesbook.ipdisk.co.kr/publist/HDD1/file/9791156934431.pdf · 둘째, 사례연습[Ⅱ] 편제상 가장 큰 특징은 사례연습[Ⅰ]에](https://img.dokumen.tips/doc/110x75/5f253fe57c9d881a3d69d2fc/eee-a-e-ea-oef-e-.jpg)























![KINS발표물(백용).ppt [호환 모드] · 제제1313회회원자력안전기술정보회의원자력안전기술정보회의 목차 Ⅰ. 지하공간굴착현장조사개요 Ⅱ](https://img.dokumen.tips/doc/110x75/605c14e784e4177ee77cb7ce/kinseoeoeeeppt-eeoe-oeoe1313oeoeeeeoeeeeoe.jpg)

![[제11회원자력안전기술정보회의] 원자력발전소2차계통설비 비 ... · 2018-01-01 · 제11회원자력안전기술정보회의 1 Ⅰ. 개요 Ⅱ. 탄소강배관감육검사](https://img.dokumen.tips/doc/110x75/5ec592f09143e50e9b03ff80/oe11oeeeeoe-eeoeoe2ee-e.jpg)


