-
8/6/2019 Imaging of Vascular Complications
1/6
1285
Im ag ing o f V ascu la r C om p lica tion sA fte r H epa tic T
ransp lan ta tio n
Kenne th D a len1Deborah L . D ay1
Nancy L . A sche rD av id W . H un te r1W illia rn M . Thom
pson1
W ilfrido R . C as taneda -Zun iga1Jan is G is se l Le tou
rneau1
R ec eiv ed D ece mb er 2 , 19 87 ; a cc ep ted a fte r re -v is
io n Jan ua ry 27 , 19 88 .
Th is w ork w as sup po rte d by a re se a rch g ra n t #SM F-5
66 -87 from the M in ne so ta M ed ica l F ou nda -t ion , M in ne
apo lis , M N, 5 545 5 .
I D epartm en t o f R ad io log y , U n iv e rs ity o f M in ne
-sets Hosp ita l an d C lin ic , Bo x 29 2 UMHC , 42 0 D e l-awa re
S t. S E ., M inne apo lis , M N 55455 . Ad dressr ep ri nt r eq u
es ts t o J . G . L et ou me au .
2 D epartm en t o f Su rge ry , U n iv e rs ity o f M in ne -s o
ta H osp ita l an d C lin ic , M in ne apo lis , M N 55455 .P resen
t ad d re ss : D epa rtm en t o f S urg e ry , U nive rs ityo f C a
lifo rn ia , Sa n F ran c is co , CA 94143 .AJ R 150:1285-1290, Jun
e 19880 36 1 - 80 3X /8 8/ 1 5 06 -1 28 5 Am eric an R oen tgen R
ay So c ie ty
Vascu la r com plica tions a fte r hepa tic transp lan ta tion
can com prom ise g ra ft and pa tien tsu rv iva l. A ng iog raphy
de fines the need fo r re vascu la riza tio n o r re tran sp lan ta
tio n , bu tth e va lue o f non in vas iv e im ag ing in th is se
thng is no t c lear. T o assess the re la tive m e rito f n on in
va siv e im a gin g te chn iques (sonog raphy , sc in tig raphy , C
T , and MR ), w e re tro -spect ively re v iewed 19 m a jo r vascu
la r com p lic a tions tha t occu r r ed in 1 5 o f 98 hepa ticrec
ip ien ts o ve r a 3 /2 -y ea r p er io d . Po rta l v enous th rom
bos is w as seen in se ven p atien ts ,dono r ao rt ic o r h epat
ic a rte ria l th rom bos is in seven , and in fe rio r v ena cava
l th rom bos isin five . S onog raphy p ro v id ed th e In itia l d
ia gnos is o f por tal venous th rom bos is in th ree ,a rte ria l
c om p ro m is e in five , and cava l obs tru c tion in fou r. C T
w as th e f i rs t d iagnos t icexam ina tion to ident i ty po rta
l oc c lu sio n in tw o , dono r ao rtlc th rom bos is in one ,
andin fe rio r vena cava l th rom bos is in one . S c in tig raphy
and MR im ag ing p ro v id ed com p le -m en ta ry da ta .
B oth s on og ra ph y and C T ar e use fu l in the eva lu a tio
n o f v ascu la r com plic a tio n s th a toccu r a fte r h epatic
tra n sp lan ta tio n ; how eve r, n e ith e r is su ffic ie n tly
sens itiv e to obv ia teang io g ra ph ic as se ssm en t
Hepa tic transp lan ta tion has becom e an accep ted therapeu
tic op tion fo r m anypa tien ts w ith irre ve rs ib le liv e r fa
ilu re [1 -3 ]. H oweve r, life - th rea ten ing com plic a
tionscan a rise in hepa tic re c ip ien ts , the m ost om inous be
ing vascu la r th rom boses , asthey frequen tly requ ire im m ed
ia te in te rven tion . C lin ica l s igns o f a rte ria l th rom
bos isin c lude feve r, sep ticem ia , e le va ted se rum live r
enzym es, and de te r io ra ting coagu -la tion pa ram e te rs [4 ,
5 ]. A rte ria l o c c lu s ion can lead to devas ta ting com p
lica tions ,such as b ilia ry s tr ic tu re and leaks and pa
renchym a l ischem ia o r nec ros is [4 , 6 ].L ikew ise , th rom
boses o f the po rta l ve in and in fe rio r vena cava can lead to
s ign ifican tp rob lem s , in c lud ing feve r, s ep ticem ia , im
pa ired hepa tic func tion , b leed ing in theuppe r gas tro in te
s tina l tra c t, a s c ite s , and pe riphe ra l edem a [7 ].
T he d iagnos is o f vascu la r th rom bos is a fte r hepa tic
transp lan ta tion has re lied onang iog raphy [8 , 9 ]. The ro le
o f non in vas ive im ag ing in th is se tting has no t beenex tens
ive ly eva lua ted [8 , 1 0]. W e rev iew ed ou r expe rience w ith
vascu la r com p li-ca tions in hepa tic re c ip ien ts to de te rm
ine the va lue o f non invas ive im ag ing in thesepat ien ts .
M a te ria ls and M ethodsBe tw een Ap ril 1 , 1984 , and Sep
tem be r 1 5 , 1987 , 98 o rtho top ic liv e r transp lan ts we
re
pe rfo rm ed in 94 pa tien ts (41 adu lts , 53 ch ild ren ) a t
the Un ive rs ity o f M inneso ta H osp ita ls .The su rg ica l te
chn iques [1 1 ] an d im munosupp ress ive reg im ens [1 2 ] used a
re desc rib ed inde ta il e lsew he re . N ine teen pos tope ra
tive vascu la r com plic a tions w ere se en in 1 5 pa tien ts(Tab
le 1 ). Ind ica tions fo r transp lan ta tion in these 1 5 pa tien
ts in c luded ex trahepa tic b ilia rya tres ia (s eve n ) , a lp
ha -1 -an t itry ps in de fic ienc y (th ree ), W ils on d isea se
(on e ), ch ron ic ac t ivehepa titis (one ), p r im ary b ilia ry
c irrhos is (one ), p r im ary hepatom a (one ), and sc le ros ing
cho lan -g it is (on e ). T he rad iog rap h ic exam ina tio ns (in
c lu d in g sc in t ig raph y , so nog ra ph y, CT , M Rim ag ing ,
and ang iog raphy) and hosp ita l re co rds o f these pa tien ts we
re rev iewed re tro spec-t ive ly .
-
8/6/2019 Imaging of Vascular Complications
2/6
1286 DA LEN ET AL . AJA: 150, Jun e 1988
Pa tien ts w e re re fe rred fo r rad io log ic eva lua tion w
hen vascu la rocc lus ion was su sp ected becau se of p ers is te
nt fe ve r, deter io ra t ingl ive r fu nc tio n, a nd /o r abno rm
a l coa gu la t ion pa ram ete rs . F rom thet ime o f transp lan
ta tion to th e tim e o f in itia l d iagnos is o f vascu la rth
rom bos is , a to ta l o f 1 05 exam ina tions w e re pe rfo rm ed
(48 sc in ti-g ram s, 33 sonog ram s, 21 C T scans , and th ree ang
iog ram s ). H epa -to bilia ry s cin tig ra ph y w as p erfo rm ed
w ith ra pid -se qu en ce ; im m ed ia te ;1 0 -, 20 -, 30 -, 40 -,
50 -, and 60 -m m; and , if necessa ry , de la yed im ag
ing.Sonography w as pe rfo rm ed as described e lsewhere ; D op ple
r d up le xscann ing techn iques we re used in the la tte r ha l f
of th e s tu dy p erio d[1 3- i 5 ]. CT scann ing was pe rfo rm ed
w ith IV con tra s t m a te ria l b yus ing bo lus and drip - in fu
s ion adm in is tra tion if poss ib le . O u r MRtechn iques fo r
de fin itio n o f the uppe r abdom ina l vascu la tu re havea lso
been repo rted [1 6 , 1 7]. A ng iog raph ic te chn iques in c
luded ab -dom ina l ao rtog raphy ; hepa tic , ce lia c , o r m
esen te ric a rte riog raphy ;sp lenopo rtog raphy ; in fe r io r
venacavog raphy ; wedged hepa tic yen -ograp hy; a nd tra ns he pa
tic p or ta l v en og ra ph y.
F ifteen cases o f vascu la r com plic a tions w ere con f i
rmed b y d ir ec texam ina tion , inc lud ing a ng iog rap hy (se
ve n ), exp lo ra to ry lap a ro tom y(one ), pos tm ortem exam ina
tion (fou r) , o r a com b ina tion o f theseexam ina tions (th ree
). F ou r pa tien ts m erited a d iagnos is o f vascu la rth rom
bos is w ith non invas ive im ag ing t ec hn iques a lone ; in c lu
s ion inth is s e ries requ ired ev idence fo r th rom bos is on a
t leas t tw o non in -v as iv e s tu dio s.
ResultsH e p a tic A rte ry /D o n o r A o rta T h ro m b o s
is
A rte ria l th rom bos is (hepa tic a rte ry in th ree cases and
dono rao rta in fou r) w as obse rved in s ix ch ild ren and one
adu lt. A llpa tien ts unde rw en t hepa tob ilia ry d iso fen in
sc in tig raphy ,w h ich show ed foca l a reas o f decreased up
take in tw o . Th rom -bos is was firs t d iagnosed by sonog raphy
in th ree pa tien ts(F ig . 1 ), C T in one (F ig . 2 ), ang iog
raphy in one , lapa ro tom y inone , and pos tm o rtem exam ina
tion in one (T ab les 2 and 3 ).F iv e cases o f a rte r ia l o cc
lu s ion w e re con firm ed by ang iog ra -phy , su rge ry , o r
pos tm o rtem exam ina tion . In one pa tien t, C T ,sonog raphy ,
and M R im ag ing we re be lie ved to be de fin itiv e
and ang iog raphy w as no t pe rfo rm ed . In one ped ia tr ic
pa tien t,C T w as fa lse ly nega tiv e fo r th rom bos is , and
ang iog raphy wasused to m ake the in itia l d iagnos is w ith in 3
days . F ive ch ild renw ith a rte ria l th rom bos is have d ied ;
the m ean in te rva l fromtransp lan ta tion to d iagnos is w as 4
w eeks (range , 1 .5 w eeksto 2 m on ths). T he m ean su rv iva l o
f these ch ild ren was 73days (range , 1 0-240 ). O f the tw o pa
tien ts su rv iv ing a rte ria lo c c lu s ion , the in te rva l
from transp lan ta tion to d iagnos is w asm uch g reate r (51
/2_38 m on ths).
P orta l V ein T h ro m bo s isSeven cases o f po rta l venous
th rom bos is w e re iden tifie d
(Tab les 2 and 3 ). R educed uptake /de la yed ex tra c tion
onhepa tob ilia ry sc in tig raphy w as seen in th ree pa tien ts .
Thed iagnos is o f th rom bos is w as firs t iden tifie d by sonog
raphy inth ree pa tien ts (F ig . 3 ), C T in tw o , ang iog raphy
in one , andlapa ro tom y in one . S ix o f the seven pa tien ts
had ve rific a tiono f th rom bos is by e ither ang iog raphy o r
pos tm o rtem exam i-na tion . O ne fa lse -nega tive sonog ram w
as iden tified a fte r an -g iog raphy la te r the sam e day show
ed po rta l ve in occ lu s ion .T he m ean in te rva l from transp
lan ta tion to d iagnos is w as 2 .3w eeks (range , 1 -6 w eeks).
Th ree ch ild ren have d ied , w h ileth ree ch ild ren and one adu
lt have su rv iv ed .
In fe rio r V e n a C av a l T h ro m bo s isIn fe r io r vena
cava l th rom bos is w as seen in fiv e pa tien ts
(Tab les 2 and 3 ); the d iagnos is w as firs t m ade by
sonographyin fou r (F ig . 4 ) and by C T in one . S u rg ica l o r
pos tm o rtemve rifica tion was ava ilab le in th ree . Hepa tob
ilia ry sc in tig raphyshow ed decreased excre tion in a ll fiv e
pa tien ts . Th ree pa tien ts(tw o adu lts , one ch ild ) expe
rienced cava l th rom bos is w ith in 2days o f transp lan ta tion
and dea th w as im m inen t (m ean su r-v iva l, 8 days a fte r
transp lan ta tion ; range , 7 -9). T he d iagnos iso f cava l th
rom bos is w as m ade la te r in the tw o su rv ivo rs (1
TABLE 1: H epa tlc T ransp lan t V ascu la r Comp l ic a t
ions
c:e Transp lant(years )
L oc atio n o f T hro m bo sis Non inva : i v e Diagnos t ic
1 40 D ono r ao rta NM , sonog raphy , CT , M R2 3V2 D onor ao
rta , in fe rio r venacavaN M, s on og ra ph y, CT
3 5 H epa tic a rte ry NM4 3 D ono r ao rta NM , sonog raphy ,
CT5 4 Po rta l v e in , h epa tic a rte ry NM6 71 /2 D on or a orta
NM , sonog raphy , CT7 1 3 Po rta l v e in NM , sonog raphy , CT8
1# {189 } Por ta l v e in NM , so nograp hy , CT9 37 In fe r io r
vena cava NM , sonog raphy , CT1 0 2 Po rta l v e in , in fe r io r
vena cava NM , sonog raphy , C T1 1 # {190 } P o rta l v e in NM ,
sonog raphy , C T12 1V 2 P orta l v e in , h ep a tic a rte ry NM ,
so no gra ph y, C T1 3 49 Po rta l v e in NM , sonog raphy , C T14
43 In fe r io r vena c ava NM , sonog raphy , C T1 5 1 V2 In fe rio
r ve na cava NM , so no gra ph y
Note -NM = n uc le ar m e da cin e (h e pa to b il ia ry s ci nt
ig ra p hy ).
-
8/6/2019 Imaging of Vascular Complications
3/6
A B C
AJA:150, June 1988 COMPL IC AT IO NS AFTER HEPAT IC TRANSP LANT
1287
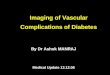
F ig . 1 .-c as e 1 2 : 1 /2 -y ea r-o ld g irl w ith seps is an
d abnorm al c oagu la t ion p aram ete rs im med ia te ly a fte r
tran sp lan ta tion . H epa tic ne cro s is w as susp ec te
dclinically.
A, Tran sv ers e dup le x so nogram of live r reve a ls abs en
ce o f h ep atic a rte ria l flow and inh om og en eous hepa tic pa
renchym a .B , A bdom ina l a o r tog ram show s occ lus ion a t an
as tom o s is o f na tive he pa tic a rte ry w ith do no r ce lia c
ax is ( ar r ow) .C, P ercu ta ne ou s cho la ng iog ram re vea ls
n um erou s in trah epa tic b il ia ry s tric tu res (lo ng a rr ow
s) an d m ult ip le a re as o f ex trad uc ta l co n tras t m ate
ria l ( shorta r r o w s ) com pa t ib le w ith b ile le ak .
F ig . 2 .-C as e 1 : 4 3 -y ea r-o ld w om an with ab dom ina l
fu lln es s and e lev a te d liv er en zym es 38 m onths a fte r h
ep at ic tra nsp la n ta tio n .A, C T s ca n th ro ug h m id ab
dom en s ho w s lo w -a tte nu atio n th ro m bu s in dono r ao
rtic g ra f t ( arrows) .B, T ra nsv erse 1 2-w eig hte d M R sc an
at sa me le ve l a ls o sh ow s h ig h-s ig na l-in ten sity a
ortic g ra ft th ro mb us ( ar r ows ) .C , C oro na l T i-w eig
hte d M R im ag e sh ow s in te rm ed ia te so ft-t is su e-d en
sity s ig na l o f th ro mb us in dono r ao rta n ea r its a nas
tom os is w ith iliac a rte ry
( arrows) .
and 6 m on ths). O ne o f these pa tien ts deve loped cava l th
rom -bos is 2 weeks a fte r dono r ao rta th rom bos is , and the o
the rdeve loped cava l th rom bos is a fte r po rta l th rom bos is
.
Discuss ionIm p roved su rv iv a l a fte r hepa tic transp lan
ta tion is a ttr ibu t-
ab le to m o re e ffe c tive im m unosupp ress ion , su rg ica l
ad -vances , and m e tic u lous pos tope ra tive ca re . N eve rthe
les s , anum be r o f pos ttransp lan ta tion com p lic a tions
occu r tha t o ftenp resen t w ith nonspec ific sym p tom s and
labo ra to ry abno r-
m a litie s . The re fo re , d iffe ren tia tion o f causes o f
g ra ft d ys func-tion (ischem ic in ju ry , b ilia ry obs tru c
tion , re je c tion , o r in fe c tion )is o ften d ifficu lt w
ithou t rad io log ic eva luation [1 0 , 1 8, 19 ].
R ad io log ic eva luation o f the hepa tic a llog ra ft frequen
tlyin vo lves the use o f seve ra l te chn iques . D iso fen in sc
in tig raphyp rim a rily assesses hepa toce llu la r func tion and
b ilia ry excre -tion [1 0 , 1 1 , 1 9]. S onog raphy can be used
to eva lua te thehepa tic pa renchym a , and the add ition o f dup
le x scann ingcapab ilitie s pe rm its d iffe ren tia tion be tween
vascu la r and b ili-a ry s tru c tu res and re liab ly docum en ts
vascu la r in teg rity [10 ,1 3, 1 4, 20 ]. C T prov ides a m eans
o f de te rm in ing the g ross
-
8/6/2019 Imaging of Vascular Complications
4/6
1288 DALEN ET AL . AJA:150, June 1988
F ig . 3 .-C as e 13 : 4 9 -y ea r-o ld m an 10 daysa f te r t r
an s p l an t a ti o n , w ith b le ed in g f rom gas t r o -eso ph
agea l va r ice s a nd increa s in g se rum live renzymes.
A, Transve rs e so nog ram w ith dup le x sc an -n in g shows no
por ta l v en ou s flow .
B , Dynam ic abdom in a l C T scan show si n h omogeneou s dens
i t y in p orta l ve in ( ar r ows ) ,co nfirm in g so no gra ph ic
find in gs . Incom ple te oc -c lu s io n o f por ta l ve in w as
sub stan t ia ted ang ie -graph ic a l l y 3 w eeks la te r w hen
dup lex sonogra -ph y a lso sh ow ed reco nstitu tio n o f flow w
ith invessel.
TAB LE 2 : Con fIrm ed Pos topera t iv e V ascu la r Com plica
tio n s A fte r L iv e r T ransp lan ta tionC om p lic a tion : M
eans o f s b uen t C onfirm ationCase No . D iagnos is u T im e a
fte rTransp lanta t ion S ta tus a tFo l low-up
H ep atic a rte ry /d on or a orta th ro mb os is :2 S onog
raphy CT , ang iog raphy 5V2 m on th s A liv e3 Au topsy None 1 1/2
w eeks D ied4 Ang iog raphy Su rge ry , au topsy 2 m on ths D ied5
Su rge ry A u topsy 2 w eeks D ied6 Sonog raphy Ang iog raphy , au
topsy 2 w eeks D ied1 2 Sonog raphy Ang iog raphy 6 w ee ks D iedP
o rt al v ei n t hr om b os is :5 S u rge ry A u topsy 2 w eeks D
ied7 CT Sonog raphy , ang iog raphy 3 w eeks D ied8 Ang iog raphy
In fe r io r venacavog raphy 1 w eek Al ive1 0 Sonog raphy CT , ang
iog raphy 1 V 2 w eeks A liv e
1 2 Sonograph y Ang io g raph y 6 w eeks D ied1 3 Sonog raphy C
T , ang iog raphy 1 V 2 w eeks A liveIn fe rio r v en a c av a th
ro m bo sis :9 S onog raphy In fe r io r venacavog raphy 2 days D
ied1 4 Sonog raphy Su rge ry 2 days D ied1 5 Sonog raphy Au topsy 1
day D ied
TABLE 3 : V ascu la r Com plic a tio ns A fte r L iv er T ransp
lan ta tio n w ith ou t A ng iog rap h ic , S u rg ica l, o r P
ostm ortem C onf irm atio nCaseN o. C om lca t nI 10 M eans o
fDiagnos is Corrobora t iveStud ies T im e a fte rTransp lan t a t
ion S ta tus a tFo l low -up
1 D ono r ao rta th rom bos is C T S onog raphy , M R 38 m onths
Al ive2 In fe rio r v en a c ava th ro mb os is S onog raphy C T 6
m onths A live1 0 In fe r io r vena cava th rom bos is C T 2D
echoca rd iog raphy 1 m onth A liv e
1 1 Po rta l ve in th rom bos is C T S onog raphy 1 w eek Al
iveNote . - 2D = two - d imens iona l .
s tru c tu ra l in teg rity o f the hepa tic a llog ra ft [1 0 ,
1 9-21 ] and thepa tency o f m ajo r vascu la r s truc tu res [21 ,
22 ]. M R appea rs tobe m os t va luab le fo r docum en ting the pa
tency o f the g ra ftvascu la tu re [1 6 , 1 7, 23 ]. H ow eve r,
the ro le o f these non in -vas ive tes ts in the d iagnos is o f
vascu la r com plic a tions a fte r
hepa tic transp lan ta tion has no t been de fined p rec ise ly
[8 , 10 ,20].
Th rom bo tic phenom ena a re pa rticu la rly c ritica l to g ra
ft func-tion because co lla te ra l c ircu la tion is no t re cons
tru c ted andm ay take m on ths o r yea rs to deve lop . The true
ra te o f
-
8/6/2019 Imaging of Vascular Complications
5/6
AJR:150, Jun e 1988 COMPL IC AT IONS AFTER HEPAT IC TRANSPLANT
1289
F ig . 4 .-C ase 9 : 3 7 -y ea r-o ld w om an with 7 .5 -k g w e
igh t ga in 2 d ay s a fte r h ep atic tra nsp la n ta -t ion .
A , Long itu d in a l so nog ram revea ls a re a o f in -c re as
ed e ch og en ic ity a t in fr ah ep atic c av al a na s-to mo sis
w Ith o blite ra tio n o f lu m en ( ar r ows ) .
B, In fe rio r v enaca vo gram show s com p le te oc -c lu s io
n o f in fe rio r v en a ca va a t d is ta l in fe r io rv en a c
av al a na st om o si s (w hite a rr o ws ) w it h c cl-la te ra l
f low through hemlazygous system ( b l a c karrows) an d ref lux
into re na l v ein s.
occu rrence o f a rte r ia l th rom bos is is unknown , bu t ra
te s of3 .4 -1 2% in adu lts and 1 1 .8 -42% in ch ild ren have
beenrepo rted [4 , 20 ]. In ou r se r ie s , 2 .3% o f adu lt and 1
0.9% ofped ia tric re c ip ien ts (ove ra ll o ccu rrence ra te , 7
.1 % ) deve lopeda rte r ia l c om p rom ise . If th rom bos is
occu rs ea r ly in the pos t-transp lan ta tion pe riod , the p
rognos is is g r im and re transp lan -ta tion m ay be ind ica ted
; if it deve lops la te r, su rv iva l is m o relik e ly and poss
ib ly is enhanced by the deve lopm en t o f co lla t-e ra l c irc u
la to ry pa thw ays [4 , 20 ]. In ou r s tudy , a rte ria l th rom
-bos is w as firs t d iagnosed by non invas ive im ag ing techn
iquesin fou r (57% ) o f seven pa tien ts . B ecause sonog raph ic
and CTexam inations can be fa ls e ly nega tiv e , agg ress ive ang
io -g raph ic eva lua tion m ay be requ ired . T he sens itiv ity
and spec -ific ity o f each non invas ive im ag ing m ethod canno
t, un fo rtu -na te ly , be de te rm ined from ou r se rie s ,
because de fin itiveang iog raphy , su rge ry , o r au topsy w as
no t pe rfo rm ed in eve ryhepa tic re c ip ien t du r ing the s
tudy pe riod .
P orta l ve in th rom bos is is a ls o assoc ia ted w ith s ign
ifican tpos ttransp lan ta tion m o rb id ity and m o rta lity .
The 7 .1% fre -quency repo rted in ou r se r ie s is s im ila r to
the 9% frequencyo f po rta l v enous th rom bos is reported by C
ien fuegos e t a l.[1 9 ]. N on invas ive techn iques p rov ided
the prim a ry d iagnos iso f porta l ve in th rom bos is in five
(71 % ) o f seven ins tances andw e re fa lse ly nega tive in one
case . In fe rio r vena cava l th rom -bos is was d iagnosed in fiv
e (5 .1 % ) o f 98 cases , and itsd iagnos is w as firs t sugges
ted by non invas ive m eans in a llfive . In one case (case 1 0)
the deve lopm en t o f im pa iredvenous d ra inage w as an tic ipa
ted a t the tim e o f transp lan ta -tion , because venous recons
tru c tion was d iffic u lt ow ing toazygous con tinua tion o f the
in fe r io r vena cava .
Ind ire c t e v idence o f vascu la r occ lu s ion can a lso be
obta inedfrom sonog raphy and C T when foca l parenchym a l abno rm
a l-itie s sugges tive o f ischem ia o r necros is a re seen . S
uch w asthe case in th ree (1 6% ) o f 1 9 com p lica tions , in c
lud ing tw ohepa tic a rte ry th rom boses and one po rta l ve in
th rom bos is . Inthese pa tien ts de fin itive assessm en t o f
these com p lica tionsw as m ad e a ng io gra ph ica lly .
In summary , non in vas ive im ag ing is va luab le in d iagnos
ingvascu la r com p lica tions a fte r hepa tic transp lan ta tion
. T he h ighfa ta lity ra te (60% in ou r se r ie s ) assoc ia ted
w ith vascu la rcom p lic a tions a fte r hepa tic transp lan ta
tion em phas izes theim po rtance o f p rom p t and accu ra te d
iagnos is fo r de te rm ina -tion o f app rop ria te trea tm en t.
In ou r s tudy , 1 4 (74% ) o f 19in s tances o f vascu la r th rom
bos is we re in itia lly d iagnosed bynon invas ive techn iques , 1
0 (53% ) by sonog raphy and fou r(2 1 % ) by CT . H oweve r, tw o
exam ina tions in ou r se rie s w e refa lse ly nega tive , and the
d iagnos is u ltim a te ly was m ade byang iog raphy in bo th . O u
r da ta re in fo rce the ro le s c ited byseve ra l au tho rs o f
sc in tig raphy , sonog raphy , and C T asscreen ing too ls in de
te rm in ing w h ich pa tien ts need m o reagg ress ive in te rven
tiona l e va lua tion [8 , 1 0, 1 5, 21 ]. The useo f M R fo r eva
lua ting uppe r abdom ina l vascu la tu re has exc itingim p lica
tions in the eva lua tion o f these pa tien ts ; re finem en tsin M
R m ay p rec lude ang iog raphy in ce rta in cases .
REFERENCES1 . S ta rz l T E , Koep U , Ha lg r im son CG , e t a
l. F iftee n ye ars o f c lin ica l liv e r
transplantat ion. G a s t r o e n t e r o l o g y 1979 ;77 :375
-3882 . S ta rz l TE , Iw a ts uk i 5 , Van T hie l D H, e t a l. E
vo lu tio n o f liv er tra ns pla nta tio n.
H e p a t o l o g y 1982 ;2 :614 -6363 . N a ja r ian JS , A
sche r N L . L ive r transp lan ta tio n . N E n g I J M e d
1984 ;311 :1179-11814 . T za k is A G , G o rdo n AD , Sh aw BW
J r, Iw atsu k i 5 , S ta rz l TE . C lin ica l
pre se n ta tio n o f h ep a tic a r te ry th rom bo s is a fte
r liv e r tra nsp la n ta tio n in thecy c lo spo rin e e ra . T r
a n s p l a n t a t i o n 1985;40 : 667 - 671
5 . C a rd e lla JF . E va lua tio n and tre a tm en t o f v as
cu la r p rob lem s a fte r live rt r ansp lan ta t ion . S em in
In te rv e n t R ad io l 1 98 6; 3:1 3 1-1 38
6 . Z a jk o A B , Cam pbe ll W L , Log sd on G A , e t a l. C
ho lan g iog rap h ic fin d in gs inh ep atic a rte ry o cc lu sio
n a fte r liv er tra nsp la nta tio n. A iR i 987 ; 149 : 485 -
489
7 . W ebb U , Sher loc k S . Th e ae tio log y , p resen ta tion
an d na tu ra l h is to ry o fe x tra -h ep a tic p o r ta l ve no
us obs tru c tion . Q J M e d 1979;48 : 627 - 639
8 . S ege l M C , Za jko AB , Bowen AB , e t a l. H ep a t ic a
rte ry th rom bos is a f te rlive r tra nsp la nta tio n: ra dio lo
gic e va lu atio n. A JR i 98 6 ;1 4 6 :1 3 7- 14 1
9 . Z a jko AB , B ro n KM , S ta rz l T E , e t a l. A n g io g
rap hy o f l ive r transp lan ta tio npa t ien t s . R a d i o l o
g y 1 9 85 ;1 5 7 :3 0 5- 31 1
1 0. P en kro t R J . N on inv as ive ev a lu a t ion o f com p
lica tio ns o f o rth o to p ic live rtransplantat ion. S em in In
te rv e n t R ad io l 1 98 6;3 : 1 20 -1 22
-
8/6/2019 Imaging of Vascular Complications
6/6
1290 DALEN ET AL .
1 1 . A scher N L , S im m ons AL Na ja r ian J5 . H os t h epa
te c tom y and liv e r trans -p la n ta tio n . In : S imm on s AL
, F inch ME , Asche r N L, N aja ria n J5 , ed s . M a n u a lo f v
a s c u la r a cc e s s , o rg a n d on atio n a nd tra n sp la n
ta t io n . N ew Y ork : S prin g-e r-V erl ag , 1 98 5: 25 5-2
84
1 2 . S toc k P , S nove r D , P ayne W , e t a l. B io ps y- gu
id ed im m un os up pre ss iv eth e rap y in the trea tm en t o f
liv e r tra nsp la nta tio n re je ctio n: in div id ua liz
edapproach . C li n T ra n sp la n t 1987;1 : 179 - 186
1 3 . B or lan d LL , Law son T L , Fo ley W D . P orta h ep a t
is : son og rap h ic d is crim i-na tio n o f b ile du c ts from a
rte r ies w ith pu lse d Dopp le r w ith n ew ana tom iccr iter ia.
Ai R i 982 ;138 :833 -840
1 4 . L e to um eau JG . Day D L , Ascher N L , e t a l. AbdOm
ina l so no gra ph y a fte rh ep atic tra ns pla nta tio n: re su
lts in 36 pa t ien t s . A JR 1987 ;149 :299 -303
1 5 . S eg a l MC , za jko AB , Bowen A B, e t a l. D op ple r u
l t r asound a s a sc re en fo rhepa tic a rte ry th rom bos is a
fte r liv e r tran sp lan ta t ion . T r a n s p l a n t a t i o ni
98 6;4 1 :5 39 -5 41
1 6 . D ay DL , Le toumeau JG , A llan BT , e t a l. M R I eva
lua t ion of u pp er a bd om in alv ascu la r a na tom y in p ed ia
tr ic live r tran sp lan t c and id a te s . AJ
A1986;147:1027-1030
AJA:150 , J un e 1 98 8
17 . L un d G , L e to um eau JG , D ay DL , C ras s JR . M A I
in o rgan tra nsp lan ta tion .R a d io l C lin N o rth A m 1987;25
( 2 ) : 281 - 288
18 . C arde lla JF , C as ta ned a-Zu n ig a W A , Hun te r DW ,
Young A T , Am p la tz K .A ng iog rap hic and in te rven tio na l
ra dio log ic c ons ide ra tion s in live r tra nsp la n-tat ion.
Ai R 1986 ;146 :143 -153
19 . C ien fU eg Os JA , D om ing ue z AM , T am elchO ff PJ , e
t a l. S urg ic a l comp l ic a -tio ns in the p os top e ra tiv e
pe riod o f live r tran sp lan ta tion in ch ild re n . T r a n s
-p la nt P ro c 1984 ;16 :1230-1235
20 . W o zn ey P , Za jk o AB , B ron KM , P o in t S , S ta rz
l TE . V as cu la r comp l ic a t ionsa fte r liv e r tra nsp la
nta tio n: a 5 -y ea r exper ience . A JR 1986 ;147 :657 -663
21 . Le toumeau JG , D ay D L , Made CW , C ras s JA , Asch er N
L , F ric k M P . L ive ra llog ra f t tran sp lan ta tion : p os
top era tiv e C T fin din gs . A JR i 987 ; 148 : 1099 -1103
22 . ze rho un i EA , Ba rth KH , S ie ge lm an SS . D em on
stra tion o f v eno us th rom -bos is by co mp ute d to mo gra ph
y. A iR 1980 ;134 :753 -758
23 . Bernad ine M E, Ste inbe rg HV , Pear son TC , G edgaud
as-M cC lees AK ,Tor r es W E, Hender son JM. Shunts for portal
hypertens ion: MR andang iog r aphy fo r de te rm ina t ion of pa
tenc y . R a d i o l o g y 1986;158 : 57 - 61