Embed Size (px)
Citation preview

University of Veterinary Medicine
Center for Systems Neuroscience Hannover
Department of Pharmacology, Toxicology and Pharmacy
Hannover Medical School
Department of Nuclear Medicine, Preclinical Molecular Imaging
_______________________________________________________________
Imaging and pharmacotherapy
of blood-brain barrier impairment
during epileptogenesis
THESIS
Submitted in partial fulfillment of the requirements for the degree
DOCTOR OF PHILOSOPHY
-Ph.D.-
In the field of Pharmacology
awarded by the
University of Veterinary Medicine Hannover
by
Heike Breuer
Preetz
Hannover, Germany 2016

-II-
Supervisor: Prof. Dr. Marion Bankstahl
Supervision Group: Prof. Dr. med. Martin Stangel
Prof. Dr. med. Xiao-Qi Ding
1st Evaluation: Prof. Dr. Marion Bankstahl
Department of Pharmacology, Toxicology and
Pharmacy
University of Veterinary Medicine Hannover
Prof. Dr. Martin Stangel
Department of Neurology
Hannover Medical School
Prof. Dr. Xiao-Qi Ding
Institute of Diagnostic and Interventional
Neuroradiology
Hannover Medical School
2nd Evaluation: Prof. Dr. rer. nat. Andreas Hess
Institute of Experimental and Clinical
Pharmacology and Toxicology
Friedrich-Alexander University Erlangen-Nürnberg
Date of final exam: 21.10.2016

-III-
Parts of the thesis have been published previously in:
BREUER, H., MEIER, M., SCHNEEFELD, S., HÄRTIG, W., WITTNEBEN, A.,
Märkel, M., ROSS, T.L., BENGEL, F. BANKSTAHL, M., BANKSTAHL, J.P. (2016).
Multimodality Imaging Of Blood-Brain Barrier Impairment during Epileptogenesis.
Journal of Cerebral Blood Flow and Metabolism, DOI: 10.1177/0271678X16659672.
This thesis was accomplished within the PhD program “Systems Neuroscience“ of
the Center for Systems Neuroscience Hannover and parts of the work belong to the
European Union’s Seventh Framework Programme (FP7/2007-2013) under grant
agreement n°602102 (EPITARGET).
Heike Breuer was supported by a doctoral scholarship of the Studienstiftung des deutschen Volkes.

-IV-
Meiner Familie

-V-

-VI-
Table of Contents
SUMMARY ................................................................................................................. 1
ZUSAMMENFASSUNG ............................................................................................. 3
1 STATE OF RESEARCH ...................................................................................... 6
1.1 Epilepsy ................................................................................................................................. 6
1.1.1 Definition and significance ..................................................................................................... 6
1.1.2 Temporal lope epilepsy ......................................................................................................... 7
1.2 Epileptogenesis ..................................................................................................................... 7
1.3 The blood-brain barrier .......................................................................................................... 9
1.3.1 The role of blood-brain barrier in epileptogenesis ............................................................... 10
1.3.2 The blood-brain barrier and inflammation ........................................................................... 12
1.4 Treatment strategies targeting blood-brain barrier integrity ................................................ 13
1.5 Animal models of epileptogenesis ....................................................................................... 16
1.5.1 The pilocarpine post status epilepticus rat model ............................................................... 16
1.5.2 The intrahippocampal kainate mouse model ....................................................................... 17
1.6 Non-invasive in vivo imaging of blood-brain barrier leakage ............................................... 17
1.6.1 Positron Emission Tomography imaging ............................................................................. 18
1.6.2 Single Photon Emission Computed Tomography imaging .................................................. 21
1.6.3 Magnetic Resonance imaging ............................................................................................. 22
1.7 Aim of the studies ................................................................................................................ 26
1.7.1 Study 1: Multimodality imaging of blood-brain barrier impairment during epileptogenesis . 26
1.7.2 Study 2: Longitudinal in vivo evaluation and pharmacotherapy of blood-brain barrier leakage in a rat model of epileptogenesis ........................................................................... 26
1.7.3 Study 3: Dexamethasone protects blood-brain barrier integrity in a mouse model of epileptogenesis .................................................................................................................... 27
2 MULTIMODALITY IMAGING OF BLOOD-BRAIN BARRIER IMPAIRMENT
DURING EPILEPTOGENESIS .......................................................................... 28
3 LONGITUDINAL IN VIVO EVALUATION AND PHARMACOTHERAPY OF
BLOOD-BRAIN BARRIER LEAKAGE IN A RAT MODEL OF
EPILEPTOGENESIS.......................................................................................... 30
3.1 Abstract................................................................................................................................ 31
3.2 Introduction .......................................................................................................................... 32
3.3 Materials and Methods ........................................................................................................ 34
3.3.1 Animals ................................................................................................................................ 34
3.3.2 Status epilepticus ................................................................................................................ 34
3.3.3 Chemicals and drugs ........................................................................................................... 35
3.3.4 Study design ........................................................................................................................ 35
3.3.5 Longitudinal in vivo assessment of blood-brain barrier leakage ......................................... 36
3.3.6 Dexamethasone treatment .................................................................................................. 36

-VII-
3.3.7 Losartan treatment .............................................................................................................. 36
3.3.8 Assessment of blood-brain barrier integrity ......................................................................... 37
3.3.9 Image analysis ..................................................................................................................... 38
3.3.10 Histological analysis of albumin extravasation .................................................................... 39
3.3.11 Statistical analysis ............................................................................................................... 40
3.4 Results ................................................................................................................................. 40
3.4.1 Status epilepticus ................................................................................................................ 40
3.4.2 Longitudinal in vivo assessment of blood-brain barrier leakage in saline-treated group .... 41
3.4.2.1 Development of T1 intensity during early epileptogenesis .......................................... 41
3.4.2.2 Development of T2 intensity during early epileptogenesis .......................................... 43
3.4.3 Pharmacotherapy with potentially blood-brain barrier protective drugs .............................. 44
3.4.3.1 Effects of dexamethasone on blood-brain barrier integrity .......................................... 45
3.4.3.2 Effects of losartan on blood-brain barrier integrity ....................................................... 47
3.4.4 Histological analysis of albumin extravasationJJJJJJJJJJJJJJJJJJ...49
3.5 Discussion ........................................................................................................................... 51
3.6 Conclusion ........................................................................................................................... 56
3.7 References .......................................................................................................................... 57
4 DEXAMETHASONE REDUCES BLOOD-BRAIN BARRIER LEAKAGE IN A
MOUSE MODEL OF EPILEPTOGENESIS ........................................................ 62
4.1 Abstract................................................................................................................................ 63
4.2 Introduction .......................................................................................................................... 64
4.3 Materials and methods ........................................................................................................ 66
4.3.1 Animals ................................................................................................................................ 66
4.3.2 Chemicals and drugs ........................................................................................................... 66
4.3.3 Status epilepticus ................................................................................................................ 67
4.3.4 Study design ........................................................................................................................ 68
4.3.5 Magnetic Resonance imaging setup ................................................................................... 69
4.3.6 Evaluation of dexamethasone treatment on blood-brain barrier integrity during early epileptogenesis .................................................................................................................... 68
4.3.7 Image analysis ..................................................................................................................... 70
4.3.8 Statistical analysis ............................................................................................................... 70
4.4 Results ................................................................................................................................. 71
4.4.1 Tolerability of dexamethasone in the intrahippocampal kainate mouse model ................... 71
4.4.2 Longitudinal Magnetic Resonance imaging during epileptogenesis reveals blood-brain barrier leakage in epilepsy associated brain regions .......................................................... 72
4.4.3 Dexamethasone treatment protects blood-brain barrier integrity ........................................ 74
4.5 Discussion ........................................................................................................................... 77
4.5.1 Longitudinal in vivo assessment of blood-brain barrier leakage during epileptogenesis .... 77
4.5.2 Dexamethasone treatment significantly reduces blood-brain barrier leakage .................... 79
4.6 Conclusion ........................................................................................................................... 80
4.7 References .......................................................................................................................... 81

-VIII-
5 GENERAL DISCUSSION .................................................................................. 85
5.1 Main findings ....................................................................................................................... 85
5.2 Multimodal imaging of blood-brain barrier leakage during epileptogenesis ........................ 85
5.3 Methodological issues ......................................................................................................... 88
5.4 Effects of losartan on blood-brain barrier integrity .............................................................. 89
5.5 Effects of dexamethasone on blood-brain barrier integrity .................................................. 89
5.6 Limitations of the studies ..................................................................................................... 91
5.7 Future directions .................................................................................................................. 91
5.8 Conclusion ........................................................................................................................... 92
6 REFERENCES ................................................................................................... 93

-IX-
List of abbreviations
µl: microliter
µm: micrometer
AG: Aktiengesellschaft
al.: alia
ANOVA: analysis of variance
b.i.d.: bis in die
BBB: blood-brain barrier
CA: contrast agent
cc: cubic centimeter
CNS: central nervous system
Co.: company
COX-2: cyclooxygenase-2
CT: computed tomography
d: day/s
Da: dalton
DAB-Ni: nickel-enhanced
diaminobenzidine
dex: dexamethasone
DOTA: 1,4,7,10-
tetraazacyclododecane-1,4,7,10-
tetraacetic acid
DTI: diffusion tensor imaging
DTPA: diethylenetriamine pentaacetic
acid
DWI: diffusion weighted imaging
ECoG: electrocorticography
EDTA: ethylenediaminetetraacetic acid
FDG: fluoro-2-deoxy-D-glucose
FOV: field of view
FP7: Seventh Framework Programme
FTY720: fingolimod
g: gram
Gd: gadolinium
GmbH: Gesellschaft mit beschränkter
Haftung
HEPES: ethanesulfonic acid
i.p.: intraperitoneal
i.v.: intravenous
ID: injection dose
IL-1ß: interleukin-1ß
ILAE: International League Against
Epilepsy
Inc.: incorporated
KA: kainate
KeV: kiloelectron volts
kg: kilogram
KG: Kommanditgesellschaft
l: liter
LLC: limited liability company
Ltd.: limited
lx: lux
m2: square meter
MBq: megabecquerel
MDEFT: modified driven equilibirum
fourier transformation
mg: milligram
MHz: megahertz
mm: millimeter
mm3: cubic millimeter
mmol: millimole
MR: magnetic resonance
MRI: magnetic resonance imaging
ms: millisecond
MSME: multi slice multi echo

-X-
n: number
NMDA: N-methyl-d-aspartate
nmol: nanomole
OSEM: ordered subset expectation
maximization
p.o.: per os
PET: positron emission tomography
pH: power of hydrogen
PhD: Philosophiae Doctor
RARE: rapid acquisition refocusing
s: second
s.c.: subcutaneous
SE: status epilepticus
SEM: standard error of the mean
SPECT: single photon emission
computed tomography
SPM: service provider mechanism
T: tesla
TE: echo time
TGFßRII: transforming growth factor ß
receptor II
TLE: temporal lobe epilepsy
TR: repetition time
UCL: University College London
UK: United Kingdom
USA: United States of America
vs.: versus

-XI-
List of figures
Figure 1: Schematic illustration of epileptogenesis ................................................... 8
Figure 2: Blood-brain barrier associated mechanisms triggering epileptogenesis .. 11
Figure 3: Epileptogenesis and possible time window for antiepileptogenic therapy 12
Figure 4: Principle mechanism for detection of blood-brain barrier leakage ........... 17
Figure 5: Positron emission tomography imaging ................................................... 19
Figure 6: Weight development ................................................................................ 41
Figure 7: Quantification of changes in T1 and T2 intensities during
epileptogenesis ........................................................................................ 43
Figure 8: Longitudinal magnetic resonance imaging during epileptogenesis .......... 44
Figure 9: Comparative T2, T1 and leakage map images following saline,
dexamethasone and losartan treatment .................................................. 45
Figure 10: Quantification of BBB leakage and edema after dexamethasone
treatment ................................................................................................. 46
Figure 11: Quantification of blood-brain barrier leakage and edema after losartan
treatment ................................................................................................. 48
Figure 12: Histological evaluation of albumin extravasation ..................................... 50
Figure 13: Localization of kainate injection as assessed by magnetic resonance
imaging (MRI) .......................................................................................... 72
Figure 14: Quantification of blood-brain barrier leakage during epileptogenesis ...... 73
Figure 15: Blood-brain barrier leakage after dexamethasone treatment ................... 75
Figure 16: Serial magnetic resonance images in kainate, dexamethasone and sham
animals .................................................................................................... 76

-XII-
List of tables
Table 1: Representation of T1- and T2-contrast on MRI .......................................... 23
Table 2: Gd-DTPA infusion protocol rats .................................................................. 38
Table 3: Model-specific criteria for animal evaluation after surgery .......................... 68
Table 4: Gd-DTPA infusion protocol mice ................................................................ 69

-1-
Summary
Heike Breuer
Imaging and pharmacotherapy of blood-brain barrier impairment during
epileptogenesis
Brain insults can result in the development of epilepsy, the most common chronic
neurologic disease worldwide. Epilepsy is a complex disease characterized by
unpredictably occurring spontaneous seizures, which cannot be treated efficiently in
approximately every third patient. The development of epilepsy is characterized by a
seizure-free latency period between the initiating brain insult and the occurrence of
spontaneous recurrent seizures, referred to as epileptogenesis. During this time,
functional and structural reorganization processes, including blood-brain barrier
(BBB) leakage, transform normal brain circuits into an epileptogenic network. To date
it is neither possible to predict which patient will develop epilepsy after a brain insult
nor to prevent epileptogenesis. Therefore, biomarkers for epileptogenesis are
urgently needed to identify at-risk patients. The latent period may offer a therapeutic
window for the prevention or modification of epileptogenesis. Given the increasing
evidence that BBB impairment following brain insults is one important trigger to set
the process of epileptogenesis in motion, non-invasive in vivo imaging of BBB
leakage might be a suitable biomarker for epileptogenesis. Moreover, strategies that
aim to restore the BBB integrity might consequently be beneficial for the prevention
of epilepsy after brain insults. However, the number of molecular imaging studies on
BBB leakage is limited and the presence of BBB leakage and its role in
epileptogenesis need to be further investigated.
Thus, the first objective of this study was to investigate whether dedicated small
animal [68Ga]-diethylenetriamine pentaacetic acid (DTPA) positron emission
tomography (PET), [99mTc]-DTPA single photon emission computed tomography
(SPECT) and contrast enhanced magnetic resonance imaging (MRI) following
infusion of gadobutrol, gadolinium (Gd)-DTPA, or Gd-albumin would be sensitive to
detect BBB leakage in animal models of epileptogenesis. Different imaging protocols
including [68Ga]-DTPA PET after bolus injection and after step-down tracer infusion

-2-
were used and results were compared to histology as gold standard using
fluorescein-iso-thiocyanate (FITC)-labeled albumin. The second objective of this
study was to evaluate whether two potentially BBB-stabilizing drugs, losartan and
dexamethasone, can preserve BBB integrity and alleviate vascular edema during
early epileptogenesis. MRI protocols including step-down infusion of Gd-DTPA were
used to assess effects of dexamethasone and losartan in the pilocarpine post status
epilepticus (SE) rat model and of dexamethasone in the intrahippocampal kainate
mouse model.
We found that [68Ga]-DTPA PET, [99mTc]-DTPA SPECT and T1-weighted MRI
following infusion of Gd-DTPA, gadobutrol or Gd-albumin are sensitive to detect BBB
leakage in early epileptogenesis. Extravasation patterns are limited to specific,
typically epilepsy-associated brain regions. Contrast-enhanced MRI and
[99mTc]-DTPA SPECT are the most sensitive techniques for detecting BBB leakage
following SE. Moreover, our results show for the first time a successful reduction of
BBB leakage by dexamethasone in mice during epileptogenesis. However, in rats,
both dexamethasone treatment and losartan treatment had no BBB protective effects
at the used dose. Our data show that molecular imaging provides an evaluative
perspective to gain further insights into the dynamics of BBB leakage and its
association with epileptogenesis progression. Moreover, the study offers suitable
imaging protocols to further evaluate the role of BBB impairment as potential
biomarker for epileptogenesis and to evaluate new anti-epileptogenic treatments.
Such therapies could minimize the risk of epilepsy development or progression after
brain insults.

-3-
Zusammenfassung
Heike Breuer
Bildgebung und Pharmakotherapie von Blut-Hirn-Schranken Veränderungen im
Verlauf der Epileptogenese
Hirninsulte können die Entwicklung einer Epilepsie initiieren, der häufigsten
chronischen neurologischen Erkrankung weltweit. Epilepsien sind komplexe
Erkrankungen, die durch unvorhersehbar auftretende spontane Anfälle
charakterisiert sind, welche bei etwa jedem dritten Patienten nicht effizient behandelt
werden können. Die Entwicklung von symptomatischen Epilepsien ist
gekennzeichnet durch eine anfallsfreie Latenzzeit, die sogenannte Epileptognese,
zwischen dem auslösenden Hirninsult und dem Auftreten wiederkehrender spontaner
Anfälle. Während dieser Zeit kommt es zu funktionellen und strukturellen
Reorganisationsprozessen im Gehirn, beispielsweise Veränderungen der
Blut-Hirn-Schranken (BHS)-Integrität. Diese tragen zur Entstehung von neuronaler
Hyperexzitabilität bei und initiieren den Prozess der Epileptogenese. Bis heute ist es
weder möglich vorherzusagen, welche Patienten nach einem Hirninsult eine
Epilepsie entwickeln werden, noch ist es möglich, die Entstehung von Epilepsien zu
verhindern. Daher besteht ein dringender Bedarf an diagnostisch nachweisbaren
Biomarkern für Epileptogenese, um Risikopatienten frühzeitig identifizieren zu
können. Die Latenzperiode nach einem Hirninsult bietet ein geeignetes Zeitfenster
für epilepsie-präventive Therapieansätze. Angesichts der zunehmenden Hinweise
darauf, dass Veränderungen der BHS-Integrität nach Hirninsulten sowohl an der
Initiierung als auch an der Progression der Epileptogenese beteiligt sind, könnte die
Visualisierung von Veränderungen der BHS-Integrität durch molekulare Bildgebung
einen geeigneten Biomarker für den Prozess der Epileptogenese darstellen. Mit Hilfe
dieser Bildgebungs-Biomarker könnte folglich ein möglicher Behandlungserfolg nach
BHS-protektiver Behandlung im Verlauf der Epileptogenese überprüft werden. Die
Zahl der bisher erfolgten molekularen Bildgebungs-Studien in diesem Bereich ist
stark limitiert, so dass weitere Untersuchungen nötig sind, um Fortschritte auf diesem
Gebiet zu erreichen.

-4-
Somit war es das erste Ziel dieser These zu untersuchen, ob die Sensitivität
dedizierter Kleintier-[68Ga]-Diethylentriaminpentaessigsäure (DTPA) Positronen-
Emissions-Tomographie (PET), [99mTc]-DTPA Einzelphotonen-Emissions-
Computertomographie (SPECT) sowie kontrastverstärkter Magnet-Resonanz-
Tomographie (MRT) nach Infusion von Gadobutrol, Gadolinium (Gd)-DTPA oder
Gd-Albumin ausreichend ist, um Veränderungen der BHS-Integrität in Tiermodellen
für Epileptogenese nachweisen zu können. Hierzu wurden für [68Ga]-DTPA PET
verschiedene Bildgebungsprotokolle einschließlich Bolus-Injektion und Step-Down
Tracer-Infusion verwendet. Zusätzlich wurden als Vergleichsverfahren
immunhistologische Untersuchungen von Gehirnschnitten nach
Fluorescein-iso-thiocyanat (FITC)-Albumin-Infusion durchgeführt.
Das zweite Ziel der These lag darin festzustellen, ob die Behandlung mit zwei
verschiedenen potentiell BHS-stabilisierenden Medikamenten, Losartan und
Dexamethason, eine Protektion der BHS-Integrität während der auf einen Status
Epilepticus (SE) folgenden frühen Epileptogenese bewirken kann. Zur Beantwortung
dieser Frage wurden MRT-Untersuchungen nach Step-Down-Infusion von Gd-DTPA
durchgeführt, um die Effekte von Dexamethason und Losartan im Lithium-Pilocarpin-
Rattenmodell sowie die von Dexamethason im intrahippocampalen Kainat-Modell der
Maus zu beurteilen.
Wir konnten zeigen, dass [68Ga]-DTPA PET, [99mTc]-DTPA SPECT sowie
T1-gewichtetes MRT nach Infusion von Gadobutrol, Gd-DTPA oder Gd-Albumin
geeignet sind, Integritätsstörungen der BHS während der frühen Epileptogenese zu
detektieren. Die Extravasationsmuster von Tracern und Kontrastmitteln sind dabei
auf bestimmte, typischerweise epilepsie-assoziierte Hirnregionen beschränkt. MRT
und SPECT haben sich als die sensitivsten Methoden zur Erkennung von
BHS-Veränderungen nach SE erwiesen. Darüber hinaus konnten wir erstmals
während der Epileptogenese eine erfolgreiche Protektion der BHS-Integrität durch
Behandlung mit Dexamethason bei Mäusen nachweisen. Diese Erkenntnis könnte
zur weiteren Entwicklung anti-epiletogener oder epilepsie-modifizierender Therapien
beitragen. Im Lithium-Pilocarpin-Rattenmodell hingegen konnte mit dem von uns
verwendeten Behandlungsschema keine BHS-protektive Wirkung von
Dexamethason oder Losartan festgestellt werden.

-5-
Unsere Daten zeigen, dass die molekulare Bildgebung eine wertvolle Methode ist,
um sowohl die Dynamik als auch die Pathogenese von BHS-Veränderungen
während der Epileptogenese zu untersuchen. Darüber hinaus können die in der
These etablierten Bildgebungsprotokolle genutzt werden, um in folgenden
Untersuchungen die Eignung der Detektion von BHS-Beeinträchtigungen als
potentiellen Biomarker für Epileptogenese weiter zu untersuchen und neue
anti-epileptogene Behandlungsansätze zu validieren. Diese Therapien könnten dann
zukünftig verwendet werden, um das Risiko der Entwicklung und der Progression
von Insult-assoziierten Epilepsien zu miniminieren.

State Of Research
6
1 State Of Research
1.1 Epilepsy
1.1.1 Definition and significance
Epilepsy is defined as a "brain disorder which is characterized by a permanent
tendency to development of epileptic seizures, as well as by the neurobiological,
cognitive, psychological and social consequences of this condition" according to the
International League Against Epilepsy (ILAE) (Fisher et al., 2005). Epileptic seizures
are defined as the "transient occurrence of signs and/or symptoms due to abnormal
excessive or synchronous neuronal activity in the brain" (Fisher et al., 2005).
Epilepsies are among the most common chronic diseases of the brain, characterized
by an excessive and abnormal electrical activity of neurons resulting in spontaneous
and recurrent seizures (Chang & Lowenstein, 2003), often accompanied by a
progressive tendency and psychiatric comorbidities like depression, anxiety as well
as learning and memory deficits (Tellez‐Zenteno et al., 2007). Approximately 1-2 %
of the population are affected by this complex disease in the course of their lives
(Löscher & Schmidt, 2002; Bialer & White, 2010). Moreover, up to 5.7 % of dogs and
cats are afflicted (Volk et al., 2008; Volk & Loderstedt, 2011), making epilepsy the
most common neurological disease in domestic animals, too (Löscher, 2003). The
underlying causes of epilepsy are categorized as genetic, structural-metabolic or
unknown (Berg et al., 2010). An accurate differentiation and diagnosis of epilepsies –
based on the type of seizures, their etiology and triggering factors as well as
electroencephalographic findings and the patient’s age at onset – is essential for a
successful treatment (Engel, 2006; Berg et al., 2010). A classification issued by the
ILAE provides the basis for this (Engel, 2006). Focal seizures are distinguished from
generalized seizures. Focal epileptic seizures originate within networks limited to one
hemisphere and each seizure type has a consistent site of onset (epileptic focus).
Starting from this focus, they can spread to both hemispheres resulting in secondarily
generalized seizures. By contrast, primarily generalized epileptic seizures originate
from bilateral networks with localization and lateralization not being consistent
between seizures (Berg et al., 2010).

State Of Research
7
1.1.2 Temporal lope epilepsy
Structural-metabolic epilepsies are diagnosed in 30-40 % of patients, making them
the most common epilepsy subtype. They are initiated by brain insults triggering
diagnostically detectable structural lesions which ultimately lead to epilepsy
(Englander et al., 2003; Pitkänen & Lukasiuk, 2009). Underlying causes involve
traumatic brain insults as well as stroke, infections, brain tumors or status epilepticus
(SE). A SE can be characterized by tonic-clonic convulsions lasting longer than 5 min
and by a loss of consciousness (Engel, 2006; Lowenstein, 2009). SE is an acute life-
threatening event (Knake et al., 2009) and contributes to increased mortality rates
among epilepsy patients (Sperling et al., 1999). Temporal lobe epilepsy (TLE) is
localization-related and clinically accompanied by partial or secondarily generalized
tonic-clonic seizures, assigned to as complex partial seizures (Mattson et al., 1992).
These seizures generally last 1-2 min and can be associated with auras occurring
prior to seizure onset as well as with emotional alterations including anxiety (Engel,
1996; Chabardès et al., 2005). The epileptic focus is often located in the temporal
lobe, particularly in the hippocampus, the amygdala and in the adjacent
parahippocampal cortex (McNamara, 1994; Chang & Lowenstein, 2003; Bertram,
2009) which is why the resulting syndrome is referred to as TLE. It is the most
common form of partial epilepsy in humans (Engel, 1996) and one of the focal
epilepsies. A hallmark of TLE is hippocampal sclerosis, affecting approximately 65 %
of patients (Wieser, 2004). It is characterized by neuronal cell loss and synaptic
reorganization in hippocampal subregions (Chang & Lowenstein, 2003; Bertram,
2009) which can often be detected as hippocampal atrophy by magnetic resonance
imaging (MRI, Berkovic et al., 1991).
1.2 Epileptogenesis
The development of structural-metabolic epilepsies, called epileptogenesis (see
figure 1) is characterized by a latency period between the initiating brain insult and
the occurrence of complex partial seizures (Englander et al., 2003). The latency
period can last weeks to years. In TLE, the mean latency phase is two years in
human patients (Berkovic et al., 1991).

State Of Research
8
Brain insult First clinical seizure Chronic epilepsy
Epileptogenesis
Neurodegeneration, Blood-brain barrier impairment, Inflammation
Figure 1: Schematic illustration of epileptogenesis
The development of insult-associated epilepsy is characterized by a latency period between the initiating insult and the first occurrence of seizures, called epileptogenesis. During this time, multiple reorganization processes occur, amongst them blood-brain barrier leakage and inflammation.
During this period, cellular and structural reorganization processes occur in the brain
(Friedman et al., 2009). These include, but are not limited to, an increase in the
permeability of the blood-brain barrier (BBB), brain inflammation, neuronal loss and
sprouting of mossy fibers (Pitkänen & Lukasiuk, 2009; Löscher & Brandt, 2010).
Subsequently, surviving neuronal populations generate abnormal electrical activity.
This activity leads to recurrent focal or generalized seizures and results in chronic
epilepsy (Sloviter & Bumanglag, 2013).
To date, epilepsies cannot be cured with medication. With the exception of epilepsy
surgery, current treatment options are purely symptomatic. Furthermore, they are
unable to prevent the development or progression of epilepsy after brain insults
(Temkin, 2001; Löscher & Brandt, 2010). A hitherto remaining problem is that
50-75 % of TLE-patients cannot be adequately treated by anti-seizure drugs
(Spencer, 2002; Löscher & Potschka, 2005; van Vliet et al., 2014a). Despite a wide
range of approved anti-seizure drugs on the market, they remain unresponsive to
symptomatic therapy (Chang & Lowenstein, 2003) and suffer from unpredictably
occurring seizures. Cognitive impairment, side effects of therapy and other factors
which affect the quality of life are often very distressing for those affected and for
their families. The everyday and professional life of these people is severely
restricted. In addition, comorbidities like anxiety- or depression-associated behavioral
changes are more frequently found in drug-resistant patients (Shihab et al., 2011;
Bankstahl & Bankstahl, 2012). This is accompanied, among other things, with an
increased susceptibility to suicide (Löscher & Brandt, 2010).

State Of Research
9
These facts emphasize the importance of understanding epileptogenesis. There is a
strong interest to discover therapies that hold potential to prevent or to modify the
process of epileptogenesis (Löscher & Brandt, 2010). However, only a limited
number of individuals actually develop epilepsy as a consequence of brain insults.
Hence, diagnostic methods for identification of patients at risk are urgently needed.
Prognostic biomarkers for epileptogenesis are a prerequisite to identify patients at
risk at an early stage in epileptogenesis. The long-term goal is to provide an
antiepileptogenic treatment for at-risk patients to prevent the development of
epilepsy.
1.3 The blood-brain barrier
By excluding entry of many potentially harmful molecules from the blood, the BBB is
an important protective factor for the brain (Abbott et al., 2006). It consists of capillary
endothelial cells, having the apical membrane facing the lumen and the basolateral
membrane facing the brain parenchyma (Betz et al., 1980). Tight junctions between
adjacent endothelial cells with lack of fenestrations and little pinocytosis prevent the
paracellular passage of molecules into the brain (Abbott et al., 2006). Endothelial
cells, along with basal lamina, pericytes, perivascular astrocytic end-feet and
neurons, form the so-called "Neurovascular Unit" which is mandatory for a
physiological neuronal functioning (Abbott et al., 2010). The BBB achieves its
protective function by different mechanisms: tight junctions make it a physical barrier
and a variety of metabolizing enzymes an enzymatic barrier. Besides, uptake or
efflux transporters enable active transportation of diverse compounds (van Vliet et
al., 2014a). Thereby, the BBB allows delivery of essential nutrients as well as
discharge of toxic metabolites out of the central nervous system (CNS) (Pardridge,
2007), but still protects the brain from potentially harmful substances (Abbott &
Friedman, 2012). Moreover, the BBB is the place of interactions between central and
peripheral immune systems (Engelhardt & Coisne, 2011). It is present through the
whole of the developed brain’s vasculature. Exceptions are the circumventricular
organs where secretion of neuropeptides and hormones as well as chemoreception
require a less restrictive BBB (Abbott et al., 2010) .

State Of Research
10
1.3.1 The role of blood-brain barrier in epileptogenesis
Accumulating evidence strongly suggests that insult-associated BBB impairment is a
key step in the initiation of epileptogenesis and may contribute to disease
progression (Janigro, 1999; Oby & Janigro, 2006; van Vliet et al., 2007b; Friedman
et al., 2009; Friedman & Heinemann, 2010; Ndode-Ekane et al., 2010; Friedman,
2011; Abbott & Friedman, 2012). Therefore, BBB-protective treatment might prevent
or attenuate epileptogenesis (Dedeurwaerdere et al., 2007; Friedman et al., 2009;
Friedman & Heinemann, 2010).
Changes in BBB integrity during epileptogenesis were found at the structural, cellular
and molecular level in animal models and in human brain tissue (van Vliet et al.,
2014a), suggesting that BBB leakage triggers a chain of events causing epilepsy
(Janigro, 1999; Seiffert et al., 2004; Ivens et al., 2007; Marchi et al., 2007a). After
kainate-induced SE in rats, increased extracellular levels of the excitatory
neurotransmitter glutamate were observed (Ueda et al., 2002). These changes were
accompanied by generation of free radicals. Subsequent excessive stimulation of
BBB endothelial N-methyl-d-aspartate (NMDA) receptors results in BBB impairment
early after SE (Sharp et al., 2005) and leads to further oxidative stress. Moreover, the
neuronal hyperexcitability accompanying seizures causes an increased glucose and
oxygen demand and thus an increased blood volume in the affected brain regions.
The resulting hypertension in the brain capillaries initiates an increased BBB
permeability and a metabolic mismatch (Lothman, 1990). Increased vascular
oxidative stress, along with increased blood pressure as well as hypoxia and
reduction of blood pH (Stanimirovic & Friedman, 2012) further impair BBB integrity.
The extravasation of blood components like albumin and immune cells into the brain
through a leaky BBB, alterations in electrolyte concentrations as well as loss of
glutamate and extracellular homeostasis favor an increased neuronal excitability
(Oby & Janigro, 2006; Ndode-Ekane et al., 2010, see figure 2) which may trigger
epileptogenesis (Ivens et al., 2007; Friedman et al., 2009). Albumin is incorporated
by astrocytes and binds to the transforming growth factor ß receptor II (TGFßRII).
Subsequently, the TGF-ß signaling cascade is activated within the neurovascular
unit, resulting in proepileptogenic alterations including astrocytic transformation and
dysfunction (Ivens et al., 2007; Friedman et al., 2009).

State Of Research
11
Figure 2: Blood-brain barrier associated mechanisms triggering epileptogenesis
Different mechanisms affecting parts of the neurovascular unit contribute to blood-brain barrier (BBB) leakage. Leucocyte-endothelial interactions directly affect endothelial cells. Potassium entering the brain lowers the seizure-threshold. Extravasation of serum components like albumin into the brain parenchyma causes astrocytic responses. Albumin is taken up into astrocytic end-feet via transforming growth factor (TGF)-ß receptors and activates the TGF-ß signaling cascade. Subsequently, the potassium channel Kir4.1 and glutamate transporters are downregulated. This mechanism results in impaired potassium- and glutamate buffering. Moreover, pro-inflammatory cytokines are released by astrocytes and microglia, resulting in downregulation of endothelial zonula occludens-1, further increasing BBB permeability. Consequently, neuronal hyperexcitability occurs, resulting in seizures. Figure modified from (Obermeier et al., 2013) and (Abbott et al., 2006).
The occurrence of increased BBB permeability is limited to specific brain regions in
epilepsy patients (Bradbury & Lightman, 1990). These regions are congruent with
regions of increased metabolic activation after SE as assessed by 2-deoxyglucose
autoradiography (Van Landingham & Lothman, 1991). Moreover, they often
anatomically overlap with those regions associated with the development and spread
of epileptic seizures, such as hippocampus, amygdala and piriform cortex. Hence, it
was suggested that a metabolic over-activation, resulting in increased glucose
demand and subsequent increase in blood-pressure in cerebral capillaries during SE
causes BBB leakage (van Vliet et al., 2014a). Conversely it was shown that the
extent of BBB impairment correlates with seizure duration (Cornford & Oldendorf,
1986). The aforementioned findings, and the fact that BBB leakage was detected in

State Of Research
12
the early phase of epileptogenesis around the time of the brain insult (Rigau et al.,
2007; van Vliet et al., 2007b; Ndode-Ekane et al., 2010), suggest that BBB-protective
therapies are promising strategies for the prevention of epilepsy (Marchi et al., 2012).
However, preclinical studies propose that the therapeutic time window after brain
insults is rather narrow (Herman, 2002). This underlines the need of suitable
biomarkers to identify patients at risk as early as possible during epileptogenesis
(figure 3). BBB leakage might be such a biomarker for epileptogenesis as it plays a
key role in the induction of epileptogenesis and in seizure generation (Vezzani &
Friedman, 2011; van Vliet et al., 2014b). Despite, the number of studies investigating
the presence of BBB leakage in this context is limited. Thus, the occurence of BBB
leakage and its role in epileptogenesis need to be further investigated. Studies are
needed to better delimit the occurrence of BBB impairment and to identify the most
suitable time window for selected BBB-protective treatment approaches. Molecular
imaging modalities provide the possibility for this by obtaining longitudinal in vivo
information on BBB integrity.
Brain insult First clinical seizure Chronic epilepsy
Blood-brain barrier disturbance
Epileptogenesis only in minority of patiens → predicitive biomarkers
urgently needed
Latency phase
Possible time window for
antiepileptogenic treatment
Epileptogenesis
Figure 3: Epileptogenesis and possible time window for antiepileptogenic therapy
As only a limited number of brain insults result in epilepsy, biomarkers for epileptogenesis are urgently needed to identify at-risk patients as early as possible during epileptogenesis. Blood-brain barrier leakage is strongly associated with the initiation and progression of epileptogenesis, thus being a candidate biomarker. The latency period between initial brain insult and first clinical seizure offers a time window for future antiepileptogenic treatments in identified patients at risk with the long-term goal to prevent the development of epilepsy.
1.3.2 The blood-brain barrier and inflammation
Interactions between brain endothelium and astrocytes can influence BBB integrity in
both physiological and pathological conditions (Abbott et al., 2006). Recent studies

State Of Research
13
point to an involvement of BBB impairment and subsequent albumin extravasation in
TGFßRII-mediated astrocytic transformation and its role in epileptogenesis (Ivens et
al., 2007). Astrocytes are involved in neuronal hyper-synchronicity and excitability
(Friedman et al., 2009). Activated Astrocytes and microglia cells can release pro-
inflammatory mediators (Allan et al., 2005) in response to seizures (Vezzani et al.,
2011). In the pilocarpine post SE rat model, increased interleukin-1ß (IL-1ß) and IL-1
receptor expression is present in parallel to BBB leakage (Ravizza et al., 2008).
Accumulating evidence suggests that IL-1ß is related to increased seizure
susceptibility and epileptogenesis (Vezzani & Baram, 2007; Ravizza et al., 2008).
Besides brain inflammation, peripheral inflammation is related to BBB impairment,
too. For example, an overexpression of BBB adhesion molecules was found to occur
in response to epileptiform neuronal activity in an experimental in vitro guinea pig
model (Librizzi et al., 2007). Circulating leucocytes bind to adhesion molecules at the
apical endothelium, a mechanism which can result in decreased BBB integrity and
subsequent brain edema as well as extravasation of blood components. These
components again trigger microglia activation (Rivest et al., 2000; Riazi et al., 2010).
Thus, a pharmacological treatment targeting inflammation and leucocyte-BBB
interactions might stabilize BBB integrity following SE.
1.4 Treatment strategies targeting blood-brain barrier integrity
Starting from the assumption (see 1.3.1) that a dysfunctional BBB integrity plays a
central role in epileptogenesis (Oby & Janigro, 2006; van Vliet et al., 2007b; Marchi
et al., 2011b; Vezzani et al., 2011; Abbott & Friedman, 2012), pharmacotherapeutic
approaches to restore or to maintain BBB integrity may help to modify or to prevent
epileptogenesis (Dedeurwaerdere et al., 2007). Possible therapeutic options include
targeting inflammation along with peripheral immune responses, changes in
metabolic equilibrium, glutamate receptor activation, increased blood pressure or
angiogenesis.
In a rat model of focal cerebral ischemia, cyclooxygenase-2 (COX-2) inhibition using
nimesulide led to decreased BBB impairment and reduced leukocyte infiltration
(Candelario‐Jalil et al., 2007). Another target for protection of BBB integrity

State Of Research
14
(see 1.3.2) are leukocyte-endothelial interactions (Fabene et al., 2008). For example,
BBB leakage was prevented by blockade of leukocyte-vascular adhesion via α4
integrin specific antibodies after pilocarpine induced SE in mice (Fabene et al.,
2008). In a mouse model of cerebral malaria, increased BBB permeability, amongst
other things, was reduced by fingolimod (FTY720), a modulator of the sphingosine-1-
phosphate signaling cascade, in combination with the tyrosine kinase inhibitor
imatinib (Nacer et al., 2012). Another possible therapeutic approach is directed to
nitric oxide which can contribute to ischemia-induced inflammation and deterioration
of BBB integrity. Curcumin is a polyphenol which balances different cell signaling
pathways (Gupta et al., 2013). A single injection of curcumin following focal
ischemia/reperfusion in rats led to a reduced extravasation of Evans blue (Jiang et
al., 2007). As underlying mechanism, the authors suggest BBB protection, mediated
by a reduced incidence of nitric oxide and subsequently a reduced damage to
endothelial cells (Jiang et al., 2007).
Another interesting approach to prevent BBB leakage is treatment with an
angiotensin II type 1 receptor antagonist, losartan, which is clinically approved for
patients with hypertension. Different studies have shown that hypertension has
detrimental effects on BBB integrity (Bauer et al., 2011) and that blood pressure
influences seizure-induced BBB impairment (Nitsch & Klatzo, 1983; Bauer et al.,
2011). In diabetic rats with epinephrine-induced hypertension, losartan treatment
resulted in a significant reduction of BBB permeability (Kaya et al., 2003).
Ivanova et al. (2013) found that in the systemic kainate rat model, all animals that
were chronically treated with losartan (treatment started during SE) developed
spontaneous seizures. However, the latent period was significantly longer in
losartan-treated rats as compared to controls, suggesting epileptogenesis-modifying
effects of losartan. Moreover, anxiety levels were reduced and diurnal rhythms in
locomotor activity were absent in losartan-treated animals.
Tchekalarova et al. (2014a) compared the onset of kainate-induced seizures in
hypertensive and normotensive rats following 14 d of subcutaneous (s.c.) losartan
application. Losartan did not affect the seizure intensity but slowed down seizure
onset in the hypertensive group. Moreover, kainate-induced lipid peroxidation was
weakened in both groups. Thus, the authors suggest losartan to be beneficial as an
adjunctive treatment in SE by limiting oxidative stress and neurotoxicity.

State Of Research
15
Pereira et al. (2010) showed that angiotensin II type 1 receptors are upregulated in
the brain of a rat epilepsy model and that the receptors are implicated in seizure
susceptibility. Losartan treatment resulted in a significant decrease in both frequency
and severity of epileptic seizures. In a recent study (Bar‐Klein et al., 2014), losartan
treatment was shown to prevent the occurrence of delayed recurrent seizures by
blocking albumin-induced TGF-ß activation in a rat model of vascular injury-induced
epileptogenesis. Tchekalarova et al. (2014b) found that losartan treatment after
kainate-induced SE alleviated seizure activity, extended the seizure-free latency
phase and decreased the frequency of seizures. Moreover, epilepsy-associated
behavioral changes like anxiety and depression were positively influenced by
losartan.
Other studies have shown that, inter alia, inflammatory reactions at the BBB are
relevant for the development of seizures (see 1.3.2). Thus, treatment with
glucocorticoids such as dexamethasone, which is widely used as an anti-
inflammatory and brain edema-reducing drug (Kaal & Vecht, 2004; Abbott et al.,
2006), may positively affect BBB integrity (Oby & Janigro, 2006; Marchi et al., 2012).
Dexamethasone increases the tightness of endothelial tight junctions (Cucullo et al.,
2004). Moreover, it can change BBB properties by regulation of efflux pumps like
p-glycoprotein which is highly expressed in endothelial brain cells (Bauer et al., 2005)
as well as by modulating gene transcription (Cucullo et al., 2004). In specific
neoplastic and inflammatory processes of the brain, glucocorticoids are BBB
protective and alleviate brain edema (Friedman & Heinemann, 2010). In a rat model
of allergic encephalomyelitis, increased BBB permeability could be counteracted
dose-dependently by short-term treatment with the broad-spectrum glucocorticoid
dexamethasone (Paul & Bolton, 1995). On the other hand, glucocorticoids are
ineffective or even harmful in patients with acute ischemic stroke (Kleinschnitz et al.,
2011). Adverse effects after dexamethasone treatment were published recently in the
lithium-pilocarpine post SE rat model, too. Duffy et al. (2014) found a deterioration of
both brain injury and survival rate following dexamethasone treatment.

State Of Research
16
1.5 Animal models of epileptogenesis
Despite major research on alternative methods, it is so far impossible to dispense the
use of rodent models in epilepsy research as appropriate in vitro models allowing for
investigation of the complex underlying pathological mechanisms of epileptogenesis
are hitherto not available (Raol & Brooks-Kayal, 2012; Stewart et al., 2012).
Thus, chronic epilepsy models with spontaneously occurring seizures following a
primary brain insult are commonly used to investigate epileptogenesis (Löscher,
2002). These include chemical and electrical post-SE models, traumatic brain insult
models, the kindling model, febrile convulsion models as well as stroke models (Ben-
Ari et al., 1979; Honchar et al., 1983). These models allow for examinations of
epileptogenesis over the entire course of time. The post SE models are characterized
by a model-dependent latency phase preceding the occurrence of seizures (see 1.2).
The post SE models are particularly recommended for anti-epileptogenesis studies
(Stables et al., 2003) because these models of epileptogenesis display different
phenotypic features, for example a latent period varying in length (Galanopoulou et
al., 2012; White & Löscher, 2014). Chemical post-SE models are characterized by a
relatively short latency period and a high seizure frequency. Models that do not
exhibit these characteristics might abet false positive or false negative results.
1.5.1 The pilocarpine post status epilepticus rat model
Pilocarpine is an excitatory acetylcholine receptor agonist that evolves
parasympathomimetic effects via binding to the muscarinic subtype of acetylcholine
receptors (Hamilton et al., 1997). Subsequently, seizures are supposed to be
maintained via activation of NMDA receptors (Smolders et al., 1997). This leads to
increased hippocampal glutamate levels, triggering limbic seizures and SE. After
pilocarpine injection, animals display akinesia, ataxia, facial automatisms and
complex partial seizures that generalize secondarily (Turski et al., 1984; Turski et al.,
1989). SE is followed by a latent period, characterized by structural reorganization
processes and later by the appearance of spontaneous recurrent seizures (Curia et
al., 2008).

State Of Research
17
1.5.2 The intrahippocampal kainate mouse model
Kainate is an agonist at glutamate receptors. It induces sustained neuronal
depolarization, resulting in SE. In the intrahippocampal kainate model, kainate is
administered via microinjection directly into the hippocampus of mice (Suzuki et al.,
1995; Bouilleret et al., 1999; Gröticke et al., 2008; Klein et al., 2014) or rats (Bragin et
al., 1999; Dudek et al., 2006). Animals develop a non-convulsive SE that persists
over several hours (Bouilleret et al., 1999; Gröticke et al., 2008; Maroso et al., 2011).
Generalized tonic-clonic seizures occur only rarely in mice (Riban et al., 2002). After
a latency period, frequent spontaneous and focally limited seizures occur. This model
is regarded one of the best models for TLE due to its resemblance to the clinical
situation (Sharma et al., 2007).
Still, the neurohistopathological changes occurring in the pilocarpine and focal
kainate models are very similar to those of patients with TLE, too. Histopathological
findings include neurodegeneration in hippocampal subregions, hippocampal
sclerosis as well as aberrant mossy fibre sprouting in the inner molecular layer of the
dentate gyrus in both models (Turski et al., 1983; Bouilleret et al., 1999; Pernot et al.,
2011). Moreover, behavioral, learning and memory deficits occur in the pilocarpine
model (Curia et al., 2008). As there is no model which simulates all relevant aspects
of disease, it can be useful to apply different models.
1.6 Non-invasive in vivo imaging of blood-brain barrier leakage
Figure 4: Principle mechanism for detection of blood-brain barrier leakage
The blood-brain barrier (BBB) functions as interface between blood and brain. Intravenously administered exogenous markers or endogenous markers deriving from the blood are excluded from entry into the brain under physiological conditions (left). A leaky BBB allows entry of these molecules, which can subsequently be detected in affected brain regions (right).
Blood vessel
Brain
BBB
Tracer / Contrastagent

State Of Research
18
Different markers and methods have been used to visualize changes in BBB integrity
in both pre-clinical and clinical settings. The mechanism underlying them all is the
detection of blood-derived endogenous molecules or injected exogenous tracers that
cannot pass the intact BBB (see
figure 4) due to their polarity or molecular weight (Friedman et al., 2009). In the event
of BBB impairment, tracer extravasation into specific brain regions can be detected
and quantified (van Vliet et al., 2014a). Suitable in vivo imaging techniques for this
purpose include positron emission tomography (PET), single photon emission
computed tomography (SPECT), MRI and optical imaging.
Nuclear medicine imaging is an evolving field in small animal imaging. Until the
1950s, hand-held Geiger-Müller tubes were in general use to detect biodistribution of
radioactivity in patients (Allen Jr et al., 1951). The tubes reacted only to about 2 % of
total gamma ray emission; images were not generated. Since then, the technology
has evolved remarkably. Recent advances in small animal imaging technology have
facilitated the application of clinical PET and SPECT radiotracers for pre-clinical
small animal imaging. The continuing improvement in resolution and sensitivity has
permitted to study biomolecular changes in the brain during epileptogenesis
(Dedeurwaerdere et al., 2007). Both PET and SPECT as well as MRI allow for serial
non-invasive measurements in the same animal, supporting accurate assessment of
pathogenesis and pharmacological agent efficacy (Roselt et al., 2004). Thus, modern
non-invasive imaging methods can be valuable diagnostic tools for in vivo
investigation of BBB permeability changes during epileptogenesis (Wunder et al.,
2012). A great advantage of these methods is the fact that the same protocols can be
used for animal research and clinical applications. This facilitates the translation of
pre-clinical research into medical practice. In addition, the statistical power of
preclinical studies can be increased if each animal serves as its own control (Cherry
& Gambhir, 2001), resulting in reduced numbers of required experimental animals
(Cherry & Gambhir, 2001; Bankstahl & Bankstahl, 2012).
1.6.1 Positron Emission Tomography imaging
PET is a dynamic and non-invasive molecular imaging technique that allows in vivo
visualization of the spatial and temporal distribution of radiolabeled biological or

State Of Research
19
pharmacological ligands or metabolic substrates, so-called radiotracers (Cherry &
Gambhir, 2001). Strengths of PET imaging involve high sensitivity, depth of
penetration and quantification. The spatial resolution is 5-7 mm in clinical and 1-2
mm in preclinical setups; the temporal resolution is seconds to minutes (James &
Gambhir, 2012). The method is based on decay of positron-emitting radionuclides
(see figure 5). After intravenous (i.v.) administration to the subject or animal, the
isotope is subjected to ß+-decay. It releases a positron from the nucleus which is
positively charged and has the mass of an electron. Upon collision with an electron
originating from the surrounding tissue, the positron annihilates, generating two
anti-parallel high energy photons of 511 keV. The emitted γ-radiation is measured
noninvasively using a PET camera as external detector. The camera comprises a
ring of detectors which are able of coincidence timing detection of the emitted
photons. Afterwards, the photons are converted into an electrical signal. Within the
field of view, iterative and non-iterative reconstruction algorithms create a map of
activity distribution over time. Thereby, dynamic images as well as time-activity
curves can be generated for regions of interest (Koeppe, 2002; Thompson, 2002;
Cherry & Dahlbom, 2004).
Radiotracer
e+
e+ e-511 keV
photon
511 keV
photon
*
*Coincidence
count
A B
Figure 5: Positron emission tomography imaging
A tracer labeled with a positron-emitting radioisotope is injected. The tracer circulates and binds to or accumulates in target structures. (A) Emitted positrons collide with electrons from the surrounding target tissue. The positron annihilates and generates two anti-parallel photons (511 keV). (B) Two photons, that strike opposing detectors at the same time, are counted as coincidences. The location of annihilations is calculated by observing multiple events. Electrical signals are converted into sinograms which are subsequently reconstructed to images. Figure modified from (Herschman, 2003).

State Of Research
20
In vivo studies of epileptogenesis can benefit from PET as it enables the study of
functional metabolic processes with high sensitivity and accurate quantification. PET
has been used to study receptor-ligand interactions, enzyme activity, protein-protein
interactions, gene expression as well as cell- and gene-therapy (Herschman, 2003).
For example, PET allows the examination of glucose metabolism, protein synthesis
and neuro-receptor status in different cerebral diseases. Suitable PET tracers and
imaging protocols would permit for early assessment of BBB leakage as a potential
biomarker for epileptogenesis and for monitoring BBB-protective pharmacological
agent efficacy (Bankstahl & Bankstahl, 2012; Neal et al., 2013).
2-[18F]-fluoro-2-deoxy-D-glucose ([18F]-FDG) is currently the most widely used tracer
in epilepsy diagnosis (Dedeurwaerdere et al., 2007). It allows an indirect statement
on neuronal activity by quantitative determination of regional cerebral glucose
metabolism. [18F]-FDG is transported into cells by glucose transporters equivalent to
normal glucose (Phelps, 2000). Inside the cell, the tracer is converted to the
phosphorylated form by hexokinase. This form cannot be further metabolized and
gets "trapped" inside the cells. Its accumulation displays regional glucose utilization
patterns which can be measured by PET. In human medicine, [18F]-FDG PET scans
are used in epilepsy patients in whom MRI cannot clearly locate the epileptic focus
prior to surgery (Bankstahl & Bankstahl, 2012). Interictally, the epileptic focus is
usually characterized by a relative glucose hypometabolism. The regional extent of
hypometabolism was shown to increase with seizure frequency and duration of
disease and extends beyond the epileptic focus (Goffin et al., 2008). The reason for
this is so far unknown (Goffin et al., 2008). Preclinical [18F]-FDG PET studies after
acute kainate-induced SE demonstrated a glucose hypermetabolism primarily in the
hippocampus and entorhinal cortex (Kornblum et al., 2000; Mirrione et al., 2006). In
analogy to the situation in patients, longitudinal [18F]-FDG PET examinations in
chronic epilepsy models revealed hypometabolic changes in the course of
epileptogenesis. These changes began shortly after the initial insult and partially
persisted in the chronic phase (Goffin et al., 2009; Guo et al., 2009; Jupp et al., 2012;
Lee et al., 2012).
In addition to [18F]-FDG PET, which contributes to a better understanding of the local
brain metabolic activity, PET radiotracers are of great interest as they might enable

State Of Research
21
investigation of changes in BBB permeability during epileptogenesis. Imaging BBB
permeability changes requires peripheral administration of non-permeable tracers
(Friedman et al., 2009). 68Gallium-ethylenediaminetetraacetate ([68Ga]-EDTA) is a
hexadentate chelator which cannot pass the intact BBB due to its molecular weight.
[68Ga]-EDTA PET was successfully used to assess BBB permeability in multiple
sclerosis patients (Pozzilli et al., 1988). So far, no PET tracers for detecting BBB
leakage have been used in epilepsy research. PET with a new tracer, [68Ga]
combined with the chelating agent diethylenetriamine pentaacetic acid
([68Ga]-DTPA), might be another appropriate approach (see manuscript 1, chapter 2).
A similar tracer, [99mTc]-DTPA, is a standard SPECT tracer for detecting BBB leakage
in patients (see 1.6.2). Moreover, a gadolinium (Gd) formulation combined with DTPA
as chelate (Gd-DTPA) is frequently used as contrast agent (CA) for detecting BBB
leakage on MRI in pre-clinic and clinic (see 1.6.3).
Other possible tracer candidates for imaging of BBB function include [68Ga]-albumin,
as albumin can only cross the BBB in pathological conditions (see 1.3.1),
[13N]-glutamate or [82Rb]-chloride (Saha et al., 1994; Wunder et al., 2012). Yen et al.
have demonstrated osmotically evoked BBB opening in rhesus monkeys using
[82Rb]-chloride (Yen & Budinger, 1981). Comparable studies in epilepsy models have
not yet been performed.
1.6.2 Single Photon Emission Computed Tomography imaging
SPECT is the most frequently used nuclear imaging technique in the clinic (Lecchi et
al., 2007). It is based on scintigraphy technique. The used nuclides emit single γ-rays
with different energies (James & Gambhir, 2012). A gamma camera captures data
from diverse positions by rotating around the subject or animal. The higher the
metabolic activity, the more accumulation of the radiolabeled tracer occurs in the
tissue. As it is not possible to obtain information on the photons origin as it is in PET,
a collimator is used which rejects diagonally incident photons. Hence, as many
photons are rejected, SPECT imaging is less sensitive than PET imaging. Its spatial
resolution is 8-10 mm in clinical and 1-2 mm in preclinical setups; its temporal
resolution is minutes (James & Gambhir, 2012). Nevertheless, SPECT tracers
generally have a longer half-life compared with PET tracers and are more readily
available. Advantages of SPECT include depth of penetration and multiplexing

State Of Research
22
capabilities, meaning that different targets can be imaged simultaneously. Moreover,
SPECT is less expensive than PET. As PET and SPECT detect biochemical changes
and these usually occur prior to anatomical changes, they have a diagnostic
advantage in imaging acute processes compared to computed tomography (CT) and
MRI (James & Gambhir, 2012). However, by combining MRI and highly sensitive
nuclear medicine molecular imaging, the advantages of both techniques can be
combined (Blamire, 2014).
The SPECT tracer [99mTc]-DTPA was developed in 1969 for the study of brain,
kidneys and vascular dynamics (Hauser et al., 1970). The aims were to combine the
physical properties of the radionuclide [99mTc] with the advantageous biological
properties of the chelating agent DTPA. About 90 % of the tracer is excreted in 24 h
via the kidneys (Hauser et al., 1970). A preclinical study has shown that ultrasound-
induced (Lin et al., 2009) increased BBB permeability can be detected and quantified
using [99mTc]-DTPA SPECT. The same is true for BBB leakage following seizures
arising in connection with stroke in humans (Gilad et al., 2012). Moreover,
[99mTc]-DTPA was used for the detection of brain tumors in an animal model and
revealed subtle BBB leakage (Singh et al., 1991). Another tracer that might be used
for SPECT-imaging of BBB leakage is [99mTc]-albumin (Saha et al., 1994). Both
tracers cannot cross the intact BBB due to their molecular weight (Lampl et al.,
2005). These facts make [99mTc]-DTPA and [99mTc]-albumin promising tracers for the
study of BBB leakage in epileptogenesis models.
1.6.3 Magnetic Resonance imaging
MRI technique is based on electromagnetic effects of rotating hydrogen nuclei in
organic compounds. When placed inside a magnet, unpaired nuclear spins inside the
body function like magnetic dipoles (James & Gambhir, 2012). A radio frequency
electromagnetic pulse is applied, followed by a return to equilibrium (Gröhn &
Pitkänen, 2007). The dipoles arrange parallel or anti-parallel to the magnetic field,
thus producing a small net difference between numbers of parallel and anti-parallel
aligned dipoles. From this difference, the nuclear magnetic resonance (NMR) signal
is generated. Magnetic field gradients can be used to locate and assign the signals
source (Gröhn & Pitkänen, 2007), providing adequate signal-to-noise ratio and
images with excellent resolution. The MR signal is primarily dependent upon three

State Of Research
23
factors: the concentration of nuclei and their constant spin around the axes, the
gyromagnetic ratio, which can be determined from the magnetization as well as from
the angular momentum (Greiner & Müller, 1994), and the polarization (James &
Gambhir, 2012).
Compared with nuclear medicine techniques, MRI stands out due to its excellent
spatial resolution (pre-clinical 25-100 µm, clinical ~ 1 mm, James & Gambhir, 2012)
and a high soft tissue contrast which makes it irreplaceable in particular for high
resolution in vivo visualization of anatomical changes in the brain and in cerebral
blood flow. The temporal resolution is minutes till hours. MRI is a very versatile
imaging technique (Blamire, 2014). However, due to its limited sensitivity, the ability
of MRI to display functional changes is limited (James & Gambhir, 2012).
Nevertheless, during recent years, spatial resolution has continuously improved in
MRI, allowing for better imaging protocols for BBB leakage in patients (Chassidim et
al., 2015) and providing the basis for evaluation of epileptic progression (Marchi et
al., 2012). Moreover, since MRI does not require exposure to radiation, it can be
performed repeatedly in both animals and patients (Runge et al., 1985; Neumann-
Haefelin et al., 2000). This is true for pre-clinical PET and SPECT as well. However,
radiation protection regulations need to be taken into consideration for personnel and
patients. Despite these advantages, MRI is still much less used in pre-clinical
epilepsy research than used in the clinic (Marchi et al., 2012).
Different changes in the brain can be assessed using MRI during epileptogenesis.
Cytotoxic edema, resulting from a breakdown of sodium-calcium pumps and
subsequent water imbalances between intracellular and extracellular compartments
(BBB is intact), occurs during and shortly after SE and can be detected using
diffusion-weighted MRI (Gröhn et al., 2011). Subsequent vasogenic edema, a
consequence of BBB leakage, can be assessed with T2-weighted MRI sequences.
T2 (transversal relaxation time) and T1 (longitudinal relaxation time) define the return
of hydrogen nuclei towards equilibrium after they were excited by radio frequency
pulses (Gröhn & Pitkänen, 2007) which are influenced by water dynamics. Thus, the
focus of contrast can be drawn for example on T2 or T1 relaxation or water diffusion
by modifying pulse sequences.

State Of Research
24
Table 1: Representation of T1- and T2-contrast on MRI
Contrast Repetition time (TR)
=Transverse magnetization
Echo time (TE)
=Selective magnetization
Representation
T1 short short (< T2) Tissue with short T1 = bright
Tissue with long T1 = dark
T2 long (> T1) long Tissue with short T2 = dark
Tissue with long T2 = bright
T1-weighted MR sequences have a short repetition time and a short echo time (TE). Therefore, proton density and T2 relaxation have only low influences. Differences in signal intensities largely depend on the T1 relaxations of the tissue. T2-weighted MR sequences have a long TE. With increasing TE, signals diverge and the signal intensity of spin echoes is dependent from the T2 relaxations of the tissue.
Water and fat appear hyperintense in T2-weighted MRI. T2-weighted MR sequences
can detect edema formation. Contrast-enhanced MRI is a method to study BBB
leakage. Extravasated CA shortens the T1-relaxation time in affected brain regions
which are subsequently represented by bright signals on MRI images. An exogenous
way of contrast modification is i.v. injection of MRI CA. The utilization of Gd-based
MRI CA, such as Gd-DTPA, is considered the gold standard for non-invasive
assessment of BBB leakage (Tofts & Kermode, 1991). Gd-DTPA was the first
paramagnetic CA and clinically approved in 1988. It is excluded from brain entry due
to its polarity and molecular weight of 550 dalton (Da) in physiological conditions
(Kassner & Thornhill, 2011), has a half-life of 1.5 h and is excreted via the kidneys.
Other MRI CA used for detecting BBB leakage include gadobutrol and Gd-albumin.
Gd injections result in T1 hyperintensity via shortening of the T1 relaxation time, thus
improving image quality.
In epilepsy models, MRI was first applied in 1988. Karlik et al. (1991) examined rats
with an epileptic focus induced via penicillin application and King et al. (1991) found a
difference in image contrast between edematous and normal brain tissue in the
kainate rat model using diffusion tensor imaging (DTI). Until today, diverse studies
were performed in animal models, including T1- und T2-weighted MRI, functional
MRI, diffusion weighted imaging (DWI) as well as DTI (Marchi et al., 2012). However,
only few longitudinal MRI studies targeting structural reorganization processes during

State Of Research
25
epileptogenesis have been performed whilst most MRI studies in epilepsy models
have concentrated on neuronal loss (Gröhn & Pitkänen, 2007).
Different studies demonstrated the usability of MRI to localize brain regions with
increased BBB permeability and to quantify the extent of BBB leakage in
experimental models and in humans (Dijkhuizen, 2011; Kassner & Thornhill, 2011).
Using bolus injections of CA in the pilocarpine post SE rat model, acute BBB leakage
was only detected in the thalamus at 2 h after SE (Roch et al., 2002). Yet, it was not
possible to detect subtle BBB leakage occurring later in disease as shown by
histology results (van Vliet et al., 2007b; van Vliet et al., 2014b). In a rat model of
stroke following unilateral reperfused cerebral ischemic infarct, Nagaraja et al. (2007)
showed that a step-down infusion of Gd-DTPA reveals subtle BBB leakage that was
not detected in the same model using bolus injection. Bolus injection caused a sharp
increase in CA concentration with peak at around 10 s after administration which
declined after a short period of time. Step-down infusion resulted in a sharp rise and
subsequently almost steady-state of CA concentration over the entire period of scan
time. The authors concluded that, using the infusion protocol, higher plasma
concentrations result in increased CA extravasation into the brain parenchyma
compared to bolus injection, thus providing the possibility to detect even subtle BBB
leakage that cannot be observed using bolus injections. The suitability of infusion
protocols was confirmed in another stroke model (Knight et al., 2009) and in an
epilepsy rat model after systemic kainate-induced SE using a dynamic and a post-pre
approach (van Vliet et al., 2014b).

State Of Research
26
1.7 Aim of the studies
1.7.1 Study 1: Multimodality imaging of blood-brain barrier impairment during
epileptogenesis
The aim of this study was to determine [68Ga]-, [99mTc]- and gadolinium Gd-labelled
DTPA as well as Gd-albumin and gadobutrol uptake for the detection of BBB leakage
after lithium-pilocarpine induced SE as an epileptogenic brain insult using small
animal PET, SPECT and MRI in rats.
The working hypotheses were:
1. [68Ga]-DTPA PET, [99mTc]-DTPA SPECT and contrast-enhanced MRI allow for
early detection of BBB leakage following lithium-pilocarpine induced SE.
2. [68Ga]-DTPA PET is the most sensitive of the evaluated molecular imaging
techniques for detection of BBB leakage during early epileptogenesis.
3. PET detects BBB leakage more sensitive after step-down infusion of [68Ga]-DTPA
compared to bolus injection of [68Ga]-DTPA.
1.7.2 Study 2: Longitudinal in vivo evaluation and pharmacotherapy of blood-
brain barrier leakage in a rat model of epileptogenesis
The first objective of this study was to assess a non-invasive theranostic imaging
marker for BBB leakage longitudinally during early epileptogenesis. The second
objective was to evaluate whether two potentially BBB-protective treatments, losartan
and dexamethasone, can alleviate vascular edema and preserve BBB integrity during
early epileptogenesis in the lithium-pilocarpine post SE rat model. To this end, the
MRI protocol for Gd-DTPA from study 1 was used.
The working hypotheses were:
1. Longitudinal MRI following step-down infusion of the CA Gd-DTPA allows
detection of the peak increase in BBB leakage during early epileptogenesis.
2. Dexamethasone and losartan possess BBB-integrity stabilizing properties which
can be detected using the aforementioned MRI protocol.

State Of Research
27
1.7.3 Study 3: Dexamethasone protects blood-brain barrier integrity in a
mouse model of epileptogenesis
The aim of this study was to assess a non-invasive theranostic imaging marker for
BBB leakage longitudinally during early epileptogenesis in the intrahippocampal
mouse model using in vivo 7 T MR imaging following a step-down Gd-DTPA infusion
protocol. Dexamethasone treatment was evaluated with regard to BBB protection at
2 d and 4 d post SE.
The working hypotheses were:
1. MRI following step-down CA infusion is a suitable imaging biomarker for the
detection of BBB leakage in the intrahippocampal kainate mouse model.
2. Dexamethasone treatment improves BBB integrity following intrahippocampal
kainate injection as assessed by MRI.

Multimodality Imaging Of Blood-Brain Barrier Impairment During Epileptogenesis
28
2 Multimodality Imaging Of Blood-Brain Barrier Impairment During Epileptogenesis
Heike Breuer1,2, Martin Meier3, Sophie Schneefeld1, Wolfgang Härtig4, Alexander
Wittneben1, Martin Märkel4, Tobias L. Ross1, Frank M. Bengel1, Marion Bankstahl2,
Jens P. Bankstahl1*
1 Department of Nuclear Medicine, Hannover Medical School, Germany
2 Institute of Pharmacology, Toxicology and Pharmacy, University of VeterinaryMedicine Hannover and Center for Systems Neuroscience, Germany
3 Preclinical Imaging Labs, Central Laboratory Animal Facility & Institute for Laboratory Animal Science, Hannover Medical School, Germany
4 Paul Flechsig Institute for Brain Research, University of Leipzig, Germany
* Corresponding author: Jens P. Bankstahl, PhD, Department of Nuclear Medicine,
Hannover Medical School, Carl-Neuberg-Str. 1, 30625 Hannover, Germany. Tel.:
+49-511-532-3504; Fax: +49-511-532-3761; Email: [email protected]
Published in
Journal of Cerebral Blood Flow and Metabolism (Epub ahead of print)
DOI: 10.1177/0271678X16659672
Financial support: This study was funded by the European Union Seventh’s
Framework Programme (FP7/2007-2013) under grant agreement n°602102
(EPITARGET). H. Breuer was supported by a scholarship from the Studienstiftung
des Deutschen Volkes.
Running headline: Multimodal BBB imaging during epileptogenesis

Multimodality Imaging Of Blood-Brain Barrier Impairment During Epileptogenesis
29
Abstract
Objective: Insult-associated blood-brain barrier (BBB) leakage is strongly suggested
to be a key step during epileptogenesis. In this study, we used three non-invasive,
translational imaging modalities, i.e. positron emission tomography (PET), single
photon emission computed tomography (SPECT), and magnetic resonance imaging
(MRI), to evaluate BBB leakage after an epileptogenic brain insult.
Materials and methods: Sprague-Dawley rats were scanned during early
epileptogenesis initiated by status epilepticus (SE). PET and SPECT scans were
performed using the novel tracer [68Ga]DTPA or [99mTc]DTPA, respectively. MRI
included T2 and post-contrast T1 sequences after infusion of Gd-DTPA, gadobutrol
or Gd-albumin.
Results: All modalities revealed increased BBB permeability 48 h post SE, mainly in
epileptogenesis-associated brain regions like hippocampus, piriform cortex,
thalamus, or amygdala. In hippocampus, Gd-DTPA-enhanced T1 MRI was increased
by 199%, [68Ga]DTPA PET by 37%, and [99mTc]DTPA SPECT by 56%. Imaging
results were substantiated by histological detection of albumin extravasation.
Conclusions: Comparison with quantitative PET and SPECT shows that MRI
sequences successfully amplify the signal from a moderate amount of extravasated
DTPA molecules, enabling sensitive detection of BBB disturbance in epileptogenesis.
Imaging of the disturbed BBB will give further pathophysiologic insights, will help to
stratify anti-epileptogenic treatment targeting BBB integrity, and may serve as a
prognostic biomarker.
Key words: Blood-brain barrier, epilepsy, imaging, MRI, PET

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
30
3 Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
H. Breuer1,2, M. Meier3, W. Härtig4, J.P. Bankstahl2, M. Bankstahl1 1 Institute of Pharmacology, Toxicology and Pharmacy, University of Veterinary
Medicine Hannover and Center for Systems Neuroscience, Germany
2 Preclinical Molecular Imaging, Department of Nuclear Medicine, Hannover Medical School, Germany
3 Preclinical Imaging Labs, Central Laboratory Animal Facility & Institute for Laboratory Animal Science, Hannover Medical School, Germany
4 Paul Flechsig Institute for Brain Research, University of Leipzig, Germany
The extent of author’s contributions to this work:
A) Design of project: J.P.B., M.B.
B) Design of experiments: H.B., J.P.B., M.B., M.M., W.H.
C) Performance of experiments: H.B., M.M., M.B., W.H.
D) Analysis of experiments: H.B., M.B.
E) Writing and revision of manuscript: H.B., M.B., J.P.B.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
31
3.1 Abstract
Objective: Blood-brain barrier (BBB) leakage is a frequent finding in association with
brain insults and may contribute to both initiation and progression of epilepsy. Hence,
BBB leakage might be a suitable biomarker for epileptogenesis and BBB-stabilizing
treatment might prevent or attenuate epileptogenesis. In this study, longitudinal
contrast-enhanced in vivo magnetic resonance imaging (MRI) was performed for
evaluation of BBB impairment during early epileptogenesis. Moreover, BBB integrity
and edema formation, as assessed by MRI, were used as surrogate markers for the
evaluation of potentially BBB-protective effects of losartan and dexamethasone.
Materials and methods: As primary brain insult, a status epilepticus (SE) was
induced by fractionated pilocarpine injection in 27 adult female Sprague-Dawley rats.
For longitudinal assessment of BBB leakage, one group of saline-treated (SE-saline)
rats was scanned before and 5 h, 48 h, 10 d (n = 5) and 4 d (n = 6 additional rats)
following SE. Six rats were treated with dexamethasone (SE-dexamethasone, 3 and
24 h post SE, 8 mg/kg i.p.; 48 h post SE, 4 mg/kg i.p.) and 5 rats with losartan
[SE-losartan, 30 min post SE, 50 mg/kg i.p.; 24 h till 5 d post SE, 5 mg/kg i.p. twice
daily; day 6 till 14, 80.4±38.1 mg/d, mean±standard error of the mean (SEM)],
respectively. Five additional rats (SE) which received no treatment after SE served
as controls for the SE-dexamethasone group. Animals of treatment groups were
scanned baseline and 48 h after SE and additionally 5 h and 10 d after SE in the
losartan-treated group. The MRI setup included a T2 sequence, followed by infusion
of gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA) and post-contrast T1
modified driven equilibrium fourier transformation (MDEFT). MR images were
analyzed by co-registration with a rat brain atlas and calculation of T1 and T2 signal
increase, normalized to pons. For histological evaluation of BBB integrity, animals
were infused with FITC-labelled albumin (100 mg/kg) and perfused thereafter.
Results: In SE-saline rats, BBB leakage was detected in hippocampus, amygdala,
thalamus, entorhinal cortex, piriform cortex, substantia nigra and frontal cortex at
48 h post SE. Moreover, BBB leakage was detected in the amygdala and in the
piriform cortex at 4 d post SE as well as in the entorhinal and piriform cortex at 10 d

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
32
post SE. Neither dexamethasone nor losartan protected BBB integrity. The spatial
extent of T1 intensity increase was comparable between SE-losartan and SE-saline
groups 48 h post SE. At 10 d, increased T1 values were only present in SE-losartan
animals (entorhinal cortex and piriform cortex). T2 signals, indicative of brain edema,
were significantly increased in SE-losartan vs. SE-saline rats at 48 h post SE in
substantia nigra and, like T1 values, present only in SE-losartan animals (entorhinal
cortex) at 10 d after SE. Dexamethasone treatment did not influence T1 values but
significantly increased T2 signals in the piriform cortex 48 h post SE vs. SE-saline.
Histological analysis revealed a significant increase of extravasation in the SE group
in amygdala, piriform and entorhinal cortex. Dexamethasone treatment resulted in
significantly more severe extravasation compared to SE-saline and to baseline in
amygdala, piriform and entorhinal cortex at all investigated section levels and in
thalamus vs baseline at section level -3.72 mm relative to bregma.
Conclusions: Gd-DTPA-enhanced MRI is sensitive to detect BBB leakage 48 h, 4 d
and 10 d after SE which could not be counteracted by two potentially BBB-protective
treatments. Furthermore, our data suggest that that losartan may exacerbate BBB
leakage and that losartan and dexamethasone can exacerbate SE-associated
cerebral edema at the chosen dosing regimen in specific brain regions in the
pilocarpine post SE rat model.
Key words: epilepsy, MRI, losartan, dexamethasone
3.2 Introduction
Status epilepticus (SE) and other brain insults can result in structural and functional
brain alterations associated with an increased risk of developing epilepsy (Herman,
2002; van Vliet et al., 2007b; Friedman et al., 2009; Pitkänen & Lukasiuk, 2009;
Löscher & Brandt, 2010). Since not all individuals develop epilepsy after brain insults
(Sloviter & Bumanglag, 2013), there is an urgent need for diagnostically detectable
biomarkers for epileptogenesis as a prerequisite to identify patients at risk as early as
possible in epileptogenesis. Recent findings strongly suggest that blood-brain barrier
(BBB) leakage as well as inflammation may contribute to both initiation and

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
33
progression of epileptogenesis (Janigro, 1999; Oby & Janigro, 2006; Friedman &
Heinemann, 2010; Ndode-Ekane et al., 2010; Friedman, 2011; Marchi et al., 2011b).
Therefore, early detection of BBB leakage by magnetic resonance imaging (MRI)
may be a suitable biomarker for epileptogenesis. Moreover, imaging biomarkers can
be used to evaluate effects and efficacy of potentially antiepileptogenic treatments in
the latency period after an epileptogenesis-triggering brain insult. Starting from the
assumption that increased BBB permeability plays a causative role in
epileptogenesis, pharmacotherapeutic approaches to restore or to maintain BBB
integrity are promising antiepileptogenic strategies (Friedman et al., 2009; Friedman
& Heinemann, 2010). In the presence of a leaky BBB, blood serum constituents
extravasate into the brain parenchyma, resulting in transforming growth factor ß
receptor II (TGF-ß)-mediated impaired astrocyte function, inflammatory signalling
responses and altered potassium distribution (Janigro et al., 1997; Heinemann et al.,
2000; Seiffert et al., 2004; Ivens et al., 2007; van Vliet et al., 2007b; Cacheaux et al.,
2009; David et al., 2009; Friedman et al., 2009; Duffy et al., 2014). It was reported by
Bar-Klein et al. (2014) that the angiotensin II type 1 receptor antagonist losartan
blocks albumin-induced TGF-ß activation in the brain and prevents delayed recurrent
seizures in a rat model of vascular injury-initiated epileptogenesis. In a recent study,
intracerebroventricular administration of losartan preceding pilocarpine-induced SE in
rats was found to inhibit SE-induced cognitive impairment and microglia-mediated
inflammation (Sun et al., 2015).
Another approach which may positively affect the recovery of BBB integrity is
treatment with glucocorticoids. Glucocorticoids exert BBB stabilizing effects and can
alleviate edema formation in specific neoplastic and inflammatory diseases of the
central nervous system (CNS, Friedman & Heinemann, 2010). Bertorelli et al. (1998)
showed that dexamethasone administration following cerebral ischemia appears to
reduce infarct volume in rats.
In the present study a non-invasive, potentially theranostic imaging marker for BBB
leakage was assessed longitudinally during early epileptogenesis. Furthermore,
gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA)-enhanced MRI was used
to evaluate whether two potentially BBB-protective compounds, losartan and

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
34
dexamethasone, can preserve BBB integrity and alleviate vascular edema during
early epileptogenesis in the pilocarpine post SE rat model.
3.3 Materials and Methods
3.3.1 Animals
All animal procedures were approved by the institutional animal care and use
committee and performed in accordance with German research regulations. Female
Sprague-Dawley rats (230-270 g, n = 27, Harlan Laboratories, Udine, Italy) were
housed in individually ventilated cages under controlled climate conditions (22±1°C,
humidity 45-55 %) and a 10/14 h dark light cycle. Food (Altromin 1324; Altromin
Spezialfutter GmbH, Lage, Germany) and autoclaved water were accessible ad
libitum. Animals were allowed to adapt to the new environment for a minimum of one
week and were handled daily before study initiation.
3.3.2 Status epilepticus
As epileptogenic brain insult, a SE was induced by fractionated pilocarpine injection.
The animals were pre-treated with lithium chloride (p.o., 127 mg/kg in 3 ml/kg 0.9 %
saline) 12-14 h and methyl-scopolamine (i.p., 1 mg/kg in 2 ml/kg 0.9 % saline) 30 min
before pilocarpine injection. Pilocarpine was injected every 30 min (bolus 30 mg/kg in
1 ml/kg, subsequently 10 mg/kg i.p.) till SE onset and limited to a maximum of three
injections per rat. Seizure onset and activity were monitored until rats developed
repetitive generalized stage 4 or 5 seizures according to Racine’s scale (Racine,
1975), which marked SE onset. This method was previously described (Glien et al.,
2001; Curia et al., 2008). Using the aforementioned protocol, all rats developed SE.
Ninety min after onset of SE, rats received two diazepam injections (10 mg/kg in
2 ml/kg i.p.) at intervals of 15-20 min to terminate seizure activity. If needed, a third
dose (5 mg/kg i.p.) was injected. Standard feed mash was fed by hand three times
daily over the first 4 d after SE. Fluid balance was stabilized with subcutaneous (s.c.)
saline and electrolyte injections (NaCl 0.9 % B. Braun and Sterofundin/G5, B. Braun

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
35
Melsungen, Germany; 5 ml s.c. each daily). This regimen was continued until
animals showed normal feed and water intake again at about 4 d after SE.
3.3.3 Chemicals and drugs
Unless otherwise stated, the chemicals used in this study (lithium-chloride, methyl-
scopolamine, pilocarpine, bovine albumin-fluorescein isothiocyanate conjugate
[FITC-albumin] and chloral hydrate) were obtained from Sigma-Aldrich Co. LLC
(Schnelldorf, Germany). Isoflurane (Isofluran Baxter) was purchased at Baxter Inc.
(Unterschleißheim, Germany) and diazepam (Diazepam-ratiopharm) from
Ratiopharm GmbH (Ulm, Germany). Gd-DTPA (Magnevist) was obtained from Bayer
HealthCare (Leverkusen, Germany), dexamethasone (Dexamethasone inject
JENAPHARM, 8 mg/2 ml) from Jena Pharm (Jena, Germany), losartan from Santa
Cruz Biotechnology, Inc. (Dallas, Texas, USA) and Sterofundin from B. Braun
Melsungen AG (Melsungen, Germany). Pilocarpine and chloral hydrate were diluted
in 0.9 % saline (B. Braun Melsungen AG). Losartan was dissolved in aqua ad
injectionem and FITC-albumin was dissolved in 0.1 M phosphate buffered saline
(PBS) prior to each administration.
3.3.4 Study design
Rats were randomly assigned to one of the following three groups: Saline treatment
after status epilepticus (SE-saline, n = 5-6), dexamethasone treatment after status
epilepticus (SE-dexamethasone, n = 6), Status epilepticus without treatment
(SE, n = 5) and losartan treatment after status epilepticus (SE-losartan, n = 5).
Animal numbers before SE are higher because baseline scans were performed on
naive animals (SE-saline and SE-losartan, n = 13; SE-dexamethasone and SE,
n = 11). For longitudinal in vivo assessment of BBB leakage during early
epileptogenesis, animals of the vehicle group (SE-saline) were scanned before and
at 5 h, 48 h, 4 d and 10 d after SE. SE-dexamethasone, SE and SE-losartan groups
were scanned baseline and 48 h after SE and additionally at 5 h and 10 d after SE in
the SE-losartan group.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
36
3.3.5 Longitudinal in vivo assessment of blood-brain barrier leakage
Firstly, the time course of BBB leakage after SE was assessed using longitudinal 7 T
MRI at baseline (n = 11-13) and during early epileptogenesis at 5 h (n = 5), 48 h
(n = 5), 4 d (n = 6) and 10 d (n = 5) post SE in SE-saline rats. Less animals than at
baseline were used for subsequent scans. Saline treatment was started 30 min after
the first diazepam injection. Rats received 0.9 % saline in a volume of 1 ml/kg i.p.
twice daily at intervals of 12-14 h for the subsequent 5 d. This dosing regimen was
chosen to match injection times and volumes of the losartan-treated group.
3.3.6 Dexamethasone treatment
Results of MRI examinations following SE were compared to extravasation patterns
and edema formation in the SE-dexamethasone group as measured by 7 T MRI at
48 h post SE. This time point was chosen based on previous work from our group
(see chapter 2) which revealed prominent BBB leakage at 48 h post SE. Rats
received 8 mg/kg dexamethasone i.p. 3 h after the first diazepam injection, followed
by two dexamethasone injections at a dose of 4 mg/kg at 24 h and 48 h after SE.
Dexamethasone was administered 1.5 h before the MRI scan 48 h after SE. Dose
selection and dosing intervals were chosen based on personal communication with
C. Stegmayr and K.J. Langen (Research Center Jülich, Institute of Neuroscience and
Medicine, Jülich, Germany and Department of Nuclear Medicine and Neurology,
University of Aachen, Aachen, Germany), who detected a reduction of tumor-
associated BBB leakage at the used dose in a glioma rat model as assessed by
Evans blue extravasation.
3.3.7 Losartan treatment
Losartan is a clinically approved angiotensin II-receptor (type AT1)-antagonist which
selectively blocks the AT1-receptor and thereby the TGF-ß signal cascade (Bar‐Klein
et al., 2014). To evaluate the efficacy of losartan in protecting BBB integrity during
early epileptogenesis, five rats were treated with a bolus of 50 mg/kg losartan in a
volume of 1 ml/kg aqua ad injectionem i.p. 30 min after SE termination.
Subsequently, losartan was administered at a dose of 5 mg/kg i.p. twice daily from
24 h till 5 d post SE, followed by 9 d of oral administration (2 g/l in drinking water,

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
37
diluted freshly every day) from day 6 till 14 post SE. Losartan doses were chosen
based on a previous study (Bar‐Klein et al., 2014) in which systemic losartan
treatment in a rat model of vascular injury has shown anti-epileptogenic effects.
Animal weights and water intake were measured daily to calculate the individual
losartan uptake (80.4±38.1 mg/d, mean±standard error of the mean [SEM]).
3.3.8 Assessment of blood-brain barrier integrity
Small animal MRI setup included a T2 (multi slice multi echo) MSME sequence,
followed by intravenous (i.v.) infusion of Gd-DTPA and post-contrast T1 modified
driven equilibrium fourier transformation (MDEFT). For contrast agent (CA) infusion,
a catheter was fixed in a lateral tail vein and connected to a syringe pump (model
PHD Ultra; Harvard Apparatus Inc.). A 20 min step down infusion schedule was used
to infuse 1.78 ml of Gd-DTPA (0.5 mmol/ml) in order to quickly achieve and obtain a
plateau level of CA in the blood (Nagaraja et al., 2007; Knight et al., 2009; van Vliet
et al., 2014b, see Table 2 and chapter 2). All MRI scans were performed on a 7 T
(300 MHz) small animal MR system (Bruker BioSpin MRI GmbH) with a 16-cm
horizontal bore (Bruker BioSpec 70/16) under isoflurane anesthesia (3 % in air/O2
[2:1] for induction of anesthesia, 1-2.5 % in air/O2 [2:1] for maintenance of
anesthesia) with continuous control of body temperature and respiration. The system
was controlled by a Bruker BioSpec console (ParaVision 5.1) equipped with a 9 cm
inner diameter gradient insert (Bruker BGA-9S) and a 38-mm circular polarized rat
head volume coil with a rat brain receive-only coil array 11483V3 in combination with
a quadrature MRI transmit-only coil with active decoupling T11070. To ensure
identical positioning of rat and coil within the magnet bore between separate
measurements, the receive coil was placed at a fixed position on the animal bed with
the rat head fixed with an incisor bar. For registration purposes, a TRIPILOT scan
was acquired. Subsequently, regions subjected to brain edema were located using a
T2 weighted MSME sequence [Repetition Time (TR) = 2500 ms, Echo Time
(TE) = 11 ms]. The geometric parameters of the 2D scan were: 96 slices of 0.8 mm,
matrix 256 x 256 and field of view [FOV] 35 x 35 x 25.6 mm, resulting in a voxel size
of 0.136 x 0.136 mm. To evaluate time-dependant changes in T1 intensity during CA
infusion, dynamic short T1 weighted rapid acquisition refocusing (RARE) sequences

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
38
were obtained simultaneously (TR = 1500 ms, TE = 9 ms, 16 slices of 0.8 mm, slice
gap 1 mm, matrix 256 x 256 and FOV 35 x 35 x 25 resulting in a voxel size of
0.136 x 0.136). The sequence was repeated eleven times in a total of 30 min and
additionally after 50 min. Brain regions of interest were assessed by MDEFT method
with MDEFT preparation 30 min after CA infusion. The following geometric
parameters were chosen for the high resolution 3D scans: matrix 256 x 256 x 32 and
FOV 35 x 35 x 25.6 mm, resulting in a voxel size of 0.136 x 0.136 x 0.8 mm. A slice
thickness of 0.8 mm was selected to obtain detailed information of anatomical
structures.
Table 2: Gd-DTPA infusion protocol rats
Duration (min) Rate (ml/min) Volume (ml)
0.5 0.340 0.17
0.5 0.265 0.13
1.0 0.195 0.20
1.0 0.140 0.14
1.0 0.110 0.11
1.0 0.095 0.10
2.0 0.085 0.17
3.0 0.070 0.21
5.0 0.060 0.30
5.0 0.050 0.25
Infusion time = 20 min Total volume = 1.78 ml
3.3.9 Image analysis
For data evaluation, the image sets obtained at baseline and 5 h, 48 h, 4 d and 10 d
after SE were reconstructed in transaxial, coronal and sagittal images and displayed
using PMOD 3.5 software. The PMOD fusion tool was used to co-register T1 and
T2 weighted MR images to a rat brain atlas (Schwarz et al., 2006). T1 and T2 signals
were calculated and normalized to pons as a reference region. A total of eight brain
regions was analyzed: hippocampus, piriform cortex, entorhinal cortex, frontal cortex,
amygdala, thalamus, substantia nigra and cerebellum. Gd-leakage maps were

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
39
calculated using MATLAB software (MathWorks, Natick, Massachusetts, USA) and
SPM12 (UCL, London, UK).
3.3.10 Histological analysis of albumin extravasation
To complement the imaging results, histology as the gold-standard for detecting BBB
leakage was performed in SE-saline and SE-dexamethasone groups. Control rats
(n = 7) were used from a previous study (see chapter 2). After MR imaging (48 ± 6 h
post SE), bovine albumin-fluoresceinisothiocyanate conjugate (FITC-albumin) was
infused i.v. (100 mg/kg in 10 ml/kg, diluted in 0.1 M phosphate buffered saline [PBS];
infusion rate 1 ml/min) under isoflurane anesthesia. Two hours after FITC-albumin
application, rats were perfused through the left ventricle in a deep anesthetic state.
The vascular system was flushed at a speed of 16.6 ml/min with 125 ml 0.01 M PBS,
followed by fixative (250 ml 4 % paraformaldehyde) using a tubing pump (Ismatec
Reglo, Cole-Parmer, Wertheim, Germany). The brains were removed one hour after
perfusion and post fixed in 4 % paraformaldehyde for 24 h before being transferred to
and stored in 30 % sucrose in 0.1 M PBS with 0.2 % sodium azide at 4 °C. Coronal
sectioning (30 µm slice thickness) was performed using a freezing microtome
(Frigomobil 1205; Jung, Heidelberg, Germany). Brain sections were transferred into
0.1 M Tris-buffered saline (TBS, pH 7.4) containing 0.2 % sodium azide. For
conversion into a nickel-enhanced diaminobenzidine (DAB-Ni) reaction product
(Michalski et al., 2010), series of brain sections were rinsed with TBS and washed
with distilled water. The sections were subsequently exposed to 0.6 % H2O2 for 30
min to abolish endogenous peroxidase activity, extensively rinsed with TBS and
blocked with TBS containing 2 % bovine serum albumin and 0.3 % Triton X-100
(TBS-BSA-T) for 1 h. Afterwards, brain sections were incubated with peroxidase-
conjugated anti-FITC IgG (1:2000 in TBS-BSA-T; Dianova, Hamburg, Germany) for
16 h and stained with the chromogen DAB-Ni as previously described (Härtig et al.,
1995). Images of whole brain sections were acquired using a light microscope
(Keyence, Neu-Isenburg, Germany) and stained areas were calculated by the total
number of pixels in the stained area relative to the total area of the respective brain
section.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
40
3.3.11 Statistical analysis
Differences in CA leakage and T2 intensities were compared by one-way analysis of
variance (ANOVA) with Dunnett’s post hoc test for individual differences.
Comparisons of two groups were performed using Bonferroni's multiple comparison
post hoc tests. GraphPad Prism 5 software (GraphPad Software Inc., La Jolla, CA,
USA) was used for statistical analysis and a p-value < 0.05 was considered
statistically significant. For MRI leakage maps, differences between baseline and
48 h post SE were calculated for SE-saline, SE-dexamethasone and SE-losartan
groups using a two-sample unpaired t-test, a significance level threshold of 0.001,
and a minimum cluster size of 100 voxels. All results are presented as mean
± standard error of the mean (SEM).
3.4 Results
3.4.1 Status epilepticus
All rats exhibited stage five seizures according to the Racine scale (Racine, 1975)
and subsequently developed SE. The latency to SE onset was not different between
the three study groups (44 ± 6 min SE-saline, 27 ± 4 min SE-dexamethasone, and
38 ± 4 min SE-losartan). Survival rate after SE was 97.3 %. All rats survived
treatment with dexamethasone or losartan, one rat (belonging to the SE-saline
group) died 12 h after SE. However, adverse effects in forms of gastric ulcers and
tympany were observed in one of the SE-dexamethasone rats during perfusion 48 h
post SE. Body weights significantly decreased after SE in all groups (SE-saline
group at day 1 and day 2, p < 0.05; SE-losartan group at day 3 and day 4, p < 0.05;
SE-dexamethasone group at day 2, p < 0.001) but returned to baseline levels in
SE-saline and SE-losartan groups at about 10 d post SE (see figure 6).

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
41
Figure 6: Weight development
Weight development in saline-treated animals post status epilepticus (SE-saline, n = 3-14), SE-dexamethasone (n = 5-6) and SE-losartan (n = 3-5) groups (mean ± SEM, one-way ANOVA, Dunnett’s post-hoc test vs. day 0, i.e. before SE induction, *p < 0.05).
3.4.2 Longitudinal in vivo assessment of blood-brain barrier leakage in saline-
treated group
To investigate the time course of BBB impairment during early epileptogenesis in the
lithium-pilocarpine post SE rat model, SE-saline animals were scanned longitudinally
at five time points during epileptogenesis: at baseline and at 5 h, 48 h, 4 d and 10 d
post SE. To improve the sensitivity for detection of BBB leakage we used the
previously adjusted step-down infusion protocol for Gd-DTPA (Nagaraja et al., 2007,
see chapter 2).
3.4.2.1 Development of T1 intensity during early epileptogenesis
Gd-DTPA leakage, resulting in elevated T1 values and being indicative of BBB
impairment, was absent at baseline and at 5 h post SE (see figure 7 A and figure 8,
only selected brain regions are shown). Significantly increased T1 values vs.
baseline were present in both limbic and cortical brain structures 48 h post SE. The
maximum permeability increase occurred in the amygdala with a mean T1 intensity
increase of 221 % (p < 0.001). Moreover, significantly increased T1 intensities were
detected in the dorsal hippocampus as well as in thalamus, entorhinal cortex, piriform
cortex, substantia nigra (p < 0.001 for all brain regions) and frontal cortex (p < 0.05).
0 1 2 3 4 5 6 7 8 9 10100
150
200
250
300
350 SE-saline
SE-dexamethasoneSE-losartan
**
**
*
Days post SE
Weig
ht
(g)

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
42
Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d0
1
2
3
4
5
* * *
Amygdala Frontal Cortex Substantia nigraPiriform cortex
B 5h 48h 10d4d 10d4d B 5h 48h 10d4d B 5h 48h 10d4d
*
B 5h 48h 10d4d B 5h 48h 10d4d B 5h 48h 10d4d B 5h 48h 10d4d
*
T1
in
ten
sit
y [
reg
ion
/po
ns
]
* * *
At 4 d post SE, Gd-DTPA leakage was present in the amygdala and in the piriform
cortex, proposing a partial recovery of BBB integrity in the other formerly affected
brain regions. The time point 10 d post SE was characterized by BBB leakage
occurring solely in cortical subregions (entorhinal cortex and piriform cortex). Visual
observation of dynamic T1 rapid acquisition refocusing (RARE) magnetic resonance
images before and after contrast agent infusion during epileptogenesis showed
similar results (see figure 8) but was not quantified.
A
Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d0
1
2
3
4
5
**
*
BaselineSE-saline
Hippocampus Entorhinal Cortex CerebellumThalamus
*
B 5h 48h 10d4d B 5h 48h 10d4d B 5h 48h 10d4d B 5h 48h 10d4dT1
in
ten
sit
y [
reg
ion
/po
ns
]

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
43
Figure 7: Quantification of changes in T1 and T2 intensities during epileptogenesis
(A) T1 intensities as surrogate marker for blood-brain barrier (BBB) leakage measured pre (n = 13), 5 h (n = 5), 48 h (n = 5), 4 d (n = 6) and 10 d (n = 5) post status epilepticus (SE). Exemplary brain regions after step-down infusion of gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA). At 48 h post SE, significantly increased T1 values vs. baseline are present in all investigated brain regions. The greatest permeability increase occurs in the amygdala at 48 h. Moreover, T1 values are significantly increased at 4d (amygdala and piriform cortex) and 10 d post SE (entorhinal and piriform cortex). (B) T2 values, indicative of brain edema, measured pre (n = 13), 5 h (n = 4), 48 h (n = 5), 4d (n = 6 ) and 10 d (n = 5) post SE. T2 values are increased at 48 h and 4 d in hippocampus, thalamus and entorhinal cortex (all regions p < 0.001), at 48 h post SE in amygdala, piriform cortex and cerebellum and at 4 d after SE in substantia nigra. Mean ± SEM, one-way ANOVA, Dunnett’s post-hoc test vs. B, *p < 0.05. B = baseline).
3.4.2.2 Development of T2 intensity during early epileptogenesis
At 48 h, T2 values, indicative of brain edema, were significantly increased in seven
examined brain regions: the anterodorsal hippocampus, thalamus, entorhinal cortex,
cerebellum, amygdala and piriform cortex (all regions p < 0.001, see figure 7 B and
figure 8). At 4 h post SE, T2 values were still increased in hippocampus, thalamus
and entorhinal cortex as well as in substantia nigra. Subsequently, values decreased.
No increased T2 values were present 10 d after SE.
B
B 5h 48h 4d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d0
1
2
3
4
5
*
Amygdala Frontal Cortex Substantia NigraPiriform Cortex
B 5h 48h 10d4d B 5h 48h 10d4d B 5h 48h 10d4dB 5h 48h 10d4d
*
B 48h 4d 10d5h B 48h 4d 10d5h B 48h 4d 10d5h
* *
T2
in
ten
sit
y [
reg
ion
/po
ns
]
B 5h 48h 4d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d Baseline5h post SE48 h 4 d 10d0
1
2
3
4
5
** *
Hippocampus Entorhinal Cortex CerebellumThalamus
B 5h 48h 10d4d B 5h 48h 10d4d B 5h 48h 10d4d
*
B 5h 48h 10d4d
**
B 48h 4d 10d5h B 48h 4d 10d5h B 48h 4d 10d5h
*
T2
in
ten
sit
y [
reg
ion
/po
ns
]

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
44
Figure 8: Longitudinal magnetic resonance imaging during epileptogenesis
Coronal T2 (left); high-resolution T1 modified driven equilibirum fourier transformation (MDEFT, center left) after contrast agent infusion and dynamic T1 rapid acquisition refocusing (RARE) magnetic resonance images before (center right) and after contrast agent infusion (right) during epileptogenesis. Changes are represented as bright enhancement in brain regions affected by blood-brain barrier leakage or cerebral edema. B = baseline.
3.4.3 Pharmacotherapy with potentially blood-brain barrier protective drugs
The results of the longitudinal examinations were subsequently compared to
extravasation patterns and edema formation in SE-dexamethasone and SE-losartan
groups.
B
5 h
48 h
4 d
10 d
T2 MSME T1 MDEFT T1 RARE pre CA T1 RARE post CA
0 166

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
45
Figure 9: Comparative T2, T1 and leakage map images following saline, dexamethasone and
losartan treatment
(A) Coronal T2 weighted MR images, (B) gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA)-enhanced T1 MR images, and (C) SPM leakage maps indicate edema formation and blood-brain barrier leakage 48 h post status epilepticus (SE) in SE-saline as well as in SE-dexamethasone and in SE-losartan groups. (A) Edematous brain tissue and (B) blood-brain barrier leakage are represented as bright enhancement in hippocampus, thalamus, amygdala, entorhinal and piriform cortex. (D) T-maps resulting from comparisons of Gd-DTPA extravasation between baseline and 48 h post SE (n = 5) confirm the results (unpaired t-test, p < 0.001, minimum cluster size of 100 voxels).
3.4.3.1 Effects of dexamethasone on blood-brain barrier integrity
Dexamethasone treatment failed to attenuate or reverse BBB leakage and edema
formation during early epileptogenesis (see figure 9 and figure 10). The extent of
BBB leakage in SE-dexamethasone rats was comparable to SE rats. T1 intensities
were significantly increased at 48 h in the hippocampus, thalamus, entorhinal cortex,
amygdala, piriform cortex, frontal cortex and substantia nigra of both groups.
Saline

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
46
Figure 10: Quantification of BBB leakage and brain edema after dexamethasone treatment
Dexamethasone treatment does not attenuate blood-brain barrier (BBB) leakage and edema formation during early epileptogenesis. Mean (A) T1 intensities as surrogate marker for BBB leakage measured pre (n = 11) and 48 h following status epilepticus (SE) in dexamethasone (SE-dexamethasone, n = 6) and status epilepticus (SE, n = 5) groups. T1 intensities are increased at 48 h in hippocampus, thalamus, entorhinal cortex, amygdala, piriform cortex, frontal cortex and substantia nigra of both groups. (B) T2 intensities. T2 values are significantly increased at 48 h in SE-dexamethasone vs. SE groups in the piriform cortex and vs. baseline in most investigated brain regions (Mean ± SEM, one-way ANOVA and Bonferroni’s post test, *p < 0.05, significance vs. baseline. #p < 0.05 SE-dexamethasone vs. SE. B = baseline).
B
A
B 48 48 dex B 48 48 dex B 48 48 dex B 48 48 dex0
1
2
3
4 CerebellumHippocampusanterodorsal
Thalamus
*
B 48h B 48h B 48h B 48h
SESE-dexamethasone
Baseline
Entorhinal cortex
*
B 48h B 48h B 48h B 48h
T2 in
ten
sit
y [
reg
ion
/po
ns]
B 48 48 Dexa B 48 48 Dexa B 48 48 Dexa B 48 48 Dexa0
1
2
3
4 Substantia nigraAmygdala Piriform Cortex
**
B 48h B 48h B 48h B 48h
Frontal Cortex
B 48h B 48h B 48h B 48h
#
T2
in
ten
sit
y [
reg
ion
/po
ns
]
B 48 48 dex B 48 48 dex B 48 48 dex B 48 48 dex0
2
4
6 CerebellumHippocampus
anterodorsalThalamus
**
**
B 48h B 48h B 48h B 48h
SESE-dexamethasone
Baseline
Entorhinal cortex
**
B 48h B 48h B 48h B 48h
*
T1 i
nte
nsit
y [
reg
ion
/po
ns]
B 48 48 Dexa B 48 48 Dexa B 48 48 Dexa B 48 48 Dexa0
2
4
6 Substantia nigraAmygdala Piriform Cortex
**
*
B 48h B 48h B 48h B 48h
Frontal Cortex
**
B 48h B 48h B 48h B 48h
*
*
* *
T1 in
ten
sit
y [
reg
ion
/po
ns]

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
47
T2 values were significantly increased in SE-dexamethasone vs. SE animals in the
piriform cortex 48 h after SE. Moreover, T2 values were significantly increased only
in SE-dexamethasone animals at 48 h in thalamus, entorhinal cortex, amygdala,
piriform cortex and substantia nigra (see figure 10 B). The mean T2 increase in the
anterodorsal hippocampus at 48 h was 37 % vs. 19 % for SE-dexamethasone and
SE groups, respectively; 38 % vs. 18 % in thalamus, 54 % vs. 23 % in the entorhinal
cortex, 59 % vs. 13 % in the piriform cortex, 52 % vs. 15 % in the amygdala and
23 % vs. 11 % in substantia nigra. Edema formation and SPM mapping are displayed
in figure 9.
3.4.3.2 Effects of losartan on blood-brain barrier integrity
Furthermore, we aimed to elucidate whether treatment with losartan, a clinically
approved angiotensin II receptor (type AT1) antagonist, preserves BBB integrity and
reduces brain edema formation following SE. We found that the CA distribution in
terms of affected brain regions as detected by high-resolution T1 MDEFT at 48 h
after SE did not differ between SE-losartan and SE-saline groups. Hippocampus,
thalamus, entorhinal cortex, amygdala, piriform cortex, substantia nigra (all regions
p < 0.001) and frontal cortex (p < 0.05) exhibited significant increases in T1 intensity
vs. baseline (see figure 11 A). At 10 d post SE increased T1 values vs. baseline were
only present in SE-losartan animals (entorhinal cortex and piriform cortex). Contrast
agent extravasation into affected brain regions and Gd-DTPA leakage maps
confirming these results are shown in figure 9.
A
Baseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d LosartanBaseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d LosartanBaseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d Losartan0
1
2
3
4
5
T1
in
ten
sit
y [
reg
ion
/po
ns
] Hippocampus Entorhinal Cortex Cerebellum
* *
* * SE-saline
Thalamus
Baseline
* * SE-losartan
*
B 5h 48h 10d B 48h 10d B 48h 10d B 48h 10d5h 5h 5h

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
48
Figure 11: Quantification of blood-brain barrier leakage and edema after losartan treatment
T1 and T2 intensities before (n = 13), 5 h (n = 4 - 5), 48 h (n = 5) and 10 d (n = 5) post status epilepticus (SE) and losartan (SE-losartan) or saline treatment (SE-saline) in different brain regions during epileptogenesis. (A) Shows T1 intensities as surrogate marker for blood-brain barrier (BBB) leakage, exemplified for different brain regions after step-down gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA) infusion. T1 intensities are significantly increased vs. baseline in the same brain regions of both groups. However, brain uptake of Gd-DTPA vs. baseline is increased only in SE-losartan animals at 10 d after SE (entorhinal and piriform cortex). (B) T2 values are significantly higher in SE-losartan vs. SE-saline groups at 48 h in substantia nigra. Increased T2 values vs. baseline are present only in SE-losartan rats at 48 h in hippocampus, thalamus and substantia nigra and at 10 d in the entorhinal cortex. Mean ± SEM, one-way ANOVA, Bonferroni's post hoc test. * p < 0.05, significance SE-losartan or SE-saline vs. baseline, # significance SE-losartan vs. SE-saline. B = baseline.
B
0
1
2
3
4
T2
in
ten
sit
y [
reg
ion
/po
ns
]
B 5h 48h 10d
Amygdala Frontal Cortex Substantia NigraPiriform Cortex
*
B 5h 10d48h B 5h 48h 10d B 5h 48h 10d
* *** *__#
0
1
2
3
4
T2
in
ten
sit
y [
reg
ion
/po
ns
]
B 5h 48h 10d
Hippocampus Entorhinal Cortex CerebellumThalamus
*
B 5h 10d48h B 5h 48h 10d B 5h 48h 10d
**
Baseline
SE-salineSE-losartan*
* *
Baseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d LosartanBaseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d LosartanBaseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d LosartanBaseline5h post SE5 h post SE Losartan48 h48 h Losartan10d10d Losartan0
1
2
3
4
5
T1
in
ten
sit
y [
reg
ion
/po
ns
] Amygdala Frontal Cortex Substantia nigra
*
*
* *
Piriform cortex
* *
*
B 5h 48h 10d B 48h 10d B 48h 10d B 48h 10d5h 5h 5h
* * *
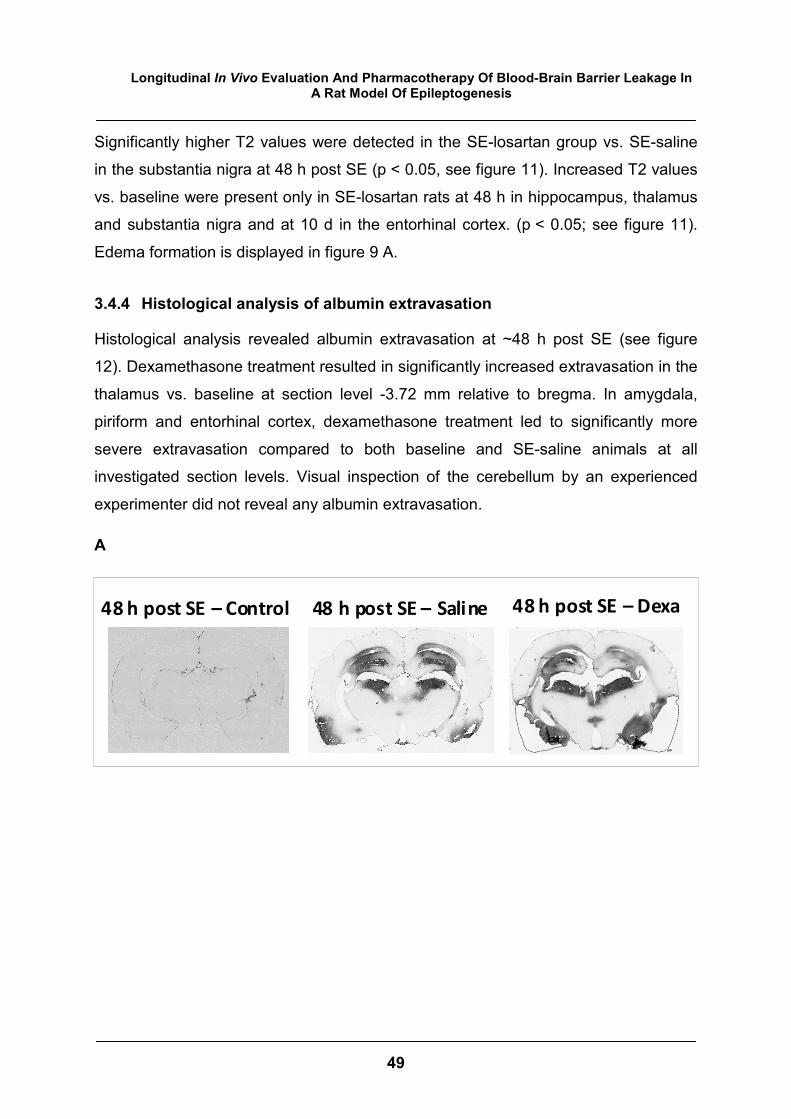
Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
49
48 h post SE – Saline 48 h post SE – Dexa48 h post SE – Control
Significantly higher T2 values were detected in the SE-losartan group vs. SE-saline
in the substantia nigra at 48 h post SE (p < 0.05, see figure 11). Increased T2 values
vs. baseline were present only in SE-losartan rats at 48 h in hippocampus, thalamus
and substantia nigra and at 10 d in the entorhinal cortex. (p < 0.05; see figure 11).
Edema formation is displayed in figure 9 A.
3.4.4 Histological analysis of albumin extravasation
Histological analysis revealed albumin extravasation at ~48 h post SE (see figure
12). Dexamethasone treatment resulted in significantly increased extravasation in the
thalamus vs. baseline at section level -3.72 mm relative to bregma. In amygdala,
piriform and entorhinal cortex, dexamethasone treatment led to significantly more
severe extravasation compared to both baseline and SE-saline animals at all
investigated section levels. Visual inspection of the cerebellum by an experienced
experimenter did not reveal any albumin extravasation.
A

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
50
B
Thalamus
0
2
4
6
+0.36 mm -3.72 mm-1.56 mm
SE-dexamethasone
Control
SE-saline
Section level relative to bregma
*
Sta
ined
are
a [
%]
Piriform/entorhinal cortex and amygdala
0
2
4
6
8
10
+0.36 mm -3.72 mm-1.56 mm
Section level relative to bregma
*
**
#
#
#
Sta
ined
are
a [
%]
Figure 12: Histological evaluation of albumin extravasation
(A) Exemplary brain sections of a control rat, a saline-treated rat 48 h post status epilepticus (SE), and a dexamethasone-treated rat 48 h post SE after conversion of FITC-albumin signal into a light-microscopy reaction product at about -3.72 mm relative to bregma. (B) Quantification of stained area relative to the total section area at +0.36, -1.56 and -3.72 mm relative to bregma. Data is presented as mean ± SEM. Asterisk indicates statistical significance compared to control (n = 4-7), # indicates statistical significance of SE-dexamethasone (n = 6) compared to SE (n = 10) after calculation by one-way ANOVA followed by Bonferroni’s multiple comparison test (p < 0.05).

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
51
3.5 Discussion
The aims of this study were to (i) longitudinally assess BBB leakage following lithium-
pilocarpine-induced SE using 7 T T1 MRI with step-down infusion of Gd-DTPA and to
(ii) investigate BBB integrity stabilizing properties of dexamethasone and losartan.
BBB leakage and edema formation as assessed by 7 T MRI served as surrogate
markers for BBB stabilizing therapeutic effects of dexamethasone and losartan
compared with rats treated with saline or without treatment.
The main findings from this study are:
1) MRI sensitively detects BBB leakage as well as edema formation during
epileptogenesis in the lithium-pilocarpine rat model.
2) BBB leakage and edema following SE are limited to specific brain regions and
subject to changes in temporal occurrence and intensity.
3) Pharmacotherapy with dexamethasone or losartan revealed no BBB protective
effect. On the contrary, we found evidence that losartan treatment may
exacerbate BBB leakage and that both treatments increase edema formation
in certain brain regions after SE.
This study longitudinally detects and quantifies BBB leakage during epileptogenesis
using high-field MRI after step-down infusion of Gd-DTPA. The time course of
T1 intensity increase, indicative of BBB leakage, was found to be different dependent
on brain regions. Quantification and spatial distribution of BBB leakage were highest
48 h after SE, affecting both limbic and cortical brain regions. A previous study using
step-down gadobutrol infusion detected increased T1 intensities 24 h post SE limited
to limbic brain regions and postulated that the motor cortex was not affected (van
Vliet et al., 2014b). In the present study we used 7 T MRI after step-down CA
infusion (Nagaraja et al., 2007; Knight et al., 2009; van Vliet et al., 2014b) to detect
BBB leakage. This approach combines high-field MRI, an imaging protocol with high
spatial resolution (Nagaraja et al., 2007; van Vliet et al., 2014b) and nearly steady-
state CA levels improving contrast enhancement throughout imaging, thus allowing
for sensitive detection of subtle changes of BBB leakage in vivo throughout

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
52
epileptogenesis. Significantly increased T1 values vs. baseline were present in both
limbic and cortical brain structures 48 h post SE with the amygdala being the region
of the highest increase in T1 intensity. By day 4, BBB leakage was still present in the
amygdala and in the piriform cortex, suggesting a partial recovery of BBB integrity in
formerly affected brain regions like hippocampus, entorhinal cortex and thalamus. At
10 d after SE, BBB leakage was detected anew, limited to the entorhinal and piriform
cortex and lower compared to 48 h. Similar results were also found in models of
traumatic brain insults (Shapira et al., 1993; Başkaya et al., 1997). A second opening
of the BBB occurred 3-7 d following traumatic brain injury and was not accompanied
by edema formation, as assessed by quantitative Evans blue measurement (Başkaya
et al., 1997). Van Vliet et al. (2014b) detected BBB leakage in the chronic phase six
weeks following kainate-induced SE in all investigated limbic brain regions in the
systemic kainate rat model. The reappearance of BBB leakage at later time points
may be caused by recurrent seizure activity.
Peak values of T2 intensities were detected 48 h post SE. This finding corresponds
to those of previous pre-clinical studies by Roch et al. (2002), Choy et al. (2010) and
Duffy et al. (2014) who detected peaks of T2 intensity around 48 h following brain
insults. Furthermore, hippocampal edema was shown to occur within 48 h after SE in
human subjects, too (VanLandingham et al., 1998; Scott et al., 2002). Cerebral
edema was limited to hippocampus, thalamus, entorhinal cortex, cerebellum,
amygdala and piriform cortex and had returned to baseline levels in all investigated
brain regions by d 10 in the present study, suggesting cerebral edema to appear
predominantly early after SE and to resolve within 10 d thereafter. These findings are
in accordance with Choy et al. (2010) who used T1 and T2 weighted sequences as
well as apparent diffusion coefficient MR imaging and found changes in MR signals
returning to baseline levels around day 7 post SE.
The second aim of this study was to evaluate effects of dexamethasone and losartan
treatment on BBB integrity following SE. Inflammation in the CNS is correlated to
impaired BBB integrity which again triggers seizures and epileptogenesis (Seiffert et
al., 2004; Ivens et al., 2007; Marchi et al., 2007b; Van Vliet et al., 2007a).
Inflammatory processes following brain insults are complex and were observed

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
53
“inside” in the brain parenchyma and “outside” at endothelial cells of the BBB
(Vezzani & Granata, 2005; Ravizza et al., 2008). Therefore, treatment with broad-
spectrum anti-inflammatory and immunosuppressive drugs like dexamethasone
(McMaster & Ray, 2007) may be beneficial in antiepileptogenic trials.
Dexamethasone acts on the glucocorticoid receptor (Auphan et al., 1995), inducing
target genes and interfering between glucocorticoid receptor and transcription factors
like NF-kappa-B, inhibiting its activity. However, the exact mechanisms of
dexamethasone-effects on BBB integrity are not known (Duffy et al., 2014).
Pilocarpine-induced seizures and SE are accompanied by activation of receptors and
adhesion molecules triggering immunologic reactions (Fabene et al., 2008; Marchi et
al., 2009). Fabene et al. (2008) showed that BBB leakage was prevented by blocking
leucocyte-endothelial adhesion. The same molecules that trigger immunologic
reactions in the lithium-pilocarpine model are target structures of corticosteroids
(Marchi et al., 2011a). Therefore, we hypothesized that dexamethasone treatment
might reveal BBB-stabilizing effects. In the present study, unexpectedly,
dexamethasone and losartan treatment failed to attenuate or reverse BBB leakage
and edema formation at the used treatment regimen during early epileptogenesis in
the pilocarpine post SE rat model.
Previous studies that evaluated effects of dexamethasone on BBB integrity have
reported conflicting findings (Duffy et al., 2014; Holtman et al., 2014). In different
inflammatory and neoplastic conditions of the central nervous system (CNS),
glucocorticoids had BBB stabilizing effects and counteracted edema formation
(Friedman & Heinemann, 2010). In specific pediatric epilepsies, for example the
Landau-Kleffner syndrome, glucocorticoids are used as treatment in clinics (Vezzani
et al., 2011). In drug-resistant pediatric epilepsies, dexamethasone can interrupt SE
and reduce seizure occurrence (Marchi et al., 2011a). However, like in the present
study, dexamethasone treatment was ineffective to harmful in a post-SE rat model as
assessed by Duffy et al. (2014) and also in patients with acute ischemic stroke
(Kleinschnitz et al., 2011). Moreover, Smith-Swintosky et al. (1996) showed that
neuronal loss in hippocampal CA3 and CA1 regions following kainate-induced SE
can be reduced by metyrapone administration which inhibits endogenous
glucocorticoid production.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
54
Interestingly, we found no differences in T1 intensities between SE-dexamethasone
and SE animals 48 h after SE. Both affected brain regions and extent of BBB leakage
after triple dexamethasone treatment were comparable between groups. On the
contrary, T2 values were significantly higher in the SE-dexamethasone group
compared with the SE-group in the piriform cortex, suggesting an exacerbation of
cerebral edema by dexamethasone. Besides, edema was detected in thalamus,
entorhinal cortex and amygdala only in the SE-dexamethasone group. Our findings
are consistent with a study from Duffy et al. (2014) who showed increased T2
alterations 48 h and 4 d after SE even at lower doses of dexamethasone (2 mg/kg)
compared with the present study. Moreover, the authors found that dexamethasone
deteriorates hippocampal injury three weeks following SE. Maintaining a balance
between damaging and rehabilitating processes is important for successful treatment
strategies (Gröhn & Pitkänen, 2007). Brain-protective effects of early inflammation
after brain insults (Serrano et al., 2011) which may be counteracted by
dexamethasone were suggested (Duffy et al., 2014) as a possible reason for the
worsening of edema formation. Moreover, dexamethasone was found to attenuate
cerebral edema in a non-acidotic state whilst aggravated brain edema was detected
after dexamethasone treatment under acidotic conditions in a study on rats following
traumatic brain injury (Tran et al., 2010). Thus, we cannot rule out that acid-base
homeostasis has had an effect on the result of dexamethasone treatment in this
study. Besides, the treatment protocol may have influenced results. The effective
therapeutic time window after brain insults can be narrow in pre-clinical studies
(Herman, 2002), and we tested only one dosing regimen. Thus, different dosing and
application intervals may reveal a different outcome. Characteristics of the lithium-
pilocarpine rat model resemble those of human temporal lobe epilepsy (TLE; Leite et
al., 2002). One example is the presence of a latency phase which is following SE and
preceding the occurrence of spontaneous recurrent seizures as well as structural
reorganization processes. However, there is no model which simulates all relevant
aspects of human TLE. Thus, the used animal model may play a role in the outcome
of BBB protective treatment, too. It can be advisable to study pathophysiological
processes in different animal models. Therefore, we re-investigated effects of

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
55
dexamethasone on BBB integrity using a different animal model and dosing regimen
(see chapter 4).
Losartan acts on angiotensin II type 1 receptors in astrocytes and blocks albumin-
induced TGF-ß activation (Bar‐Klein et al., 2014). Thus we expected that losartan
might prevent a further damaging of BBB integrity by antagonizing TGF-ß mediated
transcriptional changes, impaired astrocyte function, inflammatory signalling
responses and altered potassium equilibrium (Janigro et al., 1997; Heinemann et al.,
2000; Seiffert et al., 2004; Ivens et al., 2007; van Vliet et al., 2007b; Cacheaux et al.,
2009; David et al., 2009; Friedman et al., 2009; Duffy et al., 2014). This is the first
study to investigate BBB integrity following losartan-treatment in the lithium-
pilocarpine rat model during early epileptogenesis. Surprisingly, losartan-treatment
was found to exacerbate brain edema in substantia nigra 2 d after SE and to favor
BBB leakage at 10 d after SE.
Pereira et al. (2010) found that angiotensin II type 1 receptors were upregulated in
the brains of audiogenically induced seizure models. Losartan treatment significantly
decreased frequency and severity of epileptic seizures. In a recent study,
intracerebroventricular administration of losartan before pilocarpine induced SE in
rats was found to inhibit SE-induced cognitive impairment and microglia-mediated
inflammation (Sun et al., 2015). However, the clinical relevance is arguable as
losartan administration preceded the insult, suggesting an insult-modification.
The present study was not designed to determine the mechanism for exacerbation of
edema and BBB leakage after losartan treatment. Angiotensin II type 1 receptors are
implicated in seizure susceptibility in different epilepsy models (Tchekalarova &
Georgiev, 2005; Pereira et al., 2010). In previous studies, losartan-treatment delayed
the onset of chronic seizures in rat models of vascular injury and after kainate-
induced SE (Ivanova et al., 2013; Bar‐Klein et al., 2014; Tchekalarova et al., 2014a).
These studies have in common that they evaluated effects of losartan-treatment in
the chronic epileptic phase. Bar‐Klein et al. (2014) acquired electrocorticography
(ECoG) recordings starting from day 28 after the initial insult and one week after drug
withdrawal.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
56
In the present study, we evaluated changes in BBB-integrity during early
epileptogenesis (until day 10 post SE). Effects of losartan on acute alterations of BBB
integrity after SE have not been investigated before. We cannot rule out that losartan,
despite the lack of BBB protective effects during early epileptogenesis, may have
revealed disease modifying effects if animals had been monitored in the chronic
phase. Such modifications may include the number of animals developing epilepsy,
seizure onset or seizure frequency.
Another factor that might be considered is that albumin uptake into astrocytes seems
to be mediated not only by TGF-ß mediated changes but also by other pathways
including caveolae-mediated albumin-endocytosis (Bar‐Klein et al., 2014), indicating
that losartan might only partially block albumin uptake into astrocytes.
3.6 Conclusion
Longitudinal changes in T1 and T2 values following SE can be detected via high-field
MRI following step-down infusion of Gd-DTPA. Post SE treatment with losartan or
dexamethasone does not reduce vascular edema or BBB leakage during early
epileptogenesis in the lithium-pilocarpine rat model. Rather, both treatments can
exacerbate SE-associated cerebral edema. However, we could not rule out in this
study whether losartan or dexamethasone had epileptogenesis modifying effects.
Thus, more studies are needed to further investigate the antiepileptogenic potential
of dexamethasone and losartan.
ACKNOWLEDGEMENTS: C. Bergen and M. Märkel are gratefully acknowledged for their
technical assistance. This study is funded by the European Union’s Seventh Framework
Programme (FP7) under grant agreement n°602102 (EPITARGET). H.B. was supported by a
scholarship from the Studienstiftung des Deutschen Volkes.
CONFLICTS OF INTEREST: none

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
57
3.7 References
ABBOTT, N.J. & FRIEDMAN, A. (2012). Overview and introduction: The blood-brain barrier in health and disease. Epilepsia 53, 1-6.
AL-SHORBAGY, M.Y., EL SAYEH, B.M. & ABDALLAH, D.M. (2012). Diverse effects of variant doses of
dexamethasone in lithium-pilocarpine induced seizures in rats. Canadian Journal of Physiology and Pharmacology 90, 13-21.
AUPHAN, N., DIDONATO, J.A., ROSETTE, C., HELMBERG, A. & KARIN, M. (1995). Immunosuppression by
glucocorticoids: inhibition of NF-kappaB activity through induction of IkappaB synthesis. Science 270, 286.
BAR‐KLEIN, G., CACHEAUX, L.P., KAMINTSKY, L., PRAGER, O., WEISSBERG, I., SCHOKNECHT, K., CHENG,
P., KIM, S.Y., WOOD, L. & HEINEMANN, U. (2014). Losartan prevents acquired epilepsy via TGF‐β signaling suppression. Annals of Neurology 75, 864-875.
BAiKAYA, M.K., MURALIKRISHNA RAO, A., DOĞAN, A., DONALDSON, D. & DEMPSEY, R.J. (1997). The
biphasic opening of the blood–brain barrier in the cortex and hippocampus after traumatic brain injury in rats. Neuroscience Letters 226, 33-36.
CACHEAUX, L.P., IVENS, S., DAVID, Y., LAKHTER, A.J., BAR-KLEIN, G., SHAPIRA, M., HEINEMANN, U.,
FRIEDMAN, A. & KAUFER, D. (2009). Transcriptome profiling reveals TGF-β signaling involvement in epileptogenesis. The Journal of Neuroscience 29, 8927-8935.
CHOY, M., CHEUNG, K.K., THOMAS, D.L., GADIAN, D.G., LYTHGOE, M.F. & SCOTT, R.C. (2010).
Quantitative MRI predicts status epilepticus-induced hippocampal injury in the lithium-pilocarpine rat model. Epilepsy Research 88, 221-230.
CURIA, G., LONGO, D., BIAGINI, G., JONES, R.S. & AVOLI, M. (2008). The pilocarpine model of temporal
lobe epilepsy. Journal of Neuroscience Methods 172, 143-157.
DAVID, Y., CACHEAUX, L.P., IVENS, S., LAPILOVER, E., HEINEMANN, U., KAUFER, D. & FRIEDMAN, A. (2009).
Astrocytic dysfunction in epileptogenesis: consequence of altered potassium and glutamate homeostasis? The Journal of Neuroscience 29, 10588-10599.
DEDEURWAERDERE, S., JUPP, B. & O'BRIEN, T.J. (2007). Positron emission tomography in basic
epilepsy research: a view of the epileptic brain. Epilepsia 48, 56-64.
DUFFY, B.A., CHUN, K.P., MA, D., LYTHGOE, M.F. & SCOTT, R.C. (2014). Dexamethasone exacerbates
cerebral edema and brain injury following lithium-pilocarpine induced status epilepticus. Neurobiology of Disease 63, 229-236.
FABENE, P.F., MORA, G.N., MARTINELLO, M., ROSSI, B., MERIGO, F., OTTOBONI, L., BACH, S., ANGIARI, S.,
BENATI, D., CHAKIR, A., ZANETTI, L., SCHIO, F., OSCULATI, A., MARZOLA, P., NICOLATO, E., HOMEISTER, J.W., XIA, L., LOWE, J.B., MCEVER, R.P., OSCULATI, F., SBARBATI, A., BUTCHER, E.C. & CONSTANTIN, G. (2008). A role for leukocyte-endothelial adhesion mechanisms in epilepsy. Nature Medicine 14, 1377-1383.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
58
FRIEDMAN, A. (2011). Blood–brain barrier dysfunction, status epilepticus, seizures, and epilepsy: A
puzzle of a chicken and egg? Epilepsia 52, 19-20.
FRIEDMAN, A. & HEINEMANN, U. (2010). Role of blood–brain barrier injury in epileptogenesis. Epilepsia
51, 34-34.
FRIEDMAN, A., KAUFER, D. & HEINEMANN, U. (2009). Blood–brain barrier breakdown-inducing astrocytic
transformation: Novel targets for the prevention of epilepsy. Epilepsy Research 85, 142-149.
GLIEN, M., BRANDT, C., POTSCHKA, H., VOIGT, H., EBERT, U. & LÖSCHER, W. (2001). Repeated low-dose
treatment of rats with pilocarpine: low mortality but high proportion of rats developing epilepsy. Epilepsy Research 46, 111-119.
GRÖHN, O. & PITKÄNEN, A. (2007). Magnetic resonance imaging in animal models of epilepsy-
noninvasive detection of structural alterations. Epilepsia 48, 3-10.
HÄRTIG, W., BRUCKNER, G., HOLZER, M., BRAUER, K. & BIGL, V. (1995). Digoxigenylated primary
antibodies for sensitive dual-peroxidase labelling of neural markers. Histochemistry and Cell Biology 104, 467-472.
HEINEMANN, U., GABRIEL, S., JAUCH, R., SCHULZE, K., KIVI, A., EILERS, A., KOVACS, R. & LEHMANN, T.N.
(2000). Alterations of glial cell function in temporal lobe epilepsy. Epilepsia 41, 185-189.
HERMAN, S.T. (2002). Epilepsy after brain insult Targeting epileptogenesis. Neurology 59, 21-26.
HOLTMAN, L., VAN VLIET, E.A., APPELDOORN, C., GAILLARD, P.J., DE BOER, M., DORLAND, R., WADMAN,
W.J. & GORTER, J.A. (2014). Glutathione pegylated liposomal methylprednisolone administration after the early phase of status epilepticus did not modify epileptogenesis in the rat. Epilepsy Research 108, 396-404.
IVANOVA, N., PECHLIVANOVA, D., TCHEKALAROVA, J., POPOV, D., MARKOVA, P. & STOYNEV, A. (2013).
Beneficial effects of chronic treatment with losartan on behavioural disturbances in kainate model of temporal lobe epilepsy. Comptes rendus de l'Académie bulgare des Sciences 66, 1761-1768.
IVENS, S., KAUFER, D., FLORES, L.P., BECHMANN, I., ZUMSTEG, D., TOMKINS, O., SEIFFERT, E.,
HEINEMANN, U. & FRIEDMAN, A. (2007). TGF-β receptor-mediated albumin uptake into astrocytes is involved in neocortical epileptogenesis. Brain 130, 535-547.
JANIGRO, D. (1999). Blood–brain barrier, ion homeostasis and epilepsy: possible implications towards
the understanding of ketogenic diet mechanisms. Epilepsy Research 37, 223-232.
JANIGRO, D., GASPARINI, S., D’AMBROSIO, R., MCKHANN II, G. & DIFRANCESCO, D. (1997). Reduction of
K+ uptake in glia prevents long-term depression maintenance and causes epileptiform activity. The Journal of Neuroscience 17, 2813-2824.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
59
KLEINSCHNITZ, C., BLECHARZ, K., KAHLES, T., SCHWARZ, T., KRAFT, P., GOBEL, K., MEUTH, S.G., BUREK, M., THUM, T., STOLL, G. & FORSTER, C. (2011). Glucocorticoid insensitivity at the hypoxic blood-brain barrier can be reversed by inhibition of the proteasome. Stroke 42, 1081-1089.
KNIGHT, R.A., KARKI, K., EWING, J.R., DIVINE, G.W., FENSTERMACHER, J.D., PATLAK, C.S. & NAGARAJA,
T.N. (2009). Estimating blood and brain concentrations and blood-to-brain influx by magnetic resonance imaging with step-down infusion of Gd-DTPA in focal transient cerebral ischemia and confirmation by quantitative autoradiography with Gd-[(14)C]DTPA. Journal of Cerebral Blood Flow and Metabolism 29, 1048-1058.
LEITE, J., GARCIA-CAIRASCO, N. & CAVALHEIRO, E. (2002). New insights from the use of pilocarpine and
kainate models. Epilepsy Research 50, 93-103.
LÖSCHER, W. & BRANDT, C. (2010). Prevention or Modification of Epileptogenesis after Brain Insults:
Experimental Approaches and Translational Research. Pharmacological Reviews 62, 668-700.
MARCHI, N., FAN, Q., GHOSH, C., FAZIO, V., BERTOLINI, F., BETTO, G., BATRA, A., CARLTON, E., NAJM, I. &
GRANATA, T. (2009). Antagonism of peripheral inflammation reduces the severity of status epilepticus. Neurobiology of Disease 33, 171-181.
MARCHI, N., GRANATA, T., FRERI, E., CIUSANI, E., RAGONA, F., PUVENNA, V., TENG, Q., ALEXOPOLOUS, A.
& JANIGRO, D. (2011a). Efficacy of Anti-Inflammatory Therapy in a Model of Acute Seizures and in a Population of Pediatric Drug Resistant Epileptics. PLoS ONE 6, e18200.
MARCHI, N., OBY, E., BATRA, A., UVA, L., DE CURTIS, M., HERNANDEZ, N., BOXEL‐DEZAIRE, V., NAJM, I. &
JANIGRO, D. (2007). In vivo and in vitro effects of pilocarpine: relevance to ictogenesis. Epilepsia 48, 1934-1946.
MARCHI, N., TIERNEY, W., ALEXOPOULOS, A.V., PUVENNA, V., GRANATA, T. & JANIGRO, D. (2011b). The
etiological role of blood-brain barrier dysfunction in seizure disorders. Cardiovascular Psychiatry and Neurology 482415, 30.
MCMASTER, A. & RAY, D.W. (2007). Modelling the glucocorticoid receptor and producing therapeutic
agents with anti‐inflammatory effects but reduced side‐effects. Experimental Physiology 92, 299-309.
MICHALSKI, D., GROSCHE, J., PELZ, J., SCHNEIDER, D., WEISE, C., BAUER, U., KACZA, J., GÄRTNER, U.,
HOBOHM, C. & HÄRTIG, W. (2010). A novel quantification of blood-brain barrier damage and histochemical typing after embolic stroke in rats. Brain Research 1359, 186-200.
NAGARAJA, T.N., NAGESH, V., EWING, J.R., WHITTON, P.A., FENSTERMACHER, J.D. & KNIGHT, R.A. (2007).
Step-down infusions of Gd-DTPA yield greater contrast-enhanced magnetic resonance images of BBB damage in acute stroke than bolus injections. Magnetic Resonance Imaging 25, 311-318.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
60
NDODE-EKANE, X.E., HAYWARD, N., GROHN, O. & PITKANEN, A. (2010). Vascular changes in epilepsy: functional consequences and association with network plasticity in pilocarpine-induced experimental epilepsy. Neuroscience 166, 312-332.
OBY, E. & JANIGRO, D. (2006). The Blood–Brain Barrier and Epilepsy. Epilepsia 47, 1761-1774.
PEREIRA, M., BECARI, C., OLIVEIRA, J., SALGADO, M., GARCIA-CAIRASCO, N. & COSTA-NETO, C. (2010).
Inhibition of the renin-angiotensin system prevents seizures in a rat model of epilepsy. Clinical Science 119, 477-482.
PITKÄNEN, A. & LUKASIUK, K. (2009). Molecular and cellular basis of epileptogenesis in symptomatic
epilepsy. Epilepsy & Behavior 14, 16-25.
RACINE, R.J. (1975). Modification of seizure activity by electrical stimulation: cortical areas.
Electroencephalography and Clinical Neurophysiology 38, 1-12.
RAVIZZA, T., NOÉ, F., ZARDONI, D., VAGHI, V., SIFRINGER, M. & VEZZANI, A. (2008). Interleukin converting
enzyme inhibition impairs kindling epileptogenesis in rats by blocking astrocytic IL-1β production. Neurobiology of Disease 31, 327-333.
ROCH, C., LEROY, C., NEHLIG, A. & NAMER, IZZIE J. (2002). Magnetic Resonance Imaging in the Study
of the Lithium-Pilocarpine Model of Temporal Lobe Epilepsy in Adult Rats. Epilepsia 43, 325-335.
SCOTT, R., GADIAN, D., KING, M., CHONG, W., COX, T., NEVILLE, B. & CONNELLY, A. (2002). Magnetic
resonance imaging findings within 5 days of status epilepticus in childhood. Brain 125, 1951-1959.
SEIFFERT, E., DREIER, J.P., IVENS, S., BECHMANN, I., TOMKINS, O., HEINEMANN, U. & FRIEDMAN, A.
(2004). Lasting Blood-Brain Barrier Disruption Induces Epileptic Focus in the Rat Somatosensory Cortex. The Journal of Neuroscience 24, 7829-7836.
SERRANO, G., LELUTIU, N., ROJAS, A., COCHI, S., SHAW, R., MAKINSON, C., WANG, D., FITZGERALD, G. &
DINGLEDINE, R. (2011). Ablation of cyclooxygenase-2 in forebrain neurons is neuroprotective and dampens brain inflammation after status epilepticus. The Journal of Neuroscience 31, 14850-14860.
SHAPIRA, Y., SETTON, D., ARTRU, A.A. & SHOHAMI, E. (1993). Blood-brain barrier permeability, cerebral
edema, and neurologic function after closed head injury in rats. Anesthesia & Analgesia 77, 141-148.
SLIVKA, A.P. & MURPHY, E.J. (2001). High-dose methylprednisolone treatment in experimental focal
cerebral ischemia. Experimental Neurology 167, 166-172.
SLOVITER, R.S. & BUMANGLAG, A.V. (2013). Defining “epileptogenesis” and identifying
“antiepileptogenic targets” in animal models of acquired temporal lobe epilepsy is not as simple as it might seem. Neuropharmacology 69, 3-15.

Longitudinal In Vivo Evaluation And Pharmacotherapy Of Blood-Brain Barrier Leakage In A Rat Model Of Epileptogenesis
61
SMITH-SWINTOSKY, V.L., PETTIGREW, L.C., SAPOLSKY, R.M., PHARES, C., CRADDOCK, S.D., BROOKE,
S.M. & MATTSON, M.P. (1996). Metyrapone, an Inhibitor of Glucocorticoid Production, Reduces Brain Injury Induced by Focal and Global Ischemia and Seizures. Journal of Cerebral Blood Flow & Metabolism 16, 585-598.
SUN, H., WU, H., YU, X., ZHANG, G., ZHANG, R., ZHAN, S., WANG, H., BU, N., MA, X. & LI, Y. (2015).
Angiotensin II and its receptor in activated microglia enhanced neuronal loss and cognitive impairment following pilocarpine-induced status epilepticus. Molecular and Cellular Neuroscience 65, 58-67.
TCHEKALAROVA, J. & GEORGIEV, V. (2005). Angiotensin peptides modulatory system: how is it
implicated in the control of seizure susceptibility? Life Sciences 76, 955-970.
TCHEKALAROVA, J., IVANOVA, N., PECHLIVANOVA, D., ILIEVA, K. & ATANASOVA, M. (2014). Strain-
Dependent Effects of Sub-chronically Infused Losartan Against Kainic Acid-Induced Seizures, Oxidative Stress, and Heat Shock Protein 72 Expression. Cellular and Molecular Neurobiology 34, 133-142.
TRAN, N.D., KIM, S., VINCENT, H.K., RODRIGUEZ, A., HINTON, D.R., BULLOCK, M.R. & YOUNG, H.F.
(2010). Aquaporin-1-mediated cerebral edema following traumatic brain injury: effects of acidosis and corticosteroid administration: Laboratory investigation. Journal of Neurosurgery 112, 1095-1104.
VAN VLIET, E., DA COSTA ARAUJO, S., REDEKER, S., VAN SCHAIK, R., ARONICA, E. & GORTER, J. (2007a).
Blood–brain barrier leakage may lead to progression of temporal lobe epilepsy. Brain 130, 521-534.
VAN VLIET, E.A., DA COSTA ARAÚJO, S., REDEKER, S., VAN SCHAIK, R., ARONICA, E. & GORTER, J.A.
(2007b). Blood–brain barrier leakage may lead to progression of temporal lobe epilepsy. Brain 130, 521-534.
VAN VLIET, E.A., OTTE, W.M., GORTER, J.A., DIJKHUIZEN, R.M. & WADMAN, W.J. (2014). Longitudinal
assessment of blood-brain barrier leakage during epileptogenesis in rats. A quantitative MRI study. Neurobiology of Disease 63, 74-84.
VANLANDINGHAM, K.E., HEINZ, E.R., CAVAZOS, J.E. & LEWIS, D.V. (1998). Magnetic resonance imaging
evidence of hippocampal injury after prolonged focal febrile convulsions. Annals of Neurology 43, 413-426.
VEZZANI, A., FRENCH, J., BARTFAI, T. & BARAM, T.Z. (2011). The role of inflammation in epilepsy. Nature
Reviews Neurology 7, 31-40.
VEZZANI, A. & GRANATA, T. (2005). Brain inflammation in epilepsy: experimental and clinical evidence.
Epilepsia 46, 1724-1743.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
62
4 Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
H. Breuer1,2, M. Meier3, J.P. Bankstahl2, M. Bankstahl1
1 Institute of Pharmacology, Toxicology and Pharmacy, University of Veterinary
Medicine Hannover and Center for Systems Neuroscience, Germany
2 Preclinical Molecular Imaging, Department of Nuclear Medicine, Hannover
Medical School, Germany
3 Preclinical Imaging Labs, Central Laboratory Animal Facility & Institute for
Laboratory Animal Science, Hannover Medical School, Germany
The extent of author’s contributions to this work:
Design of project: J.P.B., M.B.
Design of experiments: H.B., J.P.B., M.B., M.M.
Performance of experiments: H.B., M.B., M.M.
Analysis of experiments: H.B.
Writing and revision of manuscript: H.B., M.B., J.P.B.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
63
4.1 Abstract
Objective: Epileptogenesis can be initiated by primary brain insults and results in
chronic epilepsy, characterized by the occurrence of spontaneous recurrent seizures.
Growing evidence suggests that brain insult-associated blood-brain barrier (BBB)
impairment is a key step in the initiation of epileptogenesis and may contribute to
disease progression. Therefore, BBB-protective treatment might prevent or attenuate
the process of epileptogenesis. In this study, longitudinal in vivo 7 T small animal
magnetic resonance imaging (MRI) was used to detect changes in BBB leakage
during epileptogenesis and to evaluate potentially BBB-protective effects of
dexamethasone treatment.
Materials and methods: As primary brain insult, status epilepticus (SE) was induced
by intrahippocampal injection of kainate in 13 male NMRI mice. Seven sham animals
received intrahippocampal injections of saline. Following SE, mice were treated with
dexamethasone [SE-dex, n = 5; 6, 24, 48, 72 h post SE, 2 mg/kg intraperitoneally
(i.p.)] or vehicle saline (SE-KA, n = 8). Dexamethasone treated mice were scanned
before (baseline), 48 h and 4 d after SE. Vehicle and sham groups were scanned
additionally on d 16 and 37 after SE or sham surgery, respectively. High field 7 T
small animal MRI consisted of a T2 map for anatomical co-localization and a T1
modified driven equilibirum fourier transformation (MDEFT) sequence after step-
down infusion of gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA). Images
were analyzed by co-registration with a standard mouse brain atlas. T1 signal
increase in dorsal and ventral hippocampus, amygdala, thalamus and cortex was
normalized to cerebellum and calculated using PMOD software (PMOD Technologies
Ltd., Zurich, Switzerland).
Results: High field MRI revealed BBB leakage in epilepsy-associated brain regions
during epileptogenesis. In the hippocampus of SE-KA mice, T1 signal after contrast
agent (CA) infusion increased up to 274 % in the ipsilateral hippocampus vs.
baseline 48 h after SE (p < 0.05). The ipsilateral ventral hippocampus as well as
amygdala, thalamus and cortex were subjected to BBB leakage at 2 d and 4 d after
SE. T1 values subsequently decreased during the five weeks of follow-up. Sixteen

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
64
days post SE, T1 values were increased in the ipsilateral dorsal hippocampus and
thalamus. At 37 d post SE, T1 values were increased in hippocampus, thalamus and
cortex but had returned to baseline levels in all other investigated brain regions. In
SE-KA vs. sham animals, significantly increased T1 signals were present 48 h after
SE in dorsal and ventral hippocampus, amygdala and thalamus. Dexamethasone
treatment resulted in significantly reduced BBB leakage in hippocampus and
thalamus. Contrast agent extravasation into the dorsal hippocampus was reduced by
20 % on day 2 (p < 0.05) in the ipsilateral brain hemisphere and by 24 % on day 4 in
the contralateral brain hemisphere in SE-dex vs. SE-KA mice (p < 0.05).
Conclusion: Contrast-enhanced MRI is sensitive to detect BBB leakage in the
intrahippocampal kainate mouse model. Our results show for the first time a
successful reduction of BBB leakage by a dosing regimen of dexamethasone in mice
during epileptogenesis using in vivo MR imaging. A potentially beneficial impact on
chronic seizure development will be tested.
Key words: antiepileptogenesis, epilepsy, imaging, pharmacotherapy
4.2 Introduction
Temporal lobe epilepsy (TLE) is the most common form of epilepsy in adults
(Sloviter, 2005). It is usually induced by a primary brain insult triggering a cascade of
structural and functional changes in the brain, termed epileptogenesis (Herman,
2002; Friedman et al., 2009; Pitkänen & Lukasiuk, 2009; Löscher & Brandt, 2010).
So far, the development of TLE in at-risk patients cannot be predicted or prevented
and no antiepileptogenic therapies have been identified (Sloviter & Bumanglag,
2013). The current antiepileptic medication for chronically epileptic patients is solely
symptomatic in terms of seizure suppression and has no anti-epileptogenic effects.
Small animal models have been comprehensively used to study epileptogenesis,
providing an abundant record of histological data (Jupp et al., 2007). In contrast to
histological methods which are performed post mortem, non-invasive in vivo
magnetic resonance imaging (MRI) enables longitudinal evaluation of changes in
blood-brain barrier (BBB) integrity on an individual basis in the same animal (Hsu et

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
65
al., 2007; Jupp et al., 2007). This provides the opportunity to further examine the
process of epileptogenesis and favours the development of early diagnostic
biomarkers and disease-modifying or anti-epileptogenic therapies. One suitable
model for in vivo imaging of BBB leakage might be the intrahippocampal kainate
mouse model. This model is suitable for the study of epileptogenesis and
antiepileptogenesis, for research on drug resistance and to evaluate antiepileptic
therapies (Stables et al., 2002; Stables et al., 2003). It was used in the present study
because it is characterized by a fast development of spontaneous seizures with high
seizure frequency, allowing for a statement on the effectiveness of potentially BBB-
stabilizing drugs early after the initial status epilepticus (SE). As epileptogenesis-
initiating brain insult, the glutamate receptor agonist kainate is injected into the dorsal
hippocampus (Suzuki et al., 1995). Subsequently, mice develop a non-convulsive SE
(Bouilleret et al., 1999; Gröticke et al., 2008).
Several neurologic diseases, including epilepsies, are accompanied by pathological
changes in BBB integrity (Abbott et al., 2006). Accumulating evidence suggests that
BBB leakage influences both initiation and progression of epileptogenesis (Oby &
Janigro, 2006; Friedman & Heinemann, 2010; Marchi et al., 2011b). Extravasation of
blood components initiates a signalling cascade resulting in increased neuronal
excitability (Oby & Janigro, 2006; Ndode-Ekane et al., 2010). Thus, pharmacotherapy
aiming to restore or maintain BBB integrity may reveal antiepileptogenic or
epileptogenesis-modifying effects (Friedman et al., 2009; Friedman & Heinemann,
2010).
Leucocyte-endothelial interactions were shown to be involved in BBB impairment
(Rivest et al., 2000; Riazi et al., 2010). Treatment with anti-inflammatory drugs like
glucocorticoids were shown to be BBB protective in brain tumors and in specific
inflammatory brain diseases in humans (Friedman & Heinemann, 2010). In rats,
dexamethasone reduced the infarct volume when administered following cerebral
ischemia (Bertorelli et al., 1998). Effects of dexamethasone on BBB integrity of
healthy mice were studied by Hedley-Whyte et al. (1986). Dexamethasone treatment
resulted in decreased BBB permeability for the macromolecule horseradish

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
66
peroxidase. Thus, dexamethasone treatment may provide BBB stabilizing effects
during epileptogenesis, too.
In the present study, we longitudinally evaluated BBB leakage during epileptogenesis
in the intrahippocampal kainate mouse model using a high field strength (7 T)
magnet. The MRI protocol was subsequently used to follow and to evaluate effects of
dexamethasone treatment on BBB integrity.
4.3 Materials and methods
4.3.1 Animals
Adult male NMRI mice (n = 20) were purchased from Charles River Laboratories, Inc.
(Sulzheim, Germany) at six weeks of age and housed in separately ventilated cages
under a 14/10 h dark light cycle and controlled climate conditions (22 ± 1 °C, humidity
45 – 55 %). Standard feed (Altromin 1324; Altromin Spezialfutter GmbH & Co. KG,
Lage, Germany) and autoclaved water were freely accessible. All mice were allowed
to adapt to the new environment for at least two weeks before being used in
experiments. Animals were handled at least three times before start of experiments.
All animal procedures were performed in accordance to the EU council directive
86/609/EWG and the German Law on Animal Protection and approved by the
institutional animal care and use committee. Greatest efforts were made to minimize
animal suffering and to reduce the number of animals used.
4.3.2 Chemicals and drugs
Chloral hydrate and kainate monohydrate were obtained from Sigma-Aldrich
Co. LLC. (Schnelldorf, Germany). Isoflurane (Isofluran Baxter) was purchased from
Baxter Inc. (Unterschleißheim, Germany), gadolinium-diethylenetriamine pentaacetic
acid (Gd-DTPA, Magnevist) was obtained from Bayer HealthCare (Leverkusen,
Germany), dexamethasone (Dexamethasone inject JENAPHARM, 8 mg/2 ml) from
Jena Pharm (Jena, Germany) and electrolyte solution (sterofundin) and saline
(NaCl 0.9 % B. Braun) from B. Braun Melsungen AG (Melsungen, Germany).

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
67
4.3.3 Status epilepticus
A SE was induced by unilateral intrahippocampal kainate injection in 13 mice as
epileptogenesis-triggering primary brain insult. For surgery, animals were
anesthetized with chloral hydrate (400 mg/kg in 10 ml/kg saline i.p.). Body
temperature, heart rate and respiratory rate were monitored continuously. Kainate
was diluted in saline (10 mg kainate in 2345 µl saline) and 50 nanoliters of the
solution, equivalent to 213,2 nanograms kainate, were injected stereotaxically
(Stoelting Co, Wood Dale, Illinois, USA) into the cornu ammonis 1 region of the right
dorsal hippocampus as previously described by Gröticke et al. (2008). Coordinates
for kainate injection were: anterior-posterior: -2.1 mm, laterolateral: -1.6 mm and
dorsoventral: -2.3 mm; relative to bregma. A micro syringe (Hamilton Company,
Franklin, Massachusetts, USA) was lowered to the correct position and left in place
for 2 min prior to injecting 0.05 µl kainate solution slowly over one minute. Sham
animals (n = 7) were injected with 0.05 µl saline instead of kainate. The needle was
left in the injection site for another 2 min to prevent reflux. After surgery, animals
were kept on a heating mat to prevent hypothermia until they were fully awake. Any
seizure activity or abnormal behavior was recorded. All mice received sterofundin
injections [0.5 ml subcutaneous (s.c.) and 0.5 ml i.p.] and body temperature was
controlled before returning to home cage. During subsequent days, body weight, feed
and water intake, movement and body posture as well as grooming and fur condition
were evaluated according to a scoring protocol twice daily (see Table 3). None of the
experiments resulted in scores above 1. Additionally, mice received sterofundin
injections twice a day (0.5 ml s.c.) and were offered standard feed mash for the first
3 d after surgery.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
68
Table 3: Model-specific criteria for animal evaluation after surgery
Parameter Feed and water intake and body weight
Movement and body posture
Grooming and fur
Score
0 normal quick and typical movement, curious, normal body posture
normal
1 reduced feed/water intake, loss of body weight < 10 %
reduced activity, normal reaction to stimuli
normal grooming behavior, reduced gloss of the fur
2 severely reduced feed/water intake, loss of body weight < 20 %
no spontaneous activity, reduced reaction to stimuli
reduced grooming behavior, reddish fur around eyes and nose; penis prolapse
3 no feed/water intake, loss of body weight > 20 %
no spontaneous activity, no reaction to stimuli and/or humpy back
no grooming, shaggy fur, red exudate around eyes and nose; penis prolapse
4.3.4 Study design
BBB integrity and response to dexamethasone treatment were assessed by MRI
(Bruker BioSpin, Ettlingen, Germany). Mice were randomly assigned to one of three
study groups prior to surgery: (1) kainate plus vehicle treatment (SE-KA, n = 8),
(2) sham (intrahippocampal saline, n = 7) and (3) kainate plus dexamethasone
treatment (SE-dex, n = 5). Mice in sham and SE-KA groups were scanned before
(baseline) and at 48 h, 4 d, 16 d and 37 d after surgery for longitudinal in vivo
evaluation of BBB leakage during epileptogenesis. To compare BBB leakage
patterns with and without dexamethasone treatment, SE-dex mice were scanned at
baseline and additionally at 48 h and 4 d after SE.
4.3.5 Evaluation of dexamethasone treatment on blood-brain barrier integrity
during early epileptogenesis
Treatment with the broad spectrum anti-inflammatory drug dexamethasone was
evaluated for BBB protective effects during the acute phase of epileptogenesis in the
intrahippocampal kainate mouse model. T1 intensities after CA infusion in SE-dex
mice were compared with extravasation patterns in SE-KA mice as measured by
MRI. Dexamethasone was used as a commercial solution and injected at a dose of
2 mg/kg i.p. five times following kainate injection (at 6 h, 24 h, 48 h, 72 h and 96 h).
Dose selection and dosing intervals were chosen based on literature (Hedley‐Whyte

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
69
& Hsu, 1986; Bertorelli et al., 1998; Campolo et al., 2013; Al-Shorbagy et al., 2012).
Saline treatment was started 6 h after kainate injection in the SE-KA group. Mice
received 0.9 % saline in a volume of 0.5 ml/kg i.p. once daily for the subsequent 4 d.
This dosing regimen was chosen to match injection times and volumes of the SE-dex
group.
4.3.6 Magnetic Resonance Imaging setup
Anesthesia for MRI was induced by isoflurane inhalation [3 % in air/O2 (2:1) for
anesthesia induction, 1-1.5 % in air/O2 (2:1) for maintaining anesthesia]. A catheter
was fixed in a lateral tail vein to allow contrast agent (CA) administration via infusion
pump (model PHD Ultra; Harvard Apparatus Inc., South Natick, Massachusetts,
USA). All investigations were performed on a 7 T (300 MHz) small animal MR system
(Bruker) with a 16-cm horizontal bore (Bruker BioSpec 70/16) and ParaVision 5.1
(Bruker) acquisition software. The MRI sequences included a T2 map for anatomical
co localization and a post-contrast high resolution T1 modified driven equilibirum
fourier transformation (MDEFT) sequence which was started 30 min after intravenous
(i.v.) infusion of gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA) to assess
BBB leakage. Step-down infusion of CA was previously reported to increase MRI
sensitivity for changes in BBB integrity and their delineation in rats (Nagaraja et al.,
2007; Knight et al., 2009). In this study, we modified our previously adjusted rat
infusion-protocol (Table 4) for imaging BBB leakage post SE in mice.
Table 4: Gd-DTPA infusion protocol mice
Step Duration (min) Rate (ml/min) Volume (ml)
1 0-0.5 0.056 0.028
2 0.5-1 0.044 0.022
3 1-2 0.033 0.033
4 2-3 0.023 0.023
5 3-4 0.018 0.018
6 4-5 0.016 0.016

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
70
Step Duration (min) Rate (ml/min) Volume (ml)
7 5-7 0.014 0.028
8 7-10 0.012 0.036
9 10-15 0.010 0.050
10 15-20 0.008 0.040
Infusion time = 20 min
Total volume = 0.294 ml
Geometric imaging parameters of the 3D scan were 25 x 25 x 13.6 mm field of view
and 256 x 256 x 34-pixel matrix, resulting in a voxel size of 0.098 x 0.098 x 0.4 mm
[repetition time (TR) = 40 ms, echo time (TE) = 3.5 ms, flip angle = 18°,
ID = 1100 ms]. As radiofrequency coil, a mouse brain receive-only coil array
11765V3 was used in combination with a quadrature MRI transmit-only coil with
active decoupling T11070. The receive coil was placed on the animal bed in a
defined position and mice were fixed with an incisor bar to allow comparable
positioning between scan time points and animals.
4.3.7 Image analysis
Accurate segmentation of epilepsy-associated brain regions was achieved by co-
registration of MR images to a mouse brain atlas (Mirrione et al., 2006) using PMOD
3.5 software (see chapter 2). The following brain regions were analyzed: dorsal
hippocampus, ventral hippocampus, amygdala, thalamus and cortex. T1 signal
increase was calculated and normalized to cerebellum as the reference region.
4.3.8 Statistical analysis
Results are displayed as mean ± standard error of the mean (SEM). Multiple
comparisons of Gd-DTPA leakage were calculated by one-way analysis of variance
(ANOVA) with or with Bonferroni’s post hoc test for individual differences using
GraphPad Prism 5 software (GraphPad Software Inc., La Jolla, CA, USA). A p-
value < 0.05 was considered statistically significant.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
71
4.4 Results
4.4.1 Tolerability of dexamethasone in the intrahippocampal kainate mouse
model
Kainate injection resulted in characteristic behavioral changes in all mice. Mild
forelimb clonus, circling, and freezing behavior as well as persisting immobility were
observed. One mouse developed generalized clonic seizures. No mouse from the
sham group displayed seizure-like behavior. Survival rate after surgery was 85.7 %
(6 out of 7 mice), 100 % (8 out of 8 mice) and 100 % (5 out of 5 mice) in sham,
SE-KA and SE-dex groups. Following surgery or SE no significant differences in
body weight were found between groups. The mean scores for movement and body
posture as well as for grooming were found to range between 0 and 1 in the first 3 d
following surgery in the SE-KA group. A score of 0 represents quick and typical
movement, curious behavior, a normal body posture and normal grooming behavior.
A score of 1 represents a reduced activity but normal reaction to stimuli and normal
grooming behavior but reduced gloss of the fur (see Table 3). In the sham group,
mice were scored 0 concerning movement and body posture and grooming from
day 1 post surgery. SE-dex mice were scored 1 in the first 2 d following SE. Score 2
or 3 did not occur in any mouse. No adverse effects of dexamethasone were
observed during the study or at necropsy thereafter.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
72
A B
D
C
Figure 13: Localization of kainate injection as assessed by magnetic resonance imaging (MRI)
(B) Kainate was injected into the cornu ammonis 1 region of the right hippocampus according to Paxinos (2001). Localization was visualized by (A) coronal, (C) sagittal and (D) horizontal MR imaging of the injection site.
4.4.2 Longitudinal Magnetic Resonance imaging during epileptogenesis
reveals blood-brain barrier leakage in epilepsy associated brain regions
Longitudinal in vivo MRI was used to assess BBB leakage before and at d 2, d 4, d
16 and d 37 following focal kainate or saline injections into the right hippocampus.
MRI revealed significantly increased T1 values, indicative of BBB leakage, in limbic
brain regions of SE-KA mice vs baseline. In the hippocampus of SE-KA mice, T1
signal after contrast agent (CA) infusion increased up to 274 % in the ipsilateral
hippocampus 48 h after SE vs. baseline (p < 0.001 , see figure 15). The ipsilateral
ventral hippocampus as well as amygdala, thalamus and cortex were subjected to
BBB leakage, too. T1 hyperintensity was still present in the ipsilateral hippocampus,
the amygdala, thalamus and cortex at 4 d post SE. T1 values subsequently
decreased during the five weeks of follow-up. Sixteen days post SE, T1 values of the
ipsilateral dorsal hippocampus and thalamus were increased. At 37 d post SE, T1

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
73
values were increased in hippocampus, thalamus and cortex but had returned to
baseline levels in all other investigated brain regions.
Moreover, longitudinal in vivo MR imaging revealed significantly increased T1 values,
indicative of BBB leakage, in limbic brain regions of SE-KA vs. sham groups
(see figure 14). Statistical analyses between groups for each time point revealed
significantly higher T1 values 2 d following surgery in the SE-KA group vs. sham in 4
of the examined brain regions: the ipsilateral dorsal hippocampus, the ipsilateral
ventral hippocampus, the ipsilateral amygdala and the ipsilateral thalamus.
Hippocampus dorsal
B li kainatB re kainatSham li 4848 li kainatSham re 4848 re kainatSham li 4d4d li kainatSham re 4d4 re kainatSham li 1616d li kainatSham re 1616 re kainatSham li B3737d li kainatSham re B3737 re kainat0
1
2
3
4 Baseline contralateral
Baseline ipsilateral
2 4 16 37
__*
* significance kainate vs. sham
Baseline
#
#
# #
Sham contralateralKainat contralateralSham ipsilateralKainat ipsilateral
# significance kainate vs. baseline
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]
Hippocampus ventral
B li kainatB re kainatSham li 4848 li kainatSham re 4848 re kainatSham li 4d4d li kainatSham re 4d4 re kainatSham li 1616d li kainatSham re 1616 re kainatSham li B3737d li kainatSham re B3737 re kainat0
1
2
3
4
2 4 16 37
*__
Baseline
#
#
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]
Amygdala
B li kainatB re kainatSham li 4848 li kainatSham re 4848 re kainatSham li 4d4d li kainatSham re 4d4 re kainatSham li 1616d li kainatSham re 1616 re kainatSham li B3737d li kainatSham re B3737 re kainat0
1
2
3
4
2 4 16 37
__*
Baseline
# #
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
74
Figure 14: Quantification of blood-brain barrier leakage during epileptogenesis
Comparison of T1 intensities between kainate (SE-KA) and sham groups for hippocampus, amygdala, thalamus and cortex before (n = 6) and at 2 d (n = 5-6), 4 d (n = 4-5), 16 d (n = 4-5) and 37 d (n = 3-5) after surgery. Longitudinal in vivo magnetic resonance imaging (MRI) analyses between groups for each time point reveal significantly higher T1 values in the SE-KA group vs. sham in the ipsilateral dorsal hippocampus, ventral hippocampus, amygdala and thalamus at 2 d following surgery. One-way ANOVA, Bonferroni’s post hoc test, data marked with * indicate a significant difference vs. sham. All values are presented as mean ± standard error of the mean (SEM).
4.4.3 Dexamethasone treatment protects blood-brain barrier integrity
Dexamethasone treatment was found to significantly reduce BBB leakage in epilepsy
associated brain regions in mice post kainate-induced SE (see figure 15 and figure
16). (1) In the dorsal hippocampus, dexamethasone treatment reduced the T1 signal
intensity by 20.43 % 2 d after SE and by 24.07 % on day 4 as compared to SE-KA
mice (ipsilateral, p < 0.05). (2) In the ventral hippocampus, dexamethasone treatment
reduced the T1 signal intensity by 33.79 % 2 d after SE as compared to SE-KA mice
(ipsilateral, p < 0.05). (3) In thalamus, dexamethasone treatment reduced the T1
signal intensity by 13.34 % 2 d after SE and by 15.31 % on day 4 as compared to
SE-KA mice (ipsilateral, p < 0.05). Moreover, significantly increased T1 values vs.
baseline were present at 2 d and 4 days, respectively, after SE only in the amygdala
of SE-KA animals. Interestingly, signal intensities in the cortex were very similar over
time in both SE-dex and SE-KA groups. BBB leakage occurred at day 2 in this region
and persisted until the end of the dexamethasone study on day 4.
Thalamus
B li kainatB re kainatSham li 4848 li kainatSham re 4848 re kainatSham li 4d4d li kainatSham re 4d4 re kainatSham li 1616d li kainatSham re 1616 re kainatSham li B3737d li kainatSham re B3737 re kainat0
1
2
3
4
2 4 16 37
*__
Baseline
## # #
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]
Cortex
B li kainatB re kainatSham li 4848 li kainatSham re 4848 re kainatSham li 4d4d li kainatSham re 4d4 re kainatSham li 1616d li kainatSham re 1616 re kainatSham li B3737d li kainatSham re B3737 re kainat0
1
2
3
4
2 4 16 37Baseline
# ##
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
75
Figure 15: Blood-brain barrier leakage after dexamethasone treatment
T1 intensities in kainate animals before and after status epilepticus (SE-KA, red) compared with dexamethasone treated (SE-dex) animals (green) for the ipsilateral and contralateral brain hemisphere. Dexamethasone treatment was found to significantly reduce blood-brain barrier leakage in typically epilepsy associated brain regions: dorsal hippocampus, ventral hippocampus and thalamus (all brain regions ipsilateral) on day 2 following SE. Furthermore, significantly lower T1 intensities were present in the dorsal hippocampus and in thalamus of SE-dex animals vs SE-KA 4 d after SE. (Mean ± SEM, baseline (n = 6), d 2 (n = 5), d 4 (n = 5, one-way ANOVA, Bonferroni’s post hoc test, p < 0.05. B = baseline).
Hippocampus dorsal
B left KainatB right Kainat48 h l Kainat48 h left Dexa48 h r Kainat48 h right Dexa4 d l Kainat4 d left Dexa4 d r Kainat4 d right Dexa0
1
2
3
4
*
*##
#
#
B left right
2d left right
4d left right
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]
Hippocampus ventral
B left KainatB right Dexa48 h l Kainat48 h left Dexa48 h r Kainat48 h right Dexa4 d l Kainat4 d left Dexa4 d r Kainat4 d right Dexa0
1
2
3
4
*#__
#
B left right
2d left right
4d left right
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]
Amygdala
B left KainatB right Dexa48 h l Kainat48 h left Dexa48 h r Kainat48 h right Dexa4 d l Kainat4 d left Dexa4 d r Kainat4 d right Dexa0
1
2
3
4
# #
B left right
2d left right
4d left right
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m] Thalamus
B left KainatB right Dexa48 h l Kainat48 h left Dexa48 h r Kainat48 h right Dexa4 d l Kainat4 d left Dexa4 d r Kainat4 d right Dexa0
1
2
3
4
##
#
* *#
#
B left right
2d left right
4d left right
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]
Cortex
B left KainatB right Kainat48 h l Kainat48 h left Dexa48 h r Kainat48 h right Dexa4 d l Kainat4 d left Dexa4 d r Kainat4 d right Dexa0
1
2
3
4
##
# # # significance vs. baseline
* significance SE-KA vs SE-dex
B left right
2d left right
4d left right
Baseline
SE-KA (saline)SE-dex (dexamethasone)
T1 in
ten
sit
y [
reg
ion
/cere
bellu
m]

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
76
Figure 16: Serial magnetic resonance images in kainate, dexamethasone and sham animals
Coronal magnetic resonance (MR) images in kainate induced status epilepticus (SE-KA, left), kainate-SE + dexamethasone (KA-dex, center) and sham (saline, right) mice. BBB leakage was assessed by longitudinal T1 weighted 7 T MRI after contrast agent infusion. BBB leakage is indicated by contrast enhancement in affected brain regions (white areas, exemplary indicated by arrows in SE-KA 4 d post SE). The comparison of SE-KA and KA-dex mice 48 h and 4 d after SE demonstrates lower T1 signals in different brain regions of the dexamethasone treated group. Comparison between SE-KA and sham mice reveals less pronounced contrast enhancement in specific brain regions of sham animals.
Kainate Dexamethasone Sh am
B
48 h
4 d
16 d
37 d

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
77
4.5 Discussion
We performed a longitudinal MR imaging study and found that in vivo MRI during
epileptogenesis is a suitable imaging biomarker for the early detection of changes in
BBB leakage in the intrahippocampal kainate mouse model. Moreover, we used the
imaging protocol to evaluate effects of anti-inflammatory treatment on BBB integrity
and showed for the first time that dexamethasone treatment following
intrahippocampal kainate injection induces a significant protection of BBB integrity in
mice as assessed by MRI following step-down infusion of Gd-DTPA.
4.5.1 Longitudinal in vivo assessment of blood-brain barrier leakage during
epileptogenesis
MRI is accepted as one of the most sensitive in-vivo molecular imaging techniques
for detection of brain lesions present in human TLE (Bouilleret et al., 2000;
Schoknecht & Shalev, 2012). Moreover, MRI is the most commonly used technique
for non-invasive imaging of BBB leakage in pre-clinical animal models, too (Rebeles
et al., 2006; Wunder et al., 2012).
BBB leakage was detected throughout epileptogenesis in the ipsilateral (kainate
injection) hemisphere of SE-KA mice vs. baseline. Two d and 4 d after SE, affected
brain regions included hippocampus, amygdala, thalamus and cortex; brain regions
which are associated with epilepsy. Intensities and spatial extent of BBB impairment
subsequently declined in the five weeks of follow-up. Sixteen days post SE,
increased T1 intensities was present in the ipsilateral dorsal hippocampus and in
thalamus. BBB leakage was still present in the ipsilateral hippocampus, in thalamus
and in the cortex in the chronic epileptic phase. Moreover, comparison between
groups for each time point revealed significantly higher T1 values in the SE-KA group
vs. sham in 4 of the examined brain regions 2 d after surgery: the ipsilateral dorsal
hippocampus, the ventral hippocampus, the amygdala and in thalamus.
The injection cannula produces a mechanical lesion (Bouilleret et al., 2000) in focal
kainate models. We saw hyperintense tissue in the cortex above the
intrahippocampal injection site which occurred solely in the ipsilateral hemisphere of

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
78
the brain at d 2 and d 4 in all investigated groups. These findings suggest that, to a
large proportion, the T1 hyperintensity along the injection track is a result of this
lesion rather than of excitotoxic effects of kainate or epileptogenesis-associated BBB
leakage. Nevertheless, diffusion of kainate into the injection track was limited as
much as possible by leaving the needle in situ for additional 2 min following kainate
injection (see 4.3.3). We observed the highest BBB permeability of all investigated
brain regions in the dorsal hippocampus of the SE-KA group at day 2 following SE.
These results are in agreement with the finding that hippocampal CA1 and CA3
subfields are particularly vulnerable to injury associated with SE (Fujikawa, 1996).
Moreover, we observed hyperintense T1 signals in the ventral hippocampus,
amygdala and thalamus on day 2 and 4. Subsequently, T1 intensities progressively
decreased during the five weeks of follow-up and significantly increased values were
present in less brain regions in the chronic epileptic phase, 37 d after SE. These
results support the assumption that BBB leakage is not static but a dynamic process
with varying degrees depending on the progress of epileptogenesis and occurring in
different brain regions during focal kainate-induced epileptogenesis.
An increase in T1 intensity was shown in the cortex (Bouilleret et al., 2000) in a
previous study. This signal appeared in the first hour and lasted until 3 d after kainate
injection. However, in other brain regions, only changes in T2 intensity but not in T1
intensity were detected. The discrepancies compared to our study presumably result
from differences in MRI technique and protocols. In our study, 7 T MRI using a high
resolution 3D T1 MDEFT imaging sequence following step-down infusion of Gd-
DTPA was applied to detect BBB leakage. Step-down infusion protocols for MRI CA
were previously shown to improve sensitivity for detection of BBB leakage compared
with bolus injection of CA (Nagaraja et al., 2007; Knight et al., 2009). Bouilleret et al.
(2000) used 4.7 T MRI after bolus injection of Gd-DOTA. They found that T2 signal
increase 7 d after kainate injection was limited to the ipsilateral hippocampus and
concluded that the reason might be absent spreading of seizure activity.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
79
4.5.2 Dexamethasone treatment significantly reduces blood-brain barrier
leakage
We found a significant reduction of BBB leakage after dexamethasone treatment in
typically epilepsy associated brain regions during early epileptogenesis. SE-KA
treated and SE-dex mice were scanned 2 d and 4 d following intrahippocampal
kainate injection. Analysis revealed that mice being treated with dexamethasone after
SE showed significantly less BBB leakage in the ipsilateral dorsal hippocampus,
ventral hippocampus and thalamus on day 2 compared with saline treated animals.
BBB leakage was reduced by dexamethasone treatment in the ipsilateral dorsal
hippocampus and thalamus on day 4, too. Thus, we conclude that dexamethasone
protects BBB integrity in the most affected brain regions after KA-induced SE. T1
hyperintensity in the cortex was not reduced or modified by dexamethasone
treatment. It is considered that the increase of T1 intensities is caused by the lesion
of the injection cannula along the injection track rather than by excitotoxic effects of
kainate or by epileptogenesis-associated BBB leakage. The cortex, therefore, may
not be suitable to assess BBB leakage in the focal kainate model as discussed
above.
Dexamethasone is a broad-spectrum anti-inflammatory drug which acts on
glucocorticoid receptors and reduces the expression of adhesion molecules,
inflammatory chemokines and cytokines (Barnes, 2006; Laurila et al., 2009). The
molecular mechanisms, underlying possible therapeutic effects on the BBB, are not
known in detail. In a recently published study, BBB-restorative effects were found to
be mediated by upregulation of ZO-1 tight junction proteins and occurred via binding
of dexamethasone to glucocorticoid receptors in an vitro model of primary blast injury
(Hue et al., 2015). The mechanism of action was confirmed by application of
mifepristone (RU-486), a steroid antagonist which prevented BBB-restorative effects
of dexamethasone. Another suggested mechanism of action is the inhibition of NF-
kappa-B activity by dexamethasone (Auphan et al., 1995). NF-kappa-B can impair
BBB function by alteration of tight junction protein expression (Brown et al., 2003).
Dexamethasone significantly reduced TNF production and reduced the infarct size by
50 % in a rat model of focal cerebral ischemia (Bertorelli et al., 1998).

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
80
However, as inflammatory processes themselves play a role in restoring brain
homeostasis following brain insults (Abbott, 2002; Serrano et al., 2011), finding the
right balance between aggravation and rehabilitation of inflammatory processes is
important (Gröhn & Pitkänen, 2007). Disturbing BBB homeostasis could entail side
effects (Abbott, 2002). Glucocorticoids are widely used in the clinic, for example for
treatment of the Landau-Kleffner syndrome, a specific form of pediatric epilepsy
(Vezzani et al., 2011). However, glucocorticoids can be harmful in patients with acute
ischemic stroke (Kleinschnitz et al., 2011). Moreover, deterioration of brain injury and
survival rate were the outcome of dexamethasone treatment in a recent study in the
lithium-pilocarpine post SE rat model (Duffy et al., 2014). These findings suggest that
the efficacy of glucocorticoids can be very different dependent on the underlying
disease. Hence, effects of dexamethasone on specific alterations occurring in the
process of epileptogenesis need to be further evaluated.
4.6 Conclusion
We demonstrate for the first time that dexamethasone protects BBB integrity in the
intrahippocampal kainate mouse model. Moreover, longitudinal in vivo MRI detects
changes in BBB leakage during epileptogenesis in this model. Restoration of
impaired BBB integrity may contribute to prevention of epilepsies following brain
insults as BBB leakage is strongly associated with the process of epileptogenesis
(Gorter et al., 2015). We hence hypothesize that BBB-protective dexamethasone
treatment may reveal antiepileptogenic or epileptogenesis-modifying effects in future
studies that include evaluation of the chronic epileptic phase.
ACKNOWLEDGEMENTS: We thank Christian Bergen and Friederike Twele for skillful technical
assistance. The study is funded by the European Union’s Seventh Framework Programme (FP7)
under grant agreement n°602102 (EPITARGET). H.B. was supported by a scholarship from the
Studienstiftung des Deutschen Volkes.
CONFLICTS OF INTEREST: none

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
81
4.7 References
ABBOTT, N.J. (2002). Astrocyte-endothelial interactions and blood–brain barrier permeability. Journal of Anatomy 200, 629-638.
ABBOTT, N.J., RONNBACK, L. & HANSSON, E. (2006). Astrocyte-endothelial interactions at the blood-
brain barrier. Nature Reviews Neuroscience 7, 41-53.
Al-Shorbagy, M.Y., El Sayeh, B.M. & Abdallah, D.M. (2012). Diverse effects of variant doses of
dexamethasone in lithium-pilocarpine induced seizures in rats. Canadian Journal of Physiology and Pharmacology 90, 13-21.
AUPHAN, N., DIDONATO, J.A., ROSETTE, C., HELMBERG, A. & KARIN, M. (1995). Immunosuppression by
glucocorticoids: inhibition of NF-kappaB activity through induction of IkappaB synthesis. Science 270, 286.
BARNES, P.J. (2006). Corticosteroid effects on cell signalling. European Respiratory Journal 27, 413-
426.
BEN-ARI, Y., LAGOWSKA, J., TREMBLAY, E. & LA SALLE, G.L.G. (1979). A new model of focal status
epilepticus: intra-amygdaloid application of kainic acid elicits repetitive secondarily generalized convulsive seizures. Brain Research 163, 176-179.
BERTORELLI, R., ADAMI, M., DI SANTO, E. & GHEZZI, P. (1998). MK 801 and dexamethasone reduce both
tumor necrosis factor levels and infarct volume after focal cerebral ischemia in the rat brain. Neuroscience Letters 246, 41-44.
BOUILLERET, V., NEHLIG, A., MARESCAUX, C. & NAMER, I.J. (2000). Magnetic resonance imaging follow-
up of progressive hippocampal changes in a mouse model of mesial temporal lobe epilepsy. Epilepsia 41, 642-650.
BOUILLERET, V., RIDOUX, V., DEPAULIS, A., MARESCAUX, C., NEHLIG, A. & LA SALLE, G.L. (1999).
Recurrent seizures and hippocampal sclerosis following intrahippocampal kainate injection in adult mice: Electroencephalography, histopathology and synaptic reorganization similar to mesial temporal lobe epilepsy. Neuroscience 89, 717-729.
BROWN, R.C., MARK, K.S., EGLETON, R.D., HUBER, J.D., BURROUGHS, A.R. & DAVIS, T.P. (2003).
Protection against hypoxia-induced increase in blood-brain barrier permeability: role of tight junction proteins and NFκB. Journal of Cell Science 116, 693-700.
CORNFORD, E.M. & OLDENDORF, W.H. (1986). Epilepsy and the blood-brain barrier. Advances in
Neurology 44, 787-812.
DUFFY, B.A., CHUN, K.P., MA, D., LYTHGOE, M.F. & SCOTT, R.C. (2014). Dexamethasone exacerbates
cerebral edema and brain injury following lithium-pilocarpine induced status epilepticus. Neurobiology of Disease 63, 229-236.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
82
FRIEDMAN, A. & HEINEMANN, U. (2010). Role of blood-brain barrier injury in epileptogenesis. Epilepsia 51, 34-34.
FRIEDMAN, A., KAUFER, D. & HEINEMANN, U. (2009). Blood-brain barrier breakdown-inducing astrocytic
transformation: Novel targets for the prevention of epilepsy. Epilepsy Research 85, 142-149.
FUJIKAWA, D.G. (1996). The temporal evolution of neuronal damage from pilocarpine-induced status
epilepticus. Brain Research 725, 11-22.
GORTER, J.A., VAN VLIET, E.A. & ARONICA, E. (2015). Status epilepticus, blood-brain barrier disruption,
inflammation, and epileptogenesis. Epilepsy & Behavior 49, 13-16.
GRÖHN, O. & PITKÄNEN, A. (2007). Magnetic resonance imaging in animal models of epilepsy-
noninvasive detection of structural alterations. Epilepsia 48, 3-10.
GRÖTICKE, I., HOFFMANN, K. & LÖSCHER, W. (2008). Behavioral alterations in a mouse model of
temporal lobe epilepsy induced by intrahippocampal injection of kainate. Experimental Neurology 213, 71-83.
HEDLEY‐WHYTE, E.T. & HSU, D.W. (1986). Effect of dexamethasone on blood‐brain barrier in the
normal mouse. Annals of Neurology 19, 373-377.
HERMAN, S.T. (2002). Epilepsy after brain insult Targeting epileptogenesis. Neurology 59, 21-26.
HSU, Y.H., LEE, W.T. & CHANG, C. (2007). Multiparametric MRI evaluation of kainic acid-induced
neuronal activation in rat hippocampus. Brain 130, 3124-3134.
HUE, C.D., CHO, F.S., CAO, S., RDALER BASS, C.R., MEANEY, D.F. & MORRISON III, B. (2015).
Dexamethasone potentiates in vitro blood-brain barrier recovery after primary blast injury by glucocorticoid receptor-mediated upregulation of ZO-1 tight junction protein. Journal of Cerebral Blood Flow & Metabolism 35, 1191-1198.
JUPP, B., WILLIAMS, J., BINNS, D. & HICKS, R. (2007). Imaging small animal models of epileptogenesis.
Neurology Asia 12, 51-54.
KLEIN, S., BANKSTAHL, M., GRAMER, M., HAUSKNECHT, M. & LÖSCHER, W. (2014). Low doses of ethanol
markedly potentiate the anticonvulsant effect of diazepam in a mouse model of difficult to-treat focal seizures. Epilepsy Research 108, 1719-1727.
KLEINSCHNITZ, C., BLECHARZ, K., KAHLES, T., SCHWARZ, T., KRAFT, P., GOBEL, K., MEUTH, S.G., BUREK,
M., THUM, T., STOLL, G. & FORSTER, C. (2011). Glucocorticoid insensitivity at the hypoxic blood-brain barrier can be reversed by inhibition of the proteasome. Stroke 42, 1081-1089.
KNIGHT, R.A., KARKI, K., EWING, J.R., DIVINE, G.W., FENSTERMACHER, J.D., PATLAK, C.S. & NAGARAJA,
T.N. (2009). Estimating blood and brain concentrations and blood-to-brain influx by magnetic resonance imaging with step-down infusion of Gd-DTPA in focal transient cerebral ischemia

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
83
and confirmation by quantitative autoradiography with Gd-[(14)C]DTPA. Journal of Cerebral Blood Flow and Metabolism 29, 1048-1058.
LAURILA, J.P., LAATIKAINEN, L.E., CASTELLONE, M.D. & LAUKKANEN, M.O. (2009). SOD3 Reduces
Inflammatory Cell Migration by Regulating Adhesion Molecule and Cytokine Expression. PLoS ONE 4, e5786.
LÖSCHER, W. & BRANDT, C. (2010). Prevention or Modification of Epileptogenesis after Brain Insults:
Experimental Approaches and Translational Research. Pharmacological Reviews 62, 668-700.
MARCHI, N., TIERNEY, W., ALEXOPOULOS, A.V., PUVENNA, V., GRANATA, T. & JANIGRO, D. (2011). The
etiological role of blood-brain barrier dysfunction in seizure disorders. Cardiovascular Psychiatry and Neurology 482415, 30.
MIRRIONE, M.M., SCHIFFER, W.K., SIDDIQ, M., DEWEY, S.L. & TSIRKA, S.E. (2006). PET imaging of
glucose metabolism in a mouse model of temporal lobe epilepsy. Synapse 59, 119-121.
NAGARAJA, T.N., NAGESH, V., EWING, J.R., WHITTON, P.A., FENSTERMACHER, J.D. & KNIGHT, R.A. (2007).
Step-down infusions of Gd–DTPA yield greater contrast-enhanced magnetic resonance images of BBB damage in acute stroke than bolus injections. Magnetic Resonance Imaging 25, 311-318.
NDODE-EKANE, X.E., HAYWARD, N., GROHN, O. & PITKANEN, A. (2010). Vascular changes in epilepsy:
functional consequences and association with network plasticity in pilocarpine-induced experimental epilepsy. Neuroscience 166, 312-332.
OBY, E. & JANIGRO, D. (2006). The Blood–Brain Barrier and Epilepsy. Epilepsia 47, 1761-1774.
PITKÄNEN, A. & LUKASIUK, K. (2009). Molecular and cellular basis of epileptogenesis in symptomatic
epilepsy. Epilepsy & Behavior 14, 16-25.
REBELES, F., FINK, J., ANZAI, Y. & MARAVILLA, K.R. (2006). Blood-brain barrier imaging and therapeutic
potentials. Topics in Magnetic Resonance Imaging 17, 107-116.
RIAZI, K., GALIC, M.A. & PITTMAN, Q.J. (2010). Contributions of peripheral inflammation to seizure
susceptibility: cytokines and brain excitability. Epilepsy Research 89, 34-42.
RIBAN, V., BOUILLERET, V., PHAM-LE, B., FRITSCHY, J.-M., MARESCAUX, C. & DEPAULIS, A. (2002).
Evolution of hippocampal epileptic activity during the development of hippocampal sclerosis in a mouse model of temporal lobe epilepsy. Neuroscience 112, 101-111.
RIVEST, S., LACROIX, S., VALLIÈRES, L., NADEAU, S., ZHANG, J. & LAFLAMME, N. (2000). How the blood
talks to the brain parenchyma and the paraventricular nucleus of the hypothalamus during systemic inflammatory and infectious stimuli. Proceedings of the Society for Experimental Biology and Medicine 223, 22-38.

Dexamethasone Reduces Blood-Brain Barrier Leakage in a Mouse Model of Epileptogenesis
84
SCHOKNECHT, K. & SHALEV, H. (2012). Blood-brain barrier dysfunction in brain diseases: Clinical experience. Epilepsia 53, 7-13.
SERRANO, G., LELUTIU, N., ROJAS, A., COCHI, S., SHAW, R., MAKINSON, C., WANG, D., FITZGERALD, G. &
DINGLEDINE, R. (2011). Ablation of cyclooxygenase-2 in forebrain neurons is neuroprotective and dampens brain inflammation after status epilepticus. The Journal of Neuroscience 31, 14850-14860.
SLOVITER, R.S. (2005). The neurobiology of temporal lobe epilepsy: too much information, not enough
knowledge. Comptes Rendus Biologies 328, 143-153.
SLOVITER, R.S. & BUMANGLAG, A.V. (2013). Defining “epileptogenesis” and identifying
“antiepileptogenic targets” in animal models of acquired temporal lobe epilepsy is not as simple as it might seem. Neuropharmacology 69, 3-15.
STABLES, J.P., BERTRAM, E., DUDEK, F.E., HOLMES, G., MATHERN, G., PITKÄNEN, A. & WHITE, H.S.
(2003). Therapy discovery for pharmacoresistant epilepsy and for disease-modifying therapeutics: summary of the NIH/NINDS/AES models II workshop. Epilepsia 44, 1472-1478.
STABLES, J.P., BERTRAM, E.H., WHITE, H.S., COULTER, D.A., DICHTER, M.A., JACOBS, M.P., LOSCHER,
W., LOWENSTEIN, D.H., MOSHE, S.L., NOEBELS, J.L. & DAVIS, M. (2002). Models for epilepsy and epileptogenesis: report from the NIH workshop, Bethesda, Maryland. Epilepsia 43, 1410-1420.
SUZUKI, F., JUNIER, M.P., GUILHEM, D., SORENSEN, J.C. & ONTENIENTE, B. (1995). Morphogenetic effect
of kainate on adult hippocampal neurons associated with a prolonged expression of brain-derived neurotrophic factor. Neuroscience 64, 665-674.
VAN VLIET, E.A., DA COSTA ARAÚJO, S., REDEKER, S., VAN SCHAIK, R., ARONICA, E. & GORTER, J.A.
(2007). Blood–brain barrier leakage may lead to progression of temporal lobe epilepsy. Brain 130, 521-534.
VEZZANI, A., FRENCH, J., BARTFAI, T. & BARAM, T.Z. (2011). The role of inflammation in epilepsy. Nature
Reviews Neurology 7, 31-40.
WUNDER, A., SCHOKNECHT, K., STANIMIROVIC, D.B., PRAGER, O. & CHASSIDIM, Y. (2012). Imaging blood-
brain barrier dysfunction in animal disease models. Epilepsia 6, 14-21.

General discussion
85
5 General Discussion
5.1 Main findings
The studies were set out to investigate suitable molecular imaging methods and
protocols for evaluation of blood-brain barrier (BBB) integrity as a prerequisite to
identify BBB leakage as a potential biomarker for epileptogenesis and as a target for
antiepileptogenic treatment which may contribute to the prevention of epilepsy
development in at-risk patients after brain insults in the future.
The main findings of the studies presented in this work are that (1) small animal
[68Ga]-diethylenetriamine pentaacetic acid (DTPA) positron emission tomography
(PET) imaging, (2) [99mTc]-DTPA single photon emission computed tomography
(SPECT) imaging and (3) magnetic resonance (MR) imaging following tracer or
contrast agent (CA) infusion allow for in vivo detection of BBB leakage in a post
status epilepticus (SE) rat model during early epileptogenesis, (4) magnetic
resonance imaging (MRI) being the most sensitive molecular imaging method.
Moreover we showed that (5) the same is true for MR imaging of the
intrahippocampal mouse model throughout the process of epileptogenesis. (6) The
pharmacological intervention with losartan may adversely affect BBB integrity and
edema formation after SE in rats. (7) Dexamethasone treatment exacerbates edema
formation in the lithium-pilocarpine rat model but (8) significantly reduces BBB
leakage following intrahippocampal kainate injections in mice.
These are the first studies showing BBB protective effects of dexamethasone in the
intrahippocampal mouse model and the first studies to use [68Ga]-DTPA PET and
[99mTc]-DTPA SPECT for pre-clinical detection of BBB leakage in the lithium-
pilocarpine rat model.
5.2 Multimodal imaging of blood-brain barrier leakage during
epileptogenesis
Dedicated small animal PET, SPECT and MR imaging in vivo enabled us to
characterize and to compare the spatial and temporal extent of BBB leakage during

General discussion
86
early epileptogenesis in the lithium-pilocarpine rat model. All imaging modalities
detect BBB leakage 48 h post SE in the hippocampus and cortex; brain regions
which are known to be connected with epilepsy. Because PET and SPECT have
higher sensitivity, specificity and signal-to-noise ratio compared with MRI (Skotland,
2012; Wunder et al., 2012), one might expect that nuclear imaging is more suitable
for detecting BBB leakage. However, our data revealed that contrast-enhanced MRI
is the most appropriate technique for this purpose. Despite its limitations in sensitivity
(Skotland, 2012) and quantification, MRI detected CA extravasation in both limbic
and cortical brain regions 48 h after SE, including the hippocampus, amygdala,
entorhinal cortex, piriform cortex, motor cortex, substantia nigra, thalamus and
different cortical sub-regions. SPECT detected BBB leakage in the hippocampus,
motor cortex, piriform cortex, cingulate cortex and septum.
Furthermore, longitudinal imaging allowed us to examine temporal patterns of BBB
leakage. No BBB leakage was detected at 5 h after SE. The highest increase in BBB
leakage was detected by both MRI and SPECT at 48 h. Moreover MRI was sensible
to detect BBB leakage at 4 d in the amygdala and in a cortical subregion. At 10 d,
SPECT did not detect BBB leakage whilst MRI found increased tracer extravasation
into hippocampal subregions. Recently, an MRI study has shown maximal MR signal
intensities in hippocampus and piriform cortex 48 h after SE which returned to
baseline levels around day 7 (Choy et al., 2010). Moreover, van Vliet et al. (2014b)
detected BBB leakage in limbic brain regions 24 h and six weeks after SE. Our
results support these findings and extend them by showing that at 48 h post SE
cortical brain regions, besides limbic structures, are subjected to BBB impairment
and by implementing the time course of T2 intensities as indicators for cerebral
edema.
MRI has the highest spatial resolution. Of the three evaluated techniques it is the
only one that can display structural changes occurring during epileptogenesis, like
hippocampal sclerosis and associated loss of hippocampal volume (Spencer, 1994).
T2 intensities reached peak values at 2 d post SE. Accordingly, edema formation
occurs early after SE, like detectable BBB leakage does. Fast edema formation is
followed by a quick resolution by day 10. The results are consistent to studies by

General discussion
87
Roch et al. (2002), Choy et al. (2010) and Duffy et al. (2014) who found that edema
formation following brain insults peaks around day 2.
The intrahippocampal mouse model was included in the studies besides the lithium-
pilocarpine rat model to take interspecies and model-specific differences into
consideration. MRI following Gd-DTPA infusion allowed for longitudinal investigation
of BBB integrity despite the small brain size of mice. SE-KA animals were scanned
baseline and at 2 d, 4 d, 16 d and 37 d after SE. BBB leakage was present in the
ipsilateral dorsal hippocampus, ventral hippocampus, cortex, amygdala and thalamus
2 d and 4 d after SE vs. baseline. Moreover, BBB leakage was found in the ipsilateral
hippocampus and thalamus at 16 d post SE. At 37 d after SE, BBB leakage was
detected in the ipsilateral hippocampus, thalamus and cortex of SE-KA mice vs.
baseline. These results show that BBB leakage is present in both the acute and the
chronic phase of epileptogenesis in mice. In agreement with the study on rats, we
observed the highest BBB permeability of all investigated brain regions in the dorsal
hippocampus at day 2 and day 4 following SE. These results are in agreement with
the finding that hippocampal CA1 and CA3 subfields are particularly vulnerable to
injury associated with SE (Fujikawa, 1996). The time course of BBB leakage is
divergent whilst affected brain regions are similar in both models. However, identical
time points for investigations in rats and mice would be needed to fully evaluate
matches in the time course of BBB leakage in both models. BBB leakage was
present in both brain hemispheres in the pilocarpine post SE rat model whilst
changes were limited to the ipsilateral brain hemisphere in the intrahippocampal
kainite mouse model. This may be explained by the fact that compared to the
systemic pilocarpine rat model, intrahippocampal kainate injection in mice induces a
focal injury.
PET detected BBB impairment 48 h post SE in rats in hippocampus and motor
cortex. A tendency towards increased tracer uptake was present in the entorhinal
cortex. Thus, unexpectedly, PET is the least sensitive imaging modality. Firstly, the
brains microvasculature may contribute to this result. The adult human blood-brain
interface amounts to an average between 12 and 18 m2 (Nag & Begley, 2005).
Hence, the background signal deriving from surrounding blood vessels may be high.
Consequently, the specific tracer signal could be too low to be distinguished from the

General discussion
88
background signal in the presence of only subtle BBB leakage. Secondly, the tracer
itself may play a role. This is the first study to use [68Ga]-DTPA for PET imaging of
BBB leakage. Thus, not much is known about the tracer kinetics in combination with
the chelator DTPA. Our proof-of-principle study showed that [68Ga]-DTPA detects
BBB leakage. However, further in vivo-research that goes behind the scope of this
study is needed to evaluate whether the tracer characteristics correspond to those of
an ideal tracer for BBB imaging. However, a structurally similar tracer, [68Ga]-
ethylenediamine tetraacetic acid, has been successfully used to detect BBB integrity
in multiple sclerosis and glioma patients (Pozzilli et al., 1988; Keith L. Black et al.,
1997). Beyond, very little literature is available on PET studies of BBB leakage. So
far most PET studies aimed at the BBB targeted multidrug transporters like
p-glycoprotein (Bankstahl et al., 2008; Bankstahl et al., 2011) or BBB penetration of
tracers (Waterhouse, 2003).
5.3 Methodological issues
The use of bolus injections of [68Ga]-DTPA in one group and step-down infusion of
tracer in another group allowed us to compare differences between the two
approaches. PET imaging following step-down infusion of [68Ga]-DTPA detects BBB
leakage in the hippocampus whilst PET imaging following bolus injection of the tracer
does not. It thus seems that PET imaging following tracer infusion is more sensitive
in detecting BBB leakage compared with injection as a bolus. These data agree with
those of previous MRI studies targeting BBB leakage after CA infusion in rat models
of transient cerebral ischemia or systemic kainate-induced SE (Nagaraja et al., 2007;
Knight et al., 2009; van Vliet et al., 2014b). These studies found that MRI following
step-down infusion of Gd-DTPA and gadobutrol, respectively, yielded greater
contrast enhancement than bolus injections. It can be assumed that these
dissimilarities result from differences in plasma-concentrations of CA. CA
concentration reaches a quick peak and subsequently decreases continuously after
bolus injection (Knight et al., 2009). Thus, spatial limits were found to be about 2 mm
for detecting BBB leakage after bolus injection of Gd-DTPA (Knight et al., 2005).
Step-down infusion allows maintenance of constant CA concentrations in the blood
(Hamilton et al., 1997). These lead to quantitatively and spatially accurate

General discussion
89
estimations of Gd-DTPA concentrations as shown in cerebral ischemia for volumes
as low as 0.5 mm3 (Knight et al., 2009). The accuracy of estimations was confirmed
by comparison with Gd-[14C]-DTPA, a radio-labeled analog of Gd-DTPA and
quantitative autoradiography.
5.4 Effects of losartan on blood-brain barrier integrity
MRI has proven to be the most sensitive imaging modality for detecting BBB
impairment. Thus, MR imaging of BBB leakage and edema formation were used as
imaging biomarkers to evaluate effects of a potentially BBB-protective losartan
treatment schedule in rats after SE. In the SE-losartan group, BBB leakage was
present at day 10 whilst it was absent in the SE-saline group. Furthermore, edema
formation was increased in SE-losartan vs. SE-saline rats in distinct brain regions. It
thus seems that losartan does not stabilize BBB integrity or attenuate cerebral
edema in the pilocarpine post SE rat model. On the contrary, losartan may adversely
affects BBB integrity and edema formation in the chosen setup. In previous studies,
losartan treatment resulted in delayed seizure onset or the prevention of seizures,
respectively (Ivanova et al., 2013; Bar‐Klein et al., 2014). A possible explanation for
the apparent discrepancy may be the study setup. We evaluated BBB leakage after
losartan treatment during early epileptogenesis. Previous epilepsy-related studies
were designed to evaluate antiepileptogenic effects of losartan. Hence, losartan was
administered chronically and the focus of examinations was monitoring the onset and
characteristics of spontaneous recurrent seizures Bar‐Klein et al. (2014) started
electrocorticography recordings from day 28. Monitoring animals until the chronic
epileptic phase was beyond the scope of this study. Therefore we cannot rule out
that losartan would have revealed disease modifying effects in the chronic epileptic
phase.
5.5 Effects of dexamethasone on blood-brain barrier integrity
The establishment of suitable imaging protocols (see chapter 2) for imaging BBB
leakage enabled us to evaluate effects of dexamethasone treatment on BBB integrity
in both rats and mice. To test the working hypothesis that dexamethasone is BBB

General discussion
90
protective, rats and mice were subjected to SE, treated with dexamethasone and
subsequently scanned on MRI.
MR imaging performed at 48 h after SE in rats revealed BBB leakage in a spatial and
quantitative extent that was comparable to SE-saline animals. However, T2 values
were found to be higher in specific brain regions of SE-dexamethasone rats. Our
results suggest that edema formation is favored by dexamethasone treatment in the
lithium-pilocarpine rat model.
As described in manuscript 3 (chapter 4), dexamethasone treatment induces a
significant reduction of BBB leakage in typically epilepsy associated brain regions in
mice. Thus, dexamethasone treatment leads to controversial results in the two
different animal models. Different conceivable reasons can be discussed for these
distinctions.
First, the dosing regimen needs to be taken into account. Rats received three
dexamethasone injections, starting 3 h after SE (8 mg/kg i.p) and 24 h (8 mg/kg i.p)
and 48 h thereafter (4 mg/kg i.p.). Mice received 2 mg/kg i.p. five times following
kainate injection (at 6 h, 24 h, 48 h, 72 h and 96 h). Thus, mice were treated with
lower but more doses of dexamethasone. The higher doses in rats may induce side
effects. Duffy et al. (2014) found that a dose of 10 mg/kg sodium phosphate
dexamethasone injected twice resulted in increased T2 values at day 2 and day 4
after SE and was accompanied by a high mortality in rats. However, also low doses
of dexamethasone (2 mg/kg i.p.) administered once resulted in increased T2 values.
This leads to a second possible explanation for the apparent discrepancy on
dexamethasone treatment in rats and mice, namely differences in animal models.
Rats after SE seem to be more sensitive to side effects deriving from
dexamethasone treatment than mice. Our finding that one rat developed visible side
effects in form of gastric ulcerations support this assumption. An accumulative effect
of more frequent dexamethasone application can be ruled out as dexamethasone
revealed BBB protective effects in mice at day 2 following SE, a time point that was
investigated in both models.

General discussion
91
Positive outcomes of glucocorticoid treatments are shown by previous reports on
cerebral ischemia. Reduced infarct volumes and tumor necrosis factor levels were
found following methyl-prednisolone or dexamethasone treatment (Bertorelli et al.,
1998; Slivka & Murphy, 2001). Moreover, a combination therapy with dexamethasone
and melatonin was neuro-protective and reduced cerebral edema in a mouse model
of traumatic brain injury (Campolo et al., 2013); agreeing with the BBB protective
results we found in mice. Further studies on epilepsy models have been performed
(Marchi et al., 2011a; Al-Shorbagy et al., 2012). However, dexamethasone was given
prior to SE. Therefore, such studies may have observed brain insult-modifying effects
of dexamethasone rather than its impact on epileptogenesis-associated mechanisms.
The use of glucocorticoids is a controversial issue and remains unsolved to date. Our
studies in two different animal models indicate that the outcome of dexamethasone
treatment is dependent on the dosing regimen and on the animal model. We showed
BBB protective effects in mice which recommend dexamethasone for further studies
of the relationship with the process of epileptogenesis.
5.6 Limitations of the studies
The present studies investigated treatment effects on acute changes in BBB integrity.
Further research may implicate continuous video/ECoG monitoring for determination
of changes during the latency phase as well as during seizure onset, seizure
frequency and seizure duration and thus further evaluate the relationship between
BBB integrity and antiepileptogenesis.
5.7 Future directions
Tracer injection as a bolus is the standard procedure in (preclinical) PET (Carson,
2000). Our results suggest that radiotracer infusion may be beneficial for detecting
BBB leakage during epileptogenesis not only in MRI but in nuclear medicine
techniques, too. Furthermore, a slower but longer lasting application as in infusion vs.
bolus provides a lesser impact on the brains endothelium. It may be taken into
consideration that a quickly administration of a volume which is high in relation to the

General discussion
92
bodyweight may per se influence BBB integrity (Nagaraja et al., 2007) in epilepsy
models.
Even though all imaging techniques reveal changes in BBB integrity, MRI detects
BBB leakage that is missed by PET and SPECT. Thus, MRI is superior to PET and
SPECT in the used study design. However, every imaging modality has its specific
limitations (James & Gambhir, 2012). A combinational use of PET, SPECT and MRI
could therefore benefit from the strength of each imaging technique.
The results of the present studies are important as they provide further insights into
the dynamics of BBB leakage and cerebral edema formation during epileptogenesis.
Moreover, they offer suitable imaging protocols to further evaluate the role of BBB
impairment as potential biomarker for epileptogenesis. A combination of MRI and
nuclear imaging may be beneficial for further investigating BBB during
epileptogenesis in the future.
5.8 Conclusion
The study has offered an evaluative perspective on multimodal molecular imaging of
changes in BBB integrity during epileptogenesis.
In the current studies, we present evidence that pre-clinical nuclear imaging is a
valuable tool for the evaluation of BBB integrity. While contrast-enhanced MRI is a
generally accepted and widely used tool for detecting BBB impairment, our
observations that [68Ga]-DTPA PET and [99mTc]-DTPA SPECT can contribute to
evaluation of BBB integrity during epileptogenesis are novel.
Our results show for the first time a successful reduction of BBB leakage by a dosing
regimen of dexamethasone in mice during epileptogenesis which may contribute to
epileptogenesis-modifying pharmacotherapies. The use of in vivo MR imaging
enables the evaluation of pharmacotherapeutic effects on BBB integrity. Thus,
assessment of patients responding to BBB-protective therapy may be feasible in the
future.

References
93
6 References
ABBOTT, N.J. (2002). Astrocyte–endothelial interactions and blood–brain barrier permeability. Journal of Anatomy 200, 629-638.
ABBOTT, N.J. & FRIEDMAN, A. (2012). Overview and introduction: The blood–brain barrier in health and
disease. Epilepsia 53, 1-6.
ABBOTT, N.J., PATABENDIGE, A.A.K., DOLMAN, D.E.M., YUSOF, S.R. & BEGLEY, D.J. (2010). Structure
and function of the blood–brain barrier. Neurobiology of Disease 37, 13-25.
ABBOTT, N.J., RONNBACK, L. & HANSSON, E. (2006). Astrocyte-endothelial interactions at the blood-
brain barrier. Nature Reviews Neuroscience 7, 41-53.
AL-SHORBAGY, M.Y., EL SAYEH, B.M. & ABDALLAH, D.M. (2012). Diverse effects of variant doses of
dexamethasone in lithium-pilocarpine induced seizures in rats. Canadian Journal of Physiology and Pharmacology 90, 13-21.
ALLAN, S.M., TYRRELL, P.J. & ROTHWELL, N.J. (2005). Interleukin-1 and neuronal injury. Nature
Reviews Immunology 5, 629-640.
ALLEN JR, H.C., LIBBY, R.L. & CASSEN, B. (1951). The scintillation counter in clinical studies of human
thyroid physiology using I131. The Journal of Clinical Endocrinology & Metabolism 11, 492-511.
AUPHAN, N., DIDONATO, J.A., ROSETTE, C., HELMBERG, A. & KARIN, M. (1995). Immunosuppression by
glucocorticoids: inhibition of NF-kappaB activity through induction of IkappaB synthesis. Science 270, 286.
BANKSTAHL, J.P. & BANKSTAHL, M. (2012). Präklinische Positronen-Emissions-Tomographie-Studien in
Epilepsiemodellen. Zeitschrift für Epileptologie 25, 200-207.
BANKSTAHL, J.P., BANKSTAHL, M., KUNTNER, C., STANEK, J., WANEK, T., MEIER, M., DING, X.-Q., MÜLLER,
M., LANGER, O. & LÖSCHER, W. (2011). A Novel Positron Emission Tomography Imaging Protocol Identifies Seizure-Induced Regional Overactivity of P-Glycoprotein at the Blood–Brain Barrier. The Journal of Neuroscience 31, 8803-8811.
BANKSTAHL, J.P., KUNTNER, C., ABRAHIM, A., KARCH, R., STANEK, J., WANEK, T., WADSAK, W., KLETTER,
K., MÜLLER, M. & LÖSCHER, W. (2008). Tariquidar-induced P-glycoprotein inhibition at the rat blood–brain barrier studied with (R)-11C-verapamil and PET. Journal of Nuclear Medicine 49, 1328-1335.
BAR‐KLEIN, G., CACHEAUX, L.P., KAMINTSKY, L., PRAGER, O., WEISSBERG, I., SCHOKNECHT, K., CHENG,
P., KIM, S.Y., WOOD, L. & HEINEMANN, U. (2014). Losartan prevents acquired epilepsy via TGF‐β signaling suppression. Annals of Neurology 75, 864-875.

References
94
BARNES, P.J. (2006). Corticosteroid effects on cell signalling. European Respiratory Journal 27, 413-426.
BAiKAYA, M.K., MURALIKRISHNA RAO, A., DOĞAN, A., DONALDSON, D. & DEMPSEY, R.J. (1997). The
biphasic opening of the blood–brain barrier in the cortex and hippocampus after traumatic brain injury in rats. Neuroscience Letters 226, 33-36.
BAUER, B., HARTZ, A.M., FRICKER, G. & MILLER, D.S. (2005). Modulation of p-glycoprotein transport
function at the blood-brain barrier. Experimental Biology and Medicine 230, 118-127.
BAUER, B., SCHLICHTIGER, J., PEKCEC, A. & HARTZ, A.M. (2011). The Blood-Brain Barrier in Epilepsy. In
Clinical and Genetic Aspects of Epilepsy, pp. 23-54: Intech.
BEN-ARI, Y., LAGOWSKA, J., TREMBLAY, E. & LA SALLE, G.L.G. (1979). A new model of focal status
epilepticus: intra-amygdaloid application of kainic acid elicits repetitive secondarily generalized convulsive seizures. Brain Research 163, 176-179.
BERG, A.T., BERKOVIC, S.F., BRODIE, M.J., BUCHHALTER, J., CROSS, J.H., VAN EMDE BOAS, W., ENGEL,
J., FRENCH, J., GLAUSER, T.A. & MATHERN, G.W. (2010). Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 51, 676-685.
BERKOVIC, S.F., ANDERMANN, F., OLIVIER, A., ETHIER, R., MELANSON, D., ROBITAILLE, Y., KUZNIECKY, R.,
PETERS, T. & FEINDEL, W. (1991). Hippocampal sclerosis in temporal lobe epilepsy demonstrated by magnetic resonance imaging. Annals of Neurology 29, 175-182.
BERTORELLI, R., ADAMI, M., DI SANTO, E. & GHEZZI, P. (1998). MK 801 and dexamethasone reduce both
tumor necrosis factor levels and infarct volume after focal cerebral ischemia in the rat brain. Neuroscience Letters 246, 41-44.
BERTRAM, E.H. (2009). Temporal lobe epilepsy: Where do the seizures really begin? Epilepsy &
Behavior 14, 32-37.
BETZ, A.L., FIRTH, J.A. & GOLDSTEIN, G.W. (1980). Polarity of the blood-brain barrier: distribution of
enzymes between the luminal and antiluminal membranes of brain capillary endothelial cells. Brain Research 192, 17-28.
BIALER, M. & WHITE, H.S. (2010). Key factors in the discovery and development of new antiepileptic
drugs. Nature Reviews Drug Discovery 9, 68-82.
BLAMIRE, A. (2014). The technology of MRI—the next 10 years? The British Journal of Radiology 81,
601-617.
BOUILLERET, V., NEHLIG, A., MARESCAUX, C. & NAMER, I.J. (2000). Magnetic resonance imaging follow-
up of progressive hippocampal changes in a mouse model of mesial temporal lobe epilepsy. Epilepsia 41, 642-650.

References
95
BOUILLERET, V., RIDOUX, V., DEPAULIS, A., MARESCAUX, C., NEHLIG, A. & LA SALLE, G.L. (1999). Recurrent seizures and hippocampal sclerosis following intrahippocampal kainate injection in adult mice: Electroencephalography, histopathology and synaptic reorganization similar to mesial temporal lobe epilepsy. Neuroscience 89, 717-729.
BRADBURY, M.W.B. & LIGHTMAN, S.L. (1990). The blood-brain interface. Eye 4, 249-254.
BRAGIN, A., ENGEL, J., WILSON, C.L., VIZENTIN, E. & MATHERN, G.W. (1999). Electrophysiologic analysis
of a chronic seizure model after unilateral hippocampal KA injection. Epilepsia 40, 1210-1221.
BROWN, R.C., MARK, K.S., EGLETON, R.D., HUBER, J.D., BURROUGHS, A.R. & DAVIS, T.P. (2003).
Protection against hypoxia-induced increase in blood-brain barrier permeability: role of tight junction proteins and NFκB. Journal of Cell Science 116, 693-700.
CACHEAUX, L.P., IVENS, S., DAVID, Y., LAKHTER, A.J., BAR-KLEIN, G., SHAPIRA, M., HEINEMANN, U.,
FRIEDMAN, A. & KAUFER, D. (2009). Transcriptome profiling reveals TGF-β signaling involvement in epileptogenesis. The Journal of Neuroscience 29, 8927-8935.
CAMPOLO, M., AHMAD, A., CRUPI, R., IMPELLIZZERI, D., MORABITO, R., ESPOSITO, E. & CUZZOCREA, S.
(2013). Combination therapy with melatonin and dexamethasone in a mouse model of traumatic brain injury. Journal of Endocrinology 217, 291-301.
CANDELARIO‐JALIL, E., GONZÁLEZ‐FALCÓN, A., GARCÍA‐CABRERA, M., LEÓN, O.S. & FIEBICH, B.L. (2007).
Post‐ischaemic treatment with the cyclooxygenase‐2 inhibitor nimesulide reduces blood–brain barrier disruption and leukocyte infiltration following transient focal cerebral ischaemia in rats. Journal of Neurochemistry 100, 1108-1120.
CARSON, R.E. (2000). PET physiological measurements using constant infusion. Nuclear Medicine and
Biology 27, 657-660.
CHABARDÈS, S., KAHANE, P., MINOTTI, L., TASSI, L., GRAND, S., HOFFMANN, D. & BENABID, A.L. (2005).
The temporopolar cortex plays a pivotal role in temporal lobe seizures. Brain 128, 1818-1831.
CHANG, B.S. & LOWENSTEIN, D.H. (2003). Mechanisms of disease - Epilepsy. New England Journal of
Medicine 349, 1257-1266.
CHASSIDIM, Y., VAZANA, U., PRAGER, O., VEKSLER, R., BAR-KLEIN, G., SCHOKNECHT, K., FASSLER, M.,
LUBLINSKY, S. & SHELEF, I. (2015). Analyzing the blood–brain barrier: The benefits of medical imaging in research and clinical practice. Seminars in Cell & Developmental Biology 38, 43-52.
CHERRY, S.R. & DAHLBOM, M. (2004). PET: Physics, instrumentation, and scanners. In PET, pp. 1-124:
Springer.
CHERRY, S.R. & GAMBHIR, S.S. (2001). Use of Positron Emission Tomography in Animal Research.
ILAR Journal 42, 219-232.

References
96
CHOY, M., CHEUNG, K.K., THOMAS, D.L., GADIAN, D.G., LYTHGOE, M.F. & SCOTT, R.C. (2010). Quantitative MRI predicts status epilepticus-induced hippocampal injury in the lithium–pilocarpine rat model. Epilepsy Research 88, 221-230.
CORNFORD, E.M. & OLDENDORF, W.H. (1986). Epilepsy and the blood-brain barrier. Advances in
Neurology 44, 787-812.
CUCULLO, L., HALLENE, K., DINI, G., DAL TOSO, R. & JANIGRO, D. (2004). Glycerophosphoinositol and
dexamethasone improve transendothelial electrical resistance in an in vitro study of the blood–brain barrier. Brain Research 997, 147-151.
CURIA, G., LONGO, D., BIAGINI, G., JONES, R.S. & AVOLI, M. (2008). The pilocarpine model of temporal
lobe epilepsy. Journal of Neuroscience Methods 172, 143-157.
DAVID, Y., CACHEAUX, L.P., IVENS, S., LAPILOVER, E., HEINEMANN, U., KAUFER, D. & FRIEDMAN, A. (2009).
Astrocytic dysfunction in epileptogenesis: consequence of altered potassium and glutamate homeostasis? The Journal of Neuroscience 29, 10588-10599.
DEDEURWAERDERE, S., JUPP, B. & O'BRIEN, T.J. (2007). Positron emission tomography in basic
epilepsy research: a view of the epileptic brain. Epilepsia 48, 56-64.
DIJKHUIZEN, R.M. (2011). Advances in MRI-based detection of cerebrovascular changes after
experimental traumatic brain injury. Translational Stroke Research 2, 524-532.
DUDEK, F.E., CLARK, S., WILLIAMS, P.A. & GRABENSTATTER, H.L. (2006). Chapter 34 - Kainate-Induced
Status Epilepticus: A Chronic Model of Accuired Epilepsy. In Models of Seizures and Epilepsy. ed. MOSHÉ, S.L., PITKÄNEN, A. & SCHWARTZKROIN, P.A., pp. 415-432. Burlington: Academic Press.
DUFFY, B.A., CHUN, K.P., MA, D., LYTHGOE, M.F. & SCOTT, R.C. (2014). Dexamethasone exacerbates
cerebral edema and brain injury following lithium-pilocarpine induced status epilepticus. Neurobiology of Disease 63, 229-236.
ENGEL, J. (1996). Introduction to temporal lobe epilepsy. Epilepsy Research 26, 141-150.
ENGEL, J. (2006). Report of the ILAE classification core group. Epilepsia 47, 1558-1568.
ENGELHARDT, B. & COISNE, C. (2011). Fluids and barriers of the CNS establish immune privilege by
confining immune surveillance to a two-walled castle moat surrounding the CNS castle. Fluids and Barriers of the CNS 8, 4.
ENGLANDER, J., BUSHNIK, T., DUONG, T.T., CIFU, D.X., ZAFONTE, R., WRIGHT, J., HUGHES, R. &
BERGMAN, W. (2003). Analyzing risk factors for late posttraumatic seizures: a prospective, multicenter investigation. Archives of Physical Medicine and Rehabilitation 84, 365-373.
FABENE, P.F., MORA, G.N., MARTINELLO, M., ROSSI, B., MERIGO, F., OTTOBONI, L., BACH, S., ANGIARI, S.,
BENATI, D., CHAKIR, A., ZANETTI, L., SCHIO, F., OSCULATI, A., MARZOLA, P., NICOLATO, E., HOMEISTER, J.W., XIA, L., LOWE, J.B., MCEVER, R.P., OSCULATI, F., SBARBATI, A., BUTCHER, E.C. &

References
97
CONSTANTIN, G. (2008). A role for leukocyte-endothelial adhesion mechanisms in epilepsy. Nature Medicine 14, 1377-1383.
FISHER, R.S., BOAS, W.V.E., BLUME, W., ELGER, C., GENTON, P., LEE, P. & ENGEL, J. (2005). Epileptic
seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia 46, 470-472.
FRIEDMAN, A. (2011). Blood–brain barrier dysfunction, status epilepticus, seizures, and epilepsy: A
puzzle of a chicken and egg? Epilepsia 52, 19-20.
FRIEDMAN, A. & HEINEMANN, U. (2010). Role of blood–brain barrier injury in epileptogenesis. Epilepsia
51, 34-34.
FRIEDMAN, A., KAUFER, D. & HEINEMANN, U. (2009). Blood–brain barrier breakdown-inducing astrocytic
transformation: Novel targets for the prevention of epilepsy. Epilepsy Research 85, 142-149.
FUJIKAWA, D.G. (1996). The temporal evolution of neuronal damage from pilocarpine-induced status
epilepticus. Brain Research 725, 11-22.
GALANOPOULOU, A.S., BUCKMASTER, P.S., STALEY, K.J., MOSHE, S.L., PERUCCA, E., ENGEL, J., JR.,
LÖSCHER, W., NOEBELS, J.L., PITKÄNEN, A., STABLES, J., WHITE, H.S., O'BRIEN, T.J. & SIMONATO, M. (2012). Identification of new epilepsy treatments: issues in preclinical methodology. Epilepsia 53, 571-582.
GILAD, R., LAMPL, Y., EILAM, A., BOAZ, M. & LOYBERBOIM, M. (2012). SPECT-DTPA as a tool for
evaluating the blood–brain barrier in post-stroke seizures. Journal of Neurology 259, 2041-2044.
GLIEN, M., BRANDT, C., POTSCHKA, H., VOIGT, H., EBERT, U. & LÖSCHER, W. (2001). Repeated low-dose
treatment of rats with pilocarpine: low mortality but high proportion of rats developing epilepsy. Epilepsy Research 46, 111-119.
GOFFIN, K., DEDEURWAERDERE, S., VAN LAERE, K. & VAN PAESSCHEN, W. (2008). Neuronuclear
assessment of patients with epilepsy. Seminars in Nuclear Medicine 38, 227-239.
GOFFIN, K., VAN PAESSCHEN, W., DUPONT, P. & VAN LAERE, K. (2009). Longitudinal microPET imaging
of brain glucose metabolism in rat lithium-pilocarpine model of epilepsy. Experimental Neurology 217, 205-209.
GORTER, J.A., VAN VLIET, E.A. & ARONICA, E. (2015). Status epilepticus, blood–brain barrier disruption,
inflammation, and epileptogenesis. Epilepsy & Behavior 49, 13-16.
GREINER, W. & MÜLLER, B. (1994). Quantum Mechanics, vol. 2: Springer Science & Business Media,
233.
GRÖHN, O. & PITKÄNEN, A. (2007). Magnetic resonance imaging in animal models of epilepsy—
noninvasive detection of structural alterations. Epilepsia 48, 3-10.

References
98
GRÖHN, O., SIERRA, A., IMMONEN, R., LAITINEN, T., LEHTIMÄKI, K., AIRAKSINEN, A., HAYWARD, N., NAIRISMAGI, J., LEHTO, L. & PITKÄNEN, A. (2011). Multimodal MRI assessment of damage and plasticity caused by status epilepticus in the rat brain. Epilepsia 52, 57-60.
GRÖTICKE, I., HOFFMANN, K. & LÖSCHER, W. (2008). Behavioral alterations in a mouse model of
temporal lobe epilepsy induced by intrahippocampal injection of kainate. Experimental Neurology 213, 71-83.
GUO, Y., GAO, F., WANG, S., DING, Y., ZHANG, H., WANG, J. & DING, M.P. (2009). In vivo mapping of
temporospatial changes in glucose utilization in rat brain during epileptogenesis: An F-18-fluorodeoxyglucose-small animal positron emission tomography study. Neuroscience 162, 972-979.
GUPTA, S.C., PATCHVA, S. & AGGARWAL, B.B. (2013). Therapeutic roles of curcumin: lessons learned
from clinical trials. The AAPS journal 15, 195-218.
HAMILTON, S.E., LOOSE, M.D., QI, M., LEVEY, A.I., HILLE, B., MCKNIGHT, G.S., IDZERDA, R.L. &
NATHANSON, N.M. (1997). Disruption of the m1 receptor gene ablates muscarinic receptor-dependent M current regulation and seizure activity in mice. Proceedings of the National Academy of Sciences of the United States of America 94, 13311-13316.
HÄRTIG, W., BRUCKNER, G., HOLZER, M., BRAUER, K. & BIGL, V. (1995). Digoxigenylated primary
antibodies for sensitive dual-peroxidase labelling of neural markers. Histochemistry and Cell Biology 104, 467-472.
HAUSER, W., ATKINS, H., NELSON, K. & RICHARDS, P. (1970). Technetium-99m DTPA: A New
Radiopharmaceutical for Brain and Kidney Scanning 1. Radiology 94, 679-684.
HEDLEY‐WHYTE, E.T. & HSU, D.W. (1986). Effect of dexamethasone on blood‐brain barrier in the
normal mouse. Annals of Neurology 19, 373-377.
HEINEMANN, U., GABRIEL, S., JAUCH, R., SCHULZE, K., KIVI, A., EILERS, A., KOVACS, R. & LEHMANN, T.N.
(2000). Alterations of glial cell function in temporal lobe epilepsy. Epilepsia 41, 185-189.
HERMAN, S.T. (2002). Epilepsy after brain insult Targeting epileptogenesis. Neurology 59, 21-26.
HERSCHMAN, H.R. (2003). Micro-PET imaging and small animal models of disease. Current Opinion in
Immunology 15, 378-384.
HOLTMAN, L., VAN VLIET, E.A., APPELDOORN, C., GAILLARD, P.J., DE BOER, M., DORLAND, R., WADMAN,
W.J. & GORTER, J.A. (2014). Glutathione pegylated liposomal methylprednisolone administration after the early phase of status epilepticus did not modify epileptogenesis in the rat. Epilepsy Research 108, 396-404.
HONCHAR, M.P., OLNEY, J.W. & SHERMAN, W.R. (1983). Systemic cholinergic agents induce seizures
and brain damage in lithium-treated rats. Science 220, 323-325.

References
99
HSU, Y.H., LEE, W.T. & CHANG, C. (2007). Multiparametric MRI evaluation of kainic acid-induced neuronal activation in rat hippocampus. Brain 130, 3124-3134.
HUE, C.D., CHO, F.S., CAO, S., RDALER BASS, C.R., MEANEY, D.F. & MORRISON III, B. (2015).
Dexamethasone potentiates in vitro blood-brain barrier recovery after primary blast injury by glucocorticoid receptor-mediated upregulation of ZO-1 tight junction protein. Journal of Cerebral Blood Flow & Metabolism 35, 1191-1198.
IVANOVA, N., PECHLIVANOVA, D., TCHEKALAROVA, J., POPOV, D., MARKOVA, P. & STOYNEV, A. (2013).
Beneficial effects of chronic treatment with losartan on behavioural disturbances in kainate model of temporal lobe epilepsy. Comptes rendus de l'Académie bulgare des Sciences 66, 1761-1768.
IVENS, S., KAUFER, D., FLORES, L.P., BECHMANN, I., ZUMSTEG, D., TOMKINS, O., SEIFFERT, E.,
HEINEMANN, U. & FRIEDMAN, A. (2007). TGF-β receptor-mediated albumin uptake into astrocytes is involved in neocortical epileptogenesis. Brain 130, 535-547.
JAMES, M.L. & GAMBHIR, S.S. (2012). A molecular imaging primer: modalities, imaging agents, and
applications. Physiological Reviews 92, 897-965.
JANIGRO, D. (1999). Blood–brain barrier, ion homeostasis and epilepsy: possible implications towards
the understanding of ketogenic diet mechanisms. Epilepsy Research 37, 223-232.
JANIGRO, D., GASPARINI, S., D’AMBROSIO, R., MCKHANN II, G. & DIFRANCESCO, D. (1997). Reduction of
K+ uptake in glia prevents long-term depression maintenance and causes epileptiform activity. The Journal of Neuroscience 17, 2813-2824.
JIANG, J., WANG, W., SUN, Y.J., HU, M., LI, F. & ZHU, D.Y. (2007). Neuroprotective effect of curcumin on
focal cerebral ischemic rats by preventing blood–brain barrier damage. European Journal of Pharmacology 561, 54-62.
JUPP, B., WILLIAMS, J., BINNS, D. & HICKS, R. (2007). Imaging small animal models of epileptogenesis.
Neurology Asia 12, 51-54.
JUPP, B., WILLIAMS, J., BINNS, D., HICKS, R.J., CARDAMONE, L., JONES, N., REES, S. & O'BRIEN, T.J.
(2012). Hypometabolism precedes limbic atrophy and spontaneous recurrent seizures in a rat model of TLE. Epilepsia 53, 1233-1244.
KAAL, E.C. & VECHT, C.J. (2004). The management of brain edema in brain tumors. Current Opinion in
Oncology 16, 593-600.
KARLIK, S., STAVRAKY, R., TAYLOR, A., FOX, A. & MCLACHLAN, R. (1991). Magnetic resonance imaging
and 31P spectroscopy of an interictal cortical spike focus in the rat. Epilepsia 32, 446-453.
KASSNER, A. & THORNHILL, R. (2011). Measuring the integrity of the human blood–brain barrier using
magnetic resonance imaging. In The Blood-Brain and Other Neural Barriers, pp. 229-245: Springer.

References
100
KAYA, M., KALAYCI, R., KÜÇÜK, M., ARICAN, N., ELMAS, I., KUDAT, H. & KORKUT, F. (2003). Effect of losartan on the blood–brain barrier permeability in diabetic hypertensive rats. Life Sciences 73, 3235-3244.
KEITH L. BLACK, TIM CLOUGHESY, SUNG-CHENG HUANG, Y. PIERRE GOBIN, YUN ZHOU, JOHN GROUS,
GILLIAN NELSON, KEYVAN FARAHANI, CARL K. HOH & MICHAEL PHELPS. (1997). Intracarotid infusion of RMP-7, a bradykinin analog, and transport of gallium-68 ethylenediamine tetraacetic acid into human gliomas. Journal of Neurosurgery 86, 603-609.
KING, M., BRUGGEN, N.V., AHIER, R., CREMER, J., HAJNAL, J., WILLIAMS, S. & DORAN, M. (1991).
Diffusion‐weighted imaging of kainic acid lesions in the rat brain. Magnetic Resonance in Medicine 20, 158-164.
KLEIN, S., BANKSTAHL, M., GRAMER, M., HAUSKNECHT, M. & LÖSCHER, W. (2014). Low doses of ethanol
markedly potentiate the anticonvulsant effect of diazepam in a mouse model of difficult to-treat focal seizures. Epilepsy Research 108, 1719-1727.
KLEINSCHNITZ, C., BLECHARZ, K., KAHLES, T., SCHWARZ, T., KRAFT, P., GOBEL, K., MEUTH, S.G., BUREK,
M., THUM, T., STOLL, G. & FORSTER, C. (2011). Glucocorticoid insensitivity at the hypoxic blood-brain barrier can be reversed by inhibition of the proteasome. Stroke 42, 1081-1089.
KNAKE, S., HAMER, H.M. & ROSENOW, F. (2009). Status epilepticus: A critical review. Epilepsy &
Behavior 15, 10-14.
KNIGHT, R.A., KARKI, K., EWING, J.R., DIVINE, G.W., FENSTERMACHER, J.D., PATLAK, C.S. & NAGARAJA,
T.N. (2009). Estimating blood and brain concentrations and blood-to-brain influx by magnetic resonance imaging with step-down infusion of Gd-DTPA in focal transient cerebral ischemia and confirmation by quantitative autoradiography with Gd-[(14)C]DTPA. Journal of Cerebral Blood Flow and Metabolism 29, 1048-1058.
KNIGHT, R.A., NAGARAJA, T.N., EWING, J.R., NAGESH, V., WHITTON, P.A., BERSHAD, E., FAGAN, S.C. &
FENSTERMACHER, J.D. (2005). Quantitation and localization of blood-to-brain influx by magnetic resonance imaging and quantitative autoradiography in a model of transient focal ischemia. Magnetic Resonance in Medicine 54, 813-821.
KOEPPE, R.A. (2002). Data Analysis and Imaging Processing. In Principles and Practice of Positron
Emission Tomography. ed. WAHL, R.L., pp. 65-99: Lippincott Williams & Wilkins.
KORNBLUM, H.I., ARAUJO, D.M., ANNALA, A.J., TATSUKAWA, K.J., PHELPS, M.E. & CHERRY, S.R. (2000).
In vivo imaging of neuronal activation and plasticity in the rat brain by high resolution positron emission tomography (microPET). Nature Biotechnology 18, 655-660.
LAMPL, Y., SHMUILOVICH, O., LOCKMAN, J., SADEH, M. & LORBERBOYM, M. (2005). Prognostic
Significance of Blood Brain Barrier Permeability in Acute Hemorrhagic Stroke. Cerebrovascular Diseases 20, 433-437.
LAURILA, J.P., LAATIKAINEN, L.E., CASTELLONE, M.D. & LAUKKANEN, M.O. (2009). SOD3 Reduces
Inflammatory Cell Migration by Regulating Adhesion Molecule and Cytokine Expression. PLoS ONE 4, e5786.

References
101
LECCHI, M., OTTOBRINI, L., MARTELLI, C., DEL SOLE, A. & LUCIGNANI, G. (2007). Instrumentation and
probes for molecular and cellular imaging. The Quarterly Journal of Nuclear Medicine and Molecular Imaging 51, 111-126.
LEE, E.M., PARK, G.Y., IM, K.C., KIM, S.T., WOO, C.-W., CHUNG, J.H., KIM, K.S., KIM, J.S., SHON, Y.-M.,
KIM, Y.I. & KANG, J.K. (2012). Changes in glucose metabolism and metabolites during the epileptogenic process in the lithium-pilocarpine model of epilepsy. Epilepsia 53, 860-869.
LEITE, J., GARCIA-CAIRASCO, N. & CAVALHEIRO, E. (2002). New insights from the use of pilocarpine and
kainate models. Epilepsy Research 50, 93-103.
LIBRIZZI, L., REGONDI, M.C., PASTORI, C., FRIGERIO, S., FRASSONI, C. & DE CURTIS, M. (2007).
Expression of adhesion factors induced by epileptiform activity in the endothelium of the isolated guinea pig brain in vitro. Epilepsia 48, 743-751.
LIN, K.-J., LIU, H.-L., HSU, P.-H., CHUNG, Y.-H., HUANG, W.-C., CHEN, J.-C., WEY, S.-P., YEN, T.-C. &
HSIAO, I.-T. (2009). Quantitative micro-SPECT/CT for detecting focused ultrasound-induced blood–brain barrier opening in the rat. Nuclear Medicine and Biology 36, 853-861.
LÖSCHER, W. (2002). Animal models of epilepsy for the development of antiepileptogenic and disease-
modifying drugs. A comparison of the pharmacology of kindling and post-status epilepticus models of temporal lobe epilepsy. Epilepsy Research 50, 105-123.
LÖSCHER, W. (2003). Pharmakologische Grundlagen zur Behandlung der Epilepsie bei Hund und
Katze. Praktischer Tierarzt 14, 574-587.
LÖSCHER, W. & BRANDT, C. (2010). Prevention or Modification of Epileptogenesis after Brain Insults:
Experimental Approaches and Translational Research. Pharmacological Reviews 62, 668-700.
LÖSCHER, W. & POTSCHKA, H. (2005). Drug resistance in brain diseases and the role of drug efflux
transporters. Nature Reviews Neuroscience 6, 591-602.
LÖSCHER, W. & SCHMIDT, D. (2002). New horizons in the development of antiepileptic drugs. Epilepsy
Research 50, 3-16.
LOTHMAN, E. (1990). The biochemical basis and pathophysiology of status epilepticus. Neurology 40,
13-23.
LOWENSTEIN, D.H. (2009). Epilepsy after head injury: an overview. Epilepsia 2, 4-9.
MARCHI, N., ANGELOV, L., MASARYK, T., FAZIO, V., GRANATA, T., HERNANDEZ, N., HALLENE, K., DIGLAW,
T., FRANIC, L., NAJM, I. & JANIGRO, D. (2007a). Seizure-Promoting Effect of Blood–Brain Barrier Disruption. Epilepsia 48, 732-742.

References
102
MARCHI, N., FAN, Q., GHOSH, C., FAZIO, V., BERTOLINI, F., BETTO, G., BATRA, A., CARLTON, E., NAJM, I. & GRANATA, T. (2009). Antagonism of peripheral inflammation reduces the severity of status epilepticus. Neurobiology of Disease 33, 171-181.
MARCHI, N., GRANATA, T., FRERI, E., CIUSANI, E., RAGONA, F., PUVENNA, V., TENG, Q., ALEXOPOLOUS, A.
& JANIGRO, D. (2011a). Efficacy of Anti-Inflammatory Therapy in a Model of Acute Seizures and in a Population of Pediatric Drug Resistant Epileptics. PLoS ONE 6, e18200.
MARCHI, N., GRANATA, T., GHOSH, C. & JANIGRO, D. (2012). Blood–brain barrier dysfunction and
epilepsy: Pathophysiologic role and therapeutic approaches. Epilepsia 53, 1877-1886.
MARCHI, N., OBY, E., BATRA, A., UVA, L., DE CURTIS, M., HERNANDEZ, N., BOXEL‐DEZAIRE, V., NAJM, I. &
JANIGRO, D. (2007b). In vivo and in vitro effects of pilocarpine: relevance to ictogenesis. Epilepsia 48, 1934-1946.
MARCHI, N., TIERNEY, W., ALEXOPOULOS, A.V., PUVENNA, V., GRANATA, T. & JANIGRO, D. (2011b). The
etiological role of blood-brain barrier dysfunction in seizure disorders. Cardiovascular Psychiatry and Neurology 482415, 30.
MAROSO, M., BALOSSO, S., RAVIZZA, T., IORI, V., WRIGHT, C.I., FRENCH, J. & VEZZANI, A. (2011).
Interleukin-1 beta Biosynthesis Inhibition Reduces Acute Seizures and Drug Resistant Chronic Epileptic Activity in Mice. Neurotherapeutics 8, 304-315.
MATTSON, R.H., CRAMER, J.A. & COLLINS, J.F. (1992). A comparison of valproate with carbamazepine
for the treatment of complex partial seizures and secondarily generalized tonic–clonic seizures in adults. New England Journal of Medicine 327, 765-771.
MCMASTER, A. & RAY, D.W. (2007). Modelling the glucocorticoid receptor and producing therapeutic
agents with anti‐inflammatory effects but reduced side‐effects. Experimental Physiology 92, 299-309.
MCNAMARA, J.O. (1994). Cellular and molecular basis of epilepsy. The Journal of Neuroscience 14,
3413-3425.
MICHALSKI, D., GROSCHE, J., PELZ, J., SCHNEIDER, D., WEISE, C., BAUER, U., KACZA, J., GÄRTNER, U.,
HOBOHM, C. & HÄRTIG, W. (2010). A novel quantification of blood–brain barrier damage and histochemical typing after embolic stroke in rats. Brain Research 1359, 186-200.
MIRRIONE, M.M., SCHIFFER, W.K., SIDDIQ, M., DEWEY, S.L. & TSIRKA, S.E. (2006). PET imaging of
glucose metabolism in a mouse model of temporal lobe epilepsy. Synapse 59, 119-121.
NACER, A., MOVILA, A., BAER, K., MIKOLAJCZAK, S.A., KAPPE, S.H. & FREVERT, U. (2012).
Neuroimmunological Blood Brain Barrier Opening in Experimental Cerebral Malaria. PLoS Pathogens 8, e1002982.
NAG, S. & BEGLEY, D. (2005). Blood-brain barrier, exchange of metabolites and gases. Pathology and
Genetics. Cerebrovascular Diseases, 22-29.

References
103
NAGARAJA, T.N., NAGESH, V., EWING, J.R., WHITTON, P.A., FENSTERMACHER, J.D. & KNIGHT, R.A. (2007).
Step-down infusions of Gd–DTPA yield greater contrast-enhanced magnetic resonance images of BBB damage in acute stroke than bolus injections. Magnetic Resonance Imaging 25, 311-318.
NDODE-EKANE, X.E., HAYWARD, N., GROHN, O. & PITKANEN, A. (2010). Vascular changes in epilepsy:
functional consequences and association with network plasticity in pilocarpine-induced experimental epilepsy. Neuroscience 166, 312-332.
NEAL, K., SHAKERDGE, N., HOU, S., KLUNK, W., MATHIS, C., NESTEROV, E., SWAGER, T., MCLEAN, P. &
BACSKAI, B. (2013). Development and Screening of Contrast Agents for In Vivo Imaging of Parkinson’s Disease. Molecular Imaging and Biology, 1-11.
NEUMANN-HAEFELIN, T., WITTSACK, H.-J., FINK, G.R., WENSERSKI, F., LI, T.-Q., SEITZ, R.J., SIEBLER, M.,
MÖDDER, U. & FREUND, H.-J. (2000). Diffusion- and Perfusion-Weighted MRI: Influence of Severe Carotid Artery Stenosis on the DWI/PWI Mismatch in Acute Stroke. Stroke 31, 1311-1317.
NITSCH, C. & KLATZO, I. (1983). Regional patterns of blood-brain barrier breakdown during epileptiform
seizures induced by various convulsive agents. Journal of the Neurological Sciences 59, 305-322.
OBERMEIER, B., DANEMAN, R. & RANSOHOFF, R.M. (2013). Development, maintenance and disruption of
the blood-brain barrier. Nature Medicine 19, 1584-1596.
OBY, E. & JANIGRO, D. (2006). The Blood–Brain Barrier and Epilepsy. Epilepsia 47, 1761-1774.
PARDRIDGE, W.M. (2007). Blood–brain barrier delivery. Drug Discovery Today 12, 54-61.
PAUL, C. & BOLTON, C. (1995). Inhibition of blood-brain barrier disruption in experimental allergic
encephalomyelitis by short-term therapy with dexamethasone or cyclosporin A. International Journal of Immunopharmacology 17, 497-503.
PEREIRA, M., BECARI, C., OLIVEIRA, J., SALGADO, M., GARCIA-CAIRASCO, N. & COSTA-NETO, C. (2010).
Inhibition of the renin-angiotensin system prevents seizures in a rat model of epilepsy. Clinical Science 119, 477-482.
PERNOT, F., HEINRICH, C., BARBIER, L., PEINNEQUIN, A., CARPENTIER, P., DHOTE, F., BAILLE, V., BEAUP,
C., DEPAULIS, A. & DORANDEU, F. (2011). Inflammatory changes during epileptogenesis and spontaneous seizures in a mouse model of mesiotemporal lobe epilepsy. Epilepsia 52, 2315-2325.
PHELPS, M.E. (2000). Positron emission tomography provides molecular imaging of biological
processes. Proceedings of the National Academy of Sciences 97, 9226-9233.
PITKÄNEN, A. & LUKASIUK, K. (2009). Molecular and cellular basis of epileptogenesis in symptomatic
epilepsy. Epilepsy & Behavior 14, 16-25.

References
104
POZZILLI, C., BERNARDI, S., MANSI, L., PICOZZI, P., IANNOTTI, F., ALFANO, B., BOZZAO, L., LENZI, G., SALVATORE, M. & CONFORTI, P. (1988). Quantitative assessment of blood-brain barrier permeability in multiple sclerosis using 68-Ga-EDTA and positron emission tomography. Journal of Neurology, Neurosurgery & Psychiatry 51, 1058-1062.
RACINE, R.J. (1975). Modification of seizure activity by electrical stimulation: cortical areas.
Electroencephalography and Clinical Neurophysiology 38, 1-12.
RAOL, Y.H. & BROOKS-KAYAL, A.R. (2012). Experimental models of seizures and epilepsies. Progress
in Molecular Biology and Translational Science 105, 57-82.
RAVIZZA, T., NOÉ, F., ZARDONI, D., VAGHI, V., SIFRINGER, M. & VEZZANI, A. (2008). Interleukin converting
enzyme inhibition impairs kindling epileptogenesis in rats by blocking astrocytic IL-1β production. Neurobiology of Disease 31, 327-333.
REBELES, F., FINK, J., ANZAI, Y. & MARAVILLA, K.R. (2006). Blood-brain barrier imaging and therapeutic
potentials. Topics in Magnetic Resonance Imaging 17, 107-116.
RIAZI, K., GALIC, M.A. & PITTMAN, Q.J. (2010). Contributions of peripheral inflammation to seizure
susceptibility: cytokines and brain excitability. Epilepsy Research 89, 34-42.
RIBAN, V., BOUILLERET, V., PHAM-LE, B., FRITSCHY, J.-M., MARESCAUX, C. & DEPAULIS, A. (2002).
Evolution of hippocampal epileptic activity during the development of hippocampal sclerosis in a mouse model of temporal lobe epilepsy. Neuroscience 112, 101-111.
RIGAU, V., MORIN, M., ROUSSET, M.-C., DE BOCK, F., LEBRUN, A., COUBES, P., PICOT, M.-C., BALDY-
MOULINIER, M., BOCKAERT, J. & CRESPEL, A. (2007). Angiogenesis is associated with blood–brain barrier permeability in temporal lobe epilepsy. Brain 130, 1942-1956.
RIVEST, S., LACROIX, S., VALLIÈRES, L., NADEAU, S., ZHANG, J. & LAFLAMME, N. (2000). How the blood
talks to the brain parenchyma and the paraventricular nucleus of the hypothalamus during systemic inflammatory and infectious stimuli. Proceedings of the Society for Experimental Biology and Medicine 223, 22-38.
ROCH, C., LEROY, C., NEHLIG, A. & NAMER, IZZIE J. (2002). Magnetic Resonance Imaging in the Study
of the Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Adult Rats. Epilepsia 43, 325-335.
ROSELT, P., MEIKLE, S. & KASSIOU, M. (2004). The role of positron emission tomography in the
discovery and development of new drugs; as studied in laboratory animals. European Journal of Drug Metabolism and Pharmacokinetics 29, 1-6.
RUNGE, V.M., CLANTON, J.A., PRICE, A.C., WEHR, C.J., HERZER, W.A., PARTAIN, C.L. & JAMES JR, A.E.
(1985). The use of GD DTPA as a perfusion agent and marker of blood-brain barrier disruption. Magnetic Resonance Imaging 3, 43-55.
SAHA, G.B., MACINTYRE, W.J. & GO, R.T. (1994). Radiopharmaceuticals for brain imaging. Seminars in
Nuclear Medicine 24, 324-349.

References
105
SCHOKNECHT, K. & SHALEV, H. (2012). Blood–brain barrier dysfunction in brain diseases: Clinical
experience. Epilepsia 53, 7-13.
SCHWARZ, A.J., DANCKAERT, A., REESE, T., GOZZI, A., PAXINOS, G., WATSON, C., MERLO-PICH, E.V. &
BIFONE, A. (2006). A stereotaxic MRI template set for the rat brain with tissue class distribution maps and co-registered anatomical atlas: application to pharmacological MRI. NeuroImage 32, 538-550.
SCOTT, R., GADIAN, D., KING, M., CHONG, W., COX, T., NEVILLE, B. & CONNELLY, A. (2002). Magnetic
resonance imaging findings within 5 days of status epilepticus in childhood. Brain 125, 1951-1959.
SEIFFERT, E., DREIER, J.P., IVENS, S., BECHMANN, I., TOMKINS, O., HEINEMANN, U. & FRIEDMAN, A.
(2004). Lasting Blood-Brain Barrier Disruption Induces Epileptic Focus in the Rat Somatosensory Cortex. The Journal of Neuroscience 24, 7829-7836.
SERRANO, G., LELUTIU, N., ROJAS, A., COCHI, S., SHAW, R., MAKINSON, C., WANG, D., FITZGERALD, G. & DINGLEDINE, R. (2011). Ablation of cyclooxygenase-2 in forebrain neurons is neuroprotective and dampens brain inflammation after status epilepticus. The Journal of Neuroscience 31, 14850-14860.
SHAPIRA, Y., SETTON, D., ARTRU, A.A. & SHOHAMI, E. (1993). Blood-brain barrier permeability, cerebral
edema, and neurologic function after closed head injury in rats. Anesthesia & Analgesia 77, 141-148.
SHARMA, A.K., REAMS, R.Y., JORDAN, W.H., MILLER, M.A., THACKER, H.L. & SNYDER, P.W. (2007).
Mesial Temporal Lobe Epilepsy: Pathogenesis, Induced Rodent Models and Lesions. Toxicologic Pathology 35, 984-999.
SHARP, C.D., HOUGHTON, J., ELROD, J., WARREN, A., JACKSON, T., JAWAHAR, A., NANDA, A., MINAGAR, A.
& ALEXANDER, J. (2005). N-methyl-D-aspartate receptor activation in human cerebral endothelium promotes intracellular oxidant stress. American Journal of Physiology-Heart and Circulatory Physiology 288, 1893-1899.
SHIHAB, N., BOWEN, J. & VOLK, H.A. (2011). Behavioral changes in dogs associated with the
development of idiopathic epilepsy. Epilepsy & Behavior 21, 160-167.
SINGH, A., BELSHE, B.D. & GUMERLOCK, M.K. (1991). Radionuclide assessment of blood-brain barrier
disruption performed for chemotherapy of high grade malignant brain gliomas. International Journal of Radiation Applications and Instrumentation. Part B. Nuclear Medicine and Biology 18, 641-645.
SKOTLAND, T. (2012). Molecular imaging: challenges of bringing imaging of intracellular targets into
common clinical use. Contrast Media & Molecular Imaging 7, 1-6.
SLIVKA, A.P. & MURPHY, E.J. (2001). High-dose methylprednisolone treatment in experimental focal
cerebral ischemia. Experimental Neurology 167, 166-172.

References
106
SLOVITER, R.S. (2005). The neurobiology of temporal lobe epilepsy: too much information, not enough knowledge. Comptes Rendus Biologies 328, 143-153.
SLOVITER, R.S. & BUMANGLAG, A.V. (2013). Defining “epileptogenesis” and identifying
“antiepileptogenic targets” in animal models of acquired temporal lobe epilepsy is not as simple as it might seem. Neuropharmacology 69, 3-15.
SMITH-SWINTOSKY, V.L., PETTIGREW, L.C., SAPOLSKY, R.M., PHARES, C., CRADDOCK, S.D., BROOKE,
S.M. & MATTSON, M.P. (1996). Metyrapone, an Inhibitor of Glucocorticoid Production, Reduces Brain Injury Induced by Focal and Global Ischemia and Seizures. Journal of Cerebral Blood Flow & Metabolism 16, 585-598.
SMOLDERS, I., KHAN, G.M., MANIL, J., EBINGER, G. & MICHOTTE, Y. (1997). NMDA receptor-mediated
pilocarpine-induced seizures: characterization in freely moving rats by microdialysis. British Journal of Pharmacology 121, 1171-1179.
SPENCER, S.S. (1994). The relative contributions of MRI, SPECT, and PET imaging in epilepsy.
Epilepsia 35, 72-89.
SPENCER, S.S. (2002). When should temporal-lobe epilepsy be treated surgically? Lancet Neurology 1,
375-382.
SPERLING, M.R., FELDMAN, H., KINMAN, J., LIPORACE, J.D. & O'CONNOR, M.J. (1999). Seizure control
and mortality in epilepsy. Annals of Neurology 46, 45-50.
STABLES, J.P., BERTRAM, E., DUDEK, F.E., HOLMES, G., MATHERN, G., PITKÄNEN, A. & WHITE, H.S.
(2003). Therapy discovery for pharmacoresistant epilepsy and for disease-modifying therapeutics: summary of the NIH/NINDS/AES models II workshop. Epilepsia 44, 1472-1478.
STABLES, J.P., BERTRAM, E.H., WHITE, H.S., COULTER, D.A., DICHTER, M.A., JACOBS, M.P., LOSCHER,
W., LOWENSTEIN, D.H., MOSHE, S.L., NOEBELS, J.L. & DAVIS, M. (2002). Models for epilepsy and epileptogenesis: report from the NIH workshop, Bethesda, Maryland. Epilepsia 43, 1410-1420.
STANIMIROVIC, D.B. & FRIEDMAN, A. (2012). Pathophysiology of the neurovascular unit: disease cause
or consequence&quest. Journal of Cerebral Blood Flow & Metabolism 32, 1207-1221.
STEWART, A.M., DESMOND, D., KYZAR, E., GAIKWAD, S., ROTH, A., RIEHL, R., COLLINS, C., MONNIG, L.,
GREEN, J. & KALUEFF, A.V. (2012). Perspectives of zebrafish models of epilepsy: what, how and where next? Brain Research Bulletin 87, 135-143.
SUN, H., WU, H., YU, X., ZHANG, G., ZHANG, R., ZHAN, S., WANG, H., BU, N., MA, X. & LI, Y. (2015).
Angiotensin II and its receptor in activated microglia enhanced neuronal loss and cognitive impairment following pilocarpine-induced status epilepticus. Molecular and Cellular Neuroscience 65, 58-67.
SUZUKI, F., JUNIER, M.P., GUILHEM, D., SORENSEN, J.C. & ONTENIENTE, B. (1995). Morphogenetic effect
of kainate on adult hippocampal neurons associated with a prolonged expression of brain-derived neurotrophic factor. Neuroscience 64, 665-674.

References
107
TCHEKALAROVA, J. & GEORGIEV, V. (2005). Angiotensin peptides modulatory system: how is it
implicated in the control of seizure susceptibility? Life Sciences 76, 955-970.
TCHEKALAROVA, J., IVANOVA, N., PECHLIVANOVA, D., ILIEVA, K. & ATANASOVA, M. (2014a). Strain-
Dependent Effects of Sub-chronically Infused Losartan Against Kainic Acid-Induced Seizures, Oxidative Stress, and Heat Shock Protein 72 Expression. Cellular and Molecular Neurobiology 34, 133-142.
TCHEKALAROVA, J.D., IVANOVA, N.M., PECHLIVANOVA, D.M., ATANASOVA, D., LAZAROV, N., KORTENSKA,
L., MITREVA, R., LOZANOV, V. & STOYNEV, A. (2014b). Antiepileptogenic and neuroprotective effects of losartan in kainate model of temporal lobe epilepsy. Pharmacology Biochemistry and Behavior 127, 27-36.
TELLEZ‐ZENTENO, J.F., PATTEN, S.B., JETTÉ, N., WILLIAMS, J. & WIEBE, S. (2007). Psychiatric
comorbidity in epilepsy: a population‐based analysis. Epilepsia 48, 2336-2344.
TEMKIN, N.R. (2001). Antiepileptogenesis and Seizure Prevention Trials with Antiepileptic Drugs: Meta-
Analysis of Controlled Trials. Epilepsia 42, 515-524.
THOMPSON, C.J. (2002). Instrumentation. In Principles and Practice of Positron Emission Tomography.
ed. WAHL, R.L., pp. 48-64: Lippincott Williams & Wilkins.
TOFTS, P.S. & KERMODE, A.G. (1991). Measurement of the blood-brain barrier permeability and
leakage space using dynamic MR imaging. 1. Fundamental concepts. Magnetic Resonance in Medicine 17, 357-367.
TRAN, N.D., KIM, S., VINCENT, H.K., RODRIGUEZ, A., HINTON, D.R., BULLOCK, M.R. & YOUNG, H.F.
(2010). Aquaporin-1-mediated cerebral edema following traumatic brain injury: effects of acidosis and corticosteroid administration: Laboratory investigation. Journal of Neurosurgery 112, 1095-1104.
TURSKI, L., IKONOMIDOU, C., TURSKI, W.A., BORTOLOTTO, Z.A. & CAVALHEIRO, E.A. (1989). Review:
cholinergic mechanisms and epileptogenesis. The seizures induced by pilocarpine: a novel experimental model of intractable epilepsy. Synapse 3, 154-171.
TURSKI, W.A., CAVALHEIRO, E.A., BORTOLOTTO, Z.A., MELLO, L.M., SCHWARZ, M. & TURSKI, L. (1984).
Seizures produced by pilocarpine in mice: a behavioral, electroencephalographic and morphological analysis. Brain Research 321, 237-253.
TURSKI, W.A., CAVALHEIRO, E.A., SCHWARZ, M., CZUCZWAR, S.J., KLEINROK, Z. & TURSKI, L. (1983).
Limbic seizures produced by pilocarpine in rats: Behavioural, electroencephalographic and neuropathological study. Behavioural Brain Research 9, 315-335.
UEDA, Y., YOKOYAMA, H., NAKAJIMA, A., TOKUMARU, J., DOI, T. & MITSUYAMA, Y. (2002). Glutamate
excess and free radical formation during and following kainic acid-induced status epilepticus. Experimental Brain Research 147, 219-226.

References
108
VAN LANDINGHAM, K.E. & LOTHMAN, E.W. (1991). Self‐sustaining limbic status epilepticus. I. Acute and chronic cerebral metabolic studies: Limbic hypermetabolism and neocortical hypometabolism. Neurology 41, 1942-1942.
VAN VLIET, E., DA COSTA ARAUJO, S., REDEKER, S., VAN SCHAIK, R., ARONICA, E. & GORTER, J. (2007a).
Blood–brain barrier leakage may lead to progression of temporal lobe epilepsy. Brain 130, 521-534.
VAN VLIET, E.A., ARONICA, E. & GORTER, J.A. (2014a). Role of blood–brain barrier in temporal lobe
epilepsy and pharmacoresistance. Neuroscience 277, 455-473.
VAN VLIET, E.A., DA COSTA ARAÚJO, S., REDEKER, S., VAN SCHAIK, R., ARONICA, E. & GORTER, J.A.
(2007b). Blood–brain barrier leakage may lead to progression of temporal lobe epilepsy. Brain 130, 521-534.
VAN VLIET, E.A., OTTE, W.M., GORTER, J.A., DIJKHUIZEN, R.M. & WADMAN, W.J. (2014b). Longitudinal
assessment of blood–brain barrier leakage during epileptogenesis in rats. A quantitative MRI study. Neurobiology of Disease 63, 74-84.
VANLANDINGHAM, K.E., HEINZ, E.R., CAVAZOS, J.E. & LEWIS, D.V. (1998). Magnetic resonance imaging
evidence of hippocampal injury after prolonged focal febrile convulsions. Annals of Neurology 43, 413-426.
VEZZANI, A. & BARAM, T.Z. (2007). New Roles for Interleukin‐1 Beta in the Mechanisms of Epilepsy.
Epilepsy Currents 7, 45-50.
VEZZANI, A., FRENCH, J., BARTFAI, T. & BARAM, T.Z. (2011). The role of inflammation in epilepsy. Nature
Reviews Neurology 7, 31-40.
VEZZANI, A. & FRIEDMAN, A. (2011). Brain inflammation as a biomarker in epilepsy. Biomarkers in
Medicine 5, 607-614.
VEZZANI, A. & GRANATA, T. (2005). Brain inflammation in epilepsy: experimental and clinical evidence.
Epilepsia 46, 1724-1743.
VOLK, H. & LODERSTEDT, S. (2011). Neuigkeiten in der Behandlung von Epilepsie bei Hund und Katze.
Kleintierpraxis 16, 649-664.
VOLK, H.A., MATIASEK, L.A., LUJÁN FELIU-PASCUAL, A., PLATT, S.R. & CHANDLER, K.E. (2008). The
efficacy and tolerability of levetiracetam in pharmacoresistant epileptic dogs. The Veterinary Journal 176, 310-319.
WATERHOUSE, R.N. (2003). Determination of lipophilicity and its use as a predictor of blood–brain
barrier penetration of molecular imaging agents. Molecular Imaging & Biology 5, 376-389.
WHITE, H.S. & LÖSCHER, W. (2014). Searching for the Ideal Antiepileptogenic Agent in Experimental
Models: Single Treatment Versus Combinatorial Treatment Strategies. Neurotherapeutics, 1-12.

References
109
WIESER, H.-G. (2004). ILAE Commission Report. Mesial temporal lobe epilepsy with hippocampal
sclerosis. Epilepsia 45, 695-714.
WUNDER, A., SCHOKNECHT, K., STANIMIROVIC, D.B., PRAGER, O. & CHASSIDIM, Y. (2012). Imaging blood-
brain barrier dysfunction in animal disease models. Epilepsia 6, 14-21.
YEN, C.K. & BUDINGER, T.F. (1981). Evaluation of blood-brain barrier permeability changes in rhesus
monkeys and man using 82Rb and positron emission tomography. Journal of Computer Assisted Tomography 5, 792-79.