Embed Size (px)
Citation preview

FRACTURES E. H. HAMBLY
:: :il:i :';·' ·····:··': ·'··:
'':i'··:·:
':···'·:·:
i:i
' ':"
":::·
:"
··ii::
.:·-·.
C:'::·::;::: :i· ··I
:·:··:···
::·
il:frii..:i iiii..: ::;::i
:' i:,::
ii:i
:"'':·'·
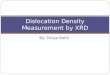
FIG. I.-Perthes disease.
liPikiiiiij ics.·iQi'%;iEtl:.:.·IIEe::.·:::::::::·:::::s;:·:;··;6:·:.`
i··:·.·
.ii;··n·i·i·.·
:n::;::··.·
ii:iil·:l··:·
'::: :'itiEI,:l·::· ··:
IZ::'·:.:··:···::i..:::
IWiilf:r;&·'::··:·
illiC;aii:.·.··ieii·il ·:::·····::
···-·;:.*:e:::::.·::i:::.::..·. .·i..i;9$:":'i'c:':' :· '··
::i:::·::....:.·:... ...i·:ii·:·iti:·:·::::r·:··:::;..·'ilijnBLI.L·lllslll.iL.ibiij::. :i::i::··:· .··i:
liil·:':
::,:,::.i·.%· .: .: :i: :· :· :·..:··:..·:·.
··F;:i:·:i::·:··:··:·"":'·:·:··'·li.::· ICil8:Si%i:;::.iiiii
ei..w:n:azw:Ri..:iai:ii·;:· ·i:;i
iililiisi;!iCisiiFit ira.:.· ·li.ii.ii;iilifiiiiiiiioa'·::a:i9i:.:··::··:·i::e:w -.I:··
.Lii.i6:ISZCiliillBli:iiiPiP';iiiiiii p::e::·:·:::·::.c:*:*::::.::i::. ::i:.-::BIIII..IZii.ZiRCi:ii::iidiiii:::ilJ 181C:::·il·i·;i:ii:$:8ill%iiiiiil::iiiiiiiSZII .iilil··i:·l
;iR. B!.f6EfB·.B'fP.;··;···· ,itilil:iiiii.ifi.il$!igi.igl,sb::i::·i. .......:E::'::;li:l::.::::::·::,:ililiJI I··:··::::::::.··i·i··i·. ·i··:··8':":":'·''·i :·:·······:·· ·:··:·(iIlbil$::·· ······ ··:s:i·;. :I.::·ii:::.':::::i·ii.:ii:iil:.IR·:· L8iiii'··i':
;i: '':'·i''.c'di·,ii.5.is.a.t.s.ai..i.:· ·:·:I.d.gE.I&IBk&.I...*p."-a.'ji.'.'.L.5.!; .I.C .:gL:pl.isi):).
i;ii·'i Ililii;iliiiiQi'fif'i. 1:. :lii::l:.'ii··i:.::: ::··I....:::::·: i.:. :· ··.·:· :a:s:
i· ··.·l··hiZlg i': :e:u:l:,:·
Idia il.iLIcililL dililPliii:;'·l·i·.:.··.iilLi.iiSi..iili.iS:.::: ::: :iriLCihLli.li.ikd.i;iiEI·:·::··::r:::,·.·····;.::s.·.r·:·.·· ·.:·
li.i.i..i..iiji.l;ii.Ei:''':::;':·Li:a:::*.::·:El:gilgliCiCB''":"llliliiX.:l,..p.......i..iiiiii.Wi:jjjl.j.i.:·'··";l:';i:ii·i8i:'·:iY:::::i·;:·;:·.· ·····:·
·..'i·i:!diiigi"l%F'i"iTI::::·r:::-::Y:iai:" '.·..·.iii.isi:i;iiii.i.'..i...!.fii.i..ii.i·:;I:B::9:s::i.·.6:al:a:ibi·r·:···. i.:.··.··
18iiL.:..i9ijiii.dlliRiiiilZii.ii.ii:.i:6i:li:!ijgi:iiil.
.;..lsic:alii'le:::l::::::ii:lsitii::ai:i:.iiiiilii5i.il$:i.:.iiiilSPi%i:i:i;:i::':'"::i'': ·····'l'i:::::·ii·"'' ··.9::i:::(.::g:.·;:ir::WLV:';'::l·:-:I-131:iiiiii;::;li::':i:::lf';i:i.i:·:.·'· .I·::i·::::4ii;.i;i.....i.;.i....ia..:.i iiii.iilL..:i::.'·i··: "':··":':"::":" iii.j.· BiijrC.iZIilLiRiE.
.'9.3.s...%:i6i:;·.
ifiii5liicii:.Il.il0ii:illi3i·:I'···
iii'·Wiliililli9iiLllltiBjj.ii.. G:;i .;·.··
LPPilfiSiii;i:i·li'l'.'· ···f.Pih:i:. .':'···':·:':i·:ii.··I';i'Rliii3iX19.ffIli.iEaii·i···::· ·:·:i'ii:i'''l·'.il4:i;iidFELiID
-,:c:vsiliieil:il::i:-:··:·'·:·
·I;::::. :i·::··la::i:i·iiil.I.,;l·i:'i·.i·:i·:"iB'iCB:iHiPI:i::i"i::::::::·i·i·S5iBi:-iliiiiil.i.::'iliie:::·.·····:gii.ii.l2i2.ifii.ii.ii:::i(:i:::lei::': ":'(·:: .:·
il·:··.'·· :··'I': I:·;D.i.L.:.:a·:-:····:·:····:··:·r:··:i·L:·6::.·1::::.:·;:.'.'I."''e·l··:,:l,·.?:iPi:.'i:i::;:::::'-:··;:·:':::·'i::·: .::.·· ...i'lii.::i:liiii:IBiliiiii.i.!iilii;.i:; :'' ':'; ';·I·:. :i5'.:.:''i:!:l:::iI::::::iBLi'#i.
:··:i· ·:::iiiiil·i:;i:illailii:i·i·l·iljli''ilefiii.ii;il:il:liii.i:il::ii:i:li·:l
`.::.::·'··llili:':I··l:iiiiiii:Wi
·li: iijlliiiidi"i
.LitrglCis·
ikiRl·rs.ie:ldl·· ;.'l:.·:·l·i·:::.:·.· .·:.:··· :··l:i:i:i:
·I: ii.i::·
···.·:.'i.lf.:::iiiiiiii Gi9illilj.il.iiili!iQ6filBlilg:··;···;····:··:·:···;a·;·a
·::iiL- fii i.isi:iiisles
iii.iii:iii:ll'::b::;:::::I·:16:'F:Fi·:::a::r:e :4···i:i.::::::':illi;illii8Fyli.iai.:·':iSi'din I::6lilii;.iidi:liiiiilR::i::..:":."":"··· .·:·::·:I:·;:·-;:
iS.ii8i!iidiili.iii.iQ9ili$iX.iitiiijiil:ii.iiiil'Si;itii:::i::is:,i
·ilLCillli6iiI'i ;I·i.:·' ·'·::l.i:':i:::::·:::ii:.:::,ii:;`i:`ri;
:iiirsil:liisRii:i..:.i.iiiil·::!figl·i::··
..ii:l:.iiiiiii:ii.ij.j.i:::lii.i'l.fi%i2.C%ii.a icipl:··l::·
j.j.l%i:':·; ···gsie:·:;·.-
li.I:.".p.""""".s"B"""".lllsls1..;...a.i:a
::-::·:·;:.·.··
www·:;·:·
li··:'·.
riii.i..!.ll i·:··:i:::,:lii;iiaaaPili.:""i ji%Ili.isi%ri
:1::I·:
i·:·.:·...
:w·.·
:.:a:;·I:··
FIG. 2.-(top right) Slipped femoral epiphysis.
FIG. 3.--bottom left) Traumatic dislocation of thehip in a boy, aged 8.
FIG. 4.-(middle right) Intra-trochanteric fractureof the neck of femur.
FIG. 5.-(bottom right) Abduction fracture of neckof femur.
by copyright. on M
ay 26, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.21.239.272 on 1 S
eptember 1945. D
ownloaded from

FRACTURES E. H. HAMBLY
:··:·i::::·i·i
:j.::li :·:·····I.,., ::8:·r:·:::.:.:;.·,·,;··:i iiiiiliIiiilliiil!:ii:i·.:iii liilii.:":b::.:ll:H
:·:r;a :I:r::··:
·:··:::::r::' ·..·..:.:'::-:
·i· ::::::i'l
··i:··::.:ili:K:k:
·''·'·':''
.: I ··;··:;·i;:i.s·I· ·:·l:·iii9iBiZ
··: ·:;·il:·:;;:;·;·:,i
·:l:··:.·i··li;:
il:jf'id·i·i:··:·;:·i:;·;: :· :·:
:i""J i··:·::·::·..·.··.:I::. ':I":' ·i··i·ii
:I.r
·:·:·:·'''liii.ilil% 'H
·;··;:· :·-:·
'·''·'·:'·:"
:'*
Y:l":"·':
i:·
Eif;iit
": ':'':::::':'':'i.i:··:isi;·il!iiiiib':'':
:··.·:':pr.:I .r:· ·:·;··:··'··.:: ·:::·..:.i:.: :I:::::.'i:'i:li8i.eiaiaiii.iif·ir·: ''' ·:'·:·;:·:··i·:l:il,·,,;,.,l.ia,,,l,···,······;sia:,i
·i···-·::·:C: ·i··i··:··:·l:·l·iyi:(i:.:·:·:·i:·:;·:··::l:.:8::t;r··*·r·I·:
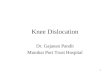
FIG. 6.-Adduction fracture bf neck of femur.
FIG. 7.-(right) Asepticnecrosis of the neck ofthe femur secondary tounsatisfactory insertior,of Smith-Petersen nail.
·:·
:·'l.i;i :'''''"': ·'
.:.i·I .:..:. :.··i;:::'i ·;·::- ····· --· :::··:··:.·.·:· ·I.iii::':';':''":'······'·-' ·:· ':;'.·.li::[l'i:::r::·.r::: :.:·:·'.:''·:'"'· :· ···':. ·i· ·:··:::::· 'd:iii
::I:·'·'·"····":::::::::::::':::.:.;.·. ··:·'.:' .:.':·:.·'··:·. ·.::.:··;'·::i:·· ·I.'·.·:;:::::i·:··':.'·:· :'···:·i..·:·.·":" :.:···:i:·.:· i····:i.. ...: I·::·.
':''":':':''
I':
' ';'
:ici
i..:·.:I
":'·:·
.·.·lil"'
··: ·. . :::
';'' ': ':
...:::I:::::.····:··.·`'
:;j::.:: :i:iii:j:i'i:···'·i···::'iii.:'·:·':
"::
..: ::.·::· .·1:1·1 ·:· :·: :··.:I·;···:·:li:,.:i:.l: ·:·..·:;·i:.::.:·:··:·:··I····I··:·:·:::··:a::.-:,.:..i·. ........ .:.:· :I:·;il::E;:igiil.E.iiiii;.ii.il6ii.II:·';il:$ii...i.iQ:.::. :.:;:i:,:l:lii::'i":··';::· ····
.:..:::::::.ltl:a: ': :::': "''' ::..::·::·:.:;a:a:·:·-w::r;::a
·.· ··· :::'::i:·BiiLiJ.·· ·:· .·. ·.··.:.::s:i.::.-d:iIigil:8:Hi
··:::isia:
izi.iai.liiii.iiliiIiiHii8i.II. ::iiBiCii·iliP$ZiEiii:iijii.i:ri.l.ii..ii.is.si.t li.i.ii.ii:i.iilii.iii.i%iLi8ii.li.i8sii$i.iL ·::::::i:::·:···:·;··:- p:.il''?i'i4iiE'.Z.LiPi ::·i;·ii
I·
i5ii·ili'li:l:l.i:i··i··i·::::::irr!I -iiifii.i.i.i
II: ii:i·;:·.:::::i:':::I:l..l:;l.l..l.'li...jii'l:. ;;:il:jjiijii:iilljI;iii:iiiiiil;;li:i·:·· I:···· :r ·:i!::niar:l: ·:I·:::··I i:l··l:iiii!iiil:i:jili:c:' i:·i··:: :::·:::·::·:::··:··::.:i:i.:i.;i.i.:i:ji:·.· :::i:i·lil.il.ii::iI··::··:··:·:;·i·'::iii:ii: ·I:.lii;:lili:%:ir:il :I:.l:i·:::::l:·l::iii.iii:i::li :, i;l'e ·i:;:;:l:;iiiiiii'·'::''':'""::':'I::liiliiiiiiifiliiiii:i·:iji·li:·iii;iiiilii;iii.iifiieiiBi·I:::::i::::a:i:il:a:v
·::··::
.ii'.iiiiil.iif:.·li·ii:ii·i':iiiliii:Z lii:: ·: iil,li.iillil;ii$j.iiiiii.''" '····':'':'
e::!::g:: '' ''''''' '''''''.ii:li;,ii:ii'd:i'i'·i'il'liiliiiiil:ii:iiliiiiiii;iiiiiiiiliriil:
..... ·.··:rv· ·· ···················:·: :::eff.I ...'.: Wp··-:··:·I:·.···-·;·····::-l::,::,·i::i.\.:p·i.i::·:; :··:.::.··:·:··:-·:··· ···-·:.:·.·
a:-.::ri i:i:'':'··'·'·'·'*;;.Pi'.
'"'"'5iI''':;':''
::::
:a;·,::.: i: i:"97'di'.'.
iii ··· ··: ·i· ·· .·. ·:s:i"ils:ia:
illi :.;.::,:;,;::.:.:.: ri:i.:l;:i:r::i::::::.;:::::··:i;
:::::· ::.: ..JIBI ..... ....;.1.:.. .:..
"::.:::;1::":.:::ii:i8i:I:18lilli:·.:.iZLi.ilaiiiilLiilii,iiiiii;iiliii'iii;;:;:;;
FIG. 8.-Unsatisfactory insertion of Smith-Petersen naildue to failure to take X-rays at every stage of the
operation.
FIG. 9.-(right) Fracture of mid-shaft of the femur whichis already the site of Paget's disease.
.:::··:··:·::-::·
:·:.·:··` .,a.snrs.sa.m.b.rspssrs....iaii;l:,.'··:·
:··:·
:··:·:·:·:
····:··:
··i:'::''i:;··;'·1"1'
··i
:·
I:
I
i·
::::i
.i
ilii."":'
·:'
by copyright. on M
ay 26, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.21.239.272 on 1 S
eptember 1945. D
ownloaded from

FRACTURES E. H. HAMBLY
.... .....
:oo:~iiioiiiii xiioW'1:-ziz
.,'-....'.... :.
:::ii j·:ii?!:]::::~:· ·:i!}1 ·i~::!:::
- i.
...' ..I~i .ii:i ·l I:i.li
.' ~3."..:::: :. :,.
l:.:.::?:
i: ..;.:.Z::i: Z' ··: :..:..·..':'"··:'..
~~~~~~· Z';:.:'":..;iii'Z`'iii.:'l·l
--.:-:.....
.N '::. .;; °ili': :''::.:l '-·::i
~8!!o qW!:'!:?;~i ·:. '"'.·.:
~~~~pgii: l,L:·.B..,B=°..'...
';. .:::iliit3 litii1; . .. ,
,.[.:,l::a:.58'!:,:::B:.Z':.:... .
.· ·m .....;..B
is:isi··ii:ii..
;.-i:?::;:
iI.ii:
i.isILi·i:
:i
i··:
i·..;.sssps.l
iii::;i
":
":;;·
iTiQ:8
1'1
·r$l -.21t.ll·.·.9.$"'l.it:":I·r. ...a.i
6:.assa.i-·r
il·i
I·:i
FIG. IO.-(top left) Compound fractures of the mid-shafts of the tibia and fibula.
FIG. ii.-(top right) Third degree abduction frac-ture-dislocation of the ankle joint.
FIG. I2.-(bottom right) Complete fracture dislocationof the ankle joint. This type of case is usually
reduced easily.
FIG. I3.-(bottom left) Fracture of the os calcisinvolving the sub-astragaloid joint.
by copyright. on M
ay 26, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.21.239.272 on 1 S
eptember 1945. D
ownloaded from

FRACTURES E. H. HAMBLY
r;·"·.:i
lil·IL···r
.::*·;·
Ci;kl.li.Chilii9.;;i:'' '''':":;
FIG. I4.-Fracture of the os calcis.
i?l:·····i
ii.sii.gii.i
$p%j;ii::i·::
I:·l:·i:·l:·:.pl"::::8:S.
ii:i·i:··:e·······::" i·..sai::9
···::":I·:'':i::i;.L.aaslllPIO.I
i%:':'·:··i*:;:.:· I··:· :···!i::·l:· i····
.:-:,I:·;···:
;:.:": :···;·i
':'''':':' i:l
FIG. I5.-Fracture of the body of the astragaluswith sub-astragaloid dislocation and dislocation of
the body of the astragalus.
FIG. I6.-Avulsion fracture of the neck of the astragalus seearrow.
FIG. I7.-Rupture of the external lateral ligament of theankle joint. X-rays should be taken with the ankle in full
invertion.
by copyright. on M
ay 26, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.21.239.272 on 1 S
eptember 1945. D
ownloaded from

September, I945 FRACTURES 277
3. MACLEOD, J., and HOTCHKISS, R.S., Am. J. Obst. & Gynae, 46,424, 1943.
4. MICHELSON, L., Cal and West Med., 58, 67, I943.5. POMMERENKE, W. T., West. J. Surg. Obst. & Gynae, 52, 1944.6. POPENHOE, PAUL J., Heredity, 34,, 83, 1943.7. TITUS, P., J.A.M.A., 105, 1257, I943.8. REYNOLDS, S. R. M. Physiology of the Uterus. Hamish Hamilton,
I939.9. WILLIAMS, W. W. Connecticut State Med. J., Aug. I943.
FRACTURES OF THE LOWER LIMB
By E. H. HAMBLY, F.R.C.S.(Surgeon E.M.S. Royal National Orthopaedic
Hospital, W.I)Fractures Involving the Hip JointThe hip joint is peculiarly affected by injury
throughout life from the nature of its position andfunction.
In the child the chief injuries of this joint arePerthes disease and slipping of the femoral epi-physis. Perthes disease, which occurs in boysbetween the ages of four to ten, is an asepticnecrosis of the head of the femur. This is secondaryto injury in which the blood supply to the femoralhead is cut off. See X-Ray, No. i. Treatment con-sists in absolute rest in bed with strapping extensionuntil the femoral head regains its full circularcontour. This usually takes from eighteen monthsto two years.
Slipping of the epiphysis of the head of thefemur occurs between the ages of twelve tofourteen and is commoner in girls. It is frequentlya bilateral condition and is associated with thefat type of pituitary disordered child. Diagnosis isconfirmed by taking X-rays in the "lithotomy"position. Treatment consists of rest in bed inextension and full abduction until the head ofthe femur has fused to the neck. (See X-ray No. 2.)
In adults traumatic dislocation of the hip jointis not uncommon. It may be associated with afracture of the acetabulum. Central fractures ofthe acetabulum are described in the next articleupon fractures of the pelvis. Sciatic paralysisassociated with dislocations of the hip are alwaysof poor prognosis. Thirty per cent of dislocatedhips show avascular necrosis with secondarygross osteoarthritis. The head of the femur maybe dislocated anteriorly or posteriorly.
Clinically, posterior dislocation of the hip putsthe leg into abduction and internal rotation.Treatment consists of reduction of the head byflexing the hip at the same time as abducting andexternally rotating it. This is best done with thepatient on the floor.The second type of dislocation anteriorly pre-
sents itselt witn one leg externany rotatea anaabducted. Reduction is performed by flexion,abduction, and internal rotation of the hip at thesame time lifting the head into the acetabulum.
Following reduction, all dislocations of the hipshould be immobilised in a plaster spica to preventre-dislocation, and to allow the torn ligaments toheal, and also to minimise myositis ossificans. Ifthe margin of the acetabulum is fractured as wellthe dislocated hip is best treated on an abductionframe. (See X-ray No. 3.)
Fracture of the Neck of the FemurA great deal of literature has already accumu-
lated upon this fracture, but the treatment isstill far from satisfactory. Fractures of thefemoral neck may be classified clinically into threegroups. They are inter-trochanteric fractures,trans-cervical fractures which do well with nailing,and thirdly, those which do not.
Inter-trochanteric fractures always unite easilywithout operation. (See X-ray No. 4.) Theseshould be treated by rest in bed in full abductionto prevent the otherwise inevitable coxa vara.External rotation is prevented by a plaster up tothe knee to which is fixed a transverse wooden barbehind the calf.
Trans-cervical fractures unite easily with nailingin some cases, and with great difficulty in others.The first type, which unite easily are abductionfractures. (See X-ray No. 5.) If these are impactedno operation is necessary. They should be treatedby rest, but it is important to X-ray them regularlyin the first few weeks in case they become dis-impacted. If they do so they should be treatedby the insertion of a Smith-Petersen nail.The third group, which do not unite easily, are
adduction fractures. (See X-ray No. 6.)In this type of fracture the fracture line is more
vertical than horizontal and thus more likely toslide. Also there is no impaction. Treatmentconsists in the insertion of a Smith-Petersen nailand non-weight bearing for twelve weeks.A vitallium nail should always be used as
stainless steel ones slip out. The writer prefersthe almost "blind" method with a two-inch incisionto the more complicated Hey-Groves, Engel-May,Eric Lloyd, and other methods. The human handis extremely accurate in the insertion of the guide-wire after practice. X-rays should be taken atall stages of the operation, i.e. after reduction,insertion of guide wire, insertion of nail and afterimpaction. (See X-ray Nos. 7 and 8.)
Fractures of Shaft of FemurThese may be classified into three anatomical
types, sub-trochanteric, middle two-thirds of shaft,
by copyright. on M
ay 26, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.21.239.272 on 1 S
eptember 1945. D
ownloaded from

POST-GRADUATE MEDICAL JOURNALand supra-condylar fractures. All of these arevery difficult to treat if perfect anatomical align-ment is required, and this must be the ideal resultof treatment to be aimed at. (See X-ray No. 9.)
In sub-trochanteric fractures the proximal frag-ment is abducted by the glutaei and flexed byilio-psoas, and the distal fragment is abductedby the abductor muscles. If the proximal frag-ment is not flexed sub-trochanteric fractures arebest treated on a Jones abduction frame. Onthe other hand, if the proximal fragment is flexedimmobilisation is maintained by a Thomas splint,with a Pearson knee flexion adjustment, and aSteinman pin through the head of the tibia.Alternatively, a well-leg traction splint is eminentlysatisfactorily for this type of fracture. Thisenables the patient to sit up at the same timeabducting and flexing the hip and maintainingthe injured femur on traction.For fractures of the middle two-thirds of the
femoral shaft the essential aim is to maintain thefull length of the limb. At the same time rotationand angulation must be prevented. Furthermore,it is essential to reduce the fracture within thefirst few days. This must be done under deepanaesthesia and not by weights on an extension.The purpose of weight extension is only to maintainthe reduction once attained by manipulation.Thus a general anaesthetic, either by inhalationor by intra-venous pentothal, is preferable to alocal anaesthetic. The latter tends to dilute thefracture haematoma and there is the constantrisk of introducing infection.There are two main methods of fixation of a
fracture of the mid-shaft of the femur. Theseare fixed traction and balanced traction.
In the former method of fixed traction, three-inchwide elastoplast strips are fixed with soft bandage,.and not by adhesive strapping, on either side ofthe leg and thigh. The outer strip lies behindthe mid-line and the inner strip anterior to the mid-line to correct external rotation. The knee jointis kept slightly flexed and two thirds of the thighare maintained in front of the side stems of theThomas splint with leather slings. A gutter splintis applied from the upper thigh to below the calfposteriorly. The side strips are fixed to the endof the Thomas splint, which is itself tied to theend of the tilted bed. Immobilisation is thusmaintained until union has occurred in abouttwelve weeks. A calliper and cloth shoe is thenworn for three months. Quadriceps drill is under-taken from three weeks after the fracture andactive exercises three weeks after union hasoccurred. Passive exercises are harmful.The second method for the treatment of fractures'
of the mid-shaft of the femur is by balancedtraction. In this method extension is maintained
by a Steinman pin through the head of the tibia,to which a weight of fourteen pounds is attached.The fracture must first be reduced under a deepanaesthetic. The leg is then placed in a Thomassplint with a Pearson's knee flexion adjustment.This is fixed to a Balkan beam. The foot of thebed is raised twelve inches. Flexion of the kneeshould be in the region of thirty degrees. Activemovements commence gently from the beginningand are further increased when the fracturebecomes firm.The writer has tried both methods, but prefers
the latter method of balanced traction. Thismethod tends to give less residual stiffness of theknee joint. It is essential that the leg be adjusteddaily by one experienced in the treatment of suchfractures.From time to time it is impossible to effect
reduction of such a fracture by manipulationunder anaesthesia. This is due to the inter-vention of muscles and soft tissues between thebone ends. Open reduction by operation isrequired immediately. It is harmful to try andreduce the fracture by prolonged heavy traction.The operation should be undertaken with theIoo per cent "no touch" technique. The boneends are placed in position and the wound closed.The leg is placed in a Thomas splint as describedabove. Fixation by plates or bone grafts isunnecessary and in some cases harmful on accountof the risk of sepsis or the fact that a bone platemay easily keep the fractured ends apart.
Infected Fractures of Shaft of FemurInfected compound fractures of the femur are
surgical problems of the first magnitude. How-ever, with the use of penicillin and sulphanilamides,and wide incision of the wound and immobilisationin a "closed plaster", union always occurs. Theincision wound through all layers of the tissuesshould be about twelve inches long. The infectedfracture haematoma is drained. No fascial normuscle layer is sutured. The wound is lightlypacked with gauze, which should be in one lengthand its measurements noted so that none is leftbehind on removal. A plaster spica is applied,which is splint in front and which incorporates atibial pin. The plaster is changed after a monthor six weeks when the smell is no longer bearable.Excoriation of the skin by the discharging pus isprevented by covering the wound edges and sur-rounding skin with vaseline gauze or "tulle gras".Before the plaster is changed the tibial pin shouldbe fixed to the fraction table. The plaster ischanged from time to time. It is, however, kepton as a complete hip spica until full union isobtained. This may take six months or more.
278 Septe·mber, x945by copyright.
on May 26, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.21.239.272 on 1 Septem
ber 1945. Dow
nloaded from

September, I945As Watson-Jones has pointed out, non-union isa complication of the past.
"Un-United" Fractures of the FemoralShaftFractures of the shaft of the femur which are
regarded as un-united are best treated with a five-inch onlay tibial graft fixed with four vitalliumscrews. The screws must penetrate to the oppositecortical layer of compact bone. Full "no touch"technique is essential. The bone graft is liableto fracture itself from the eighth to the twelfthweeks. All onlay grafts should be completelyimmobilised in plaster until strong bony union isobtained.
Supra-Condylar Fractures of the FemurThese are most difficult to reduce. There is no
doubt that the best and easiest reduction iseffected immediately after the injury under deepanaesthesia. Delay of a few days appears tomake full reduction almost impossible.
Reduction is maintained by a tibial pin withthe leg on a Thomas splint with knee flexionadjustment and a weight of ten pounds.Watson-Jones has devised a method of re-
duction and immobilisation. This is by verticaltraction with a pin through the lower femoralfragment, and horizontal traction through thehead of the tibia. These are incorporated in aplaster spica. He has had satisfactory resultswith this method, but the danger appears to liein the insertion of the femoral pin. If it is insertedtoo high infection is not unlikely in the fracturehaematoma, and if too low, in the knee joint.Mild infection is common with Steinman pins andis due to their rotation in their tracks. This isminimised by incorporation of the pins in theplaster spica.
T- and Y-Shaped Fractures of the FemoralCondylesAlthough these fractures appear very serious in
the X-rays they unite readily when immobilisedon a Thomas splint with pin or skin traction. Itis of value to aspirate the haemarthrosis.
Fracture of One Femoral CondyleThese are treated with a Thomas splint and
pin or skin traction. Operative reduction andfixation with a vitallium screw may be necessary.
Displacement of Lower FemoralThe lower femoral epiphysis is usually displaced
anterior to the lower end of the shaft. Thegastrocnemius flexes the epiphyseal fragment.There is danger of thrombosis of the poplitealvessels due to stretching over the lower marginof the shaft.
This type of injury is relatively easy to treat.It is reduced by manipulation under anaesthesiaby traction and flexion of the knee to a rightangle. An anterior plaster shell with the knee inthis position maintains the reduction.
Injuries to the KneeFrom the terms of reference of this article only
fractures are considered. These include fracturesof the patella, the tibial spine, and tibial tuberosity,and Schlatter's disease.
Fracture of the PatellaFractures of the patella are in every case,
where there is a stellate fracture or transversefracture with separation, best treated by excisionof the patella. Exceptions to this rule are fissurefractures with minimal separation, and polar ones.In the latter instance it may be necessary to excisethe polar fragment.
Fracture of the Tibial SpineThis is associated with avulsion of the anterior
cruciate ligament, and occurs between the agesof ten and twenty. The best treatment is theconservative one. The knee is plastered for six toten weeks in ten degrees of flexion.
Fractures of the Tibial TuberosityThis is quite distinct from Schlatter's disease.
Usually no treatment is necessary. The writerhas been forced to excise two cases of un-unitedfractures of the tibial tuberosity, which gave riseto pain.Avulsion of the Tibial Epiphysis
In these cases operative repair with catgutpassed through holes in the fragment and in thetibia is necessary if the fragment is completelyavulsed. When the fragment is partially attachedmanipulation is sufficient.
Osgood-Schlatter's DiseaseThis is a common condition in which there is
aseptic necrosis of the tibial tuberosity. Treat-
FRACTURES 279by copyright.
on May 26, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.21.239.272 on 1 Septem
ber 1945. Dow
nloaded from

POST-GRADUATE MEDICAL JOURNALment consists of plaster with the knee straightfor two months.
Fractures of the TibiaFractures of the Head of the Tibia
Fractures of the external tibial tuberosity are oftwo types. (See Diagrams Nos. I and 2.)The first type is one in which the outer femoral
condyle smashes its way through the outer tibialcondyle like a wedge. The cruciate ligamentsare torn and the external semi-lunar cartilage isdriven into the head of the tibia. The outlook isbad for this type as severe osteoarthritis is inevi-table. Treatment consists of reduction underanaesthesia and immobilisation for three months.The main fragment is manipulated and the smaller
fragments are crushed into position with a Bohlertype of clamp. An arthrodesis may be necessaryif pain and stiffness persist.The second type of injury shows an oblique
injury right through the joint. There is a tearof the internal lateral ligament, with a depressedfracture of the external tibial tuberosity, and afracture of the neck of the fibula. This prognosisis good. Treatment consists of reduction withstrong traction and immobilisation for twelve weeksin plaster with quadriceps drill.
Fracture of the Medial Tuberosity of theTibiaThis is a not uncommon injury. The best
treatment is to keep the patient in bed and togive him active movements and quadriceps drillfrom the beginning. Alternatively, operative re-duction and fixation with a bone peg may beundertaken with removal of the ruptured internalsemi-lunar cartilage.
Fractures of the Shaft of the TibiaGreenstick fractures of the tibia in children
require immobilisation in plaster for twelve weeksto prevent angulation.
In adults, fractures of the tibial shaft are easyto treat provided the surgeon is prepared toaccept one half of an inch shortening in the case ofoblique fractures. If full length and full anato-mical correction are required great risks have tobe undertaken. Either the fracture must betreated by some form of distraction apparatuswith the risk of delayed or non-union. Alterna-tively, open operation and fixation with vitalliumscrews must be undertaken. This involves a riskof infection of the fracture haematoma.The writer thus prefers to reduce the fracture
by manipulation under deep anaesthesia with theaid of a pin through the os calcis or the lowerend of the tibia. The reduction is maintained ina plaster up to the groin with the knee flexed toforty degrees. The pin is incorporated in theplaster and removed after six weeks. Watson-Jones has devised an excellent tibial tractionapparatus for the purpose of reduction of suchfractures.
Rigid claw toes are prevented by flexion exercisesand moulding the plaster to fit the concave trans-verse arch. The plaster is kept on right up tothe groin until the fracture is united.
Un-United Fractures of the TibiaSlow or delayed union of the tibia are best
treated by freshening of the bone ends and drilling.Alternatively, and especially if sclerosis is present,a sliding graft is required. In every case a full-length plaster to the upper thigh is necessaryuntil union has occurred.
Infected Compound Fractures of theTibiaThis is a serious surgical problem. (See X-ray
No. Io.) The secret of success lies in completeand prolonged immobilisation of the fracture andcomplete drainage of the infected haematoma.This type of injury is thus treated best by theWinnett-Orr-Trueta "closed plaster" technique.The wound is widely opened and gently packedwith vaseline gauze. The surrounding skin is alsocovered with vaseline gauze to prevent excoriationby pus. Penicillin and chemotherapy are indicated.A padded plaster with no windows is applied.Some surgeons prefer to have a window over thewound, but this is not essential. If necessary,sequestrectomy is performed after two monthsand is done gently with a scalpel and dissecting
280 September, r945by copyright.
on May 26, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.21.239.272 on 1 Septem
ber 1945. Dow
nloaded from

September, I945forceps only. At the earliest opportunity a skingraft is applied if the loss of skin is severe. Arectangular flap from the other calf with thelonger side as the base is useful. The plaster ischanged after six weeks and repeatedly if thedischarge of pus is severe. A full plaster is kepton until strong union has occurred. This maytake twelve months or longer.Fractures of the Fibula
Fractures of the neck and shaft of the fibulaonly require a light walking plaster or evenelastoplast.Fracture-Dislocations of the AnkleAbout go per cent of such injuries are of the
Pott's abduction fracture-dislocation type. Theastragalus is displaced outwards and backwardsand is tilted outwards. There may be a fractureof one or both malleoli. These are divided intofirst, second, and third- degree types. (See X-rayNos. ii and I2.)
It is important to realise that a first-degreeinjury must be treated just as seriously as third-degree ones. Treatment of an abduction fracture-dislocation consists of reduction under deepanaesthesia. The heel and astragalus are pressedforwards and rotated inwards. A plaster to theknee with the heel in full inversion is applied. Noweight-bearing is permitted for six weeks in thecase of first-degree injuries. A walking plaster isthen worn for three weeks and an elastoplastbandage for a further three weeks. In the caseof third-degree injuries the patient must not bearweight until union has occurred.Abduction fracture-dislocations of the ankle are
treated similarly. Vitallium screws are beingincreasingly employed for fractures of the malleoli,especially of the medial, the "anterior", and the"posterior" malleoli. These methods are still ontrial.
Fractures of the Os CalcisFractures of the os calcis have been classified
at great length by many writers. (See X-rayNos. I3 and I4.) There is profound disagreementabout the best methods of treatment. The writerprefers to put the patient to bed for twelve weeks.Active movements and radiant heat are com-menced from the first day. Valgus insoles arerequired afterwards on account of pes plano-valgusdeformity. Plaster causes stiff and painful feet.
Fractures of the AstragalusFractures of the neck of the astragalus may
occur without displacement or with sub-astragaloid
dislocation or with dislocation of the body of theastragalus backwards. (See X-ray No. I5.)
In the latter two types the dislocation is reducedunder deep anaesthesia or even by open operation.The foot is plastered in equinus. The maincomplication is aseptic necrosis of the body ofthe astragalus. This may require arthrodesis ofthe sub-astragaloid joint and even of the anklejoint. The X-ray No. I5 is that of a patienttreated by the writer. The body of the astragaluswas dislocated completely. Although this wasreduced back into the ankle joint under anaesthesia,it was not possible to fully correct the dislocationat the sub-asfragaloid joint and to bring the neckof the astragalus into good apposition with thebody. A triple arthrodesis was performed at onceand the patient has done well.
Fracture of the Tarsal ScaphoidIf the scaphoid is fractured into two halves
immediate astragaloscaphoid arthrodesis is indi-cated.
Fractures of the MetatarsalsThese are easily treated by a well-moulded
walking plaster for six weeks. Flexion movementsof the toes must be encouraged from the beginning.
Fracture of the PhalangesA collodion gauze dressing and immediate weight
bearing in a walking plaster or a boot with thetoe-cap cut out and fitted with a metatarsal bar,is the best treatment for comminuted fractures ofthe phalanges. In the case of the big toe it maybecome necessary to arthrodese the inter-phalangealjoint.
3.
Operation devised by writer in which half of the peroneuslongus tendon threaded through the,external malleolus and
the os calcis, and back again on itself.
(Published by kind permission of the British MedicalJournal).
FRACTURES 281by copyright.
on May 26, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.21.239.272 on 1 Septem
ber 1945. Dow
nloaded from

282 POST-GRADUATE MEDICAL JOURNAL September, I945
Recurrent Dislocation of the AnkleRecurrent dislocation is frequently due to
rupture of the external lateral ligament of theankle joint. Diagnosis is confirmed by X-ray ofthe ankle in full inversion after the injection ofnovocaine into the region of the external lateralligament. (See X-ray No. I7.)The writer has devised an operation for the
repair of this ruptured ligament. The PeronaeusLongus tendon is split longitudinally from abovedownwards and left attached at the lower end ofthe wound. The free half of the tendon is threadedthrough the external malleolus and the os calcisand sutured back on itself. (See diagram No. 3.)
BOOK REVIEWSPHYSICAL MEDICINE IN GENERAL PRACTICEPublished by Dr. WILLIAM BIERMAN. Medical Books.
Price 37s.It is a little difficult for me to entirely comprehend
for which type of practitioner this book is written, althoughit is dedicated to the practitioner in general practice in theUnited States of America, certainly no practitioner in thiscountry could deal with the many technical problemsraised in this book, whereas from a physical medicinespecialist's point of view the book is very unbalanced.There is very little detail about electrical apparatus.There is too much on experimental pathology, yet notenough on the actual mechanical details of giving physicaltreatment. The chapter on massage is extremely sketchilydone. The illustrations throughout the book are ex-tremely mediocre and disappointing and there is a markedabsence of pictures illustrating electrical apparatus. Thechapters on the Application of Physical Medicine to theVarious Systems and Diseases is very helpful, but is hardlyfull enough.
TEXTBOOK OF MEDICINE7th edition
Edited by J. J. CONYBEARE, M.C., D.M., F.R.C.P. Living-stone. Pp. I,I64. Price 30s.A textbook which has reached its seventh edition in
sixteen years neither needs the reviewer's praise nor fearshis criticism. Its success is assured, and the chief functionof the reviewer is to suggest any further improvementsthat might be introduced in the future.Among the duties of every teacher is that of advising
his students as to the textbooks they should buy, and thisis ever a difficult problem. One common suggestion isthe purchase initially of a "smaller" textbook-withinwhich class "Conybeare" is usually included-followedlater by a larger book, or by a number of books devotedto individual systems. It is far from certain that thisis good advice; indeed, there is a real danger that under-graduates may read too deeply in systematic medicine.Nevertheless, there is certainly great need for a basic book,containing neither too little nor too much for the averagestudent's needs. "Conybeare" goes far towards meetingthis requirement, although with a little judicious pruning,or the introduction of some system of type distinctionseparating the essential from the non-essential, it wouldapproximate still more closely to' the ideal.An alternative approach would be to include an intro-
ductory note on the reading of systematic medicine.Using this particular book, the student might be advised
to read certain small sections as eaily as possible-forexample the first fifteen pages of Renal Diseases and thefirst fifteen pages of Nervous System. Thereafter, fora considerable period, he should read diseases only as hesees them clinically, and it is convenient to tick them offin the contents as they are read; full tabulated contents,as printed in this book, are ideal for this purpose. When atlast the time comes to systematise his work, the bulk ofthe ground has already been covered. Some printingdistinction might well be made in the contents to indicatewhich sections must be studied, irrespective of whetherthey have been encountered clinically or not, and whichsections are included for the sake of completeness.The special features of "Conybeare," as compared with
its contemporaries, are that it is a comparatively compactand elementary account of the subject, although it iscompletely adequate for all ordinary examination andpractice requirements. It is particularly to be recom-mended to those who prefer the narrative to the tabulativestyle.
PSYCHOLOGY AND PSYCH[OTH. RAPY5th edition
By WILLIAM BROWN. Edward Arnold & Co., London.1944. Price 14S.The fifth edition of this popular classic by the Wilde
Reader in Mental Philosophy and Director of the Instituteof Experimental Psychology in the University of Oxford,the last edition of which was published in I940 and re-printed a year later, contains two new chapters. InChapter xi the author maintains that in all normal peoplethe sexual instinct can be adequately controlled withoutthe slightest danger to health. Chapter xvii, "The Psy-chology of Modern Germany," all the more valuable ascoming from one who knew the old Germany and realisedhow great was her intellectual and artistic contributionto modern civilisation, should be read by politicians,legislators, historians, educationists, and social workers.Hitler is described in a penetrating study as the greatestparanoiac in history, or at least the most paranoid rulerof modern times. In the last chapter the problems andfindings of psychical research are fascinatingly andsympathetically discussed.Those who do not always agree with the views expressed
by the author will, nevertheless, find this monographintensely readable throughout, delighting in its elegant,lucid, forceful style.Could not Dr. Brown be persuaded in the next edition
to add a new chapter on Courage ?
CLINICAL ASPECTS OF SEPSIS IN GUNSHOTWOUNDS
By A. V. MELNIKOV. Medical Publications Ltd., I945.Price 15s.This monograph by Col. A. V. Melnikov, Consulting
Surgeon, Red Army Medical Services, will be welcomedby many British surgeons, though the translation fromthe Russian original of I943 is somewhat too literal andtends to be cumbersome. The first 72 pages describegeneral facts concerning sepsis, while the remaining103 pages deal with the individual organs and tissues, andwith surgical, medicinal, and other forms of treatment.Sulphonamide therapy and blood transfusion are dis-cussed in a page each, and vitamin treatment is dismissedin 25 lines. Chapter xvi is devoted to peculiarities ofsepsis in relation to regional anatomy: pelvic wounds,fractured femur, multiple arthritis of foot, etc. Thereis no bibliography and no index, but the case-histories areinteresting and valuable.The appearance of further monographs from the U.S.S.R.
in this series is looked forward to-in a happier translation,it is hoped.
by copyright. on M
ay 26, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.21.239.272 on 1 S
eptember 1945. D
ownloaded from















![Anatomy Of A Bodyof Ethics Complianceand Requirements 2010[1]](https://img.dokumen.tips/doc/110x75/54c4b5cc4a795943038b456f/anatomy-of-a-bodyof-ethics-complianceand-requirements-20101.jpg)