Embed Size (px)
Citation preview

ICCS e-Newsletter CSI Fall 2014UniPath - Denver, CORichard Quinones, MLS(ASCP)
Hong Lin, PhDCristina McLaughlin, MD

2
PresentationClinical History• 67-year-old female with history of T-prolymphocytic leukemia (T-PLL).• Originally presented in 2010 with leukocytosis, anemia, thrombocytopenia, peripheral
lymphadenopathy and massive splenomegaly.• Currently status post second allogeneic stem cell transplant, after multiple rounds of
treatment with anti-CD52 antibody (Campath; alemtuzumab).– First transplant with matched related donor in 2013 after first relapse.– Second transplant with matched unrelated donor in 2014 after 2 extramedullary relapses.
Specimens Submitted for Analysis• Bone marrow for 60-day evaluation post second transplant.
– Peripheral blood received in EDTA for morphology.– Bone marrow aspirate received in EDTA for morphological and molecular testing.– Bone marrow aspirate received in NaHep for flow cytometry and cytogenetics.– Two trephine needle core biopsies of bone marrow (0.6cm and 0.8cm in length by 0.4cm each in diameter)
received in B+ for fixation and decalcification.
• Subsequent soft tissue biopsy of a right neck mass for flow cytometry.• Follow-up peripheral blood for morphology and flow cytometry.

3
Flow Cytometric AnalysisInstrumentation• Acquired on Beckman Coulter Gallios 10 Color Flow Cytometer• Analyzed using Beckman Coulter Kaluza Software, Version 1.2
Tubes Acquired (on all 3 specimens)
Panel Markers (FITC/PE/ECD/PC5.5/PC7/APC/AF700/AF750/PB/KrO)
Tube 1 Kappa Lambda CD23 CD38 CD34 CD20 CD10 CD19 CD5 CD45
Tube 2 CD8 CD2 CD7 CD3 CD34 CD56 CD16 CD4 CD5 CD45

BONE MARROW FINDINGS60 days post second transplant

5
Peripheral Blood Count at time of BMParameter Result Unit Normal Range
WBC 4.7 103/μL 4.5-11.0
RBC 3.09 106/μL 4.10-6.00
HGB 9.8 g/dL 14.0-18.0
HCT 28.4 % 40.0-54.0
MCV 91.7 fL 79-101
MCH 31.6 pg 28.0-34.0
MCHC 34.5 g/dL 32.0-36.0
RDW 17.5 % 11.5-14.7
PLT 111 103/μL 150-400
6
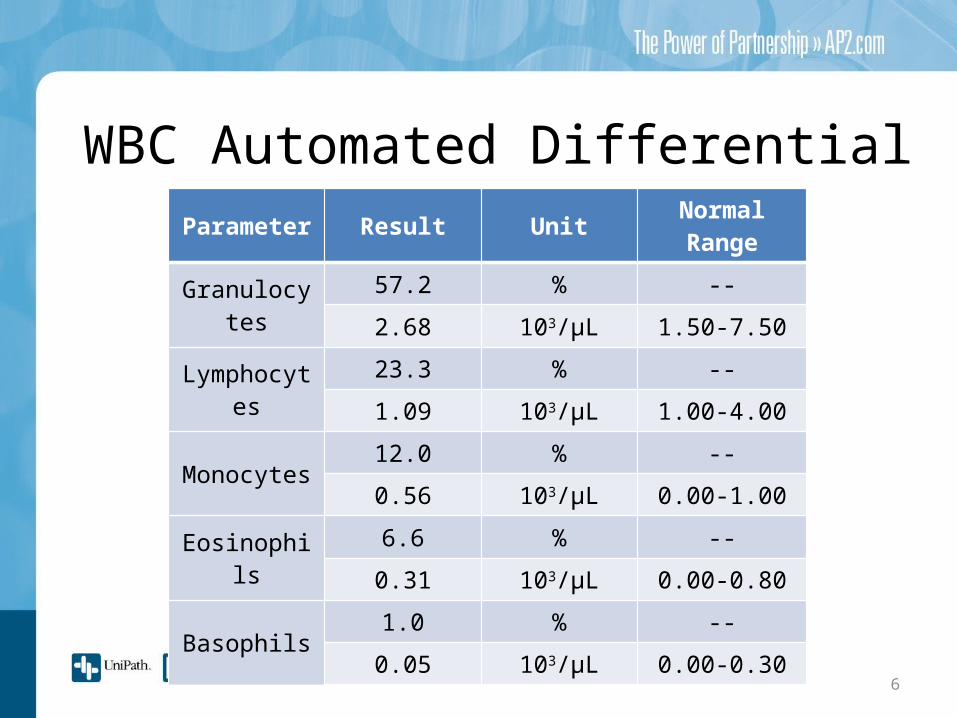
WBC Automated DifferentialParameter Result Unit Normal Range
Granulocytes57.2 % --
2.68 103/μL 1.50-7.50
Lymphocytes23.3 % --
1.09 103/μL 1.00-4.00
Monocytes12.0 % --
0.56 103/μL 0.00-1.00
Eosinophils6.6 % --
0.31 103/μL 0.00-0.80
Basophils1.0 % --
0.05 103/μL 0.00-0.30

7
Bone Marrow DifferentialParameter Result Unit Normal Range
Blast 1.50 % 0.1-1.7
Promyelocyte 1.50 % 1.9-4.7
Maturing Myeloid Cells 52.75 % 28.8-52.7
Lymphocytes 10.50 % 8.6-23.8
Monocytes 3.50 % 0.1-0.6
Eosinophils 7.50 % 0.4-7.4
Basophils 0.25 % 0.0-0.2
Plasma Cells 1.00 % 0.0-3.5
Erythroid Cells 21.50 % 13.9-37.3
M/E Ratio 3.1:1 -- 2.1-4.1

8
Morphology - Bone MarrowAspirate• There is trilineage hematopoiesis with maturation. Myeloid and erythroid
lineages show no evidence of dysplasia. No increase in blasts. No lymphoid or plasma cell aggregates.
• Iron staining demonstrated markedly increased storage iron with decreased iron utilization. No ring sideroblasts were noted.
Particle Prep• Rare interstitial and perivascular aggregates of small, mature lymphocytes
which show slight/moderate nuclear irregularities, condensed chromatin, and scant cytoplasm.
Core Biopsy• Patient exhibits normal cellularity of 30-40%. Bone trabeculae are
appropriate.

The particle preparation shows an interstitial aggregate of small, mature lymphocytes with nuclear irregularities, condensed chromatin, and scant cytoplasm (blue arrows). Immunostains show the lymphocytes are positive for CD3, CD2, CD4, with rare CD8 positive T cells and rare CD20 positive B cells.
Morphology - Bone Marrow

10
Flow Data - Bone Marrow - Tube 1CD45 vs Side Scatter plot shows normal distribution of lymphocytes, monocytes, granulocytes, dim CD45 population and debris. The Blymphocytes are clearly polyclonal with no expression of CD5.
Non-B-lymphocytes
B-lymphocytes
Polyclonal B-lymphocytes
Non-B-lymphocytes
B-lymphocytes
Bright light blue= B cellsBlue= T cells

11
Flow Data - Bone Marrow - Tube 2The abnormal T lymphocyte population, which represents 0.57% of total events (shown in maroon), expresses partial CD2, CD5, CD7, CD4, bright CD45; and is negative for CD3, CD8, CD16 and CD56.
Maroon=abnormal T cellsBlue= normal polytypic T cellsGold= NK cells
Polytypic T cells NK cells

12
Cytogenetic Studies - Bone MarrowChromosome Analysis• Patient shows a normal karyotype.
FISH• A dual color assay using a break
apart translocation probe for the human T-cell receptor alpha/delta (TCRAD) was performed.
• 3.3% of cells analyzed post transplant were positive for the TCRAD rearrangement at the 14q11 locus.

RIGHT NECK MASS
Patient developed an increasingly uncomfortable and rapidly growing right neck mass. Needle core biopsy with flow cytometry analysis was performed one week after the bone marrow biopsy.
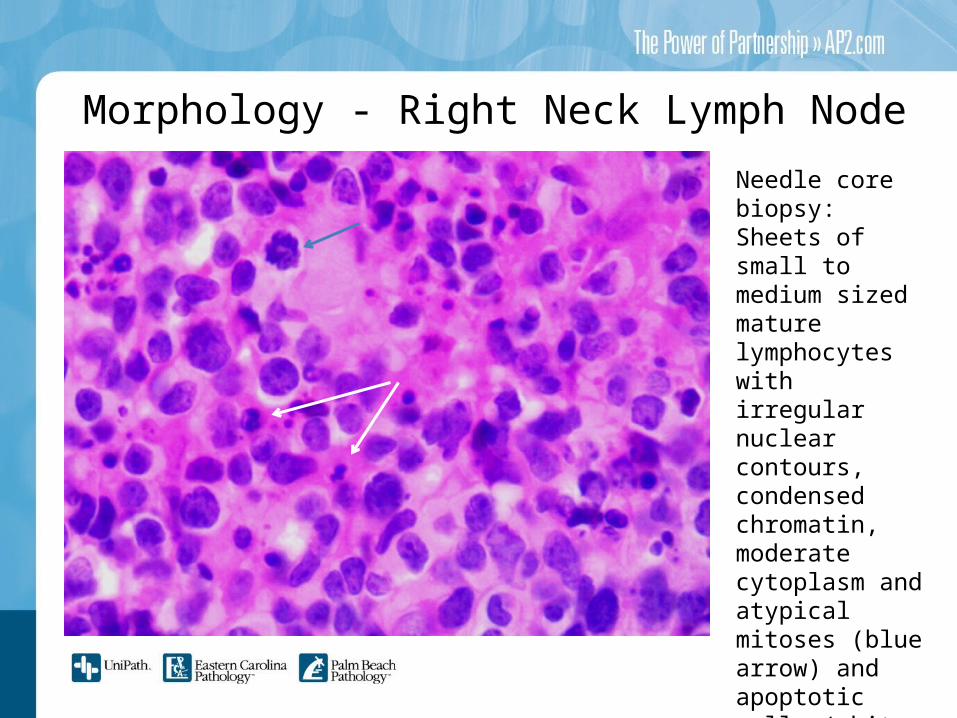
Needle core biopsy:Sheets of small to medium sized mature lymphocytes with irregular nuclear contours, condensed chromatin, moderate cytoplasm and atypical mitoses (blue arrow) and apoptotic cells (white arrow).
Morphology - Right Neck Lymph Node

15
Flow Data - Right Neck Mass - Tube 1The CD45 vs Side Scatter plot shows mostly degenerating cells with dim to negative CD45, exhibiting the low viability (56%). There is a small lymphocyte population with bright CD45. Very few B lymphocytes are detected.

cells
Flow Data - Right Neck Mass - Tube 2The lymphocytes show an abnormal population with a nearly identical immunophenotype to the bone marrow aspirate: positive for CD2, CD4, CD5, CD7, and bright CD45; negative for CD3,CD8, CD16, and CD56.
16
NK cells
Maroon=abnormal T cellsBlue= polytypic T cellsOrange= NK cells
Abnormal T cells
Polytypic T cells

PERIPHERAL BLOOD
The right neck mass was treated with palliative radiation. Approximately one month later, the patient presented with a lower extremity deep venous thrombosis and a rapidly increasing white blood cell count (up to 51,000, with 20% lymphocytes). Therefore, peripheral blood was submitted for flow cytometry analysis.

Morphology- Peripheral Blood Smear and Cytospin Preparation
Both the cytospin and the peripheral smear show numerous medium sized atypical lymphocytes featuring mildly irregular nuclear contours and central, prominent nucleoli (highlighted by black arrow).

19
Flow Data - Peripheral Blood-Tube 1In tube 1, very few B lymphocytes were detected with no aberrant immunophenotype.
B lymphocytes Polyclonal B cells
debris
Bright light blue= B cellsBlue= T cellsGrey=debris

20
Flow Data - Peripheral Blood-Tube 2There is a significantly abnormal population of T lymphocytes (41.9% of total events) shown in maroon, which express bright CD45, partial CD3, partial CD2, CD5, CD7, CD4; and are negative for CD8, CD56 and CD16.
Polytypic T cells
Abnormal T cells
debris
NK cells
Maroon=abnormal T cellsBlue= polytypic T cellsOrange= NK cells Grey=debris

21
Final DiagnosisRecurrent T-Prolymphocytic Leukemia (T-PLL)• Following a 2nd allogeneic, matched, unrelated bone marrow transplant, a
persistent small abnormal T-cell population was detected in marrow and tissues (0.57% and 2.11% respectively).
• A peripheral blood drawn 90 days post transplant exhibited full relapse with the aberrant T-cell population growing to 41.90% of total events.
• Key immunophenotypic findings across all specimens included negative to partial/dim surface CD3; and CD2, CD4, CD5, CD7, bright CD45 positive; CD8, CD16, CD56 negative.
• Morphology consistently showed medium-sized atypical lymphocytes with slightly dispersed chromatin, 1-3 variably prominent nucleoli, irregular nuclear contours, and moderate lightly basophilic cytoplasm.
• The patient previously showed a complex abnormal karyotype with a derivative chromosome 14 from a t(14;14)(q11;q32), which is the second most common cytogenetic abnormality seen in T-PLL (10% of patients). FISH for TCRAD rearrangement was positive in the relapsed specimens, c/w persistence of the rearrangement of the TCRAD locus at 14q11.2.

22
T-Prolymphoctyic Leukemia (T-PLL)WHO Classification/Definition• An aggressive T-cell leukemia characterized by a proliferation of small to medium-sized
prolymphocytes.
Epidemiology• Represents only 2% of mature lymphocytic leukemias in adults over 30.• Median age of incidence is 65 years, with a range of 30-94 years.
Sites of Involvement• Peripheral blood and bone marrow are the major sites of involvement.• Infiltrates may also be seen in the spleen, liver, and skin.
Clinical Features• Anemia, thrombocytopenia, and absolute lymphocytosis.• Hepatosplenomegaly and generalized lymphadenopathy are common.• Skin infiltration in 20% of cases, with serous effusions appearing in few cases.
23
T-Prolymphoctyic LeukemiaDiagnostic Testing• Peripheral Blood/Bone Marrow Morphology
– Abundant small to medium-sized lymphs.– Non-granular basophilic cytoplasm.– Round, oval, or markedly irregular nuclei and visible nucleolus.
• Immunophenotype is consistent with that of peripheral T-cells– Negative for TdT, CD1a, CD16, CD56; Positive for CD2, CD3 (may be weak to negative
on membrane), CD5, CD7, bright CD45. – CD4+8- (60% of cases), CD4+8+ (25% of cases), CD4-8+ (15% of cases).– CD52 testing may be requested to determine treatment.
• Cytogenetic testing– Rearrangement between T-cell receptor genes beta and gamma.– Inv (14)(q11q32) in 80% of cases; t(14;14)(q11;q32) in 10% of cases– Trisomy 8q, idic (8p11), and t(8;8)(p11-12;q12) in 70-80% of cases.

24
T-Prolymphoctyic LeukemiaPrognosis• Aggressive disease course with a median survival of less than 1 year.• Chronic courses may accelerate after 2 to 3 years.• Patient declined further therapy and opted for hospice care.
Treatment Options• Monoclonal antibody therapy with anti-CD52 (alemtuzumab). Has a
median survival of 20 months.• Autologous or allogeneic stem cell transplant following successful
immunotherapy and remission. Median survival of 48 months.

25
References• Dearden C. B- and T-cell prolymphocytic leukemia: antibody approaches.
Hematology Am Soc Hematol Educ Program. 2012;2012:645-51. doi: 10.1182/asheducation-2012.1.645. Review. PubMed PMID: 23233647.
• Dearden C. How I treat prolymphocytic leukemia. Blood. 2012 Jul 19;120(3):538-51. doi: 10.1182/blood-2012-01-380139. Epub 2012 May 30. PubMed PMID: 22649104.
• Foucar K. Mature T-cell leukemias including T-prolymphocytic leukemia, adult T-cell leukemia/lymphoma, and Sézary syndrome. Am J Clin Pathol. 2007 Apr;127(4):496-510. PubMed PMID: 17369126.
• Graham RL, Cooper B, Krause JR. T-cell prolymphocytic leukemia. Proc (Bayl Univ Med Cent). 2013 Jan;26(1):19-21. PubMed PMID: 23382603; PubMed Central PMCID: PMC3523759
• Swerdlow, Steven H. “T-cell prolymphocytic leukemia." WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon, France: International Agency for Research on Cancer, 2008. 270-271.





























