Embed Size (px)
Citation preview

1
The Difficult AirwayThe Difficult Airway
Robert J. Vissers, MD FACEPDepartment of Emergency Medicine
Legacy, Emanuel Hospital
Robert J. Vissers, MD FACEPRobert J. Vissers, MD FACEPDepartment of Emergency Medicine Department of Emergency Medicine
Legacy, Emanuel HospitalLegacy, Emanuel Hospital
The Difficult AirwayThe Difficult Airway
Defining the problemDefining the difficult airwayIdentifying the difficult airwayManaging the difficult airway
DefDefiinniing the problemng the problemDefDefiinniing the dng the diiffffiicult acult aiirwayrwayIdIdententiifyfyiing the dng the diiffffiicult acult aiirwayrwayManagManagiing the dng the diiffffiicult acult aiirwayrway
Difficult Airway Algorithms: ASADifficult Airway Algorithms: ASAFig 1ASA DIFFICULT AIRWAY ALGORITHM
Anesthesiology 1996;84:686A
Fig 1ASA DIFFICULT AIRWAY ALGORITHM
Anesthesiology 1996;84:686A
Cancel Case
Awaken
Ectopic AnesthesiaEctopic Anesthesia
Problem:UrgencyCost of failure Formula for error
Problem:Problem:UrgencyUrgencyCost of failure Cost of failure Formula for errorFormula for error
2
Emergency Airway Management
Emergency Airway Management
Solution:PreparationAnticipate difficulties Simple, consistent, reproducible approach
Solution:Solution:PreparationPreparationAnticipate difficulties Anticipate difficulties Simple, consistent, reproducible Simple, consistent, reproducible approachapproach
Difficult Airway AlgorithmsDifficult Airway Algorithms
Common principles Assessment of ventilation difficultyAssessment of intubation difficultyAwake vs. induction and paralysisCalling for helpSurgical airway is a potential endpoint
Common principles Common principles Assessment of ventilation difficultyAssessment of ventilation difficultyAssessment of intubation difficultyAssessment of intubation difficultyAwake vs. induction and paralysisAwake vs. induction and paralysisCalling for helpCalling for helpSurgical airway is a potential endpointSurgical airway is a potential endpoint
Decision to intubate
Near death?Unresponsive?
Difficult Airway?
Rapid Sequence Intubation
Failed AirwayDifficult
Airway Techniques
Crash Airway
Adapted from: Walls RM, Ed. The Manual of Emergency Airway Management Philadelphia, Lippincott, 2000.
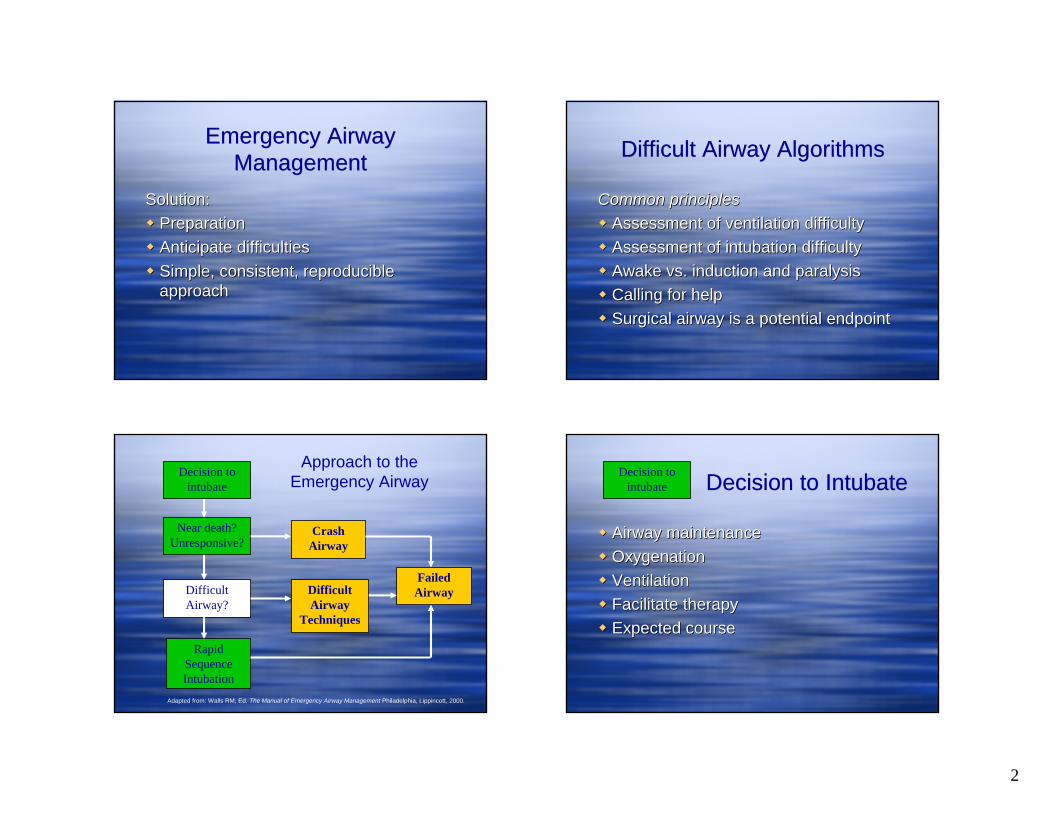
Approach to the Emergency Airway Decision to IntubateDecision to Intubate
Airway maintenanceOxygenationVentilationFacilitate therapyExpected course
Airway maintenanceAirway maintenanceOxygenationOxygenationVentilationVentilationFacilitate therapyFacilitate therapyExpected courseExpected course
Decision to intubate
3
Decision to Intubate: ModifiersDecision to Intubate: Modifiers
Operator experienceSetting Potential for a difficult airway
Never take away what you cannot replace
Operator experienceOperator experienceSetting Setting Potential for a difficult airwayPotential for a difficult airway
Never take away what you cannot replaceNever take away what you cannot replace
National Emergency Airway Registry (NEAR)
National Emergency Airway Registry (NEAR)
Prospective airway registry n = 12,000<1% fail rate with RSICricothyrotomy rate 0.6% No cases of “cannot intubate, cannot ventilate” with death
Prospective airway registry n = 12,000Prospective airway registry n = 12,000<1% fail rate with RSI<1% fail rate with RSICricothyrotomy rate 0.6% Cricothyrotomy rate 0.6% No cases of No cases of ““cannot intubate, cannot cannot intubate, cannot ventilateventilate”” with deathwith death
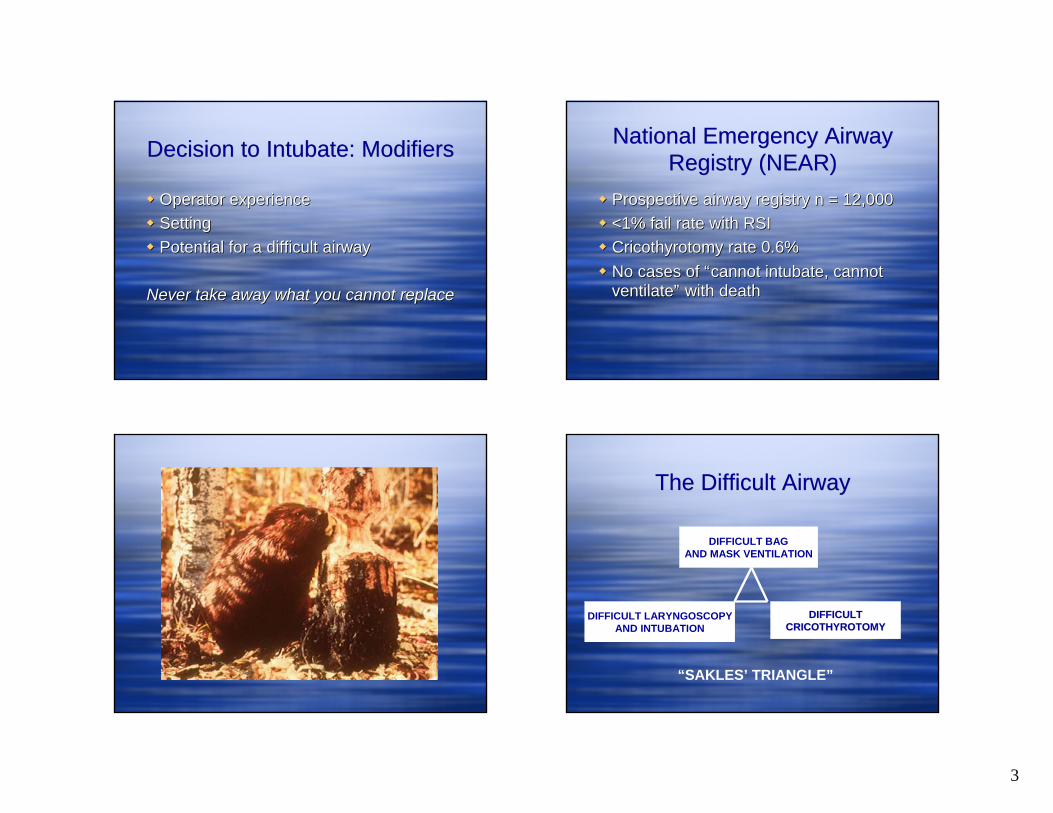
The Difficult AirwayThe Difficult Airway
DIFFICULT BAGAND MASK VENTILATION
DIFFICULT LARYNGOSCOPYAND INTUBATION
DIFFICULTDIFFICULTCRICOTHYROTOMYCRICOTHYROTOMY
“SAKLES’ TRIANGLE”
4
The Difficult AirwayThe Difficult Airway
DIFFICULT BAGAND MASK VENTILATION
DIFFICULT LARYNGOSCOPYAND INTUBATION
DIFFICULTCRICOTHYROTOMY
“SAKLES’ TRIANGLE”
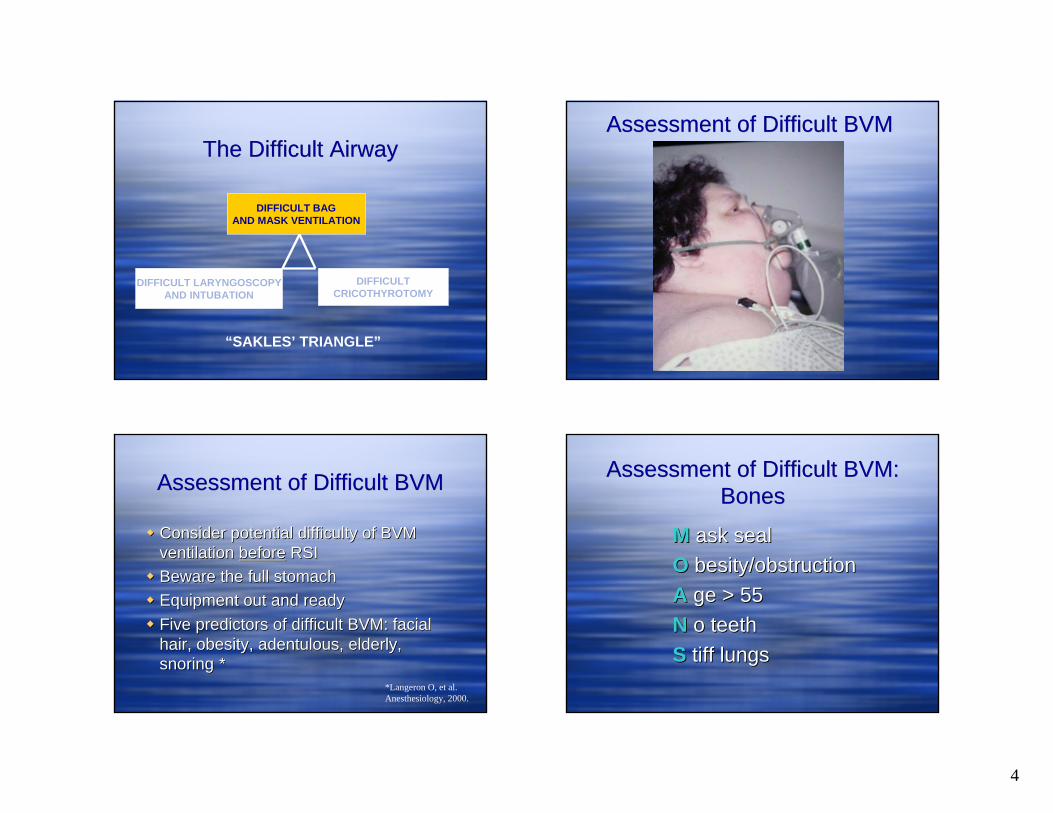
Assessment of Difficult BVMAssessment of Difficult BVM
Assessment of Difficult BVMAssessment of Difficult BVM
Consider potential difficulty of BVM ventilation before RSIBeware the full stomachEquipment out and readyFive predictors of difficult BVM: facial hair, obesity, adentulous, elderly, snoring *
Consider potential difficulty of BVM Consider potential difficulty of BVM ventilation ventilation beforebefore RSIRSIBeware the full stomachBeware the full stomachEquipment out and readyEquipment out and readyFive predictors of difficult BVM: facial Five predictors of difficult BVM: facial hair, obesity, hair, obesity, adentulousadentulous, elderly, , elderly, snoringsnoring **
*Langeron O, et al. Anesthesiology, 2000.
Assessment of Difficult BVM: Bones
Assessment of Difficult BVM: Bones
M ask sealO besity/obstructionA ge > 55N o teethS tiff lungs
MM ask sealask sealOO besitybesity/obstruction/obstructionAA gege > 55> 55NN o teetho teethSS tiff lungstiff lungs
5
The Difficult AirwayThe Difficult Airway
DIFFICULT BAGAND MASK VENTILATION
DIFFICULT LARYNGOSCOPYAND INTUBATION
DIFFICULTCRICOTHYROTOMY
“SAKLES’ TRIANGLE”
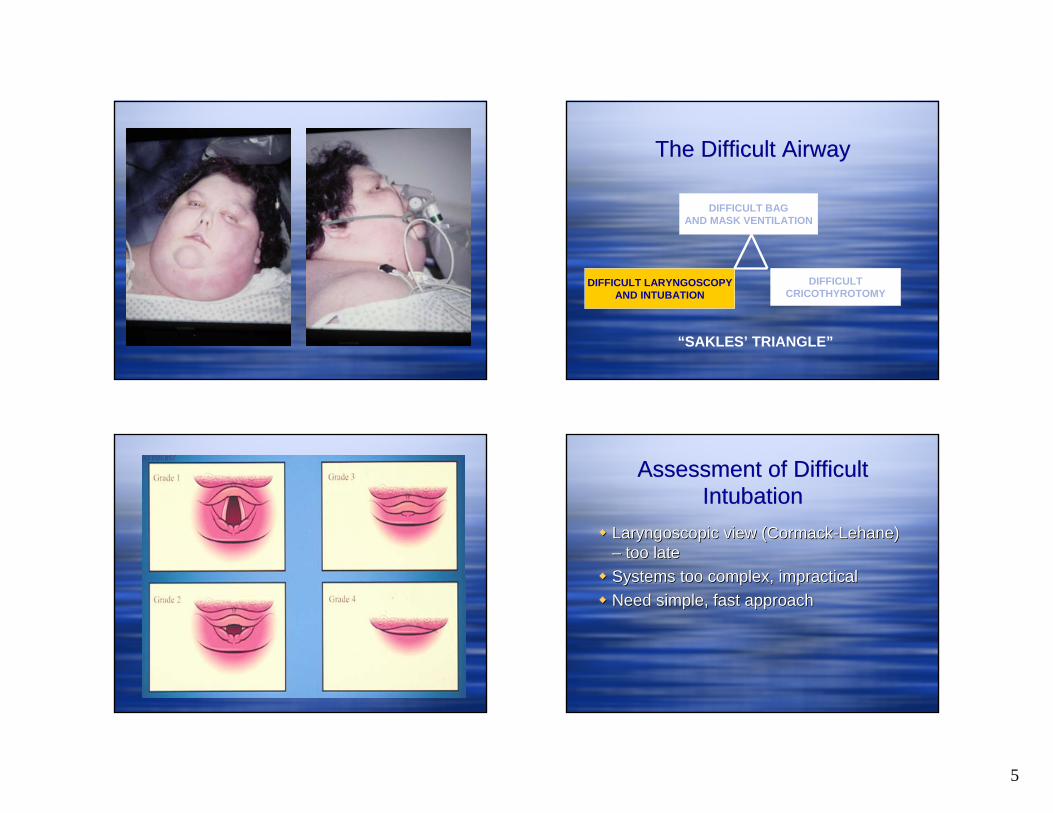
Assessment of Difficult Intubation
Assessment of Difficult Intubation
Laryngoscopic view (Cormack-Lehane) – too lateSystems too complex, impracticalNeed simple, fast approach
LaryngoscopicLaryngoscopic view (Cormackview (Cormack--LehaneLehane) ) –– too latetoo lateSystems too complex, impracticalSystems too complex, impracticalNeed simple, fast approachNeed simple, fast approach

6
Difficult Airway…? “LEMON” Law“LEMON” Law
L ook externallyE xamine (3-3-2)M allampati gradeO bstructionN eck mobility
LL ookook externallyexternallyEE xaminexamine (3(3--33--2)2)MM allampatiallampati gradegradeOO bstructionbstructionNN eckeck mobilitymobility
Cognitive forcing strategies in clinical decisionmaking. P Croskerry. Ann Emerg Med Jan, 2003.
Adapted from: Walls RM, Ed. The Manual of Emergency Airway ManagementPhiladelphia, Lippincott, 2000.
LEMON: LookLEMON: Look
Simple visual inspection often reveals obvious potential difficulties
Simple visual inspection often reveals Simple visual inspection often reveals obvious potential difficultiesobvious potential difficulties
7
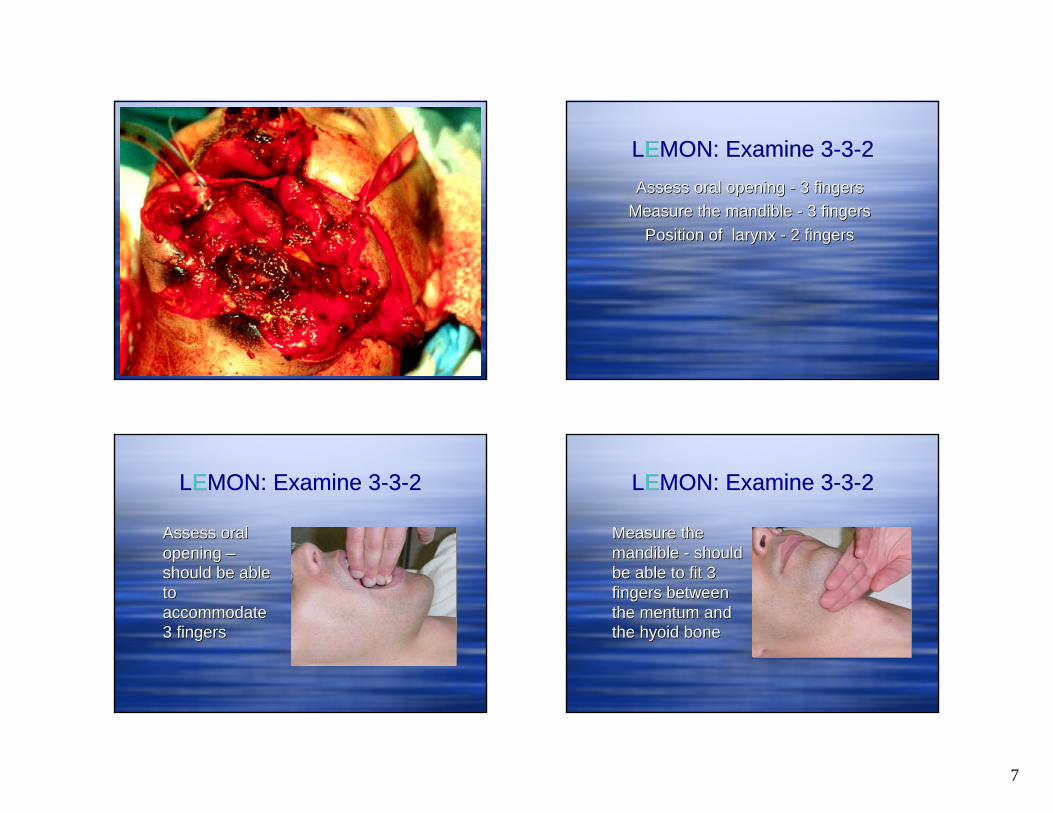
LEMON: Examine 3-3-2LEMON: Examine 3-3-2Assess oral opening - 3 fingers
Measure the mandible - 3 fingers Position of larynx - 2 fingers
Assess oral opening Assess oral opening -- 3 fingers3 fingersMeasure the mandible Measure the mandible -- 3 fingers 3 fingers
Position of larynx Position of larynx -- 2 fingers 2 fingers
LEMON: Examine 3-3-2LEMON: Examine 3-3-2
Assess oral opening –should be able to accommodate 3 fingers
Assess oral Assess oral opening opening ––should be able should be able to to accommodate accommodate 3 fingers3 fingers
LEMON: Examine 3-3-2LEMON: Examine 3-3-2
Measure the mandible - should be able to fit 3 fingers between the mentum and the hyoid bone
Measure the Measure the mandible mandible -- should should be able to fit 3 be able to fit 3 fingers between fingers between the the mentummentum and and the hyoid bonethe hyoid bone

8
LEMON: Examine 3-3-2LEMON: Examine 3-3-2
Assess position of larynx – should get 2 fingers between the thyroid cartilage and the mandible
Assess position of Assess position of larynx larynx –– should should get 2 fingers get 2 fingers between the between the thyroid cartilage thyroid cartilage and the mandibleand the mandible

9
Class I
Class IV
Class II
Class III
LEMON: MallampatiLEMON: Mallampati
LEMON: Obstruction?LEMON: Obstruction?
1) Location? 2) Fixed or mobile?
3) Speed of progression?
1) Location? 1) Location? 2) Fixed or mobile?2) Fixed or mobile?
3) Speed of progression?3) Speed of progression?

10
LEMON: Neck MobilityLEMON: Neck Mobility
Can the patient flex and extend the neck?Actively assess in the non-trauma obtunded patient.Cervical spine immobilization - remove anterior collar while c-spine is immobilized.
Can the patient flex and extend the Can the patient flex and extend the neck?neck?Actively assess in the nonActively assess in the non--trauma trauma obtunded patient.obtunded patient.Cervical spine immobilization Cervical spine immobilization -- remove remove anterior collar while canterior collar while c--spine is spine is immobilized.immobilized.

11
“LEMON” Law“LEMON” Law
L ook externallyE xamine (3-3-2)M allampati gradeO bstructionN eck mobility
LL ookook externallyexternallyEE xaminexamine (3(3--33--2)2)MM allampatiallampati gradegradeOO bstructionbstructionNN eckeck mobilitymobility
LEMON: Predictive?LEMON: Predictive?
156 ED patients requiring intubationScored using LEMONSimple point system used (0 to 10)Compared to laryngoscopic view (Cormack –Lehane)Felt to be predictive, P<0.05
156 ED patients requiring intubation156 ED patients requiring intubationScored using LEMONScored using LEMONSimple point system used (0 to 10)Simple point system used (0 to 10)Compared to Compared to laryngoscopiclaryngoscopic view (Cormack view (Cormack ––LehaneLehane))Felt to be predictive, P<0.05Felt to be predictive, P<0.05
Reed MJ et al. Can an airway assessment score predict difficulty at intubation in the emergency department? Emerg Med J 2005 Feb; 22:99-102.

12
LEMON: Predictive?LEMON: Predictive?
Reed MJ et al. Can an airway assessment score predict difficulty at intubation in the emergency department? EmergMed J 2005 Feb; 22:99-102.
Reed MJ et al. Can an airway assessment score predict Reed MJ et al. Can an airway assessment score predict difficulty at intubation in the emergency department? difficulty at intubation in the emergency department? EmergEmergMed JMed J 2005 Feb; 22:992005 Feb; 22:99--102. 102.
Airway alternatives
Airway alternatives
BVMIntubating LMA®LightwandGlidescopeFiberopticsBougieCombitubeKing-LT
TTJVCricothyrotomy
Zone of Increasing Sphincter Tone
Supraglottic:
Infraglottic:
ZIST
Nasal
BNTIFiberoptics
13
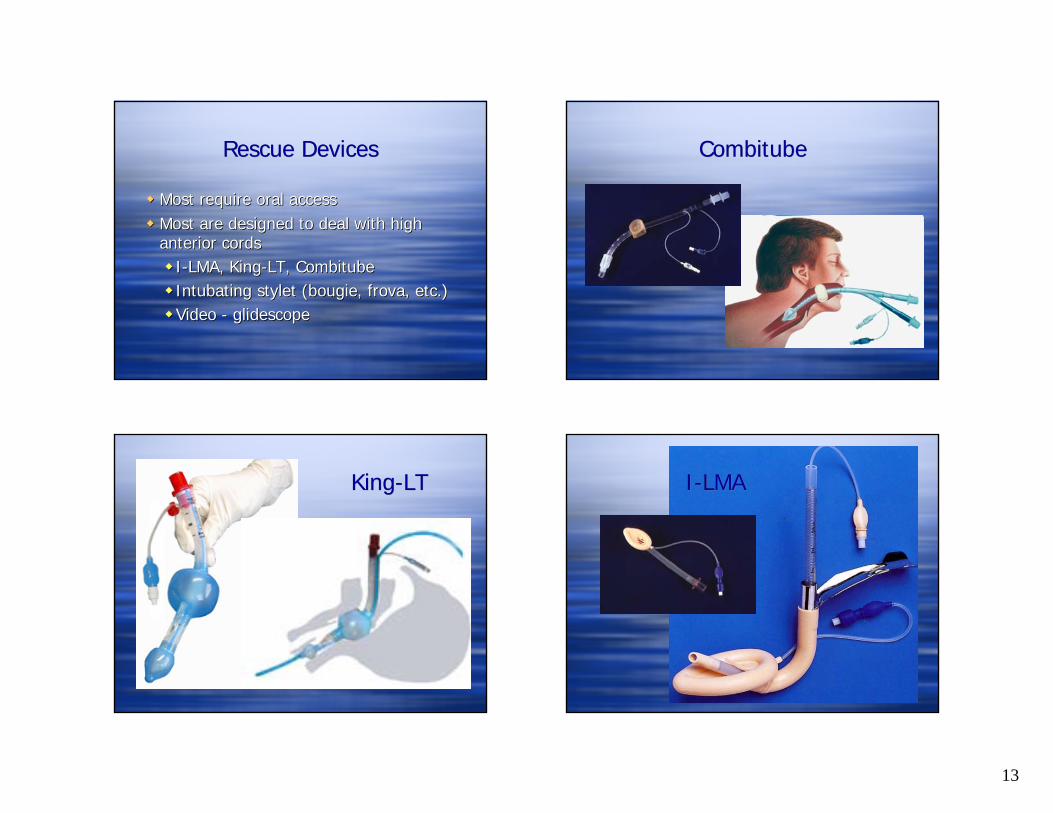
Rescue DevicesRescue Devices
Most require oral accessMost are designed to deal with high anterior cords
I-LMA, King-LT, CombitubeIntubating stylet (bougie, frova, etc.)Video - glidescope
Most require oral accessMost require oral accessMost are designed to deal with high Most are designed to deal with high anterior cordsanterior cords
II--LMA, KingLMA, King--LT, LT, CombitubeCombitubeIntubatingIntubating styletstylet ((bougiebougie, , frovafrova, etc.), etc.)Video Video -- glidescopeglidescope
CombitubeCombitube
King-LTKing-LT I-LMA I-LMA
14
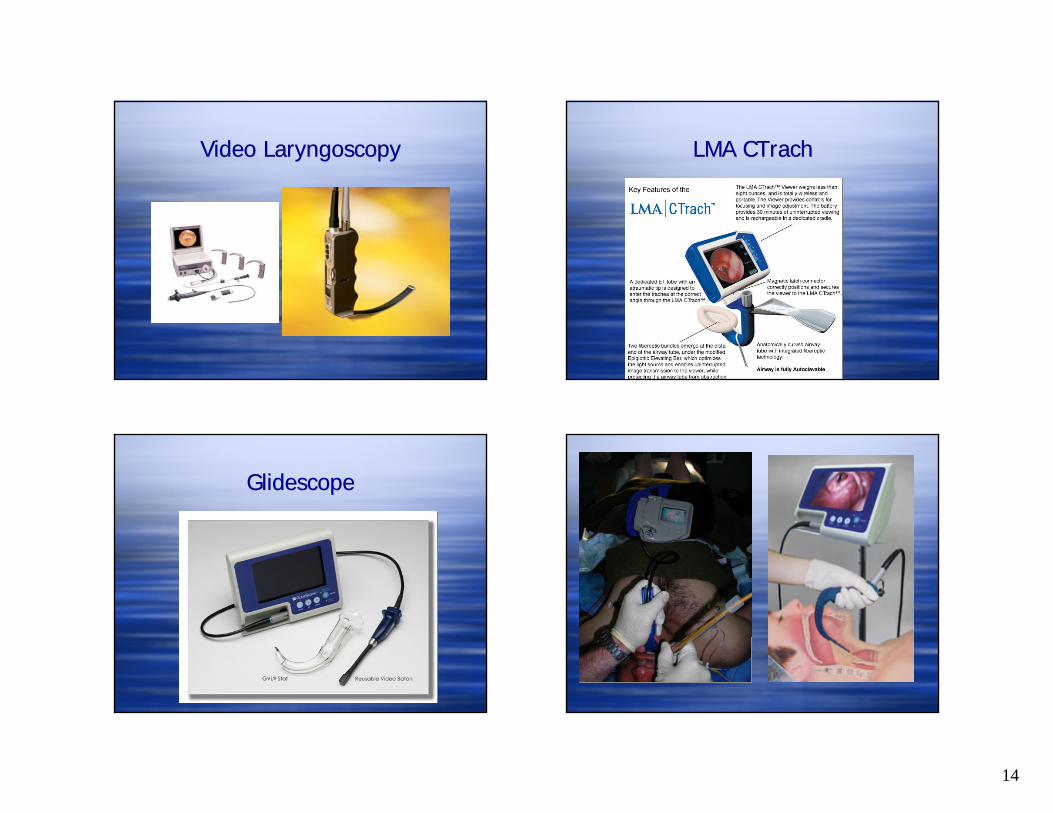
Video LaryngoscopyVideo Laryngoscopy LMA CTrachLMA CTrach
GlidescopeGlidescope
15
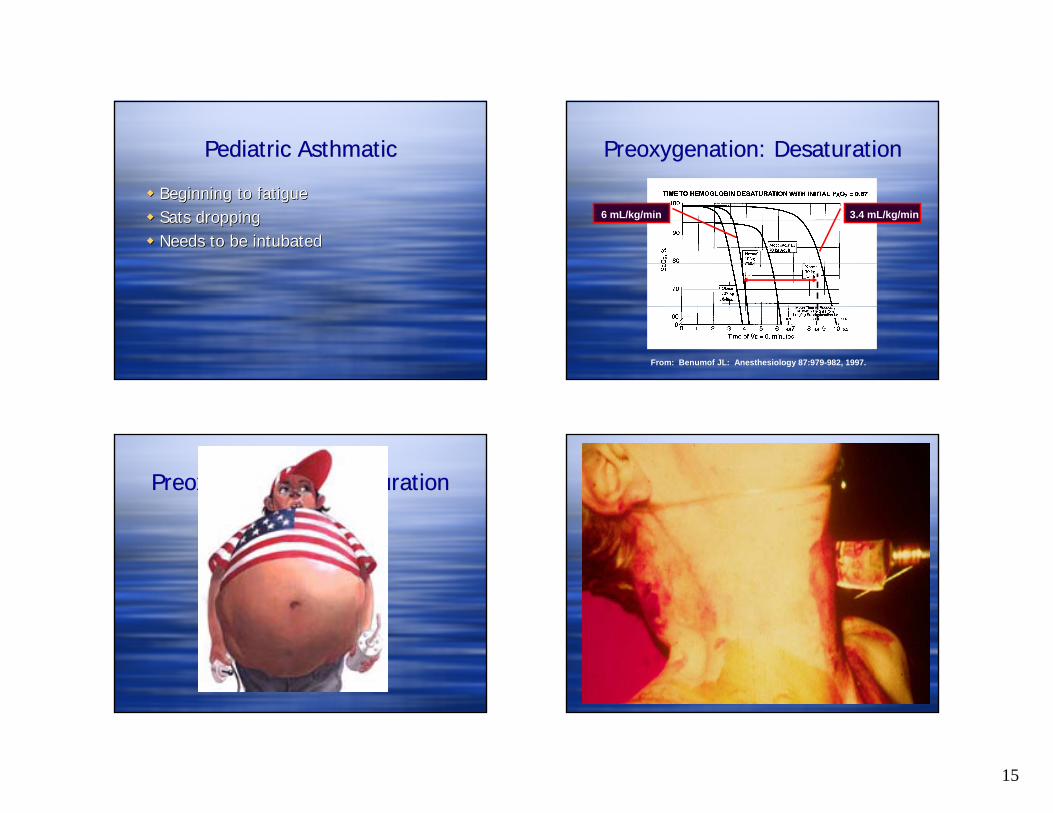
Pediatric AsthmaticPediatric Asthmatic
Beginning to fatigueSats droppingNeeds to be intubated
Beginning to fatigueBeginning to fatigueSatsSats droppingdroppingNeeds to be Needs to be intubatedintubated
Preoxygenation: DesaturationPreoxygenation: Desaturation
From: Benumof JL: Anesthesiology 87:979-982, 1997.
3.4 mL/kg/min6 mL/kg/min
Preoxygenation: DesaturationPreoxygenation: Desaturation
16
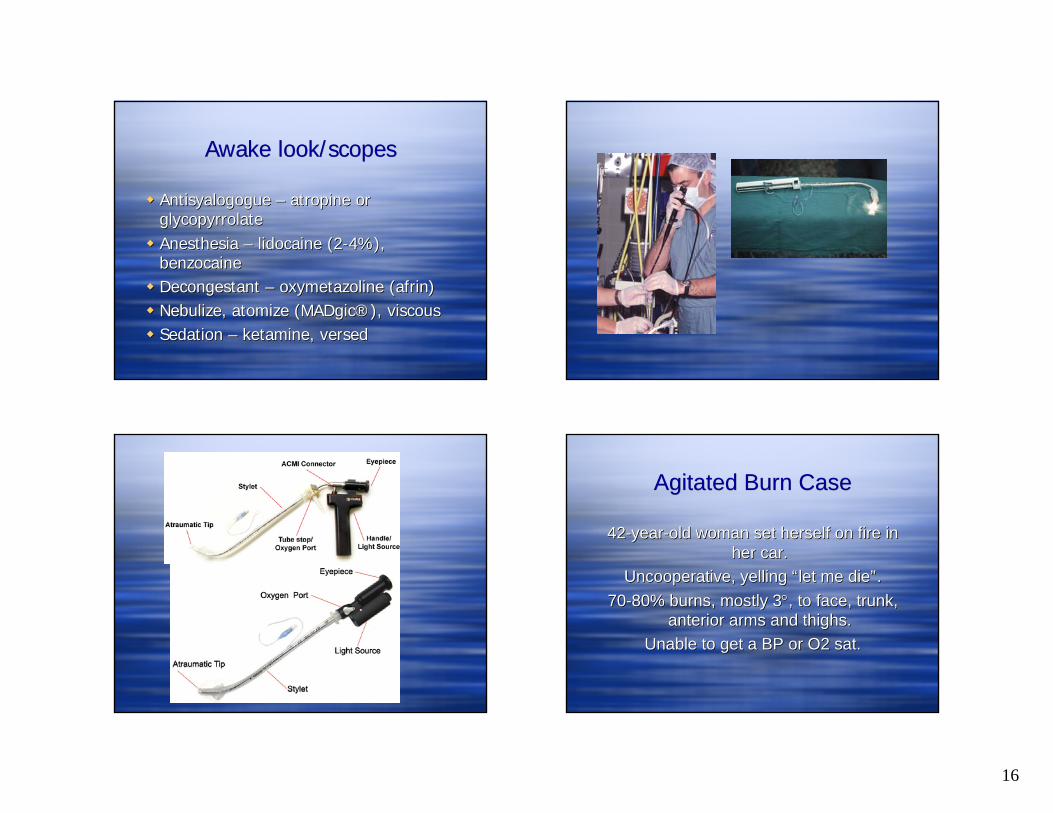
Awake look/scopesAwake look/scopes
Antisyalogogue – atropine or glycopyrrolateAnesthesia – lidocaine (2-4%), benzocaineDecongestant – oxymetazoline (afrin)Nebulize, atomize (MADgic®), viscousSedation – ketamine, versed
AntisyalogogueAntisyalogogue –– atropine or atropine or glycopyrrolateglycopyrrolateAnesthesia Anesthesia –– lidocainelidocaine (2(2--4%), 4%), benzocainebenzocaineDecongestant Decongestant –– oxymetazolineoxymetazoline ((afrinafrin))NebulizeNebulize, atomize (, atomize (MADgicMADgic®®), viscous), viscousSedation Sedation –– ketamineketamine, versed, versed
Agitated Burn Case Agitated Burn Case
42-year-old woman set herself on fire in her car.
Uncooperative, yelling “let me die”. 70-80% burns, mostly 3°, to face, trunk,
anterior arms and thighs. Unable to get a BP or O2 sat.
4242--yearyear--old woman set herself on fire in old woman set herself on fire in her car. her car.
Uncooperative, yelling Uncooperative, yelling ““let me dielet me die””. . 7070--80% burns, mostly 380% burns, mostly 3°°, to face, trunk, , to face, trunk,
anterior arms and thighs. anterior arms and thighs. Unable to get a BP or O2 sat.Unable to get a BP or O2 sat.

17
Intubating Stylet/BougieIntubating Stylet/Bougie
Clinical Issues: Agitated PatientClinical Issues: Agitated Patient
Assessment of the difficult airway –beware ego, fear, urgency The agitated or violent trauma patient
Haldol, Droperidol, Midazolam, Ketamine
Assessment of the difficult airway Assessment of the difficult airway ––beware ego, fear, urgency beware ego, fear, urgency The agitated or violent trauma patientThe agitated or violent trauma patient
HaldolHaldol, , DroperidolDroperidol, , MidazolamMidazolam, , KetamineKetamine
Oh, nuts…Oh, nuts…
5 yo girl, choked on peanuts last nightUnable to sleep, trouble breathingLooks tired, respdistress, tripod
5 5 yoyo girl, choked on girl, choked on peanuts last nightpeanuts last nightUnable to sleep, Unable to sleep, trouble breathingtrouble breathingLooks tired, Looks tired, resprespdistress, tripoddistress, tripod

18
Airway alternatives
Airway alternatives
BVMIntubating LMA®LightwandGlidescopeFiberopticsBougieCombitubeKing-LT
TTJVCricothyrotomy
Zone of Increasing Sphincter Tone
Supraglottic:
Infraglottic:
ZIST
Nasal
BNTIFiberoptics

19
No landmarks?No landmarks?
The tongue is your friend – find it and follow it to the glottisSuction, suction, suction…4-finger rule for the cricothyroid membrane
The The tonguetongue is your friend is your friend –– find it and find it and follow it to the glottisfollow it to the glottisSuctionSuction, suction, suction, suction, suction……44--finger rulefinger rule for the cricothyroid for the cricothyroid membranemembrane
Cricothyroid membrane under the 4th finger
Cricothyroid membrane under the 4th finger

20
Consider surgical airway earlyConsider surgical airway early SummarySummary
Organized, rapid, simple approachAssess for difficult ventilationBONES
Assess for difficult intubationLEMON
Organized, rapid, simple approachOrganized, rapid, simple approachAssess for difficult ventilationAssess for difficult ventilationBONESBONES
Assess for difficult intubationAssess for difficult intubationLEMONLEMON

21
Obese asthmaticObese asthmatic





























