Embed Size (px)
Citation preview

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 1
SUMMARY OF SAFETY AND EFFECTIVENESS DATA (SSED)
I. GENERAL INFORMATION
Device Generic Name: Temporary Ventricular Support Device
Device Trade Name: Impella Ventricular Support Systems
Device Classification: OZD
Applicant Name and Address: Abiomed, Inc.
22 Cherry Hill Drive
Danvers, MA 01923
Date of Panel Recommendation: None
Pre-market Approval (PMA) Number: P140003/S005
Date of Notice of Approval to Applicant: April 7, 2016
The original PMA for the Impella 2.5 System (PMA P140003) was approved on March
23, 2015. The approved indication for use for the Impella 2.5 System is:
The Impella 2.5 System is a temporary (< 6 hours) ventricular support device indicated
for use during high risk percutaneous coronary interventions (PCI) performed in elective
or urgent, hemodynamically stable patients with severe coronary artery disease and
depressed left ventricular ejection fraction, when a heart team, including a cardiac
surgeon, has determined high risk PCI is the appropriate therapeutic option. Use of the
Impella 2.5 in these patients may prevent hemodynamic instability which can result from
repeat episodes of reversible myocardial ischemia that occur during planned temporary
coronary occlusions and may reduce peri- and post-procedural adverse events.
Additional information about the Impella 2.5 System is available in its Summary of
Safety and Effectiveness Data (SSED), which can be found on the FDA CDRH web-site.
The purpose of this supplement (P140003/S005) is to expand the indication for use to
include the treatment of ongoing cardiogenic shock that occurs immediately following
open heart surgery and to include additional Impella Catheters for this indication.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 2
II. INDICATIONS FOR USE
The Impella 2.5, Impella CP, Impella 5.0, and Impella LD catheters, in conjunction with
the Automated Impella Controller, are temporary ventricular support devices intended for
short term use (≤ 4 days for the Impella 2.5 and Impella CP, and ≤ 6 days for Impella 5.0
and LD) and indicated for the treatment of ongoing cardiogenic shock that occurs
immediately (< 48 hours) following acute myocardial infarction or open heart surgery as
a result of isolated left ventricular failure that is not responsive to optimal medical
management and conventional treatment measures.* The intent of the Impella system
therapy is to reduce ventricular work and to provide the circulatory support necessary to
allow heart recovery and early assessment of residual myocardial function.
*optimal medical management and conventional treatment measures include volume loading and use of pressors and inotropes, with or without IABP.
III. CONTRAINDICATIONS
• Mural thrombus in the left ventricle
• Mechanical aortic valve or heart constrictive device
• Aortic valve stenosis/calcification (equivalent to an orifice area of 0.6 cm2 or
less)
• Moderate to severe aortic insufficiency (echocardiographic assessment graded
as ≥ +2)
• Severe peripheral arterial disease precluding placement of the Impella Catheters
• Significant right heart failure
• Combined cardiorespiratory failure
• Presence of an atrial or ventricular sepal defect (including post-infarct VSD)
• Left ventricular rupture
• Cardiac tamponade
IV. WARNINGS AND PRECAUTIONS
The warnings and Precautions can be found in the approved labeling for the Impella
Ventricular Support Systems.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 3
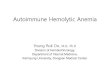
V. DEVICE DESCRIPTION
To accommodate a range of cardiac flow requirements and implant techniques, four
different Impella support Catheters are available. Figure 1 shows general overall design
for the Impella Catheters. All of the Impella Catheters consist of a micro-axial rotary
blood pump mounted on a 9F drive catheter, which is connected to an external controller,
the Automatic Impella Controller (AIC).
Figure 1: Impella Ventricular Support Catheter Design

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 4
There are four different Impella Catheters, as shown in Figure 2. The peripherally
placed catheters are the Impella 2.5, the Impella CP, and the Impella 5.0, which have
blood pump diameters of 12F, 14F, and 21F, respectively. In addition, a fourth 21F
surgically placed Impella Catheter, the Impella LD, is available.
Figure 2: The Impella Ventricular Support Catheters
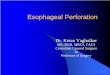
The Impella Catheters shown above are all placed with the cannula inflow located in
the left ventricle and the outflow located in the ascending aorta, as shown in Figure 3.
Blood is drawn through the cannula situated in the left ventricle and expelled into the
aorta. As shown in Figures 2 and 3, the three peripherally placed pumps (the Impella
2.5, Impella CP, and Impella 5.0) have 6F pigtails attached to their tips, to enable
device placement over the wire and positioning in the correct anatomical position.
When placing an Impella Catheter peripherally (via a guidewire), the device is loaded
over the wire through the pigtail. The Impella 5.0, while placed peripherally, requires
a graft and a surgical cut-down and can access the circulation through either the
femoral or axillary artery. Alternatively, the Impella LD is surgically placed directly
through the aorta into the heart (see in Figure 3).

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 5
Figure 3: Ventricular placement of the Impella Catheters
The Impella Catheters are operated by the same external drive console, the Automatic
Impella Controller (AIC), shown in Figure 4. The AIC generates signals required to
power the drive motor of the Impella Catheters and provides a user interface. The AIC
also incorporates the disposable Impella Purge Cassette system, which provides a fluid
pressure barrier to prevent blood from entering the Impella Catheter’s drive motor. A
dextrose (5-40% with 50 Units/ml of heparin added) solution is used as a purge fluid. The
AIC is portable and has been qualified for use for patient transport by trained healthcare
professionals within healthcare facilities and during medical transport between hospitals
(i.e., ambulance, helicopter, or fixed-wing aircraft).
Blood outlet
Blood inlet
Surgical Catheter Placement (Impella LD)
Percutaneous Catheter Placement (Impella 2.5, Impella CP, Impella 5.0)
Blood outlet
Blood inlet

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 6
Figure 4: The AIC with an Impella Catheter and its Impella Purge Cassette
Additional sterile, disposable implant accessories are provided with the Impella Catheters
to assist in their percutaneous insertion. For the Impella 2.5, these components are a 13F
peel-away introducer kit (manufactured by Merit Medical) and an 0.018” placement
guidewire (manufactured by Lake Region Medical). The Impella CP accessories are a
14F peel-away introducer kit (manufactured by Oscor Medical) and the identical
placement guidewire packaged with the Impella 2.5. The Impella 5.0 is packaged with a
23F peel-away introducer kit (manufactured by Oscor Medical), an 0.018” guidewire
(manufactured by Lake Region Medical), and a surgical clamp to assist in hemostasis.
A reusable cart for the AIC is also provided for ease of patient transport within the
hospital.
VI. ALTERNATIVE PRACTICES AND PROCEDURES
The alternative therapies used to treat left ventricular failure (LVF) in the post-
cardiotomy cardiogenic shock (PCCS) setting are inotropic support, intra-aortic balloon
pump (IABP) counterpulsation therapy, or surgical left ventricular assist devices.
Impella Purge Cassette Impella Support Catheter

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 7
VII. MARKETING HISTORY
The Impella pumps have received CE Mark in the European Union (EU) as well as
approval in Canada for a similar intended use as is being approved in this supplement.
Neither the AIC nor any of the Impella pumps have been withdrawn from marketing for
any reason related to its safety or effectiveness.
VIII. POTENTIAL ADVERSE EFFECTS OF THE DEVICE ON HEALTH
The following adverse events may be associated with use of the Impella Ventricular
Support Systems:
• Acute renal dysfunction
• Aortic insufficiency
• Aortic valve injury
• Atrial fibrillation
• Bleeding
• Cardiogenic shock
• Cardiac tamponade
• Cardiopulmonary resuscitation
• Cerebral vascular accident/Stroke
• Death
• Device malfunction
• Failure to achieve angiographic
success
• Hemolysis
• Hepatic failure
• Insertion site infection
• Limb ischemia
• Myocardial infarction
• Need for cardiac, thoracic or
abdominal operation
• Perforation
• Renal failure
• Repeat revascularization
• Respiratory dysfunction
• Sepsis
• Severe hypotension
• Thrombocytopenia
• Thrombotic vascular (non-CNS)
complication
• Transient ischemic attack
• Vascular injury
• Ventricular arrhythmia,
fibrillation or tachycardia
For the specific adverse events that occurred in the clinical studies, please see Section X.
below.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 8
IX. SUMMARY OF PRECLINICAL STUDIES
Preclinical testing was conducted on the Impella 2.5 Catheter, the AIC, and the Impella
Purge Cassette in support of P140003 and summaries can be found in the original SSED,
here: http://www.accessdata.fda.gov/cdrh_docs/pdf14/P140003b.pdf. The testing
summarized below was reviewed to support the increased duration of use for the new
AMICS indication (the original indication was for <6 hours, while the AMICS indication
is for 4-6 days) and to support the addition of the additional Impella Catheters (Impella
CP, Impella 5.0, and Impella LD).
A. Laboratory Testing
In-vitro studies were performed for the Impella Ventricular Support Systems, including
the disposable components, specifically the Impella Support Catheters. The results of the
in-vitro studies were combined with the animal study results and the clinical results in the
overall review of safety and effectiveness the Impella Ventricular Support Systems.
Biocompatibility Studies
Toxicology and biocompatibility tests for the Impella Catheters were conducted in
accordance with Good Laboratory Practices (21 CFR §58) and ISO 10993-1: 2003
Biological Evaluation of Medical Devices Part 1: Evaluation and Testing. All acceptance
criteria were met.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 9
Structural Integrity Testing
Structural tests of each Impella Catheter’s components were conducted. Summaries of the
test results for the Impella Catheters are provided in Table 2.
Table 2: Summary of Structural Integrity Testing on Impella Catheters and Accessories
Test Purpose Acceptance Criteria Results
Bend
This test verified that the Impella catheters can survive the bending stresses expected during clinical use.
All catheters tested must remain intact/functional after their bend tests (for their intended durations of use).
Passed
Tensile
This test verified that the Impella catheters joints strengths are compatible with the forces expected during clinical use.
Under tensile load, all joint strengths must exceed their pre-set tensile limits.
Passed
Temperature
This test verified that the temperature of the Impella catheters’ blood contacting surfaces were acceptable for clinical use.
The surface temperatures must remain below a maximum allowable temperature.
Passed
Fluid Tightness (Introducer System)
This test verified that the Impella catheters’ introducer systems were acceptable with minimal blood loss during clinical use.
Each introducer system must not leak more than its pre-set amount during simulated use.
Passed
Electrical Compatibility, Immunity Standards & Safety Testing
The Impella Ventricular Support Systems (all of the Impella Catheters, the AIC and the
Impella Purge Cassette) were tested for Electromagnetic Compatibility (EMC),
Electromagnetic Immunity (EMI), and Electrical Safety against the relevant national and
international standards. Testing verified compliance to recognized FDA Standards,
including to IEC 60601-1, 2nd and 3rd editions. Where applicable, testing was also
performed in accordance with IEC 60601-1-2 Issued: 2007 (3rd edition). All of the EMC,
EMI and Electrical Safety tests passed.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 10
Performance Testing
Performance tests for the Impella Catheters were conducted. Summaries of the test results
are provided in Table 3.
Table 3: Summary of Performance Testing on Impella Catheters and Accessories
Test Purpose Acceptance Criteria Results
Flow Characterization
This test verified that the Impella catheters provided their specified flow, and that the flow was accurately reported (on the AIC) for the expected range of clinical use conditions.
The Impella catheters’ flow must be within a pre-set range, and be reported correctly (±0.3 LPM versus an external flow meter) over the pre-set range tested.
Passed
Simulated Placement & Cannula Kink
This test verified that the Impella catheters can be easily placed using their introducer systems and will not kink during use.
Simulated delivery must meet a pre-defined ease of use criteria, and each catheters’ cannulae must not kink (at a pre-set diameter).
Passed
Computer Fluid Dynamics (CFD)
This test evaluated the flow fields in the Impella pumps to quantify pressure and fluid stress levels in the pumps.
The pressures & fluid stress levels must remain within pre-set limits (compatible with red blood cell survival).
Passed
Hemolysis
This test (run in accordance with ASTM F1841-97(2005)) verified that the Impella catheters would not cause excessive blood hemolysis when run at their maximum flow setting.
Each catheters’ hemolysis profiles must be equivalent to other approved devices, and must meet their design requirement (must be less than a pre-set Modified Index of Hemolysis (MIH)).
Passed

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 11
Reliability Testing
Reliability tests of the Impella catheters were conducted. The purpose of the testing was
to demonstrate that each Impella catheter has acceptable reliability for its intended
duration of use. Multiple pumps were tested in a customized test loop, which was
designed to mimic the clinical use conditions (e.g., the temperature, flow, and pressure).
The test duration was to twice the intended duration of use. The pre-set pass/fail criteria
were related to the reliability and confidence levels appropriate for temporary life support
devices. All of the Impella catheters were tested, and all of tests were completed
successfully (i.e., the acceptance criteria were met). The results of the tests support the
approved intended durations of use (See Section II above).
Hazard Analysis
Potential hazards associated with the use of the Impella Ventricular Support Systems, in
both normal operation and potential abnormal conditions, were identified and analyzed
for their short-term and long-term effects. This information was used in Abiomed’s
internal hazard analysis process. Based on this analysis, measures were taken to minimize
the occurrence of the hazards and the remaining risks were deemed to be acceptable.
B. Animal Studies
Extended animal studies were completed to evaluate each Impella catheter. The purpose
of the testing was to demonstrate the safe use of the Impella catheter for extended implant
durations, which were up to 5 days, 12 days, and 10 days for the Impella 2.5, Impella CP,
and Impella 5.0/LD, respectively. Each study had pre-set acceptance criteria related to
safe device use, which included a hemolysis endpoint, evaluation of potential heart
device interactions, and animal survivability/adverse events. In addition, the study
endpoints included an assessment of overall in vivo device performance. Overall, the
animal tests were successfully completed, and the endpoints were met for each study. The
animal studies validated that each Impella catheter could be used safely in animals for its
intended duration of use without causing adverse reactions or unexpected product
performance failures or malfunctions.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 12
C. Sterilization
The Impella Catheters are all sterilized using 100% ethylene oxide (EO). The
sterilization process was validated to provide a sterility assurance level (SAL) of 10-6 in
accordance with international standards for sterilization processes for medical devices,
ANSI/AAMI/ISO 11135:1994, ANSI/AAMI/ISO 14937:2000 and EN 550:1994. A
validated post-sterilization aeration process assures that residual levels of EO and ECH
(ethylene chlorohydrin) are within acceptable limits specified by ANSI/AAMI/ISO
10993-7:1995.
D. Shelf Life
Packaging and product integrity studies were conducted to ensure that the shelf life for
each package and product is maintained for a minimum of two (2) years for all of the
Impella Catheters and Impella Purge Cassette. A suite of tests were completed to verify
that two (2) years of aging does not affect key aspects of the device safety or
performance. Testing was also completed to demonstrate packaging integrity for 2 years
of shelf life. All of the shelf tests passed.
X. SUMMARY OF PRIMARY CLINICAL STUDIES
The totality of the human clinical data includes an FDA-approved, prospective, single-
arm study (RECOVER I), data from a retrospective registry, the Impella Registry, a
benchmark analysis comparing device performance with an approved surgical VAD, and
a literature review. This section is focused primarily on RECOVER I. Data from this
clinical trial and the other data are the basis for this PMA approval decision.
RECOVER I Clinical Study
A. Study Design
RECOVER I was a single arm study designed to evaluate the safety, hemodynamic
potency and outcomes of the Impella 5.0/LD in patients presenting with cardiogenic
shock or low cardiac output syndrome post weaning from cardiopulmonary bypass.
Details of the study design are below.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 13
1. Clinical Inclusion/Exclusion Criteria
Inclusion Criteria:
• Signed Informed Consent • Age Eligible (18 ≤ Age ≤ 75) • Body Surface Area (1.5 m2 ≤ BSA ≤ 2.5 m2) • Received stable infusion of one (1) high dose inotrope or two (2)
medium dose inotropes • Cardiac Index (1.3 L/min/m2 ≤ Cardiac Index ≤ 2.2 L/min/m2) after
the respective minimum inotrope infusion time • Elevated Filling Pressures: 30 ≥ PCWP ≥ 20 mmHg OR 35 ≥ PA
Diastolic ≥ 25 mmHg • Time to enrollment within 48 hours of weaning from bypass
Exclusion Criteria
• Concomitant enrollment in another investigational device or drug trial that did not complete the required follow-up
• BUN ≥ 100 mg/dL • Renal dysfunction • Hepatic dysfunction • Presence of any cardiac assist device (other than an IABP) • Right ventricular failure • Evidence of any vascular disease that would have precluded
placement of the device (e.g., severely calcified vessel) • Evidence of LV or RV thrombus • Documented presence of aortic insufficiency • Aortic valve stenosis/calcification • Presence of mechanical aortic valve • Obstructive, hypertrophic cardiomyopathy • Evidence of uncorrected Ventricular Septal Defect or Atrial Septal
Defect (VSD/ASD) or Patent Foramen Ovale (PFO) • Mechanical manifestation of AMI (e.g., ventricular septal rupture,
papillary muscle rupture) • Any disorder causing fragility of blood cells or hemolysis • Patient actively receiving cardiopulmonary resuscitation (CPR) or
any resuscitative maneuver for cardiac arrest • Sustained or non-sustained ventricular tachycardia/ventricular
fibrillation (VT/VF), unresponsive to treatment

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 14
• Other co-morbid condition(s) that could have limited the patient’s ability to participate in the study or impact its scientific integrity
2. Follow-up Schedule
Patients were assessed at 30, 60, 180 days and 1 year. During the assessments,
clinical data was obtained to assess the endpoints below.
3. Clinical Endpoints
Primary Endpoints- • Safety – Frequency of Major Adverse Events:
- Death - Stroke
• Effectiveness – Survival to: - Recovery defined as 30-day survival post-explant or hospital
discharge (whichever is longer) with no other mechanical support or IABP
- Bridge-to-other-therapy defined as induction of anesthesia for surgery for cardiac transplantation OR approved Ventricular Assist Device
Secondary Endpoints- • Safety
- Frequency of other Adverse Events (at 30, 60, 180, 365 days) • Effectiveness
- Improved Hemodynamics – Post-device implant improvements in hemodynamics were to be demonstrated without additional adjunctive inotropic or vasoactive medications versus baseline
- Device Placement and Technical Success - Time-to-Recovery - Reduction in Inotropic/Pressor Support
B. Accountability of PMA Cohort
The study enrolled 17 patients at 7 enrolling sites from October 18, 2006, to June
4, 2008. The overall enrollment for the RECOVER I trial is shown in Figure 5.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 15
Figure 5: RECOVER I enrollment
AMI: Acute Myocardial Infarction; CABG: Coronary Artery Bypass Grafting; FDA: Food and Drug Administration; MVR: Mitral Valve Repair or Replacement; OHT: Orthotopic Heart Transplant; VAD: Ventricular Assist Device
C. Study Baseline Parameters
The baseline patient characteristics and hemodynamics are provided below.
Table 2: Baseline patient characteristics
Patient Characteristic RECOVER I Patients (N=16) [95% CI]
Age Mean±SD(N) 58.38±8.94 (16) [53.61,63.14] Gender – Male 81.25% (13/16) [54.35%,95.95%] Weight (kg) Mean±SD(N) 90.96±23.03 (16) [78.69,103.23] Height (cm) Mean±SD(N) 174.21±10.36 (16) [168.68,179.73] BSA (m2) Mean±SD(N) 2.05±0.28 (16) [1.90,2.20] Race Caucasian 50.00% (8/16) [24.65%,75.35%] African American 31.25% (5/16) [11.02%,58.66%]

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 16
Patient Characteristic RECOVER I Patients (N=16) [95% CI]
Asian Pacific 18.75% (3/16) [4.05%,45.65%] Medical History
CAD 81.25% (13/16) [54.35%,95.95%] Unstable Angina 43.75% (7/16) [19.75%,70.12%] Myocardial Infarction 68.75% (11/16) [41.34%,88.98%] CHF 75.00% (12/16) [47.62%,92.73%] Valve Disease 46.67% (7/15) [21.27%,73.41%] Pacemaker/AICD 12.50% (2/16) [1.55%,38.35%] Peripheral Vascular Disease
14.29% (2/14) [1.78%,42.81%]
Prior Stroke 6.25% (1/16) [0.16%,30.23%] Diabetes Mellitus 37.50% (6/16) [15.20%,64.57%] Hypertension 62.50% (10/16) [35.43%,84.80%] COPD 12.50% (2/16) [1.55%,38.35%]
NYHA Class I 8.33% (1/12) [0.21%,38.48%] II 16.67% (2/12) [2.09%,48.41%] III 25.00% (3/12) [5.49%,57.19%] IV 50.00% (6/12) [21.09%,78.91%] III or IV 75.00% (9/12) [42.81%,94.51%]
Prior Cardiac Procedures Thrombolytic Therapy
18.75% (3/16) [4.05%,45.65%]
PCI 33.33% (5/15) [11.82%,61.62%] CABG 12.50% (2/16) [1.55%,38.35%] Valve Surgery 0.00% (0/16) [0.00%,20.59%] Transplant Surgery 6.25% (1/16) [0.16%,30.23%]
Left Ventricular Ejection Fraction (%) Mean±SD(N) 23.47±7.04 (15) [19.57,27.36] Logistic EuroScore (%) Mean±SD(N) 36.08±26.77 (16) [21.82,50.34]

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 17
Table 3: Baseline hemodynamics
Measurements RECOVER I Patients (N=16) [95% CI] Heart Rate (bpm) Mean±SD (N) 87.3±16.1 (16) [78.7, 95.9] Systolic Arterial Pressure (mmHg) Mean±SD (N) 105.4±20.4 (16) [94.6, 116.3] Diastolic Arterial Pressure (mmHg) Mean±SD (N) 61.0±13.9 (16) [53.6, 68.4] Mean Arterial Pressure (mmHg) Mean±SD (N) 69.3±15.0 (13) [60.2, 78.4] PCWP (mmHg) Mean±SD (N) 14.0±. (1) N/A PA Systolic (mmHg) Mean±SD (N) 45.3±14.8 (16) [37.4, 53.2] PA Diastolic (mmHg) Mean±SD (N) 26.3±10.6 (16) [20.7, 32.0] Cardiac Index (l/min/m2) Mean±SD (N) 1.6±0.4 (12) [1.4, 1.9] CVP (mmHg) Mean±SD (N) 13.9±6.1 (15) [10.5, 17.2] Number of Inotropes Mean±SD (N) 1.56±0.63 (16) [1.23, 1.90] Number of Pressors Mean±SD (N) 0.40±0.63 (15) [0.05, 0.75]
D. Safety and Effectiveness Results
Data for the 16 patients who were consented for the RECOVER I study was
analyzed. The primary endpoint (survival) was met in 88% of the cases. A
Kaplan-Meier curve for survival to 1 year is provided in Figure 6. In addition, the
implant of the Impella 5.0 and the Impella LD in the RECOVER I was successful
in all but one patient. The average support time was 3.7 ± 3 days, with the range
of support from 1.7 days to 12.6 days. The pump provided an overall average
flow during support of 3.8 ± 0.6 L/min.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 18
Figure 6: Kaplan-Meier survival curve for freedom from death (to 1 year)
There were no Unanticipated Adverse Device Effects (UADEs) over the duration
of the RECOVER I trial. There were two (2) serious adverse events (SAEs) (each
effecting one (1) patient), which were adjudicated by a Medical Monitor (per
protocol) as being potentially device-related. One SAE was an incidence of
hemolysis, which fully resolved post-explant. A second SAE was an incidence of
sepsis or bacteremia, which was treated with antibiotics and resolved.
In addition, data was obtained to evaluate the device safety with respect to its
placement across the aortic valve. A total of 50 echocardiograms available on 14
subjects were analyzed by an independent Core Lab research group. The analysis
showed that there was no evidence of structural damage to the heart during use or
in any subsequent follow-up. These results were also submitted to FDA in the
510(k) submission for the Impella 5.0 and Impella LD (K08331), which was
cleared in 2009.
Overall, the RECOVER I study demonstrated that the Impella 5.0 and Impella
LD could be used in the selected patient group, resulting in:
• A high survival rate of treated patients; • A consistent and reproducible hemodynamic support; • A rapid wean of patients off of inotropes and pressors; and • An excellent device safety profile with a low rate of SAEs and other device
related morbidities.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 19
E. Device Failures and Replacements
There were no device failures or replacements reported during the study.
F. Financial Disclosure
The Financial Disclosure by Clinical Investigators regulation (21 CFR 54) requires
applicants who submit a marketing application to include certain information
concerning the compensation to, and financial interests and arrangement of, any
clinical investigator conducting clinical studies covered by the regulation. This
clinical study included 7 investigators. None of the clinical investigators had
disclosable financial interests/arrangements as defined in sections 54.2(a), (b), (c),
and (f). The information provided does not raise any questions about the reliability of
the data.
XI. SUMMARY OF SUPPLEMENTAL CLINICAL INFORMATION
Supplemental data was provided to demonstrate a reasonable assurance of safety and
effectiveness of the Impella devices during use. Results from the Impella Registry for the
real-world use of the Impella catheters were provided. The sponsor also provided a
benchmark comparison of the Impella Registry data to a comparable registry dataset for
its surgical VAD, the AB5000 Ventricle (PMA-approved for a similar indication). As
further evidence, a detailed literature review was provided to support the overall safety
and effectiveness of the Impella devices.
A. Impella Registry
The Impella Registry is an ongoing, multi-center, retrospective, observational
registry for collection of de-identified data for patients treated with the Impella
2.5, Impella CP, Impella 5.0, and Impella LD Support Systems. The registry,
which was started by Abiomed in 2009, is open for participation by qualifying
sites in the U.S. and Canada. A total 59 sites have participated in the registry
since its initiation. As of June 30, 2015, there were 40 open sites. The sites
include high and low volume centers, academic (teaching) and non-academic

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 20
hospitals, public and private institutions as well as for profit and not for profit
centers, almost entirely from the United States. Data is collected at all
participating sites retrospectively without pre-selection of patients, and included
PCCS patients treated with the Impella 2.5, Impella CP, and Impella 5.0/LD
Systems. These registry data were used as supplemental informative clinical data
for FDA review of the Impella Ventricular Support Systems under
P140003/S005, within context of the indications for use.
The data collection from the Impella Registry includes IRB approval, complete
data monitoring, adverse events (AEs) monitoring and CEC adjudication of
major AEs. All data is entered electronically by the sites. For this submission, the
time during which the Impella Registry data was collected is shown in Figure 7.
Eligible patients were those who were reported in the Impella Registry,
underwent open-heart surgery and required mechanical circulatory support with
Impella devices within 48 hours post-surgery.
Figure 7: Time intervals for Impella implants data collection by type of device
Cases were initially identified using Abiomed’s commercial patient tracking
system, and then further reviewed to verify that each case was applicable for this
supplement (i.e., was a PCCS patient). Using this method, seventy-seven (77)
Impella cases were enrolled into the U.S. Impella Registry for this analysis.
These included 19 Impella 2.5 cases, 14 Impella CP cases, and 44 (combined)
Impella 5.0 and Impella LD cases.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 21
The overall results (Kaplan-Meier curve estimates) for survival (to 30 days) for
the patients are shown in Figure 8. Figure 9 provides the results for the different
devices used. Overall outcome results appear favorable for this sick patient
group, particularly when compared to the historical results for similar patients
(see the benchmark and literature review sections below).
Figure 8: Kaplan-Meier curve estimates for 30 day survival – all patients cohort
Figure 9: Kaplan-Meier curve estimates for 30 day survival – for different devices
In addition, analyses were completed using two different classification schemes.
In one analysis, Classification A, the patients were categorized in three (3)

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 22
different groups based on an incremental ascending risk for mortality, which
were: (1) Post-cardiotomy Low Cardiac Output Syndrome (LCOS), (2) Post-
cardiotomy Cardiogenic Shock (PCCS-CS), and (3) Post-cardiotomy Failure to
Wean (PCCS-FW). In the other analysis, Classification B, which was specifically
requested by FDA, the patients were categorized in three (3) different groups, to
evaluate separately patients that received Impella before, during the operating
time (during the surgical procedure) and after the surgery. The groups included in
each category are shown in Figure 10.
Figure 10: Groups used for each Classification analysis
Classification A Classification B
For Classification A, the overall results (Kaplan-Meier curve estimates) for
survival (to 30 days) for the patients are shown in Figure 11. Figures 12, 13 and
14 give the results for the different devices used. The results show that high-risk
patients in whom hemodynamic support is initiated early prior to surgery (LCOS
group) tend to do better than those without support prior to surgery and who
develop cardiogenic shock post-weaning from CPB or those who cannot wean
from CPB.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 23
Figure 11: Kaplan-Meier curve for 30-day survival using Classification A (all patients)
Figure 12: Kaplan-Meier curve for 30-day survival using Classification A (patients with Impella 5.0/LD)
PCCS-LCOSPCCS-CS
PCCS-FW
Log-rank test, p=0.166

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 24
Figure 13: Kaplan-Meier curve for 30-day survival using Classification A (patients with Impella CP)
Figure 14: Kaplan-Meier curve for 30-day survival using Classification A
(patients with Impella 2.5)
For Classification B, the overall results (Kaplan-Meier curve estimates) for
survival (to 30 days) for the patients are shown in Figure 15. Figures 16, 17 and
18 give the results for the different devices used. Using this classification, the
trends suggest that patients with support prior to the procedure have better
outcomes, which mirrors the results observed with Classification A.
PCCS-LCOSPCCS-CS
PCCS-FW
Log-rank test, p=0.166

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 25
Figure 15: Kaplan-Meier curve for 30-day survival using Classification B
(all patients)
Figure 16: Kaplan-Meier curve for 30-day survival using Classification B (patients with Impella 5.0/LD)
Prior index procedure
During index procedureAfter index procedure
Log-rank test, p=0.535

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 26
Figure 17: Kaplan-Meier Curve for 30-Day Survival using Classification B (patients with Impella CP)
Figure 18: Kaplan-Meier Curve for 30-Day Survival using Classification B
(patients with Impella 2.5)
The Impella Registry data provides a real-world perspective on the use of the
device in routine practice in the proposed clinical setting for the Impella devices.
Although some limitations exist with respect to the interpretation of some of the
data, the Impella Registry data showed the following:
• Patients that require hemodynamic support in the setting of PCCS are sick and present with a broad spectrum of pre-existing co-morbidities and risk factors;
• The overall outcomes are favorable; and • Despite the limited sample size, the data suggests that the Impella CP,
Impella 5.0, and Impella LD patients do somewhat better than Impella 2.5 (in the proposed clinical setting).
Prior index procedure
During index procedureAfter index procedure
Log-rank test, p=0.261

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 27
B. Benchmarking Impella vs. Approved VAD in PCCS
In order to provide a benchmark for the Impella devices in a comparable clinical
setting, Abiomed analyzed the results from its real-world registry for the AB5000
Ventricle. The AB5000 Ventricle was PMA approved (P900023/S038) in 2003 as
a temporary VAD for use to treat PCCS. The AB5000 Registry was a
retrospective registry, which included data collected from U.S. sites between
October 3, 2003, and December 11, 2007. The AB5000 Registry included IRB
approval and data for demographics, procedural and hemodynamic
characteristics, outcomes and adverse events.
To better match the two cohorts, AB5000 patients who either received bi-
ventricular or right ventricular support were excluded from the benchmark
analysis. The AB5000 Registry included 1234 patients (387 of which received
only LVAD). Of those patients, 89 were classified as PCCS patients; however,
only 79 cases had enough data to confirm the severity of the presentation (to
serve as the AB5000 benchmark cohort against the Impella Registry cohort). The
Impella Registry benchmark included Impella 5.0/LD patients that presented
either with PCCS-CS or PCCS-FW. The LCOS patients were excluded from the
Impella cohort so the analysis is conservative (considering the invasiveness of the
AB5000, it is very unlikely that it (i.e., the AB5000) was used for LCOS
patients). The Impella 2.5 and Impella CP patients were also excluded since both
the AB5000 and the Impella 5.0/LD provide full flow, whereas the Impella 2.5
and Impella CP only provide partial flow. The selection of cases for the
benchmark comparison is provided schematically in Figure 19.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 28
Figure 19: Flow diagram of the distribution of the AB5000 LVAD PCCS patient cohort
The benchmark analysis included the overall survival to 30 days and to discharge
in the PCCS. The 30-day Kaplan-Meier estimates are provided in Figure 20. For
the survival to discharge, the Impella survival rate (50%) was statistically higher
that the AB5000 survival (15%, p=0.002), as shown in Table 2.
Figure 20: Kaplan-Meier curve estimates for 30 day survival

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 29
Table 2: Site-reported adverse events (to discharge) by Classification
In-Hospital Adverse Events Impella 5.0/LD
Patients (N=24)
AB5000 Patients (N=79) P-value
Death 50.00% (12/24) 84.81% (67/79) 0.002 CVA/Stroke 4.17% (1/24) 20.25% (16/79) 0.112 TIA 0.00% (0/24) 2.53% (2/79) 1.000 Acute Renal Dysfunction/Failure
41.67% (10/24) 29.11% (23/79) 0.318
Hemolysis 8.33% (2/24) 6.33% (5/79) 0.663 Acute Hepatic Failure 16.67% (4/24) 18.99% (15/79) 1.000 Bleeding 45.83% (11/24) 41.77% (33/79) 0.815 Infection 37.50% (9/24) 22.78% (18/79) 0.187 Supraventricular Arrhythmia 12.50% (3/24) 7.59% (6/79) 0.432 Respiratory Dysfunction/Failure
33.33% (8/24) 17.72% (14/79) 0.153
Sepsis 4.17% (1/24) 0.00% (0/79) 0.068 Multi System Organ Failure 8.33% (2/24) 35.44% (28/79) 0.010 Other 29.17% (7/24) 45.57% (36/79) 0.167 CVA: Cerebrovascular accident; TIA: Transient Ischemic Attack
In addition, the rates of site-reported in-hospital adverse events, which were captured in
both registry CRFs, were compared. The results of this comparison are provided in Table
2. Of note, the rate of multi-system organ failure was lower in the Impella Registry PCCS
group, and the stroke rate was also numerically lower compared with the AB5000 PCCS
benchmark cohort. The other site-reported adverse events including bleeding, hemolysis
and infection were comparable between the two cohorts. Given the clinical presentation
of these patients (all undergoing major cardiac surgery), similar bleeding and infection
rates are expected.
Overall, Abiomed’s benchmark analysis revealed that post-cardiotomy patients in the
Impella Registry are comparable with the post-cardiotomy patients treated with the

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 30
AB5000 device. Although the devices provided a similar amount of circulatory support, it
appears that the patients in the Impella Registry had better outcomes than the patients in
the AB5000 Registry.
C. Hemodynamic Effectiveness Results
The Impella Catheters directly unload the left ventricle (LV) and propel blood forward,
from the left ventricle into the aorta, in a manner most consistent with normal physiology.
Impella provides both an active forward flow1,2 and systemic aortic pressure (AOP)
contribution,1,2,3 leading to an effective increase in mean arterial pressure (MAP) and
overall cardiac power output (CPO).1,4 Combined with LV unloading, Impella support
reduces end-diastolic volume and pressure (EDV, EDP) and augments peak coronary
flow,1,2,5,6 leading to a favorable alteration of the balance of myocardial oxygen supply
and demand. This cascade of hemodynamic effects has been described in the literature7
and validated in computational modeling and a variety of pre-clinical and clinical
studies.1-7
For the RECOVER I study (see above), hemodynamic data was collected at baseline and
over time to evaluate the robustness of the hemodynamic support with the Impella 5.0
and Impella LD devices in patients experiencing hemodynamic compromise or
cardiogenic shock post-cardiac surgery. The data collected showed an immediate
improvement of the hemodynamics of PCCS patients post-device implant, as shown in
Figure 17. In addition, as patients’ hemodynamics improved, a rapid and sustained
weaning of inotropic and pressor support was also concomitantly observed, which is
shown in Figure 18.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 31
Figure 17: Improvement in patient hemodynamics (from baseline to 48 hr post-device implant) for RECOVER I patients
A. Cardiac Output (mean±SE)
B. Cardiac Index (mean±SE)
C. Cardiac Power Output (mean±SE)
D. Cardiac Power Index (mean±SE)
E. Mean Arterial Pressure (mean±SE)
F. Pulmonary Artery Diastolic Pressure (mean±SE)

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 32
Figure 18: Decrease in inotropes and pressors (post-device placement) for RECOVER I patients
D. Average number of inotropes infused over time daily (Mean ± SE)
E. Average number of pressors infused over time daily (Mean ± SE)
Additional prospective clinical study data was provided to demonstrate a similar
hemodynamic effect for the Impella 2.5 device.
D. Literature Review
The literature review provided has three different components. The first component is a
review and characterization of the use of Impella in post-cardiotomy cardiogenic shock.
The second component is a comparison of the results of the Impella literature review to a
literature review of Abiomed’s approved surgical VADs (the BVS and AB5000) in
PCCS. The third component is a review of extracorporeal membrane oxygenation
(ECMO) in this population, since ECMO is used as an alternate device to support these
patients as well, albeit off-label.
The Impella review encompassed a large body of scientific evidence with over 230
publications available for review. Included in this Impella PCCS analysis were 223
patients treated for the proposed indications for use. The literature review provides
further insight into the use of the Impella devices in routine clinical practice.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 33
The literature analysis shows that PCCS patients who are deemed to require urgent
hemodynamic support are, in general, older and present with high-risk features and co-
morbidities, poor functional status and greatly depressed cardiac function. Overall, the
use of Impella devices to support these patients appears to be safe and effective based on
the studies published in the literature. The survival rates and morbidities appear to be
favorable for use of the Impella devices as compared to surgical VADs (see table below).

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 34
Impella Publications BVS/AB5000
Lemaire Engström Granfeldt Higgins Siegenthaler Meyns Garatti Pappalardo
PCCS / LOS
patients (range or n)
All patients
(range or n)
Sample Size (thereof PCCS / LOS, if not 100%)
n=47 (68%) n=46
n=33 (88%)
n=35 (19%) n=24
n=16 (56%)
n=12 (25%)
n=10 (50%) 521 841
Pump type 2.5, 5.0 5.0 2.5, 5.0, LD, RD
2.5, 5.0, RD LD 5.0, LD 5.0, LD 2.5, CP
BVS – biV / LV /
RV
BVS – biV / LV /
RV
Age (yrs) 60±13 61±13 58 53±14 66±8 60 36±12 54±15 Mean: 48 - 58 (23-82)
Mean: 40 - 58 (13-82)
Gender (% male) 70 85 73 70 83 69 74 90 61-68 39-78
LVEF (%) 23.6 N/A 67% <30%
N/A N/A N/A N/A N/A N/A N/A
Diabetes (%) 30 41 21 22 N/A 25 N/A N/A N/A 32
Renal insuff. (%) 17 N/A 12 62 N/A N/A N/A N/A N/A N/A
Prior revasc. (%) N/A 81 42 N/A 87 N/A N/A N/A 27-89 49-79
CPR (%) N/A N/A N/A 58 N/A 38 N/A N/A 45 N/A
Mechanical ventilation (%)
N/A 100 21* 97 N/A 100 N/A 100 N/A N/A
Inotropes (%) N/A 100 33* 100 100 100 100 N/A 100 100
IABP (%) N/A 54 25* 40 67 69 75 60 90-94 67 Survival to discharge (%)
79 N/A N/A N/A 50 N/A 42
PCCS: 33
N/A 19-49 27-47
30 day survival (%) 75 39.5 All: 55
LV only: 64 60 N/A
37
N/A N/A 29 38
* before surgery

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 35
The review of ECMO in these same patients yielded a mean survival to either discharge
of 30 days at 33.9% (range 8% to 53%) representing 14 studies and over 1400 patients.
The results of the ECMO review indicate that the use of ECMO, which is a much more
invasive system, yielded a higher morbidity profile during support than the Impella
devices.
Overall, the literature analysis provides further reasonable assurance of safety and
effectiveness of the Impella devices in the proposed indications for use.
XII. PANEL MEETING RECOMMENDATION AND FDA’S POST-PANEL
ACTION
In accordance with the provisions of section 515(c)(3) of the act as amended by the Safe
Medical Devices Act of 1990, this PMA was not referred to the Circulatory System
Devices Panel, an FDA advisory committee, for review and recommendation because the
information in the PMA substantially duplicates information previously reviewed by this
panel.
XIV. CONCLUSIONS DRAWN FROM PRECLINICAL AND CLINICAL
STUDIES
A. Safety Conclusions
There were two potentially device-related serious adverse events in the
RECOVER I study; 1 event of hemolysis, and 1 event of infection. Both events
resolved without clinical sequelae for the patients. The safety profile of the
Impella devices was favorable when compared with the AB5000 surgical VAD in
the benchmark analysis, including a decreased death rate.
B. Effectiveness Conclusions
In the PCCS patient population, the primary outcome of interest is survival to
discharge. Recovery, defined as survival to discharge (or 30 days, whichever was
longer) in RECOVER I was 87.5%. Survival in a PCCS population as recorded in
the Impella Registry shows an approximate survival to discharge rate of 60%.
When registry results were benchmarked against similar data from the AB5000

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 36
surgical VAD registry, a trend for better survival outcomes was observed in favor
of the Impella devices. Historical data from the clinical literature in similar
populations supports this trend when compared with the AB5000 and ECMO.
Additionally, RECOVER I showed improvement in average hemodynamic
parameter values (including cardiac output, cardiac index, cardiac power output,
cardiac power index, mean arterial pressure, and pulmonary artery diastolic
pressure) from baseline to 48 hours post-initiation of support with the Impella
5.0/LD. Other clinical benefits may include decrease in inotropic usage, as
demonstrated in RECOVER I.
In conclusion, given the totality of the information available for the Impella
Ventricular Support Systems, the data demonstrate a beneficial therapeutic effect
in patients experiencing PCCS.
C. Benefit-Risk Conclusions
Patients experiencing PCCS in need of circulatory support due to ongoing
cardiogenic shock refractory to other available therapies are exposed to imminent
risk of mortality if hemodynamic support that results in augmentation of cardiac
output is not provided.
The probable benefits of the device as compared to other available treatments
such as IABP or surgical VADs include potential improved survival to discharge,
improved hemodynamic support, and reduction in the use of inotropes.
The probable risks of the Impella Ventricular Support Systems in this patient
population were evaluated using the RECOVER I study and the supportive data
from the Impella Registry. The safety profile was favorable compared with other
approved VADs. Risks of bleeding and the need for transfusion in general remain
high, mainly driven by the patient’s general situation (not device-related), but are
numerically lower than other surgical VADs. Because most of the risks were
deemed to be procedure-related, results may improve with training.
The benefit-risk evaluation is favorable for use of the Impella 2.5, Impella CP,
and 5.0/LD as temporary ventricular support devices to support hemodynamics

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 37
and augment the circulation in patients who are suffering from PCCS where other
standard therapies (pressors, inotropes, IABP) have failed.
D. Overall Conclusions
The data in this application support the reasonable assurance of safety and
effectiveness of this device when used in accordance with the indications for use.
XV. CDRH DECISION
FDA issued an approval order on April 7, 2016.
The applicant’s manufacturing facilities have been inspected and found to be in
compliance with the Quality System (QS) regulation (21 CFR 820).
The final conditions of approval cited in the approval order are described below.
OSB Lead PMA Post-Approval Study – Impella PCCS PAS: This PAS will be
an observational clinical investigation of post-cardiotomy cardiogenic shock
patients indicated for receipt of an Impella device. A minimum of 44 participants
will be evaluable to compare the survival rate at 30 days or discharge, whichever
is longer, to a performance goal of 30%. It is estimated that 48 participants will be
enrolled, assuming 10% loss to follow-up to 30 days post-procedure. In addition
to survival rates, information on technical success at exit from the catheterization
lab or operating room, device and patient success, descriptions of adverse events
through three months follow-up (as well as one year, when available) and the
adverse event rate at 30 days or discharge, whichever is longer, will be provided.
XVI. APPROVAL SPECIFICATIONS
Directions for use: See labeling (Instructions for Use).
Hazards to Health from Use of the Device: See Indications, Contraindications, Warnings,
Precautions and Adverse Events in the labeling (Instructions for Use).
Post-approval Requirements and Restrictions: See Approval Order.

PMA P140003/S005: FDA Summary of Safety and Effectiveness Data Page | 38
XVII. REFERENCES
1. Burkhoff D et al. The science behind percutaneous hemodynamic support: A
review and comparison of support strategies. Catheter Cardiovasc Interv.
2012;80(5):816–829.
2. Remmelink M et al. Effects of left ventricular unloading by Impella Recover LP
2.5 on coronary hemodynamics. Catheter Cardiovasc Interv. 2007;70(4):532-537.
3. Seyfarth M et al. A randomized clinical trial to evaluate the safety and efficacy of
a percutaneous left ventricular assist device versus intra-aortic balloon pumping for
treatment of cardiogenic shock caused by myocardial infarction. Journal of the American
College of Cardiology. 2008; 52(19): 1584-1588.
4. O'Neill W et al. A Prospective, Randomized Clinical Trial of Hemodynamic
Support With Impella 2.5 Versus Intra-Aortic Balloon Pump in Patients Undergoing
High-Risk Percutaneous Coronary Intervention - The PROTECT II Study. Circulation.
2012; 126 (14): 1717-1727.
5. Sauren LD et al. Combined Impella and Intra-Aortic Balloon Pump Support to
Improve Both Ventricular Unloading and Coronary Blood Flow for Myocardial
Recovery: An Experimental Study. Artificial Organs. 2007;31(11):839-842.
6. Reesink et al. Miniature intracardiac assist device provides more effective cardiac
unloading and circulatory support during severe left heart failure than intraaortic balloon
pumping. CHEST Journal. 2004;126(3):896–902.
7. Naidu S. Novel percutaneous cardiac assist devices: the science of and indications
for hemodynamic support. Circulation. 2011;123(5):533-543.