Embed Size (px)
Citation preview
Jugdeep Dhesi & Jason Cross, Proactive care of older people
undergoing surgery (POPS), Dept of Ageing and Health,
Guy’s and St Thomas’ , London


Average Number of New Cases Per Year and Age-Specific Incidence Rates per 100,000 Population, UK

The NSQIP top 7 EGS Intestinal obstruction, perforation, ischemia, Gallbladder disease, Gastroduodenal ulcer disease, Diverticulitis, Abdominal wall hernia


Mean age 67 years Approx 40% >70 years
0
1,0
00
2,0
00
3,0
00
4,0
00
5,0
00
Patie
nts
<31 31-40 41-50 51-60 61-70 71-80 81-90 >90


McCoy J Trauma Acute Care Surg. 2015;78(5):912-8;
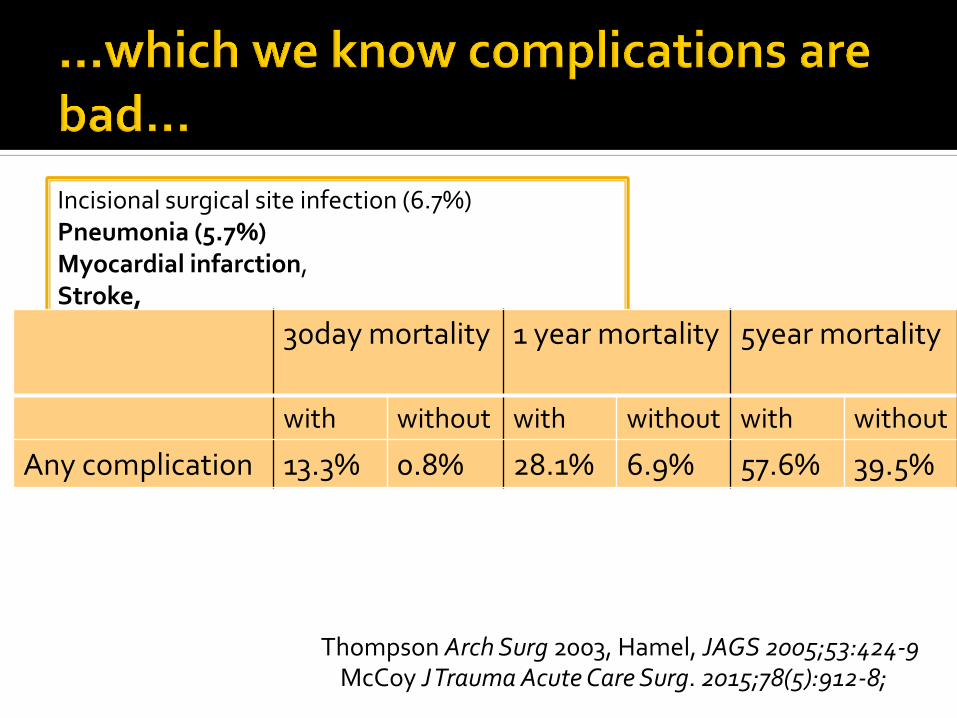
Common postop complications Incisional surgical site infection (6.7%) Pneumonia (5.7%) Myocardial infarction, Stroke, Major bleeding Organ/space surgical site infection, Thromboembolic process, Urinary tract infection
McCoy J Trauma Acute Care Surg. 2015;78(5):912-8;
Incisional surgical site infection (6.7%) Pneumonia (5.7%) Myocardial infarction, Stroke, Major bleeding Organ/space surgical site infection, Thromboembolic process, Urinary tract infection
30day mortality 1 year mortality 5year mortality
with without with without with without
Any complication 13.3% 0.8% 28.1% 6.9% 57.6% 39.5%
Thompson Arch Surg 2003, Hamel, JAGS 2005;53:424-9

McCoy J Trauma Acute Care Surg. 2015;78(5):912-8;
Incisional surgical site infection (6.7%) Pneumonia (5.7%) Myocardial infarction, Stroke, Major bleeding Organ/space surgical site infection, Thromboembolic process, Urinary tract infection
30day mortality 1 year mortality 5year mortality
with without with without with without
Any complication 13.3% 0.8% 28.1% 6.9% 57.6% 39.5%
CONCLUSION: Of the potential postoperative targets for quality improvement, pneumonia, myocardial infarction, stroke, and major bleeding have the strongest associations with subsequent mortality. Since pneumonia is both relatively common after emergency surgery and strongly associated with postoperative death, it should receive priority as a target for surgical quality improvement initiatives.

Copyright © 2016 American Medical
Association. All rights reserved.
Percentage of Patients Discharged to Postacute Care (PAC)
Facilities According to Age, Number of Postoperative
Complications, and Functional Status
…as well as on patient reported outcomes
Lawrence J Am Coll Surg 2004 JAMA Surg. 2016;151(8):759-766


Barnett, Lancet 2012

• 4 in 5 high risk patients to general ward
• Management on wards by junior staff
• Poor recognition of medical problems
• Reliance on on-call staff • Multiple medical team
involvement

Assessment of risk
Modification of risk
Care in the right place
Optimal management of complications
Documentation of outcomes that matter
Shared decision making

Right team at the right time in the right place Preoperatively
Screening, assessment and investigation
Optimisation
Shared decision making (Advanced care planning)
Intraoperatively
Timely, tailored surgical and anaesthetic care
Right destination
Postoperatively
Proactive identification & standardised mx of comps ▪ Surgical, medical, rehabilitation and discharge planning


70% describe inadequate training in mx of complex older patients
85% often need medical advice
68% difficulty in accessing medical support
92% felt need for closer collaboration
Ideal components of a collaborative geriatric medicine-surgical service
Medical Optimisation 79%
Mental Capacity Assessment 71%
Quantifying Medical Risks of Surgery
64%
Managing Medical Complications
87%
Communication with patients and families
38%
Post-op rehab/ discharge planning
92%
Shipway J Surg Ed 2015

‘Routine daily input from medicine for older people should be available to elderly patients undergoing surgery and is integral to inpatient care pathways in this population’ An Age Old Problem 2010
‘Geriatricians play a key role in helping to evaluate
and manage risk and promoting shared decision approaches. Effective MDT working to bring together physician, surgeon, anaesthetist and geriatrician is critical’ Access All Ages 2012
‘Geriatricians should work more closely alongside teams both inside and outside hospital’ RCS Nov 2014
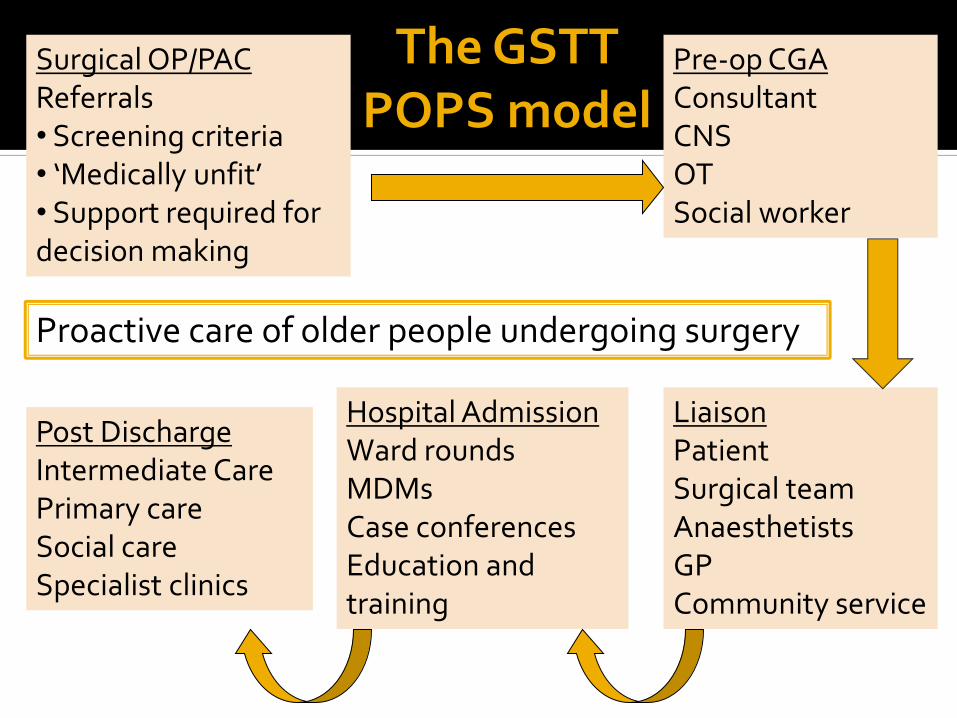
Surgical OP/PAC Referrals • Screening criteria • ‘Medically unfit’ • Support required for decision making
Pre-op CGA Consultant CNS OT Social worker
Hospital Admission Ward rounds MDMs Case conferences Education and training
Post Discharge Intermediate Care Primary care Social care Specialist clinics
Liaison Patient Surgical team Anaesthetists GP Community service
The GSTT POPS model
Proactive care of older people undergoing surgery


Parameter Screening Assessment
Physiological status
Reported exercise tol
METS
Multimorbidity Disease specific tools
Frailty Simple question EFS
Cognition 4AT MoCA
Nutrition MUST Dietitician
Social/function Structured history
Barthel, NEADL
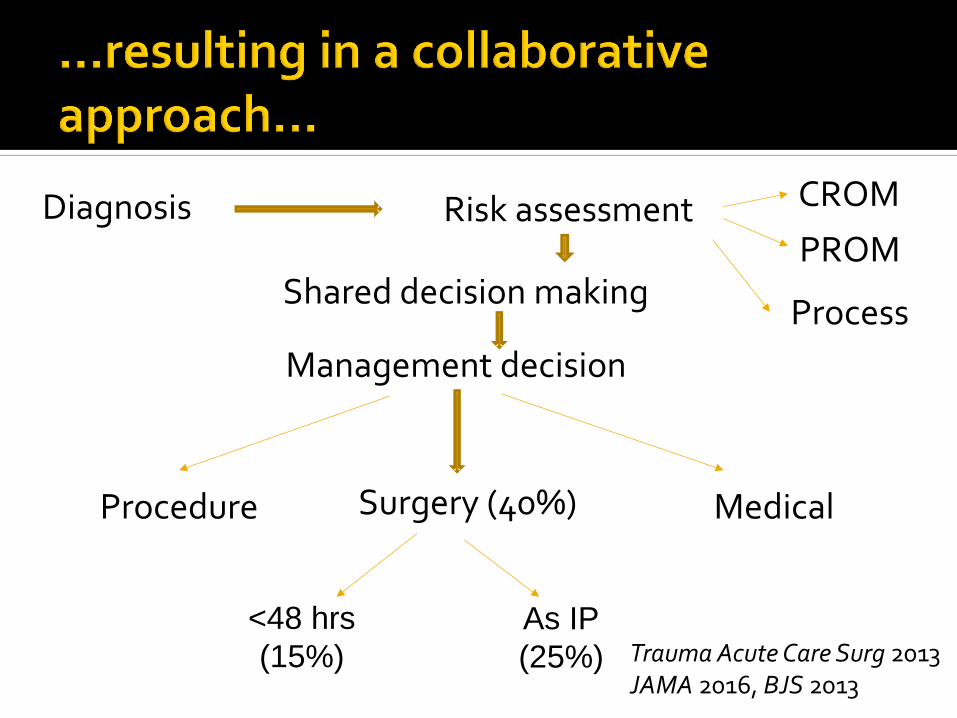
Diagnosis
Management decision
Surgery (40%) Procedure Medical
As IP
(25%)
<48 hrs
(15%) Trauma Acute Care Surg 2013 JAMA 2016, BJS 2013
Risk assessment CROM
PROM Shared decision making
Process
Preoperative care (inc conservative management)
Medical optimisation
Fluids, AKI, delirium, sepsis, drug management
Communication with patient/carers
Capacity, consent, shared decision making
Advance care planning – ceilings of care
Communication across teams to optimise mx
Focus on reducing risk of predictable comps
Ensuring proactive approach to diagnosis & mx

Ensuring continuity of postoperative care
NEWS/Medical/geriatric complications Psychological health mx Goal setting/rehabilitation Discharge planning
POC, ICT, care home
Communication
Patient
Family/carers
Primary/community care
Nursing handover Surgical handover Joint ward rounds MDTMs Physical presence

Partridge, Age & Ageing 2014
NELA data shows that for patients ≥70 years 10% assessed postop by EM 1/5 hospitals 0% assessed by EM


Ensuring a clear focus
Courtesy of
Dr Vilches-Moraga
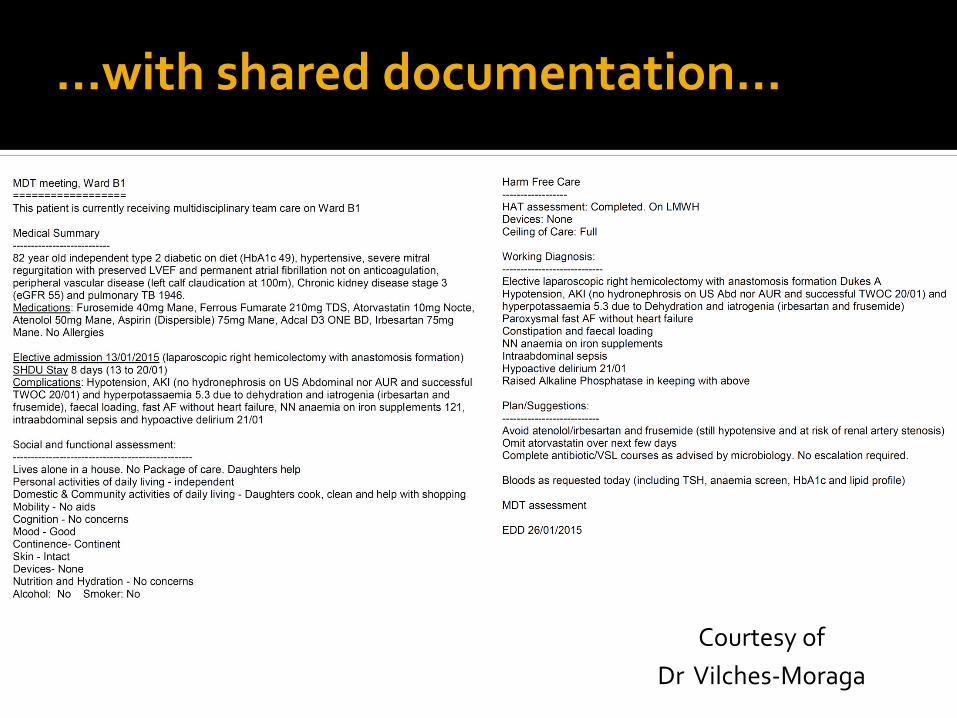
…with shared documentation…
Courtesy of
Dr Vilches-Moraga

…resulting in…
Before February 1st 11 Median
After February1st 7 Median
Length of stay (mean 13 median 9)(↓ 4 days) 30 day readmission rate (↓ 13.2%) Times seen by non surgical doctor (↓ 18%) Medication reviews (↑51%) Coding/recognition complications ↑↑ Coding comorbidities ↑↑
Courtesy of
Dr Vilches-Moraga

Chelmsford
Imperial
Belfast Edinburgh
Nottingham
Guildford
Southmead
North Tees Salford
GSTT, London
Cambridge
Kings, London
Oxford
Portsmouth
Royal Free, London
Derby
Leicester

(Ann Surg 2016;264:437–447)

76 year old gentleman Incarcerated hernia Requires emergency surgery Discussed at EGS handover meeting
Concerns raised
Nursing home resident
Patient confused ‘has dementia’
Would palliative care be more appropriate

CGA on the ward PMH
Confused and agitated
Atrial fibrillation on warfarin
HTN
Osteoarthritis / multiple joints / severe
Collateral History from family / care home
▪ Residential care
▪ MCI
▪ Independent with personal cares
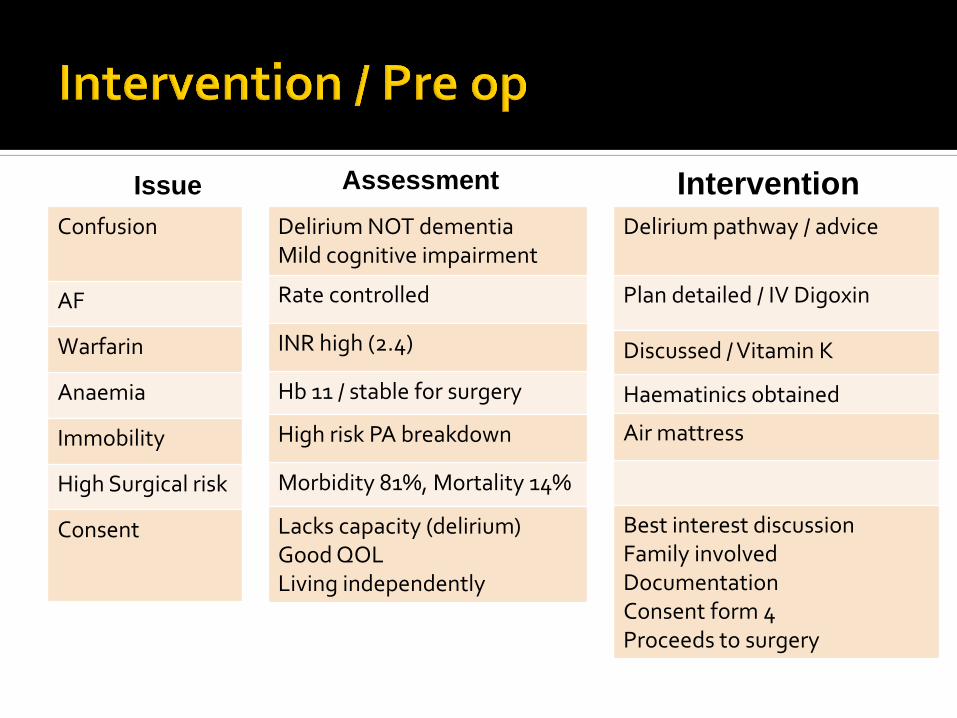
Confusion
AF
Warfarin
Anaemia
Immobility
High Surgical risk
Consent
Delirium pathway / advice
Plan detailed / IV Digoxin
Discussed / Vitamin K
Haematinics obtained
Air mattress
Best interest discussion Family involved Documentation Consent form 4 Proceeds to surgery
Delirium NOT dementia Mild cognitive impairment
Rate controlled
INR high (2.4)
Hb 11 / stable for surgery
High risk PA breakdown
Morbidity 81%, Mortality 14%
Lacks capacity (delirium) Good QOL Living independently
Issue Assessment Intervention

Ileus
AF
AKI
Delirium
Functional decline
Dietetic review TPN
IV Digoxin /Advice / pathway
Fluid resus / Pathway followed
Haloperidol (not used) / pathway
Early therapy Rehab referral
Albumin dropping NMB prolonged
Fast rate
Baseline 3a 20% increase in Cr
Acute / multi-factorial
Global weakness Deconditioned
Issue Assessment Intervention
Delirium resolved day 5 post op 14 day IP stay Early therapy input facilitates d/c to rehab unit 4 week stay at rehab – back to residential care

89 year old lady / on admissions
ward
Proactive case finding with assessment
Multimorbidty
Abdominal pain
No surgical issues / requesting transfer
to elderly care
Nurses report patient has care
needs / daughter struggling

Constipation
Frail with functional
Social care
Laxatives prescribed / advice
OT referral and assessment
Discussed / advice / community ref
Faecal loading on imaging
Risk of falls / increased care
Living with daughter / requesting care input
Issue Assessment Intervention
Proactive case funding with holistic
assessment
Admission avoidance with
appropriate community referral

Delivering evidence based clinical practice
Do we have the evidence to inform practice ?
How do we translate into routine care?
Education and training
Is our workforce ready? Which workforce?
How do we ensure they are?
Research and QIP
Making it relevant to the ‘messy’ patient, the context and the workforce

NELA, EBPOM www.popsteam.co.uk British Geriatrics Society POPS SIG (www.bgs.org.uk) POPS annual education conf (March, register via BGS) POPS Clinical Fellow posts (advertised every April) RCoA Perioperative medicine programme UCL Perioperative Medicine MSc Age Anaesthesia Association (May 2017) [email protected]


Clinical services
Patient not specialty centred services
Whole system reorganisation (cultural change)
Funding (CCGs)
Workforce/education/training
Surgeons, anaesthetists, physicians, geriatricians
Alternative workforce – ANP
Research
Patient centred, new methodologies

Cognitive impairment Functional impairment Undernutrition Frailty

Three way between geriatricians, surgeons, anaesthetists
Health care professionals across disciplines
Surgical teams, nursing staff, therapists
e.g. AF, delirium, catheter related issues, rehabilitation
Patient and carers
e.g. delirium, rehabilitation
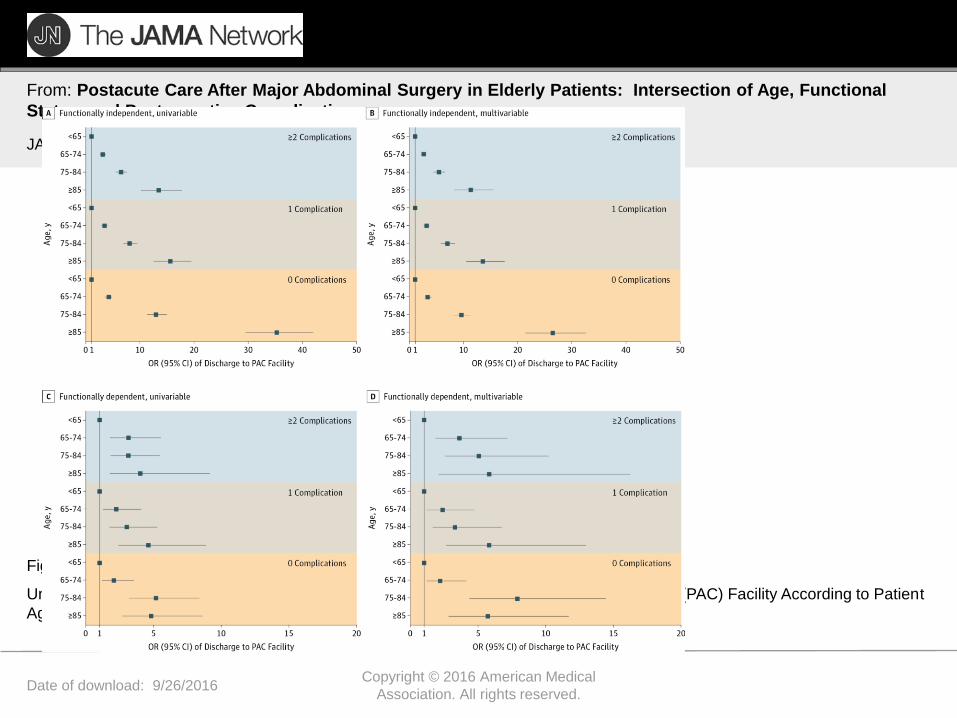
Date of download: 9/26/2016 Copyright © 2016 American Medical
Association. All rights reserved.
From: Postacute Care After Major Abdominal Surgery in Elderly Patients: Intersection of Age, Functional
Status, and Postoperative Complications
JAMA Surg. 2016;151(8):759-766. doi:10.1001/jamasurg.2016.0717
Univariable and Multivariable Estimates for Odds Ratio (OR) of Discharge to Postacute Care (PAC) Facility According to Patient
Age, Number of Postoperative Complications, and Functional Status
Figure Legend:

Date of download: 9/26/2016 Copyright © 2016 American Medical
Association. All rights reserved.
From: Postacute Care After Major Abdominal Surgery in Elderly Patients: Intersection of Age, Functional
Status, and Postoperative Complications
JAMA Surg. 2016;151(8):759-766. doi:10.1001/jamasurg.2016.0717
Percentage Discharged to Each Postacute Care (PAC) Setting for Functionally Independent and Dependent Patients by Number of
Postoperative Complications
Figure Legend:

“With an ageing population
there are more patients who
we’re now being able to offer
surgery to that previously we
weren’t. What that means is that
the volume of the workload is
increasing but, also, the
complexity of the workload that
we’re undertaking is getting
greater. And ... their
expectations are very high.”
(Interview participant)

Wilson Br J Anaesth 2010;105:297 Roche BMJ 2005;331:1374 Makary 2010 Partridge Age & Ageing 2012;41:142
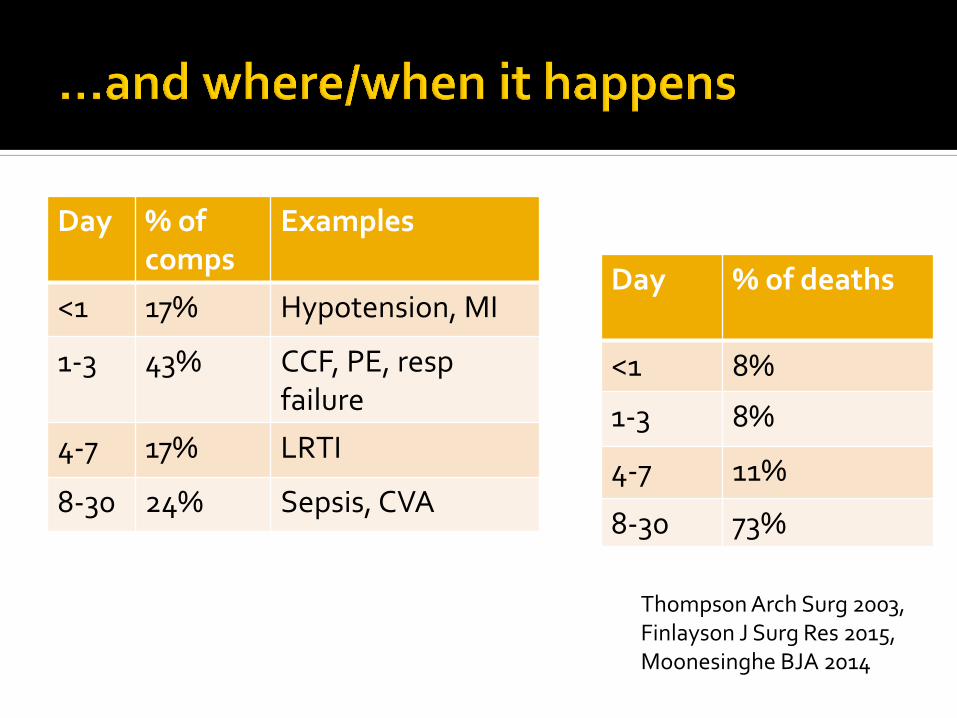
Day % of comps
Examples
<1 17% Hypotension, MI
1-3 43% CCF, PE, resp failure
4-7 17% LRTI
8-30 24% Sepsis, CVA
Day % of deaths
<1 8%
1-3 8%
4-7 11%
8-30 73%
Thompson Arch Surg 2003, Finlayson J Surg Res 2015, Moonesinghe BJA 2014



27.7 million EGS admissions Over 10 yr period admissions increased by 27.5% 30% required surgery Mean age 58.7yrs
J Trauma Acute Care Surg 2014;77(2):202-8.