Embed Size (px)
Citation preview

Hypofractionated radiotherapy for
early (operable) breast cancer:
technical document
Part 1 - Hypofractionated Radiotherapy Systematic
Review Update 2014
Part 2 - Overview of Left vs Right sided tumour
evidence October 2014
Part 3 - Hypofractionated Radiotherapy Systematic
Review 2011
November 2014

Hypofractionated radiotherapy for the
treatment of early breast cancer
An updated systematic review
August 2014

Hypofractionated radiotherapy for the treatment of early breast cancer: an updated systematic review, was
prepared and produced by:
Cancer Australia
Locked Bag 3 Strawberry Hills NSW 2012 Australia
Tel: +61 2 9357 9400 Fax: +61 2 9357 9477
Website: www.canceraustralia.gov.au
© Cancer Australia (2014)
ISBN Online: 978-1-74127-266-6
Copyright statement:
Internet sites
This work is copyright. You may download, display, print and reproduce the whole or part of this work in unaltered
form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only
if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice
and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act
1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the
whole or any part of this work in any way (electronic or otherwise) without first being given the specific written
permission from Cancer Australia to do so. Requests and inquiries concerning reproduction and rights are to be sent
to the Publications and Copyright contact officer, Cancer Australia, Locked Bag 3, Strawberry Hills, NSW 2012
Copies of Hypofractionated radiotherapy for the treatment of early breast cancer: an updated systematic review
can be downloaded from the Cancer Australia website: www.canceraustralia.gov.au or ordered by telephone: 1800
624 973.
Recommended citation
Cancer Australia. Hypofractionated radiotherapy for the treatment of early breast cancer: an
updated systematic review. Cancer Australia, Surry Hills, NSW, 2014.

Hypofractionated radiotherapy for the treatment of early breast cancer iii
Contents
Acknowledgments ............................................................................................................................... v
Executive summary ............................................................................................................................ vii
1 Background .............................................................................................................................. 1
1.1 Breast cancer in Australia ...............................................................................................1
1.2 Use of radiotherapy for the treatment of early breast cancer ...............................1
1.3 Existing Cancer Australia clinical practice guidelines ..............................................2
2 Methods .................................................................................................................................... 3
2.1 Inclusion criteria ................................................................................................................3
2.2 Literature search ..............................................................................................................3
2.3 Exclusion criteria ...............................................................................................................4
2.4 Data extraction ................................................................................................................5
2.5 Quality assessment ..........................................................................................................5
3 Results ........................................................................................................................................ 7
3.1 International guidelines ..................................................................................................7
3.2 Systematic reviews ...........................................................................................................8
3.3 Randomised controlled trials .........................................................................................8
3.4 Ongoing trials ................................................................................................................. 16
4 Discussion ............................................................................................................................... 18
5 Conclusion .............................................................................................................................. 21
Appendix A Contributors.................................................................................................................... 22
Appendix B Literature databases searched ................................................................................... 23
Appendix C Search strategy ............................................................................................................. 24
Appendix D Guideline and clinical trial sites searched ................................................................ 25
Appendix E Flowchart of inclusion/exclusion ................................................................................. 26
Abbreviations ...................................................................................................................................... 27
References ........................................................................................................................................... 28

iv Hypofractionated radiotherapy for the treatment of early breast cancer
Tables
Table 1 Study characteristics of included RCTs from new publications .................................... 1
Table 2 Patient characteristics of included RCTs from new publications ................................. 2
Table 3 Study characteristics of conference abstracts ................................................................ 2
Table 4 All-cause mortality reported in START A and START B trials (2013)17 .............................. 3
Table 5 Causes of death in START A and START B trials (2013)17 .................................................. 3
Table 6 Any breast cancer-related events reported in START A and START B trials
(2013)17 ..................................................................................................................................... 4
Table 7 Cumulative incidence-free estimates reported by Spooner et al (2012)19 ................ 5
Table 8 START A and START B relapses17 ........................................................................................... 6
Table 9 Physician-assessed normal tissue effects by fraction schedule in START A
(2013)17 ................................................................................................................................... 11
Table 10 Physician-assessed normal tissue effects by fraction schedule in START B
(2013)17 ................................................................................................................................... 12
Table 11 Incidence of other late adverse effects according to fractionation
schedule in START (2013)17 .................................................................................................. 13
Table 12 Change in photographic breast appearance at 2 years by fractionation
schedule20 ............................................................................................................................. 14
Table 13 Acute skin reactions during treatment by fractionation schedule in UK FAST
trial (2011)20 ........................................................................................................................... 15

Hypofractionated radiotherapy for the treatment of early breast cancer v
Acknowledgments
Funding
The development of this report was funded by the Australian Government through Cancer
Australia.
Contributors
Cancer Australia gratefully acknowledges the support of the many individuals and groups
who contributed to the development of this report. See Appendix A
Hypofractionated radiotherapy for the treatment of early breast cancer: an updated
systematic review was developed with input from an expert multidisciplinary Working Group
with the following members:
Dr Marie-Frances Burke (Chair) Radiation Oncologist
Ms Jan Rice Breast Care Nurse
Dr Patsy Soon Breast Surgeon
Dr Kirsty Stuart Radiation Oncologist
Ms Bronwyn Wells Consumer Representative


Hypofractionated radiotherapy for the treatment of early breast cancer vii
Executive summary
Cancer Australia published clinical practice guidelines on the use of hypofractionated
radiotherapy for early (operable) breast cancer in November 2011. The guidelines were
based on a Cancer Australia systematic review which included available evidence from
randomised controlled trials (RCTs) published between January 2001 and March 2010. The
RCT evidence in the first systematic review came from five trials: RMH/GOC, Canadian trial,
two Standardisation of Breast Radiotherapy Trials (START A and START B) and Spooner. At that
time full publications were available for the first four of these, whilst the Spooner trial was
described in abstract form only.
Since the publication of the 2011 Cancer Australia clinical practice guidelines, further
evidence on hypofractionated radiotherapy for the treatment of early breast cancer has
been published, including 10 year follow-up results from the two START trials. The current
systematic review was undertaken to identify new and updated evidence on the use of
hypofractionated radiotherapy for the treatment of early breast cancer following surgery
and to support the update of Cancer Australia’s 2011 clinical practice guidelines.
An updated literature search of electronic databases was undertaken in November 2013
(search span from January 2010 to November 2013) to identify relevant literature published
since the 2011 systematic review search dates. The primary search was limited to randomised
controlled trials conducted in humans published in the English language.
The literature search identified one new RCT (UK FAST 2011) and updated full publications
from trials included in the first systematic review: the START A, START B trials (Haviland 2013)
and the Spooner trial (Spooner 2012). Three further RCTs were identified that have only been
published as conference abstracts to date. The updated search identified three international
guidelines , but no systematic reviews. One meta-analysis (of START A, START B, and their pilot
trial RMH/GOC) was identified in the search (Haviland 2013).
Standard radiotherapy is typically delivered over a period of five to six weeks using a
standard 2 Gy (Gray) radiation dose per fraction, in 25 to 30 fractions, to a total dose of 50 to
60 Gy.1 Hypofractionated radiotherapy involves fewer, larger-dose radiation treatments that
are usually delivered over a shorter time period compared to standard radiotherapy
regimens.2 The total dose of radiation used in a course of hypofractionated radiotherapy is
reduced to compensate for the increased toxicity of larger daily fractions.
With regard to overall survival, all RCTs have demonstrated that hypofractionated
radiotherapy is equivalent or superior to conventionally fractionated radiotherapy. The START
B trial reported a statistically significantly higher overall survival rate and significantly longer
disease-free survival in the hypofractionated radiotherapy arm compared with the standard
radiotherapy arm. The START A trial reported no significant difference in all-cause 10 year
mortality rates between the hypofractionated radiotherapy schedules and standard
radiotherapy. Spooner et al (2012) reported no significant difference between
hypofractionated radiotherapy and standard radiotherapy schedules for 2, 5, 10 and 15 year
overall survival estimates. The Spooner trial also reported similar 2, 5, 10 and 15 year relapse-
free survival estimates and cumulative incidence-free estimates between the
hypofractionated radiotherapy and standard radiotherapy regimens.

viii Hypofractionated radiotherapy for the treatment of early breast cancer
Local relapse rates were similar between hypofractionated radiotherapy regimens and
standard radiotherapy for START A, START B and the Spooner 2012 trials. START A and START B
also reported no significant difference in 10 year local-regional relapse rates between
hypofractionated radiotherapy schedules and standard radiotherapy.
START B reported significantly fewer distant relapses at 10 years in patients receiving
hypofractionated radiotherapy (40 Gy in 15 fractions over 3 weeks) compared with patients
receiving standard radiotherapy.
Moderate or marked breast shrinkage, telangiectasia, and breast oedema were
experienced significantly less ofen in patients who received hypofractionated radiotherapy
regimens of 39 Gy in 13 fractions over 5 weeks in the START A trial and 40 Gy in 15 fractions
over 3 weeks in the START B trial compared with patients receiving standard radiotherapy.
The UK FAST trial reported increased risk for mild or marked change in 2 year photographic
breast appearance for patients in the hypofractionated radiotherapy group (30 Gy in 5
once weekly fractions of 6.0 Gy) compared with conventionally fractionated radiotherapy,
and compared with the hypofractionated radiotherapy schedule of 28.5 Gy in 5 once
weekly fractions of 5.7 Gy. Results were comparable between the 28.5 Gy schedule and 50
Gy. Three-year rates of physician-assessed moderate/marked adverse effects in the breast
were also significantly higher in the hypofractionated radiotherapy group of 30 Gy in 5 once
weekly fractions of 6.0 Gy compared with the standard radiotherapy group and the
hypofractionated radiotherapy group of 28.5 Gy in 5 once weekly fractions of 5.7 Gy. The
rates were similar between the 28.5 Gy and 50 Gy groups

Hypofractionated radiotherapy for the treatment of early breast cancer 1
1 Background
1.1 Breast cancer in Australia
In 2009, breast cancer was the most common cancer in Australian women (excluding non-
melanoma skin cancer), accounting for 27.4 per cent of all new cancers in women.3 In 2014
it is estimated that 15,800 women will be diagnosed with breast cancer in Australia.4 At the
end of 2008, it was estimated that there were 159,325 Australian women alive who had been
diagnosed with breast cancer in the previous 27 years, including 57,327 women diagnosed in
the previous 5 years.5
1.2 Use of radiotherapy for the treatment of early breast cancer
Early breast cancer is defined as tumours not more than five centimetres in diameter, with
either impalpable or palpable but not fixed lymph nodes and with no evidence of distant
metastases.6 Breast conserving surgery (BCS) plus radiotherapy is a standard alternative to
mastectomy for eligible patients with stage I or II invasive breast cancer.2 A meta-analysis by
the Early Breast Cancer Trialists Group (EBCTG) of 10,801 women from 17 randomised trials of
radiotherapy vs. no radiotherapy following breast conserving surgery reported that following
BCS, radiotherapy to the conserved breast halves recurrence rates and reduces breast
cancer death rate by about a sixth.7
Standard radiotherapy is typically delivered over a period of five to six weeks using a
standard 2 Gy (Gray) radiation dose per fraction (treatment), in 25 to 30 fractions, to a total
dose of 50 to 60 Gy.1 Hypofractionated radiotherapy has been demonstrated to have
comparable outcomes to standard radiotherapy in recent randomised controlled trials
(RCTs).2,8 Hypofractionated radiotherapy involves fewer, larger-dose radiation treatments
that are usually delivered over a shorter time period compared to standard radiotherapy
regimens.2 As each daily fraction is larger than a conventional daily fraction and the
radiation therapy is delivered in a shorter time period; the total delivered dose of radiation is
reduced, to account for the more intense treatment. Based on radiobiological principles,
calculations using the number of fractions (time), total dose, dose per fraction and the
alpha-beta ratio, indicate the hypofractionated biological effective dose is often similar to a
conventional dose.
Sensitivity of tissues to radiation fraction size is described by the α/β ratio. Lower α/β values
indicate greater sensitivity to fraction size than higher α/β values.9 It has been hypothesised
that breast cancer is as sensitive to fraction size as normal breast tissue with a low α/β value,
and confirmation from the RMH/GOC trial of hypofractionated radiotherapy would indicate
that fewer, larger fractions are as effective as conventional 2 Gy fractions.9
The National Breast Cancer Audit reported that in Australia most breast cancer patients
receive radiotherapy following BCS (86%) and 71% of patients who undergo mastectomy
with large tumours (>5cm) receive radiotherapy.10

2 Hypofractionated radiotherapy for the treatment of early breast cancer
1.3 Existing Cancer Australia clinical practice guidelines
Cancer Australia published clinical practice guidelines on the use of hypofractionated
radiotherapy for early (operable) breast cancer in November 2011.11 The guidelines were
based on a Cancer Australia systematic review which included available evidence from
randomised controlled trials published between January 2001 and March 2010. The 2011
clinical practice guideline included the following:
In women with early breast cancer who require post-operative whole breast radiotherapy
and for whom hypofractionated radiotherapy is being considered, women should be
informed of the potential benefits and risks, and potential side effects and adverse events
of hypofractionated radiotherapy and conventionally fractionated radiotherapy.
Hypofractionated radiotherapy can be offered as a suitable alternative to conventionally
fractionated radiotherapy for women:
aged 50 years and over
with pathological stage T1-2, N0, M0
with low or intermediate histologic grade breast cancer
who have undergone breast conserving surgery
with clear surgical margins
There is insufficient evidence to make a recommendation for or against the use of
hypofractionated radiotherapy for women:
aged less than 50 years
with pathologic stage T3+ and/or N1+ tumour
with high histologic grade breast cancer
who are treated with total mastectomy
who receive chemotherapy and/or targeted biological therapies
Optimal schedule:
Recommended hypofractionated schedules for whole breast radiotherapy, based on
current evidence are:
42.5 Gy in 16 fractions given at the rate of one fraction per day, 5 fractions per
week over 22 days
40 Gy in 15 fractions given at the rate of one fraction per day, 5 fractions per
week over 21 days
Adverse events and toxicity
When selecting an appropriate radiotherapy schedule, consideration should be given to
the possibility of adverse events including early acute reactions and late toxic effects

Hypofractionated radiotherapy for the treatment of early breast cancer 3
2 Methods
The current systematic review addresses the following research question:
1. What is the effectiveness of hypofractionated radiotherapy compared to
conventionally fractionated radiotherapy for the treatment of early breast cancer?
2.1 Inclusion criteria
Participants
Women with early (invasive) breast cancer treated with surgery (BCS or mastectomy).
Intervention/comparison
Hypofractionated radiotherapy following surgery compared with either:
a) Standard radiotherapy following surgery
b) Other regimens of radiotherapy following surgery.
Outcome measures
Outcome measures of interest were:
Overall survival
Disease-free survival
Recurrence
Adverse events
Toxicity
Cosmetic outcomes
Quality of Life (QoL).
2.2 Literature search
A systematic literature search was conducted in November 2013 to identify relevant studies
which addressed the inclusion criteria. The search was conducted using several databases
(see Appendix B), including:
4 Hypofractionated radiotherapy for the treatment of early breast cancer
Medline
Embase
Pubmed
Cochrane Library.
The search strategy, based on the previous systematic review, used combined key terms
which described early (invasive) breast cancer and hypofractionated radiotherapy (see
Appendix C). The primary search was limited to randomised controlled trials (RCTs)
conducted in humans which were published from January 2010 to November 2013 in the
English language.
After the removal of duplicates and the addition of further citations identified via cascade
searching, a total of 384 unique citations remained. The titles and abstracts of these citations
were assessed independently by two reviewers to determine eligibility for the current review
based on the criteria described previously. Ineligible studies were classified using the
exclusion criteria below. For citations which provided insufficient information to assess
eligibility, the full text was retrieved for assessment, by the same two reviewers.
In addition to the above databases, guidelines and clinical trial websites were searched for
relevant information. Specific international guideline organisations were searched as well as
the National Guidelines Clearinghouse and the Guidelines International Network (GIN)
guideline database. Clinical trial sites searched included clinical trials.gov (USA) and
controlled trials.com (UK). Further information on sites can be found in Appendix D.
The following websites were searched from January 2010 to November 2013 to identify
recently published abstracts about hypofractionated radiotherapy for early breast cancer:
American Society of Clinical Oncology (ASCO)
San Antonio Breast Cancer Symposium (SABCS)
2.3 Exclusion criteria
Papers were excluded if they met any of the following criteria:
Inappropriate study type: studies other than randomised controlled trials
Inappropriate population: studies in a population other than as defined in the
inclusion criteria
Inappropriate interventions: studies not investigating hypofractionated radiotherapy
regimens as defined in the inclusion criteria
Inappropriate outcomes: studies not reporting on one or more the outcomes defined
in the inclusion criteria
Not published in the English language
Published prior to 2010.
Based on these criteria, 299 articles were excluded. The full texts of the remaining 85 citations
were retrieved and assessed to identify which met the inclusion criteria for the review. After
full text assessment, nine citations were identified as eligible for the current review (see
Appendix E).
Hypofractionated radiotherapy for the treatment of early breast cancer 5
2.4 Data extraction
Data extraction was performed by two reviewers and verified by both to ensure accuracy.
Descriptive data extracted from these studies included characteristics of the patient
population, study interventions and primary outcomes.
Outcome data extracted from the studies included overall survival, local recurrence,
adverse events, toxicity, cosmetic outcomes and quality of life.
2.5 Quality assessment
Primary studies included in the systematic review were critically appraised according to
criteria previously published by the National Health and Medical Research Council (NHMRC).
The following questions were considered:
Was an appropriate method used for treatment assignment?
Was there control of selection bias after treatment assignment (such as intention to
treat analysis, minimal patients lost to follow-up)
Was the study blinded?
Was there standardised outcome assessment (if blinding was not possible)?
Were groups well matched at baseline?
Was the study powered to detect a difference in primary outcome?
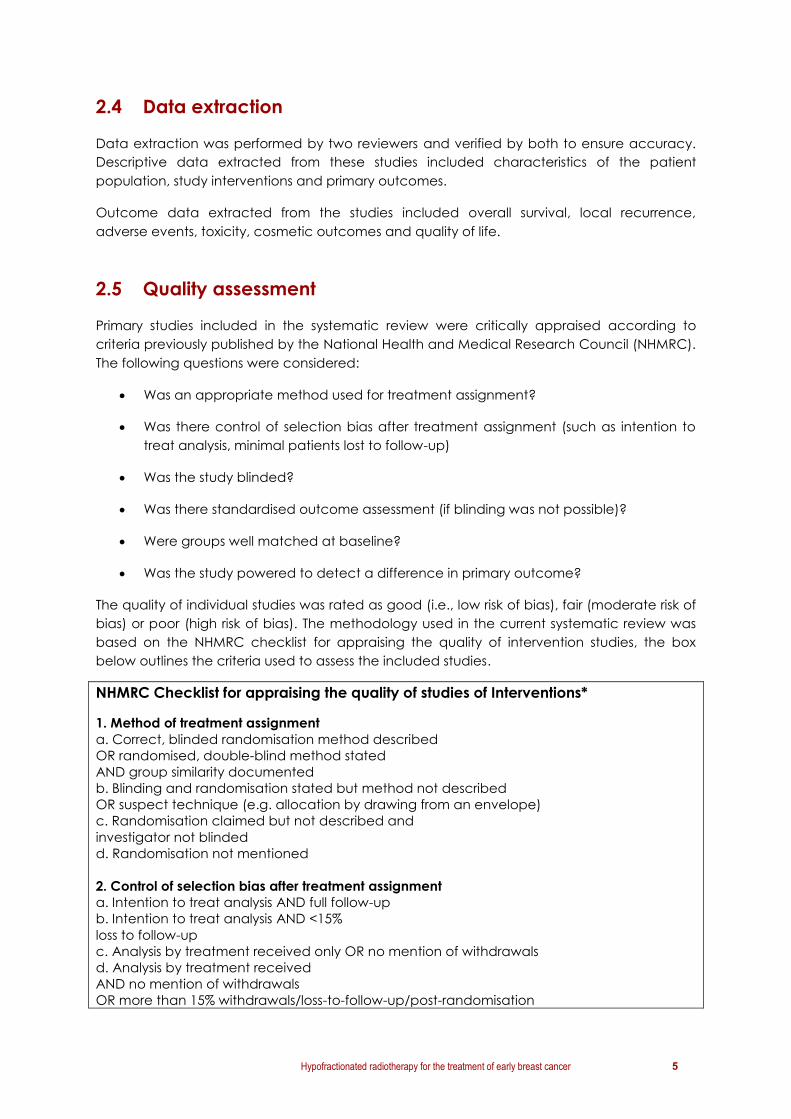
The quality of individual studies was rated as good (i.e., low risk of bias), fair (moderate risk of
bias) or poor (high risk of bias). The methodology used in the current systematic review was
based on the NHMRC checklist for appraising the quality of intervention studies, the box
below outlines the criteria used to assess the included studies.
NHMRC Checklist for appraising the quality of studies of Interventions*
1. Method of treatment assignment
a. Correct, blinded randomisation method described
OR randomised, double-blind method stated
AND group similarity documented
b. Blinding and randomisation stated but method not described
OR suspect technique (e.g. allocation by drawing from an envelope)
c. Randomisation claimed but not described and
investigator not blinded
d. Randomisation not mentioned
2. Control of selection bias after treatment assignment
a. Intention to treat analysis AND full follow-up
b. Intention to treat analysis AND <15%
loss to follow-up
c. Analysis by treatment received only OR no mention of withdrawals
d. Analysis by treatment received
AND no mention of withdrawals
OR more than 15% withdrawals/loss-to-follow-up/post-randomisation

6 Hypofractionated radiotherapy for the treatment of early breast cancer
exclusions
3. Blinding
a. Blinding of outcome assessor
AND patient and care giver
b. Blinding of outcome assessor
OR patient and care giver
c. Blinding not done
4. Outcome assessment (if blinding was not possible)
a. All patients had standardised assessment
b. No standardised assessment OR not mentioned
*Source: modified from I Chalmers, Cochrane Handbook; available on the Cochrane Library
CDROM

Hypofractionated radiotherapy for the treatment of early breast cancer 7
3 Results
3.1 International guidelines
Four relevant international guidelines were identified in the previous Cancer Australia
systematic review:
American Society for Radiation Oncology (ASTRO) 2010: guidelines on fractionation
for whole breast irradiation
New Zealand Guidelines Group (NZGG) 2009: guidelines for management of early
breast cancer
National Institute of Clinical Excellence (NICE) 2009: guidelines for early and locally
advanced breast cancer
Scottish Intercollegiate Guidelines Network (SIGN) 2005: management of breast
cancer in women
This updated systematic review identified a further three relevant clinical practice
recommendations from the European Society of Medical Oncology (ESMO) (2013),12 German
Society of Radiation Oncology (DEGRO) (2013),13 and Nice-Saint-Paul de Vence guidelines
(2013).14 No updates of the four guidelines identified in the previous systematic were
identified.
The ESMO guidelines for diagnosis, treatment and follow-up of primary breast cancer,
published in November 2013, included the following recommendation regarding
hypofractionated radiotherapy:
Shorter fractionation schemes (e.g. 15-16 fractions with 2.5-2.67 Gy single dose) have
shown similar effectiveness and comparable side-effects [Level of evidence I, Grade
A].12
DEGRO published practical guidelines in 2013 on radiotherapy for breast cancer which
updated guidelines published in 2007. The guideline included the following recommendation
for hypofractionated radiotherapy:
In elderly patients with tumours <5cm and without locoregional lymph node disease,
who do not receive chemotherapy, as an alternative to normofractionated whole
breast radiotherapy, hypofractionated schedules (e.g. 5 x 2.666 Gy/week up to 40
Gy) may be considered (Level of evidence 1a, Grade B).13
The guideline also included the following conclusion from the DEGRO panel:
Normofractionated whole breast irradiation plus sequential boost remains standard.13
Hypofractionated whole breast irradiation with single doses up to 2.7 Gy in 15-16
fractions to total doses of 40-42 Gy is an option for older women with pT1-2 pN0
tumours who need no chemotherapy. The additional use of a sequential boost is
possible.13

8 Hypofractionated radiotherapy for the treatment of early breast cancer
Hypofractionated whole breast irradiation plus boost either by simultaneously
integrated boost or by hypofractionated sequential application is discouraged
outside clinical trials.13
The French expert review board of Nice-Saint-Paul de Vence published the 4th edition of the
adjuvant radiotherapy Nice-Saint-Paul de Vence guidelines.14 The guideline included the
following indications regarding hypofractionation and whole breast irradiation:
Eligibility for hypofractionated whole breast irradiation was defined by the most
representative breast cancer patients enrolled in clinical trials (START A, START B,
Canadian trial), which are: patients older than 50 years with invasive ductal
carcinoma, pT1, pN0, histological grade I/II, HR+, HER2-, having complete surgical
excision (experts’ agreements).14
Hypofractionated schemes are as follows: total dose= 42.4 Gy/15 fractions/ 3 weeks;
or total dose= 41.6 Gy/13 fractions/5 weeks; or total dose= 40 Gy/15 fractions/3 weeks
(Level of evidence I, grade A).14
The value of a boost to the lumpectomy cavity has not been established (Level of
evidence 1, grade A) and should not be recommended but rather could be left to
the discretion of the treating physician.14
The indication for a hypofractionated schedule (± boost to the lumpectomy site) in
breast cancer patients who do not belong to the subgroup mentioned above, should
be left to the discretion of the treating physician (experts’ agreements).14 The
treatment planning should keep the dose homogeneity index (less than 10%), as well
as the heart and lung exposure as low as possible.
3.2 Systematic reviews
Two published systematic reviews were identified by the first Cancer Australia review: James
2008 and Kalogeridi 2009. No new systematic reviews were identified in the updated
systematic search for the current review. A meta-analysis of locoregional recurrence rates
from three of the included RCTs (START A, START B and RMH/GOC) was identified (Haviland
2013). The objective of this post hoc sub-group analysis was to explore whether the following
characteristics modify response to hypofractionated radiotherapy: patient age, breast size,
tumour grade, axillary node status, type of surgery, cytotoxic chemotherapy, tumour bed
boost radiotherapy, and lymphatic radiotherapy.
3.3 Randomised controlled trials
In total, six RCTs were identified, all of which compared one or more hypofractionated
radiotherapy regimen to a standard radiotherapy regimen of 50 Gy in 25 fractions over 5
weeks for the treatment of early breast cancer. Of these six RCTs, five were previously
identified in the first systematic review, and one is newly published. In addition to the newly
published trial (UK FAST), updated publications were identified for START A and B, and for
Spooner. An additional three RCTs published as conference abstracts were identified,
although these provide limited information regarding study design and results.

Hypofractionated radiotherapy for the treatment of early breast cancer 9
It should be noted that the current review provides a detailed description of the newly
identified evidence only. This relates to four out of the six RCTs in the evidence base.
However, to provide context for the derivation of the current recommendations, the
accompanying guidelines include a consolidated summary of information for all six RCTs.
Study/Author Publication(s) in first Cancer Australia
systematic review (2011)
New publication(s) in current Cancer
Australia systematic review
RMH/GOC
Owen 2006; Yarnold 2005 Haviland 2010
Canadian
Whelan 2010; Whelan 2002 -
START A
Bentzen 2008a; Hopwood 2010 Haviland 2013; Haviland 2010
START B
Bentzen 2008b; Hopwood 2010 Haviland 2013; Haviland 2010
Spooner Spooner 2008 (conference abstract only) Spooner 2012
UK FAST Identified as an ongoing clinical trial FAST 2011
Study characteristics
The four RCTs with new, full publications included patients with early invasive breast cancer
(stage I-II, T1-3a, N0-1, M0). The studies examined a range of hypofractionated radiotherapy
regimens, including:
39 Gy in 13 fractions over 35 days(RMH/GOC trial9,15 and START A16,17)
40 Gy in 15 fractions over 21 days (START B17,18 and Spooner trial19)
41.6 Gy in 13 fractions over 35 days (START A16,17)
30 Gy in 5 fractions over 5 weeks (UK FAST20)
28.5 Gy in 5 fractions over 5 weeks (UK FAST20)
The START A trial tested two hypofractionated radiotherapy regimens. The START B, Spooner
trial and UK FAST trial each tested one hypofractionated radiotherapy regimen. In all trials,
the conventional radiotherapy regimen used as a comparator was 50 Gy in 25 fractions,
delivered over 5 weeks.
All studies compared conventional radiotherapy and hypofractionated radiotherapy
following surgery. Two trials included women who had undergone breast conserving surgery
only (Spooner trial, UK FAST trial). Two trials included women who had undergone breast
conserving surgery or mastectomy (START A and START B).
Median follow up ranged from 37.3 months to 16.9 years.
Study characteristics of the four included RCTs for which there are new publications are
presented in table 1 and patient characteristics are presented in table 2. A more detailed
discussion of the design and patient characteristics of these studies is presented below, by

10 Hypofractionated radiotherapy for the treatment of early breast cancer
study. Study characteristics of the RMH/GOC and Canadian trials are available in the 2011
systematic review in table 17. Note: a consolidated summary of study and patient
characteristics from all six RCTs included in the evidence base (i.e., those listed below plus
RMH/GOC and Canadian) is included in the accompanying guidelines document.

Hypofractionated radiotherapy for the treatment of early breast cancer 1
Table 1 Study characteristics of included RCTs from new publications
Author,
Year,
Location
Patients (N) Median
follow-up
Intervention Comparator Tumour bed
boost
Outcomes
START A ,
2013
UK17
Moderate
risk of bias
2236
9.3yrs
41.6 Gy in 13
Fractions over 5
weeks (n=750) OR
39Gy in 13
fractions over 5
weeks (n=737)
50 Gy in 25 fractions
over 5 weeks (n=749)
Both START trials
permitted
prescription of a
sequential tumour
bed boost dose of
10 Gy in five fractions
BCS: 1512 (61%)
Primary: local-regional
relapse and late
normal tissue effects.
Secondary: local
relapse, distant
relapse, DFS, OS
START B
2013
UK
Moderate
risk of bias
2215 9.9yrs
40 Gy in 15
fractions over 3
weeks (n=1110)
50 Gy in 25 fractions
over 5 weeks (n=1105)
Both START trials
permitted
prescription of a
sequential tumour
bed boost dose of
10 Gy in five fractions
BCS: 868 (43%)
Spooner,
2012
UK19
Moderate
risk of bias
707
n=358*
(radiotherapy)
n=349 (no
radiotherapy)
16.9yrs
40 Gy in 15
fractions over 3
weeks (n=181)
Supplementary boost
of direct 10-14 MeV
electron field of 15
Gy in five daily
fractions
50 Gy in 25 fractions
over 5 weeks (n=177)
Supplementary boost
of direct 10-14 MeV
electron field of 15 Gy
in five daily fractions
All irradiated patients:
358 (100%)
Primary: locoregional
relapse rate 5 years.
Secondary: survival
and locoregional
tumour control
n=707 randomised to:
radiotherapy (n=358) or no radiotherapy

2 Hypofractionated radiotherapy for the treatment of early breast cancer
(n=349)
UK FAST trial,
2011
UK20
Moderate
risk of bias
915 3.1yrs
30 Gy in 5 once
weekly fractions of 6
Gy over 5 weeks
(n=308) or
28.5 Gy in 5 once
weekly fractions of
5.7 Gy
over 5 weeks
(n=305)
50 Gy in 25 fractions of
2 Gy over 5 weeks
(n=302)
No boost Primary: change in
photographic breast
appearance.
Secondary: radiation-
induced changes in
the breast, and local
tumour control
*Group of interest. Abbreviations: DFS=Disease Free Survival; Gy=Gray; OS=overall survival.
Table 2 Patient characteristics of included RCTs from new publications
Study/Author Patient inclusion criteria Demographics Prior Surgery Prior treatment
START A17
Women with operable invasive breast cancer (pT1-
3a, pN0-1, M0) requiring radiotherapy after surgery
(BCS or mastectomy, with clear tumour margins ≥1
mm)Age > 18 yrs.
Median age: 57 (25-85)yrs.
Tumour size <2cm: 1138 (51%)
Positive lymph nodes: 643 (29%)
Tumour grade 1 or 2: 1572 (70%)
BCS: 1900 (85%) Adjuvant chemo: 793
(35%)
Tamoxifen: 1758 (79%)
Lymphatic radiotherapy:
318 (14%)
START B17
Women with operable invasive breast cancer (pT1-
3a, pN0-1, M0) requiring radiotherapy after surgery
(BCS or mastectomy, with clear tumour margins ≥1
mm)Age > 18 yrs.
Median age: 57 (23-86)yrs.
Tumour size <2cm: 1412 (64%)
Positive lymph nodes: 504 (23%)
Tumour grade 1 or 2: 1667 (75%)
BCS: 2038 (92%) Adjuvant chemo: 491
(22%)
Tamoxifen: 1928 (87%)
Lymphatic radiotherapy:
161 (7.3%)
Spooner,
201219
Patients with early clinical stage I and II breast
cancer
Women were eligible if they had histologically
proven adenocarcinoma of the breast that had
been completely surgically removed resulting in a
cosmetically satisfactory breast; clinical tumour
measurement had to be less than 5 cm with no
clinically palpable axillary nodes and no evidence
of systemic disease. Age not included in inclusion
criteria
Median age: 59 (28-80)yrs.
Menopausal status: pre- 87 (24%),
post- 237 (66%), peri- 34 (10%)
Infiltrating ductal carcinoma: 75%
Tumour grade 1 or 2: 39 (17%) or
134 (57%)
Tumour size: 2.0 (0.12-8.0)cm
BCS: 358 (100%) Tamoxifen: 358 (100%)

Hypofractionated radiotherapy for the treatment of early breast cancer 3
UK FAST trial20
Women with early stage breast cancer (invasive
carcinoma) and favourable prognostic features
including age > 50 yrs., BCS, pathological tumour
size <3.0 cm, complete microscopic resection of
tumour and negative axillary node status
established by appropriate surgical staging.
Median age: 63.2 (50-88)yrs.
Tumour size: 1.3 (0.05-3.0)cm
Tumour grade 1 or 2: 50Gy- 94
(31%) or 176 (58%), 30Gy- 113
(37%) or 159 (52%), 28.5- 102 (33%)
or 168 (55%)
BCS with complete
microscopic
resection of tumour
Tamoxifen: 50Gy- 227
(75%), 30Gy- 243 (79%),
28.5Gy- 224 (73%)
No chemotherapy
(exclusion criteria)
Abbreviations: BCS=breast conserving surgery


Hypofractionated radiotherapy for the treatment of early breast cancer 1
UK Standardisation of Breast Radiotherapy (START) trials
The START trials began in 1998, on the basis of results of the UK START pilot study (the
RMH/GOC trial) that assessed two lower dose regimens (39 Gy and 42.9 Gy) of a 13 fraction
regimen delivered over 5 weeks compared with 50 Gy in 25 fractions over 5 weeks.17 The
START trials were two randomised, unmasked trials of women recruited between 1999 and
2002, from UK radiotherapy centres; START A and START B.17
A total of 2236 early breast cancer patients were included in START A. Patients were
randomly assigned to either 50 Gy in 25 fractions over 5 weeks (control group) (n=749) or 41.6
Gy in 13 fractions over 5 weeks (n=750) or 39 Gy in 13 fractions over 5 weeks (n=737) after
complete excision (BCS or mastectomy).17 START A was designed as a superiority trial, with a
target sample size of 2,000 providing 80% power to detect a difference of 5% between the
control group and each hypofractionated regimen (two-sided alpha=0.05).
START B randomised 2215 early breast cancer patients to either 50 Gy in 25 fractions over 5
weeks (control group) (n=1110) or 40 Gy in 15 fractions over 3 weeks (n=1105) after complete
excision (BCS or mastectomy).17 START B was designed as a non-inferiority trial, with a target
sample size of 1,840 providing 95% power to exclude an increase of 5% in the primary
outcome for the control group versus the hypofractionated regimen (one-side alpha=0.025).
Both START trials permitted a sequential tumour bed boost dose of 10 Gy in 5 fractions. This
was required to be planned before randomisation.17
Haviland et al (2013) reported 10 year follow-up results of both START trials for local-regional
relapse, late normal tissue effects, local relapse, distant relapse, disease-free survival and
overall survival.17 The authors also reported post-hoc subgroup meta-analysis, which
compared the combined hypofractionated radiotherapy regimens of START A and B and the
pilot trial versus the control groups for local-regional relapse and the incidence of any
moderate or marked physician-assessed normal tissue effects in the breast (shrinkage,
induration, oedema, or telangiectasia). This updated search also identified a 2010 meta-
analysis of the START trials by Haviland et al (2010) (published as a letter to the editor),
however this was for 5-year follow-up and therefore the Haviland 2013 meta-analysis of 10-
year follow-up is reported in this systematic review.
The START trials were previously included in the 2011 Cancer Australia systematic review.
Spooner 2012
Spooner et al (2012) reported results of a UK based RCT which compared immediate
radiotherapy or delayed salvage treatment (no radiotherapy) following BCS (mastectomy
was excluded).19 Patients receiving radiotherapy were further randomised to either standard
radiotherapy (50 Gy in 25 fractions over 5 weeks) or hypofractionated radiotherapy (40 Gy in
15 fractions over 3 weeks). All irradiated patients received a supplementary tumour bed
boost of 15 Gy in five daily fractions. The outcomes for these two patient groups who
received radiotherapy will be reported in this systematic review. A total of 358 patients were
randomised to immediate radiotherapy; 177 to standard radiotherapy regimen and 181 to
short course radiotherapy regimen. Median follow-up was 16.9 years. The primary outcome
of the study was 5 year locoregional relapse rate, with survival and locoregional control
reported as secondary outcomes.19

2 Hypofractionated radiotherapy for the treatment of early breast cancer
UK FAST trial 2011
The FAST trialists group reported results of a randomised trial comparing standard
radiotherapy to two hypofractionated radiotherapy schedules following BCS (mastectomy
patients were excluded).20 Nine-hundred and fifteen women with node negative early breast
cancer were randomised to receive either standard radiotherapy regimen of 50 Gy in 25
fractions over 5 weeks (n=302) or a hypofractionated radiotherapy regimen of either 30 Gy in
5 once weekly fractions of 6.0 Gy over 5 weeks (n=308) or 28.5 Gy in 5 once weekly fractions
of 5.7 Gy over 5 weeks (n=305). Median follow-up was 37.3 months. The first published results
of the trial reported change in photographic breast appearance, radiation induced breast
changes, and local tumour control.20
Conference abstracts
An additional three RCTs published as conference abstracts were also identified however
these included limited results. The characteristics of these studies are presented in table 3
Table 3 Study characteristics of conference abstracts
Author
Location
Patients
(n)
Median
follow-
up
Intervention Comparator Outcomes
Barsoum,
2010, Egypt
308 Not
reported
40 Gy in 15
fractions over 3
weeks
50 Gy in 25
fractions over 5
weeks
Locoregional DFS,
distant-free survival,
overall survival
Patni, 2012,
India
40 7mths 40Gy in 15
fractions over 3
weeks
50Gy in 25
fractions over 5
weeks
Locoregional control,
disease-free survival
Fragandrea,
2012,
Greece
61 Not
reported
43.2 Gy in 16
fractions over
22 days with
boost 10 Gy in 5
fractions over 1
week
50 Gy in 25
fractions over 5
weeks with boost
10 Gy in 5 fractions
over 1 week
NR
Quality
The quality of each of the four included trials with full publications was considered to be fair
(moderate risk of bias). All trials were randomised, with the methods of randomisation
described, usually of a high quality. The majority of trials reported survival outcomes by
intention-to-treat analysis and limited numbers of patients were lost to follow-up. Trials were
not blinded. All trials had standardised assessment of outcomes and had well matched
population characteristics between treatment arms at baseline. Most of the phase III trials
were powered to detect a significant difference in primary outcomes.

Hypofractionated radiotherapy for the treatment of early breast cancer 3
Outcomes
3.3.1 Overall survival
Three studies reported on overall survival; START A, START B and Spooner 2012. OS was not a
primary outcome in any of the RCTs included in the evidence base.
START A and START B trials both reported all-cause mortality rates at 5 and 10 years as well as
causes of death, including breast cancer and other causes.17
START A reported a total 392 deaths in the study population with no significant difference in
all-cause 10 year mortality rates between the hypofractionated radiotherapy schedules and
standard radiotherapy.17 See table 4. At the time of analysis, 69.6% (273 deaths) of deaths in
START A were from breast cancer, 6.6% (26 deaths) were related to cardiac disease only,
8.7% (34 deaths) were from other cancers, 11.2% (44 deaths) were from other non-cancer
causes and 3.8% (15 deaths) were from unknown cause. Table 5 details causes of death for
each of the radiotherapy schedules.17
In the START B trial there were a total of 351 deaths.17 The 10 year all-cause mortality rate was
significantly lower in the hypofractionated radiotherapy arm than the standard radiotherapy
arm; HR=0.80 (95% CI 0.65-0.99), p= 0.042. See table 4. Of the 351 deaths in START B, 67.2%
(236 deaths) were from breast cancer, 4.8% (17 deaths) were related to cardiac disease
only, 13.7% (48 deaths) were from other causes, 11.4% (40 deaths) were from other non-
cancer causes, and 2.8% (10 deaths) were from unknown cause. Table 5 details causes of
death for each of the radiotherapy schedules.17
Table 4 All-cause mortality reported in START A and START B trials (2013)17
Events
(n/patients; %)
Estimated
proportion of
patients with
event by 5 years
(%; 95% CI)
Estimated
proportion of
patients with
event by 10
years (%; 95% CI)
Crude hazard
ratio (95% CI)
P value
START A
50 Gy 130/749 (17.4%) 10.5% (8.5-13.0) 19.8% (16.8-23.2) 1.00
41.6 Gy 128/750 (17.1%) 10.7% (8.7-13.2) 18.4% (15.7-21.6) 0.96 (0.75-1.17
)
0.74
39 Gy 134/737 (18.2%) 9.9% (8.0-12.4) 20.3% (17.3-23.7) 1.05 (0.82-1.34) 0.69
START B
50 Gy 192/1105 (17.4%) 10.9% (9.1-12.9) 19.2% (16.8-21.9) 1.00
40 Gy 159/1110 (14.3%) 7.9% (6.4-9.6) 15.9% (13.7-18.4) 0.80 (0.65-0.99) 0.042
Table 5 Causes of death in START A and START B trials (2013)17
Breast cancer Cardiac disease
only
Other cancers Other non-
cancer causes
Unknown
cause
START A
50 Gy 92/130 (71%) 7/130 (5%) 9/130 (7%) 16/130 (12%) 6/130 (5%)

4 Hypofractionated radiotherapy for the treatment of early breast cancer
41.6 Gy 86/128 (67%) 13/128 (10%) 10/128 (8%) 16/128 (13%) 3/128 (2%)
39 Gy 95/134 (71%) 6/134 (4%) 15/134 (11%) 12/134 (9%) 6/134 (4%)
START B
50 Gy 130/192 (68%) 12/192 (6%) 25/192 (13%) 21/192 (11%) 4/192 (2%)
40 Gy 106/159 (67%) 5/159 (3%) 23/159 (14%) 19/159 (12%) 6/159 (4%)
The study by Spooner et al (2012) reported 2, 5, 10, and 15 year estimates for overall
survival.19 The 2, 5, 10 and 15 year overall survival estimates for short course radiotherapy
were 94%, 85%, 70%, 53% respectively. For long course radiotherapy the 2, 5, 10 and 15 year
overall survival estimates were 92%, 81%, 67%, 52% respectively. There was no significant
difference between long- and short-course radiotherapy schedules for 2, 5, 10 and 15 year
overall survival estimates (HR 1.02, 95% CI 0.76-1.35).19
One additional RCT, published as a conference abstract only, also reported overall survival.
Barsoum et al (2013) reported no significant difference between hypofractionated
radiotherapy and standard radiotherapy (84.8% vs. 79.2% respectively, p=0.408).21
3.3.2 Disease-free survival
Haviland et al (2013) reported disease-free survival (DFS) for both START A and START B trials.
For START A there was no significant difference in DFS between the hypofractionated
radiotherapy schedules and standard radiotherapy (41.6 Gy vs. 50 Gy HR=0.94, 95% CI 0.75-
1.17, p=0.57; 39 Gy vs. 50 Gy HR=1.08, 95% CI 0.87-1.35, p=0.48).17 Whereas START B reported
significantly higher rates of DFS in patients receiving hypofractionated radiotherapy
compared to standard radiotherapy (40 Gy vs. 50 Gy HR=0.79, 95% CI 0.65-0.97, p=0.022).17
See table 6.
Table 6 Any breast cancer-related events reported in START A and START B trials (2013)17
Events
(n/patients; %)
Estimated
proportion of
patients with
event by 5 years
(%; 95% CI)
Estimated
proportion of
patients with
event by 10
years (%; 95% CI)
Crude hazard
ratio (95% CI)
P value
START A
50 Gy 154/749 (20.6%) 14.0% (11.6-16.7) 22.6% (19.5-26.1) 1.00
41.6 Gy 149/750 (19.9%) 11.7% (9.5-14.2) 22.7% (19.5-26.3) 0.94 (0.75-1.17) 0.57
39 Gy 163/737 (22.1%) 15.5% (13.0-18.3) 24.3% (21.1-28.0) 1.08 (0.87-1.35) 0.48
START B
50 Gy 222/1105 (20.1%) 14.3% (12.3-16.5) 22.2% (19.7-25.0) 1.00
40 Gy 182/1110 (16.4%) 10.4% (8.7-12.4) 18.3% (16.0-20.9) 0.79 (0.65-0.97) 0.022
3.3.3 Relapse-free survival
Spooner et al (2012) reported relapse-free survival estimates at 2, 5, 10 and 15 years. For
short-course radiotherapy the 2, 5, 10 and 15 year relapse-free estimates were 89%, 81%, 61%

Hypofractionated radiotherapy for the treatment of early breast cancer 5
and 46% respectively.19 The 2, 5, 10 and 15 year relapse-free estimates for long-course
radiotherapy were 86%, 73%, 59% and 44% respectively. There was no significant difference
between short- and long-course radiotherapy (HR 0.98, 95% CI 0.75-1.29).19
3.3.4 Event-free rates
Spooner et al (2012) reported 2, 5, 10 and 15 year cumulative incidence-free estimates
including: locoregional relapse event-free rates, distant relapse event-free rates, death
event-free rates, and overall competing event-free rates.19 No significant differences were
reported by short- or long-course radiotherapy treatment group. Table 7 reports the
cumulative incidence-free estimates.19
Table 7 Cumulative incidence-free estimates reported by Spooner et al (2012)19
Factor n (events) Cumulative incidence-free estimates (%)*
2 year 5 year 10 year 15 year
Locoregional relapse event-free rates
Short course 181 (25) 97 94 87 86
Long course 177 (21) 97 91 88 87
Distant relapse event-free rates
Short course 181 (29) 96 92 87 83
Long course 177 (24) 95 89 86 86
Death event-free rates
Short course 181 (98) 95 86 72 54
Long course 177 (92) 93 83 67 50
Overall competing event-free rates
Short course 181 (110)^ 88 75 54 38
Long course 177 (105)^ 86 67 51 38
* based on 1-cumulative incidence function for competing risks
^ events are the number of women with at least one competing event. Total numbers of competing
events: short course 152, long course 137.
3.3.5 Recurrence/relapse
Haviland et al (2013) reported that in the START A trial at a median follow-up 9.3 years 76% of
patients were alive and without relapse, 2.5% were alive with local-regional relapse (without
distant relapse), 3.5% were alive with distant relapse (including patients with local-regional
relapse), 17.5% had died (including 66 with local-regional relapse), and 0.4% had had no
follow-up.17 In START B, at a median follow-up of 9.9 years, 78.2% of patients were alive and
without relapse, 2.3% were alive with local-regional relapse (without distant relapse), 2.8%
were alive with distant relapse (including 10 patients with local-regional relapse), 15.8% had
died (including 35 patients with local-regional relapse) and 0.9% had no follow-up.17
Spooner et al (2012) reported that 15% of short-course radiotherapy patients and 21% of
long-course radiotherapy patients had relapse within 5 years.19 Overall relapse, at analysis
(median follow-up 16.9 years) occurred in 32% of hypofractionated radiotherapy patients
and in 29% of long-course radiotherapy patients.19

6 Hypofractionated radiotherapy for the treatment of early breast cancer
Local relapse
Four of the RCTs reported on local relapse; START A, START B, Spooner and UK FAST trial.
Both START A and START B trials reported 10 year local relapse rates, with both trials reporting
no significant difference between hypofractionated radiotherapy and conventional
radiotherapy regimens.17 See table 8.
Spooner et al (2012) reported on 5 year local relapse and overall local relapse.19 Overall
local relapse rates were similar across long- and short-course radiotherapy regimens. In the
short course radiotherapy arm 6.6% of patients relapsed within 5 years compared with 9.6%
of long-course radiotherapy patients (p value was not reported). Overall local relapse
occurred in 13.8% of short course radiotherapy patients compared with 11.9% of long course
radiotherapy patients.19
The UK FAST trial reported two local tumour relapses at median follow-up of 37.3 months; both
relapses were in the standard radiotherapy arm.20
Table 8 START A and START B relapses17
Events
(n/patients; %)
Estimated
proportion of
patients with
event by 5
years (%; 95%
CI)
Estimated
proportion of
patients with
event by 10
years (%; 95% CI)
Crude hazard
ratio (95% CI)
P value
START A
Local relapse
50 Gy 40/749 (5.3%) 3.4% (2.3-5.1) 6.7% (4.9-9.2) 1.00
41.6 Gy 37/750 (4.9%) 3.1% (2.0-4.7) 5.6% (4.1-7.8) 0.90 (0.57-1.40) 0.63
39 Gy 47/737 (6.4%) 4.4% (3.1-6.2) 8.1% (6.1-10.7) 1.20 (0.79-1.83) 0.39
Local-regional relapse
50 Gy 45/749 (6.0%) 4.0% (2.8-5.7) 7.4% (5.5-10.0) 1.00
41.6 Gy 42/750 (5.6%) 3.8% (2.6-5.5) 6.3% (4.7-8.5) 0.91 (0.59-1.38) 0.65
39 Gy 52/737 (7.1%) 5.1% (3.7-7.1) 8.8% (6.7-11.4) 1.18 (0.79-1.76) 0.41
Distant relapse
50 Gy 100/749 (13.3%) 9.8% (7.9-12.3) 14.7% (12.2-17.7) 1.00
41.6 Gy 110/750 (14.7%) 9.5% (7.6-11.9) 16.8% (14.0-20.0) 1.08 (0.82-1.41) 0.58
39 Gy 121/737 (16.4%) 11.8% (9.7-14.4) 18.0% (15.1-21.2) 1.24 (0.95-1.61) 0.11
START B
Local relapse
50 Gy 50/1105 (4.5%) 3.3% (2.4-4.6) 5.2% (3.9-6.9) 1.00
40 Gy 36/1110 (3.2%) 1.9% (1.2-3.0) 3.8% (2.7-5.2) 0.70 (0.46-1.07) 0.10
Local-regional relapse
50 Gy 53/1105 (4.8%) 3.5% (2.5-4.8) 5.5% (4.2-7.2) 1.00
40 Gy 42/1110 (3.8%) 2.3% (1.5-3.4) 4.3% (3.2-5.9) 0.77 (0.51-1.16) 0.21
Distant relapse
50 Gy 158/1105 (14.3%) 10.5% (8.8-12.5) 16.0% (13.8-18.5) 1.00
40 Gy 121/1110 (10.9%) 7.5% (6.0-9.2) 12.3% (10.3-14.6) 0.74 (0.59-0.94) 0.014

Hypofractionated radiotherapy for the treatment of early breast cancer 7
Local-regional relapse
Three RCTs reported on local-regional relapse; START A, START B, and UK FAST trial.
Haviland et al (2013) reported no significant difference in 10 year local-regional relapse rates
between hypofractionated radiotherapy regimens and standard radiotherapy regimen in
both START A and START B trials.17 See table 8. The authors reported that at the time of
analysis, 6.2% of patients in START A had local-regional tumour relapse compared with 4.3% of
patients in START B. It was noted that the lower proportion of local-regional tumour relapses in
START B was probably a result of the slightly better prognosis of patients recruited into START B
compared with START A.17
In START A Haviland et al (2013) reported that the estimated absolute differences in the
proportion of patients with local-regional relapses at 10 years compared with 50 Gy were
-0.6% (95% CI -3.0 to 2.7) for 41.6 Gy and 1.3% (95% CI -1.5 to 5.2) for 39 Gy.17 The upper limits
of the one-sided 95% CI for the absolute difference in 10 year local-regional relapse rates
indicated an estimated maximum 2.0% excess risk with 41.6 Gy and 4.5% with 39 Gy
compared with 50 Gy.17 See figure 1.
The estimated α/β value for local-regional relapse in START A was 4 Gy (95% CI 0.0-8.9),
adjusting for age, tumour size, type of primary surgery, use of adjuvant chemotherapy, use of
tamoxifen, lymphatic radiotherapy, and tumour bed boost radiotherapy. 17 Meta-analysis of
START A and the START pilot trial (349 events, 3646 women), provided an adjusted α/β value
for local regional relapse of 3.5 Gy (95% CI 1.2-5.7). 17
In the START B trial the estimated absolute difference in the proportion of patients with 10
year local-regional relapse for 40 Gy compared with 50 Gy was -1.2% (95% CI -2.6 to 1.0%).17
The upper limit of the one-sided 95% CI for the absolute difference in 10 year local-regional
relapse rates suggested an estimated 0.4% excess risk associated with the 15 fraction
schedule. See figure 1.

8 Hypofractionated radiotherapy for the treatment of early breast cancer
Figure 1: Cumulative risk of local-regional tumour relapse In START-A (A) and START-B (B).
Haviland et al (2013) reported that in a post-hoc subgroup meta-analysis, which compared
the combined hypofractionated radiotherapy regimens of START A and B and the pilot trial
(n=5861) versus the control groups for local-regional relapse, the treatment effect was not

Hypofractionated radiotherapy for the treatment of early breast cancer 9
significantly different irrespective of age, type of primary surgery, axillary node status, tumour
grade, adjuvant chemotherapy use, or use of tumour bed boost radiotherapy, see figure 2.17
Figure 2 Meta-analysis of local-regional relapse comparing hypofractionated regimens versus 50 Gy in
25 fractions Includes 5861 patients from the START pilot trial, START-A, and START-B.
The FAST trialists group reported regional relapse at median follow-up of 37.3 months.20 A total
of three regional relapses were reported in the UK FAST trial; two in the 28.5 Gy schedule and
one in the standard radiotherapy arm.20
Distant relapse
Four of the identified RCTs reported distant relapses; START A, START B, Spooner 2012 and UK
FAST trial.

10 Hypofractionated radiotherapy for the treatment of early breast cancer
START A trial reported no significant difference in 10 year distant relapse rates between the
hypofractionated radiotherapy schedules and standard radiotherapy.17 START B reported
significantly less distant relapses at 10 years in the hypofractionated radiotherapy group (40
Gy in 15 fractions over 3 weeks) compared with the standard radiotherapy group; 12.3% vs.
16% respectively (HR 0.74, 95% CI 0.59-0.94, p=0.014).17 See table 8.
The RCT by Spooner et al (2012) reported overall distant relapses and distant relapses within 5
years.19 Overall, distant relapses occurred in 16% of short-course radiotherapy patients and
13.6% of long-course radiotherapy patients. Within 5 years 8.8% of short course radiotherapy
patients and 11.3% of long-course radiotherapy patients experienced distant relapse. P
values were not reported.19
The UK FAST trial reported at total of 17 distant relapses at median follow-up; 10 in the 28.5 Gy
arm, two in the 30 Gy arm and five in the standard radiotherapy arm.20
3.3.6 Adverse events
Three of the identified RCTs reported on adverse events; START A, START B, and UK FAST trial
(2011). Additional RCTs reported as conference abstracts only also reported on adverse
events.
Late normal tissue effects
Both START A and START B reported late normal tissue effects as a primary endpoint. Normal
tissue effects in the breast, arm, and shoulder were assessed by physician, photographic
comparison with baseline, and patient self-reports.17 Table 9 and table 10 present physician-
assessed normal tissue effects for START A and START B respectively, including breast
shrinkage, breast induration, telangiectasia, breast oedema, shoulder stiffness, arm oedema,
and other.17
In START A the most common normal tissue effects at 10 years were breast shrinkage and
induration. In comparison to standard radiotherapy, patients in the 39 Gy regimen were
significantly less likely to have moderate or marked breast induration, telangiectasia, and
breast oedema, see table 9.17 Moderate or marked normal tissue effects did not differ
significantly between 41.6 Gy and 50 Gy groups.
Similar to START A, breast shrinkage and induration were the most common late normal tissue
effects at 10 years in START B.17 In comparison to standard radiotherapy patients, those
receiving hypofractionated radiotherapy (40 Gy) were significantly less likely to experience
moderate or marked breast shrinkage, telangiectasia, and breast oedema, see table 10.17
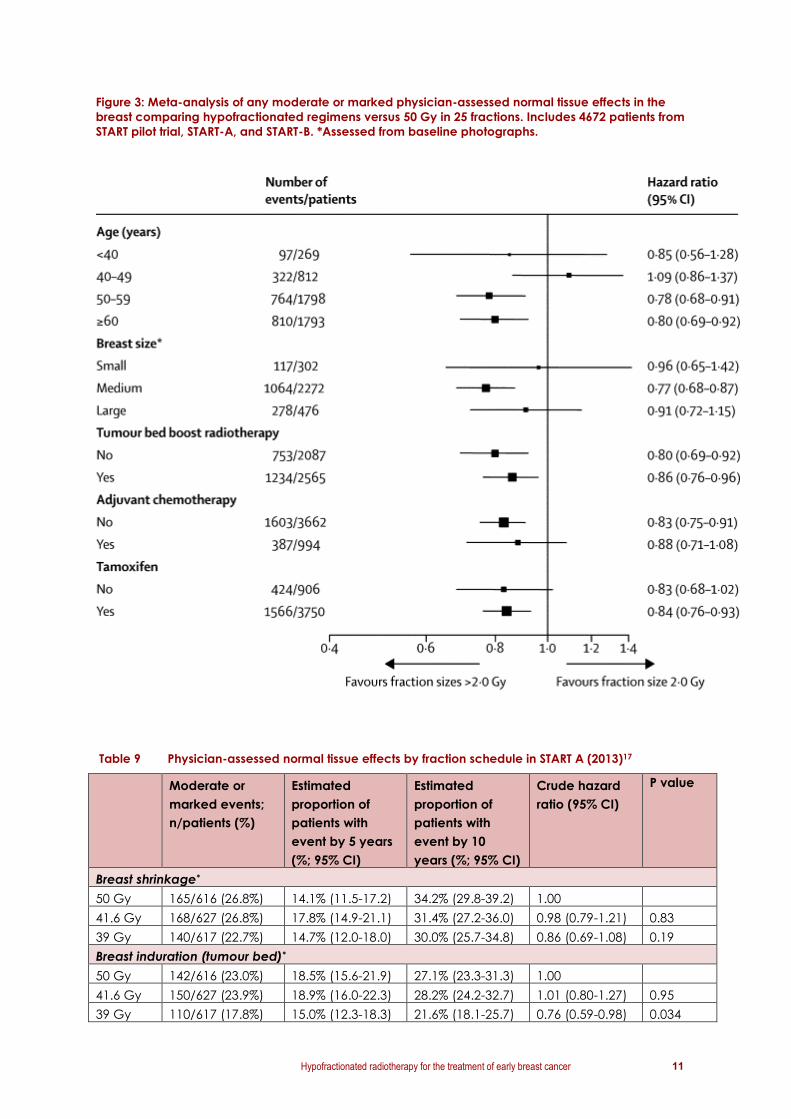
Haviland et al (2013) reported that in a post-hoc analysis, the incidence of any moderate or
marked physician-assessed normal tissue effects in the breast (shrinkage, induration,
oedema, or telangiectasia) for the 4,660 women with data available from START A, START B,
and the pilot study showed that the treatment effect was similar irrespective of age, breast
size, use of tumour bed boost radiotherapy, adjuvant chemotherapy, or tamoxifen, see figure
3.17
Hypofractionated radiotherapy for the treatment of early breast cancer 11
Figure 3: Meta-analysis of any moderate or marked physician-assessed normal tissue effects in the
breast comparing hypofractionated regimens versus 50 Gy in 25 fractions. Includes 4672 patients from
START pilot trial, START-A, and START-B. *Assessed from baseline photographs.
Table 9 Physician-assessed normal tissue effects by fraction schedule in START A (2013)17
Moderate or
marked events;
n/patients (%)
Estimated
proportion of
patients with
event by 5 years
(%; 95% CI)
Estimated
proportion of
patients with
event by 10
years (%; 95% CI)
Crude hazard
ratio (95% CI)
P value
Breast shrinkage*
50 Gy 165/616 (26.8%) 14.1% (11.5-17.2) 34.2% (29.8-39.2) 1.00
41.6 Gy 168/627 (26.8%) 17.8% (14.9-21.1) 31.4% (27.2-36.0) 0.98 (0.79-1.21) 0.83
39 Gy 140/617 (22.7%) 14.7% (12.0-18.0) 30.0% (25.7-34.8) 0.86 (0.69-1.08) 0.19
Breast induration (tumour bed)*
50 Gy 142/616 (23.0%) 18.5% (15.6-21.9) 27.1% (23.3-31.3) 1.00
41.6 Gy 150/627 (23.9%) 18.9% (16.0-22.3) 28.2% (24.2-32.7) 1.01 (0.80-1.27) 0.95
39 Gy 110/617 (17.8%) 15.0% (12.3-18.3) 21.6% (18.1-25.7) 0.76 (0.59-0.98) 0.034

12 Hypofractionated radiotherapy for the treatment of early breast cancer
Telangiectasia
50 Gy 42/730 (5.7%) 4.2% (3.0-6.1) 7.2% (5.2-9.8) 1.00
41.6 Gy 43/733 (5.9%) 4.9% (3.5-6.8) 7.1% (5.2-9.5) 1.00 (0.65-1.53) 0.99
39 Gy 18/723 (2.5%) 1.3% (0.6-2.5) 3.0% (1.8-5.0) 0.43 (0.25-0.75) 0.003
Breast oedema*
50 Gy 78/616 (12.7%) 12.1% (9.7-15.0) 13.5% (10.9-16.6) 1.00
41.6 Gy 67/627 (10.7%) 9.2% (7.1-11.7) 11.8% (9.2%-14.8) 0.82 (0.59-1.14) 0.24
39 Gy 43/617 (7.0%) 7.3% (5.5-9.7) 7.3% (5.5-9.7) 0.54 (0.37-0.78) 0.001
Shoulder stiffness^
50 Gy 14/117 (12.0%) 8.8% (4.7-16.4) 17.5% (10.2-29.1) 1.00
41.6 Gy 10/95 (10.5%) 7.1% (3.3-15.2) 14.8% (8.0-26.6) 0.85 (0.38-1.90) 0.69
39 Gy 8/92 (8.7%) 7.5% (3.4-16.0) 11.0% (5.6-21.0) 0.74 (0.31-1.76) 0.49
Arm oedema^
50 Gy 15/117 (12.8%) 12.8% (7.6-21.2) 16.3% (9.9-26.2) 1.00
41.6 Gy 16/95 (16.8%) 11.9% (6.6-21.0) 22.5% (14.1-34.7) 1.31 (0.65-2.66) 0.45
39 Gy 6/92 (6.5%) 6.4% (2.7-14.7) 8.2% (3.7-17.6) 0.50 (0.20-1.30) 0.16
Other
50 Gy 18/729 (2.5%) 1.3% (0.7-2.6) 3.4% (2.1-5.4) 1.00
41.6 Gy 20/733 (2.7%) 2.0% (1.2-3.4) 3.7% (2.3-6.1) 1.09 (0.58-2.06) 0.79
39 Gy 24/724 (3.3%) 2.3% (1.4-3.8) 3.9% (2.6-5.9) 1.37 (0.74-2.52 0.31
*Only assessed in women who had BCS. ^ Restricted to women who received lymphatic radiotherapy
(to axilla or supraclavicular).
Table 10 Physician-assessed normal tissue effects by fraction schedule in START B (2013)17
Moderate or
marked events;
n/patients (%)
Estimated
proportion of
patients with
event by 5 years
(%; 95% CI)
Estimated
proportion of
patients with
event by 10
years (%; 95% CI)
Crude hazard
ratio (95% CI)
P value
Breast shrinkage*
50 Gy 256/1003 (25.5%) 15.8% (13.6-18.3) 31.2% (27.9-34.9) 1.00
40 Gy 221/1006 (22.0%) 11.4% (9.5-13.6) 26.2% (23.1-29.6) 0.80 (0.67-0.96) 0.015
Breast induration (tumour bed)*
50 Gy 153/1003 (15.3%) 12.1% (10.2-14.4) 17.4% (14.9-20.3) 1.00
40 Gy 129/1006 (12.8%) 9.6% (7.9-11.6) 14.3% (12.1-16.9) 0.81 (0.64-1.03) 0.084
Telangiectasia
50 Gy 52/1081 (4.8%) 3.8% (2.8-5.2) 5.8% (4.4-7.7) 1.00
40 Gy 34/1094 (3.1%) 1.8% (1.1-2.8) 4.2% (2.9-5.9) 0.62 (0.40-0.96) 0.032
Breast oedema*9.0% (7.3-11.0)
50 Gy 86/1003 (8.6%) 8.1% (6.6-10.1) 9.0% (7.3-11.0) 1.00
40 Gy 49/1006 (4.9%) 4.7% (3.5-6.2) 5.1% (3.9-6.7) 0.55 (0.39-0.79) 0.001
Shoulder stiffness^
50 Gy 4/73 (5.5%) 2.9% (0.7-11.0) 8.2% (2.9-21.8) 1.00
40 Gy 3/81 (3.7%) 3.1% (0.8-11.9) 3.1% (0.8-11.9) 0.76 (0.17-3.39) 0.71
Arm oedema^
50 Gy 7/73 (9.6%) 6.0% (2.3-15.3) 13.5% (6.4-27.0) 1.00
40 Gy 3/81 (3.7%) 2.8% (0.7-10.7) 4.7% (1.5-14.0) 0.42 (0.11-1.63) 0.21

Hypofractionated radiotherapy for the treatment of early breast cancer 13
Other
50 Gy 77/1082 (7.1%) 5.6% (4.3-7.2) 8.1% (6.5-10.2) 1.00
40 Gy 53/1095 (4.8%) 3.3% (2.4-4.6) 6.4% (4.8-8.4) 0.65 (0.46-0.93) 0.018
*Only assessed in women who had BCS. ^ Restricted to women who received lymphatic radiotherapy
(to axilla or supraclavicular.
Late adverse effects
Haviland et al (2013) reported on late adverse effects for both START A and START B including
symptomatic rib fracture, symptomatic lung fibrosis, ischaemic heart disease and brachial
plexopathy.17 For both START A and START B, ischaemic heart disease, symptomatic rib
fracture and symptomatic lung fibrosis were rare at 10 years and incidence was similar
between radiotherapy schedules, see table 11.17
Table 11 Incidence of other late adverse effects according to fractionation schedule in START
(2013)17
START A START B
50 Gy
(n=749)
41.6 Gy
(n=750)
39 Gy
(n=737)
Total
(n=2236)
50 Gy
(n=1105)
40 Gy
(n=1110)
Total
(n=2215)
Symptomatic rib fracture*
Reported 5 (0.7%) 8 (1.1%) 9 (1.2%) 22 (1.0%) 17 (1.5%) 24 (2.2%) 41 (1.9%)
Confirmed^ 0 0 1 (0.1%) 1 (<0.1%) 3 (0.3%) 3 (0.3%) 6 (0.3%)
Symptomatic lung fibrosis
Reported 6 (0.8%) 9 (1.2%) 8 (1.1%) 23 (1.0%) 19 (1.7%) 19 (1.7%) 38 (1.7%)
Confirmed^ 0 2 (0.3%) 1 (0.1%) 3 (0.1%) 2 (0.2%) 8 (0.7%) 10 (0.5%)
Ischaemic heart disease#
Reported 14 (1.9%) 11 (1.5%) 8 (1.1%) 33 (1.5%) 23 (2.1%) 17 (1.5%) 40 (1.8%)
Confirmed^
Total
Left-sided
7 (0.9%)
4 (0.5%)
5 (0.7%)
1 (0.1%)
6 (0.8%)
4 (0.5%)
18 (0.8%)
9 (0.4%)
16 (1.4%)
5 (0.5%)
8 (0.7%)
4 (0.4%)
24 (1.1%)
9 (0.4%)
Brachial
plexopathy
0 1 (0.1%) 0 1 (<0.1%) 0 0 0
*reported cases include seven after trauma (5 START A, 2 START B), and 10 after metastases (5 in START A
and 5 in START B). # 26 patients in START A and 22 in START B had pre-existing heart disease at enrolment
and were excluded. ^ after imaging and further investigations.
Change in breast appearance
The UK FAST trial’s primary endpoint was change in photographic breast appearance
measured by photographic assessments at baseline and at 2 years and 5 years.20
Assessments of 2-year change in photographic breast appearance were available for 81% of
patients still alive and disease free (729/901). The trial reported the risk ratio for mild or marked
change in 2 year photographic breast appearance for 30 Gy vs. 50 Gy was 1.70 (95% CI 1.26-
2.29, p=<0.001) and for 28.5 Gy vs. 50 Gy the risk ratio was 1.15 (95% CI 0.82-1.60, p=0.489).
The trial demonstrated a clear and statistically significant dose response between 28.5 Gy
and 30 Gy with worse results for change in photographic breast appearance at 2 years in
the 30 Gy patients. Outcomes were comparable between the 28.5 Gy schedule and 50 Gy

14 Hypofractionated radiotherapy for the treatment of early breast cancer
schedule, see table 12.20 Physician-assessed adverse effects in the breast confirmed the
findings of photographic assessment of breast appearance. Moderate or marked adverse
effects in the breast were reported in 155 patients overall. Three-year rates of physician-
assessed moderate/marked adverse effects in the breast were 17.3% (13.3-22.3%) for 30 Gy
and 11.1% (7.9-15.6%) for 28.5 Gy compared with 9.5% (6.5-13.7%) after 50 Gy; the rate in the
30 Gy group was significantly higher than in 50 Gy (p=<0.001) and in 28.5 Gy (p=<0.006). The
rates were similar between the 28.5 Gy and 50 Gy groups (p=0.18).20
The UK FAST trial reported that the most common moderate or marked adverse effects in the
breast were shrinkage (n=106) and induration (n=40), with some reports of oedema (n=27)
and telangiectasia (n=15).20 Rates of induration and shrinkage were similar in the 50 Gy and
28.5 Gy schedules but higher in the 30 Gy group.20 Results for breast shrinkage were also
significantly higher among patients in the 30 Gy group; 30 Gy vs. 50 Gy p=0.002 and 30 Gy vs.
28.5 Gy p=0.016 and similar between the 28.5 Gy and 50 Gy groups; p=0.455. 20
Change in photographic breast appearance gave an estimate of α/β of 2.6 Gy (95% CI 1.4-
3.7) in the UK FAST trial.20 Using this estimate, the isoeffect doses expressed in 2.0 Gy
equivalents for 30 and 28.5 Gy in 5 fractions are 56.3 and 51.6 Gy, respectively. Adjustment
for breast size and surgical deficit at baseline made little difference to the α/β estimate viz.
2.5 Gy (95% CI 1.2-3.7). Estimates of α/β for the physician-assessed adverse effects are similar
to the result for the photographic endpoint.20
Table 12 Change in photographic breast appearance at 2 years by fractionation schedule20
Fractionation schedule Total
n=729 (%)
RR for 30 Gy
vs. 50 Gy
(95% CI), p-
value
RR for 28.5
Gy vs. 50
Gy (95%
CI), p-
value
RR for 30
Gy vs.
28.5 Gy
(95% CI),
p-value
50 Gy,
n=239 (%)
30 Gy,
n=248 (%)
28.5 Gy
n=242 (%)
No
change
189 (79.1) 160 (64.5) 184 (76.0) 533 (73.1) 1, p=<0.001 1, p=0.26 1, p=0.002
Mild
change
46 (19.2) 65 (26.2) 49 (20.2) 160 (22.0) 1.48
(1.06-2.05)
1.07
(0.75-15.4)
1.37
(1.00-1.90)
Marked
change
4 (1.7) 23 (9.3) 9 (3.7) 36 (4.9) 6.06
(2.14-17.20)
2.25
(0.70-7.18)
2.70
(1.28-5.67)
Abbreviations: RR=risk ratio
In the conference abstract by Patni et al (2012), acute breast pain was observed more
frequently in the hypofractionated radiotherapy arm (52.63% vs. 80%, p=0.141) at the
completion of radiotherapy.22 This became statistically significant at 7-10 days of completion
of radiotherapy (57.89% vs. 95%, p=0.018). Breast pain was similar in both groups after 6
months of treatment. Breast oedema and heat sensation were similar at both points of
assessment in both study groups.22
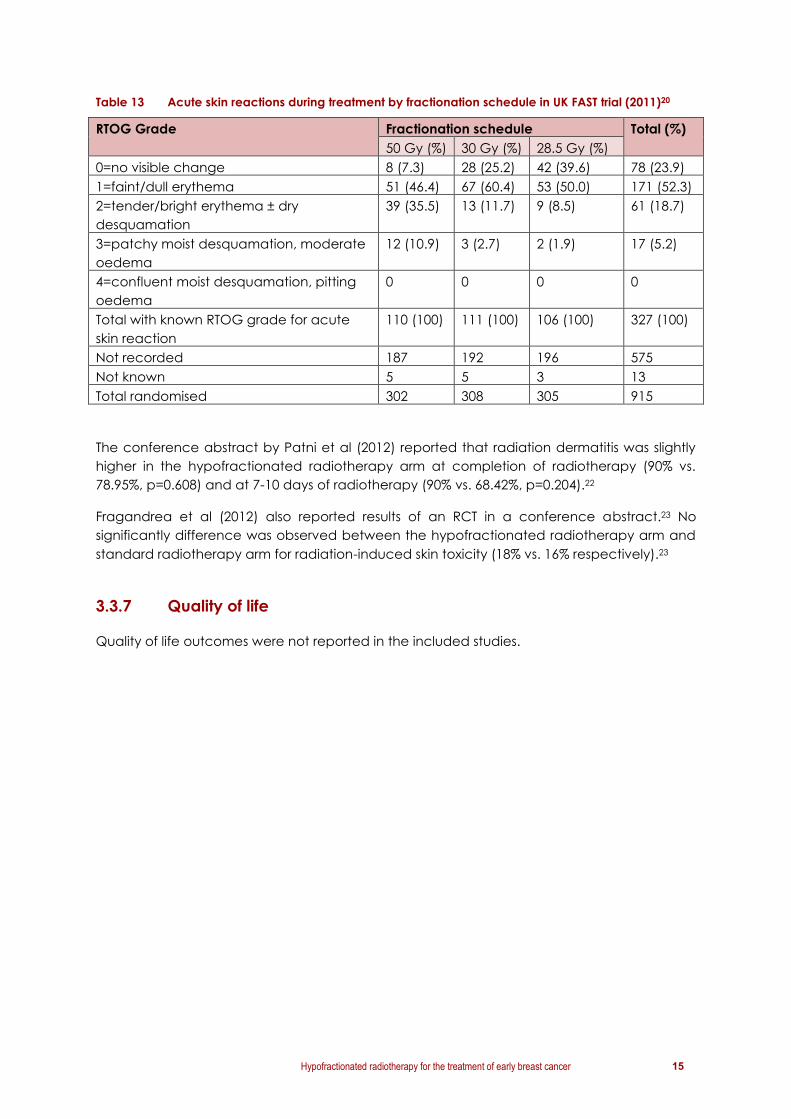
Skin toxicity
Data from 327 consecutive patients on acute skin reactions in the UK FAST trial showed milder
acute reactions in both hypofractionated radiotherapy schedules, see table 13.20
Hypofractionated radiotherapy for the treatment of early breast cancer 15
Table 13 Acute skin reactions during treatment by fractionation schedule in UK FAST trial (2011)20
RTOG Grade Fractionation schedule Total (%)
50 Gy (%) 30 Gy (%) 28.5 Gy (%)
0=no visible change 8 (7.3) 28 (25.2) 42 (39.6) 78 (23.9)
1=faint/dull erythema 51 (46.4) 67 (60.4) 53 (50.0) 171 (52.3)
2=tender/bright erythema ± dry
desquamation
39 (35.5) 13 (11.7) 9 (8.5) 61 (18.7)
3=patchy moist desquamation, moderate
oedema
12 (10.9) 3 (2.7) 2 (1.9) 17 (5.2)
4=confluent moist desquamation, pitting
oedema
0 0 0 0
Total with known RTOG grade for acute
skin reaction
110 (100) 111 (100) 106 (100) 327 (100)
Not recorded 187 192 196 575
Not known 5 5 3 13
Total randomised 302 308 305 915
The conference abstract by Patni et al (2012) reported that radiation dermatitis was slightly
higher in the hypofractionated radiotherapy arm at completion of radiotherapy (90% vs.
78.95%, p=0.608) and at 7-10 days of radiotherapy (90% vs. 68.42%, p=0.204).22
Fragandrea et al (2012) also reported results of an RCT in a conference abstract.23 No
significantly difference was observed between the hypofractionated radiotherapy arm and
standard radiotherapy arm for radiation-induced skin toxicity (18% vs. 16% respectively).23
3.3.7 Quality of life
Quality of life outcomes were not reported in the included studies.
16 Hypofractionated radiotherapy for the treatment of early breast cancer
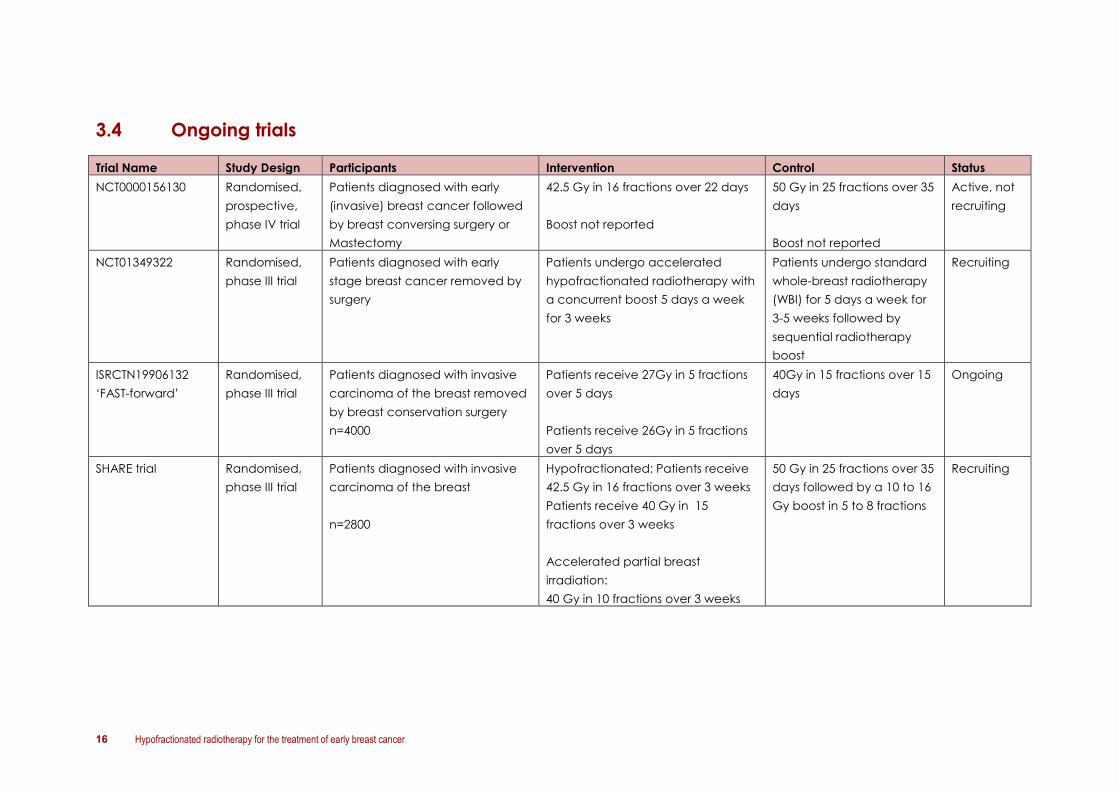
3.4 Ongoing trials
Trial Name Study Design Participants Intervention Control Status
NCT0000156130
Randomised,
prospective,
phase IV trial
Patients diagnosed with early
(invasive) breast cancer followed
by breast conversing surgery or
Mastectomy
42.5 Gy in 16 fractions over 22 days
Boost not reported
50 Gy in 25 fractions over 35
days
Boost not reported
Active, not
recruiting
NCT01349322 Randomised,
phase III trial
Patients diagnosed with early
stage breast cancer removed by
surgery
Patients undergo accelerated
hypofractionated radiotherapy with
a concurrent boost 5 days a week
for 3 weeks
Patients undergo standard
whole-breast radiotherapy
(WBI) for 5 days a week for
3-5 weeks followed by
sequential radiotherapy
boost
Recruiting
ISRCTN19906132
‘FAST-forward’
Randomised,
phase III trial
Patients diagnosed with invasive
carcinoma of the breast removed
by breast conservation surgery
n=4000
Patients receive 27Gy in 5 fractions
over 5 days
Patients receive 26Gy in 5 fractions
over 5 days
40Gy in 15 fractions over 15
days
Ongoing
SHARE trial Randomised,
phase III trial
Patients diagnosed with invasive
carcinoma of the breast
n=2800
Hypofractionated: Patients receive
42.5 Gy in 16 fractions over 3 weeks
Patients receive 40 Gy in 15
fractions over 3 weeks
Accelerated partial breast
irradiation:
40 Gy in 10 fractions over 3 weeks
50 Gy in 25 fractions over 35
days followed by a 10 to 16
Gy boost in 5 to 8 fractions
Recruiting

Hypofractionated radiotherapy for the treatment of early breast cancer 17
Investigators of ongoing trials were contacted in May 2014 to seek additional information on the trial and anticipated availability of results. The
information obtained from the investigators is listed below:.
Trial When will there be additional
information/data available
on trial?
Does the trial have an
expected date for
publication of results?
Will the trial include cost
effectiveness analysis?
Will patient preferences be
examined?
ISRCTN19906132 ‘FAST-
forward’
The trial has recently closed
(N=4000)
Data available probably in
2016 (secondary endpoints
focusing on clinical
assessment and patient self-
assessments of adverse
effects)
No, primary endpoint analysis
at a median 5 year (likely
2017)
Yes No
SHARE/NCT01247233 trial 2020
No Yes in a subset of patients
Yes, in Quality of Life
questionnaire

18 Hypofractionated radiotherapy for the treatment of early breast cancer
4 Discussion
Cancer Australia published clinical practice guidelines on the use of hypofractionated
radiotherapy for early (operable) breast cancer in November 2011. The guidelines were
based on a Cancer Australia systematic review which included available evidence from
January 2001 to March 2010 from randomised controlled trials. The RCT evidence in the first
systematic review came from five trials: RMH/GOC, Canadian trial, two Standardisation of
Breast Radiotherapy Trials (A and B) and Spooner (conference abstract only).
This current systematic review was undertaken to identify new and updated evidence on the
use of hypofractionated radiotherapy for the treatment of early breast cancer. The literature
search identified one new RCT (UK FAST 2011) and updated full publications from trials
included in the first systematic review: the START A, START B trials (Haviland 2013) and the
Spooner trial (Spooner 2012). Three further RCTs were identified that have only been
published as conference abstracts to date. The updated search identified three international
guidelines , but no systematic reviews. One meta-analysis was identified in the search
(Haviland 2010).
The body of evidence on hypofractionated radiotherapy for early (operable) breast cancer
from these two systematic reviews includes:
six primary RCTs: START A trial, START B trial, a trial by Spooner et al, the UK FAST trial,
the Canadian trial and the United Kingdom Royal Marsden Hospital/Gloucestershire
Oncology Centre (RMH/GOC) trial
three RCTs published as conference abstracts only.
The RMH/GOC, START A and the UK FAST trials tested two hypofractionated radiotherapy
regimens. The Canadian trial, the START B and Spooner trial each tested one
hypofractionated radiotherapy regimen. In all trials, the conventional radiotherapy regimen
used as a comparator was 50 Gy in 25 fractions, delivered over 5 weeks.
A range of hypofractionated radiotherapy regimens were examined, including
39 Gy in 13 fractions over 35 days(RMH/GOC trial and START A)
40 Gy in 15 fractions over 21 days (START B and Spooner trial)
41.6 Gy in 13 fractions over 35 days (START A)
42.5 Gy in 16 fractions over 22 days(Canadian trial)
42.9 Gy in 13 fractions over 35 days(RMH/GOC trial)
30 Gy in 5 once weekly fractions of 6Gy over 5 weeks (UK FAST)
28.5 Gy in 5 once weekly fractions of 5.7Gy over 5 weeks (UK FAST)
Four trials included women who had undergone breast conserving surgery only (Spooner
trial, UK FAST trial, Canadian trial, RMH/GOC).9,15,19,20,24,25 Two trials included women who had
undergone breast conserving surgery or mastectomy (START A and START B).16-18
Median follow up ranged from 37.3 months in the UK FAST trial to 16.9 years in the Spooner
trial.

Hypofractionated radiotherapy for the treatment of early breast cancer 19
From this updated systematic review and the 2011 systematic review, three studies examined
hypofractionated radiotherapy in patients with high grade tumours; the Canadian trial and
START trials as well as an additional retrospective population based cohort study included in
the original guideline, by Herbert et al (2012).26 The 2010 publication of the Canadian trial by
Whelan et al included an unplanned subgroup analysis including tumour grade.25 An
unplanned subgroup analysis of the Canadian trial showed that for patients with high grade
tumours, the hypofractionated radiotherapy regimen of 42.5 Gy in 16 fractions over 22 days
was associated with a higher local recurrence rate compared with conventionally
fractionated radiotherapy at 12 years follow-up (p=0.01).25 However, an updated analysis of
the Canadian trial by Bane et al (2014), reported no statistically significant difference for
local recurrence between grade 1-2 and grade 3 breast cancers (p=0.11).27 In the 2013
meta-analysis of the START A, START B trial and their pilot study no significant difference in
locoregional relapse between grade 1 and 2 tumours and grade 3 tumours (p=0.12) was
reported.17 A retrospective population based cohort study by Herbert et al (2012) of patients
with grade 3 breast cancer reported the 10-year cumulative incidence of local relapse was
6.9% in the hypofractionated group and 6.2% in the conventionally fractionated
radiotherapy group (p=0.99).26
In this updated systematic review, overall survival outcomes were consistent with the overall
survival outcomes reported in the 2011 systematic review. In both systematic reviews the
START B trial was the only study to report significantly higher overall survival rates in the
hypofractionated radiotherapy arm (40 Gy in 15 fractions over 3 weeks) compared with the
standard radiotherapy arm (updated systematic review: HR 0.80, 95% CI 0.65-0.99, p=0.042).
The START A, the Spooner 2012 trial and the Canadian trial (Whelan 2010) reported no
statistically significant differences in overall survival between hypofractionated radiotherapy
and standard radiotherapy.
START B reported significantly longer disease-free survival at 10 years in patients receiving
hypofractionated radiotherapy compared with patients receiving standard radiotherapy (HR
0.79, 95% CI 0.65-0.97, p=0.022). START A reported no significant difference for disease-free
survival between the hypofractionated radiotherapy schedules and standard radiotherapy.
Similar 2, 5, 10 and 15 year relapse-free survival estimates and cumulative incidence-free
estimates between the hypofractionated radiotherapy and standard radiotherapy regimens
were reported in the Spooner 2012 trial.
Five trials reported on local recurrence (START A, START B, Spooner 2012, RMH/GOC trial,
Canadian trial). All trials reported similar rates of local relapse for women treated with
hypofractionated radiotherapy and standard radiotherapy.9,17,19,25 RMH/GOC noted a
statistically significant difference in recurrence rates between the two hypofractionated
regimens (42.9 Gy vs. 39 Gy: 9.6% vs. 14.8%, p=0.027) but not when either of the
hypofractionated regimens was compared to 50 Gy in 25 fractions.9
START A and START B also reported no significant difference in 10 year local-regional relapse
rates between hypofractionated radiotherapy schedules and standard radiotherapy. Post-
hoc meta-analysis also demonstrated no significant difference in local-regional relapse rates
when stratified by age, type of primary surgery, axillary node status, tumour grade, adjuvant
chemotherapy use, or use of tumour bed boost radiotherapy.

20 Hypofractionated radiotherapy for the treatment of early breast cancer
START B reported significantly less distant relapses in patients receiving hypofractionated
radiotherapy (40 Gy in 15 fractions over 3 weeks) compared with patients receiving standard
radiotherapy (distant relapse rate: HR 0.74, 95% CI 0.59-0.94, p=0.014). Similar rates of distant
relapse were reported between patients receiving hypofractionated radiotherapy and
patients receiving conventionally fractionated radiotherapy in the START A, Spooner 2012
and UK FAST trials.17,19,20
Moderate or marked breast shrinkage, telangiectasia, and breast oedema were
experienced significantly less in patients who received 39 Gy in 13 fractions over 5 weeks in
the START A trial and 40 Gy in 15 fractions over 3 weeks in the START B trial compared with
patients receiving standard radiotherapy. There was no significant difference between 41.6
Gy in 13 fractions over 5 weeks and standard radiotherapy in the START A trial.
The UK FAST trial reported risk ratios for mild or marked change in 2 year photographic breast
appearance. The trial reported the risk ratio for mild or marked change in 2 year
photographic breast appearance for 30 Gy vs. 50 Gy was 1.70 (95% CI 1.26-2.29, p=<0.001)
and for 28.5 Gy vs. 50 Gy the risk ratio was 1.15 (95% CI 0.82-1.60, p=0.489). The trial
demonstrated a clear and statistically significant dose response between 28.5 Gy and 30 Gy
with worse results for change in photographic breast appearance at 2 years in the 30 Gy
patients. Outcomes were comparable between the 28.5 Gy schedule and 50 Gy schedule..
Three-year rates of physician-assessed moderate/marked adverse effects in the breast were
also significantly higher in the hypofractionated radiotherapy group of 30 Gy in 5 once
weekly fractions over 5 weeks compared with the standard radiotherapy group (p=<0.001)
and the hypofractionated radiotherapy group of 28.5 Gy in 5 once weekly fractions over 5
weeks (p=<0.006). The rates were similar between the 28.5 Gy and 50 Gy groups (p=0.18).20
Results for breast shrinkage were also significantly higher among patients in the 30 Gy group;
30 Gy vs. 50 Gy p=0.002 and 30 Gy vs. 28.5 Gy p=0.016 and similar between the 28.5 Gy and
50 Gy groups; p=0.455.
The Canadian trial reported that following assessments at baseline, three, five and ten years
after randomisation, the global cosmetic outcome worsened over time however there were
no significant differences observed between the 42.5 Gy group and the 50 Gy group at any
time.25 At ten years follow-up, 71.3% of women in the 50 Gy group compared to 69.8% of
women in the hypofractionated radiotherapy treatment group had an excellent or good
cosmetic outcome.25 Cosmetic outcome was shown to be affected by time from
randomisation, patient’s age and tumour size but there was no interaction with the
treatment.25
For photographically assessed changes in breast appearance, the RMH/GOC trial found a
higher risk of developing any radiation effect for patients allocated to 42.9 Gy in 13 fractions,
compared to those allocated to 39 Gy in 13 fractions or 50 Gy in 25 fractions (p=<0.001 for
comparison of three fractionation schedules).15 Clinical assessment of patients also indicated
significant differences between the three fractionation schedules, with the 42.9 Gy group
experiencing the highest incidence of events for overall breast cosmesis (p=<0.001), breast
shrinkage (p=0.026), breast distortion (p=0.005), breast oedema (p=0.004), induration
(p=0.001) and shoulder stiffness (p=0.001).15

Hypofractionated radiotherapy for the treatment of early breast cancer 21
5 Conclusion
This updated systematic review considered the evidence on the effectiveness of
hypofractionated radiotherapy for the treatment of early breast cancer compared with
standard radiotherapy following surgery.
The updated 10 year follow-up results from START A and START B and the published results
from the Spooner trial and UK FAST trial provide further evidence that hypofractionated
radiotherapy is equivalent to standard radiotherapy for women with early (operable) breast
cancer. Primary outcomes of overall survival, disease-free survival and recurrence were
similar for hypofractionated radiotherapy compared to standard radiotherapy and in some
instances were improved for those receiving hypofractionated radiotherapy.

22 Hypofractionated radiotherapy for the treatment of early breast cancer
Appendix A Contributors
Working group members
The hypofractionated radiotherapy for the treatment of early breast cancer systematic
review was developed with input from an expert multidisciplinary working group with the
following members:
Dr Marie-Frances Burke (Chair) Radiation Oncologist
Ms Jan Rice Breast Care Nurse
Dr Patsy Soon Breast Surgeon
Dr Kirsty Stuart Radiation Oncologist
Ms Bronwyn Wells Consumer Representative
Cancer Australia staff
The following Cancer Australia staff were involved in the development of the
hypofractionated radiotherapy for the treatment of early breast cancer systematic review:
Ms Katrina Anderson Senior Project Officer, Evidence Review
Ms Ornella Care Manager, Breast Cancer
Ms Medora Lee Project Officer, Evidence Review
Dr Anne Nelson Manager, Evidence Review

Hypofractionated radiotherapy for the treatment of early breast cancer 23
Appendix B Literature databases searched
Source Results/Retrievals
Medline (OVID) 172
Embase 322
Pubmed 86

24 Hypofractionated radiotherapy for the treatment of early breast cancer
Appendix C Search strategy
Breast cancer 1. "Breast Neoplasms"[MeSH] OR “breast cancer” OR
“breast carcinoma” OR “breast neoplasm” OR
“breast tumour” OR “breast tumor”
Hypofractionated radiotherapy 2. “radiation dose fractionation”[MeSH] OR
“radiation dose fractionation” OR “dose
fractionation”[MeSH] OR “dose fractionation” OR
“hypofractionated radiotherapy” OR
“fractionated radiotherapy”
3. fractionated OR hypofractionated OR fraction OR
fractio*)
4. “radiotherapy”[MeSH] OR “radiotherapy” OR
“irradiation therapy”[MeSH] OR “irradiation
therapy” OR “irradiation treatment”[MeSH] OR
“irradiation treatment” OR “radiation
therapy”[MeSH] OR “radiation therapy” OR
“radiation treatment”[MeSH] OR “radiation
treatment” OR “therapeutic radiology”[MeSH] OR
“therapeutic radiology” OR “radiation, therapy”
OR “treatment, irradiation”[MeSH] OR “treatment,
irradiation”
Search combination for hypofractionated radiotherapy
term: (#3 AND #4) OR #2
RCTS and meta-analyses 5. ("Randomized Controlled Trial"[MeSH] OR
"randomized controlled trial" OR "randomized
controlled trials" OR "randomised controlled trial*"
OR "random*" OR "random allocation" OR
"controlled clinical trial" OR "controlled trial" OR
"double blind method" OR "single blind method"
OR ("meta-analysis"[MeSH] OR "meta-analysis" OR
"meta analysis") OR "systematic review" OR "pooled
analysis")
FINAL COMBINATION #1 AND #hypofractionated radiotherapy terms combination AND #5

Hypofractionated radiotherapy for the treatment of early breast cancer 25
Appendix D Guideline and clinical trial sites searched
Acronym Organisation Website
Australia
ANZHSN Australia and New
Zealand Horizon
Scanning Network
http://www.horizonscanning.gov.au/
MSAC Medical Services
Advisory Committee
http://www.msac.gov.au/
NHMRC National Health and
Medical Research
Council
http://www.nhmrc.gov.au/
Canada
CCO Cancer Care Ontario http://www.cancercare.on.ca/
CADTH Canadian Agency for
Drugs and Technologies
in Health
http://www.cadth.ca/
International
HTAi Health Technology
Assessment International
http://www.htai.org/
Scotland
SIGN Scottish Intercollegiate
Guidelines Network
http://www.sign.ac.uk/
UK
CCT Current Controlled Trials http://www.controlled-trials.com/
NICE National Institute for
Health and Clinical
Excellence
http://www.nice.org.uk/
NRR National Research
Register
http://www.nrr.nhs.uk/
US
CT ClinicalTrials.gov http://www.clinicaltrials.gov/
NCI National Cancer Institute
Clinical Trials
http://www.cancer.gov/clinicaltrials
NGC National Guideline
Clearinghouse
http://www.guideline.gov/
AHRQ Agency for Healthcare
Research and Quality
http://www.ahrq.gov/

26 Hypofractionated radiotherapy for the treatment of early breast cancer
Appendix E Flowchart of inclusion/exclusion

Hypofractionated radiotherapy for the treatment of early breast cancer 27
Abbreviations
ASCO American Society of Clinical Oncology
ASTRO American Society for Radiation Oncology
BCS Breast conserving surgery
DEGRO German Society of Radiation Oncology
DFS Disease-Free Survival
EBCTG Early Breast Cancer Trialists Group
ESMO European Society of Medical Oncology
GIN Guidelines International Network
Gy Gray
HR Hazards ratio
IMRT Intensity Modulated Radiotherapy
NICE National Institute of Clinical Excellence
NZGG New Zealand Guidelines Group
OS Overall survival
RCTs Randomised controlled trials
RR Risk ratio
SABCS San Antonio Breast Cancer Symposium
SIGN Scottish Intercollegiate Guidelines Network
SHARE trial Standard or Hypofractionated Radiotherapy versus
Accelerated Breast Irradiation for Breast Cancer
START trials Standardisation of Breast Radiotherapy trials

28 Hypofractionated radiotherapy for the treatment of early breast cancer
References
1. James ML, Lehman M, Hider PN, et al. Fraction size in radiation treatment for breast
conservation in early breast cancer. Cochrane Database Syst Rev. 2010;11):CD003860.
2. Freedman GM. Hypofractionated radiation therapy in the treatment of early-stage breast
cancer. Curr Oncol Rep. 2012;14(1):12-9.
3. Australian Institute of Health and Welfare & Australasian Association of Cancer Registries.
Cancer in Australia: an overview, 2012. Cancer series no. 74. Cat. no. CAN 70. AIHW,
Canberra, 2012.
4. Australian Institute of Health and Welfare. Cancer incidence and projections: Australia,
2011 to 2020. Cancer series no. 66. Cat no. CAN 62. AIHW, Canberra, 2012.
5. Australian Institute of Health and Welfare & Cancer Australia 2012. Breast cancer in
Australia: an overview. Cancer series no. 71. Cat no. CAN 67. AIHW, Canberra, 2012.
6. National Breast Cancer Centre (NBCC). Clinical practice guidelines for the management
of early breast cancer (2nd edition). Commonwealth of Australia, Canberra, 2001.
7. Early Breast Cancer Trialists' Collaborative G, Darby S, McGale P, et al. Effect of
radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast
cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised
trials. Lancet. 2011;378(9804):1707-16.
8. Smith BD, Bentzen SM, Correa CR, et al. Fractionation for Whole Breast Irradiation: An
American Society for Radiation Oncology (ASTRO) Evidence-Based Guideline. Int J Radiat
Oncol Biol Phys. 2011;81(1):59-68.
9. Owen JR, Ashton A, Bliss JM, et al. Effect of radiotherapy fraction size on tumour control in
patients with early-stage breast cancer after local tumour excision: long-term results of a
randomised trial. Lancet Oncol. 2006;7(6):467-71.
10. Cuncins-Hearn AV, Boult M, Babidge W, et al. National breast cancer audit: overview of
invasive breast cancer management. ANZ J Surg. 2006;76(8):745-50.
11. Cancer Australia. Recommendations for use of Hypofractionated radiotherapy for early
(operable) breast cancer. Cancer Australia, Surry Hills, NSW, 2011.
12. Senkus E, Kyriakides S, Penault-Llorca F, et al. Primary breast cancer: ESMO Clinical
Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24 Suppl 6(vi7-
23.

Hypofractionated radiotherapy for the treatment of early breast cancer 29
13. Sedlmayer F, Sautter-Bihl ML, Budach W, et al. DEGRO practical guidelines: radiotherapy
of breast cancer I: radiotherapy following breast conserving therapy for invasive breast
cancer. Strahlenther Onkol. 2013;189(10):825-33.
14. Bourgier C, Aimard L, Bodez V, et al. Adjuvant radiotherapy in the management of
axillary node negative invasive breast cancer: a qualitative systematic review. Crit Rev Oncol
Hematol. 2013;86(1):33-41.
15. Yarnold J, Ashton A, Bliss J, et al. Fractionation sensitivity and dose response of late
adverse effects in the breast after radiotherapy for early breast cancer: long-term results of a
randomised trial. Radiother Oncol. 2005;75(1):9-17.
16. Bentzen SM, Agrawal RK, Aird EG, et al. The UK Standardisation of Breast Radiotherapy
(START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a
randomised trial. Lancet Oncol. 2008;9(4):331-41.
17. Haviland JS, Owen JR, Dewar JA, et al. The UK Standardisation of Breast Radiotherapy
(START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year
follow-up results of two randomised controlled trials. Lancet Oncol. 2013;14(11):1086-94.
18. Bentzen SM, Agrawal RK, Aird EG, et al. The UK Standardisation of Breast Radiotherapy
(START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a
randomised trial. Lancet. 2008;371(9618):1098-107.
19. Spooner D, Stocken DD, Jordan S, et al. A Randomised Controlled Trial to Evaluate both
the Role and the Optimal Fractionation of Radiotherapy in the Conservative Management of
Early Breast Cancer. Clinical Oncology. 2012;24(10):697-706.
20. FAST Trialists group, Agrawal RK, Alhasso A, et al. First results of the randomised UK FAST Trial
of radiotherapy hypofractionation for treatment of early breast cancer (CRUKE/04/015).
Radiother Oncol. 2011;100(1):93-100.
21. Barsoum MS, El Mongi MM, Khalil EM, et al. Prospective randomized trial comparing
postoperative adjuvant concurrent versus sequential hormonal and different radiation
fractionation schedule in breast cancer patients. Journal of Clinical Oncology.
2010;28(15s):abstr 544.
22. Patni N, Jain M, Patni S and Bapna A. A comparison of acute and chronic toxicity profile
between conventional and hypofractionated whole breast irradiation in patients undergoing
breast conserving surgery. International Journal of Radiation Oncology Biology Physics.
2012;84(Issue 3 Supplement):S232.
23. Fragandrea I, Kouloulias V, Sotiropoulou A, et al. Radiation induced skin toxicity following
hypofractionated radiotherapy treatment in early breast cancer: Single institution
experience. European Journal of Cancer. 2012;48(Supplement 1):S158.

30 Hypofractionated radiotherapy for the treatment of early breast cancer
24. Whelan T, MacKenzie R, Julian J, et al. Randomized trial of breast irradiation schedules
after lumpectomy for women with lymph node-negative breast cancer. J Natl Cancer Inst.
2002;94(15):1143-50.
25. Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation
therapy for breast cancer. N Engl J Med. 2010;362(6):513-20.
26. Herbert C, Nichol A, Olivotto I, et al. The Impact of Hypofractionated Whole Breast
Radiotherapy on Local Relapse in Patients with Grade 3 Early Breast Cancer: A Population-
based Cohort Study. Int J Radiat Oncol Biol Phys. 2012;82(5):2086-92.
27. Bane AL, Whelan TJ, Pond GR, et al. Tumor Factors Predictive of Response to
Hypofractionated Radiotherapy in a Randomized Trial Following Breast Conserving Therapy.
Ann Oncol. 2014.

1
Hypofractionated radiotherapy for early breast cancer
Left- vs. right-sided breast cancers
October 2014
Background
Cancer Australia is currently updating the 2011 topic-specific guideline Recommendations
for use of hypofractionated radiotherapy for the treatment of early (operable) breast cancer
to incorporate new and updated evidence and revise the statements of evidence and
recommendations. At working group meetings it was agreed that consideration needed to
be given to whether or not the recommendations be updated to include right-sided tumours
as a patient inclusion criterion for offering hypofractionated radiotherapy and left-sided
tumours be included as a criterion with insufficient evidence to recommend for or against
hypofractionated radiotherapy.
The systematic review to support the update of the guideline did not identify/report
evidence for left-vs. right-sided tumours. This section of the Technical Document provides
evidence on cardiotoxicity left- vs. right-sided breast cancers from the randomised
controlled trials (RCTs) included in the guideline. Evidence from additional non-randomised
trials has also been included.
Method
Evidence on left- vs. right-sided tumours was extracted from RCTs identified in either the 2011
systematic review and/or the updated 2014 systematic review. Additional evidence from
non-randomised studies was identified in a supplementary literature search. The search was
undertaken in August 2014 in the electronic database PubMed and included key words
“breast cancer”, “hypofractionated radiotherapy” and “left”. The search identified seven
citations of which four are included in this evidence summary.
1. Evidence from randomised controlled trials (RCTs)
The topic-specific guideline Recommendations for use of hypofractionated radiotherapy for
the treatment of early (operable) breast cancer is based on evidence from six RCTs
comparing hypofractionated radiotherapy to conventionally fractionated radiotherapy;
START A, START B, Spooner 2012, UK FAST trial, Canadian trial, and RMH/GOC trial. None of the
trials included left- and right-sided tumours in their inclusion or exclusion criteria. Only three of
the six trials reported cardiac outcomes by left- vs right-sided tumours: START A, START B and
UK FAST. Table 1 shows the total number of deaths reported in each of these three trials, with
breakdowns by cardiac disease related, breast cancer related, other cancer related or
other non-cancer related. Cardiac disease related deaths are shown by tumour side, where
reported. The median duration of follow-up most recently reported for START A, START B and
UK FAST is 9.3, 9.9 and 3.1 years, respectively.

2
Table 1: Mortality in hypofractionated radiotherapy RCTs showing cardiac disease-related deaths by tumour side
Start A (Haviland 2013)1
(median follow-up 9.3yrs)
Start B (Haviland 2013)1
(median follow-up 9.9yrs
UK-FAST 20113
(median follow-up 3.1yrs)
50Gy 41.6Gy 39Gy Total 50Gy 40Gy Total 30Gy 28.5Gy 50Gy Total
N=749 N=750 N=737 N=2236 N=1105 N=1110 N=2215 N=308 N=305 N=302 N=915
All cause 130 128 134 392 192 159 351 5 12 6 23
Breast cancer related 92 86 95 273 130 106 236 2 6 2 10
Other cancer related 9 10 15 34 25 23 48 NR NR NR NR
Cardiac disease related only 7 13 6 26 12 5 17 NR NR NR 4
Left sided 4 10 1 15 8 3 11 NR NR NR 2
Right sided 3 3 5 11 4 2 6 NR NR NR 2
Othera 16 16 12 44 21 19 40 3 6 4 13
Unknown 6 3 6 15 4 6 10 NR NR NR NR
Abbreviations NR: not reported; a defined as non-cancer, non-cardiac disease in START A and START B, and as non-breast cancer related in UK FAST

3
As shown in table 1, the most common cause of death in patients across these three RCTs
was breast or other cancer. In START A after 9.3 years median follow-up, 26/392 (6.6%) deaths
were related to cardiac disease (seven with 50 Gy, 13 with 41.6 Gy, and six with 39 Gy).
Fifteen (57.7%) of the 26 deaths from cardiac disease were in women with left-sided primary
tumours (four of seven with 50 Gy, ten of 13 with 41.6 Gy, and one of six with 39 Gy). In START
B, after 9.9 years median follow-up, 17/351 (4.8%) deaths were related to cardiac disease (12
with 50 Gy and five with 40 Gy). Eleven (64.7%) of the 17 deaths from cardiac disease were in
women with left-sided primary tumours (eight of 12 with 50 Gy and three of five with 40 Gy).
In UK FAST after 3.1 years median follow-up, 4/23 (17.4%) deaths were attributed to cardiac
disease, with two deaths in women with left sided tumours, and two deaths in women with
right-sided tumours. However, the UK FAST publication does not report the treatment group
assignment for any of these cardiac disease related deaths.In addition, while the Canadian
trial did not report results for left- and right-sided breast cancers, the authors did note that at
a median follow-up of 12 years few cardiac-related deaths were observed and no increase
occurred in patients who received the hypofractionated regimen.4
When interpreting the mortality rates from START A, B and UK FAST a number of factors should
be kept in mind. The number of events in each study is low and the number of deaths due to
unknown causes is relatively high. For example, in START A only four of the fifteen deaths from
unknown causes need to be cardiac-disease related in right-sided tumours for the observed
event rates to be equivalent. Furthermore, although women with pre-existing heart disease
were excluded from START A and START B, none of the three studies stratified patients at
baseline by cardiac risk factors. And finally, interpretation of the available evidence is
difficult given that subsequent chemotherapy regimens will likely have differed among
women and not been matched across radiotherapy treatment groups. Differences in the
cardiotoxicity of subsequent chemotherapy regimens may confound the attribution of
cardiotoxicity to a particular radiotherapy regimen.
Haviland et al (2013) concluded that the START A and B trial results showed that although
follow-up was still shorter than would be desired for cardiac events, there was no major
difference between the fractionation schedules for the number of cases of heart disease in
women with left-sided primary tumours, see table 2.1 Haviland et al (2013) also note that the
heart is sensitive to radiation whatever fractionation is used with no lower dose threshold for
adverse effects. A commentary on the 2013 START trial results agreed with the START trial
authors that techniques to protect the heart are important for both radiotherapy schedules
and the choice of fractionation should not be affected by whether the tumour is in the right
or left breast.6
Table 2: Incidence of ischaemic heart disease according to fractionation schedule (START
trials) 1
Ischaemic
heart
disease*
START A START B
50 Gy
n=749
41.6 Gy
n=750
39 Gy
n=737
Total
n=2236
50 Gy
n=1105
40 Gy
n=1110
Total
n=2215
Reported 14 (1.9%) 11 (1.5%) 8 (1.1%) 33 (1.5%) 23 (2.1%) 17 (1.5%) 40 (1.8%)
Confirmed
Total 7 (0.9%) 5 (0.7%) 6 (0.8%) 18 (0.8%) 16 (1.4%) 8 (0.7%) 24 (1.1%)
Left sided 4 (0.5%) 1 (0.1%) 4 (0.5%) 9 (0.4%) 5 (0.5%) 4 (0.4%) 9 (0.4%)
4
*26 patients in START A and 22 in START B had pre-existing heart disease at enrolment and were
excluded
2. Evidence from additional non-randomised studies
Four additional non-randomised studies were identified which include outcomes for left- and
right-sided breast cancers.
A population-based retrospective study by Chan et al was reported in two 2014 publications.
The first paper aimed (median follow-up 13.2 years; Ontario) to determine if there is an
increase in hospital-related morbidity from cardiac causes with either hypofractionated
radiotherapy (40-44 Gy in 16 fractions) or conventional radiotherapy (45-50 Gy in 25 fractions
or 50.4 Gy in 28 fractions).7 For left-sided cases, 15-year cumulative hospital-related morbidity
from cardiac causes was not different between the two radiotherapy regimens (both 21%,
p=0.93). The difference was also not significant for right-sided cases (hypofractionated 18%,
conventional 19%; p=0.76). The 15-year cumulative mortality before first cardiac
hospitalisation between hypofractionated radiotherapy and conventional radiotherapy was
not statistically different; 20.7% vs. 23.8% respectively (p= NR). Right-sided cases were also not
significantly different.
The authors concluded that for women with left-sided early-stage breast cancer who
received postoperative radiation therapy to the whole breast or chest wall, there was no
difference in the 15-year cumulative morbidity due to cardiac causes, between
conventionally fractionated and hypofractionated treatment schedules. Even after
adjustment for baseline patient, tumour, and treatment factors between the two radiation
therapy fractionation groups, no difference was seen in the incidence of cardiac morbidity.7
The second publication from the population-based retrospective study by Chan et al (2014)
(median follow-up 14 years; Ontario) reported on if there is an increase in cardiac mortality
with hypofractionated radiotherapy relative to conventional radiotherapy.10 For left-sided
cases, at 15-years follow-up, the rate of cardiac mortality for hypofractionated radiotherapy
was 4.8% and for conventional radiotherapy it was 4.2%, this difference was not statistically
significant (p = 0.74). The difference was also not significant for right-sided cases
(hypofractionated 4.9%, conventional 3.5%, p=0.21). The 15-year cumulative mortality due to
breast cancer, cardiovascular and other causes was calculated separately, comparing
hypofractionated and conventional radiotherapy for the left and right-sided cases; none of
the results were statistically significant.
The authors concluded that at 15-years follow-up, cardiac mortality is not statistically
different among left-sided breast cancer patients treated with hypofractionated
radiotherapy and conventional radiotherapy.
The authors noted that additional unpublished analyses were undertaken in which cardiac
cause of death was prioritised a priori. In other words, for cases where breast cancer and a
cardiac event were listed as cause of death, the main analysis indexed breast cancer as the
cause of death. However, in the additional analyses the cardiac event was indexed as the
cause of death. These analyses are therefore highly conservative with respect to cardiac
mortality (i.e., likely to over-estimate cardiac attribution).
From personal correspondence with the study authors two additional analysis were provided,
with:
1. cardiac cause as a priority
2. cardiac cause not including cardiac arrest as a priority

5
For both analyses there was no significant difference between hypofractionated
radiotherapy and conventional radiotherapy for death from cardiac causes at 10 or 15 years
(p=0.206 and p=0.406, respectively).
The additional analyses are consistent with the overall conclusion of the study that at 15-
years follow-up, cardiac mortality is not statistically different among left-sided breast cancer
patients treated with hypofractionated radiotherapy or conventionally fractionated
radiotherapy.
Appelt et al (2013) analysed dose plans for 60 left-sided breast cancer patients to compare
fraction size-corrected dose distributions to the heart for four hypofractionated schedules
with the normofractionated schedule of 50 Gy in 25 fractions, for a range of α/β values.8 All
patients were planned with tangential fields for whole breast irradiation. Dose distributions
were corrected to the equivalent dose in 2 Gy fractions (EQD2) using the linear quadratic
model for five different fractionation schedules (50 Gy/25 fractions and four
hypofractionated regimens) and for a range of α/β values (0-5 Gy). The mean EQD2 to the
heart (DEQD2 mean) and the volume receiving 40 Gy (VEQD2 40 Gy), both as calculated from
the EQD2 dose distributions, were compared between schedules.
The authors concluded that for standard tangential field whole breast irradiation, most of the
examined hypofractionated schedules are estimated to spare the heart when compared
with normofractionation. The dose to the heart, adjusted for fraction size using the linear
quadratic model, will generally be lower after hypofractionated compared with
normofractionated schedules, even for very low values of α/β values.8
Holm Tjessem (2013) reported results of a retrospective case-control study that analysed the
20-year risk of death from ischemic heart disease (IHD) in breast cancer patients who
received hypofractionated locoregional radiation therapy at the Norwegian Radium
Hospital between 1975 and 1991 (median follow-up: all patients 4.5yrs, surviving patients
20yrs). Two hypofractionated radiotherapy regimens were used: 4.3 Gy x 10 given as 2
weekly fractions (n=1107) and 2.5 Gy x 20 given as 4 weekly fractions (n=459). Controls were
cancer-free (n=10). In the 4.3 Gy group, 86% of patients died, compared with 84% in the 2.5
Gy group. In the 4.3 Gy group, 4% died of IHD compared with 2% in the 2.5 Gy group
(HR=2.37, 95% CI 1.06-5.32, p=0.036), with the difference emerging first after 10 to 15 years. In
multivariate analysis the 4.3 Gy still had an associated increased risk of IHD but with
borderline significance only (HR=2.90, 95% CI 0.97-8.76, p=0.057). Patients in the 4.3 Gy group
had an increased risk of dying of IHD compared with controls (HR 1.59, 95% CI 1.13-2.23,
p=0.008). No elevated risk of death resulting from IHD was found in the 2.5 Gy group
compared with controls.
Treatment before 1984 was associated with an increased risk of dying of IHD (HR 2.87, 95% CI
1.34-6.17, p=0.006) compared with treatment from 1984 onwards. Patients treated for left-
sided cancer did not have increased risk of dying of IHD compared with right-sided breast
cancer.
The authors concluded that the degree of fractionation and photon beams in the
parasternal contributed to increased IHD mortality in the patient cohort. The differences in
IHD mortality emerged 12 to 15 years after treatment and the increased risk among breast
cancer patients treated with hypofractionated radiation therapy thus indicates that a follow-
up time of at least two decades is needed to evaluate safety of such irradiation.

6
Marhin et al (2007) in an earlier retrospective study of the Ontario cases(median follow-up 7.9
years), assessed whether an adjuvant hypofractionated radiotherapy schedule with fraction
sizes >2 Gy would increase the risk of cardiac mortality in women with localised left-sided
breast cancer compared with schedules with fraction sizes ≤2 Gy.9 The study reported there
was no significant difference in cardiac mortality for women ≤60 or >60 years of age who
received adjuvant radiotherapy for left-sided vs. right-sided cancer. There was no difference
in cardiac mortality for women who received adjuvant radiotherapy with fraction sizes ≤2 vs.
>2 Gy for left- or right-sided cancer. The study reported that the relative risk of cardiac death
for left- relative to right-sided radiotherapy with >2 Gy fractions was 1.07 (95% CI 0.68-1.69).
The authors concluded that the absence of a difference in cardiac mortality between
women treated for left-sided breast cancer with hypofractionated vs. conventional
fractionated radiotherapy adds further support to the efficacy of hypofractionated regimens
in this clinical setting.9
An additional randomised study of 60 patients was identified (Ibrahim 2014), however the
study population was small and had limited results. The authors concluded hypofractionated
radiotherapy decreased cardiac toxicity though not statistically significant, however it is
more cost effective and time consuming.
References
1. Haviland JS, Owen JR, Dewar JA, et al. The UK Standardisation of Breast Radiotherapy
(START) trials of radiotherapy hypofractionation for treatment of early breast cancer:
10-year follow-up results of two randomised controlled trials. Lancet Oncol.
2013;14(11):1086-94.
2. Spooner D, Stocken DD, Jordan S, et al. A Randomised Controlled Trial to Evaluate
both the Role and the Optimal Fractionation of Radiotherapy in the Conservative
Management of Early Breast Cancer. Clinical Oncology. 2012;24(10):697-706.
3. FAST Trialists group, Agrawal RK, Alhasso A, et al. First results of the randomised UK FAST
Trial of radiotherapy hypofractionation for treatment of early breast cancer
(CRUKE/04/015). Radiother Oncol. 2011;100(1):93-100
4. Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation
therapy for breast cancer. N Engl J Med. 2010;362(6):513-20.
5. Owen JR, Ashton A, Bliss JM, et al. Effect of radiotherapy fraction size on tumour
control in patients with early-stage breast cancer after local tumour excision: long-
term results of a randomised trial. Lancet Oncol. 2006;7(6):467-71.
6. Haffty BG, Buchholz TA. Hypofractionated breast radiation: preferred standard of
care? Lancet Oncol. 2013;14(11):1032-4.
7. Chan EK, Woods R, McBride ML, et al. Adjuvant hypofractionated versus conventional
whole breast radiation therapy for early-stage breast cancer: long-term hospital-
related morbidity from cardiac causes. Int J Radiat Oncol Biol Phys. 2014;88(4):786-92.
8. Appelt AL, Vogelius IR, Bentzen SM. Modern hypofractionation schedules for
tangential whole breast irradiation decrease the fraction size-corrected dose to the
heart. Clin Oncol (R Coll Radiol). 2013;25(3):147-52.
9. Marhin W, Wai E, Tyldesley S. Impact of fraction size on cardiac mortality in women
treated with tangential radiotherapy for localized breast cancer. Int J Radiat Oncol
Biol Phys. 2007;69(2):483-9.

7
10. Chan EK, Woods R, Virani S, et al. Long-term mortality from cardiac causes after
adjuvant hypofractionated vs. conventional radiotherapy for localized left-sided
breast cancer. Radiother Oncol. 2014 early online 13th September 2014.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic
review
November 2011

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review was
developed by:
Cancer Australia
Locked Bag 3 Strawberry Hills NSW 2012 Australia
Tel: +61 2 9357 9400 Fax: +61 2 9357 9477
Website: www.canceraustralia.gov.au
© Cancer Australia 2011
ISBN Online: 978-1-74127-180-5
Recommended citation
Cancer Australia. Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review.
National Breast and Ovarian Cancer Centre, Surry Hills, NSW, 2011
Copyright statements:
Paper-based publications
This work is copyright. You may reproduce the whole or part of this work in unaltered form for your own personal use
or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation do
not use the reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as
part of that reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this
copyright notice, all other rights are reserved and you are not allowed to reproduce the whole or any part of this
work in any way (electronic or otherwise) without first being given the specific written permission from Cancer
Australia to do so. Requests and inquiries concerning reproduction and rights are to be sent to the Publications and
Copyright contact officer, Cancer Australia, Locked Bag 3, Strawberry Hills, NSW 2012.
Internet sites
This work is copyright. You may download, display, print and reproduce the whole or part of this work in unaltered
form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only
if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice
and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act
1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the
whole or any part of this work in any way (electronic or otherwise) without first being given the specific written
permission from Cancer Australia to do so. Requests and inquiries concerning reproduction and rights are to be sent
to the Publications and Copyright contact officer, Cancer Australia, Locked Bag 3, Strawberry Hills, NSW 2012
Copies of Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review can be
downloaded from the Cancer Australia website: www.canceraustralia.gov.au.

Acknowledgments
This report was prepared on behalf of National Breast and Ovarian Cancer Centre (NBOCC)* by
Lisa Elliott, Gregory Merlo and Adele Watson of Health Technology Analysts.
NBOCC gratefully acknowledges the contribution of the Hypofractionated Radiotherapy Working
Group, chaired by Associate Professor Boon Chua (see Appendix A).
Funding
Funding for the development of this systematic review was provided by the Australian
Government Department of Health and Ageing.
*On 1 July 2011, National Breast and Ovarian Cancer Centre (NBOCC) amalgamated with Cancer Australia to form a single national agency, Cancer Australia, to provide leadership in cancer control and improve outcomes for Australians affected by cancer.


Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
v
Contents
Executive summary ...................................................................................................................... ix
1 Introduction ........................................................................................................................ 1
2 Method ................................................................................................................................ 3
2.1 Criteria for determining study eligibility ................................................................... 3
2.2 Literature search methodology ............................................................................... 3
2.3 Assessment of study eligibility ................................................................................ 6
2.4 Included trials .......................................................................................................... 7
2.5 Appraisal of included trials ...................................................................................... 8
2.6 Limitations of the review ....................................................................................... 10
3 Description of included studies ..................................................................................... 12
3.1 Systematic reviews ............................................................................................... 12
3.2 Primary studies ..................................................................................................... 13
4 Results of included trials ................................................................................................ 23
4.1 Local recurrence ................................................................................................... 23
4.2 Local-regional recurrence ..................................................................................... 28
4.3 Distant relapse ...................................................................................................... 30
4.4 Overall survival ...................................................................................................... 32
4.5 Adverse events and toxicity .................................................................................. 35
4.6 Cosmetic outcome ................................................................................................ 41
4.7 Quality of life ......................................................................................................... 54
5 Guidelines ........................................................................................................................ 58
5.1 Guidelines search ................................................................................................. 58
5.2 Results .................................................................................................................. 58
6 Conclusions ..................................................................................................................... 63
7 References ....................................................................................................................... 65
Appendix A Contributors ........................................................................................................ 67

vi Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Tables
Table 1 Summary of key results for local recurrence ................................................................ x
Table 2 Summary of key results for regional recurrence .......................................................... xi
Table 3 Summary of key results for distant relapse .................................................................. xi
Table 4 Summary of key results for overall survival ................................................................. xii
Table 5 Summary of key results for adverse events and toxicity ............................................ xiii
Table 6 Summary of key results for adverse cosmetic outcomes ........................................... xiv
Table 7 Criteria for determining study eligibility ......................................................................... 3
Table 8 Search strategy ............................................................................................................. 5
Table 9 Exclusion criteria ........................................................................................................... 6
Table 10 Included and excluded citations .................................................................................... 7
Table 11 Included systematic reviews ......................................................................................... 8
Table 12 Included RCTs ................................................................................................................. 8
Table 13 NHMRC Dimensions of evidence21
................................................................................. 9
Table 14 NHMRC Interim Levels of Evidence (NHMRC 2009) for evaluating interventions and diagnostic accuracy studies
22 ........................................................... 9
Table 15 Quality criteria for different levels of evidence21
........................................................ 10
Table 16 Reporting biases in systematic reviews23
...................................................................... 11
Table 17 Key characteristics of included studies ....................................................................... 14
Table 18 RMH/GOC trial: Demographic and clinical characteristics of 1410 patients randomised
8 ................................................................................................................ 16
Table 19 Canadian trial: Patient characteristics7 ....................................................................... 17
Table 20 START A: Patient characteristics4 .............................................................................. 19
Table 21 START B: Patient characteristics5 .............................................................................. 21
Table 22 RMH/GOC trial: Survival analysis of local relapse according to fractionation schedule
1 ..................................................................................................................... 23
Table 23 START A: Survival analyses of relapse and mortality according to fractionation schedule (Local relapse)
4 ....................................................................... 27
Table 24 START B: Survival analyses of relapse and mortality according to fractionation schedule (local relapse)
5 ........................................................................ 27
Table 25 Summary of key results for local recurrence .............................................................. 28
Table 26 START A: Survival analyses of relapse and mortality according to fractionation schedule (Local-regional relapse)
4 ......................................................... 29
Table 27 START B: Survival analyses of relapse and mortality according to fractionation schedule (Local-regional Relapse)
5 ....................................................... 29
Table 28 Summary of key results for local-regional recurrence4-5
............................................. 30
Table 29 START A: Survival analyses of relapse and mortality according to fractionation schedule (Distant relapse)
4 ................................................................... 30
Table 30 START B: Survival analyses of relapse and mortality according to fractionation schedule (Distant relapse)
5 .................................................................... 31

Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
vii
Table 31 Summary of key results for distant relapse4-5
............................................................. 31
Table 32 Canadian trial: Cause of deaths2 ................................................................................ 33
Table 33 START A: Survival analyses of relapse and mortality according to fractionation schedule (All-cause mortality)
4 ............................................................... 33
Table 34 START B: Survival analyses of relapse and mortality according to fractionation schedule (All-cause mortality)
5 ............................................................... 34
Table 35 Summary of key results for overall survival ................................................................ 34
Table 36 Canadian trial: Late toxic effects of radiation, assessed according to the RTOG-EORTC late radiation morbidity scoring scheme
a2 ......................................... 35
Table 37 START A: Incidence of ischemic heart disease, symptomatic rib fracture, and symptomatic lung fibrosis according to fractionation schedule
4 ................................. 36
Table 38 START A: Contralateral and other secondary cancers4 ............................................. 36
Table 39 START B: Incidence of ischemic heart disease, symptomatic rib fracture, and symptomatic lung fibrosis according to fractionation schedule
5 ................................. 37
Table 40 START B: Contralateral and other secondary cancers5 ............................................. 37
Table 41 Summary of key results for adverse events and toxicity ............................................ 40
Table 42 RMH/GOC trial: Survival analyses of change in breast appearance and clinical assessments of late radiation effects according to fractionation schedule
8 .................................................................................................................... 44
Table 43 START A AND B: Survival analyses of moderate or marked grade normal tissue effects from patients’ self-assessments, according to fractionation schedule, type of primary surgery
6.............................................................................. 46
Table 44 Canadian trial: Global cosmetic outcome assessed according to the EORTC scale
a2 .......................................................................................................................... 47
Table 45 START A AND B: Survival analyses of moderate or marked grade normal tissue effects from patients’ self-assessments according to fractionation schedule, type of primary surgery
6.............................................................................. 48
Table 46 START A: Mild or marked change in breast appearance4 .......................................... 49
Table 47 START B: Mild or marked change in breast appearance5 .......................................... 50
Table 48 Summary of key results for cosmetic outcomes ......................................................... 53
Table 49 START A AND B: Breast, arm, or shoulder symptoms and body image scale scores at 5 years
a according to radiotherapy regimen, type of primary
surgery6 ....................................................................................................................... 55
Table 50 START A AND B: Breast, arm, or shoulder symptoms and body image scale scores at 5 years
a according to radiotherapy regimen, type of primary
surgery6 ....................................................................................................................... 56
Table 51 START A AND B: Breast, arm, or shoulder symptoms and body image scale scores, according to radiotherapy regimen, over time from randomisation
6 .............. 57
Table 52 Search terms for guidelines websites ......................................................................... 58

viii Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Figures
Figure 1 RMH/GOC trial: Local ipsilateral relapse in the breast according to fractionation scheudule
1 .............................................................................................. 24
Figure 2 Canadian trial: Kaplan-Meier estimates for local recurrencea2
................................... 25
Figure 3 Canadian trial: Hazard ratios for Ipsilateral recurrence of breast cancer in subgroups of patients
2 ................................................................................................. 26
Figure 4 Canadian trial: Kaplan-Meier estimate for overall survival2 ........................................ 32
Figure 5 START A AND B: Forest plots of normal tissue effects assessed as moderate or marked by patients, according to radiotherapy regimens
6 ..................................... 39
Figure 6 RMH/GOC trial: Probability of any change in breast appearance late radiation effect ten years after radiotherapy by fractionation schedule
8 .................................... 42
Figure 7 RMH/GOC trial: Probability of marked change in breast appearance late radiation effect ten years after radiotherapy by fractionation schedule
8..................... 42
Figure 8 RMH/GOC trial: Probability of palpable breast induration ten years after radiotherapy by fractionation schedule
8 ...................................................................... 43
Figure 9 START A: Kaplan-Meier plot of mild/marked change in breast appearance (photographic) in 1055 patients with breast conserving surgery
4 ............................... 49
Figure 10 START B: Kaplan-Meier plot of mild/marked change in breast appearance (photographic) in 923 patients with breast conserving surgery
5 ................................. 50
Figure 11 START A AND B: Forest plots of normal tissue effects assessed as moderate or marked by patients, according to radiotherapy regimen
6 ....................................... 52

Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
ix
Executive summary
Introduction and methods
This review was commissioned by the National Breast and Ovarian Cancer Centre (NBOCC).
The use of hypofractionated radiotherapy in early breast cancer has been identified as a topic for
evidence review and guideline recommendation development. The following clinical question was
selected as the focus of the systematic literature review:
What are the key outcomes associated with different dose fractionation
(dosage/scheduling) for radiotherapy treatment of early (invasive) breast cancer?
A systematic method of literature searching and selection was employed in the preparation of
this review. Searches were conducted in EMBASE and Medline (via EMBASE.com) and the
Cochrane Database of Systematic Reviews to identify citations published between January 2001
and March 2010. A search of conference websites was also conducted. These were the
American Society of Clinical Oncology, American Society of Radiation Oncology and San
Antonio Breast Cancer Symposium. A total of 682 non-duplicate citations were identified. The
exclusion criteria was applied to all citations, with a total of 10 publications meeting the inclusion
criteria.
Key findings
Local recurrence
All five included trials reported local recurrence (RMH/GOC, Canadian, Spooner, START A and
START B) (see Table 1). There was no evidence that any hypofractionated radiotherapy regimen
was associated with a statistically significant difference in local recurrence rate when compared
with a control arm. The Royal Marsden Hospital/Gloucester Oncology Centre (RMH/GOC) trial
noted a statistically significant difference in recurrence rates when the two hypofractionated
radiotherapy regimens were compared (42.9 Gy vs 39 Gy: 9.6% vs 14.8%, p=0.027), but not
when each regimen was compared to the control arm (50 Gy in 25 fractions).1
Subgroup analyses were performed in the Canadian trial.2 There were no significant differences
in any subgroup, with the exception of tumour grade. The impact of the 42.5 Gy regimen on local
recurrence was less in patients with high-grade tumours compared to patients with low-grade
tumours (p=0.01).2
On 1 July 2011, National Breast and Ovarian Cancer Centre (NBOCC) amalgamated with Cancer Australia to form a single national agency, Cancer Australia, to provide leadership in cancer control and improve outcomes for Australians affected by cancer.

x Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 1 Summary of key results for local recurrence
Study ID Study arms Results
Post breast conserving surgery
RMH/GOC1 39 Gy in 13 fractions over 5 weeks
42.9 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local recurrence
39 Gy vs 50 Gy: 9.1% vs 7.9%, p=NR
42.9 Gy vs 50 Gy: 7.1% vs 7.9%, p=NR
42.9 Gy vs 39 Gy: 7.1% vs 9.1%, p=NR
10 year local recurrence
39 Gy vs 50 Gy: 14.8% vs 12.1%, p=NS
42.9 Gy vs 50 Gy: 9.6% vs 12.1%, p=NS
42.9 Gy vs 39 Gy: 9.6% vs 14.8%, p=0.027
39 Gy: HR 1.33 (95% CI 0.92, 1.92), p=NS
42.9 Gy: HR 0.86 (95% CI 0.57, 1.30), p=NS
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
10 year cumulative incidence of local recurrence
42.5 Gy vs 50 Gy: 6.2% vs. 6.7%, p=NS
10 year cumulative incidence of invasive or non-invasive local recurrence 42.5 Gy vs 50 Gy: 7.4% vs. 7.5%, p=NS
Subgroup analyses
Patient age, tumour size, oestrogen-receptor status, tumour grade, systemic therapy, p=NS
High-grade vs low grade tumours, p=0.01
Any surgery
Spooner3
40 Gy in 15 fractions once a day
50 Gy in 25 fractions once a day
Delayed salvage treatment
17 year relapse frequency
No difference, data not reported
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local relapse rate
50 Gy vs 41.6 Gy vs 39 Gy: 3.2% vs 3.2% vs 4.6%, p=NR
5 year local relapse
39 Gy: HR 1.25 (95% CI 0.74, 2.12), p=0.40
41.6 Gy: HR 1.09 (95% CI 0.64, 1.88), p=0.74
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local relapse rate
50 Gy vs 40 Gy: 3.3% vs 2.0%, p=NR
5 year local relapse
40 Gy: HR 0.72 (95% CI 0.43, 1.21), p=0.21
Abbreviations: CI=confidence interval, HR=hazard ratio, NR=not reported, NS=not significant * control arm
Local-regional recurrence
The Standardisation of Breast Radiotherapy Trials A and B (START A and START B) reported
regional recurrence (see Table 2).4-5
There was no evidence that any hypofractionated
radiotherapy regimen was associated with a statistically significant difference in local recurrence
rate when compared with 50 Gy in 25 fractions over 5 weeks (control).

Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
xi
Table 2 Summary of key results for regional recurrence
Study ID Study arms Results
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local-regional relapse rate
50 Gy vs 41.6 Gy vs 39 Gy: 3.6% vs 3.5% vs 5.2%, p=NR
5 year local-regional relapse
39 Gy: HR 1.26 (95% CI 0.77, 2.08), p=0.35
41.6 Gy: HR 1.05 (95% CI 0.63, 1.75), p=0.86
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local-regional relapse rate
50 Gy vs 40 Gy: 3.3% vs 2.2%, p=NR
5 year local-regional relapse
40 Gy: HR 0.79 (95% CI 0.48, 1.29), p=0.35
Abbreviations: CI=confidence interval; HR=hazard ratio; NR=not reported * control arm
Distant relapse
Two trials reported distant relapse (START A and START B) (see
Table 3).4-5
In START A, there was no statistical difference between either of the
hypofractionated regimen compared with the control arm.4 START B reported that the 40 Gy
study arm had a statistically significantly lower rate of distant relapse when compared with the
control arm (HR 0.69 95% CI 0.53, 0.91, p=0.01).5
Table 3 Summary of key results for distant relapse
Study ID Study arms Results
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year distant relapse rate
50 Gy vs 41.6 Gy vs 39 Gy: 9.8% vs 9.5% vs 11.9%, p=NR
5 year local-regional relapse
39 Gy: HR 1.29 (95% CI 0.95, 1.76), p=0.10
41.6 Gy: HR 0.92 (95% CI 0.66, 1.28), p=0.64
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local-regional relapse rate
50 Gy vs 40 Gy: 10.2% vs 7.6%, p=NR
5 year local-regional relapse
40 Gy: HR 0.69 (95% CI 0.53, 0.91), p=0.01
Abbreviations: CI=confidence interval; HR=hazard ratio; NR=not reported * control arm
Overall survival
A total of four trials reported overall survival (RMH/GOC, Spooner, START A and START B) (see
Table 4).2-5
Most studies reported that there was no evidence that hypofractionated radiotherapy
was associated with a statistically significantly difference in overall survival. START B found that
40 Gy in 15 fractions over three weeks was associated with a statistically significantly lower all-
cause mortality rate when compared with 50 Gy in 25 fractions over five weeks (HR 0.76 95% CI

xii Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
0.59, 0.98, p=0.03).5 Therefore, there was no evidence that any hypofractionated radiotherapy
regimen was associated with a worse overall survival rate (i.e. the only study that reported a
significant difference showed lower mortality for patients treated with hypofractionated
radiotherapy).
Table 4 Summary of key results for overall survival
Study ID Study arms Results
Post breast conserving surgery
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
10 year survival
42.5 Gy vs 50 Gy: 84.6% vs 84.4%, p=0.79
Any surgery
Spooner3 40 Gy in 15 fractions once a day
50 Gy in 25 fractions once a day
17 year survival
No difference, data not reported
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year all cause mortality
39 Gy: HR 1.00 95% CI 0.74, 1.36, p=0.99
41.6 Gy: HR 1.04 95% CI 0.77, 1.40, p=0.81
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year all cause mortality
40 Gy: HR 0.76 95% CI 0.59, 0.98, p=0.03
Abbreviations: CI=confidence interval, HR=hazard ratio * control arm
Adverse events and toxicity
A total of three trials reported adverse events and toxicity outcomes (Canadian, START A and
START B) (see Table 5).2, 4-5
Most studies reported that there was no difference in adverse
events and toxicity. Combined results from the START A and START B trials found that a change
in skin appearance occurred significantly less often in the 39 Gy and 40 Gy arms when
compared with the control arm (39 Gy HR 0.63 95% CI 0.47, 0.84, p=0.0019 and 40 Gy HR 0.76
95% CI 0.60, 0.97, p=0.0262).6

Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
xiii
Table 5 Summary of key results for adverse events and toxicity
Study ID Study arms Results
Post breast conserving surgery
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
Late toxic radiation effects, : NS
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
Ischemic heart disease, symptomatic rib fracture, symptomatic lung fibrosis, contralateral breast cancer, other secondary primary cancers: NS
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
Ischemic heart disease, symptomatic rib fracture, symptomatic lung fibrosis, contralateral breast cancer, other secondary primary cancers: NS
Combined QoL data from START A and B6
As for START A and START B Tissue effects, arm and shoulder symptoms: NS
Skin appearance: 39 Gy HR 0.63 (95% CI 0.47, 0.84), p=0.0019
40 Gy HR 0.76 (95% CI 0.60, 0.97), p=0.0262
Abbreviations: CI=confidence interval, HR=hazard ratio, NS=not significant * control arm a Assessed 3, 5, and 10 years after randomisation
Cosmetic outcome
A total of four trials reported cosmetic outcome (RMH/GOC, Canadian, START A and START B)
(see Table 6).2, 4-5, 7-8
There was no statistically significant difference in the majority of cosmetic
outcomes assessed by the included publications. RMH/GOC reported that the risk of developing
any late radiation effect was statistically significantly lower for patients in the 39 Gy arm
compared to the 50 Gy arm (p=0.01). For most clinically assessed breast and arm outcomes
estimated at 10 years, compared to the 50 Gy arm, there were fewer events for patients in the 39
Gy arm and more in the 42.9 Gy arm.
The START A trial reported that the 39 Gy arm was associated with significantly less mild or
marked change in photographic breast appearance by photographic assessment (HR 0.69 95%
CI 0.52, 0.91, p=0.01),4 and change in skin appearance by patient self-assessment (HR 0.63
95% CI 0.47, 0.84, p=0.0019).6 The 40 Gy arm of the START B trial was associated with
significantly less change in skin appearance by patient self assessment (40 Gy: HR 0.76 95% CI
0.60, 0.97, p=0.0262).6
In subgroup analyses for the START A and START B trials, the relative effects of the randomised
radiation schedules on patient reported symptoms did not vary significantly according to type of
primary surgery (breast conserving surgery or mastectomy).6

xiv Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 6 Summary of key results for adverse cosmetic outcomes
Study ID Study arms Results
Post breast conserving surgery
RMH/GOC8 39 Gy in 13 fractions over 5 weeks
42.9 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
39 Gy: adverse cosmetic outcomes were reported less frequently when compared to the 50 Gy arm (p=0.01)
42.9 Gy: Cosmetic outcomes were reported more frequently when compared to the 50 Gy arm (p=0.05)
Canadian2, 7 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
No statistically significant differences in any cosmetic outcome
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
41.6 Gy: No statistically significant differences in any cosmetic outcome
39 Gy: No statistically significant differences in cosmetic outcome, with the exception of mild or marked change in breast appearance (HR 0.69 95% CI 0.52, 0.91, p=0.01)
START B5 40 Gy in 15 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
0.77 (95% CI 0.61-0.98) p=0.02
Combined data from START A and B6
As for START A and START B Change in skin appearance
39 Gy: HR 0.63 (95% CI 0.47, 0.84), p=0.0019
40 Gy: HR 0.76 (95% CI 0.60, 0.97), p=0.0262
Subgroup analysis by breast conserving surgery and mastectomy: NS
Abbreviations: CI=confidence interval, HR=hazard ratio, NS=not significant * control arm
Quality of life
A total of two studies reported quality of life outcomes (START A and START B). 6 There was no
evidence that any hypofractionated radiotherapy regimen was associated with a statistically
significant difference in quality of life score as measured by the BR23 breast symptom subscale.
Subgroup analysis was performed, with results analysed by surgery type. There were no
statistically significant differences in outcomes, nor were any interaction tests significant overall.
Guidelines
In order to identify current recommendations in existing radiotherapy guidelines, a systematic
search of guidelines was undertaken.
The American Society for Radiation Oncology (ASTRO)9 reported that evudebce supports the
equivalence of hypofractionated whole breast irradiation with conventionally fractionated whole
breast irradiation for patients who satisfy all these criteria:
Patient is 50 years or older at diagnosis.
Pathologic stage is T1-2 N0 and patient has been treated with breast-conserving surgery.
Patient has not been treated with systemic chemotherapy.

Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
xv
Within the breast along the central axis, the minimum does is no less than 93% and
maximum dose is no greater than 107% of the prescription does ±7% (as calculated with
2-dimensional treatment planning without heterogeneity corrections)
For patients who do not satisfy all of these criteria, the task force could not reach consensus and
therefore chose not to render a recommendation.9
The New Zealand Ministry of Health guidelines10
made the following recommendation
regarding hypofractionated radiotherapy:
Recommendation
• Radiotherapy treatment for early invasive breast cancer should use an accepted regimen such
as: 50 Gy in 25 fractions over 5 weeks (Grade A†), 45 Gy in 20 fractions over 5 weeks (Grade
B‡), 42.5 Gy in 16 fractions over 3.5 weeks for those with small or medium breasts, not requiring
boost or nodal radiation (Grade B†), 40 Gy in 15 fractions over 3 weeks (Grade B
2)
Good practice points
• If boost radiotherapy is used after a hypofractionated regimen it should be at the standard 2 Gy
per fraction
• Women with large breasts and those with significant postoperative induration, oedema,
erythema, haematoma or infection should be considered for extended fractionation, with smaller
daily doses over 5–6 weeks
The NICE 2009 guidelines11
made the following recommendation regarding dose fractionation:
Recommendation
• Use external beam radiotherapy giving 40 Gy in 15 fractions as standard practice for patients
with early invasive breast cancer after breast conserving surgery or mastectomy.
Qualifying statement: This recommendation is based on RCT evidence of clinical effectiveness
and the guideline development group agreeing that a regimen using fewer fractions would
probably be cost effective.
The Scottish Intercollegiate Guidelines Network (SIGN)12
management of breast cancer in
women guidance paper was developed in 2005, prior to the publication of a number of key RCTs
(such as the START trials). No formal recommendations were made.
† ie, body of evidence can be trusted to guide practice.
‡ ie, body of evidence can be trusted to guide practice in most situations


A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 1
1 Introduction
Aim
This review was commissioned by the National Breast and Ovarian Cancer Centre
(NBOCC), Australia’s national authority and source of evidence-based information on
breast and ovarian cancer. In 2001, NBOCC published the second edition of the “Clinical
practice guidelines for the management of early breast cancer”13
which replaced the first
edition released in 1995. NBOCC’s approach to maintaining the currency of these
guidelines is to produce timely topic-specific guideline recommendations in key areas of
changing evidence.
Based on input from a multidisciplinary Steering Committee and additional consultation by
NBOCC, the use of hypofractionated radiotherapy in early breast cancer was identified as a
topic for evidence review and guideline recommendation development. The
Hypofractionated Radiotherapy Working Group selected the following clinical question as
the focus of the systematic literature review:
What are the key outcomes associated with different dose fractionation
(dosage/scheduling) for radiotherapy treatment of early (invasive) breast cancer?
In order to answer this clinical question, a systematic literature search was conducted. The
methods and results are described in detail in the following sections.
Radiotherapy for treatment of early breast cancer
Early breast cancer has been defined as tumours of not more than five centimetres
diameter, with either impalpable or palpable but not fixed lymph nodes and with no
evidence of distant metastases.13
This corresponds to tumours that are T1-2, N0-1, M0 as
currently defined by the International Union Against Cancer (UICC).7
Early breast cancer can be treated with a range of therapies including surgery, radiotherapy
and systematic adjuvant therapy. A recent Cochrane Review noted that over the last three
decades standard management practices have changed.14
Previously, most women with
early breast cancer underwent removal of the whole breast (mastectomy). However,
following a number of clinical studies, breast conserving surgery followed by radiotherapy
has become the recommended option for women with early breast cancer.13-15
Different tissue types (including malignant tissue types) have different sensitivities to
radiation and therefore respond to different radiotherapy fraction sizes. In clinical oncology
a model is used in which the sensitivity to fraction size (measured by the degree of tissue
damage for normal tissues, and tumour recurrence rates for malignant tumours) is
represented by the constants α and β.4 The lower the ratio of these constants (expressed in
Gy), the greater the effect of fraction size on the tissue. The most appropriate radiotherapy
regimen may therefore differ between tissue types. The choice of dose in radiotherapy
must balance the risk of local cancer recurrence against the harmful effects on healthy
tissues.

2 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
In a “standard” whole breast radiotherapy regime, radiation is delivered over a period of 5
to 6 weeks using a standard 2 Gy radiation dose per fraction, in 25 to 30 treatment
episodes, to a total dose of 50 to 60 Gy.14
Some regimens include an additional boost of
radiation. In hypofractionated radiotherapy, patients receive fewer fractions, however each
fraction contains a larger dose of radiation. Although the dose of each individual fraction is
higher than the conventional regimen, the total dose of radiotherapy is lower. Concerns
have been raised, however, as to whether shorter fractionation schedules have equivalent
outcomes in terms of local tumour control, breast appearance (cosmesis), overall survival,
and patient satisfaction. The concern with larger fraction sizes has been raised as
radiobiological principles state that the fraction size is the dominant factor in determining
late side effects.14
Higher fraction size could lead to increased scarring and retraction of
breast tissue as well as skin atrophy (thinning) and telangiectasia (dilated blood vessels).
Economic considerations
One consequence of the increase in breast conserving surgery and radiotherapy is the
extra demand placed on health services.14, 16-17
Shorter fractionation schedules have the
advantages of using machine and staff time more efficiently and reducing patient
inconvenience. 18
Hypofractionated radiotherapy significantly reduce the amount of time
that patients require radiotherapy equipment. A reduction of time per patient on the
machine of about 50 minutes and 100 minutes for the patients exposed to 35 Gy over two
weeks and those exposed to 27 Gy over one week respectively, compared with those
exposed to 40 Gy in three weeks has been reported.18
A cohort study (n=313) conducted in
Brisbane’s Princess Alexandra Hospital found that, compared to conventional radiotherapy,
hypofractionated radiotherapy was associated with a 26% reduction per patient in the cost
to Medicare *.19
* Dwyer et al 2009 is a conference abstract and little detail is provided of the resource utilization. The estimation for the reduction in Medicare cost appears to be based on the inference from the cohort study results that had the entire cohort received hypofractionated radiotherapy, 288 fractions per month would be ‘saved’ and available for treatment in other cancer patients.

A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 3
2 Method
2.1 Criteria for determining study eligibility
The criteria for determining study eligibility are shown in Table 7. Publications were eligible
for inclusion in the systematic literature review if they described a randomised controlled
trial (RCT) which recruited women with early (invasive) breast cancer and patients treated
by breast conserving surgery or total mastectomy.
Hypofractionated radiotherapy was defined by the Hypofractionated Radiotherapy Working
Group as ‘giving larger doses of radiotherapy per fraction, but giving fewer fractions
compared with standard radiotherapy’. RCTs must have compared hypofractionated
radiotherapy with either standard radiotherapy, or an alternative regimen of
hypofractionated radiotherapy.
The following outcomes were extracted from the publications: 1) local recurrence, 2) overall
survival, 3) adverse events, 4) toxicity, 5) cosmetic outcome and 6) quality of life (assessed
using a quality of life instrument). Results for subgroups were extracted where available.
The pre-defined subgroups were age, breast size/width, tumour grade, nodal status,
surgical margins, use in conjunction with nodal irradiation, post breast conserving surgery
and total mastectomy.
Table 7 Criteria for determining study eligibility
Study design Randomised, controlled trials
Population Women with early (invasive) breast cancer treated with surgery
Intervention Hypofractionated radiotherapy
Comparator 1. Standard radiotherapy
2. Other regimens of hypofractionated radiotherapy
Outcomes a 1. Local recurrence
2. Overall survival
3. Adverse events
4. Toxicity (including burns and blisters)
5. Cosmetic outcome
6. Quality of life (assessed using a quality of life instrument)
a The predefined subgroups were: age, breast size/width, tumour grade, nodal status, surgical margins, use in conjunction with nodal irradiation, post breast conserving surgery and total mastectomy
2.2 Literature search methodology
A systematic method of literature searching and selection was employed in the preparation
of this review. Searches for full-length publications and abstracts were conducted in
EMBASE and Medline (via EMBASE.com) and the Cochrane Database of Systematic
Reviews. At the request of the NBOCC and the Hypofractionated Radiotherapy Working
Group, searches were restricted to English language studies published from 2001 onwards.
Search terms were approved by the NBOCC prior to searches being conducted. The
reference lists of included papers were reviewed to identify any peer-reviewed evidence

4 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
that may have been missed in the literature search. Contacting of authors for unpublished
research was not undertaken. The searches were conducted prior to the 31st of March,
2010. Therefore, studies published after this time were not eligible for inclusion in the
systematic review.
The search strategy for the online bibliographic databases is shown in Table 8. A search of
conference websites was also conducted. Three conferences were selected by the NBOCC
and Hypofractionated Radiotherapy Working Group: American Society of Clinical Oncology,
American Society of Radiation Oncology and San Antonio Breast Cancer Symposium. The
same search terms were used for all conference abstracts. A total of 682 non-duplicate
citations were identified.

A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 5
Table 8 Search strategy
Database Date searched
# Search terms Citations
EMBASE + Medline
<1950 – 26 Mar 2010
1
'breast cancer'/exp OR 'breast cancer' OR 'breast gland cancer'/exp OR 'breast gland cancer' OR 'breast gland neoplasm'/exp OR 'breast gland neoplasm' OR 'mammary cancer'/exp OR 'mammary cancer' OR 'mammary gland cancer'/exp OR 'mammary gland cancer' OR 'breast neoplasm'
227,592
2 ('breast' OR 'breast'/exp OR breast) AND ('cancer' OR 'cancer'/exp OR cancer OR 'carcinoma' OR 'carcinoma'/exp OR carcinoma OR 'tumour' OR 'tumour'/exp OR tumour OR 'tumour' OR 'tumour'/exp OR tumour OR 'neoplasm'/exp OR neoplasm)
288,233
3 #1 OR #2 288,591
4
'radiotherapy'/exp OR 'radiotherapy' OR 'irradiation therapy'/exp OR 'irradiation therapy' OR 'irradiation treatment'/exp OR 'irradiation treatment' OR 'radiation therapy'/exp OR 'radiation therapy' OR 'radiation treatment'/exp OR 'radiation treatment' OR 'therapeutic radiology'/exp OR 'therapeutic radiology' OR 'radiation; therapy' OR 'treatment, irradiation'/exp OR 'treatment, irradiation'
385,244
5 fractionated OR hypofractionated OR fraction OR fractio* 418,274
6 #4 AND #5 26,442
7 'radiation dose fractionation'/exp OR 'radiation dose fractionation' OR 'dose fractionation'/exp OR 'dose fractionation' OR 'hypofractionated radiotherapy' OR 'fractionated radiotherapy'
10,331
8 #6 OR #7 26,554
9 #3 AND #8 2,275
10 #9 AND [1-1-2001]/sd NOT [9-4-2010]/sd 1,336
11
'clinical trial'/exp OR 'clinical trial' OR 'randomized controlled trial'/exp OR 'randomized controlled trial' OR 'randomised controlled trial'/exp OR 'randomised controlled trial' OR 'randomization' OR 'randomization'/exp OR randomization OR 'randomisation' OR 'randomisation'/exp OR randomisation OR 'meta-analysis'/exp OR 'meta-analysis' OR 'systematic review'/exp OR 'systematic review' OR 'guideline' OR 'single blind procedure'/exp OR 'single blind procedure' OR 'double blind procedure'/exp OR 'double blind procedure' OR 'triple blind procedure'/exp OR 'triple blind procedure' OR 'crossover procedure'/exp OR 'crossover procedure' OR 'placebo' OR 'placebo'/exp OR placebo OR randomi?ed:ab,ti OR rct:ab,ti OR 'random allocation':ab,ti OR 'randomly allocated':ab,ti OR 'allocated randomly':ab,ti OR (allocated NEAR/2 random*):ab,ti OR 'single blind':ab,ti OR 'single blinded':ab,ti OR 'double blind':ab,ti OR 'double blinded':ab,ti OR 'treble blind':ab,ti OR 'treble blinded':ab,ti OR 'triple blind':ab,ti OR 'triple blinded':ab,ti OR placebo*:ab,ti OR 'prospective study'/exp OR 'prospective study' NOT ('case study'/exp OR 'case study' OR 'case report':ab,ti OR 'abstract report'/exp OR 'abstract report' OR 'letter' OR 'letter'/exp OR letter)
1,344,424
12 #11 AND #10 535
Cochrane Library
1800 –30 Mar 2010
1 "breast cancer" or "breast gland cancer" OR "breast gland neoplasm" OR mammary cancer" OR "mammary gland cancer" OR "breast neoplasm"
11,726
2 breast AND (cancer OR carcinoma OR tumour OR tumour OR neoplasm) 13,831
3 radiotherapy OR "irradiation therapy" OR "irradiation treatment" OR "radiation therapy" OR radiology OR "therapeutic radiology"
17,142
4 fractionated OR hypofractionated OR fraction OR fractio* 11,864
5 ( #1 OR #2 ) AND #3 AND #4 211
ASCO 31 Mar 2010
1 “hypofractionated radiotherapy” OR “fractionated radiotherapy” OR “irradiation therapy” OR “irradiation treatment” OR “hypofractionated radiation treatment” OR “fractionated radiation treatment” OR “therapeutic radiology”
1
ASTRO 0
SABCS 3
Manual search 4
Total number of citations 756
Total number of non-duplicate citations 682
Abbreviations: ASCO=American Society of Clinical Oncology, ASTRO=American Society of Radiation Oncology, SABCS=San Antonio Breast Cancer Symposium

6 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
2.3 Assessment of study eligibility
Publications identified in the literature search were reviewed and the exclusion criteria
shown in Table 9 applied hierarchically. As the Cochrane search was not restricted by date,
the first exclusion criteria were all publications published prior to 2001 (the cut-off date for
inclusion in the systematic review). Publications were excluded if they were the wrong
study type (not an RCT), if they were in the wrong population (not women with early breast
cancer treated with surgery), evaluated the wrong intervention (not hypofractionated
radiotherapy) or the wrong comparator (not standard radiotherapy or another regimen of
hypofractionated radiotherapy). Publications were excluded if they reported the wrong
outcomes (as described in Table 9). Only English language publications were eligible for
inclusion.
Table 9 Exclusion criteria
Wrong year Study published prior to 2001
Wrong study type Not randomised controlled trials
Wrong population Not in women with early (invasive) breast cancer or patients treated with surgery
Wrong intervention Not hypofractionated radiotherapy
Wrong comparator Not standard radiotherapy or another regimens of hypofractionated radiotherapy
Wrong outcome Study did not report local recurrence, overall survival, adverse events, toxicity, cosmetic outcome, quality of life or a subgroup analysis of age, breast size/width, tumour grade, nodal status, surgical margins, use in conjunction with nodal irradiation, post breast conserving surgery or total mastectomy
Insufficient follow-up Follow-up of less than 5 years
Not in English Not in English
The exclusion criteria was applied to all citations by reviewing the abstract and title, with
665 publications excluded (shown in Table 10). A total of 17 publications remained, and the
full text version of each publication was retrieved and reviewed. The same exclusion criteria
were then applied to the full text articles. A total of 10 publications met the inclusion criteria.
In Taher et al. 2004,20
women with early breast cancer (n=30) were randomised to either i)
50 Gy in 25 fractions, followed by a boost to the tumour bed of 10 Gy in five fractions over
five days or ii) 42.5 Gy in 16 fractions over 22 days with no boost. The RCT was excluded
as the median follow-up was only 1.7 years. No statistical difference in acute skin reactions
or cosmetic outcomes was observed between patients in the treatment arms. The study did
not report local or regional recurrence, survival, or quality of life as outcomes.
Shahid et al. 200918
was excluded because although it included women with early breast
cancer, it was not limited to this population. For inclusion into this RCT, the primary lesion
must have been T2, T3, or T4, with a nodal status of N1, N2, N3, Nx or N0. The study did
not conduct subgroup analyses of women with early breast cancer.
In Shahid et al. 200918
, women were randomised to either i) 27 Gy in five fractions over one
week or ii) 35 Gy in 10 fractions over two weeks or iii) 40 Gy in 15 fractions over three
weeks (the control arm). The percentage of patients with local recurrence was 11%, 12%,
and 10% for those patients in the 27 Gy, 35 Gy, and 40 Gy arms respectively (p=0.91). The
five year overall survival was 87%, 83%, and 82% (p=0.89). Grade 1 skin reactions
occurred significantly more often in the 40 Gy arm compared with the 27 Gy arm and the 35

A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 7
Gy arm (62% vs 33% and 35%, p<0.05). However, the 40 Gy arm had a significantly lower
incidence of Grade 3 and 4 skin reactions compared with the 27 Gy arm, but not the 35 Gy
arm (14% vs 37% and 28%, p<0.05). No other adverse outcomes had a statistically
significant difference in incidence rates.
Table 10 Included and excluded citations
Exclusion criteria Number
Total citations 682
Citations excluded after review of abstract/title
Wrong year
Wrong study type
Wrong population
Wrong intervention
Wrong comparator
Wrong outcome
Not in English
Total excluded citations
88
186
57
334
0
0
0
665
Full papers reviewed 17
Citations excluded after review of full publication
Wrong study type
Wrong population
Wrong intervention
Wrong comparator
Wrong outcome
Insufficient follow-up
Not in English
Total excluded citations
2
2
1
1
0
1
0
7
Total included citations 10
2.4 Included trials
The literature search identified two systematic literature reviews (shown in Table 11) and
eight publications describing five RCTs (shown in Table 12). Hopwood et al. 20106
described combined results from both START A and START B and is therefore shown
twice in Table 12 (i.e. there are 11 citations in the table but only 10 included publications).
For all included trials (with the exception of Spooner 20083) there were at least two
publications describing the results of the same clinical trial. In almost all instances, the first
paper describes interim results (e.g. 5 years of follow-up) whereas the second paper
describes the full study results (e.g. 10 years of follow-up). Throughout the report data has
been taken from the most recent publication. In rare instances where this was not the case
(e.g. the earlier paper reporting different outcome to the more recent paper) this has clearly
been stated. Hopwood et al 2010 reported combined results from both the START A and
START B trials and therefore contained data not reported in the individual START A and
START B publications.6 This has been clearly referenced throughout the report.

8 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 11 Included systematic reviews
Study ID Citation
James 2008 James ML, Lehman M, Hider PN, Jeffery M, Francis DP, Hickey BE. Fraction size in radiation treatment for breast conservation in early breast cancer. Coch Data Syst Rev 2008;(3).
Kalogeridi 2009 Kalogeridi MA, Kelekis N, Kouvaris J, Platoni K, Kyrias G, Pectasides D et al. Accelerated hypofractionated radiotherapy schedules in breast cancer: A review of the current literature. Rev Recent Clin Trials 2009; 4(3):147-151.
Table 12 Included RCTs
Study ID Citations
Royal Marsden Hospital/Gloucester Oncology Centre (RMH/GOC)
Yarnold J, Ashton A, Bliss J, Homewood J, Harper C, Hanson J et al. Fractionation sensitivity and dose response of late adverse effects in the breast after radiotherapy for early breast cancer: Long-term results of a randomised trial. Radiother Oncol 2005; 75(1):9-17.
Owen JR, Ashton A, Bliss JM, Homewood J, Harper C, Hanson J et al. Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: long-term results of a randomised trial. Lancet Oncology 2006; 7(6):467-471.
Spooner (abstract only)
Spooner D, Stocken DD, Jordan S, Bathers S, Dunn JA, Jevons C, Morrison M, Oates G, Grieve R. A randomised controlled trial to evaluate both the role and optimal fractionation of radiotherapy in the conservative management of early breast cancer. San Antonio Breast Cancer Symposium, 2008.
Standardisation of Breast Radiotherapy Trial A (START A)
-START-Trialists'-Group, Bentzen SM, Agrawal RK, Aird EG, Barrett JM, Barrett-Lee PJ et al. The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet Oncol 2008; 9:331-341.
Hopwood P, Haviland JS, Sumo G, Mills J, Bliss JM, Yarnold JR. Comparison of patient-reported breast, arm, and shoulder symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol 2010; 11(3):231-240.
Standardisation of Breast Radiotherapy Trial B (START B)
-START-Trialists'-Group, Bentzen SM, Agrawal RK, Aird EG, Barrett JM, Barrett-Lee PJ et al. The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet 2008; 371:1098-1107.
Hopwood P, Haviland JS, Sumo G, Mills J, Bliss JM, Yarnold JR. Comparison of patient-reported breast, arm, and shoulder symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol 2010; 11(3):231-240.
Canadian Whelan T, MacKenzie R, Julian J, Levine M, Shelley W, Grimard L et al. Randomized trial of breast irradiation schedules after lumpectomy for women with lymph node-negative breast cancer. J Natl Inst 2002; 94(15):1143-1150.
Whelan TJ, Pignol JP, Levine MN, Julian JA, MacKenzie R, Parpia S et al. Long-term results of hypofractionated radiation therapy for breast cancer. New Engl J Med 2010; 362(6):513-520.
2.5 Appraisal of included trials
Dimensions of evidence
The aim of this review was to find the highest quality evidence to answer the clinical
questions being asked. In accordance with National Health and Medical Research Council
(NHMRC) guidance, the following dimensions of evidence were reviewed for each of the

A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 9
included studies (shown in Table 13). It is important to recognise that the value of a piece
of evidence is determined by all of these dimensions, not just the level of evidence.
Table 13 NHMRC Dimensions of evidence21
Dimension Reviewers definition
Strength of the evidence
Level
Quality
Statistical precision
The study design used, as an indication of the degree to which bias has been eliminated by the design alone. The levels reflect the effectiveness of the study design to answer the research question.
The methods used to minimise bias within an individual study (i.e., other than design per se)
An indication of the precision of the estimate of effect reflecting the degree of certainty about the existence of a true effect, as opposed to an effect due to chance
Size of effect Determines the magnitude of effect and whether this is of clinical importance
Relevance of evidence Considers the relevance of the study to the specific research question and the context in which the information is likely to be applied, with regard to a) the nature of the intervention, b) the nature of the population and c) the definition of the outcomes.
Each study was also assigned a level of evidence in accordance with the NHMRC (2009)
interim levels of evidence (see Table 14).22
The highest level of evidence available is a
systematic review of RCTs, which is considered the study type least subject to bias.
Individual RCTs also represent high-level evidence. Only systematic reviews and RCTs
were eligible for inclusion in this systematic review.
Table 14 NHMRC Interim Levels of Evidence (NHMRC 2009) for evaluating interventions and diagnostic accuracy studies22
Level Intervention
I * A systematic review of level II studies
II A randomised controlled trial
III-1 A pseudorandomised controlled trial
(i.e., alternate allocation or some other method)
III-2 A comparative study with concurrent controls:
• Non-randomised, experimental trial a
• Cohort study
• Case-control study
• Interrupted time series with a control group
III-3 A comparative study without concurrent controls:
• Historical control study
• Two or more single arm studies b
• Interrupted time series without a parallel control group
IV Case series with either post-test or pre-test/post-test outcomes
Source: National Health and Medical Research Council (2009)22 Note: When a level of evidence is attributed in the text of a document, it should also be framed according to its corresponding research question e.g., level II intervention evidence; level IV diagnostic evidence; level III-2 prognostic evidence. * A systematic review will only be assigned a level of evidence as high as the studies it contains, excepting where those studies are of level II evidence. a This also includes controlled before-and-after (pre-test/post-test) studies, as well as indirect comparisons (i.e., utilise A vs B and B vs C, to determine A vs C). b Comparing single arm studies i.e., case series from two studies.

10 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Even within the levels of evidence stated above, there is considerable variability in the
quality of evidence. In accordance with NHMRC guidelines, it was necessary to consider
the quality of each of the included studies. Quality assessment was based on criteria
reported by the NHMRC (2000), as shown in Table 15, with studies rated as good, fair or
poor quality.21
Table 15 Quality criteria for different levels of evidence21
Study type Quality criteria
Systematic review
Was an adequate search strategy used?
Were the inclusion criteria appropriate and applied in an unbiased way?
Was a quality assessment of included studies undertaken?
Were the characteristics and results of the individual studies appropriately summarised?
Were the methods for pooling the data appropriate?
Were sources of heterogeneity explored?
Randomised controlled trials
Was allocation to treatment groups concealed from those responsible for recruiting patients?
Was the study double-blinded?
Where outcomes assessors blinded to treatment allocation?
Were all randomised participants included in the analysis?
Were treatment groups well matched at baseline?
Was the study powered to detect a difference in primary outcome?
Source: Adapted from NHMRC (2000)21
Data synthesis
In addition to the level and quality of evidence of individual studies, the review considered
the body of evidence in total. This involved consideration of the volume of evidence and its
consistency.
The review presented the statistical precision of the estimated effect size, together with a
discussion of its clinical significance. Finally, the review considered the relevance of the
evidence, both with regard to the generalisablity of the patient population and the
intervention, as well as the applicability to the Australian health care setting.
2.6 Limitations of the review
This review used a structured approach to review the literature. However, there are some
inherent limitations with this approach. All types of study are subject to bias, with
systematic reviews, such as the one conducted here, being subject to the same biases
seen in the original studies they include, as well as biases specifically related to the
systematic review process. Reporting biases are a particular problem related to systematic
reviews and include publication bias, time-lag bias, multiple publication bias, language bias
and outcome reporting bias. A brief summary of the different types of reporting bias is
shown in Table 16. Other biases can result if the methodology to be used in a review is not
defined a priori (i.e., before the review commences). Detailed knowledge of studies
performed in the area of interest may influence the eligibility criteria for inclusion of studies
in the review and may therefore result in biased results. For example, studies with more
positive results may be preferentially included in a review, thus biasing the results and
overestimating treatment effect.

A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 11
Table 16 Reporting biases in systematic reviews23
Type of bias Definition and effect on results of review
Publication bias The publication or non-publication of research findings.
Small, negative trials tend not to be published and this may lead to an overestimate of results of a review if only published studies are included.
Time-lag bias The rapid or delayed publication of research findings.
Studies with positive results tend to be published sooner than studies with negative findings and hence results may be overestimated until the negative studies ‘catch up’.
Multiple publication bias The multiple or singular publication of research findings.
Studies with significant results tend to be published multiple times which increases the chance of duplication of the same data and may bias the results of a review.
Citation bias The citation or non-citation of research.
Citing of trials in publications is not objective so retrieving studies using this method alone may result in biased results. Unsupported studies tend to be cited often which may also bias results.
Language bias The publication of research findings in a particular language.
Significant results are more likely to be published in English so a search limited to English-language journals may result in an overestimation of effect.
Outcome reporting bias The selective reporting of some outcomes but not others.
Outcomes with favourable findings may be reported more. For example, adverse events have been found to be reported more often in unpublished studies. This may result in more favourable results for published studies.
Source: Adapted from Egger et al. (2001).23
Some of these biases are potentially present in this review. The search was limited to
English-language publications only, so language bias is a potential problem. Outcome
reporting bias and inclusion criteria bias are unlikely as the reviewers had no detailed
knowledge of the topic literature, and the methodology used in the review and the scope of
the review were defined a priori.
The majority of studies included in this review were conducted outside Australia, and
therefore, their generalisablity to the Australian population and context needs to be
considered. This review was confined to an examination of the efficacy and safety of the
interventions and did not consider ethical or legal considerations associated with those
interventions.
The studies were initially selected by examining the abstracts of these articles. Therefore, it
is possible that some studies were inappropriately excluded prior to examination of the full
text article. However, where detail was lacking, ambiguous papers were retrieved as full
text to minimise this possibility. Data extraction, critical appraisal and report preparation
was performed by one reviewer and double-checked by another. The review was
conducted over a limited timeframe (March 2010 – June 2010).

12 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
3 Description of included studies
3.1 Systematic reviews
The literature search identified two systematic literature reviews.
3.1.1 James 2008
This Cochrane Review aimed to assess the effects of altered fraction size on women with
early breast cancer who have undergone breast conserving surgery. The Cochrane Breast
Cancer Group Specialised Register, MEDLINE, EMBASE, reference lists for articles and
relevant conference proceeding were searched. The inclusion criteria were randomised
controlled trials of unconventional versus conventional fractionation in women with early
breast cancer who had undergone breast conserving surgery. Two trials were included:
RMH/GOC1, 8
and Canadian.2, 7
Both trials were identified in the literature search conducted
for this systematic literature review, and have been discussed in detail in the following
sections.
There were no significant differences between the fractionation regimens in regard to
cosmesis, late skin toxicity, or late radiation toxicity. For overall survival, there was no
significant difference between the regimens. No data were available for costs, quality of life,
or women’s preference. The publication acknowledged the limitations related to
assessment of subjective outcomes, such as cosmesis and breast induration.
Although both trials independently showed no difference in local control with altered
fractionation, the reporting did not allow combination of data. The findings of this review
provided reassurance that the practice of offering shortened radiation fractionation regimes
to carefully selected groups of patients is unlikely to be detrimental in terms of breast
appearance, late radiation breast toxicity, or survival.
3.1.2 Kalogeridi 2009
The authors conducted a literature search using MEDLINE, although the search strategy
was not reported in the publication. Eight non-randomised trial and four randomised trials
(RMH/GOC1, 8
, Canadian2, 7
, START A4 and START B
5) were identified. All randomised
studies were identified in the literature search conducted for this systematic literature
review, and have been discussed in detail in the following sections.
The publication concluded that there are some significant concerns when short
fractionation schedules are used for breast radiotherapy. Particularly, the authors
concluded that a large dose per fraction could increase late normal tissue toxicity.
However, case series, cohort studies and recently published randomised trials support the
idea of hypofractionation for breast cancer, giving comparable control rates with
conventional fractionation and acceptable toxicity. The authors cautioned that at least 15-
20 years of follow-up was needed to assess the long-term sequelae and confirm the safety
of the hypofractionated regimens.

A systematic literature review of hypofractionated radiotherapy for the treatment of early breast cancer Page 13
3.2 Primary studies
The literature search identified five RCTs which met the inclusion criteria. The key
characteristics are shown in Table 12. Two trials were in patients who had undergone
breast conserving surgery (RMH/GOC and Canadian trials)1-2, 7-8
and three were in patients
who had undergone any form of surgery (START A, START B and Spooner trials)3-5
. All
studies were considered fair quality, with the exception of Spooner which was considered
poor*. Spooner 2008 is a conference abstract; no full publication of this abstract was
identified in this systematic review conducted for this technical report.3 The studies
evaluated a range of hypofractionated radiotherapy regimens.
The following section includes further discussion of each study design and patient
population.
* The conference abstract provided insufficient study detail to rate it as either fair or good. It is unclear from the abstract whether allocation was concealed from those responsible for recruiting subjects, whether outcome assessement was blinded, and whether there was loss to follow up,

14 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 17 Key characteristics of included studies
Study ID Study type
Quality Population, median follow-up
Country Intervention Comparator Outcomes
Post breast conserving surgery
RMH/GOC1, 8 RCT
Fair
T1-3, N0-1, M0, <75years N=1,410
9.7 years (range 7.8-11.8 years)
UK
39 Gy in 13 fractions over 5 weeks (N=474)
42.9 Gy in 13 fractions over 5 weeks (N=466)
50 Gy in 25 fractions over 5 weeks (N=470)
Local recurrence
Cosmetic outcomes
Canadian2, 7 RCT
Fair
Invasive carcinoma with negative axillary nodes,
N=1,234
12 years (range not reported)
Canada
42.5 Gy in 16 fractions over 22 days (N=622)
50 Gy in 25 fractions over 35 days (N=612)
Local recurrence (including subgroup analysis)
Overall survival
Adverse events and toxicity
Cosmetic outcome
Post breast conserving surgery or mastectomy
START A4, 6 RCT
Fair
T1-3a, N0-1, M0
N=2,236
5.1 years (range 4.4-6.0)
UK
39 Gy in 13 fractions over 5 weeks (N=737)
41.6 Gy in 13 fractions over 5 weeks (N=750)
50 Gy in 25 fractions over 5 weeks (N=749)
Local recurrence
Overall survival
Adverse events and toxicity
Cosmetic outcome (including subgroup analysis)
Quality of life (including subgroup analysis)
START B5, 6 RCT
Fair
T1-3a, N0-1, M0
N=2,215
6 years (range 5.0-6.2)
UK
40 Gy in 15 fractions over 3 weeks (N=1,110)
50 Gy in 25 fractions over 5 weeks (N=1,105)
Local recurrence
Overall survival
Adverse events and toxicity
Cosmetic outcome (including subgroup analysis)
Quality of life (including subgroup analysis)
Spooner3 RCT (conference abstract)
Poora
Stage 1 or 2, median tumour size 2cm N=707
16.9 years (range 15.4-18.8 years)
UK
40 Gy in 15 daily fractions (N=NR)
50 Gy in 25 daily fractions (N=NR)
Delayed salvage treatment
Time to first relapse
Abbreviations: NR=not reported, RCT=randomised controlled trial a The conference abstract provided insufficient study detail to rate it as either fair or good. It is unclear from the abstract whether allocation was concealed from those responsible for recruiting subjects, whether outcome assessment was blinded, and whether there was loss to follow up,

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 15
3.2.1 Royal Marsden Hospital/Gloucester Oncology Centre trial (RMH/GOC)1, 8
Patients with operable invasive breast cancer (T1–3, N0–1, M0) who needed radiotherapy were
eligible for the trial. Inclusion criteria were <75 years of age, completed breast conserving
surgery and complete macroscopic resection of invasive carcinoma. The study was conducted in
the UK.
Patients (N=1,410) were randomised to either i) 50 Gy in 25 fractions (control group), or ii) 39 Gy
in 13 fractions or iii) 42.9 Gy in 13 fractions (experimental schedules). All regimens were
administered over five weeks. Patients with a complete macroscopic resection who were judged
eligible by the clinician were further randomly allocated to receive a tumour bed boost or no
boost. This process ended in July 1997, and all patients were offered an elective boost
thereafter. The proportion of patients who received a boost was similar in all three treatment
groups: 348 (74%) patients for 50 Gy, 348 (75%) for 42.9 Gy, and 351 (74%) for 39 Gy.
The trial was powered to detect a difference in tumour recurrence between each study arm, with
the aim to enrol 2,250 subjects. However, recruitment was stopped prior to this number being
reached as this trial was superseded by the START trials. Recruitment occurred between 1986
and 1998. The median follow-up period was 9.7 years, with a maximum of 18.4 years of follow-
up. The publications did not report baseline characteristics in each study arm. Patient
characteristics are shown in Table 18.

16 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 18 RMH/GOC trial: Demographic and clinical characteristics of 1410 patients randomised8
Patient characteristic Number (%)
Age at randomisation
20-29 9 (0.9)
30-39 98 (7.0)
40-49 316 (22.4)
50-59 503 (35.7)
60-69 425 (30.1)
70-79 59 (4.2)
Breast size (from photographs)
Small 186 (13.2)
Medium 952 (67.5)
Large 203 (14.4)
Not known 69 (4.9)
Surgical deficit (from photographs)
Small 845 (59.9)
Medium 415 (29.4)
Large 76 (5.4)
Not known 74 (5.2)
cT stage
T0 59 (4.2)
T1 749 (53.1)
T2 575 (40.8)
T3 22 (1.6)
T4 2 (0.1)
TX 3 (0.2)
cN stage
N0 1,187 (84.7)
N1 219 (15.5)
N2 3 (0.2)
NX 1 (0.1)
Number of nodes pathologically involved
0 564 (67.3)
1-3 202 (24.1)
4+ 72 (8.6)
No axillary surgery 572 (40.6)
Adjuvant treatment
None 289 (20.5)
Tamoxifen only 918 (65.1)
Chemotherapy only 40 (2.8)
Tamoxifen and chemotherapy 156 (11.1)
Other 7 (0.5)
Axillary supraclavicular fossa treatment
None 337 (23.9)
Axillary supraclavicular fossa radiotherapy, no axillary surgery 231 (16.4)
Surgery, no radiotherapy 782 (55.5)
Surgery and supraclavicular fossa radiotherapy 59 (4.2)
Not known 1 (0.1)
Breast boost
Randomised to no boost 359 (25.5)
Randomised to boost 364 (25.8)
Non-randomised boost given 687 (48.7)
Source: Yarnold 20058, Table 1 page 12

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 17
3.2.2 Canadian trial2, 7
Patients with invasive carcinoma of the breast treated by breast conserving surgery and axillary
dissection with pathologically negative axillary lymph nodes were eligible for inclusion in the trial.
Key exclusion criteria were invasive disease or ductal carcinoma in situ involving the margins of
excision, tumours that were larger than 5 cm in diameter, and a breast width of more than 25 cm
at the posterior border of the medial and lateral tangential beams. The study was conducted in
Canada.
Patients (N=1,234) were randomised to either i) 50 Gy in 25 fractions over 35 days or ii) 42.5 Gy
in 16 fractions over 22 days. The 50 Gy arm was considered the control arm.
The study was designed to assess the non-inferiority of the hypofractionated regimen relative to
the standard schedule for radiation therapy in terms of local recurrence. Recruitment occurred
between 1993 and 1996. The study had a median follow-up of 12 years. The authors noted that
the patients in each treatment arm were reasonably comparable with respect to their baseline
characteristics. This is shown in Table 19.
Table 19 Canadian trial: Patient characteristics7
Characteristic Number (%)
42.5 Gy N=622
Number (%)
50 Gy N=612
Age
<50 y 157 (25) 148 (24)
50–59 y 186 (30) 155 (25)
60–69 y 181 (29) 200 (33)
≥70 y 98 (16) 109 (18)
Tumour size
≤1 cm 183 (29) 192 (31)
>1–2 cm 317 (51) 302 (49)
>2 cm 122 (20) 118 (19)
Tumour grade
I 215 (35) 209 (34)
II 244 (39) 236 (39)
III 117 (19) 116 (19)
Unknown 46 (7) 51 (8)
Oestrogen receptor status
Positive 440 (71) 434 (71)
Negative 165 (27) 157 (26)
Unknown 17 (3) 21 (3)
Systemic therapy
None 298 (48) 295 (48)
Tamoxifen 254 (41) 251 (41)
Chemotherapy 70 (11) 66 (11)
Source: Whelan 20027 Table 1 page 1146

18 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
3.2.3 Standardisation of Breast Radiotherapy Trial A (START A)4
The START A and START B trials were conducted in parallel.4-5
Centres in the UK could elect to
enter either Trial A (17 centres) or Trial B (23 centres). Due to earlier completion of recruitment in
Trial B, those centres were invited to join Trial A after accrual to Trial B was complete. The study
was conducted in the UK.
Women with operable invasive breast cancer (T1-3a, N0-1 M0) requiring radiotherapy after
surgery (breast-conserving surgery or mastectomy, with clear tumour margins ≥1 mm) were
eligible for the trial if they were aged over 18 years and did not have an immediate surgical
reconstruction.
Patients (N=2,236) were randomised to either i) 50 Gy in 25 fractions (control group) or ii) 41.6
Gy in 13 fractions or iii) 39 Gy in 13 fractions (experimental schedules). All regimens were
administered over five weeks to eliminate treatment time as a variable.
The trial was powered to detect a difference in local-regional tumour relapse between each 13
fraction schedule and the control group. Recruitment occurred between 1998 and 2002. The
median follow-up period was 5.1 years, with a maximum of 8 years of follow-up. Demographic
and clinical characteristics at randomisation were well balanced between treatment groups. This
is shown in Table 20.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 19
Table 20 START A: Patient characteristics4
Characteristic
Fractionation schedule
50 Gy n=749 (%)
41.6 Gy n=750 (%)
39 Gy n=737 (%)
Total N=2,236 (%)
Age years
20–29 5 (0.7) 4 (0.5) 3 (0.4) 12 (0.5)
30–39 38 (5.1) 40 (5.3) 38 (5.2) 116 (5.2)
40–49 116 (15.5) 136 (18.1) 129 (17.5) 381 (17.0)
50–59 280 (37.4) 283 (37.7) 286 (38.8) 849 (38.0)
60–69 215 (28.7) 192 (25.6) 194 (26.3) 601 (26.9)
70–79 87 (11.6) 85 (11.3) 78 (10.6) 250 (11.2)
80– 8 (1.1) 10 (1.3) 9 (1.2) 27 (1.2)
Mean (SD) 57.6 (10.5) 57.0 (10.7) 57.1 (10.5) 57.2 (10.6)
Time from surgery to randomisation (weeks)
Median time (IQR) 8.8 (5.3–20.8) 9.4 (5.9–20.2) 9.3 (5.4–21.1) 9.1 (5.4–20.7)
Range 0.4–71.3 1.0–50.3 1.1–53.6 0.4–71.3
Primary surgery
Breast conserving surgery 631 (84.2) 641 (85.5) 628 (85.2) 1900 (85.0)
Mastectomy 118 (15.8) 109 (14.5) 109 (14.8) 336 (15.0)
Histological type
Invasive ductal 581 (77.6) 585 (78.0) 584 (79.2) 1750 (78.3)
Invasive lobular 88 (11.7) 95 (12.7) 83 (11.3) 266 (11.9)
Mixed ductal/lobular 21 (2.8) 17 (2.3) 17 (2.3) 55 (2.5)
Other 57 (7.6) 51 (6.8) 52 (7.1) 160 (7.2)
Not known 2 (0.3) 2 (0.3) 1 (0.1) 5 (0.2)
Pathological node status
Positive 222 (29.6) 197 (26.3) 224 (30.4) 643 (28.8)
Negative 514 (68.6) 536 (71.5) 497 (67.4) 1547 (69.2)
Not known (no axillary surgery) 12 (1.6) 17 (2.3) 15 (2.0) 44 (2.0)
Not known (missing data) 1 (0.1) 0 (0.0) 1 (0.2) 2 (0.1)
Tumour size (cm)
<1 24 (3.2) 26 (3.5) 24 (3.3) 74 (3.3)
1– 362 (48.3) 347 (46.3) 355 (48.2) 1064 (47.6)
2– 202 (27.0) 203 (27.1) 198 (26.9) 603 (27.0)
3– 156 (20.8) 169 (22.5) 157 (21.3) 482 (21.6)
Not known 5 (0.7) 5 (0.7) 3 (0.3) 13 (0.6)
Tumour grade
1 157 (21.0) 150 (20.0) 149 (20.2) 456 (20.4)
2 369 (49.3) 379 (50.5) 368 (49.9) 1116 (49.9)
3 212 (28.3) 207 (27.6) 210 (28.5) 629 (28.1)
Not known (not applicable) a 11 (1.5) 10 (1.3) 6 (0.8) 27 (1.2)
Not known 0 (0.0) 4 (0.6) 4 (0.5) 8 (0.4)
Adjuvant therapy
None 52 (6.9) 53 (7.1) 67 (9.1) 172 (7.7)
Tamoxifen/no chemotherapy 416 (55.5) 418 (55.7) 376 (51.0) 1210 (54.1)
Chemotherapy/no tamoxifen 86 (11.5) 77 (10.3) 82 (11.1) 245 (11.0)
Tamoxifen + chemotherapy 173 (23.1) 187 (25.0) 188 (25.5) 548 (24.5)

20 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Characteristic
Fractionation schedule
50 Gy n=749 (%)
41.6 Gy n=750 (%)
39 Gy n=737 (%)
Total N=2,236 (%)
Other endocrine therapy b 17 (2.3) 13 (1.7) 17 (2.3) 47 (2.1)
Not known 5 ( 0.7) 2 ( 0.2) 7 ( 0.9) 14 ( 0.6)
Lymphatic treatment
None 8 (1.1) 14 (1.9) 13 (1.8) 35 (1.6)
Surgery/no radiotherapy 610 (81.4) 636 (84.8) 620 (84.1) 1866 (83.5)
Radiotherapy/no surgery 3 (0.4) 4 (0.5) 2 (0.3) 9 (0.4)
Surgery + radiotherapy 119 (15.9) 95 (12.7) 95 (12.9) 309 (13.8)
Not known 9 (1.2) 1 (0.1) 7 (0.9) 17 (0.8)
Boost (breast conserving surgery patients only)
Number n=631 n=641 n=628 n=1,900
Yes 381 (60.4) 391 (61.0) 380 (60.5) 1152 (60.6)
No 242 (38.3) 249 (38.8) 241 (38.4) 732 (38.5)
Not known 8 (1.3) 1 (0.2) 7 (1.1) 16 (0.8)
From Baseline photographs
Number n=413 n=421 n=416 n=1250
Breast size
Small 43 (10.4) 47 (11.2) 41 (9.9) 131 (10.5)
Medium 294 (71.2) 324 (77.0) 322 (77.4) 940 (75.2)
Large 76 (18.4) 50 (11.9) 53 (12.7) 179 (14.3)
Surgical deficit
Small 232 (56.2) 235 (55.8) 249 (59.9) 716 (57.3)
Medium 142 (34.4) 146 (34.7) 132 (31.7) 420 (33.6)
Large 39 (9.4) 40 (9.5) 35 (8.4) 114 (9.1)
Source: START A4 Table 1 page 332 Abbreviations: IQR=Interquartile range, SD=Standard deviation a Lobular and other histological types. b Other endocrine therapies include combinations of tamoxifen/anastrozole/letrozole/exemestane/goserelin, mostly within randomised trials.
3.2.4 Standardisation of Breast Radiotherapy Trial B (START B)5
As noted above, the START A and START B trials were conducted in parallel. Women with
operable invasive breast cancer (T1-3a, N0-1, M0) requiring radiotherapy after surgery (breast-
conserving surgery or mastectomy, with clear tumour margins ≥1 mm) were eligible for the trial if
they were aged over 18 years and did not have an immediate surgical reconstruction.
Patients (N=2,215) were randomised to either i) 50 Gy in 25 fractions over five weeks or ii) 40 Gy
in 15 fractions over three weeks. The 50 Gy arm was considered the control arm. The trial was
powered to detect a difference in local-regional tumour relapse between each study arm.
Recruitment occurred between 1998 and 2001. The median follow-up period was 6.0 years, with
a maximum of 8 years of follow-up. Demographic and clinical characteristics at randomisation
were well balanced between treatment groups. This is shown in Table 21.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 21
Table 21 START B: Patient characteristics5
Characteristic
Fractionation schedule
50 Gy n=1,105 (%)
40 Gy n=1,110 (%)
Total N=2,215 (%)
Age years
20–29 7 (0.6) 0 (0.0) 7 (0.3)
30–39 62 (5.6) 39 (3.5) 101 (4.6)
40–49 179 (16.2) 170 (15.3) 349 (15.8)
50–59 427 (38.6) 447 (40.3) 874 (39.5)
60–69 304 (27.5) 327 (29.5) 631 (28.5)
70–79 117 (10.6) 119 (10.7) 236 (10.7)
80– 9 (0.8) 8 (0.7) 17 (0.8)
Mean (SD) 57.0 (10.4) 57.8 (9.5) 57.4 (10.0)
Time from surgery to randomisation (weeks)
Median time (IQR) 7.3 (4.9–12.3) 7.1 (4.9–11.9) 7.3 (4.9–12.0)
Range 0.9–45.3 0.6–49.3 0.6–49.3
Primary surgery
Breast conserving surgery 1020 (92.3) 1018 (91.7) 2038 (92.0)
Mastectomy 85 (7.7) 92 (8.3) 177 (8.0)
Histological type
Invasive ductal 865 (78.3) 843 (75.9) 1708 (77.1)
Invasive lobular 122 (11.0) 132 (11.9) 254 (11.5)
Mixed ductal/lobular 20 (1.8) 25 (2.3) 45 (2.0)
Other 95 (8.6) 103 (9.3) 198 (8.9)
Not known 3 (0.3) 7 (0.6) 10 (0.5)
Pathological node status
Positive 238 (21.5) 266 (24.0) 504 (22.8)
Negative 831 (75.2) 804 (72.4) 1635 (73.8)
Not known (no axillary surgery) 36 (3.3) 39 (3.5) 75 (3.4)
Not known (missing data) 0 (0.0) 1 (0.1) 1 (0.04)
Tumour size (cm)
<1 151 (13.7) 167 (15.0) 318 (14.4)
1– 552 (50.0) 542 (48.8) 1094 (49.4)
2– 287 (26.0) 288 (25.9) 575 (26.0)
3– 113 (10.2) 107 (9.6) 220 (9.9)
Not known 2 (0.2) 6 (0.5) 8 (0.4)
Tumour grade
1 306 (27.7) 311 (28.0) 617 (27.9)
2 518 (46.9) 532 (47.9) 1050 (47.4)
3 261 (23.6) 248 (22.3) 509 (23.0)
Not known (not applicable) a 15 (1.4) 15 (1.3) 30 (1.3)
Not known 5 (0.4) 4 (0.4) 9 (0.4)
Adjuvant therapy
None 37 (3.3) 47 (4.2) 84 (3.8)
Tamoxifen/no chemotherapy 782 (70.8) 810 (73.0) 1592 (71.9)
Chemotherapy/no tamoxifen 77 (7.0) 78 (7.0) 155 (7.0)
Tamoxifen + chemotherapy 181 (16.4) 155 (14.0) 336 (15.2)

22 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Characteristic
Fractionation schedule
50 Gy n=1,105 (%)
40 Gy n=1,110 (%)
Total N=2,215 (%)
Other endocrine therapy b 16 (1.4) 11 (1.0) 27 (1.2)
Not known 12 (1.1) 9 (0.8) 21 (0.9)
Lymphatic treatment
None 32 (2.9) 36 ( 3.2) 68 (3.1)
Surgery/no radiotherapy 980 (88.7) 984 (88.6) 1964 (88.7)
Radiotherapy/no surgery 5 (0.4) 3 (0.3) 8 (0.4)
Surgery + radiotherapy 74 (6.7) 79 (7.1) 153 (6.9)
Not known 14 (1.3) 8 (0.7) 22 (1.0)
Boost (breast conserving surgery patients only)
Number n=1020 n=1018 n=2038
Yes 422 (41.4) 446 (43.8) 868 (42.6)
No 584 (57.3) 565 (55.5) 1149 (56.4)
Not known 14 (1.4) 7 (0.7) 21 (1.0)
From Baseline photographs
Number n=522 n=514 n=1036
Breast size
Small 49 (9.4) 42 (8.2) 91 (8.8)
Medium 377 (72.2) 390 (75.9) 767 (74.0)
Large 96 (18.4) 82 (16.0) 178 (17.2)
Surgical deficit
Small 307 (58.8) 286 (55.6) 593 (57.2)
Medium 164 (31.4) 177 (34.4) 341 (32.9)
Large 51 (9.8) 51 (9.9) 102 (9.8)
Source: START B5 Table 1 page 1100 Abbreviations: IQR=Interquartile range, SD=Standard deviation a Lobular and other histological types. b Other endocrine therapies include combinations of tamoxifen/anastrozole/letrozole/exemestane/goserelin, mostly within randomised trials.
3.2.5 Spooner3
This citation was a conference abstract, therefore limited information was available. Patients with
clinical stage 1 and 2 disease (N=707) were randomised to receive immediate postoperative
radiotherapy or delayed salvage treatment (no radiotherapy). The study was conducted in the
UK.
Patients receiving radiotherapy (N=NR) were further randomised to short (40 Gy in 15 daily
fractions) or long (50 Gy in 25 daily fractions). The 50 Gy arm was considered the control arm.
Recruitment occurred between 1985 and 1992. Patients were followed for a mean of 16.9 years.
No information about patient characteristics was available.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 23
4 Results of included trials
The results of the identified systematic reviews are not shown here as all trials that were
identified in their literature searches have been described in detail below.
4.1 Local recurrence
All five included trials reported local recurrence. Two trials described patients who had
undergone breast conserving surgery (RMH/GOC and Canadian)1-2
and three trials did not
include type of surgery as an inclusion criteria (Spooner, START A and START B).3-5
4.1.1 Post breast conserving surgery
RMH/GOC trial1
This trial compared i) 39 Gy in 13 fractions and ii) 42.9 Gy in 13 fractions with iii) 50 Gy in 25
fractions (the control arm). All fractions were administered over a five week period.
The results are shown in Table 22. Compared with the 50 Gy arm, the hazard ratio for the 42.9
Gy arm was 0.86 (95% CI 0.57, 1.30), and for the 39 Gy arm was 1.33 (95% CI 0.92, 1.92). The
Kaplan-Meier estimates of local recurrence at 10 years were 12.1% (95% CI 8.8, 15.5) for the 50
Gy arm, 9.6% (95% CI 6.7, 12.6) for the 42.9 Gy arm and 14.8% (95% CI 11.2, 18.3) for the 39
Gy arm. There was a significant difference in the probability of local recurrence after 10 years
between the 42.9 Gy and 39 Gy arms of the study (3・7%, 95% CI 0・3–8・3; χ2 test, degrees
of freedom [df]=1,p=0.027), with a higher rate of recurrence in the 39 Gy arm.
Table 22 RMH/GOC trial: Survival analysis of local relapse according to fractionation schedule1
Arm Number of local
recurrence / person-years
Crude hazard ratio
(95% CI) a
Kaplan-Meier estimates of local recurrence
(95% CI)
Smoothed estimate of absolute difference (95% CI) a
5 years follow-up
10 years follow-up
5 years follow-up
10 years follow-up
50 Gy 50/3965 1 7.9% (5.4, 10.4)
12.1% (8.8, 15.5)
NR NR
42.9 Gy 42/3840 0.86 (0.57, 1.30)
7.1% (4.6, 9.5)
9.6% (6.7, 12.6)
-1.1% (-3.3, 2.3)
-1.6% (-5.0, 3.3)
39 Gy 66/3890 1.33 (0.92, 1.92)
9.1% (6.4, 11.7)
14.8% (11.2, 18.3)
2.5% (-0.6, 6.7)
3.7% (-0.9, 9.8)
Source: Owen 20061, Table page 469 Abbreviations: CI=confidence interval a Compared with 50 Gy
Figure 1 shows the recurrence-free Kaplan-Meier curves. The curves for each fractionation
schedule begin to diverge after 5 years of follow-up. Hazard ratios were calculated by comparing
the 42.9Gy arm and the 39 Gy arm with the 50 Gy arm. The hazard ratios for the first five years

24 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
of follow-up were 0.90 (95% CI 0.55, 1.46) for 42.9 Gy arm and 1.14 (95% CI 0.72, 1.79) for the
39 Gy arm. The hazard ratios for the period from 5 years until the end of follow-up were 0.77
(95% CI 0.36, 1.69) for the 42.9 Gy arm and 1.81 (95% CI 0.96, 3.41) for 39 Gy arm. This
difference was not significant (p=0.1).
Figure 1 RMH/GOC trial: Local ipsilateral relapse in the breast according to fractionation scheudule1
Source: Owen 20061, Figure 2 page 470
Canadian trial2
This trial compared i) 42.5 Gy in 16 fractions over 22 days with ii) 50 Gy in 25 fractions over 35
days (the control arm). The cumulative incidence of local invasive recurrence was similar in the
two groups (as shown in Figure 2). At 10 years, the cumulative incidence of local invasive
recurrence was 6.2% in the 42.5 Gy arm compared with 6.7% in the 50 Gy arm (absolute
difference,0.5 percentage points; 95% CI, −2.5, 3.5). The pre-defined criteria for non-inferiority
was met (with a p value for non-inferiority of <0.001), indicating that the 42.5 Gy arm was not
inferior to the 50 Gy arm.
Non-invasive recurrences occurred in six patients in the 42.5 Gy arm and seven patients in the
50 Gy arm. The 10 year cumulative incidence of invasive or non-invasive local recurrence was
7.4% in the 42.5 Gy arm as compared with 7.5% in the 50 Gy arm (absolute difference, 0.1
percentage points; 95% CI, −3.1, 3.3). A hazard ratio for the entire population was not reported.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 25
Figure 2 Canadian trial: Kaplan-Meier estimates for local recurrencea2
Source: Whelan 20102 Figure 1a page 516 a p<0.001 for non-inferiority Standard regimen = 50 Gy arm Hypofractionated regimen = 42.5 Gy arm
A subgroup analysis of local recurrence rate showed that the treatment effect of the
hypofractionated protocol was similar regardless of patient age, tumour size, oestrogen-receptor
status, or use of systemic therapy (shown in Figure 3). The hypofractionated regimen appeared
to be less effective at preventing local recurrence in patients with high-grade tumours (p=0.01).
For these patients, the 10 year cumulative incidence of local recurrence was 4.7% in the control
group as compared with 15.6% in the hypofractionated-radiation group (absolute difference, -
10.9; 95% CI: -19.1, -2.8). In the high grade (grade 3) patient group, the hazard ratio was 3.08
(95% CI 1.22, 7.76), compared with 0.70 (95% CI 0.31, 1.58) in the low grade patient group.

26 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Figure 3 Canadian trial: Hazard ratios for Ipsilateral recurrence of breast cancer in subgroups of patients2
Source: Whelan 20102 Figure 2 page 517
4.1.2 Any surgery
Spooner3
This study compared i) 40 Gy in 15 fractions once a day or ii) 50 Gy in 25 fractions once a day
with iii) delayed salvage treatment. The abstract stated that there was no difference in relapse
frequency, or site between the two radiotherapy study arms, however no data was reported in the
abstract.
START A4
This trial compared i) 39 Gy in 13 fractions over five weeks or ii) 41.6 Gy in 13 fractions over five
weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The relapse rates are
shown in
Table 23. The crude hazard ratios for local relapse, relative to the 50 Gy arm, were 1.09 (95% CI
0.64, 1.88) for the 41.6 Gy arm and 1.25 (95% CI 0.74, 2.12) for the 39 Gy arm. These
differences were not statistically significant.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 27
Table 23 START A: Survival analyses of relapse and mortality according to fractionation schedule (Local relapse)4
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
50 Gy 25/749 (3.3) 3.2 (1.9, 4.6) 1 -
41.6 Gy 28/750 (3.7) 3.2 (1.9, 4.5) 1.09 (0.64, 1.88) 0.74
39 Gy 31/737 (4.2) 4.6 (3.0, 6.2) 1.25 (0.74, 2.12) 0.40
Source: Bentzen 20084 Table 2 page 335 Abbreviations: CI=confidence interval
START B5
This trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions over
five weeks (the control arm). The relapse rates are shown in Table 24. The crude hazard ratio for
local relapse, relative to the 50 Gy arm, was 0.72 (95% CI 0.43, 1.21) for the 40 Gy arm. This
was not statistically significant.
Table 24 START B: Survival analyses of relapse and mortality according to fractionation schedule (local relapse)5
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
50 Gy 34/1105 (3.1) 3.3 (2.2, 4.4) 1 -
40 Gy 25/1110 (2.2) 2.0 (1.1, 2.8) 0.72 (0.43, 1.21) 0.21
Source: Bentzen 20085 Table 2 page 1102 Abbreviations: CI=confidence interval
4.1.3 Conclusions: Local recurrence
The results are summarised in Table 25. There was no evidence that any hypofractionated
radiotherapy regimen was associated with a statistically significant difference in local recurrence
rate when compared with a control arm. The RMH/GOC trial noted a statistically significant
difference in recurrence rates when the two hypofractionated radiotherapy regimens were
compared (42.9 Gy vs 39 Gy: 9.6% vs 14.8%, p=0.027), but not when each regimen was
compared to the control arm.1
Subgroup analyses were performed in one publication.2 The Canadian trial analysed local
recurrence by patient age, tumour size, oestrogen-receptor status, tumour grade or use of
systemic therapy. There were no significant differences in any subgroup, with the exception of
tumour grade. The 42.5 Gy regimen was least effective in patients with high-grade tumours
compared to patients with low grade tumours (p=0.01).2
These results must be considered in the context of the range of hypofractionated radiotherapy
regimes evaluated and different study designs used in these publications. Any imbalance
between study arms in the treatments received may influence long term outcomes such as local
recurrence.

28 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 25 Summary of key results for local recurrence
Study ID Study arms Results
Post breast conserving surgery
RMH/GOC1 39 Gy in 13 fractions over 5 weeks
42.9 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local recurrence
39 Gy vs 50 Gy: 9.1% vs 7.9%, p=NR
42.9 Gy vs 50 Gy: 7.1% vs 7.9%, p=NR
42.9 Gy vs 39 Gy: 7.1% vs 9.1%, p=NR
10 year local recurrence
39 Gy vs 50 Gy: 14.8% vs 12.1%, p=NS
42.9 Gy vs 50 Gy: 9.6% vs 12.1%, p=NS
42.9 Gy vs 39 Gy: 9.6% vs 14.8%, p=0.027
39 Gy: HR 1.33 (95% CI 0.92, 1.92), p=NS
42.9 Gy: HR 0.86 (95% CI 0.57, 1.30), p=NS
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
10 year cumulative incidence of local recurrence
42.5 Gy vs 50 Gy: 6.2% vs. 6.7%, p=NS
10 year cumulative incidence of invasive or non-invasive local recurrence 42.5 Gy vs 50 Gy: 7.4% vs. 7.5%, p=NS
Subgroup analyses
Patient age, tumour size, oestrogen-receptor status, tumour grade, systemic therapy, p=NS
High-grade vs low grade tumours, p=0.01
Any surgery
Spooner3
40 Gy in 15 fractions once a day
50 Gy in 25 fractions once a day
Delayed salvage treatment
17 year relapse frequency
No difference, data not reported
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local relapse rate
50 Gy vs 41.6 Gy vs 39 Gy: 3.2% vs 3.2% vs 4.6%, p=NR
5 year local relapse
39 Gy: HR 1.25 (95% CI 0.74, 2.12), p=0.40
41.6 Gy: HR 1.09 (95% CI 0.64, 1.88), p=0.74
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local relapse rate
50 Gy vs 40 Gy: 3.3% vs 2.0%, p=NR
5 year local relapse
40 Gy: HR 0.72 (95% CI 0.43, 1.21), p=0.21
Abbreviations: CI=confidence interval, HR=hazard ratio, , NR= not reported, NS=not significant * control arm
4.2 Local-regional recurrence
Two trials reported local-regional recurrence, both in studies that did not include surgery type as
an inclusion criteria (START A and START B).4-5

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 29
4.2.1 Any surgery
START A4
This trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13 fractions over
five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The relapse rates are
shown in Table 26. The hazard ratios for local-regional tumour relapse were 1.05 (95% CI 0.63,
1.75) for the 41.6 Gy arm and 1.26 (95% CI 0.77, 2.08) for the 39 Gy arm. These differences
were not statistically significant.
Table 26 START A: Survival analyses of relapse and mortality according to fractionation schedule (Local-regional relapse)4
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
Local-regional relapse
50 Gy 28/749 (3.7) 3.6 (2.2, 5.1) 1 –
41.6 Gy 30/750 (4.0)) 3.5 (2.1, 4.3) 1.05 (0.63, 1.75) 0.86
39 Gy 35/737 (4.7) 5.2 (3.5, 6.9) 1.26 (0.77, 2.08) 0.35
Source: Bentzen et al 20084 Table 2 page 335 Abbreviations: CI=confidence interval
START B5
This trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions over
five weeks (the control arm). The relapse rates are shown in Table 27. The hazard ratios for
local-regional tumour relapse was 0.79 (95% CI 0.48, 1.29) for the 40 Gy arm, which was not
statistically significant.
Table 27 START B: Survival analyses of relapse and mortality according to fractionation schedule (Local-regional Relapse)5
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
Local-regional relapse
50 Gy 36/1105 (3.2) 3.3 (2.2, 4.5) 1 –
40 Gy 29/1110 (2.6) 2.2 (1.3, 3.1) 0.79 (0.48, 1.29) 0.35
Source: Bentzen et al 20085 Table 2 page 1102 Abbreviations: CI=confidence interval
4.2.2 Conclusions: Local-regional recurrence
The results are summarised in Table 28. There was no evidence that any hypofractionated
radiotherapy regimen was associated with a statistically significant difference in regional
recurrence rate when compared with a control arm.
These results must be considered in the context of the range of hypofractionated radiotherapy
regimes evaluated and different study designs used in these publications. Any imbalance

30 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
between study arms in the treatments received may influence long term outcomes such as local-
regional recurrence.
Table 28 Summary of key results for local-regional recurrence4-5
Study ID Study arms Results
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local-regional relapse rate
50 Gy vs 41.6 Gy vs 39 Gy: 3.6% vs 3.5%vs 5.2%, p=NR
5 year local-regional relapse
39 Gy: HR 1.26 (95% CI 0.77, 2.08), p=0.35
41.6 Gy: HR 1.05 (95% CI 0.63, 1.75), p=0.86
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local-regional relapse rate
50 Gy vs 40 Gy: 3.3% vs 2.2%, p=NR
5 year local-regional relapse
40 Gy: HR 0.79 (95% CI 0.48, 1.29), p=0.35
Abbreviations: CI=confidence interval, HR=hazard ratio, NR=not reported * control arm
4.3 Distant relapse
Two trials reported distant relapse, both in studies that did not include surgery type as an
inclusion criteria (START A and START B).4-5
4.3.1 Any surgery
START A4
This trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13 fractions over
five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The distant relapse
rates are shown in Table 29. The hazard ratios for distant relapse, compared to the 50 Gy arm,
were 0.92 (95% CI 0.66, 1.28) for the 41.6 Gy arm and 1.29 (95% CI 0.95, 1.76) for the 39 Gy
arm. These ratios were not statistically significant.
Table 29 START A: Survival analyses of relapse and mortality according to fractionation schedule (Distant relapse) 4
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
Distant relapse
50 Gy 73/749 (9.7) 9.8 (7.5, 12.0) 1 –
41.6 Gy 69/750 (9.2) 9.5 (7.3, 11.7) 0.92 (0.66, 1.28) 0.64
39 Gy 93/737 (12.6) 11.9 (9.5, 14.4) 1.29 (0.95, 1.76) 0.10
Source: Bentzen et al 20084 Table 2 page 335 Abbreviations: CI=confidence interval

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 31
START B5
This trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions over
five weeks (the control arm). The distant relapse rates are shown in Table 30. The hazard ratios
for distant relapse was 0.69 (95% CI 0.53, 0.91) for the 40 Gy arm. This result was statistically
significant (p=0.01).
Table 30 START B: Survival analyses of relapse and mortality according to fractionation schedule (Distant relapse)5
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
Distant relapse
50 Gy 122/1105 (11.0) 10.2 (8.4, 12.1) 1 –
40 Gy 87/1110 (7.8) 7.6 (6.0, 9.2) 0.69 (0.53, 0.91) 0.01
Source: Bentzen et al 20085 Table 2 page 1102 Abbreviations: CI=confidence interval
4.3.2 Conclusions: Distant relapse
The results are summarised in Table 31. START A reported no statistical difference between
either of the hypofractionated regimens compared with control. START B reported that the 40 Gy
study arm had a significantly lower rate of distant relapse when compared with the control arm
(HR 0.69 95% CI 0.53, 0.91, p=0.01).
These results must be considered in the context of the range of hypofractionated radiotherapy
regimes evaluated and different study designs used in these publications. Any imbalance
between study arms in the treatments received may influence long term outcomes such as local
recurrence.
Table 31 Summary of key results for distant relapse4-5
Study ID Study arms Results
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year distant relapse rate
50 Gy vs 41.6 Gy vs 39 Gy: 9.8% vs 9.5% vs 11.9%, p=NR
5 year local-regional relapse
39 Gy: HR 1.29 (95% CI 0.95, 1.76), p=0.10
41.6 Gy: HR 0.92 (95% CI 0.66, 1.28), p=0.64
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year local-regional relapse rate
50 Gy vs 40 Gy: 10.2% vs 7.6%, p=NR
5 year local-regional relapse
40 Gy: HR 0.69 (95% CI 0.53, 0.91), p=0.01
Abbreviations: CI=confidence interval, HR=hazard ratio, NR=not reported * control arm

32 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
4.4 Overall survival
A total of four trials reported overall survival (Canadian, Spooner, START A and START B). 2, 4-5,
7 The Canadian trial
2 described patients who had undergone breast conserving surgery and
three publications did not include surgery type as an inclusion criteria (Spooner, START A and
START B).3-5
4.4.1 Post breast conserving surgery
Canadian trial2
This trial compared i) 42.5 Gy in 16 fractions over 22 days with ii) 50 Gy in 25 fractions over 35
days (the control arm). During the study there were 126 deaths in the 50 Gy arm (20.6%) and
122 deaths in the in the 42.5 Gy arm (19.6%). At 10 years, the probability of survival was 84.4%
in the 50 Gy arm compared with 84.6% in the 42.5 Gy arm (shown in Figure 4). The absolute
difference was -0.2 percentage points (95% CI -4.3, 4.0). This difference was not statistically
significant (p=0.79).
Figure 4 Canadian trial: Kaplan-Meier estimate for overall survival2
Source: Whelan 20102 Figure 1b page 516 p=0.79
The cause of death is shown in Table 32. In the 50 Gy arm 13.4% of deaths were related to
cancer, 1.5% were related to cardiac disease and 5.7% were due to other causes. In the 42.5 Gy
arm 13.2% were related to cancer, 1.9% were related to cardiac disease and 4.5% were due to
other causes. None of these differences were statistically significant.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 33
Table 32 Canadian trial: Cause of deaths2
Arm 50 Gy n (%)
42.5 Gy n (%)
P value
Deaths related to cancer 82 (13.4) 82 (13.2) NS
Deaths related to cardiac disease 9 (1.5) 12 (1.9) NS
Deaths related to other causes 35 (5.7) 28 (4.5) NS
Source: Whelan 20102 page 517 Abbreviations: NS=not significant
4.4.2 Any surgery
Spooner3
This study compared i) 40 Gy in 15 fractions once a day or ii) 50 Gy in 25 fractions once a day
with delayed salavage treatment. The abstract noted that there was no difference in overall
survival between the two study arms, however no data was reported in the abstract.
START A4
This trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13 fractions over
five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The START A trial
reported all-cause mortality, rather than survival. As shown in Table 33, the hazard ratios for all-
cause mortality, compared with the 50 Gy arm, were 1.04 (95% CI 0.77, 1.40) for the 41.6 Gy
arm and 1.00 (95% CI 0.74, 1.36) for the 39 Gy arm. These ratios were not statistically
significant.
Table 33 START A: Survival analyses of relapse and mortality according to fractionation schedule (All-cause mortality)4
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
50 Gy 84/749 (11.2) 11.1 (8.7, 13.4) 1 –
41.6 Gy 89/750 (11.9) 11.3 (8.9, 13.7) 1.04 (0.77, 1.40) 0.81
39 Gy 83/737 (11.3) 10.7 (8.3, 13.1) 1.00 (0.74, 1.36) 0.99
Source: Bentzen et al 20084 Table 2 page 335 Abbreviations: CI=confidence interval
START B5
This trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions over
five weeks (the control arm). The START B trial reported all-cause mortality, rather than survival.
As shown in Table 34, the hazard ratio for all-cause mortality for the 40 Gy arm was 0.76 (95%
CI 0.59, 0.98) compared with the 50 Gy arm. This was statistically significant (p=0.03).

34 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 34 START B: Survival analyses of relapse and mortality according to fractionation schedule (All-cause mortality)5
Arm Events/total (%) Estimated % with event by 5 years
(95% CI) Crude hazard ratio (95%
CI) P value
50 Gy 138/1105 (12.5) 11.0 (9.1, 12.9) 1 –
40 Gy 107/1110 (9.6) 8.0 (6.4, 9.7) 0.76 (0.59, 0.98) 0.03
Source: Bentzen et al 20085 Table 2 page 1102 Abbreviations: CI=confidence interval
4.4.3 Conclusions
The results are summarised in Table 35. Most studies reported that there was no evidence that
hypofractionated radiotherapy was associated with a statistically significantly difference in overall
survival. START B found that 40 Gy in 15 fractions over three weeks was associated with a
statistically significantly lower all-cause mortality rate when compared with 50 Gy in 25 fractions
over five weeks (HR 0.76 95% CI 0.59, 0.98, p=0.03). Therefore, there was no evidence that any
hypofractionated radiotherapy regimen was associated with a worse overall survival rate (i.e. the
only study that reported a significant difference showed lower mortality for patients treated with
hypofractionated radiotherapy).
These results must be considered in the context of the range of hypofractionated radiotherapy
regimes evaluated and different study designs used in these publications. None of the
publications described the treatments that patients in each study arm received after radiotherapy
(e.g. chemotherapy). Any imbalance between study arms in the treatments received may
influence long term outcomes such as overall survival.
Table 35 Summary of key results for overall survival
Study ID Study arms Results
Post breast conserving surgery
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
10 year survival
42.5 Gy vs 50 Gy: 84.6% vs 84.4%, p=0.79
Any surgery
Spooner3 40 Gy in 15 fractions once a day
50 Gy in 25 fractions once a day
17 year survival
No difference, data not reported
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
5 year all cause mortality
39 Gy: HR 1.00 (95% CI 0.74, 1.36), p=0.99
41.6 Gy: HR 1.04 (95% CI 0.77, 1.40), p=0.81
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
5 year all cause mortality
40 Gy: HR 0.76 (95% CI 0.59, 0.98), p=0.03
Abbreviations: CI=confidence interval, HR=hazard ratio * control arm

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 35
4.5 Adverse events and toxicity
A total of three trials reported adverse events and toxicity outcomes (Canadian, START A and
START B).2, 4-5, 7
The Canadian trial2, 7
described patients who had undergone breast conserving
surgery and two trials did not include surgery type as an inclusion criteria (START A4 and START
B5, as well as combined data from both studies
6).
4.5.1 Post breast conserving surgery
Canadian trial2
This trial compared i) 42.5 Gy in 16 fractions over 22 days with ii) 50 Gy in 25 fractions over 35
days (the control arm). The late toxic effects of radiation are shown in Table 36. The results were
generally consistent between study arms. No grade 4 skin ulceration or soft-tissue necrosis was
observed in any subjects.
Table 36 Canadian trial: Late toxic effects of radiation, assessed according to the RTOG-EORTC late radiation morbidity scoring schemea2
Site and Grade
5 year follow-up 10 year follow-up
50 Gy n=424 %
42.5 Gy n=449 %
50 Gy n=220 %
42.5 Gy n=235 %
Skin
0b 82.3 86.1 70.5 66.8
1 14.4 10.7 21.8 24.3
2 2.6 2.5 5.0 6.4
3 0.7 0.7 2.7 2.5
Subcutaneous tissue
0c 61.4 66.8 45.3 48.1
1 32.5 29.5 44.3 40.0
2 5.2 3.8 6.8 9.4
3 0.9 0.9 3.6 2.5
Source: Whelan 20102 Table 1 page 518 Abbreviations: CI=confidence interval, RTOG-EORTC=Radiation Therapy Oncology Group and the European Organization for Research and Treatment of Cancer. a Effects of radiation therapy on skin and subcutaneous tissue were graded on a scale of 0 to 4 (with 0 indicating no toxic effects and grade 4 indicating skin ulceration or soft-tissue necrosis). RTOG–EORTC denotes the Radiation Therapy Oncology Group and the European Organization for Research and Treatment of Cancer. b The absolute difference at 5 years was -3.8 percentage points (95% CI: -8.7, 1.0), and at 10 years the absolute difference was 3.7 percentage points (95% CI: -4.9, 12.1). c The absolute difference at 5 years was -5.4 percentage points (95% CI: -11.9, 0.9), and at 10 years the absolute difference was -2.8 percentage points (95% CI: -11.7, 6.5).
4.5.2 Any surgery
START A4
This trial compared i) 39 Gy in 13 fractions over five weeks or ii) 41.6 Gy in 13 fractions over five
weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The incidence of ischemic

36 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
heart disease, symptomatic rib fracture and symptomatic lung fibrosis was low, with no
differences between the study arms (shown in Table 37).
Table 37 START A: Incidence of ischemic heart disease, symptomatic rib fracture, and symptomatic lung fibrosis according to fractionation schedule4
Outcome Arm Reported
n, (%) Confirmed
n, (%) a
Ischemic heart disease b
50 Gy 12 (1.6) 3 (0.4) [1]c
41.6 Gy 7 (0.9) 2 (0.3) [0]c
39 Gy 8 (1.1) 5 (0.7) [4]c
Total 27(1.2) 10 (0.4) [5]c
Symptomatic rib fractures d
50 Gy 8 (1.1) 1 (0.1)
41.6 Gy 9 (1.2) 2 (0.3)
39 Gy 10 (1.4) 1 (0.1)
Total 27 (1.2) 4 (0.2)
Symptomatic lung fibrosis
50 Gy 5 (0.7) 0 (0)
41.6 Gy 6 (0.8) 2 (0.3)
39 Gy 7 (0.9) 1 (0.1)
Total 18 (0.8) 3 (0.1)
Source: Bentzen et al 20084 Table 3 page 337 a Cases confirmed after imaging and further investigations. b 18 patients had pre-existing heart disease at randomisation and were excluded. c Confirmed cases of ischemic heart disease in patients with left-sided primary tumours. d Reported cases include three with rib fracture after bone metastases and nine after trauma.
Other adverse events were discussed in the publication. In the 41.6 Gy arm, there was one case
of pneumonitis which occurred nine months after treatment and one patient who developed mild
symptoms and signs of brachial plexopathy two years after treatment. Two patients in the 50 Gy
arm experienced an unusually marked acute skin reaction during their radiotherapy treatment,
culminating in extensive moist desquamation. Neither patient had received adjuvant
chemotherapy.4 It was assumed that no cases were reported in the other study arms, although
this was not explicitly stated in the publication.
As shown in Table 38, a small number of patients had contralateral breast cancer (26 patients
(1.2%)) or a secondary primary cancer (44 patients (2%))..4
Table 38 START A: Contralateral and other secondary cancers4
Outcome Arm n, (%)
Contralateral breast cancer
50 Gy 13 (1.7)
41.6 Gy 5 (0.7)
39 Gy 8 (1.1)
Other secondary primary cancers
50 Gy 15 (0.7)
41.6 Gy 10 (0.4)
39 Gy 19 (0.8)
Source: Bentzen et al 20084 page 338

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 37
Patient self-assessments of late normal tissue effects are discussed in the combined START A
and B publication results.6
START B5
This study compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions over
five weeks (the control arm). The incidence of ischemic heart disease, symptomatic rib fracture
and symptomatic lung fibrosis was low, with no differences between the study arms (shown in
Table 39).
Table 39 START B: Incidence of ischemic heart disease, symptomatic rib fracture, and symptomatic lung fibrosis according to fractionation schedule5
Outcome Arm Reported (%) Confirmed (%) a
Ischemic heart disease b
50 Gy 19 (1.7) 12 (1.1) [4]c
40 Gy 15 (1.3) 7 (0.6) [3]c
Total 34 (1.5) 19 (0.9) [7] c
Symptomatic rib fractures d
50 Gy 17 (1.5) 2 (0.2)
40 Gy 16 (1.4) 2 (0.2)
Total 33 (1.5) 4 (0.2)
Symptomatic lung fibrosis
50 Gy 15 (1.4) 1 (0.1)
40 Gy 16 (1.4) 3 (0.3)
Total 31 (1.4) 4 (0.2)
Source: Bentzen et al 20085 Table 3 page 1104 a Cases confirmed after imaging and further investigations. b 11 patients had pre-existing heart disease at randomisation and were excluded. c Confirmed cases of ischemic heart disease in patients with left-sided primary tumours. d Reported cases include four with rib fracture after bone metastases and three after trauma.
Other adverse events were discussed in the publication. There were no cases of brachial
plexopathy in either study arm. Thirteen patients in the 50 Gy arm (1.2%) and three patients in
the 40 Gy arm (0.3%) reported a marked acute reaction during radiotherapy.5
As shown in Table 40, a small number of patients had contralateral breast cancer (36 patients
(1.6%)) or a secondary primary cancer (58 patients (2.6%)).5
Table 40 START B: Contralateral and other secondary cancers5
Outcome Arm n, (%)
Contralateral breast cancer 50 Gy 19 (1.7)
40 Gy 17 (1.5)
Other secondary primary cancers 50 Gy 32 (2.9)
40 Gy 26 (2.3)
Source: Bentzen et al 20085 page 1103
Patient self-assessments of late normal tissue effects are discussed in the combined START A
and B publication results.6

38 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm). Combined patient-reported quality-of-life results from Start A
and B are reported in Hopwood et al 2010.6
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were
accrued into the quality-of-life study (1,129 from START A and 1,079 from START B).6
Figure 5 shows the forest plot for patient reported normal tissue effects in the START A and
START B trials. Two sets of outcomes were reported: breast symptoms and arm or shoulder
symptoms. Many of the breast symptoms can also be considered adverse events as well as
cosmetic outcomes, and have therefore been discussed here as well as in the following section
on cosmetic outcomes. Breast symptom outcomes are discussed first, followed by arm or
shoulder symptoms.
Breast Symptoms
In the START A trial, there were no statistically significant differences between the 41.6 Gy and
50 Gy arms. Change in breast appearance, breast hardness, breast shrinkage, pain in area of
affected breast and oversensitivity in area of affected breast favoured the 50 Gy arm, while
change in skin appearance and swelling in area of affected breast favoured the 41.6 Gy arm.
Skin problems on or in area of affected breast had a hazard ratio of 1.01.6
When the 39 Gy and 50 Gy arms in the START A trial were compared, all outcomes favoured the
39 Gy arm (with the exception of breast shrinkage which had a hazard ratio of 1.00). The only
outcome which statistically significantly favoured the 39 Gy arm was change in skin appearance
(hazard ratio 0.63 95% CI 0.47, 0.84, p=0.0019).6
In the START B trial, all outcomes favoured the 40 Gy arm, with the exception of oversensitivity
in area of affected breast. The only outcome which statistically significantly favoured the 40 Gy
arm was change in skin appearance (hazard ratio 0.76 95% CI 0.60, 0.97, p=0.0262).6
Arm or shoulder symptoms
In the START A trial, shoulder stiffness, difficult in raising or moving arm sideways and swelling
in arm or hand favoured the 41.6 Gy arm compared to the 50 Gy arm, although this was not
statistically significant. Pain in arm or shoulder had a hazard ratio of 1.00. When the 39 Gy and
50 Gy arms were compared, shoulder stiffness and swelling in arm or hand favoured the 39 Gy
arm, while pain in arm or shoulder favoured the 50 Gy arm, but these differences were not
statically significant..6
In the START B trial there were no differences in arm or shoulder symptoms. The hazard ratios
ranged from 0.95 to 1.05.6

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 39
Figure 5 START A AND B: Forest plots of normal tissue effects assessed as moderate or marked by
patients, according to radiotherapy regimens6
Source: Hopwood et al 20106 Figure 2 page 6 Positions of squares in the forest plot show the estimate of the hazard ratio describing relative effect of the test schedule compared with control, with the 95% CI represented by horizontal lines. Squares to the left of the vertical line indicate when rates of adverse effects are lower in the test schedule compared with control; estimates to the right of the line indicate whether rates are higher in the test schedule. Size of squares is proportional to the precision of the estimate, with larger squares indicating greater precision. *In patients who had completed breast-conserving surgery only.

40 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
4.5.3 Conclusions
The results are summarised in Table 41. Most trials reported that there was no difference in
adverse events and toxicity. Combined results from the START A and START B trials found that
a change in skin appearance occurred significantly less often in the 39 Gy and 40 Gy arms when
compared with the control arm (39 Gy HR 0.63 95% CI 0.47, 0.84, p=0.0019 and 40 Gy HR 0.76
95% CI 0.60, 0.97, p=0.0262).6
These results should be considered in the context of the difference in adverse event and toxicity
outcomes assessed in each publication, and the difference in hypofractionated radiotherapy
regimens evaluated.
Table 41 Summary of key results for adverse events and toxicity
Study ID Study arms Results
Post breast conserving surgery
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
Late toxic radiation effects: NS
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
Ischemic heart disease, symptomatic rib fracture, symptomatic lung fibrosis, contralateral breast cancer, other secondary primary cancers: NS
START B5 40 Gy in 15 fractions over 3 weeks
50 Gy in 25 fractions over 5 weeks*
Ischemic heart disease, symptomatic rib fracture, symptomatic lung fibrosis, contralateral breast cancer, other secondary primary cancers: NS
Combined QoL data from START A and B6^
As for START A and START B Tissue effects, arm and shoulder symptoms: NS
Skin appearance: 39 Gy HR 0.63 95% CI 0.47, 0.84, p=0.0019
40 Gy HR 0.76 (95% CI 0.60, 0.97), p=0.0262
Abbreviations: CI=confidence interval, HR=hazard ratio, NS=not significant, QoL=Quality-of-life * control arm ^ Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were accrued into the quality-of-life study (1,129 from START A and 1,079 from START B)

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 41
4.6 Cosmetic outcome
A total of four trials reported cosmetic outcomes. Four of the trials described patients who had
undergone breast conserving surgery (RMH/GOC, START A, START B and Canadian trials). 2, 8
6 Two trials described patients who had undergone mastectomy (START A and START B).
6. The
same two trials reported results for surgery types combined.4-5
4.6.1 Post breast conserving surgery
RMH/GOC trial8
This study compared i) 39 Gy in 13 fractions and ii) 42.9 Gy in 13 fractions with iii) 50 Gy in 25
fractions (the control arm). All fractions were administered over a five week period. Note that the
cosmetic outcomes described here were all reported in Yarnold 20058, but not the follow-up
publication.1 Therefore, the source for all data in this section is Yarnold 2005.
8 A subset of 1,202
patients underwent breast appearance assessment. Change in breast appearance was assessed
using photographs which were scored by blinded assessors. Clinician assessments were also
performed.
The change in breast appearance, based on photographic and clinical assessment, is shown in
Table 42. There was a significant difference between the three study arms in terms of any
change in breast appearance, and a marked change in breast appearance (p<0.001). Patients in
the 39 Gy arm were the least likely to have a marked change in breast appearance at 10 years
(93.4% with no event) compared with the 50 Gy arm and 42.9 Gy arm (90.2% and 84.4% with
no event respectively).8
The publication noted for change in breast appearance based on photographic assessment, that
there was some evidence of variation in the difference between the fractionation schedules as
follow-up increased, as the 50 and 39 Gy arms appear to be converging, but analysis shows this
not to be statistically significant (p=0.08). The probability of any change in breast appearance ten
years after radiotherapy is shown in Figure 6. The risk of developing any radiation effect was
much lower for patients allocated to the 39 Gy arm compared with those allocated to the 42.9 Gy
arm. There was a statistically significant difference between the 50 and 39 Gy arms of the trial
over this time period (p=0.01), but weaker evidence for the difference between 50 and 42.9 Gy
(p=0.05).8 Evidence was observed of a lower risk of marked changed in the patients treated with
39 Gy compared to 42.9 Gy. The probability of no change was highest in the 39 Gy arm, followed
by the 50 Gy arm and the 42.9 Gy arm. A similar pattern was seen for a marked change in breast
appearance, as shown in Figure 7.

42 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Figure 6 RMH/GOC trial: Probability of any change in breast appearance late radiation effect ten years after
radiotherapy by fractionation schedule8
Source: Yarnold 20058, Figure 2 page 13
Figure 7 RMH/GOC trial: Probability of marked change in breast appearance late radiation effect ten years
after radiotherapy by fractionation schedule8
Source: Yarnold 20058, Figure 3 page 14
Clinical assessments of overall breast cosmesis (involving an aesthetic judgement), breast
shrinkage, breast distortion, breast oedema, induration and shoulder stiffness showed a
significant difference between the treatment arms. For all outcomes (except shoulder stiffness),
the estimated percent of subjects with no event at 10 years was highest in the 39 Gy arm and
lowest in the 42.9 Gy arm.
The probability of palpable breast induration ten years after radiotherapy is shown in Figure 8.
The 39 Gy arm had the highest probability of no change, followed by the 50 Gy arm and the 42.9
Gy arm.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 43
Figure 8 RMH/GOC trial: Probability of palpable breast induration ten years after radiotherapy by
fractionation schedule8
Source: Yarnold 20058, Figure 4 page 14
For telangiectasia, the estimated percent of subjects with no event at 10 years was 88.0% in the
39 Gy arm, 81.9% in the 50 Gy arm, and 82.0% in the 42.9 Gy arm. The only outcome which
failed to show a dose response was arm oedema (92.3% 50 Gy vs 89.5% 42.9 Gy vs 93.0% 39
Gy). The authors noted that this may be due to the small proportion (20.6%) of patients who
experienced any form of lymphatic radiotherapy.

44 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 42 RMH/GOC trial: Survival analyses of change in breast appearance and clinical assessments of late radiation effects according to fractionation schedule 8
Endpoint Arm Events/total (%) Estimated % with no event at 5 years (95%
CI)
Estimated % with no event at 10 years (95%
CI) P value
Photographic assessment
Any change in breast appearance
50 Gy 140/396 (35.4) 60.4 (54.9, 65.8) 46.6 (37.2, 55.9)
<0.001 42.9 Gy 168/397 (42.3) 54.3 (48.9, 59.7) 42.0 (33.0, 51.0)
39 Gy 112/409 (27.4) 69.7 (64.6, 74.8) 43.9 (30.8, 57.0)
Marked change in breast appearance
50 Gy 22/396 (5.6) 93.6 (90.8, 96.4) 90.2 (85.0, 95.5)
<0.001 42.9 Gy 40/397 (10.1) 88.8 (85.3, 92.2) 84.4 (77.7, 91.1)
39 Gy 14/409 (3.4) 96.1 (93.9, 98.2) 93.4 (87.8, 99.0)
Clinical assessment
Cosmesis (fair/poor)
50 Gy 165/271 (60.9) 44.1 (37.7, 50.4) 28.8 (22.3, 35.4)
<0.001 42.9 Gy 175/266 (65.8) 37.9 (31.7, 44.1) 25.6 (19.3, 31.8)
39 Gy 136/269 (50.6) 54.6 (48.3, 60.9) 42.0 (34.9, 49.1)
Breast shrinkage (moderate/marked)
50 Gy 147/271 (54.6) 49.9 (43.5, 56.3) 36.2 (29.3, 43.1)
0.026 42.9 Gy 148/266 (55.8) 47.2 (40.8, 53.7) 34.2 (27.0, 41.5)
39 Gy 124/269 (46.1) 56.9 (50.6, 63.2) 44.4 (37.0, 51.7)
Breast distortion (moderate/marked)
50 Gy 132/271 (48.9) 54.6 (48.2, 61.0) 41.5 (34.4, 48.6)
0.005 42.9 Gy 148/266 (55.8) 45.7 (39.9, 52.1) 38.0 (31.4, 44.6)
39 Gy 115/269 (42.8) 59.3 (53.1, 65.4) 51.4 (44.4, 58.4)
Breast oedema (moderate/marked)
50 Gy 34/271 (12.6) 87.6 (83.6, 91.7) 86.2 (81.8, 90.7)
0.004 42.9 Gy 54/266 (20.3) 80.2 (75.3, 85.2) 78.5 (73.1, 83.9)
39 Gy 29/269 (10.8) 89.4 (85.6, 93.2) 88.5 (84.4, 92.7)
Induration (moderate/marked)
50 Gy 77/271 (28.6) 76.9 (71.5, 82.3) 63.7 (56.6, 70.7)
<0.001 42.9 Gy 108/266 (40.8) 64.4 (58.1, 70.6) 48.9 (41.5, 56.4)
39 Gy 55/269 (20.4) 84.0 (79.2, 88.8) 72.3 (65.5, 79.2)
Telangiectasia (moderate/marked)
50 Gy 37/271 (13.8) 88.0 (83.8, 92.3) 81.9 (76.5, 87.3)
0.065 42.9 Gy 38/266 (14.3) 87.0 (82.7, 91.4) 82.0 (76.5, 87.5)
39 Gy 23/269 (8.6) 94.4 (91.4, 97.4) 88.0 (83.0, 92.9)
Arm oedema (moderate/marked)
50 Gy 17/271 (6.3) 93.8 (90.7, 97.0) 92.3 (88.6, 96.1)
0.494 42.9 Gy 22/266 (8.3) 91.7 (88.1, 95.3) 89.5 (85.1, 93.8)
39 Gy 16/269 (5.9) 95.4 (92.7, 98.1) 93.0 (89.2, 96.8)
Shoulder stiffness (moderate/marked)
50 Gy 21/271 (7.8) 94.1 (91.2, 97.0) 90.0 (85.6, 94.3)
<0.001 42.9 Gy 48/266 (18.1) 84.0 (79.3, 88.6) 78.2 (72.3, 84.0)
39 Gy 19/269 (7.1) 94.2 (91.2, 97.2) 89.9 (85.3, 94.6)
Source: Yarnold 20058, Table 2 page 13

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 45
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm).6
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were
accrued into the quality-of life study (1,129 from START A and 1,079 from START B). Of these
2,208 patients, 1831 had undergone breast-conserving surgery before radiotherapy (885 from
START A and 946 from START B).6
Table 43 reports the self-reported cosmetic outcomes for the women who underwent breast
conserving surgery before radiotherapy. These outcomes were similar between treatment arms
across the two RCTs. The low numbers of patients and events in some subgroups limited the
statistical power of these analyses.6

46 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 43 START A AND B: Survival analyses of moderate or marked grade normal tissue effects from patients’ self-assessments, according to fractionation schedule, type of primary surgery6
Study Arm Hazard ratio (95% CI)
Change in skin appearance since radiotherapy
START A
50 Gy 1
41.6 Gy 0.92 (0.68–1.25)
39 Gy 0.63 (0.45–0.88)
START B 50 Gy 1
40 Gy 0.80 (0.63–1.03)
Skin problems on or in area of affected breast a
START A
50 Gy 1
41.6 Gy 1.02 (0.70–1.50)
39 Gy 0.87 (0.58–1.30)
START B 50 Gy 1
40 Gy 0.86 (0.65–1.15)
Pain in area of affected breast a
START A
50 Gy 1
41.6 Gy 1.29 (0.92–1.82)
39 Gy 1.01 (0.70–1.45)
START B 50 Gy 1
40 Gy 0.97 (0.74–1.26)
Oversensitivity in area of affected breast a
START A
50 Gy 1
41.6 Gy 1.14 (0.81–1.58)
39 Gy 0.79 (0.55–1.12)
START B 50 Gy 1
40 Gy 1.18 (0.91–1.53)
Swelling in area of affected breast a
START A
50 Gy 1
41.6 Gy 0.87 (0.58–1.32)
39 Gy 0.68 (0.44–1.05)
START B 50 Gy 1
40 Gy 0.89 (0.62–1.29)
Arm or shoulder pain a
START A
50 Gy 1
41.6 Gy 1.05 (0.79–1.39)
39 Gy 1.11 (0.83–1.48)
START B 50 Gy 1
40 Gy 1.03 (0.83–1.29)
Shoulder stiffness a
START A
50 Gy 1
41.6 Gy 0.94 (0.65–1.37)
39 Gy 0.98 (0.67–1.41)
START B 50 Gy 1
40 Gy 0.94 (0.70–1.25)
Difficulty in raising or moving arm sideways a
START A
50 Gy 1
41.6 Gy 1.16 (0.76–1.77)
39 Gy 1.15 (0.75–1.76)
START B 50 Gy 1
40 Gy 0.99 (0.73–1.35)
Arm or hand swelling a
START A
50 Gy 1
41.6 Gy 0.77 (0.49–1.21)
39 Gy 0.92 (0.60–1.42)
START B 50 Gy 1
40 Gy 1.12 (0.78–1.60)
Source: Hopwood et al 20106 Table 3 page 7 and Table 4 page 8 Abbreviations: CI=confidence interval a Results adjusted for baseline scores.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 47
Canadian trial2
This trial compared i) 42.5 Gy in 16 fractions over 22 days with ii) 50 Gy in 25 fractions over 35
days (the control arm). Table 44 reports the cosmetic outcome at baseline, 5 years, and 10
years. Although the global cosmetic outcome worsened over time, no significant differences were
observed between the groups at any time. The repeated-measures logistic-regression analysis
suggested that the cosmetic outcome was affected by the time from randomisation as well as by
the patient’s age and tumour size, but there was no interaction with treatment.
Table 44 Canadian trial: Global cosmetic outcome assessed according to the EORTC scalea2
Rating
Baseline 5-year follow-up 10-year follow-up
50 Gy %
42.5 Gy %
50 Gy %
42.5 Gy %
50 Gy %
42.5 Gy %
Excellent 46.3 46.8 34.3 36.4 27.8 30.6
Good 36.3 37.0 44.9 41.5 43.5 39.2
Fair 15.1 14.6 17.3 19.0 25.5 25.4
Poor 2.3 1.6 3.5 3.1 3.2 4.8
Excellent or good
82.6 83.8 b 79.2 77.9 c 71.3 69.8 d
Source: Whelan 20102 Table 2 page 519 Abbreviations: CI=confidence interval a Absolute differences were calculated as the value in the group that received the standard regimen minus the value in the group that received the hypofractionated regimen. b Absolute difference at baseline, -1.2 percentage points (95% CI: -5.4, 3.1). c Absolute difference at 5-year follow-up, 1.3 percentage points (95% CI: -4.2, 6.7). d Absolute difference at 10-year follow-up, 1.5 percentage points (95% CI: -6.9, 9.8).
4.6.2 Post mastectomy
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm).
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were
accrued into the quality-of life study (1,129 from START A and 1,079 from START B). Of these
2,208 patients, 377 had undergone a mastectomy before radiotherapy (244 from START A and
133 from START B).
Table 45 reports the self-reported cosmetic outcomes for the women who underwent
mastectomy before radiotherapy. These outcomes were similar between treatment arms across
the two RCTs. The low numbers of patients and events in some subgroups limited the statistical
power of these analyses.

48 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 45 START A AND B: Survival analyses of moderate or marked grade normal tissue effects from patients’ self-assessments according to fractionation schedule, type of primary surgery6
Study Arm Hazard ratio (95% CI)
Change in skin appearance since radiotherapy
START A
50 Gy 1
41.6 Gy 0.53 (0.28–0.99)
39 Gy 0.64 (0.34–1.17)
START B 50 Gy 1
40 Gy 0.48 (0.20–1.16)
Skin problems on or in area of affected breast a
START A
50 Gy 1
41.6 Gy 0.90 (0.39–2.10)
39 Gy 1.07 (0.48–2.38)
START B 50 Gy 1
40 Gy 2.26 (0.43–11.80)
Pain in area of affected breast a
START A
50 Gy 1
41.6 Gy 0.82 (0.42–1.61)
39 Gy 0.87 (0.45–1.69)
START B 50 Gy 1
40 Gy 0.63 (0.22–1.79)
Oversensitivity in area of affected breast a
START A
50 Gy 1
41.6 Gy 0.87 (0.42–1.81)
39 Gy 0.81 (0.39–1.68)
START B 50 Gy 1
40 Gy 0.55 (0.19–1.54)
Swelling in area of affected breast a
START A
50 Gy 1
41.6 Gy 0.40 (0.11–1.51)
39 Gy 0.98 (0.36–2.61)
START B 50 Gy 1
40 Gy 4.18 (0.61–28.37)
Arm or shoulder pain a
START A
50 Gy 1
41.6 Gy 0.83 (0.47–1.47)
39 Gy 0.97 (0.56–1.69)
START B 50 Gy 1
40 Gy 0.92 (0.47–1.80)
Shoulder stiffness a
START A
50 Gy 1
41.6 Gy 0.74 (0.37–1.46)
39 Gy 0.45 (0.20–0.99)
START B 50 Gy 1
40 Gy 1.10 (0.47–2.58)
Difficulty in raising or moving arm sideways a
START A
50 Gy 1
41.6 Gy 0.61 (0.30–1.24)
39 Gy 0.61 (0.31–1.23)
START B 50 Gy 1
40 Gy 0.79 (0.35–1.77)
Arm or hand swelling a
START A
50 Gy 1
41.6 Gy 1.09 (0.50–2.35)
39 Gy 0.88 (0.40–1.95)
START B 50 Gy 1
40 Gy 0.65 (0.20–2.17)
Source: Hopwood et al 20106 Table 3 page 7 and Table 4 page 8 Abbreviations: CI=confidence interval a Results adjusted for baseline scores.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 49
4.6.3 Any surgery
START A4
This trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13 fractions over
five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The change in breast
appearance was assessed by photograph in 1,055 patients who had undergone breast
conserving surgery.
The hazard ratios for a mild or marked change in breast appearance, compared with the 50 Gy
arm, were 1.09 (95% CI 0.85, 1.40) for the 41.6 Gy arm and 0.69 (95% CI 0.52, 0.91) for the 39
Gy arm. This difference was not significant for the 41.6 Gy arm (p=0.62), but was significant for
the 39 Gy arm (p=0.01). This is shown in Table 46. A Kaplan-Meier plot is shown in Figure 9.
Table 46 START A: Mild or marked change in breast appearance4
Study arm Crude hazard ratio (95% CI) P value
50 Gy 1 –
41.6 Gy 1.09 (95% CI 0.85, 1.40) 0.62
39 Gy 0.69 (95% CI 0.52, 0.91) 0.01
Source: Bentzen et al 20084 page 337 Abbreviations: CI=confidence interval
Figure 9 START A: Kaplan-Meier plot of mild/marked change in breast appearance (photographic) in 1055
patients with breast conserving surgery4
Source: Bentzen et al 20084 Figure 3 page 337
Other cosmetic outcomes are discussed on page 50 as part of the combined START A and B
study data.

50 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
START B5
This trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions over
five weeks (the control arm). The change in breast appearance was assessed by photograph in
923 patients who had undergone breast conserving surgery.
The hazard ratio for a mild or marked change in breast appearance for the 40 Gy arm (compared
with the 50 Gy arm) was 0.83 (95% CI 0.66, 1.04; p=0.06). This is shown in Table 47. A Kaplan-
Meier plot is shown in Figure 10.
Table 47 START B: Mild or marked change in breast appearance5
Study arm Crude hazard ratio (95% CI) P value
50 Gy 1 –
40 Gy 0.83 (0.66, 1.04) 0.06
Source: Bentzen et al 20085 page 1103 Abbreviations: CI=confidence interval
Figure 10 START B: Kaplan-Meier plot of mild/marked change in breast appearance (photographic) in 923
patients with breast conserving surgery5
Source: Bentzen et al 20085 Figure 4 page 1103
Other cosmetic outcomes are discussed below as part of the of the combined START A and B
trials data.
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 51
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm).
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were
accrued into the quality-of life study (1,129 from START A and 1,079 from START B).
Figure 11 shows the forest plot for patient reported normal tissue effects in the START A and
START B trials. Two sets of outcomes were reported: breast symptoms and arm or shoulder
symptoms. Arm or shoulder symptoms have been discussed in the previous section on adverse
events and toxicity.
In the START A trial, there were no statistically significant differences between the 41.6 Gy and
50 Gy arms. Change in breast appearance, breast hardness, breast shrinkage, pain in area of
affected breast and oversensitivity in area of affected breast favoured the 50 Gy arm, while
change in skin appearance and swelling in area of affected breast favoured the 41.6 Gy arm.
Skin problems on or in area of affected breast had a hazard ratio of 1.01.
When the 39 Gy and 50 Gy arms in the START A trial were compared, all outcomes favoured the
39 Gy arm (with the exception of breast shrinkage which had a hazard ratio of 1.00 ). The only
outcome which statistically significantly favoured the 39Gy arm was change in skin appearance
(hazard ratio 0.63 95% CI 0.47, 0.84, p=0.0019).
In the START B trial, all outcomes favoured the 40 Gy arm, with the exception of oversensitivity
in area of affected breast which favoured the 50 Gy arm. The only statistically significant
difference was change in skin appearance, which favoured the 40 Gy arm (hazard ratio 0.76 95%
CI 0.60, 0.97; p=0.0262).

52 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Figure 11 START A AND B: Forest plots of normal tissue effects assessed as moderate or marked by
patients, according to radiotherapy regimen6
Source: Hopwood et al 20106 Figure 2 page 6 Positions of squares in the forest plot show the estimate of the hazard ratio describing relative effect of the test schedule compared with control, with the 95% CI represented by horizontal lines. Squares to the left of the vertical line indicate when rates of adverse effects are lower in the test schedule compared with control; estimates to the right of the line indicate whether rates are higher in the test schedule. Size of squares is proportional to the precision of the estimate, with larger squares indicating greater precision. *In patients who had completed breast-conserving surgery only. (A) START trial A, 41.6 Gy vs 50 Gy. (B) START trial A, 39 Gy vs 50 Gy. (C) START Trial B, 40 Gy vs 50 Gy.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 53
4.6.4 Conclusions
The results are summarised in Table 48. There was no statistically significant difference in the
majority of cosmetic outcomes assessed by the included publications.
RMH/GOC reported the risk of developing any late radiation effect was statistically significantly
lower for patients in the 39 Gy arm compared to the 50 Gy arm (p=0.01). For most clinically
assessed breast and arm outcomes estimated at 10 years, compared to the 50 Gy arm, there
were fewer events for patients in the 39 Gy arm and more in the 42.9 Gy arm.8
The START A trial reported that the 39 Gy arm was associated with significantly less mild or
marked change in photographic breast appearance (HR 0.69 95% CI 0.52, 0.91, p=0.01)4 and
change in skin appearance (HR 0.63 95% CI 0.47, 0.84, p=0.0019).6 The 40 Gy arm of the
START B trial was associated with significantly less change in skin appearance (40 Gy: HR 0.76
95% CI 0.60, 0.97, p=0.0262).6
In subgroup analyses for the START A and START B trials, the relative effects of the
randomised radiation schedules on patients reported symptoms did not vary significantly
according to type of primary surgery (breast conserving or mastectomy). . 8
These results should be considered in the context of the difference in cosmetic outcomes
assessed in each publication, the methods of assessing cosmetic outcome and the difference in
hypofractionated radiotherapy regimens.
Table 48 Summary of key results for cosmetic outcomes
Study ID Study arms Results
Post breast conserving surgery
RMH/GOC8 39 Gy in 13 fractions over 5 weeks
42.9 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
39 Gy: adverse cosmetic outcomes were reported less frequently when compared to the 50 Gy arm (p=0.01)
Canadian2 42.5 Gy in 16 fractions over 22 days
50 Gy in 25 fractions over 35 days*
No statistically significant differences in any cosmetic outcome
Any surgery
START A4 39 Gy in 13 fractions over 5 weeks
41.6 Gy in 13 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
41.6 Gy: No statistically significant differences in any cosmetic outcome
39 Gy: No statistically significant differences in cosmetic outcome, with the exception of mild or marked change in breast appearance (HR 0.69 95% CI 0.52, 0.91, p=0.01)
START B5 40 Gy in 15 fractions over 5 weeks
50 Gy in 25 fractions over 5 weeks*
0.77 (95% CI 0.61-0.98), p=0.02
Combined data from START A and B6^
As for START A and START B Change in skin appearance
39 Gy: HR 0.63 95% CI 0.47, 0.84, p=0.0019
40 Gy: HR 0.76 95% CI 0.60, 0.97, p=0.0262
Subgroup analysis by breast conserving surgery and mastectomy: NS
Abbreviations: CI=confidence interval, HR=hazard ratio, NS=not significant * control arm ^ Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were accrued into the quality-of-life study (1,129 from START A and 1,079 from START B)

54 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
4.7 Quality of life
The START A and START B trials reported quality of life outcomes .6
4.7.1 Post breast conserving surgery
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm).
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were
accrued into the quality-of life study (1,129 from START A and 1,079 from START B). Of these
2,208 patients, 1831 had undergone breast-conserving surgery before radiotherapy (885 from
START A and 946 from START B).
Table 49 shows the results of three self-reported scales assessed using the EORTC (European
Organisation for Research and Treatment of Cancer) modules for subjects who underwent
breast-conserving surgery: the BR23 breast symptoms subscale, the BR23 arm or shoulder
symptoms subscale and the body image scale.6 There was no significant difference in outcomes
based on study arm. The low numbers of patients and events in some subgroups limited the
statistical power of these analyses.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 55
Table 49 START A AND B: Breast, arm, or shoulder symptoms and body image scale scores at 5 yearsa according to radiotherapy regimen, type of primary surgery6
Study Arm Median (IQR)
BR23 breast symptoms subscale (0–100)
START A
50 Gy 8.3 (0–25.0)
41.6 Gy 8.3 (0–16.7)
39 Gy 8.3 (0–16.7)
START B 50 Gy 8.3 (0–16.7)
40 Gy 8.3 (0–16.7)
BR23 arm or shoulder symptoms subscale (0–100)
START A
50 Gy 11.1 (0–22.2)
41.6 Gy 11.1 (0–22.2)
39 Gy 11.1 (0–22.2)
START B 50 Gy 11.1 (0–22.2)
40 Gy 11.1 (0–22.2)
Body image scale (0–30)
START A
50 Gy 1.0 (0–5.0)
41.6 Gy 2.0 (0–7.0)
39 Gy 1.0 (0–5.0)
START B 50 Gy 1.0 (0–5.0)
40 Gy 1.0 (0–5.0)
Source: Hopwood et al 20106 Table 5 page 9 Higher scores indicate more symptoms or concerns. a Subgroup analyses undertaken with all follow-up data in generalised estimating equation models, but only 5-year data are shown for simplicity of presentation
4.7.2 Post mastectomy
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm).
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients were
accrued into the quality-of life study (1,129 from START A and 1,079 from START B). Of these
2,208 patients, 377 had undergone a mastectomy before radiotherapy (244 from START A and
133 from START B).
Table 50 shows the results of three self-reported scales for subjects who underwent mastectomy:
the BR23 breast symptoms subscale, the BR23 arm or shoulder symptoms subscale and the
body image scale. There was no significant difference in outcomes based on study arm. The low
numbers of patients and events in some subgroups limited the statistical power of these
analyses.

56 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Table 50 START A AND B: Breast, arm, or shoulder symptoms and body image scale scores at 5 yearsa according to radiotherapy regimen, type of primary surgery6
Study Arm Mastectomy Median (IQR)
BR23 breast symptoms subscale (0–100)
START A
50 Gy 8.3 (0–20.8)
41.6 Gy 8.3 (0–25.0)
39 Gy 8.3 (0–22.9)
START B 50 Gy 8.3 (0–16.7)
40 Gy 8.3 (0–16.7)
BR23 arm or shoulder symptoms subscale (0–100)
START A
50 Gy 11.1 (5.6–33.3)
41.6 Gy 11.1 (0–33.3)
39 Gy 11.1 (0–22.2)
START B 50 Gy 11.1 (0–22.2)
40 Gy 11.1 (0–22.2)
Body image scale (0–30)
START A
50 Gy 8.0 (2.2–15.5)
41.6 Gy 3.0 (0–8.0)
39 Gy 6.0 (1.0–11.0)
START B 50 Gy 4.0 (1.0–9.5)
40 Gy 4.0 (0–7.0)
Source: Hopwood et al 20106 Table 5 page 9 Higher scores indicate more symptoms or concerns. a Subgroup analyses undertaken with all follow-up data in generalised estimating equation models, but only 5-year data are shown for simplicity of presentation
4.7.3 Any surgery
START A and B6
The START A trial compared i) 39 Gy in 13 fractions over five weeks and ii) 41.6 Gy in 13
fractions over five weeks with iii) 50 Gy in 25 fractions over five weeks (the control arm). The
START B trial compared i) 40 Gy in 15 fractions over three weeks with ii) 50 Gy in 25 fractions
over five weeks (the control arm).
Of the 4,451 patients enrolled in either the START A or START B trials, 2,208 patients entered
the quality-of life study (1,129 from START A and 1,079 from START B). Quality of life was
assessed using the European Organisation for Research and Treatment of Cancer (EORTC)
breast-cancer module BR23. This consists of six subscales, of which three were used in the
analysis: breast symptoms subscale (pain, swelling, oversensitivity, and skin problems in the
breast), arm subscale (swelling in arm or hand, arm or shoulder pain, and difficulty moving the
arm), and body image (containing four items which were not reported in the publication).
Table 51 shows the results of three self-reported scales: the BR23 breast symptom subscale, the
BR23 arm or shoulder symptoms subscale and the BR23 body image scale. There was no
significant differences between regimens for the breast symptom subscale (START A p=0.5558,
START B p=0.8757), the arm or shoulder symptoms subscale (START A p=0.2071, START B
p=0.3101) or the body image scale (START A p=0.9990, START B p=0.3405). For all

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 57
radiotherapy regimens across each of the three scales, scores declined significantly indicating
improved body image, between baseline and 60 months (p=<0.0001).
Table 51 START A AND B: Breast, arm, or shoulder symptoms and body image scale scores, according to radiotherapy regimen, over time from randomisation6
0 months
median (IQR) 6 months
median (IQR) 12 months
median (IQR) 24 months
median (IQR) 60 months
median (IQR)
BR23 breast symptoms subscale (0–100)
Trial A
50 Gy 16.7 (8.3–25.0) 16.7 (8.3–33.3) 16.7 (8.3–25.0) 8.3 (0–25.0) 8.3 (0–25.0)
41.6 Gy 16.7 (8.3–25.0) 16.7 (8.3–33.3) 16.7 (0–25.0) 8.3 (0–25.0) 8.3 (0–16.7)
39 Gy 16.7 (8.3–25.0) 16.7 (8.3–25.0) 16.7 (0–25.0) 8.3 (0–16.7) 8.3 (0–16.7)
Trial B
50 Gy 16.7 (8.3–25.0) 16.7 (8.3–33.3) 16.7 (8.3–25.0) 8.3 (0–16.7) 8.3 (0–16.7)
40 Gy 16.7 (8.3–25.0) 16.7 (8.3–33.3) 16.7 (0–25.0) 8.3 (0–16.7) 8.3 (0–16.7)
BR23 arm or shoulder symptoms subscale (0–100)
Trial A
50 Gy 22.2 (0–33.3) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2)
41.6 Gy 11.1 (0–33.3) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2)
39 Gy 22.2 (11.1–33.3) 11.1 (0–33.3) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2)
Trial B
50 Gy 11.1 (11.1–33.3) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2)
40 Gy 22.2 (11.1–33.3) 11.1 (0–33.3) 11.1 (0–22.2) 11.1 (0–22.2) 11.1 (0–22.2)
Body image scale (0–30)
Trial A
50 Gy 3.0 (1.0–8.0) 3.0 (0–7.0) 3.0 (0–7.0) 2.0 (0–7.0) 2.0 (0–7.0)
41.6 Gy 4.0 (1.0–8.7) 2.0 (0–6.0) 2.0 (0–6.0) 2.0 (0–6.0) 2.0 (0–7.0)
39 Gy 4.0 (1.0–9.0) 2.0 (0–7.0) 2.0 (0–7.0) 2.0 (0–7.0) 2.0 (0–6.0)
Trial B
50 Gy 3.0 (0–8.0) 2.0 (0–6.0) 1.0 (0–5.0) 1.0 (0–5.7) 1.5 (0–6.0)
40 Gy 3.0 (0–7.0) 2.0 (0–6.0) 1.0 (0–5.0) 1.0 (0–5.0) 1.0 (0–5.0)
Source: Hopwood et al 20106 Table 2 page 5 Abbreviations: IQR=interquartile range Higher scores indicate more symptoms or concerns.
4.7.4 Conclusions
The START A and START B trials evaluated quality of life outcomes.6 There was no evidence
that any hypofractionated radiotherapy regimen was associated with a statistically significant
difference in quality of life score as measured by the BR23 breast symptom subscale.24
Subgroup analysis was performed, with results analysed by surgery type. There were no
statistically significant differences in outcomes, nor were any interaction tests significant overall.
These results must be considered in the context of the range of hypofractionated radiotherapy
regimes and single quality of life instrument used to assess this outcome.

58 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
5 Guidelines
5.1 Guidelines search
In order to identify current recommendations in existing radiotherapy guidelines, a systematic
search of guidelines was undertaken in March 2010. The nine guideline websites which were
searched are shown in Table 52. The same search terms were used for all websites. Manual
searching of reference lists was also performed. A total of three citations were identified. One set
of guidelines9, that was published after the literature search date, was included post hoc.
Table 52 Search terms for guidelines websites
Guideline websites Search terms Citations
Agency for Healthcare Research and Quality
“hypofractionated radiotherapy” OR “fractionated radiotherapy” OR “irradiation therapy” OR “irradiation treatment” OR “hypofractionated radiation treatment” OR “fractionated radiation treatment” OR “therapeutic radiology” OR (“breast cancer” AND radiotherapy)
0
EuroScan 0
Australia and New Zealand Horizon Scanning Network 0
Centre for Reviews and Dissemination 0
MSAC 0
National Guideline Clearinghouse 0
NHMRC 0
NHS Evidence 2
CADTH 0
Manual 1
Total 3
5.2 Results
The American Society for Radiation Oncology (ASTRO) guidelines on fractionation for
whole breast irradiation 20109
Based on the same body of evidence evaluated in this systematic review, ASTRO found that
evidence supports the equivalence of hypofractionated whole breast irradiation with
conventionally fractionated whole breast irradiation for patients who satisfy all these criteria:
Patient is 50 years or older at diagnosis.
Pathologic stage is T1-2 N0 and patient has been treated with breast-conserving surgery.
Patient has not been treated with systemic chemotherapy.
Within the breast along the central axis, the minimum dose is no less than 93% and
maximum dose is no greater than 107% of the prescription dose (±7%) (as calculated
with 2-dimensional treatment planning without heterogeneity corrections).
For patients who do not satisfy all of these criteria, the task force could not reach consensus and
therefore chose not to render a recommendation.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 59
There were few data to define the indications for and toxicity of a tumour bed boost in patients
treated with hypofractionated radiotherapy. The task force agreed that the use of
hypofractionated radiotherapy alone (without a boost) is not appropriate when a tumour bed
boost is thought to be indicated. When a boost is indicated, there was lack of consensus
regarding the appropriateness of hypofractionated radiotherapy. Although the majority of the task
force members thought that there were sufficient data showing safety of hypofractionated
radiotherapy followed by a tumour bed boost to recommend its use in otherwise suitable patients,
a minority believed that conventional radiotherapy should be used instead when a tumour bed
boost is indicated.
For patients not receiving a tumour-bed boost, the task force favoured a dose of 42.5 Gy in 16
fractions over approximately 22 days when hypofractionated radiotherapy was planned. The
optimal hypofractionated radiotherapy regimen to use when a boost is given and the optimal
tumour-bed boost dose-fractionation to use in conjunction with hypofractionated radiotherapy
have not been determined.
Two-dimensional treatment planning with optimisation of dose homogeneity in the central axis is
the minimum acceptable standard for hypofractionated radiotherapy treatment planning.
However, CT-guided treatment planning using three-dimensional dose compensation is strongly
recommended to optimise dose homogeneity throughout the entire breast. As a conservative
measure, the task force recommended exclusion of the heart from the primary treatment fields
provided that coverage of the primary tumour site is not compromised.
The New Zealand Ministry of Health Guidelines for Management of Early Breast Cancer
200910
The New Zealand Ministry of Health guidelines made the following recommendation regarding
hypofractionated radiotherapy:
Recommendation
• Radiotherapy treatment for early invasive breast cancer should use an accepted regimen such
as:
50 Gy in 25 fractions over 5 weeks (Grade A)
45 Gy in 20 fractions over 5 weeks (Grade B)
42.5 Gy in 16 fractions over 3.5 weeks for those with small or medium breasts, not requiring
boost or nodal radiation (Grade B)
40 Gy in 15 fractions over 3 weeks* (Grade B)
Good practice points
• If boost radiotherapy is used after a hypofractionated regimen it should be at the standard 2 Gy
per fraction
• Women with large breasts and those with significant postoperative induration, oedema,
erythema, haematoma or infection should be considered for extended fractionation, with smaller
daily doses over 5–6 weeks
* It should be noted that the data for long-term follow-up in the latter three schedules of this recommendation is still awaited Notes Grades indicate the strength of the supporting evidence, rather than the importance of the recommendations A good practice point represents the opinion of the Guideline Development Team, or feedback from consultation within New Zealand where no evidence is available

60 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
A summary of the findings of the systematic review used to inform the guidelines is presented
below.
Survival
The SIGN guideline12
reported data from the Canadian trial that found no significant difference in
overall survival rate at the five-year follow-up with a hypofractionated compared with standard
regimen.7 The START Trialists Group reported that in the START B trial there were significant
differences in disease-free and overall mortality rates in favour of the group who received the
hypofractionated regimen (40 Gy in 15 fractions over 3 weeks).5 The authors anticipate that this
effect will diminish over time, and the long-term follow-up of the trial continues.
Loco-regional recurrence
In the Canadian trial study reported in the SIGN guideline, no significant difference in local
recurrence free rate at the five-year follow-up was seen (96.8% with 25 fractions vs 97.2% with
16 fractions; 95% CI 1.5–2.4).7 At the five-year follow-up, RMH/GOC reported hazard ratios
comparing 50 Gy to 42.9 Gy of 0.90 (95% CI 0.55–1.46) and 1.14 (95% CI 0.72–1.79) for 39 Gy
compared to 50 Gy.1 After 10 years, the probability of recurrence was significantly greater in the
39 Gy than in the 42.9 Gy group (difference 3.7%, 95% CI 0.3–8.3, p=0.027). RMH/GOC
concluded that the results were consistent with the hypothesis that fewer, larger fractions are at
least as safe and as effective as ‘standard’ regimens but that the shorter schedule should be
restricted to clinical trials.1 At the five-year follow-up, the START Trialists Group reported of the
START B trial that the absolute difference in loco-regional recurrence could be up to 1.7% better
and at most 1% worse with the hypofractionated regimen. The trial authors concluded that the
delivery of 40 Gy in 15 fractions appeared to result in a loco-regional recurrence rate that was at
least as favourable as the ‘standard’ 50 Gy in 25 fractions.5
Other outcomes
Cosmetic results at five years were similar between fractionation schedules. However, in a 12-
year update of the Canadian trial data, the incidence of moderate to severe late radiation
morbidity (subcutaneous fibrosis) at 10 years doubled (8% vs 4%)††
in the shorter fractionation
schedule.7 The START A trial reported in a quality of life assessment that changes in breast
appearance and breast hardness were the most commonly reported side effects. These side
effects were less marked in the 39 Gy group and similar in the 41.6 Gy and 50 Gy groups, in
contrast to those found at 10 years by RMH/GOC. (11.2% for 42.9 Gy in 13 fractions of 3.3 Gy vs
6.4% for 50 Gy in 25 fractions of 2 Gy). Both the START A and START B trials reported that the
follow-up period of five years was too short to assess potential late normal tissue effects, such as
cardiac damage.4-5
Follow-up continues for these trials. The long-term safety of the short fractionation schedule for
the nodal areas has not been established.
Conclusions
Based on a review of the published evidence it was noted that there is currently insufficient
evidence to identify one optimum fractionation schedule. The results of ongoing clinical trials will
††
The 8% vs 4% values come directly from the text of the The New Zealand Ministry of Health Guidelines. It has been noted that these values are not consistent with the results reported in Whelan 2010, however the The New Zealand Ministry of Health Guidelines do not cite a page or table reference, or note if this data was calculated post hoc or obtained from the authors.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 61
inform guidelines in the future. To minimise late tissue damage whilst maximising tumour control,
the Guideline Development Team supported the administration of boost dose radiotherapy at 2
Gy per fraction where indicated following a hypofractionated regimen. The Guideline
Development Team also noted that extended fractionation with smaller doses over five to six
weeks should be considered in women with large breasts and postoperative side effects.
NICE 2009 guidelines for early and locally advanced breast cancer11
The NICE 2009 guidelines made the following recommendation regarding dose fractionation:
Recommendation
• Use external beam radiotherapy giving 40 Gy in 15 fractions as standard practice for patients
with early invasive breast cancer after breast conserving surgery or mastectomy.
Qualifying statement: This recommendation is based on RCT evidence of clinical effectiveness
and the guideline development group agreeing that a regimen using fewer fractions would
probably be cost effective.
The summary of the clinical evidence noted that rates of local recurrence were not significantly
different between conventional 50 Gy fractions and hypofractionated schedules. One study
(START B) found that distant relapse was lower in the hypofractionated arm which improved the
rates of disease-free survival and overall survival.5 Assessments of cosmetic outcomes were less
consistent, and depended on the comparisons made. One RCT7 reported no significant
difference between the 50 Gy and 42.5 Gy arms, whilst another 8 reported a significantly poorer
cosmetic outcome in the 42.9 Gy arm when compared to the 39 Gy arm. The hazard ratio for no
change in breast appearance was significantly improved in the 39 Gy arm of the START A trial4
compared to 50 Gy; whilst there was no difference between the 50 Gy and 41.6 Gy arms in
START A4 or between 50 Gy and 40 Gy in START B
5.
Global cosmetic outcomes were also less consistent since effects were reported at different
times and between different fractionation doses. Breast oedema, fibrosis, lymphoedema and
telangiectasia were reported in few studies.
The guidelines advised that careful treatment planning is required for all patients to avoid
potential hotspots in the breast but this may be particularly important with hypofractionated
schedules. Patients with breast reconstruction/augmentation or large breast size may have a
better cosmetic result using conventional dose radiotherapy of 50 Gy in 25 fractions (lower dose
per fraction), although 3D radiotherapy planning may make hypofractionated regimens
equivalent.
The use of hypofractionated regimes should result in considerable saving of resources, both
human and financial.
SIGN 200512
The Scottish Intercollegiate Guidelines Network (SIGN) management of breast cancer in women
guidance paper was developed in 2005, prior to the publication of a number of key RCTs (such
as the START trials). No formal recommendations were made.

62 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
The guidelines noted that “current evidence is not able to identify an optimal dose/fractionation
for post-operative radiotherapy. It is therefore reasonable to treat patients with currently accepted
regimens such as 50 Gy in 25 daily fractions over five weeks, 45 Gy in 20 fractions, or 40 Gy in
15 or 16 fractions. Results of ongoing trials investigating fractionated are awaited”.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 63
6 Conclusions
A systematic review of the literature identified five clinical trials of hypofractionated radiotherapy
for the treatment of early breast cancer. Two trials were in patients who had undergone breast
conserving surgery (RMH/GOC and Canadian trials)1-2, 7-8
and three were in patients who had
undergone any form of surgery (START A, START B and Spooner)3-5
. The studies evaluated a
number of different hypofractionated radiotherapy regimens.
All five trials reported local recurrence rates (RMH/GOC, Canadian, Spooner, START A and
START B trials). There was no evidence that any hypofractionated radiotherapy regimen was
associated with a statistically significantly difference in local recurrence rate when compared to a
control arm. The Canadian trial reported no difference when subgroups were analysed, with the
exception of tumour grade. The impact of the 42.5 Gy regimen on local recurrence was less in
patients with high-grade tumours compared to patients with low-grade tumours (p=0.01).2
Two studies (START A and START B) reported local-regional and distant relapse. The studies
found no significant difference in local-regional relapse.4-5
START B reported that the 40 Gy
study arm had a statistically significantly lower rate of distant relapse when compared with the
control arm (p=0.01).5
Four studies reported overall survival (Canadian, START A, START B and Spooner). Most
studies reported that there was no evidence that hypofractionated radiotherapy was associated
with a statistically significantly difference in overall survival. The START B study found that 40 Gy
in 15 fractions over three weeks was associated with a statistically significantly lower all-cause
mortality rate when compared with 50 Gy in 25 fractions over five weeks (p=0.03).5 Therefore,
there was no evidence that any hypofractionated radiotherapy regimen was associated with a
worse overall survival rate (i.e. the only study that reported a significant difference showed lower
mortality for patients treated with hypofractionated radiotherapy).
Three studies reported adverse events and toxicity outcomes (Canadian, START A and START
B). There were generally no differences in adverse events and toxicity outcomes between the
study arms. START A and START B noted a statistically significant difference in skin appearance
(favouring the 39 Gy arm, p=0.0019 and 40 Gy arm, p=0.0262 when compared with the control
arm).6
Four studies reported cosmetic outcomes (RMH/GOC, Canadian, START A and START B).
Some studies reported differences in cosmetic outcomes between study arms. The RMH/GOC
trial reported that the risk of developing any late radiation effect was statistically significantly
lower for patients in the 39 Gy arm compared to the 50 Gy arm (p=0.01), but more often in the
42.9 Gy arm compared to the control (p=0.05).8 START A and START B reported that changes
in skin appearance were less frequent in patients receiving 39 Gy in 13 fractions (p=0.0019) and
patients receiving 40 Gy in 13 fractions (p=0.0262), when compared to 50 Gy in 25 fractions.6
START A and START B reported quality of life outcomes. There was no evidence that any
hypofractionated radiotherapy regimen was associated with a statistically significant difference in
quality of life score as measured by the BR23 breast symptom subscale. There was no
difference in cosmetic outcomes or quality of life when outcomes were evaluated by surgery
type.6

64 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
Overall, there was no evidence that the evaluated hypofractionated radiotherapy regimens were
associated with an increased rate of local recurrence or reduced survival. There were some
differences in adverse events and toxicity, as well as cosmetic outcomes.
All of the reported outcomes need to be considered in the context of range of hypofractionated
radiotherapy regimens that were evaluated. Although 50 Gy in 25 fractions was used as a control
arm in all trials, no two trials compared the same two radiotherapy regimens, making
comparisons difficult. The study design should also be considered. Not all studies were powered
to detect a difference in all outcomes. RMH/GOC1, 8
was powered to detect late change in breast
appearance and the Canadian2, 7
trials were powered to detect a difference in local recurrence.
START A4 and START B
5 were powered to detect a difference in local-regional tumour relapse
rate. The included studies had a follow-up period of 6 – 10 years. This length of follow-up should
be sufficient to detect a difference in outcome.
The generalisablity the findings must also be considered. For example, the Canadian trial
excluded patients who had node-positive invasive carcinoma, or patients with a breast width of
more than 25 cm.7 It may be that the results of this study may not apply to women with ductal
carcinoma in situ only, women with node-positive cancer or women with large breasts.
The literature review did not identify any studies which specifically assessed the use of
hypofractionated radiotherapy in conjunction with chemotherapy or other biological therapies.
The Canadian trial assessed local recurrence by systematic therapy use, and found no difference
recurrence rates.2
Overall, there was no evidence that any hypofractionated radiotherapy regimen was associated
with a statistically significantly difference in local recurrence rate or a significantly worse overall
survival rate. There were some differences in adverse event, toxicity and cosmetic outcomes,
although this was not consistent across all hypofractionated radiotherapy protocols. These
results should be considered in the context of the included patient populations, statistical power
of the studies, different hypofractionated radiotherapy regimens used and length of follow-up.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 65
7 References
1. Owen JR, Ashton A, Bliss JM, et al. Effect of radiotherapy fraction size on tumour control in patients
with early-stage breast cancer after local tumour excision: long-term results of a randomised trial.
Lancet Oncol 2006;7(6):467-71.
2. Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation therapy for
breast cancer. N Engl J Med 2010;362(6):513-20.
3. Spooner D, Stocken DD, Jordan S, et al. A randomised controlled trial to evaluate both the role and
optimal fractionation of radiotherapy in the conservative management of early breast cancer. San
Antonio Breast Cancer Symposium, 2008.
4. Bentzen SM, Agrawal RK, Aird EG, et al. The UK Standardisation of Breast Radiotherapy (START)
Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial.
Lancet Oncol 2008;9(4):331-41.
5. Bentzen SM, Agrawal RK, Aird EG, et al. The UK Standardisation of Breast Radiotherapy (START)
Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial.
Lancet 2008;371(9618):1098-107.
6. Hopwood P, Haviland JS, Sumo G, et al. Comparison of patient-reported breast, arm, and shoulder
symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the
randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol 2010;11(3):231-40.
7. Whelan T, MacKenzie R, Julian J, et al. Randomized trial of breast irradiation schedules after
lumpectomy for women with lymph node-negative breast cancer. J Natl Cancer Inst
2002;94(15):1143-50.
8. Yarnold J, Ashton A, Bliss J, et al. Fractionation sensitivity and dose response of late adverse
effects in the breast after radiotherapy for early breast cancer: long-term results of a randomised trial.
Radiother Oncol 2005;75(1):9-17.
9. Smith BD, Bentzen SM, Correa CR, et al. Fractionation for Whole Breast Irradiation: An American
Society for Radiation Oncology (ASTRO) Evidence-Based Guideline. Int J Radiat Oncol Biol Phys
2010;July 15(Epub ahead of print):1-10.
10. New Zealand Guidelines Group (NZGG). Management of early breast cancer. NZGG: Wellington
New Zealand, 2009.
11. National Institute for Health and Clinical Excellence (NICE). Early and locally advanced breast
cancer: diagnosis and treatment. NICE: UK, 2009.
12. Scottish Intercollegiate Guidelines Network (SIGN) Management of breast cancer in women: A
national clinical guideline. SIGN: Edinburgh Scotland, 2005.
13. National Breast Cancer Centre. Clinical practice guidelines for the management of early breast
cancer (2nd edition). Commonwealth of Australia: Canberra, 2001.
14. James ML, Lehman M, Hider PN, et al. Fraction size in radiation treatment for breast conservation
in early breast cancer. Cochrane Database Syst Rev 2008;3):CD003860.
15. NIH consensus conference. The treatment of early breast cancer. JAMA 1991;265(3):391-5.
16. Ash D. Waiting times for cancer treatment. Clin Oncol (R Coll Radiol) 2000;12(3):140.
17. Mackillop WJ, Fu H, Quirt CF, et al. Waiting for radiotherapy in Ontario. Int J Rad Oncol, Biol,
Phys 1994;30(1):221-8.
18. Shahid A, Athar MA, Asghar S, et al. Post mastectomy adjuvant radiotherapy in breast cancer: A
comparision of three hypofractionated protocols. J Pak Med Assoc 2009;59(5):282-87.
19. Dwyer P, Hickey B and Burmeister B. Hypofractionated breast radiotherapy: impact on
departmental waiting times and cost. J Med Imag Radiat Oncol 2009;54(3):229-34.

66 Hypofractionated radiotherapy for the treatment of early breast cancer:
a systematic review
20. Taher AN, El-Baradie MM, Essa H, et al. Hypofractionation versus conventional fractionation
radiotherapy after conservative treatment of breast cancer: early skin reactions and cosmetic results.
J Egypt Natl Canc Inst 2004;16(3):178-187.
21. National Health and Medical Research Council. How to use the evidence: assessment and
application of scientific evidence. Canberra: Commonwealth of Australia, 2000.
22. National Health and Medical Research Council. NHMRC additional levels of evidence and grades
for recommendations for developers of guidelines. Commonwealth of Australia: Canberra, 2009.
23. Egger M, Smith GD and Sterne JA. Uses and abuses of meta-analysis. Clin Med 2001;1(6):478-
84.
24. Sprangers MA, Groenvold M, Arraras JI, et al. The European Organization for Research and
Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: first results from a
three-country field study. J Clin Oncol 1996;14(10):2756-2768.

Hypofractionated radiotherapy for the treatment of early breast cancer: a systematic review Page 67
Appendix A Contributors
Working group members
The following people were members of the working group:
Associate Professor Boon Chua (Chair) Radiation oncologist
Dr Marie-Frances Burke Radiation oncologist
Professor Geoff Delaney Radiation oncologist
Dr Jane O’Brien Surgeon
Ms Jan Rice Breast care nurse
Ms Geraldine Robertson Consumer representative
Dr Kirsty Stuart Radiation oncologist
Cancer Australia staff
The following Cancer Australia staff were involved in the project:
Ms Katrina Anderson Project Officer – Research
Ms Phillipa Hastings Project Officer
Dr Anne Nelson Evidence Review & Research Leader
Ms Sue Sinclair General Manager
Ms Heidi Wilcoxon Program Manager





























