Embed Size (px)
Citation preview

Hypersensitivities 1
Immune HypersensitivityChapter 18
Self-Test Questions:Intro: allA1-2: allA3: 1, 3, 5A4: allB: 1, 2, 4, 5C: 1 - 4D: 1 - 4

Hypersensitivities 2
What characteristics are shared by all hypersensitivies?
Immune responses: Primary (sensitization) responseSecondary (activation) response
Abnormal (hyper-) response to antigens (allergens)
Symptoms: localized or systemic
Onset can be: Early, Late or Chronic

Hypersensitivities 3
What are hypersensitivities?
4 types of hypersensitivities (Gel and Combs classification) Immune
Name system involved Effectors Effects OnsetType 1 “Atopic” Humoral (IgE) mast cells inflammation seconds
eosinophils (anaphylaxsis)
Type II “Cytotoxic” Humoral/ macrophages cell destruction hours Complement complement (hemolysis)
Type III “Im. Complex” Humoral/ granulocytes inflammation hours Complement
Type IV “Delayed type” Cell-mediated macrophages inflammation days
-- TH1

Hypersensitivities 4
Type I – Atopic hypersensitivities
AG presentationDCs, even Basos & Eosinosactivate TH2 cells
IgE productionclass switching to IgE
Mast cell sensitizationIgE binding to Fc receptors
Mast cell activationDegranulationsecretionsynthesis
Early phase& late phaseresponses
McGraw-HillType-I

Hypersensitivities 5
Early phase responses
Molecular Mediators:Primary – in granules
Secondary – synthesized later
(w/in 1- few minutes)
Localized clinical response (Atopy)atopic asthma:urticaria (hives)eczema (skin lesions)atopic rhinitisfood allergies
Systemic clinical response (anaphylaxis)anaphylatic shock

Hypersensitivities 6
e.g., Erythema, etc“peak flow rate” measurements
Due to:
-- Cytokines from mast cells
-- Recruited eosinophils & TH2
-- degranulation
Chronic Type I-- eosinophilia
-- inflammation: damaged
airways & mucous membranes
Late phase responses-- 4-6 hours later
Early phase Late phase

Hypersensitivities 7
What factors affect predisposition toward Type I hypersensitivities?
Genetic factors
Environmental factors
Hygiene hypothesis

Hypersensitivities 8
Treatment
Skin testing-- carries some risk
Drugs therapies-- Theophylline (blocks degranulation)
-- antihistamines (block histamine receptors)
-- epinephrine (reverses trachael & bronchiole SM
and contracts arteriole SM)
Desensitization
Desensitization Therapy

Hypersensitivities 9
Type II hypersensitivity-- “Cytotoxic”
Ig binding to AG on cells-- triggers cell lysisComplement mediatedMacrophage mediated
Various types of hemolytic disorderse.g., Blood transfusion incompatibility
{see section in chapter 17}
Autoimmune disorderse.g.. Goodpasture’s syndrome
RBC being phagocytosed in fetal erythroblastosis
1967 Science 158: cover
Hypersensitivities 10
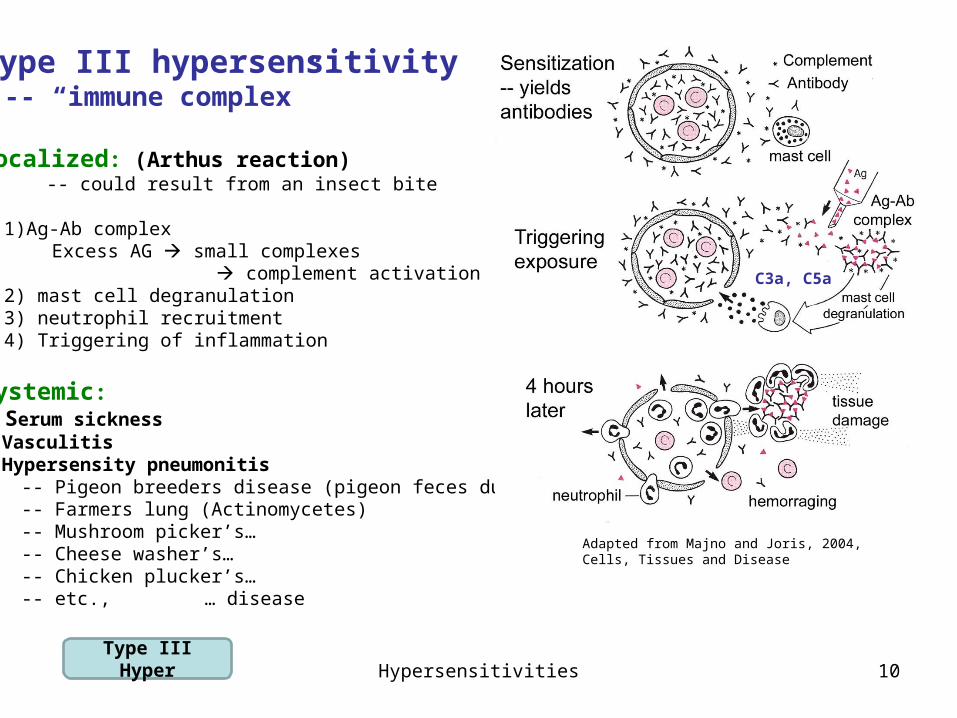
Type III hypersensitivity -- “immune complex”
Localized: (Arthus reaction) -- could result from an insect bite
1)Ag-Ab complex Excess AG small complexes
complement activation2) mast cell degranulation3) neutrophil recruitment4) Triggering of inflammation
Systemic: Serum sickness Vasculitis Hypersensity pneumonitis
-- Pigeon breeders disease (pigeon feces dust)-- Farmers lung (Actinomycetes)-- Mushroom picker’s… -- Cheese washer’s…-- Chicken plucker’s…-- etc., … disease
Adapted from Majno and Joris, 2004, Cells, Tissues and Disease
Type III Hyper
C3a, C5a

Hypersensitivities 11
Type IV hypersensitivity“Delayed-type”-- slow onset ~day(s) (if sensitized)
TH1-cell mediated
Sensitization phase -- week(s) onset-- TH1 expansion
Effector stage – day(s) onset-- TH1 & macrophage activation-- inflammation
Latex type IV hypersensitivity

Hypersensitivities 12
Type IV hypersensitivities, con’t
Contact dermatis reactionsOften involves hapten productione.g. to: hair sprays, plant toxins, turpentine
TH1

Hypersensitivities 13
Tuberculosis(see Chapter 14 pp 212-213)
-- Persistent Mycobacterium tuberculosis
Granuloma (tubercule) formation TH1 cells and activated macrophages
‘caseous’ regions extended tissue destruction





























