Embed Size (px)
Citation preview

Can J Gastroenterol Vol 27 No 11 November 2013 621
Hypersecretory villous adenoma as the primary cause of intestinal intussusception and McKittrick-Wheelock syndrome
Susana Sanchez Garcia MD, Pedro Villarejo Campos MD, Maria del Carmen Manzanares Campillo MD, Aurora Gil Rendo MD, Virginia Muñoz Atienza MD, Esther Pilar García Santos MD,
Francisco Javier Ruescas García MD, Jose Luis Bertelli Puche MD
Hospital General Universitario, Ciudad Real, SpainCorrespondence: Dr Susana Sanchez Garcia, Hospital General Universitario, Valencia Street, No6 4A, 13002 Ciudad Real, Spain.
Telephone 66-117-9720, e-mail [email protected] for publication May 21, 2013. Accepted June 16, 2013
Intestinal invagination or intussusception is the most common cause of intestinal obstruction in children and represent 5% of adult cases.
This intestinal obstruction is due to a lesion in the intestinal mucosa that initiates intussusception or intestinal invagination (90% of adult cases are malignant). Moreover, villous adenomas, which represent malignant potential, are found within these lesions of intestinal mucosa. There are variants of villous adenomas known as hypersecre-tory adenomas, which are described as intestinal lesions located more frequently in the rectum and distal colon. In addition, these variant adenomas can cause hypersecretory diarrhea and an electrolyte dis-turbance known as McKittrick-Wheelock syndrome.
CASE prESEntAtionA 77-year-old woman was hospitalized due to rectal prolapse and a large rectal polypoid mass, with symptoms of rectal bleeding that developed weeks before. Forty-eight hours after hospitalization, she experienced progressive clinical worsening. On physical examination, a painful abdomen without any sign of peritonitis was noted. After rectal touch, a rough, hard tumour located 5 cm from the anus was palpated with some bleeding.
Laboratory data revealed slight leukocytosis with neutrophilia (leukocytes 12.7×109/L, 88% neutrophils); anemia (hemoglobin 91 g/L, hematocrit 27.3%); a worsening of previous renal insufficiency (blood urea nitrogen 55.3 mmol/L, creatinine 415.5 μmol/L); marked hypokalemia (2.9 mmol/L) with normonatremia (146 mEq/L); meta-bolic acidosis with normal lactic acid and high anion GAP levels (pH 7.16, bicarbonate 17.8 mmol/L, lactic acid 7 g/L, anion GAP 21.4 mg/dL).
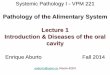
Abdominal computed tomography (CT) with intravenous contrast was performed and revealed a giant hiatal hernia, intestinal loops and significant stomach distention, and colon distention to the rectal level. CT imaging also suggested significant colorectal invagination (Figure 1).
At the rectal level, imaging revealed a mass approximately 4 cm in diameter that appeared to correspond to the polypoid lesion visualized in a previous colonoscopy focused at the head of the invagination.
Given the clinical, laboratory and radiological data, and after pro-gressive worsening, the woman underwent emergent surgery. Suspecting tumoural complications (eg, perforation, intestinal obstruction, intes-tinal pain, etc), a laparotomy revealed a rectal tumour that was hard on palpitation, suggestive of rectal intussuception.
Thus, given the exceedingly low possibility of manual reduction and the presence of ischemic lesions in the rectal wall, an anterior ultralow resection and terminal colostomy (Hartman’s intervention) was performed (Figure 2).
Pathology results documented a villous and adenomatous polyp 3.7 cm in size, with sites of moderate dysplasia associated with areas of ischemic colitis and lymphatic glands with a nonspecific reactive pattern. The patient was diagnosed with McKittrick-Wheelock syn-drome related to a hypersecretory villous adenoma that caused rectal intussuception and secondary intestinal obstruction.
DiSCUSSionIntestinal invagination is defined as prolapse of a part of intestine into an adjacent portion. In adults, only 5% of intestinal obstruction symp-toms are due to intussuception, and 90% of intestinal intussuception cases are due to pathological processes. In 66% of cases, intussuception of the bowel is caused by a malignant lesion. However, in the small intestine, causative lesions of the invagination progress from benign neoplasic lesions (Meckel diverticulum or inflammatory lesions) to intestinal adhesions. In fact, malignant lesions represent 30% of invaginations in the small intestine (1-6).
Our patient presented with atypical symptoms, experiencing intes-tinal obstruction secondary to rectal intussuception, together with sig-nificant alterations in electrolyte levels (acute kidney failure, marked
iMage of tHe MontH
©2013 Pulsus Group Inc. All rights reserved
Figure 1) Computed tomography image suggesting the presence of a colo-rectal invagination
Figure 2) Portion of resected bowel demonstrating the intussusception

Sanchez Garcia et al
Can J Gastroenterol Vol 27 No 11 November 2013622
hypokalemia and metabolic acidosis, with normal lactic acid and high anion GAP levels) (1,2,5).
These electrolyte alterations fulfilled the diagnostic criteria for McKittrick-Wheelock syndrome, first described in 1954, and refer-enced hypersecretory diarrhea symptoms as well as a state of severe electrolyte depletion in relation to large rectal villous adenomas. These lesions have a high potential for malignancy and may appear asymptomatically. Among these lesions, villous adenomas represent 3% to 6% of all colonic tumours, of which only 3% are hypersecretory adenomas (7,8). Villous adenomas causing McKittrick-Wheelock syn-drome are characterized by their hypersecretory capacity. Hypersecretion of fluids and electrolytes is due to an increase in cyclic AMP produced by adenylate cyclase and elevated levels of prostaglandin E2, a medi-ator involved in the development of secretory diarrhea (9,10). This electrolyte depletion causes a typical syndrome characterized by dehydration, confusion and even death (7,10). In the present case, the lesion was caused by a hypersecretory villous adenoma, which not only led to symptoms of intestinal obstruction, but was also associated with electrolyte alterations typical of McKittrick-Wheelock syndrome.
The diagnosis of intussusception was based on imaging tests such as CT: a part of the intestine prolapsed into another (double-wall image) is considered pathognomonic of intussusceptions, distinguishing the head of the invagination among the edematous intestines in 70% of cases (10-16). The management of intestinal intussusception depends on the patient’s clinical status and the time of symptom onset. Conservative treatment is indicated in cases for which there are no clinical signs or lesions on the head of demonstrable intussusception(s). These data are considered to be predictors of spontaneous symptom resolution; there have been reports of intussusceptions with these fea-tures that have resolved spontaneously and were treated conserva-tively with periodic radiological monitoring. However, surgical
treatment is indicated for the majority of intestinal intussusceptions due to the risk of an intestinal ischemia and the possibility of a malig-nant lesion in the head of the intussusception, which can go unnoticed.
Treatment of hypersecretory villous adenomas is mainly surgical. Use of indomethacin in patients with McKittrick-Wheelock syndrome has been reported to inhibit or decrease electrolyte secretion in indi-viduals who refuse surgery. Among the surgical options, transanal resection (transanal endoscopic microsurgery) using a posterior presac-ral approach (anterior tumours) or mucosectomy, and abdominal sur-gery for large tumours, are preferred. This type of benign tumour has the potential to become malignant; the only treament option that has been proven to be effective is surgery involving complete excision of the lesion, which results in normalization of electrolyte levels and prevents progression to a malignant tumour (17,18).
rEFErEnCES1. Wang N, Cui XY, Liu Y, et al. Adult intussusception:
A retrospective review of 41 cases. World J Gastroenterol 2009;15:3303-8.
2. Yakan S, Caliskan C, Makay O, et al. Intussusception in adults: Clinical characteristics, diagnosis and operative strategies. World J Gastroenterol 2009;15:1985-9.
3. Dvorkin LS, Knowles CH, Scott SM, et al. Rectal intussusception: Characterization of symptomatology. Dis Colon Rectum 2005;48:824-31.
4. Seguridad en los pacientes quirúrgicos Tratado de cirugía. Fundamentos biológicos de la práctica quirúrgica moderna. Sabiston, Cap. 71:2063-4.
5. Guillén Paredes MP, Campillo Soto A, Martín Lorenzo JG, et al. Adult intussusception − 14 case reports and their outcomes. Rev Esp Enferm Dig 2010;102:32-40.
6. Morera-Ocón FJ, Hernández-Montes E, Bernal-Sprekelsen JC. Intestinal invagination in adults: Presentation of a case and a review of the Spanish literature. Cir Esp 2009;86:358-62.
7. Murature Stordiau GE, Suárez Alecha J, Zazpe Ripa C, et al. Acute renal failure and profund hypokalemia caused by a villous adenoma in the rectum: McKittrick-Wheelock syndrome. Rev Esp Enferm Dig 2009;101:78-9.
8. Dagan A, Reissman P. Giant secretory villous adenoma of the rectum and sigmoid presenting as McKittrick-Wheelock syndrome. Int J Colorectal Dis 2010;25:909-10.
9. Chand M, Bradford L, Nash GF. Intussusception in colorectal cancer. Clin Colorectal Cancer 2008;7:204-5.
10. Kim SW, Shin HC, Kim IY, et al. CT findings of colonic complications associated with colon cancer. Korean J Radiol 2010;11:211-21.
11. Seguridad en los pacientes quirúrgicos Tratado de cirugía. Fundamentos biológicos de la práctica quirúrgica moderna. Sabiston, Cap. 45; p.1180-1198
12. Tresoldi S, Kim YH, Blake MA, et al. Adult intestinal intussusception: Can abdominal MDCT distinguish an intussusception caused by a lead point? Abdom Imaging 2008;33:582-8.
13. Takeuchi K, Tsuzuki Y, Ando T, et al. The diagnosis and treatment of adult intussusception. J Clin Gastroenterol 2003;36:18-21.
14. Thomas AW, Mitre R, Brodmerkel GJ Jr. Sigmoidorectal intussusception from a sigmoid lipoma. J Clin Gastroenterol 1995;21:257.
15. Wang LT, Wu CC, Yu JC, et al. Clinical entity and treatment strategies for adult intussusceptions: 20 years’ experience. Dis Colon Rectum 2007;50:1941-9.
16. Jiménez-Rodríguez RM, Díaz-Pavón JM, González JM, et al. Adenoma velloso gigante secretor de iones. Revisión de la literatura y estado actual de su tratamiento. Rev Esp Enferm Dig 2007;99:616-17.
17. Rea JD, Lockhart ME, Yarbrough DE, et al. Approach to management of intussusception in adults: A new paradigm in the computed tomography era. Am Surg 2007;73:1098-105.
18. Martínez García R, Gómez Abril SA, Trullenque Juan R, Martínez Mas E, Martínez Abad M. McKittrick-Wheelock syndrome: Giant secretor rectal adenoma. Cir Esp 2010;87:117-9.
ConCLUSionSIntestinal intussusception in adults is rare; therefore, considering a malignant intestinal lesion is important because it is the most com-mon cause. Its diagnosis is based on visualization of an area of intestine prolapsed into another (wall or double-wall thickening) using CT imaging.
Within intestinal mucosal lesions, <1% of hypersecretory villous adenomas represent malignant potential. In fact, they can cause symptoms of hypersecretory diarrhea with electrolyte disturbances characteristic of McKittrick-Wheelock syndrome, in addition to the possibility of intestinal intussusception given their significant size.
Surgery is the definitive treatment for intestinal intussuscep-tions and villous adenomas. It improves electrolyte disturbances and eliminates the possibility of malignancy.
OLESTYR® absorbs and combines with the bile acids in the intestine which are then excreted in the feces, resulting in a partial removal of bile acids from the enterohepatic circulation by preventing their absorption1,*
Taking aim at bile acids
Montreal, CANADA H4P 2T4
OLESTYR® is indicated for the symptomatic control of bile acid-induced diarrhea due to short bowel syndrome and for the relief of pruritus associated with partial biliary obstruction. OLESTYR® is contraindicated in patients with complete biliary obstruction where bile is not excreted into the intestine and in those individuals who have shown hypersensitivity to any of its components. OLESTYR® (CHOLESTYRAMINE RESIN) SHOULD NOT BE TAKEN IN ITS DRY FORM. ALWAYS MIX OLESTYR® WITH WATER OR OTHER FLUIDS BEFORE INGESTING. SINCE OLESTYR® MAY BIND OTHER DRUGS GIVEN CONCURRENTLY, PATIENTS SHOULD TAKE OTHER DRUGS AT LEAST ONE HOUR BEFORE OR 4-6 HOURS AFTER OLESTYR® (OR AT AS GREAT AN INTERVAL AS POSSIBLE) TO AVOID IMPEDING THEIR ABSORPTION. Drug interactions: OLESTYR® may delay or reduce the absorption of concomitant oral medication such as thyroid and thyroxine preparations, warfarin, chlorothiazide (acidic), phenylbutazone, phenobarbital, tetracycline, penicillin G and digitalis. The concomitant drug should be re-titrated to avoid overdosage when OLESTYR® is discontinued. The discontinuance of cholestyramine could pose a hazard to health if a potentially toxic drug such as digitalis has been titrated to maintenance level while the patient was taking cholestyramine. Also, OLESTYR® may interfere with the pharmacokinetics of drugs (e.g. estrogens) that undergo enterohepatic recirculation. It should be assumed that concomitantly administered drugs have the potential of interacting with OLESTYR® unless clinical studies have shown otherwise. OLESTYR® binds to bile acids and may interfere with absorption of fat-soluble vitamins such as A, D and K. In long-term treatment with OLESTYR®, concomitant supplementation with water-miscible parenteral forms or oral administration of vitamins A, D and K as appropriate should be considered. Chronic use of OLESTYR® may be associated with increased bleeding tendency due to hypoprothrombinemia associated with vitamin K de� ciency. This will usually respond promptly to parenteral vitamin K1 and recurrences can be prevented by oral administration of vitamin K1. Reduction of serum or red cell folate has been reported over long term administration of cholestyramine resin. Supplementation with folic acid should be considered in these cases. Adverse reactions: The most frequent adverse effect of cholestyramine resin is constipation. OLESTYR® may produce or worsen pre-existing constipation. Dosage should be reduced or discontinued in such cases. Fecal impaction and aggravation of hemorrhoids may occur. Cholestyramine potentially may cause steatorrhea or accentuate pre-existing steatorrhea and this may require reduction and adjustment of dosage. Warnings and Precautions: Pregnancy or lactation: Since OLESTYR® is not absorbed systemically, it is not expected to cause fetal harm when administered during pregnancy in recommended dosages. There are, however, no adequate and well-controlled studies in pregnant or lactating women, and the known interference with absorption of fat-soluble vitamins may be detrimental even in the presence of supplementation. Use in pregnancy or lactation requires that the potential bene� ts of drug therapy be weighed against the possible hazards to the mother and the child. Caution should be exercised when OLESTYR® is administered to a nursing mother. The possible lack of proper vitamin absorption may have an effect on nursing infants. Use in children: The effects of long-term drug administration in pediatric patients are unknown. A pediatric dosage schedule has not been established. Because bile acid sequestrants may interfere with absorption of fat-soluble vitamins, appropriate monitoring of growthand development is essential if OLESTYR® is used in children. Geriatrics: Appropriate studies on the relationship of age to the effects of OLESTYR® have not been performed in the geriatric population. However, patients over 60 years of age may be more likely to experience gastrointestinal side effects.1
Please refer to the Product Monograph for important information about contraindications, warnings, precautions, adverse events, dosing, and patient selection. Full Product Monograph is available upon request. Should you have any questions, please contact PENDOPHARM at 1-888-550-6060 or email us at [email protected].
Fully covered on all provincial
formularies
ChChCh amineamine
*Clinical signi� cance is unknown
© 2013 PENDOPHARM, a division of Pharmascience Inc. All rights reserved.OLESTYR® is a registered trademark used under license by Pharmascience Inc.
See prescribing summary on page
March_Olestyr_Journal_Ad_E.indd 1 13-02-18 10:25 AM

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com




![ReviewArticle - Hindawi Publishing Corporationdownloads.hindawi.com/journals/cjgh/2018/6150861.pdfCanadianJournalofGastroenterologyandHepatology .; %CI: .-., p = . ) []. Lastly, in](https://img.dokumen.tips/doc/110x75/5fd365b36bdb6805366effb8/reviewarticle-hindawi-publishing-canadianjournalofgastroenterologyandhepatology.jpg)

![Quantitative Assessment of Endoscopic Images for Degree of ......of villous atrophy classified using the scoring system for villous atrophy developed by Marsh [14] and modified by](https://img.dokumen.tips/doc/110x75/6052605b579c49341e0a18ad/quantitative-assessment-of-endoscopic-images-for-degree-of-of-villous-atrophy.jpg)
![ClinicalSignificanceofHepatocyteGrowthFactorand ...downloads.hindawi.com/journals/cjgh/2020/2104314.pdf · positivelywiththelevelofbothTGF-β andHGF.esefindingsaresimilartotheresultsobtainedbyCiecko-Michalskaetal.[1],whileotherstudiesreportednorela-tionshipbetweenTGF](https://img.dokumen.tips/doc/110x75/5f0419717e708231d40c50d7/clinicalsignificanceofhepatocytegrowthfactorand-positivelywiththelevelofbothtgf-.jpg)




![Surgical Approach of Degenerated Giant Rectal Villous ......endoscopic resection of a circumferential lesion: is the occurrence of a stenosis [19]. The huge villous tumor constitutes](https://img.dokumen.tips/doc/110x75/60f7dd8ee931e11a5d1b5077/surgical-approach-of-degenerated-giant-rectal-villous-endoscopic-resection.jpg)















