Embed Size (px)
Citation preview

HYPERLIPIDEMIA AND METABOLIC SYNDROME IN SCHIZOPHRENIAA study of the Northern Finland 1966 Birth Cohort
KAISASAARI
Faculty of Medicine,Department of Psychiatry,
Department of Public Health Scienceand General Practice,
University of Oulu
OULU 2005


KAISA SAARI
HYPERLIPIDEMIA AND METABOLIC SYNDROME IN SCHIZOPHRENIAA study of the Northern Finland 1966 Birth Cohort
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in the Väinö Pääkkönen Hall of the Departmentof Psychiatry, on June 10th, 2005, at 12 noon
OULUN YLIOPISTO, OULU 2005

Copyright © 2005University of Oulu, 2005
Supervised byProfessor Matti IsohanniProfessor Hannu KoponenDocent Sari Lindeman
Reviewed byProfessor Preben Bo MortensenProfessor Leo Niskanen
ISBN 951-42-7727-9 (nid.)ISBN 951-42-7728-7 (PDF) http://herkules.oulu.fi/isbn9514277287/
ISSN 0355-3221 http://herkules.oulu.fi/issn03553221/
OULU UNIVERSITY PRESSOULU 2005

Saari, Kaisa, Hyperlipidemia and metabolic syndrome in schizophrenia. A study ofthe Northern Finland 1966 Birth CohortFaculty of Medicine, Department of Psychiatry, Department of Public Health Science and GeneralPractice, University of Oulu, P.O.Box 5000, FIN-90014 University of Oulu, Finland 2005Oulu, Finland
AbstractSchizophrenia is associated with a shortened life expectancy and increased somatic comorbidity withe.g. cardiovascular disorders. The purpose of this study was to evaluate hyperlipidemia and metabolicsyndrome in schizophrenia and thus find specific risk factors for excess mortality and morbidity.
The study population was a subsample of the Northern Finland 1966 Birth Cohort, a generalpopulation-based birth cohort. In 1997, 8,463 members of the cohort were invited to a clinicalexamination, where e.g. blood samples were taken after an overnight fast. Total cholesterol (TC),high-density lipoprotein (HDL), low-density lipoprotein (LDL) and triglycerides (TG) weredetermined. The following psychiatric diagnostic categories were used: 1) DSM-III-R schizophrenia(n = 31), 2) other psychoses (n = 21), 3) non-psychotic disorders (n = 104), 4) comparison group(n = 5,498), having no psychiatric hospital treatment.
Mean TC (5.5 mmol/l) and TG (1.5 mmol/l) were significantly higher in the schizophrenia groupthan in the comparison group (5.1 mmol/l and 1.2 mmol/l, respectively).
To evaluate serum lipid levels in subjects with and without antipsychotic medication the samplewas analyzed according to used medication. The prevalence of hypercholesterolemia, high LDLcholesterol and hypertriglyceridemia was high in persons using antipsychotic medication (31%, 20%and 22%, respectively) compared to persons without such medication (12%, 10% and 7%,respectively).
We found higher triglyceride levels in patients who were ≤ 20 years old at the onset ofschizophrenia (mean 1.7 mmol/l; N = 17) as compared with patients with later onset (mean 1.4 mmol/l; N = 14) or non-hospitalized controls (mean 1.2 mmol/l; N = 5,453). The difference between thefirst and third group was significant (p < 0.01), and there was a negative correlation between the ageat onset and the level of serum triglycerides (r = -0.35, p = 0.05).
To evaluate the prevalence of metabolic syndrome, the subjects were assessed for the presence ofmetabolic syndrome according to the criteria of the National Cholesterol Education Program. Theprevalence of metabolic syndrome was high in subjects with schizophrenia compared with thecomparison group (19% vs. 6%, p = 0.010).
The results indicate an elevated risk for hyperlipidemia and metabolic syndrome in persons withschizophrenia or on antipsychotic medication. Regular monitoring of weight, serum lipid and glucoselevels and blood pressure is important. Comprehensive efforts directed at controlling weight andimproving physical activity are needed.
Keywords: antipsychotic agents, cohort studies, hyperlipidemia, metabolic syndrome x,psychotic disorders, schizophrenia


Acknowledgements
This work was carried out at the Department of Psychiatry and at the Department of Public Health Science and General Practice, University of Oulu. During this study I have had the opportunity to draw upon the knowledge, expertise and experience of numerous friends and co-workers, acknowledged below, without whom this study would not have been completed.
I wish to express my sincere gratitude to Professor (emerita) Paula Rantakallio, Department of Public Health Science and General Practice, University of Oulu, for making it possible to use the valuable data represented by the Northern Finland 1966 Birth Cohort as a basis for this study.
I am most grateful to my supervisor Professor Matti Isohanni, Department of Psychiatry, University of Oulu. He has always found time for discussions and guidance, and by arranging financial support he has also created an environment where I have been able to carry out this study successfully.
I want to express my most sincere and special thanks to my other supervisor, Docent Sari Lindeman, Department of Psychiatry, University of Oulu, who prompted me to begin this project and was the first promoter of this study. She has always believed in this study, even during the hard moments, and given me the support I have needed.
I am very grateful to Professor Hannu Koponen, Department of Psychiatry, University of Oulu, who has also supervised this thesis. His excellent knowledge of scientific work and his rational advice have been an essential part of carrying out this study.
I also want to extend my warmest thanks to Docent Juha Moring, Head of the Department of Psychiatry, Oulu University Hospital, for the facilities and the help during this work.
My sincere thanks are due to Professor Marjo-Riitta Järvelin, Department of Public Health Science and General Practice, University of Oulu and Department of Epidemiology and Public Health, Imperial College London, for valuable advice and a supportive attitude during preparation of the original publications.
It is my pleasure to thank the other co-authors, Professor Markku Savolainen, Department of Internal Medicine, University of Oulu, Jari Jokelainen, MSc, Department of Public Health Science and General Practice, University of Oulu, Professor Juha Veijola, Department of Psychiatry, University of Oulu, Professor Peter Jones, Department

of Psychiatry, University of Cambridge, Liisa Laurén, PhD, Department of Epidemiology and Public Health, Imperial College London, Jaana Laitinen, PhD, Oulu Regional Institute of Occupational Health, and Kaisa Viilo, BSc, Department of Psychiatry, University of Oulu, for their important collaboration and expert knowledge.
I also acknowledge my deep indebtedness to the official referees of the dissertation. Professor Preben Bo Mortensen, National Centre for Register-based Research, Aarhus University, Denmark, and professor Leo Niskanen, Department of Internal Medicine, University of Kuopio, have carefully reviewed the manuscript and provided valuable advice and constructive criticism.
I am most grateful to Richard Burton, BSc and to Anna Vuolteenaho, MA, for their corrections of the English language, and to Kaisa Viilo, BSc, for checking the layout of this dissertation.
Many persons at the Department of Psychiatry and Department of Public Health Science and General Practice, University of Oulu, and Oulu University Hospital have supported this work. I wish to thank especially Ms. Pirkko Kaan, Ms. Anja Kylmänen, Ms. Minna Lakkapää and Ms. Tuula Ylitalo for their help with several practical details.
The following foundations are acknowledged for having provided financial support for the study: the Academy of Finland, the Sigrid Juselius Foundation, Stanley Medical Research Institute and Lilly Säätiö (Lilly Foundation of Finland).
I owe special thanks to my father and my mother, who have always loved me and made me state arguments for my opinions since my early childhood; maybe that is why I had to do this work. I also want to thank my brother and my sister for being what they are.
Finally, I want to thank my cohabitant Mika for teaching me to see things I would not have seen without him, and my daughter Vilma for bringing so much happiness and joy into my life.
Oulu, April 26, 2005 Kaisa Saari

Abbreviations
ANOVA Analysis of variance ATP III The Adult Treatment Panel III BMI Body Mass Index CI Confidence interval CPZ Chlorpromazine DSM-III-R Diagnostic and Statistical Manual of Mental Disorders, Third
Edition, Revised DSM-IV-TR Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition, Text Revision FHDR Finnish Hospital Discharge Register HDL High density lipoprotein ICD International Classification of Diseases IFG Impaired Fasting Glycemia IGT Impaired Glucose Tolerance LDL Low density lipoprotein SD Standard deviation SI International System SMR Standardized mortality ratio TC Total cholesterol TG Triglycerides WHO Word Health Organization


Conversion factors
In Finland SI units are used in determining cholesterol and triglyceride levels, but in the USA lipid levels are usually given in conventional units, mg/dL. To translate SI units into U.S. values the following conversion factors were used: for converting mmol/l to mg/dL the cholesterol values were divided by 0.02586, triglycerides by 0.01129, glucose levels by 0.0555 (New Mexico AIDS InfoNet).
− Cholesterol: 1 mmol/l equals about 40 mg/dL (for example 6.2 mmol/l equals 240
mg/dL) − Triglycerides: 1 mmol/l equals about 90 mg/dL (for example 1.7 mmol/l equals about
150 mg/dL) − Glucose: 1 mmol/l equals about 20 mg/dL (for example 6.1 mmol/l equals about 110
mg/dL)


List of original publications
This thesis is based on the following original publications, which are referred to in the text by the Roman numerals I-V. I Koponen H, Saari K, Savolainen M, Isohanni M (2002) Weight gain and glucose
and lipid metabolism disturbances during antipsychotic medication. A review. European Archives of Psychiatry & Clinical Neuroscience 252:294-298.
II Saari K, Jokelainen J, Veijola J, Koponen H, Jones PB, Savolainen M, Järvelin M-
R, Laurén L, Isohanni M, Lindeman S (2004) Serum lipids in schizophrenia and other functional psychoses: a general population northern Finland 1966 birth cohort survey. Acta Psychiatrica Scandinavica 110:279-285.
III Saari K, Lindeman S, Koponen H, Jokelainen J, Isohanni M (2004) Higher serum
triglyceride levels in early-onset schizophrenia. American Journal of Psychiatry 161:176 (letter).
IV Saari K, Koponen H, Laitinen J, Jokelainen J, Laurén L, Isohanni M, Lindeman S
(2004) Hyperlipidemia in persons using antipsychotic medication: a general population-based birth cohort study. Journal of Clinical Psychiatry 65:547-550.
V Saari K, Lindeman S, Viilo K, Isohanni M, Järvelin M-R, Laurén L, Savolainen
M, Koponen H (2005) A 4-fold risk of metabolic syndrome in patients with schizophrenia. The Northern Finland 1966 Birth Cohort study. Journal of Clinical Psychiatry 66:559-563.
The original papers have been reprinted with permission from Springer (I), Blackwell Publishing (II), the American Journal of Psychiatry, American Psychiatric Association (III), and Physicians Postgraduate Press (IV and V). In addition, some unpublished data have been included in this thesis.

Contents
Abstract Tiivistelmä Acknowledgements Abbreviations Conversion factors List of original publications Contents 1 Introduction ...................................................................................................................15 2 Review of the literature .................................................................................................17
2.1 Definition of schizophrenia ....................................................................................17 2.2 Epidemiology of schizophrenia ..............................................................................18 2.3 Weight gain in association with use of antipsychotics............................................18 2.4 Serum lipids and antipsychotic medication ............................................................19 2.5 Definition and epidemiology of hypercholesterolemia...........................................24 2.6 Definition and epidemiology of metabolic syndrome ............................................25 2.8 Pathogenesis of metabolic syndrome......................................................................26 2.7 Schizophrenia, hypercholesterolemia and metabolic syndrome: how are they linked together?.................................................................................27
3 Aims of the present study ..............................................................................................31 4 Material and methods ....................................................................................................32
4.1 Material and methods for the review ......................................................................32 4.2 Study population and data collection......................................................................32 4.3 Outcome measures, selected covariates and measure procedures ..........................36 4.4 Statistical methods..................................................................................................36 4.5 Ethical considerations.............................................................................................37 4.6 Personal involvement .............................................................................................37
5 Results ...........................................................................................................................38 5.1 Weight gain and glucose and lipid metabolism disturbances during antipsychotic medication (I)........................................................................38 5.2 Serum lipids in schizophrenia and other functional psychoses (II) ........................38 5.3 Serum triglycerides in early onset schizophrenia (III)............................................45

5.4 Hyperlipidemia in subjects using antipsychotic medication (IV)...........................46 5.5 Metabolic syndrome in schizophrenia (V)..............................................................49
6 Discussion .....................................................................................................................52 6.1 Methodic discussion ...............................................................................................52
6.1.1 Strengths of the study ......................................................................................52 6.1.2 Limitations of the study...................................................................................53
6.2 Discussion of the results .........................................................................................54 6.2.1 Weight gain, glucose and lipid metabolism disturbances during antipsychotic medication (I).................................................................54 6.2.2 Serum lipids in schizophrenia and other functional psychoses (II) .................55 6.2.3 Serum triglyceride levels in early onset schizophrenia (III) ............................56 6.2.4 Hyperlipidemia in subjects using antipsychotic medication (IV) ....................56 6.2.5 Metabolic syndrome in schizophrenia (V).......................................................57 6.2.6 Theoretical considerations ...............................................................................58
7 Conclusions ...................................................................................................................61 7.1 Main results ............................................................................................................61 7.2 Clinical and practical implications .........................................................................61 7.3 Implications for further studies...............................................................................64
References

1 Introduction
Schizophrenia is a syndrome causing a major public health problem. It usually begins early in adult life, its prognosis is often poor and it causes excess morbidity and mortality, as well as extensive negative personal, familial, social, occupational and educational consequences.
Those who suffer from schizophrenia have a life expectancy which is approximately 20% shorter than that of the general population (Newman & Bland 1991). A meta-analysis concludes that 60% of the excess mortality in patients with schizophrenia is attributable to physical illness (Brown 1997). The causes of death comprise a broad range of conditions, similar to the general population, but schizophrenic patients die at a younger age. Mortality from cardiovascular disease is increased in both men and women with schizophrenia (Newman & Bland 1991). The greatest research need at the moment seems to be identification of specific risk factors for the excess mortality among schizophrenic patients (Mortensen 2003).
The rates of cardiovascular events and new-onset diabetes are higher than expected in patients with schizophrenia and on antipsychotic medication (Enger et al. 2004). The major risk factors for cardiovascular disease include obesity, dyslipidemia, hypertension and hyperglycemia (Hennekens 1998). These risk factors are key elements defining the metabolic syndrome (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001).
Metabolic syndrome, also called syndrome X (Reaven 1988), or the insulin resistance syndrome (Haffner et al. 1992), includes five major features: 1) abdominal obesity, 2) hypertriglyceridemia, 3) low high-density lipoprotein (HDL) cholesterol, 4) high blood pressure, 5) high fasting glucose (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001). Previous studies on patients with schizophrenia have mainly focused on individual components of metabolic syndrome.
The purpose of this study was to 1) review weight gain and glucose and lipid metabolism disturbances during antipsychotic medication, and to investigate 2) serum lipids in schizophrenia and other functional psychoses, 3) serum triglyceride levels in early onset schizophrenia, 4) hyperlipidemia in subjects using antipsychotic medication,

16
and 5) the risk of metabolic syndrome in schizophrenia in a general population-based birth cohort.

2 Review of the literature
2.1 Definition of schizophrenia
International classifications, such as DSM (Diagnostic and Statistical Manual of Mental Disorders) and ICD (International Classification of Diseases), provide the criteria for diagnosing schizophrenia and other psychotic disorders. In this study the diagnoses have been scrutinized and validated for the DSM-III-R (Diagnostic and Statistical manual of Mental Disorders, third Edition-Revised) criteria (American Psychiatric Association 1987). The diagnostic criteria for schizophrenia in DSM-III-R are the following: A. Presence of characteristic psychotic symptoms in the active phase: either (1), (2), or (3) for at least one week (unless the symptoms are successfully treated): (1) two of the following: delusions, prominent hallucinations, incoherence or marked loosening of associations, catatonic behavior, flat or grossly inappropriate affect, (2) bizarre delusions, (3) prominent hallucinations of a voice with content having no apparent relation to depression or elation, or a voice keeping up a running commentary on the person’s behavior or thoughts, or two or more voices conversing with each other. B. During the course of the disturbance, functioning in such areas as work, social relations, and self-care is markedly below the highest level achieved before onset of the disturbance. C. Schizoaffective disorder and mood disorder with psychotic features have been ruled out. D. Continuous signs of the disturbance for at least six months. In this classification the following schizophrenia diagnoses are given: catatonic, disorganized, paranoid, undifferentiated and residual type (American Psychiatric Association 1987).
In the current Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR) (American Psychiatric Association 2000) diagnosis of schizophrenia is based on same short of criteria as in DSM-III-R. In clinical work in Finland the currently used diagnostic system is ICD-10 (the Tenth Revision of The International Statistical Classification of Diseases and Related Health Problems) (Word Health Organization 1993). When DSM-III-R and DSM-IV-TR are compared to ICD-10 perhaps the only clinically relevant difference is in the time criteria. In ICD-10, symptoms continuing for at least one month’s time are considered schizophrenia.
18
2.2 Epidemiology of schizophrenia
The majority of studies estimating the prevalence of schizophrenia have produced prevalence figures in the range 1.4-4.6 per 1,000 population at risk (Jablensky 2003). The incidence rate of schizophrenia ranges from 0.17 to 0.54 per 1,000 population per year, i.e. they show a threefold difference. In Scandinavian studies incidence rates of 0.20-0.27 per 1,000 have been estimated (Jablensky 2003).
Patients with schizophrenia are at special risk for metabolic disorders because of their unhealthy lifestyle habits: cigarette smoking, unhealthy diet and alcohol consumption leading to obesity and its consequences. Mechanisms causing metabolic disorders are not well understood, involving many factors intercorrelated with each other.
Excess body weight substantially increases the risk of morbidity from a number of other conditions, including hypertension, dyslipidemia, type 2 diabetes mellitus, coronary heart disease, stroke, gallbladder disease, osteoarthritis, sleep apnea and respiratory problems, as well as endometrial, breast, prostate, and colon cancers (National Heart, Lung, and Blood Institute 2001). Increases in all-cause mortality are also associated with higher body weight, as are social stigmatization and discrimination (National Heart, Lung, and Blood Institute 2001).
2.3 Weight gain in association with use of antipsychotics
Weight gain in association with use of conventional antipsychotics was noted as early as the 1950s in connection with the use of chlorpromazine (Stanton 1995). At the time, greater attention was paid to the neurological adverse effects of antipsychotics, although weight gain can be observed in up to 50% of patients on long-term antipsychotic medication. Weight gain is common with conventional low-potency antipsychotics such as thioridazine and chlorpromazine (Allison et al. 1999a, Stanton 1995). Weight gain caused by them has been found to be between 1.5 and 4 kg during the first month of treatment, usually ceasing within one to two years of starting drug treatment. A meta-analysis by Allison et al. (1999a) included over 80 studies and over 30,000 patient measurements. The estimated weight gain at 10 weeks was 0.04 kg for ziprasidone, 0.43 kg for fluphenazine, 0.48 kg for haloperidol, 2.00 kg for risperidone, 2.10 kg for chlorpromazine, 3.49 kg for thioridazine, 3.51 kg for olanzapine and 3.99 kg for clozapine.
With the second-generation antipsychotics clozapine and olanzapine, most weight gain occurs during the first four to five months of treatment, but with olanzapine it continues for up to a year, and with clozapine even longer (Henderson et al. 2000, Kinon et al. 2001). With risperidone there is weight gain for some two to three months after the start of treatment. There are differences between the second-generation antipsychotics, because e.g. the weight gain associated with the use of olanzapine and risperidone has been reported to be more easily reversed than the weight gain associated with clozapine. The effects of quetiapine and ziprasidone on weight have been less prominent (Wirshing et al. 1999, Brecher et al. 2000, Kingsbury et al. 2001). However, the current Consensus

19
Statement (American Diabetes Association et al. 2004) and a review of physical health monitoring of patients with schizophrenia (Marder et al. 2004) both agree that data support a continuum of weight gain liability among second-generation antipsychotics. Ziprasidone is associated with minimal risk, risperidone with medium risk, and olanzapine and clozapine with the greatest risk. Data of quetiapine have been variable, but suggest that its weight gain liability is likely similar to risperidone (Marder et al. 2004). In the Consensus Statement weight gain liabilities of different second generation antipsychotics had been estimated in the same order as described before, and aripiprazole was associated with the same amount of effect as ziprasidone. Limited long-term data are available for these two newer drugs (American Diabetes Association et al. 2004).
2.4 Serum lipids and antipsychotic medication
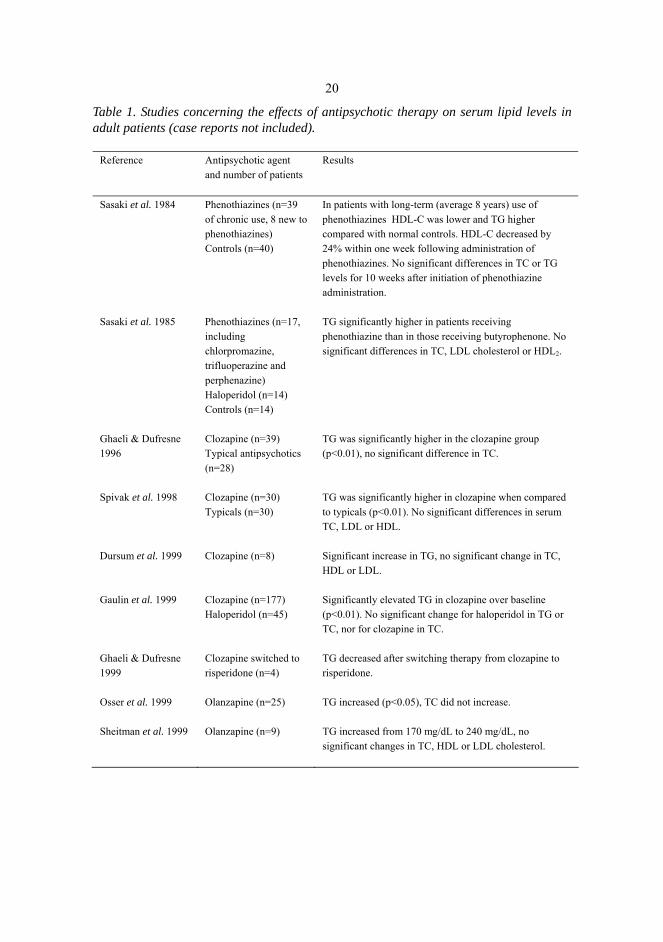
The elevating effect of antipsychotics on serum lipids is well documented in several clinical-based studies involving typical and atypical antipsychotics (Table 1) and recently in one large matched case-control study (Koro et al. 2002).
20
Table 1. Studies concerning the effects of antipsychotic therapy on serum lipid levels in adult patients (case reports not included).
Reference Antipsychotic agent and number of patients
Results
Sasaki et al. 1984 Phenothiazines (n=39 of chronic use, 8 new to phenothiazines) Controls (n=40)
In patients with long-term (average 8 years) use of phenothiazines HDL-C was lower and TG higher compared with normal controls. HDL-C decreased by 24% within one week following administration of phenothiazines. No significant differences in TC or TG levels for 10 weeks after initiation of phenothiazine administration.
Sasaki et al. 1985 Phenothiazines (n=17, including chlorpromazine, trifluoperazine and perphenazine) Haloperidol (n=14) Controls (n=14)
TG significantly higher in patients receiving phenothiazine than in those receiving butyrophenone. No significant differences in TC, LDL cholesterol or HDL2.
Ghaeli & Dufresne 1996
Clozapine (n=39) Typical antipsychotics (n=28)
TG was significantly higher in the clozapine group (p<0.01), no significant difference in TC.
Spivak et al. 1998 Clozapine (n=30) Typicals (n=30)
TG was significantly higher in clozapine when compared to typicals (p<0.01). No significant differences in serum TC, LDL or HDL.
Dursum et al. 1999 Clozapine (n=8) Significant increase in TG, no significant change in TC, HDL or LDL.
Gaulin et al. 1999 Clozapine (n=177) Haloperidol (n=45)
Significantly elevated TG in clozapine over baseline (p<0.01). No significant change for haloperidol in TG or TC, nor for clozapine in TC.
Ghaeli & Dufresne 1999
Clozapine switched to risperidone (n=4)
TG decreased after switching therapy from clozapine to risperidone.
Osser et al. 1999 Olanzapine (n=25) TG increased (p<0.05), TC did not increase.
Sheitman et al. 1999 Olanzapine (n=9) TG increased from 170 mg/dL to 240 mg/dL, no significant changes in TC, HDL or LDL cholesterol.

21
Table 1. Continued.
Reference Antipsychotic agent and number of patients
Results
Spivak et al. 1999 Clozapine (n=70) Typical antipsychotics (n=30)
Significant increase in TG for clozapine (p<0.005), in TC for typical antipsychotics (p<0.05).
Henderson et al. 2000
Clozapine (n=82) Significant increase in TG level (p=0.04), a non-significant increase in TC.
Melkersson et al. 2000
Olanzapine (n=14) 62% had hypertriglyceridemia and 85% had hypercholesterolemia.
Bouchard et al. 2001
Risperidone (n=22) Olanzapine (n=22)
Olanzapine-treated patients had significantly higher TG levels, a significantly higher VLDL, a trend for a higher cholesterol/HDL ratio, as well as a trend for lower HDL. TC and LDL did not differ significantly between the two groups.
Lund et al. 2001 Clozapine (n=552) Typicals (n=2461)
In patients aged 20-34 years, clozapine was associated with a significantly increased relative risk of hyperlipidemia, but not in older patients.
Kingsbury et al. 2001
Ziprasidone (n=37); Prior medications: olanzapine, 15; risperidone, 12; typical antipsychotics, 10
TC and TG decreased significantly.
Kinon et al. 2001 Olanzapine (n=573) Haloperidol (n=103)
Median non-fasting TC was significantly higher for olanzapine-treated patients than for haloperidol-treated patients (p=0.002).
Wiltfang et al. 2001 Clozapine (n=25) Healthy controls (n=104)
No significant differences in TG or TC levels between patients and controls.
Baymiller et al. 2002 Clozapine (n=50) Statistically significant changes from the baseline in TG and TC levels, no significant changes in HDL and LDL.

22
Table 1. Continued
Reference Antipsychotic agent and number of patients
Results
Meyer 2002 Risperidone (n=47) Olanzapine (n=47)
TG increased by 88 mg/dL with olanzapine and 30 mg/dL with risperidone (p=0.042), TC by 24 mg/dL with olanzapine and 7 mg/dL with risperidone (p=0.029).
Wirshing et al. 2002 Clozapine (n=39) Olanzapine (n=32) Risperidone (n=49) Quetiapine (n=13) Haloperidol (n=41) Fluphenazine (n=41)
TC decreased significantly from baseline with fluphenazine, TG increased significantly with clozapine and olanzapine, LDL with olanzapine, risperidone and quetiapine. HDL decreased significantly with olanzapine.
Koro et al. 2002 Any conventional or atypical antipsychotic exposure, altogether 1268 cases of hyperlipidemia
Olanzapine use was associated with nearly a fivefold increase in the odds of developing hyperlipidemia compared with no antipsychotic exposure and more than a threefold increase compared with those receiving conventional agents.
Atmaca et al. 2003a Quetiapine (n=14) Olanzapine (n=14) Risperidone (n=14) Clozapine (n=14) Control group (n=11)
Significant increase in fasting TG for olanzapine (+31 mg/dL, p<0.001), clozapine (+36 mg/dL, p<0.001) and quetiapine (+12 mg/dL, p<0.05), but not for risperidone (+4 mg/dL, p=0.76).
Atmaca et al. 2003b Quetiapine (n=15) Olanzapine (n=15) Haloperidol (n=15)
There was a remarkable increase in TG (p<0.05 for the olanzapine vs. quetiapine and quetiapine vs. haloperidol groups; p<0.01 for olanzapine vs. haloperidol groups) in the olanzapine group compared to quetiapine and haloperidol groups.
Kelly et al. 2003 Olanzapine (n=55) Risperidone (n=34) Clozapine (n=10) Quetiapine (n=8)
TC levels rose by 20% with clozapine, yet were essentially unchanged with the other SGAs (p=0.071). TG levels increased by 40% in patients treated with clozapine, in 6% in patients treated with olanzapine, in 48% in patients treated with quetiapine, and 15% in patients treated with risperidone. After controlling for baseline differences in TG, the endpoint values did not represent significant differences in the amount of change among groups.

23
Table 1. Continued.
Reference Antipsychotic agent and number of patients
Results
Lindenmayer et al. 2003
Clozapine (n=28) Haloperidol (n=25) Olanzapine (n=26) Risperidone (n=22)
Significant increase in TC with clozapine after 8 weeks, and with olanzapine after 8 and 14 weeks. No significant change in TC with haloperidol or risperidone.
Wen & Tan 2003 Phenothiazines (chlorpromazine, perphenazine) (n=120)
The patient group had much lower blood HDL-C and higher TG than those in the control group (p<0.01), TC levels in both groups were similar (p>0.05).
Melkersson & Dahl 2003
Clozapine (n=18) Olanzapine (n=16)
No significant differences were found in the rate of elevated blood lipids or in median lipid levels between groups. The TG levels were elevated in 8 (44%), TC in 7 (39%), LDL in 3 (17%), HDL in one patient treated with clozapine. The TG levels were elevated in 9 (56%), TC in 10 (63%), LDL in 6 (38%), HDL in one patient treated with clozapine.
Pigott et al. 2003 Aripiprazole (n=155) Placebo (n=155)
HDL increased 2 mg/dL with aripiprazole and 1 mg/dL with placebo. LDL decreased 5 mg/dL with aripiprazole and 3 mg/dL with placebo. TG changed –37 mg/dL with aripiprazole and –3 mg/dL with placebo.
Alméras et al. 2004 Olanzapine (n=42) Risperidone (n=45)
Olanzapine-treated patients had significantly higher plasma TG concentrations, lower HDL cholesterol levels and higher cholesterol/HDL cholesterol ratios.
Simpson et al. 2004 Ziprasidone (n=113)
Olanzapine (n=120) Significant increase in TC, LDL and TG for olanzapine, no significant changes for ziprasidone.
McQuade et al. 2004 Olanzapine (n=114) Aripiprazole (n=108)
Mean changes in TG were +79 mg/dL with olanzapine and 7 mg/dL with aripiprazole (p<0.05). The changes in HDL were -3.4 mg/dL with olanzapine and +3.6 mg/dL with aripiprazole (p<0.05). The differences between the changes in TC and LDL cholesterol were not statistically significant.
Paton et al. 2004 Clozapine (n=28) Olanzapine (n=41) Risperidone (n=31) Other atypical (n=7) Typical (n=27) Polypharmacy (n=24)
Those prescribed clozapine were more likely to have raised triglycerides than those prescribed other antipsychotic drugs (p=0.042). Those prescribed clozapine had a higher ratio of total cholesterol: HDL (p=0.002) than those prescribed any other antipsychotic drug(s).

24
The available evidence suggests that changes in serum lipids are concordant with changes in body weight. High-potency conventional antipsychotics (e.g., haloperidol) appear to be associated with lower risk of hyperlipidemia compared to low-potency conventional antipsychotics (e.g., chlorpromazine, thioridazine) (Meyer & Koro 2004). Among the atypical antipsychotics, clozapine and olanzapine, which produce the greatest weight gain, are associated with the greatest increases in total cholesterol, LDL cholesterol, and triglycerides and with decreased HDL cholesterol. Aripiprazole and ziprasidone, which are associated with the least amount of weight gain, do not seem to be associated with a worsening of serum lipids. Risperidone and quetiapine appear to have intermediate effects on lipids (American Diabetes Association 2004).
Most studies concerning the association between specific antipsychotics and risk for hyperlipidemia are case-control studies and outcomes research. Evidence from randomized, controlled trials is needed.
2.5 Definition and epidemiology of hypercholesterolemia
In Finland, SI units are used in determining cholesterol and triglyceride levels, but in the USA lipid levels are usually given in conventional units mg/dL. To translate SI units into U.S. values the following conversion factors were used: for converting mmol/l to mg/dL the cholesterol values were divided by 0.02586, triglycerides by 0.01129, glucose levels by 0.0555 (New Mexico AIDS InfoNet).
In the Adult Treatment Panel III (ATP III) hypercholesterolemia was determined as total cholesterol (TC) ≥ 240 mg/dL (6.2 mmol/l), hypertriglyceridemia as triglycerides (TG) ≥ 200 mg/dL (2.3 mmol/l), high low-density lipoprotein (LDL) as LDL ≥ 160 mg/dL (4.1 mmol/l) (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001). According to the recent Finnish treatment recommendation dyslipidemia is considered to be present if LDL is over 3.0 mmol/l, or if triglyceride level is over 2.0 mmol/l, or if HDL-cholesterol is low (under 1.0 mmol/l), especially TC:HDL ratio, is over 4. In Finland total cholesterol < 5.0 mmol/l and LDL-cholesterol <3.0 mmol/l is considered the target (Suomen Sisätautilääkärien Yhdistys ry:n asettama työryhmä 2004). In patients with high risk for developing a fatal cardiovascular disease event the targets are lower: TC under 4.5 mmol/l, LDL-cholesterol under 2.5 mmol/l.
According to the recent Finnish epidemiological Health 2000 study the total cholesterol was over 5.0 mmol/l in over 80% of the population, and over 6.4 mmol/l in over 30% of the population. LDL-cholesterol was ≥ 3.0 mmol/l in 85% of men and 81% of women. HDL-cholesterol was under 1.0 mmol/l in 29% of men and 11% of women. In men < 65 years, 31% had serum triglycerides over 2.0 mmol/l (Aromaa & Koskinen 2000). In the Finriski 2002 study (Vartiainen et al. 2003) the prevalences of hyperlipidemia were slightly lower than in the Health 2000 study. Total cholesterol was ≥ 5.0 mmol/l in 70% of men and women aged 25-74. In about 60% of men and 55% of women the LDL-cholesterol was over 3.0 mmol/l.

25
2.6 Definition and epidemiology of metabolic syndrome
According to Alberti et al. (1998), Impaired Glucose Tolerance (IGT) is categorized as a stage in the natural history of disordered carbohydrate metabolism. IGT is diagnosed when the result of a fasting plasma test is below 7.0 mmol/l (126 mg/dL), and in an oral glucose tolerance test the glucose concentration is ≥7.8 mmol/l (140 mg/dL) and under 11.1 mmol/l (200 mg/dL). A stage of Impaired Fasting Glycemia (IFG) is also recognized because such subjects, like those with IGT, have an increased risk of progressing to diabetes. An individual with a fasting plasma glucose concentration of 6.1 mmol/l (110 mg/dL) or greater, but less than 7.0 mmol/l was considered to have IFG. Impaired glucose regulation (IGT and IFG) refers to a metabolic state intermediate between normal glucose homeostasis and diabetes (Alberti et al. 1998). Recently the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2003) reduced the lower cut point for IFG to 5.6 mmol/l (100 mg/dL).
Even studies in the pre-neuroleptic era clearly suggested that schizophrenia might be a risk factor for the development of diabetes (Bushe & Holt 2004). Various mental disorders, e.g. depression, bipolar affective disorder and schizophrenia have been reported to be associated with increased risk of diabetes (Dixon et al. 2000, Cassidy et al. 1999, Haupt & Newcomer 2002, Newcomer 2004).
Use of second-generation antipsychotics has been reported to be associated with deterioration of therapeutic equilibrium in diabetes, especially when patients have been obese on starting treatment, or have gained weight significantly during the initial stages of treatment (Henderson et al. 2000, Sernyak et al. 2002, Haupt & Newcomer 2002, Newcomer 2004, Newcomer et al. 2002). Studies consistently show an increased risk for diabetes in patients treated with clozapine or olanzapine compared with patients not receiving treatment with first-generation antipsychotics or with other second-generation antipsychotics. The risk in patients taking risperidone and quetiapine is less clear; some studies show an increased risk for diabetes, while others do not. Relatively limited epidemiological data is available for aripiprazole and ziprasidone, but available clinical trial experience with these drugs has not shown an increased risk for diabetes (American Diabetes Association et al. 2004). Ryan and colleagues (2003) have reported results of a study concerning young, first-episode, drug-naïve patients with schizophrenia. More than 15% of the individuals had already developed impaired fasting glucose tolerance, compared to none of the matched healthy control groups. Weight gain is associated with increased insulin resistance and impairment of glucose control. Second-generation antipsychotics may also reduce insulin secretion while 5-HT-1A receptor blockade reduces the response of β-cells of the pancreas. Some second-generation antipsychotics may be also associated with insulin resistance (Melkersson et al. 2000).
For a long time there were no accepted criteria for metabolic syndrome. In 1998, the Word Health Organization (WHO) proposed a unifying definition for the syndrome and chose to call it the metabolic syndrome (Alberti et al. 1998). The following is suggested according to WHO as a working definition: glucose intolerance, impaired glucose tolerance or diabetes mellitus and/or insulin resistance together with two or more of the following other components: 1. impaired glucose regulation or diabetes. 2. Insulin

26
resistance (under hyperinsulinemic euglycemic conditions, glucose uptake below lowest quartile for background population under investigation). 3. Raised arterial pressure ≥160/90 mmHg. 4. Raised plasma triglycerides (≥1.7 mmol/l; 150 mg/dL) and/or low high density lipoprotein (HDL) -cholesterol (<0.9 mmol/l, 35 mg/dL men; <1.0 mmol/l, 39 mg/dL women). 5. Central obesity (males: waist to hip ratio >0.90; females: waist to hip ratio >0.85) and/or BMI >30 kg/m2. 6. Microalbuminuria (urinary albumin excretion rate ≥20 µg/min or albumin: creatine ratio ≥20 mg/g). Although microalbuminuria predicts clinical nephropathy and death in patients with diabetes (Dinneen & Gerstein 1997), the inclusion of microalbuminuria as a core component has been criticized. In contrast to the NCEP definition (see below), however, the WHO definition cannot be readily applied clinically (Laaksonen et al. 2004a).
In 2001 the Adult Treatment Panel III (ATP III) guidelines from the U.S. National Heart, Lung, and Blood Institute described the metabolic syndrome as consisting of three or more of the following conditions: abdominal obesity (waist circumference) men >102 cm, women >88 cm, triglycerides ≥150 mg/dL (1.7 mmol/l), high-density lipoprotein cholesterol men <40 mg/dL (1.0 mmol/l), women <50 mg/dL (1.3 mmol/l), blood pressure ≥130/85 mmHg, fasting glucose ≥110 mg/dL (6.1 mmol/l) (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001). Despite the differences in the definitions, the ATP III and WHO definitions identify the same individuals about 85% of the time (Ford & Giles 2003).
In the Botnia study the prevalence of metabolic syndrome in Finland and Sweden was estimated using the definition of the World Health Organization. A prevalence of 10% in women and 15% in men was found in subjects with normal glucose tolerance. The prevalence rose to 42% (women) and 64% (men) in those with impaired fasting glucose/impaired glucose tolerance, and 78% (women) and 84% (men) in those with type 2 diabetes mellitus (Isomaa et al. 2001). In the Kuopio Ischemic Heart Disease Risk Factor Study the prevalence of metabolic syndrome in adult men with diabetes or cardiovascular disease excluded, ranged from 8.8 to 14.3%, depending on the definition (Lakka et al. 2002). In Unites States, the ATP III definition of the metabolic syndrome affects approximately 22% of US adults (Ford et al. 2002).
2.8 Pathogenesis of metabolic syndrome
The pathogenesis of metabolic syndrome is poorly understood. Visceral intra-abdominal fat is closely linked to insulin resistance. Even in normal-weight subjects increased waist circumference is associated with increased risk for diabetes, dyslipidemia, hypertension, and cardiovascular disease because of excess abdominal fat (National Heart, Lung, and Blood Institute 2001). Abdominal obesity and ectopic fat deposition in the liver, pancreas and skeletal muscle seem particularly deleterious. Triglyceride accumulation in the liver may decrease hepatic insulin sensitivity and contribute to dyslipidemia. Hepatic insulin resistance also results in inappropriate fasting and postprandial gluconeogenesis. Intramuscular lipid deposits may contribute to decreased glucose uptake in skeletal muscle (Laaksonen et al. 2004a).

27
Adipose tissue is a major endocrine organ secreting many substances that may play a critical role in the pathogenesis of the metabolic syndrome. The hypothalamic-adrenal-pituitary axis and sex steroid metabolism may also contribute (Laaksonen et al. 2004a).
Chronic inflammation has been hypothesized to be a common antecedent for the metabolic syndrome. Inflammation appears to be associated with each of the components of the metabolic syndrome, and C-reactive protein levels have been found to increase with an increasing number of components of the metabolic syndrome (Festa et al. 2000, Ridker et al. 1997). In addition, low-grade inflammation has been associated with increased risk of the metabolic syndrome (Laaksonen et al. 2004b). Low-grade inflammation may predispose to the development of metabolic syndrome by several mechanisms. However, some of the risk is mediated through obesity and factors related to insulin resistance (Laaksonen et al. 2004b).
Environmental factors including a sedentary lifestyle and poor physical fitness, a diet rich in saturated fat and low in fiber, low socioeconomic status, low birth weight and rapid childhood growth as well as genetic factors contribute both to the development of overweight and the propensity for insulin resistance and ectopic fat deposition and other manifestations of the metabolic syndrome (Laaksonen et al. 2004a).
2.7 Schizophrenia, hypercholesterolemia and metabolic syndrome: how are they linked together?
Individuals with schizophrenia are as obese as or more obese than individuals without schizophrenia (Allison et al. 1999b). As described earlier, antipsychotics are associated with weight gain and elevated lipid and glucose values. Obesity and weight gain have been associated with type II diabetes (National Institute of Health 1998), hypercholesterolemia and hypertriglyceridemia (Janssen et al. 2002). Hypercholesterolemia is a well-known risk factor for coronary heart disease. The effect of high plasma TG concentration on atherosclerosis and its complications is more controversial than the effect of TC. However, a gradient of risk of ischemic heart disease is associated with increasing TG levels, also after controlling for the other major risk factors of ischemic heart disease (Jeppesen et al. 1998). Consequently, hyperlipidemia can have a negative effect on the prognosis of somatic health in a patient with schizophrenia. The prognosis is often further adversely affected by other factors prejudicial to health, such as smoking and poor dietary habits (Brown et al. 2000, Patten 2001). In addition, recently Heiskanen et al. (2003) reported a 2-to-4-fold higher prevalence of metabolic syndrome in long-term schizophrenia outpatients than was previously found in the same area in both men and women.
In addition to suicides and accidental deaths, the standardized mortality ratios (SMR) for diseases of the circulatory, digestive, nervous and respiratory systems are higher than expected in subjects with schizophrenia (Brown et al. 2000). In the case of circulatory disease this may be due to adverse metabolic disturbances in psychotic disorders (Fontaine et al. 2001). These metabolic disturbances could be followed based on the current recommendations (Table 2). There were no general population-based reports

28
studying lipid levels in subjects with schizophrenia; neither did we find any general population- based reports concerning lipid levels in subjects using antipsychotic medication. There were no reports available concerning the duration of schizophrenia and serum triglyceride levels either, or reporting the prevalence of metabolic syndrome in schizophrenia in a general population-based sample.

Tabl
e 2.
Cur
rent
rec
omm
enda
tions
of
mon
itori
ng m
etab
olic
side
effe
cts i
n pa
tient
s with
schi
zoph
reni
a/ a
typi
cal a
ntip
sych
otic
s. R
ecom
men
datio
n (y
ear)
Pe
rson
al/
fam
ily
hist
ory
Wei
ght
Wai
st
circ
umfe
renc
e B
lood
pr
essu
re
Fast
ing
plas
ma
gluc
ose
Fast
ing
lipid
pr
ofile
B
ody
Mas
s In
dex
Seru
m
insu
lin
Am
eric
an D
iabe
tes
Ass
ocia
tion
et a
l. (2
004)
Bas
elin
e
and
annu
ally
Bas
elin
e an
d 4,
8
and
12 w
eeks
af
ter i
nitia
ting
or c
hang
ing
SGA
1) th
erap
y an
d qu
arte
rly
ther
eafte
r
Bas
elin
e an
d an
nual
ly
Bas
elin
e, 3
m
onth
s afte
r an
d an
nual
ly
Bas
elin
e, 3
mon
ths a
fter
and
annu
ally
Bas
elin
e, 3
m
onth
s afte
r an
d ev
ery
5 ye
ars
...2)
...
Lehm
an e
t al.
(200
4)
...
See
BM
I ...
B
asel
ine
with
pu
lse
and
tem
pera
ture
. Th
erea
fter a
s cl
inic
ally
in
dica
ted.
Bas
elin
e an
d fa
stin
g pl
asm
a gl
ucos
e or
he
mog
lobi
n A
1c a
t 4
mon
ths a
nd a
nnua
lly
Bas
elin
e an
d at
le
ast e
very
5
year
s
Bas
elin
e,
ever
y vi
sit f
or
6 m
onth
s and
at
leas
t qu
arte
rly
...
Mar
der e
t al.
(200
4)
...
See
BM
I ...
...
B
asel
ine
fast
ing
plas
ma
gluc
ose
leve
l or
hem
oglo
bin
A1c
and
ye
arly
/with
pat
ient
s with
si
gnifi
cant
risk
fact
ors
for d
iabe
tes a
nd th
ose
who
are
gai
ning
wei
ght
also
at 4
mon
ths
Ever
y 2
year
s or
mor
e of
ten
if lip
id le
vels
are
in
the
norm
al
rang
e; e
very
6
mon
ths i
f the
LD
L le
vel i
s >3
.4 m
mol
/l
Bas
elin
e, a
t ev
ery
visi
t for
6
mon
ths a
nd
quar
terly
...

Tabl
e 2.
Con
tinue
d.
R
ecom
men
datio
n (y
ear)
Pe
rson
al/
fam
ily
hist
ory
Wei
ght
Wai
st
circ
umfe
renc
e B
lood
pr
essu
re
Fast
ing
plas
ma
gluc
ose
Fast
ing
lipid
pr
ofile
B
ody
Mas
s In
dex
Seru
m
insu
lin
Cas
ey e
t al.
(200
4)
Bas
elin
e B
asel
ine
and
at
ever
y vi
sit
Bas
elin
e an
d at
eve
ry v
isit
Bas
elin
e an
d at
eve
ry v
isit
Bas
elin
e fa
stin
g,
post
pran
dial
or p
ostlo
ad
plas
ma
gluc
ose
leve
l and
at
leas
t yea
rly
Bas
elin
e an
d at
le
ast y
early
Bas
elin
e an
d at
eve
ry v
isit
...
Mel
kers
son
& D
ahl3
(200
4)
...
Bas
elin
e an
d th
en a
t reg
ular
in
terv
als
...
...
Bas
elin
e an
d th
en a
t re
gula
r int
erva
ls
Bas
elin
e an
d th
en a
t reg
ular
in
terv
als
...
At
base
line
and
then
at
regu
lar
inte
rval
s 1 SG
A=
seco
nd-g
ener
atio
n an
tipsy
chot
ics =
aty
pica
l ant
ipsy
chot
ics
2 da
ta n
ot g
iven
3 co
ncer
ning
pat
ient
s who
are
goi
ng to
be,
or a
re a
lread
y, tr
eate
d w
ith c
loza
pine
, ola
nzap
ine
or z
otep
ine,
and
pos
sibl
y qu
etia
pine

3 Aims of the present study
The general purpose of the present study was to investigate specific metabolic disorders in schizophrenia. The numbers I-V hereafter refer to the original publications. The detailed aims of the present study were: 1. To review weight gain and glucose and lipid metabolism disturbances during antipsychotic medication (I). 2. To investigate serum lipids in schizophrenia and other functional psychoses (II). 3. To investigate serum triglyceride levels in early onset schizophrenia (III). 4. To investigate hyperlipidemia in subjects using antipsychotic medication (IV). 5. To investigate the prevalence of metabolic syndrome in patients with schizophrenia (V).

4 Material and methods
4.1 Material and methods for the review
Publications concerning weight gain and glucose and lipid metabolism disturbances during antipsychotic medication were sought using the Medline database (from 1966 to 2002). The search terms were “antipsychotic medication”, “weight”, “glucose”, “hyperglycemia”, “hyperlipidemia”, “diabetes mellitus”. Additional relevant papers were obtained from the bibliographies of articles retrieved through the Medline search.
4.2 Study population and data collection
The study population in this study was a subsample of the Northern Finland 1966 Birth Cohort originally assembled by Professor (emerita) Paula Rantakallio. She aimed to describe and analyze the risk factors for perinatal deaths and low birth weight. This cohort is based on the unselected general population: In the provinces of Oulu and Lapland, 96% of all women (n=12,068) with an expected delivery date in 1966 were evaluated. They gave birth to 12,058 liveborn infants. Data on biological, socio-economic and health conditions, living habits and family characteristics of the cohort members have been collected prospectively from pre-natal stages up to the age of 31 (Rantakallio 1969, 1988, Rantakallio et al. 1995, 1997). Three main follow-up surveys have been conducted: the first at age one, the second at age 14 (Rantakallio 1988, Järvelin et al. 1997), and the third in 1997-98, at the age of 31 (Sorri & Järvelin 1998). In this 31-year follow-up survey, postal questionnaires were sent to 11,541 cohort members, and the response rate was 75.3%. All cohort members living in Northern Finland or in the capital area (Helsinki) were invited to a clinical examination. Of those invited, 5,654 subjects (67%) participated in the present study and gave written informed consent.
The national Finnish Hospital Discharge Register (FHDR) covers all general and mental hospitals. Its coverage and validity have been shown to be acceptable (Poikolainen 1983). Diagnoses in the FHDR during the period 1969-1986 were coded

33
with the ICD-8 classification, in 1987-1995 with the ICD-9 along with DSM-III-R criteria (Kuoppasalmi et al. 1989), and since January 1st 1996 according to the ICD-10. All cohort members over 16 years appearing in the FHDR up until the end of 1997 with a FHDR diagnosis number 290-309 or 790.20 (ICD-8), 290-316 (ICD-9), or F00-F69 or F99 (ICD-10) were selected. All diagnoses were scrutinized and validated for the DSM-III-R criteria (Isohanni et al. 1997, Moilanen et al. 2003). Since non-fasting lipid values differ significantly from fasting values (Folsom et al. 1983), only fasting values were accepted.
In order to study the differences between schizophrenia and other psychotic disorders, non-psychotic disorders and the comparison group, the subjects were divided into four groups according to their diagnosis (original study II / V): 1. Schizophrenia, defined as having at any time met DSM-III-R criteria for schizophrenia (n=31/31). 2. Other psychoses, meaning all functional psychoses except DSM-III-R schizophrenia (n=21/22). 3. Non-psychotic disorders (n=104/105). 4. No psychiatric hospital treatment (n=5,498/5,455). This group represented the unaffected population and served as the comparison group.

34
The Northern Finland 1966 Birth Cohort12 058 liveborn children
Hospital diagnoses
Finnish Hospital Discharge Register (FHDR)Covering years 1982-1997
31-year follow-up
Postal questionnaire11541 sent, 8767 answered
Clinical examination 8463 invited, 6033 participated
Smoking Alcohol consumption Physical activity Medication
Blood samples Weight Height Waist circumference Blood pressure
Schizophrenia (n=100) Other psychoses (n=55) Non-psychotic disorders (n=315) No psychiatric hospital treatment (n=10464)
Schizophrenia (n=31*) Other psychoses (n=21*) Non-psychotic disorders (n=104*) No psychiatric hospital treatment (n=5498*)
*participants with non-fasted blood samples excluded
Fig. 1. The flowchart of the data collection procedure in the Northern Finland 1966 Birth Cohort Study and the main data used in the original publications II-V.

35
The participants were asked to fast overnight before coming to clinical examination, where their weight, height, waist circumference and blood pressure were measured, Body Mass Index (BMI) was calculated and blood samples were taken. Waist circumference was measured at the level midway between the lowest rib margin and the iliac crest. In men waist circumference 100 cm and under was defined as normal, over 100 cm as obese, and in women 90 cm was defined as cut-off point. Diet was taken to be unhealthy when it included daily or almost daily consumption of sausages, and consumption of rye bread or crisp bread, fresh vegetables and salads, berries or fruit twice a week or less often, one point being assigned to each of these counts, so that a sum of four to five points indicated an unhealthy diet and three or less a healthy diet (Laitinen et al. 2004).
Subjects were considered smokers if they reported smoking at least occasionally, even if irregularly. Questions on alcohol use measured the average frequency of consumption of beer, wine and spirits during the last year, and the usual amount of each consumed on one occasion. The amount of alcohol consumed per day was calculated, and the validity of questions was ascertained (Laitinen et al. 2004). Subjects were thereby divided into light (≤15 grams per day) and moderate (>15 grams per day) drinkers. Physical activity was recoded into two categories (regular vs. non-regular). Regular physical activity was regarded as consisting of exercise at least two times per week that makes the person become breathless and sweat at least mildly.
The participants also completed a questionnaire including questions of medication. In cases of incomplete answers, psychiatric medication at the time of blood sampling was identified by referring to case records. Doses of antipsychotic medication were converted to chlorpromazine (CPZ) equivalent daily doses according to the Schizophrenia Patient Outcomes Research Team (PORT) Treatment Recommendations (Lehman & Steinwachs 1998). Because these recommendations did not include CPZ equivalents of zuclopenthixol, the equivalent of 100 mg CPZ to zuclopenthixol 25 mg per os/day and 100 mg/week depot was used (Bazire 1999).
In order to study serum triglyceride levels in early onset schizophrenia the subjects with schizophrenia were divided into two groups: 1) subjects who were ≤ 20 years old at the onset of schizophrenia, and 2) subjects with later onset (original study III).
In order to study the lipid concentrations and the risk of hyperlipidemia in subjects using antipsychotic medication the subjects were divided into four groups according to the used medication: 1) atypical medication, 2) typical medication, 3) atypical and typical medication, 4) no antipsychotic medication (original study IV). Hypercholesterolemia was determined as TC ≥ 240 mg/dL (6.2 mmol/l), hypertriglyceridemia as TG ≥ 200 mg/dL (2.3 mmol/l), high LDL as LDL ≥ 160 mg/dL (4.1 mmol/l) (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001).
To investigate the prevalence of metabolic syndrome in schizophrenia the subjects were divided into four groups according to their diagnosis (original study V) in the same way as in original study II. The subjects were assessed for the presence of metabolic syndrome according to the criteria of the ATP III (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001)

36
4.3 Outcome measures, selected covariates and measure procedures
Main outcome measures for the original study II were serum total cholesterol (TC), high density lipoprotein (HDL), low density lipoprotein (LDL), triglycerides (TG) and glucose. Selected covariates were sex, overweight, smoking and alcohol consumption. For original study III the main outcome measure was serum triglycerides.
Main outcome measures for original study IV were TC, HDL, LDL, TG and the prevalence of hyperlipidemia. Selected covariates were sex, BMI, diet, physical exercise, smoking and alcohol consumption. For study number V the main outcome measure was metabolic syndrome, and the selected covariate was sex.
4.4 Statistical methods
In original study II, a Chi-Square test was used in the analysis for categorical variables. Analysis of variance (ANOVA) adjusting for sex, body mass index (BMI), alcohol consumption and smoking was used to compare serum lipid variables between the diagnostic categories. TG was transformed to the natural logarithm to reduce skewness of the distribution. The non-parametric Kruskal-Wallis test was used in the analysis for glucose, and the Mann-Whitney U test in the analysis of clinical course variables (days in hospital after diagnoses, proportion of time spent in hospital after diagnoses, number of treatment episodes in hospital after diagnoses and age at onset). Two-tailed significance levels were used for all comparisons. All the statistical analyses were performed using the SAS software (version 8e) for Windows.
In original study III, the Mann-Whitney U-test was used to study the difference between subjects who were ≤20 years old at the beginning of schizophrenia compared to patients with later onset or non-hospitalized controls. The Pearson correlation coefficient was used to study the correlation between the age at onset and the level of serum triglycerides.
In original study IV, because data were non-normally distributed, all comparisons were made by using nonparametric test. The significance of differences in serum lipid levels between the study groups according to antipsychotic medication was tested with non-parametric one way Kruskal-Wallis analysis of variance and pairwise comparisons with Mann-Whitney U-test. The Pearson Chi-Square test was used to test the statistical significance between antipsychotic medication and hyperlipidemia. The multiple logistic regression analysis with adjustment of waist circumference (>100 for male, >90 for female/normal), diet (unhealthy diet: yes/no), smoking (yes/no), alcohol consumptions (moderate/light drinkers) and physical activity (yes/no). The results were shown in odds ratios (OR) with 95% confidence intervals (95% CI). The statistical analyses were performed using SAS system version 8.2 for Windows.
In original study V, the significance of differences in proportions was analyzed with Fisher’s exact test and differences in continuous variables using the Mann-Whitney U test. Logistic regression analysis was used to estimate the risk for metabolic syndrome between study groups.

37
4.5 Ethical considerations
Permission for gathering data for the entire Cohort was obtained from the ministry of Social Welfare and health Affairs in 1993. The Ethics Committee of the University Hospital of Oulu keeps the study design of the Northern Finland 1966 Birth Cohort under review. The research plan for the Northern Finland 1966 Birth Cohort 31-year follow-up study was accepted by the Ethical Committee of Oulu University, Faculty of Medicine on 17 June 1996. Informed consent was obtained from all participants.
4.6 Personal involvement
The author of this thesis has participated in the Northern Finland 1966 Birth Cohort Project as a researcher since 2000. The author has been accorded permission to use the data, and has made a substantial contribution towards the conception and design of this study and interpretation of the data and some statistical analysis. As first author, the author has drafted the main content of original studies number II-V, made a substantial contribution for study I, as well as reviewed and revised them for intellectual content.

5 Results
5.1 Weight gain and glucose and lipid metabolism disturbances during antipsychotic medication (I)
As a result of our review we concluded that disadvantages associated with the use of medication should be minimized e.g. by appropriate monitoring and by documenting in patient charts the effects of regular antipsychotic medication on patient’s weight and metabolism.
As far as we know, in 2002 there were no established consensus guidelines for follow-up, prevention and treatment of the adverse effects of antipsychotic drugs on glucose and lipid metabolism. We recommended monitoring and documenting in patient charts the effects of antipsychotic medication on patient’s weight and metabolism (Koponen et al. 2002). We recommended monitoring weight and body mass index or waist circumference and blood pressure during every visit. We also recommended determination of blood glucose, triglyceride, cholesterol and prolactin levels once or twice a year, or more often (e.g. every three months) in high-risk patients. Furthermore, we recommended that the patient should keep a food record in case of weight gain of more than 4 kg since the beginning of treatment. In case of a weight increase of over 7% compared to the weight when starting treatment a consultation with a dietician or nutritionist, caloric restriction and more effective physical exercise should be carried out.
5.2 Serum lipids in schizophrenia and other functional psychoses (II)
In the schizophrenia group (n=31) 16 had conventional medication, mean dosage 452 CPZ equivalents. Five subjects had atypical antipsychotic medication, mean dosage 725 CPZ equivalents per day. Five subjects had both atypical and conventional medication, mean dosage 580 CPZ equivalents. The mean daily dosage of antipsychotic medication with schizophrenia was 440 CPZ equivalents. We were able to identify the medicine in

39
use but not the precise dose in 5 out of these 26 persons in the schizophrenia group. Five persons did not report using any neuroleptic medication.
In the group of other psychoses (n=21) 5 subjects had conventional medication, mean daily dosage 119 CPZ equivalents. One subject had atypical medication. The mean dosage of antipsychotic medication with other psychoses was 133 CPZ equivalents. Fifteen out of 21 subjects did not report using any antipsychotic medication. None of the subjects using antipsychotic medication reported taking any lipid-lowering medication.
Of all 8,463 invited subjects 5,983 (71%) participated in the field study. The rates of non-participants in different diagnostic categories were as follows: 51% in the schizophrenia group, 46% in the group of other psychoses, 48% in the group of non-psychotic disorders and 31% in the comparison group.
In order to evaluate possible selection bias in the groups with psychiatric hospital treatment we compared several clinical course variables between participants and non-participants: 1) days in hospital after diagnoses, 2) proportion of time spent in hospital after diagnoses, 3) number of treatment episodes in hospital after diagnoses, and 4) age at onset. We found no major differences between non-participants and participants, except in the schizophrenia group for days in hospital after diagnoses (median 381 days vs. 163 days, respectively; p=0.078) and proportion of time spent in hospital after diagnoses (median 0.11 vs. 0.06; p=0.059), and in the group of other psychoses for the same variables (median 69 vs. 43; p<0.01, and median 0.03 vs. 0.03, respectively; p=0.01).
Mean TC (5.5 mmol/l) and TG (1.5 mmol/l) were significantly higher in the schizophrenia group than in the comparison group (5.1 mmol/l and 1.2 mmol/l, respectively) (Table 3a and Table 3b). Mean TC (5.5 mmol/l) and TG (1.4 mmol/l) in the group of other functional psychoses were similar to the schizophrenia group, and TC and TG levels in hospital treated non-psychotic disorders (mean 5.0 mmol/l and 1.3 mmol/l, respectively) were similar to the comparison group. No statistically significant differences were found in glucose levels between groups.

Tabl
e 3a
. Se
rum
tot
al c
hole
ster
ol,
HD
L an
d LD
L ch
oles
tero
l an
d tr
igly
ceri
des
in s
chiz
ophr
enia
, ot
her
func
tiona
l ps
ycho
ses,
non-
psyc
hotic
dis
orde
rs a
nd th
e co
mpa
riso
n gr
oup.
Schi
zoph
reni
a (n
=31)
O
ther
func
tiona
l psy
chos
es
(n=2
1)
Non
-psy
chot
ic d
isor
ders
(n
=104
) C
ompa
rison
gro
up
(n=5
,498
)
M
ean
(mm
ol/l)
Sd
M
ean
(mm
ol/l)
Sd
M
ean
(mm
ol/l)
Sd
M
ean
(mm
ol/l)
Sd
Tota
l cho
lest
erol
5.
5 0.
87
5.5
0.67
5.
0 1.
0 5.
1 1.
0 H
DL
chol
este
rol
1.4
0.40
1.
5 0.
33
1.5
0.39
1.
6 0.
38
LDL
chol
este
rol
3.4
0.79
3.
4 0.
68
3.0
0.93
3.
0 0.
89
Trig
lyce
rides
1.
51
1.4
1.
3
1.2
1 ge
omet
ric m
ean
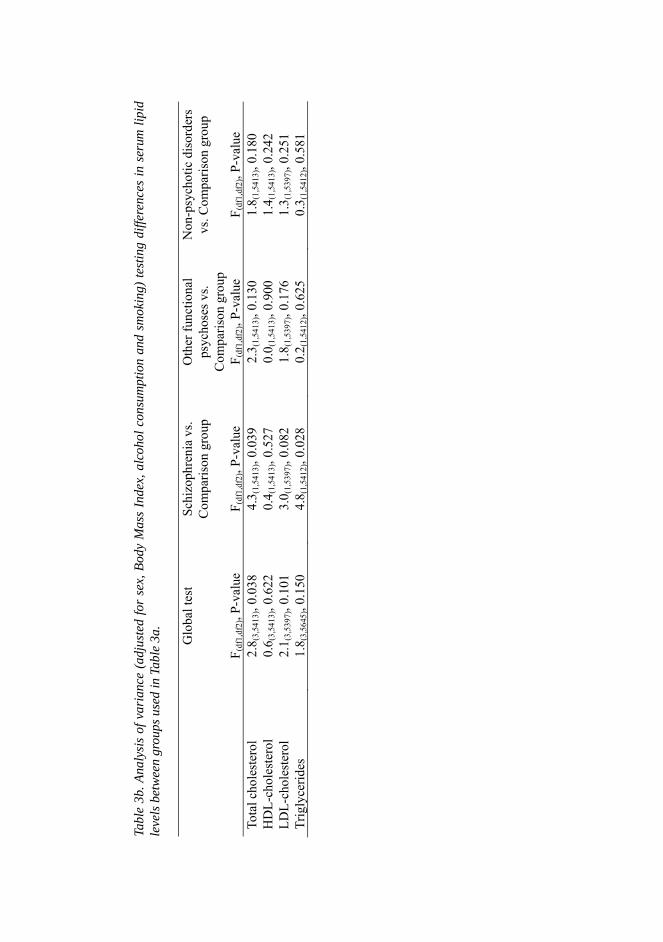
Tabl
e 3b
. Ana
lysi
s of
var
ianc
e (a
djus
ted
for
sex,
Bod
y M
ass
Inde
x, a
lcoh
ol c
onsu
mpt
ion
and
smok
ing)
test
ing
diffe
renc
es in
ser
um li
pid
leve
ls b
etw
een
grou
ps u
sed
in T
able
3a.
Glo
bal t
est
Schi
zoph
reni
a vs
. C
ompa
rison
gro
up
Oth
er fu
nctio
nal
psyc
hose
s vs.
Com
paris
on g
roup
Non
-psy
chot
ic d
isor
ders
vs
. Com
paris
on g
roup
F (
df1,
df2)
, P-v
alue
F (
df1,
df2)
, P-v
alue
F (
df1,
df2)
, P-v
alue
F (
df1,
df2)
, P-v
alue
To
tal c
hole
ster
ol
2.8 (
3,54
13),
0.03
8 4.
3 (1,
5413
), 0.
039
2.3 (
1,54
13),
0.13
0 1.
8 (1,
5413
), 0.
180
HD
L-ch
oles
tero
l 0.
6 (3,
5413
), 0.
622
0.4 (
1,54
13),
0.52
7 0.
0 (1,
5413
), 0.
900
1.4 (
1,54
13),
0.24
2 LD
L-ch
oles
tero
l 2.
1 (3,
5397
), 0.
101
3.0 (
1,53
97),
0.08
2 1.
8 (1,
5397
), 0.
176
1.3 (
1,53
97),
0.25
1 Tr
igly
cerid
es
1.8 (
3,56
45),
0.15
0 4.
8 (1,
5412
), 0.
028
0.2 (
1,54
12),
0.62
5 0.
3 (1,
5412
), 0.
581

42
The proportions of sex, overweight study subjects, light/moderate alcohol consumption, and smokers are presented in Table 4. Chi-Square test was used for analyzing potential confounding factors. Subjects with schizophrenia were more often overweight (58%) than subjects in the comparison group (40%). Subjects with schizophrenia were less often moderate drinkers (10% vs. 19%), and more persons with schizophrenia smoked (45% vs. 29%) than did those in the comparison group. All of these differences were statistically significant (p<0.01).

43
Table 4. Gender, body mass index, alcohol consumption and smoking in schizophrenia, other psychoses, non-psychotic disorders and comparison group.
Schizophrenia
Other psychoses
Non-psychotic disorders
Comparison group
(n=31) (n=21) (n=104) (n=5498) N % N % N % N % Male 18 58 11 52 66 63 2583 47 Female 13 42 10 48 38 37 2915 53 BMI Normal (<25) 13 42 9 43 51 50 3292 60 Overweight (≥25 <30)
14 45 10 48 38 37 1672 31
Obese (≥30) 4 13 2 10 14 14 497 9 Alcohol consumption
Light (≤15g/day)
27 90 15 75 65 66 4313 81
Moderate (>15g/day)
3 10 5 25 34 34 1014 19
Smoking No 17 55 12 71 52 50 3842 71 Yes 14 45 9 29 52 50 1562 29
In the schizophrenia group those who had both atypical and typical antipsychotic
medication had the highest TC (Figure 2) (median 6.3 mmol/l) and TG (Figure 3) (median 1.7 mmol/l). Their median glucose level was 5.4 mmol/l. In schizophrenia subjects without any antipsychotic medication TC (median 5.1 mmol/l), TG (median 1.2 mmol/l) and glucose (median 5.1 mmol/l) were lower than in subjects using antipsychotic medication. The highest glucose level was in the group with atypical medication (median 5.4 mmol/l). However, none of the above-mentioned differences were statistically significant.

44
3
53
103
153
203
253
303
Tota
l cho
lest
erol
mg/
dl
Atypical Typical Atypical & Typical
No anti-psychotics
Fig. 2. Serum total cholesterol of subjects with schizophrenia according to type of medication.
0
50
100
150
200
250
300
350
Trig
lyce
rides
mg/
dl
Atypical Typical Atypical &
TypicalNo anti-
psychotics
Fig. 3. Serum triglycerides of subjects with schizophrenia according to type of medication.

45
5.3 Serum triglycerides in early onset schizophrenia (III)
We found higher triglyceride levels in subjects who were ≤ 20 years old at the beginning of schizophrenia (mean ± S.D. 1.7 mmol/l ± 0,7; n=17) as compared to patients with later onset (1.4 mmol/l ± 0.9; n=14) or non-hospitalized controls (1.2 mmol/l ± 0.7; n= 5453). The Mann-Whitney U-test showed a significant difference between the first and third group (p<0.01), and the Pearson correlation coefficient showed a negative correlation between the age at onset and the level of serum triglycerides (r=-0.35, p=0.05) (Figure 4).
Fig. 4. Serum triglyceride levels according to age at onset of schizophrenia.

46
5.4 Hyperlipidemia in subjects using antipsychotic medication (IV)
Forty-five subjects reported using antipsychotic medication (58% having DSM-III-R diagnosis of schizophrenia, 13% other psychosis, and 29% without hospital treated diagnosis of psychosis), while 5,609 did not. Out of these 45 subjects 6 (13%) had atypical, 32 (71%) typical and 7 (16%) both atypical and typical antipsychotic medication. In all, 5,609 subjects had no antipsychotic medication.
We found high lipid levels in persons with both atypical and typical medication (mean TC 6.0 mmol/l, TG 1.8 mmol/l). Mean TC and TG were also high in the subjects with only typical medication (5.6 mmol/l and 1.7 mmol/l, respectively) (Table 5).

Tabl
e 5.
Ser
um to
tal c
hole
ster
ol, H
DL
and
LDL
chol
este
rol a
nd tr
igly
ceri
des a
ccor
ding
to a
ntip
sych
otic
med
icat
ion.
Aty
pica
l (n=
6)1)
Typi
cal (
n=32
) 2)
Aty
pica
l and
ty
pica
l (n=
7) 3
)
No
antip
sych
otic
m
edic
atio
n (n
=5,6
09)
Aty
pica
l m
edic
atio
n vs
. no
med
icat
ion
grou
p
Typi
cal
med
icat
ion
vs.
no m
edic
atio
n
grou
p
Aty
pica
l and
ty
pica
l m
edic
atio
n vs
. no
med
icat
ion
grou
p
Med
ian
4)
Mea
n
Med
ian
Mea
n
Med
ian
Mea
n M
edia
n M
ean
p-va
lue
p-va
lue
p-va
lue
Tota
l cho
lest
erol
5.
5 5.
3 5.
5 5.
6 6.
2
6.0
5.0
5.1
0.30
66
0.00
71
0.02
34
HD
L ch
oles
tero
l 1.
5 1.
4 1.
4 1.
4 1.
5
1.6
1.5
1.6
0.62
87
0.00
54
0.89
14
LDL
chol
este
rol
3.4
3.3
3.2
3.4
3.8
3.6
2.2
2.7
0.32
26
0.00
64
0.10
16
Trig
lyce
rides
1.
2 1.
3 1.
4 1.
7 2.
1 1.
8 1.
0 1.
2 0.
4300
0.
0039
0.
0103
1) in
clud
ing
4 cl
ozap
ine,
and
2 ri
sper
idol
2)
inc
l. 7
thio
ridaz
ine,
7 p
erfe
nazi
ne,
4 ha
lope
ridol
, 3
chlo
rpro
tixhe
ne,
2 zu
clop
hent
ixol
, 1
peric
yazi
ne,
1 ch
lorp
rom
azin
e, 1
lev
omep
rom
azin
e, 1
ha
lope
ridol
and
thi
orid
azin
e, 1
per
fena
zine
and
chl
orpr
omaz
ine,
2 p
erfe
nazi
ne a
nd t
hior
idaz
ine,
1 h
alop
erid
ol a
nd t
hior
idaz
ine
and
flufe
nazi
ne,
1 su
lpiri
de, z
uclo
phen
tixol
and
levo
mep
rom
azin
e 3)
incl
. 1 h
ad c
loza
pine
and
hal
oper
idol
, 1 ri
sper
idol
and
thio
ridaz
ine,
1 c
loza
pine
and
thio
ridaz
ine,
one
risp
erid
ol a
nd c
hlor
prot
hixe
ne, 1
clo
zapi
ne a
nd
thio
ridaz
ine,
1 o
lanz
apin
e an
d ch
lorp
rom
azin
e, 1
risp
erid
ol a
nd c
hlor
prom
azin
e 4)
cho
lest
erol
and
trig
lyce
ride
valu
es g
iven
in m
mol
/l

48
Persons using antipsychotic medication had higher prevalences of hypercholesterolemia (31.1%) and hypertriglyceridemia (22.2%) than those without such medication (12.2% and 7.0%, respectively, p<0.001, p<0.001). In addition, high LDL cholesterol was more prevalent in subjects using antipsychotic medication (20.0%) than in non-users (10.2%, p=0.03). (Figure 5)
*p < 0.001
12,210,2
7,0
31,1
20,022,2
0
5
10
15
20
25
30
35
Hypercholesterolemia * High LDL-cholesterol ** Hypertriglyceridemia *
%
No antipsychotic medicationAntipsychotic medication
**p = 0.03 Abbreviation: LDL = low-density lipoprotein
Fig. 5. Prevalence of hypercholesterolemia, high LDL cholesterol and hypertriglyceridemia in subjects who used antipsychotic medication and in those who did not.
In subjects with antipsychotic medication, the proportions of those with an unhealthy diet did not differ from the subjects without such medication: in both groups 12% of the subjects had an unhealthy diet. Subjects with antipsychotic medication exercised less than subjects without such medication: 43% of subjects without antipsychotic medication and 30% of subjects with such medication exercised at least two times per week (p=0.07).
After adjusting for sex, diet, waist circumference, physical exercise, smoking and alcohol consumption for hyperlipidemia, the results of logistic regression analysis showed that in persons with antipsychotic medication the risk of hypercholesterolemia was 2.8 (95% CI 1.4-5.6), of hypertriglyceridemia 2.3 (95% CI 1.0-5.4), and that of high LDL cholesterol 1.6 (95% CI 0.7-3.5).

49
5.5 Metabolic syndrome in schizophrenia (V)
Of all 8,463 invited subjects 5,613 (66%) were included in the present study. The rates of non-participants in different diagnostic categories were as follows: 58% in the schizophrenia group, 52% in the group of other psychoses, 53% in the group of non-psychotic disorders and 32% in the comparison group. In order to evaluate possible selection bias in the groups we compared sex, age at onset, days at hospital and the number of hospital treatment episodes between participants and non-participants. In the non-psychotic disorders group and the comparison group, women participated more often (p=0.012 and p=0.000, respectively, Chi-Square Test). There were no other statistically significant differences between the participants and non-participants.
The prevalence of metabolic syndrome was 19% in schizophrenia (p=0.01 vs. comparison group), 5% in other psychoses, 9% in non-psychotic disorders and 6% in the comparison group (Table 6). After adjusting for sex the results of logistic regression analysis showed that the risk of metabolic syndrome was 3.7 (95% CI 1.5-9.0) in schizophrenia. Table 6. The frequency of metabolic syndrome in diagnostic groups.
Metabolic syndrome Diagnostic category Yes % (n) No% (n) p-value1
Schizophrenia (n=31)a 19.4 (6) 80.6 (25) 0.010
Other psychoses (n=22)b 4.5 (1) 95.5 (21) 1.000
Non-psychotic disorders (n=105)
8.6 (9) 91.4 (96) 0.295
Comparison group (n=5,455) 6.0 (326) 94.0 (5129) 1Fisher’s exact test testing the difference between each group and comparison group aMedications were as follows: clozapine, n=4; risperidone, n=1; thioridazine, n=4; perphenazine, n=2; haloperidol, n=3; chlorprothixene n=1; zuclopenthixol, n=1; chlorpromazine, n=1, clozapine and haloperidol, n=1; clozapine and thioridazine, n=2; risperidone and thioridazine, n=1; risperidone and chlorpromazine, n=1, haloperidol and thioridazine, n=1, perphenazine and thioridazine, n=2; sulpiride, zuclopenthixol, and levomepromazine, n=1; five persons did not report using any antipsychotic medication. bMedications were as follows: risperidone, n=1; haloperidol, n=1; thioridazine, n=2; perphenazine, n=2; others did not report using any antipsychotic medication.
The presence of each criterion of metabolic syndrome in different diagnostic groups is presented in Table 7. Schizophrenic subjects had more often abdominal obesity and hypertriglyceridemia compared with the comparison group (p<0.001 and p=0.001, respectively, Fisher’s exact test). No other significant differences were found.

50
Table 7. The presence of each criterion of metabolic syndrome in different diagnostic groups.
Criterion of metabolic syndrome
Schizophrenia (n=31) (%)
Other psychoses (n=22) (%)
Non-psychotic disorders (n=105) (%)
Comparison group (n=5,455) (%)
Abdominal obesity1 13 (42) 4 (18) 21 (20) 683 (13) Triglycerides ≥1.7 mmol/l
12 (39) 6 (27) 19 (18) 831 (15)
HDL cholesterol men <1.0 mmol/l, women <1.3 mmol/l
5 (16) 1 (5) 21 (20) 588 (11)
Blood pressure ≥130/85 mmHg
15 (48) 10 (45) 38 (36) 2,209 (40)
Fasting glucose ≥6.1 mmol/l
0 (0) 0 (0) 3 (3) 157 (3)
1) waist circumference in men >102 cm, in women >88 cm
Demographic and clinical characteristics (age at onset, days at hospital, number of
hospital treatment sessions and daily dose of antipsychotics) of subjects with schizophrenia in relation to the presence of metabolic syndrome did not differ statistically significantly between the groups (Table 8).

51
Table 8. Clinical variables in the schizophrenia group in relation to the presence of metabolic syndrome.
Metabolic syndrome Clinical variable Yes
(n=6) No (n=25)
p-value
Gender male 5 13 0.3591
female 1 12 Age at onset of schizophrenia median 20.0 22.0 0.4082
range 16-24 16-31 Days at hospital after diagnosis median 163.0 121.0 0.8622
range 44-606 5-1361 Number of treatment episodes in hospital median 3.0 4.5 0.9542
range 2-11 1-27 Daily dose of antipsychotic medication3 median 350 150 0.3922
range (100-1665) (0-2000) 1Fisher’s exact test 2Mann-Whitney U test 3Chlorpromazine equivalents

6 Discussion
6.1 Methodic discussion
6.1.1 Strengths of the study
The major strengths of this study come from the large, unselected, general population- based study sample: the Northern Finland 1966 Birth Cohort. The birth cohort design means that the subjects are all the same age, eliminating confounding from this factor, and the population-based design means that the sample is also comparatively free from selection bias. A simple, yet compelling strength of birth cohort studies is that the prospective collection of data covers all or the majority of the period of risk during which causal processes may accumulate (Colman & Jones 2004).
Most previous studies concerning lipid values or metabolic syndrome in schizophrenia or on patients with antipsychotics are based on clinical samples, mostly on patient series. Here we were able to study the lipid values and metabolic syndrome in a population- based sample.
In the provinces of Lapland and Oulu 96% of all women (n=12,068), with an expected delivery date in 1966 were evaluated (Rantakallio 1969). A large amount of information concerning their health habits and clinical variables were gathered in 1997-98, making analysis of confounding factors possible. We were able to adjust several confounding factors including sex, diet, waist circumference, physical exercise, smoking and alcohol consumption when estimating the risk of hyperlipidemia in persons using antipsychotic medication. As far as we know, this many confounding factors have not been taken into account in previous studies.
All cohort members aged over 16 years appearing in the Finnish Hospital Discharge register (FHDR) with mental disorder have been selected for the study. FHDR covers all general and mental hospitals, bed wards of local health centers, military wards, prison hospitals and private hospitals. Its coverage and validity have been shown to be acceptable (Poikolainen 1983). All diagnoses have been scrutinized and validated for the

53
DSM-III-R criteria. Interrater reliability has been good, with kappa values from 0.6 to 0.9 (Isohanni et al. 1997, Moilanen et al. 2003).
Psychiatry is constantly faced with challenges related to the medical status of its patients and the comorbid effects of the pharmacologic treatment of psychiatric disorders (Sacks 2004). The original papers included in this thesis are very timely as there is a continuously rising amount of articles concerning obesity, diabetes, dyslipidemia and metabolic syndrome in schizophrenia or subjects using antipsychotic medication.
Since the WHO (Alberti et al. 1998) and the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) (2001) published definitions of the metabolic syndrome, research on this syndrome has developed and become easier; we were thus able to produce clinically relevant information in this study as well.
6.1.2 Limitations of the study
Although the original study sample is large, the study sample contains a limited number of schizophrenia patients due to the rarity of schizophrenia. The relatively small size of the schizophrenia group makes type II error possible, meaning the possibility of missing the effect (i.e. declaring that there is no significant effect) although there really is one. The limited number of individuals with schizophrenia also made it impossible to analyze all confounding factors, especially in original studies III and V. In original study V we studied another relatively rare phenomenon, metabolic syndrome. In original study III subjects with schizophrenia were divided into two groups. Hence in these studies the group sizes became smaller, making analysis of confounding factors impossible.
In original studies II and V the analysis of missing data was completed in different ways. In original study II, only subjects who did not came to clinical examination were considered as missing; in original study V also subjects who were excluded because of non-fasted blood samples were considered as missing. The results of these two analyses are different. In the first one we concluded that no statistical differences existed between non-participants and participants, except that non-participants had spent more days in hospital after diagnosis, and the proportion of time spent in hospital after diagnosis was also higher in the non-participants’ group. This might indicate that the participants were healthier than the non-participants. In the latter analysis we concluded that in the groups of non-psychotic disorders and comparison group, women participated more often (p=0.012 and p=0.000, respectively, Chi-Square Test), and there were no other statistically significant differences between the participants and the non-participants. Thus we concluded that our sample is representative and reflects the frequency of metabolic syndrome in schizophrenia and other psychoses. In any case, our results are not exaggerated; the lipid values and the frequency of metabolic syndrome might rather be somewhat conservative.
In this study only hospital-treated mental disorders were taken into account. We assume that almost all cases of schizophrenia and other psychotic disorders are

54
sometimes treated in mental hospitals, and are thus included in the FHDR. Non-psychotic disorders are rarely treated in hospitals and thereby this group is probably highly selected, including only the most severe cases, and the results concerning this group should not be generalized to cases treated outside hospitals.
The lipid values were taken only once and therefore we do not know what the levels were before starting the antipsychotic medication, or before the patients fell ill. The data on medication were also gathered only once. We were thus not able to take into account whether somebody had had antipsychotic medication and stopped using it sometime before the blood samples were taken. Furthermore, we were not able to estimate the effect of time of the exposure to antipsychotics.
6.2 Discussion of the results
6.2.1 Weight gain, glucose and lipid metabolism disturbances during antipsychotic medication (I)
A major obstacle to improving the quality of physical health monitoring of patients with schizophrenia has been the lack of a consensus regarding which health parameter should be monitored and when they should be monitored (Marder et al. 2004).
The heightened health risks associated with schizophrenia and the medications used in its treatment, together with the belief that the health needs of people with schizophrenia who take antipsychotic medications are typically not adequately addressed by clinicians in specialty mental health programs or in primary care settings (Marder et al. 2004) has produced a number of recommendations concerning physical heath monitoring of these patients, published in 2004 (Table 2). Compared to newer guidelines, we recommended more frequent monitoring of physical health parameters. In Finland the frequency of hyperlipidemia is high (Vartiainen et al. 2003, Aromaa & Koskinen 2004), and the frequency of monitoring the metabolic side effects of the medication could therefore be more frequent in Finnish population than in other countries. There has also been discussion as to whether the monitoring protocol proposed by the ADA consensus report (American Diabetes Association et al. 2004) is appropriate. It has been said that the asterisk that indicates that more intensive monitoring may be required is very important to note. If someone experiences a rapid increase in waist circumference, or if they start out with a high level of baseline risk, physicians should not wait three months before they measure weight, blood pressure, glucose and lipids. The repeat lipid screen at 5 years is questioned as being insufficient, given the high risk in this population (Kane et al. 2004).
Of the severe mental disorders, particularly schizophrenia results in incapacity to work, impairs the quality of life, and is associated with a substantially high mortality rate from suicide even at a relatively young age (Räsänen et al. 1998). Because the disorder is so severe and its treatment so difficult, the adverse effects associated with its treatment have been considered more acceptable than those associated with the treatment of some

55
other disorders. As antipsychotics have improved, the attitude towards serious adverse effects has started to change, and the second-generation antipsychotics have in many respects significantly improved the drug treatment of severe mental disorders. They cause less neurological adverse effects than the conventional antipsychotics. During the last few years a number of publications has been published on weight gain, glucose and lipid metabolism disturbances during antipsychotic medications, and clinicians should pay attention to the selection of antipsychotic medication.
6.2.2 Serum lipids in schizophrenia and other functional psychoses (II)
TC and TG levels in subjects with schizophrenia were significantly higher (10% and 29% higher, respectively) compared to the comparison group. A meta-analysis shows that a 10% change in the concentration of plasma TC is associated with a 10% decrease of the odds of death (Marchioli et al. 1996). The effect of high plasma TG concentration on atherosclerosis and its complications is more controversial, with some data supporting the role of plasma TG level as an independent risk factor (Eberly et al. 2003). The higher total cholesterol level could mainly be due to higher LDL cholesterol. This is in accordance with the findings in many epidemiological studies. The trend of the LDL cholesterol level followed closely that of the total cholesterol across the various groups in the present study as well. The fact that the difference in LDL cholesterol between the schizophrenia group and the comparison group did not reach statistical significance may simply reflect the lack of statistical power in the study. The correlation between total cholesterol and HDL cholesterol is much weaker and depends markedly on other confounders, such as BMI and smoking, which have a decreasing effect on HDL cholesterol (Tornwall et al. 2000), while alcohol consumption tends to increase it (Rimm et al. 1999).
Lipid levels in the group of other psychoses resembled the schizophrenia group, while lipid levels in the group with hospital-treated non-psychotic disorders did not differ from the control group. This may be due to antipsychotic medication which is commonly used in all psychotic disorders.
Study subjects in the schizophrenia group with antipsychotic medication had higher TC and TG compared to those without any antipsychotic medication, and those with both atypical and typical antipsychotic medication had the highest lipid levels. However, the within group analyses are somewhat unreliable taking into account the small number of subjects. The results may also be confounded by different clinical profiles of the subgroups. The mean dosage of antipsychotic medication in the schizophrenia group was in accordance with recommendations. Hence the high lipid levels were not due to excess dosage of antipsychotic medication.
In addition, the study by Yamada et al. (1999) suggests that 5-HT has a role in the regulation of leptin (an adiposity signal) secretion. Recently Baptista et al. (2001, 2002) suggested that antipsychotics may induce e.g. sudden body weight gain, insulin resistance and increased appetite which, in turn, may be involved in the development of

56
dyslipidemia in predisposed persons. However, we could not estimate the contribution of medication, diet and physical exercise, among other things, to lipid levels. In our study, subjects using conventional antipsychotics also had high lipid levels, although these medications are not 5-HT2c receptor antagonists. Hence, the findings highlight the importance of health habits.
The major weakness of the study is the small sample size of the psychiatric patients, divided further into sub-groups according to pharmacological treatment. The rarity of schizophrenia and other functional psychoses means that Type II statistical errors are possible. The beta value was 28%, i.e. slightly higher than generally accepted. There is also the possibility of Type I errors since multiple comparisons were performed, and this was not taken into account in analyses.
6.2.3 Serum triglyceride levels in early onset schizophrenia (III)
Patients with early onset schizophrenia had higher triglyceride levels than those with later onset of this disease. One explanation may be genetic linkage, as hypertriglyceridemia may be related to the more severe forms of schizophrenia. On the other hand, cognitive disorders in these patients may cause poor dieting, and a more prolonged exposure to antipsychotics may further raise the triglyceride levels. The effect of high plasma TG concentration on atherosclerosis and its complications is more controversial than the effect of TC. However, a gradient of risk of ischemic heart disease has been associated with increasing TG levels, also after controlling for the other major risk factors of ischemic heart disease (Jeppesen et al. 1998). Our finding may imply that patients with early onset schizophrenia are at special risk for the cardiovascular complications of hypertriglyceridemia.
6.2.4 Hyperlipidemia in subjects using antipsychotic medication (IV)
We found a high prevalence of hyperlipidemia in subjects using antipsychotic medication independent of other known risk factors for hyperlipidemia. Diet, alcohol consumption and other health parameters were ascertained as part of the larger structured postal questionnaire, which the study subjects returned at the clinical examination. This method is commonly used in Finnish population-based surveys of health behavior (National Public Health Institute 1998, Helakorpi et al. 1997) and has been found to be valid (Pietinen et al. 1988, Männistö et al. 1996). In addition, to examine the validity of variables measuring unhealthy diet and alcohol consumption in the Northern Finland 1966 Birth Cohort, a subsample of 196 cohort members participating in the health examination recorded immediately after the health examination, during 7 days, all drinks, including alcohol beverages, and foods eaten, with amounts and a detailed description of the quality. Food records were compared to questions measuring alcohol use and diet in

57
the questionnaire and analyzed thereafter with the computer program. The authors concluded that self-reported questions measuring alcohol use and unhealthy diet were sufficiently valid (Laitinen et al. 2004).
The mechanisms for antipsychotic-induced elevation of blood lipid levels are discussed in the chapter Theoretical considerations. The combination of conventional and atypical medication should be very carefully considered. Our findings highlight the importance of regular monitoring of lipid levels in persons using antipsychotic medication.
6.2.5 Metabolic syndrome in schizophrenia (V)
Using the National Cholesterol Education Program’s definition (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001), we estimated that a fifth (19%) of the schizophrenia patients in their early thirties had metabolic syndrome, whereas the prevalence of metabolic syndrome in the comparison group was 6%. Individuals with metabolic syndrome are at special risk for coronary heart disease. The metabolic syndrome alone predicts about 25% of all new-onset cardiovascular disease, and the presence of metabolic syndrome is also highly predictive of new-onset diabetes (Grundy et al. 2004). Our finding may thus explain at least part of the excess mortality of schizophrenic patients due to cardiovascular disease.
Because there were no differences in the age at onset, days at hospital or the number of hospital treatment sessions between participants and non-participants, we think that our sample is representative and reflects the frequency of metabolic syndrome in schizophrenia and other psychoses.
Almost all psychotic patients in Finland are at some time treated in hospital, whereas non-psychotic disorders are commonly treated outside hospitals, which is why this group in our study may not be representative. Regarding diagnostic specificity, increased probability of metabolic syndrome was associated with DSM-III-R schizophrenia but not with non-schizophrenic psychoses (although the number of cases was small) or hospital-treated non-psychotic disorders. This preliminary finding of diagnostic specificity requires replications within larger study samples.
Although patients with schizophrenia are more at risk for abnormal glucose than matched controls (Ryan et al. 2003), in the present study none of the schizophrenia patients or subjects with other psychoses had fasting glucose higher than or equal to 6.1 mmol/l (110 mg/dL). Only 3% of the subjects met the criteria for high fasting glucose in the other groups as well; hence this phenomenon may simply reflect the limited number of subjects with psychotic illness in this study. It also brings to fore the issue that in order to have metabolic syndrome, one does not need to have impaired fasting glucose.
In the only previous study on this subject the prevalence of metabolic syndrome was 37% in long-term schizophrenics, with a mean age of 45 years (Heiskanen et al. 2003). The lower prevalence (19%) of metabolic syndrome found here may partly be due to younger age of our study group and the increasing prevalence of metabolic syndrome

58
with age (Ford et al. 2002). In the previous study the study sample consisted of 35 long-term schizophrenia patients from the psychiatric rehabilitation ward, having many hospital-treatment sessions and hospital days. Compared to that, the subjects in the present study seem to have less hospital-treatment episodes and days at hospital, suggesting that patients with more severe illness might be at higher risk of metabolic syndrome. However, in our study there was no association in relation to the presence of metabolic syndrome in demographic or clinical variables. Further studies in a larger population based sample are therefore needed to investigate whether the severity of schizophrenia or the daily dose or type of antipsychotic medication correlates with the incidence of metabolic syndrome.
It is unclear as to how much of the increased risk of metabolic syndrome in the sample was due to unhealthy lifestyle issues, e.g. poor diet, lack of exercise and cigarette smoking, which are known to have higher prevalence in schizophrenics than in the general population. Schizophrenia and high blood glucose may also be linked independently of medication (Koro et al. 2002, Expert group 2004). Although there is some evidence that atypical antipsychotics can cause increased risk of diabetes mellitus (Henderson et al. 2000), the attributable risk of diabetes mellitus associated with atypical antipsychotics when compared to conventional antipsychotics seems to be small, about 2% for clozapine and less than 1% for quetiapine, olanzapine and risperidone (Leslie & Rosenhech 2004). The use of antipsychotics may also partly explain the higher prevalence of metabolic syndrome in schizophrenia. Clinicians should pay attention to the selection of antipsychotic medication, because different antipsychotics seem to have different effects on glucose and lipid levels (Melkersson & Dahl 2004).
The basic causes and mechanisms of the metabolic syndrome are not known, but for the majority of patients improper nutrition and inadequate physical activity are of importance. Some interventions for managing weight gain associated with atypical antipsychotics have been studied (Vreeland et al. 2003, Ball et al. 2001), but further studies of interventions and their effectiveness are needed. There is currently very limited evidence available that behavioral interventions actually work in overweight patients treated with antipsychotics (Werneke et al. 2003). The characteristics of schizophrenia sufferers mean that weight management will be even more difficult to achieve than in populations without mental health difficulties. The high prevalence of this syndrome in schizophrenia even at such a young age underscores the need to develop comprehensive efforts directed at controlling weight and improving physical activity as well as the importance of selecting antipsychotic medications with no or little capability to induce metabolic side effects.
6.2.6 Theoretical considerations
Compared with the general population, patients with schizophrenia are overrepresented in the higher BMI categories and underrepresented in the lower (Allison et al. 1999b). It is unclear whether the weight gain is caused by the disease state itself (i.e. the biology of

59
the psychiatric disorder) or by the socioeconomic and behavioral correlates of the disease, such as reduced access to medical care or poor food choices (Kane et al. 2004).
Food intake is controlled by a highly complex process. Emotions, social factors, time of day, convenience and cost are but a few of the variables that are not biologically regulated, but nonetheless affect meal-to-meal energy intake. Despite short-term mismatches in energy balance, most of us do however match cumulative energy intake to energy expenditure with great precision when measured over a period that spans many meals. This phenomenon reflects an active regulatory process, termed energy homeostasis, that promotes stability in the amount of body energy stored in the form of fat (Schwartz et al. 2000). Recently, there has been an explosion in the understanding of the neurochemical systems that regulate body weight. A number of interrelated signals give the brain information about the nutritional state of the organism. The signals then produce changes in the levels of several neurotransmitters within specific brain regions that ultimately increase or decrease feeding behaviors (Bessesen 2003). These neurotransmitters are either anorexigenic (appetite inhibiting) and catabolic or orexigenic (appetite stimulating) and anabolic (Schwartz et al. 2000). Anorexic substances include leptin, corticotrophin-releasing hormone, α-melanocyte-stimulating hormone, cocaine-amphetamine-related transcript, cholecystokinin, peptide YY, insulin and serotonin. Insulin, which enters the brain from the circulation and acts there to reduce energy intake, was the first hormonal signal to be implicated in the control of body weight by the central nervous system. Leptin is a hormone secreted by adipocytes, which act in the hypothalamus. Administration of either insulin or leptin directly into the brain reduces food intake. Obesity has been thought to be associated with leptin resistance in the hypothalamus (Atmaca et al. 2003a). Orexigenic substances include agouti, agouti-related peptide, ghrelin, melanin-concentrating hormone, neuropeptide Y, orexibs A and B and noradrenalin (Schwartz et al. 2000).
Atypical antipsychotics are potent antagonists of both 5- HT2a and 5- HT2c receptors, with the latter implicated in hyperphagia and the subsequent development of obesity and adult-onset diabetes, although this does not seem to directly induce hyperlipidemia (Meyer 2001). The correlation between serotonin 5-HT2cantagonism and weight gain is poor since the atypical antipsychotic with the greatest affinity, ziprasidone, appears to be the most weight neutral (Meyer & Koro 2004).
Clozapine and olanzapine seem to increase serum leptin levels, whereas quetiapine seems to increase leptin modestly and haloperidol and risperidone minimally (Melkersson & Dahl 2004). Many antipsychotics bind to and block histamine receptors, especially the H1 subtype. Activation of histamine receptors in the hypothalamus is associated with reduced food intake (Sakata et al. 1997). Antipsychotic-associated weight gain has been correlated with H1 receptor affinity (Wirshing et al. 1999).
The mechanism for the elevation in lipid levels is somewhat obscure, but it has been previously attributed to weight gain associated with the use of antipsychotic medication. Accumulation of fat in the waist enhances release of free fatty acids in the liver and accelerates liver triglyceride synthesis and very-low-density lipoprotein secretion. Increases in free fatty acid concentrations may also inhibit metabolism of glucose,

60
especially in muscle tissue, resulting in impaired glucose tolerance and type-2 diabetes (National Heart, Lung and Blood Institute 2001). Olanzapine, quetiapine, and clozapine are structurally related and are derived from dibenzodiazepine-derived compounds, whereas aripiprazole is not structurally related to any of the other atypical antipsychotics (Casey et al. 2004). It has been postulated that changes in lipid levels may be related to the 3-ring structure of the dibenzodiazepine-derived compounds. This structure is conformationally similar to the phenothiazide nucleus, which has a known propensity to increase serum triglyceride levels (Meyer 2001).

7 Conclusions
7.1 Main results
TC and TG were high in schizophrenia and other psychoses (II). In the schizophrenia group those who had both atypical and typical medication had the highest TC and TG. (II). We found higher triglyceride levels in patients who were ≤ 20 years old at the beginning of schizophrenia as compared with patients with later onset or non-hospitalized controls (III). The prevalence of hypercholesterolemia, high LDL-cholesterol and hypertriglyceridemia were high in persons using antipsychotic medication compared to persons without such medication (IV). In the whole sample we found high lipid levels in persons with both atypical and typical medication. Mean TC and TG were also high in the subjects with only typical medication (IV). The prevalence of hypercholesterolemia, high LDL-cholesterol and hypertriglyceridemia were high in persons using antipsychotic medication compared to persons without such medication (IV). The prevalence of metabolic syndrome was high in subjects with schizophrenia compared with the comparison group (V).
7.2 Clinical and practical implications
These results indicate the importance of regular monitoring of weight, waist circumference, serum lipid and glucose levels and blood pressure, thus screening for the possibility of hyperlipidemia, high glucose levels and metabolic syndrome in patients with schizophrenia or other psychoses or on antipsychotic medication, with special attention to those with both atypical and typical medication or early onset schizophrenia. The combination of conventional and atypical antipsychotics should be very carefully considered.
Recommendations on the treatment of hyperlipidemia (Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults 2001, Suomen Sisätautilääkärien Yhdistys ry:n asettama työryhmä 2004), guidelines for the treatment of patients with clinically significant obesity (The Expert Consensus Panel for Optimizing

62
Pharmacologic Treatment of Psychotic Disorders 2003, Suomen lihavuustutkijat ry:n asettama työryhmä 2002) and on monitoring and therapeutic interventions in patients on second-generation antipsychotics (Table 2) should be followed. The monitoring protocol for patients on second-generation antipsychotics by American Diabetes Association et al. (2004) is shown in Table 9. According to this recommendation, at the baseline monitoring these assessments can determine whether the patient is overweight (BMI 25.0-29.9) or obese (BMI ≥30), has pre-diabetes (fasting plasma glucose 5.6 mmol/l or 100 mg/dL-7.0 mmol/l or 125 mg/dL) or diabetes (fasting plasma glucose ≥126 mg/dL), hypertension (blood pressure > 140/90 mmHg) or dyslipidemia. If any of these conditions are identified, appropriate treatment should be initiated. Psychiatrists should not hesitate to refer the patient to the appropriate health care professionals or specialist knowledgeable about these disorders. The panel recommended that nutrition and physical activity counseling be provided for all patients who are overweight or obese. Health care professionals, patients, family members and caregivers should be aware of the signs and symptoms of diabetes. If possible, clinicians should try to choose medications that have a lower risk of causing weight gain, worsening of lipid profile or risk for diabetes. If a patient gains ≥5 % of his or her initial weight at any time during the therapy one should consider switching the antipsychotic medication. Physical health monitoring and interventions should be initiated in routine psychiatric settings and they should become a part of routine care. Clinicians should sensitize patients and their caregivers to the health risks associated with schizophrenia and other psychoses and their treatment, and they should encourage patients to self-monitor their weight. As the population in general becomes more obese and sedentary over time, risk factors for cardiovascular disease and diabetes are increasing in prevalence, and their effect should be considered in the treatment of any psychiatric condition.

Tabl
e 9.
Mon
itori
ng p
roto
col f
or p
atie
nts o
n se
cond
-gen
erat
ion
antip
sych
otic
s (D
iabe
tes C
are
2004
)*
B
asel
ine
4 w
eeks
8
wee
ks
12 w
eeks
Q
uarte
rly
Ann
ually
Ev
ery
5 ye
ars
Pers
onal
/fam
ily h
isto
ry (
obes
ity,
dysl
ipid
emia
, hy
perte
nsio
n or
ca
rdio
vasc
ular
dis
ease
)
x
x
Wei
ght (
BM
I)
x
x x
x x
Wai
st c
ircum
fere
nce
x
x
Blo
od p
ress
ure
x
x
x
Fast
ing
plas
ma
gluc
ose
x
x
x
Fast
ing
lipid
pro
file
x
x
x
* M
ore
freq
uent
ass
essm
ents
may
be
war
rant
ed b
ased
on
clin
ical
stat
us

64
Ideally, a weight restriction program that includes either habitual or formal exercise should be tailored to the patient’s needs at the outset of antipsychotic treatment and the program should then be regularly monitored (Malhi 2003). Psychotic patients with lipid metabolism disorders can also be treated with e.g. statins, with careful consideration of potential interactions with antipsychotic medications. Results of open trials show that triglyceride levels in patients who received gemfibrozil or pravastatin did not increase during treatment with olanzapine (Osser et al. 1999). Most statins are metabolized through the cytochrome 3A4 enzyme, which may result in interactions with higher doses of second-generation antipsychotics, such as clozapine, olanzapine and quetiapine, which also partly use this pathway (Cozza et al. 2003). Attempts can also be made to reduce the adverse effects of lipid metabolism disorders by means of low-dose acetylsalicylic acid medication. It is also important to remember that even if the initial dosage of antipsychotic medication to relieve an acute symptom episode exceeds the recommendations for maintenance therapy, efforts should be made to gradually reduce the dosage. Moreover, because there may be a relationship between the dose of antipsychotic agent and weight gain (Basson et al. 2001), the lowest effective dose should be used. Clinicians should also pay attention to the selection of antipsychotic medication, because different antipsychotics seem to have different effects on blood lipid levels (Melkersson & Dahl 2004). In this way we might be able to influence the risk factors of cardiovascular diseases and thus decrease the excess morbidity and mortality associated with schizophrenia.
7.3 Implications for further studies
Because of the limited number of patients with schizophrenia in studies concerning serum lipids and the prevalence of metabolic syndrome in schizophrenia and other functional psychoses, these studies should be replicated in larger samples.
In original study IV we found higher triglyceride levels in subjects who were ≤ 20 years old at the beginning of the schizophrenia. This is the first study reporting such a finding. One explanation may be genetic linkage, as hypertriglyceridemia may be related to the more severe forms of schizophrenia. On the other hand, cognitive disorders in these patients may cause poor dieting, and a more prolonged exposure to antipsychotics may raise the triglyceride levels further. This study needs to be replicated and the influence of the above-mentioned factors should be analyzed. If the result is confirmed and other factors do not explain the result, further studies of possible genetic linkage between triglyceride levels and the age at onset of schizophrenia should be carried out.
There are a lot of confounding factors when metabolic issues of patients with schizophrenia are studied. Because studies with drug-naïve patients with first-episode schizophrenia appear to indicate that these patients have higher than expected rates of visceral obesity (Thakore et al. 2002) and impaired fasting glucose concentrations (Ryan et al. 2003), one might also hypothesize that high lipid and glucose values and schizophrenia (i.e. the biological illness it self) are somehow linked. This linkage could be genetic, or one or more factors influencing the developmental phase of an embryo or a

65
child. These possible linkages should deserve more attention in future research; for example, studies of a possible genetic factor producing both schizophrenia and metabolic disturbances could be carried out.
The knowledge of risk factors for metabolic disturbances in the premorbid phase of psychoses is still very limited, and further studies are needed in this field. Further studies in a larger nation-wide sample are needed to investigate whether the severity of schizophrenia or daily dose or type of antipsychotic medication correlates with lipid levels or the prevalence metabolic syndrome. The consequences of metabolic disturbances, e.g. their effect on the morbidity and mortality to cardiovascular diseases, could also be studied in a larger sample. Preventive interventions and treatment approaches targeted at the cardiovascular risk factors should be developed further, and studies are needed on their influence to morbidity and mortality.
The longitudinal database of the Northern Finland 1966 Birth Cohort has thus far provided unique opportunities to investigate various outcomes up to early adulthood. In the future there will be even more possibilities for research, and it would be interesting to know e.g. whether the lipid values and the prevalence of metabolic syndrome will change differently in different diagnostic categories as the cohort members get older. However, the low number of subjects with schizophrenia will limit the possibilities of studying metabolic disturbances in our sample and thus other, larger prospective studies need to be performed.

References
Alberti KG & Zimmet PZ, for the WHO Consultation (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus, provisional report of a WHO consultation. Diabet Med 15: 539-553.
Allison DB, Mentore JL, Moonseong H, Chandler LP, Cappelleri JC, Infante MC & Weiden PJ (1999a) Antipsychoyic-Induced weight gain: a comprehensive research synthesis. Am J Psychiatry 156: 1686-1696.
Allison DB, Fontaine KR, Moonseong H, Mentore JL, Cappelleri JC, Chandler LP, Weiden PJ & Cheskin LJ (1999b) The distribution of Body Mass Index among individuals with and without schizophrenia. J Clin Psychiatry 60: 215-220.
Alméras N, Després J-P, Villeneuve J. Demers M-F, Roy M-A, Cadrin C, Mottard J-P & Bouchard R-H (2004) Development of an atherogenic metabolic risk factor profile associated with the use of atypical antipsychotics. J Clin Psychiatry 65:557-564.
American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists & North American Association for the study of Obesity (2004) Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes. Diabetes Care 27:2: 596-601.
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rd edition-revised (DSM-III-R). Washington, DC, American Psychiatric Association.
American Psychiatric Association (2000) Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text revision. Washington, DC, American Psychiatric Association.
Aromaa A & Koskinen S (ed.) (2004) Health and functional capacity in Finland. Baseline results of the health 2000 Health Examination Survey. Hakapaino Oy. Available at: http://www.ktl.fi/terveys2000/index.uk.html. Accessed in January 22, 2005.
Atmaca M, Kuloglu M, Tezcan E & Ustundag B (2003a) Serum leptin and triglyceride levels in patients on treatment with atypical antipsychotics. J Clin Psychiatry 64: 598-604.
Atmaca M, Kuloglu M, Tezcan E & Gecici O (2003b) Weight gain, serum leptin and triglyceride levels in patients with schizophrenia on antipsychotic treatment with quetiapine, olanzapine and haloperidol. Sch Research 60: 99-100

67
Baptista T, Lacruz A, Angeles F, Silvera R, de Mendoza S, Mendoza MT & Hernandez L (2001) Endocrine and metabolic abnormalities involved in obesity associated with typical antipsychotic drug administration. Pharmacopsychiatry 34(6): 223-31.
Baptista T, Kin NM, Beaulieu S & de Babtista EA (2002) Obesity and related metabolic abnormalities during antipsychotic drug administration: mechanisms, management and research perspectives. Pharmacopsychiatry 35(6): 205-19.
Ball MP, Coons VB & Buchanan RW (2001) A program for treating olanzapine-related weight gain. Psychiatric Services 52(7): 967-969
Basson B, Kinon B, Taylor C, Szymanski K, Gilmore J & Tollefson G (2001) Factors influencing acute weight change in patients with schizophrenia treated with olanzapine, haloperidol, or risperidone. J Clin Psychiatry 62: 231-138.
Baymiller SP, Ball P, McMahon RP & Buchanan RW (2002) Serum glucose and lipid changes during the course of clozapine treatment: the effect of concurrent ß-adrenergic antagonist treatment. Sch Research 59: 49-57
Bazire S (1999) Psychotropic Drug Directory 1999. The professionals pocket handbook and aide memoire. Dinton:Quay Books Division, Mark Allen Publishing Ltd.
Bessesen DH (2003) Future Directions in weight control. Molecular and genetic discoveries pave the way. Postgraduate Medicine 114:30-38.
Bouchard RH, Demers M-F, Simoneau I, Almeras N, Villeneuve J, Mottard J-P, Cardin C, Lemieux I & Despres J-P (2001) Atypical antipsychotics and cardiovascular risk in schizophrenic patients. J Clin Psychopharmacol 21: 110-111
Brecher M, Rak IW, Melvin K & Jones AM (2000) The long-term effect of quetiapine (Seroquel) monotherapy on weight in patients with schizophrenia. Int J Psych Clin Pract 4: 287-291
Brown S (1997) Excess mortality of schizophrenia. A meta-analysis. Br J Psychiatry 171: 502-8. Brown S, Inskip H & Barraclough B (2000) Causes of the excess mortality of schizophrenia. Br J
Psychiatry 177: 212-217. Bushe C & Holt R (2004) Prevalence of diabetes and impaired glucose tolerance in patients with
schizophrenia. Br J Psychiatry 184(suppl 47): 67-71. Casey DE (2004) Dyslipidemia and atypical antipsychotic drugs. J Clin Psychiatry 65[suppl 18]:
27-35. Casey DE, Haupt DW, Newcomer JW, Henderson DC, Sernyak MJ, Davidson M, Lindenmayer JP,
Manoukian SV, Banerji MA, Lebovitz HE & Hennekens CH (2004) Antipsychotic-induced weight gain and metabolic abnormalities: implications for increased mortality in patients with schizophrenia. J Clin Psychiatry. 65 (Suppl 7): 4-18.
Cassidy F, Ahearn E & Carrol BJ (1999) Elevated frequency of diabetes mellitus in hospitalized manic-depressive patients. Am J Psychiatry 156: 1417-1420.
Colman I & Jones PB (2004) Birth cohort studies in psychiatry: beginning at the beginning. Psychological Medicine 34: 1375-1383.
Cozza KL, Armstrong SC & Oesterheld JR (2003) Drug interaction principles for medical practice. American Psychiatric Publishing, Washington, D.C.
Dinneen SF & Gerstein HC (1997) The association of microalbuminuria and mortality in non-insulin-dependent diabetes mellitus. A systematic overview of the literature. Arch Intern Med 157:1413-1418.

68
Dixon L, Weiden P, Delahanty J, Goldberg R, Postrado L, Lucksted A & Lehman A (2000) Prevalence and correlates of diabetes in national schizophrenia samples. Sch Bulletin 26: 903-912.
Dursum SM, Szemis A, Andrews H & Releley MA (1999) The effects of clozapine on levels of total cholesterol and related lipids in serum of patients with schizophrenia: a prospective study. J Clin Neurosci 24(5): 453-5.
Eberly LE, Stamler J, Neaton JD & Multiple Risk Factor Intervention Trial Research Group (2003) Relation of triglyceride levels, fasting and nonfasting, to fatal and nonfatal coronary heart disease. Archives of Internal Medicine. 163(9): 1077-83.
Enger C, Weatherby L, Reynolds RF, Glasser DB & Walker AM (2004) Serious cardiovascular events and mortality among patients with schizophrenia. J Nerv Mant Dis 192:19-27.
Expert group (2004) Schizophrenia and diabetes 2003’ expert consensus meeting, Dublin, 3-4 October 2003: consensus summery. Br J Psychiatry 184 (47, suppl): 112-114.
Expert Panel in Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (2001) Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 285:2486-2497.
Festa A, D´Agostino R Jr, Howard G, Mykkanen L, Tracy RP & Haffner SM (2000) Chronic subclinical inflammation as part of the insulin resistance syndrome: the Insulin Resistance Atherosclerosis Study (IRAS). Circulation 102:42-47.
Folsom AR, Kuba K, Leupker RV, Jacobs DR & Frantz ID Jr (1983) Lipid concentrations in serum and EDTA-treated plasma from fasting and nonfasting normal persons, with particular regard to high-density lipoprotein cholesterol. Clinical Chemistry. 29(3):505-8.
Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshminarayanan M, Casey DE & Allison DB (2001) Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 15;101(3):277-88.
Ford ES, Giles WH & Dietz WH (2002) Prevalence of the metabolic syndrome among US adults. Findings from the third national health and nutrition examination survey. JAMA 287:356-359.
Ford ES & GilesWH (2003) A comparison of the prevalence of the metabolic syndrome using two proposed definitions. Diabetes Care 26:575-581.
Gaulin BD, Markowitz JS, Caley CF, Nesbitt LA & Dufresne RL (1999) Clozapine-associated elevation in serum triglycerides. Am J Psychiatry 156:1270-1272.
Ghaeli P & Dufresne RL (1996) Serum triglyceride levels in patients treated with clozapine. Am J Health-Syst Pharm 53:2079-81.
Ghaeli P & Dufresne RL (1999) Elevated serum triglycerides with clozapine resolved with risperidone in four patients. Pharmacotherapy19(9):1099-101.
Grundy SM, Brewer B, Cleeman JI, Smith SC Jr, Lenfant C, American Heart Association & National Heart, Lung, and Blood Institute (2004) Definition of Metabolic Syndrome. Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Circulation 109:433-438.
Haffner SM, Valdez RA, Hazuda HP, Mitchell BD, Morales PA & Stern MP (1992) Prospective analysis of the insulin resistance syndrome (syndrome X). Diabetes 41:715-722.

69
Haupt DW & Newcomer JW (2002) Abnormalities in glucose regulation associated with mental illness and treatment. J Psychosom Res 53 (4):925-33.
Heiskanen T, Niskanen L, Lyytikäinen R, Saarinen PI & Hintikka J (2003) Metabolic Syndrome in Patients With Schizophrenia. J Clin Psychiatry 64:575-579.
Helakorpi S, Uutela A, Prättälä R & Puska P (1997) Suomalaisen aikuisväestön terveyskäyttäytyminen, kevät 1997. [Health Behaviour Among Finnish Adult Population, Spring 1997]. Helsinki, Finland, National Public Health Institute.
Henderson D, Cagliero E, Gray C, Nasrallah R, Hayden D, Schoenfeld D & Goff D (2000) Clozapine, Diabetes Mellitus, Weight Gain, and Lipid Abnormalities: A Five-Year Naturalistic Study. Am J Psychiatry 157:975-981.
Hennekens C (1998) Increasing Burden of Cardiovascular Disease: Current Knowledge and Future Directions for Research on Risk Factors. Circulation 97:1095-1102.
Isohanni M, Mäkikyrö T, Moring J, Räsänen P, Hakko H, Partanen U, Koiranen M & Jones P (1997) Comparison of clinical and research DSM-III-R diagnoses of schizophrenia in a Finnish national birth cohort. Soc Psychiatry Psychiatr Epidemiol 32: 303-308.
Isomaa B, Almgren P, Tuomi T, Forsen B, Lahti K, Nissen M, Taskinen M-R & Groop L (2001) Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 24(4):683-689.
Jablensky A (2003) The epidemiological horizon. In Schizophrenia, ed Hirsch SR and Weinberger D. Blackwell Science.
Janssen I, Katzmarzyk PT & Ross R (2002) Body mass index, waist circumference, and health risk: evidence in support of current National Institutes of Health guidelines. Arc Intern Med 162:2074-2079.
Jeppesen J, Hein HO, Suadicani P & Gyntelberg F (1998) Triglyceride concentration and ischemic heart disease: an eight-year follow-up in the Copenhagen Male Study. Circulation 97(11):1029-36.
Järvelin M, Mäki-Torkko E, Sorri MJ & Rantakallio PT (1997) Effect of hearing impairment on educational out-comes and employment up to the age 25 years in northern Finland. Br J Audiol 31:165-175
Kane JM, Barret EJ, Casey DE, Correl CU, Gelenberg AJ, Klein S & Newcomer JW (2004) Metabolic Effects of Treatment With Atypical Antipsychotics. J Clin Psychiatry 65:1447-1455.
Kelly DL, Kreyenbuhl J, Love RC, Van-Duong Q & Conley RR (2003) Six-Month review of weight and metabolic parameters in patients receiving clozapine, risperidone, olanzapine, or quetiapine. J Clin Psychiatry 64 (9):1133-1134
Kingsbury SJ, Fayek M, Trufasiu D, Zada J & Simpson GM (2001) The apparent effect of ziprasidone on plasma lipids and glucose. J Clin Psychiatry 62:347-349
Kinon BJ, Basson BR, Gilmore JA & Tollefson GD (2001) Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 62:92-100
Koponen H, Saari K, Savolainen M & Isohanni M (2002) Weight gain and glucose and lipid metabolism disturbances during antipsychotic medication. A review. Eur Arch Psychiatry Clin Neurosci 252:294-298.

70
Koro CE, Fedder DO, L´Italien G, Weiss S, Magder LS, Kreyenbuhl J, Revicki D & Buchanan RW (2002) An assessment of the Independent Effects of Olanzapine and Risperidone Exposure on the Risk of Hyperlipidemia in Schizophrenic Patients. Arc Gen Psychiatry 59:1021-1026.
Kuoppasalmi K, Lönnqvist J, Pylkkänen K & Huttunen M (1989) Classification f Mental Disorders in Finland. A Comparison of the Finnish classification of mental disorders in 1987 with DSM-III-R. Psychiatria Fennica 65-81.
Laaksonen DE, Niskanen L, Lakka H-M, Lakka TA & Uusitupa M (2004a) Epidemiology and treatment of the metabolic syndrome. Ann Med 36:1-15.
Laaksonen DE, Niskanen L, Nyyssönen K, Punnonen K, Tuomainen T-P, Valkonen V-P, Salonen R & Salonen JT. C-reactive protein and the development of the metabolic syndrome and diabetes in middle-aged men (2004b) Diabetologia 47:1403-1410.
Laitinen J, Pietiläinen K, Wadsworth M, Sovio U & Järvelin MR (2004) Predictors of abdominal obesity among 31-y-old men and women born in Northern Finland in 1966. Eur J Clin Nutr 58(1):180-90.
Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomilehto J & Salonen JT (2002) The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 288:2709-2716.
Lehman AF & Steinwachs DM (1998) At Issue: Translating Research Into Practice: The Schizophrenia Patient Outcomes Research Team (PORT) Treatment Recommendations. Schizophr Bull 24:1-10
Lehman AF, Lieberman JA, Dixon LB, McGlashan TH, Miller AL, Perkins DO & Kreyenbuhl J (2004) American Psychiatric Association. Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry 161(suppl 2):1-56.
Leslie DL & Rosenhech RA (2004) Incidence of newly diagnosed diabetes attributable to atypical antipsychotic medications. Am J Psychiatry 161:1709-1711
Lindenmayer J-P, Czobor P, Volavka J, Citrome L, Sheitman B, McEvoy JP, Cooper TB, Chakos M & Lieberman JA (2003) Changes in glucose and cholesterol levels in patients with schizophrenia treated with typical and atypical antipsychotics. Am J Psychiatry 160:290-296.
Lund BC, Perry PJ, Brooks JM & Arndt S (2001) Clozapine use in patients with schizophrenia and the risk of diabetes, hyperlipidemia, and hypertension. A claims-based approach. Arch Gen Psychiatry 58:1172-1176
Malhi GS (2003) Weight gain: gained by waiting. Acta Psychiatr Scand 108: 249-251. Marchioli R, Marfisi RM, Carinci F & Tognoni G (1996) Meta-analysis, clinical trials, and
transferability of research results into practice: The Case of cholesterol-lowering interventions in the secondary prevention of coronary heart disease. Arch Intern Med 156:1158-1172.
Marder SR, Essock SM, Miller AL, Buchanan RW, Casey DE, Davis JM, Kane JM, Lieberman JA, Schooler NR, Covell N, Stroup S, Weissman EM, Wirshing DA, Hall CS, Pogach L, Pi-Sunyer X, Bigger JT Jr, Friedman A, Kleinberg D, Yevich SJ, Davis B & Shon S (2004) Physical heath monitoring of patients with schizophrenia. Am J Psychiatry 161:1334-1349.
McQuade RD, Stock E, Marcus R, Jody D, Gharbia NA, Vanvegel S, Archibald D & Carson WH (2004) A comparison of weight change during treatment with olanzapine or aripiprazole: results from a randomized, double-blind study. J Clin Psychiatry 65(suppl 18):47-56

71
Melkersson KI, Hulting A-L & Brismar KE (2000) Elevated levels of insulin, leptin, and blood lipids in olanzapine-treated patients with schizophrenia or related psychosis. J Clin Psychiatry 61:742-749.
Melkersson K & Dahl M-L (2003) Relationship between levels of insulin or triglycerides and serum concentrations of the atypical antipsychotics clozapine and olanzapine in patients on treatment with therapeutic doses. Psychopharmacology 170:157-166
Melkersson K & Dahl M-L (2004) Adverse Metabolic Effects Associated with Atypical Antipsychotics. Literature Review and Clinical Implications. Drugs 64(7):701-723
Meyer JM (2001) Effects of atypical antipsychotics in weight and serum lipid levels. J Clin Psychiatry 62 (suppl27):27-34
Meyer JM (2002) A retrospective comparison of weight, lipid, and glucose changes between risperidone- and olanzapine-treated inpatients: metabolic outcomes after 1 year. J Clin Psychiatry 63:425-433
Meyer JM & Koro CE (2004) The effects of antipsychotic therapy on serum lipids: a comprehensive review. Schizophrenia Research 70:1-17.
Moilanen K, Veijola J, Laksy K, Mäkikyrö T, Miettunen J, Kantojärvi L, Kokkonen P, Karvonen JT, Herva A, Joukamaa M, Järvelin MR, Moring J, Jones PB & Isohanni M (2003) Reasons for the diagnostic discordance between clinicians and researchers in schizophrenia in the Northern Finland 1966 Birth Cohort. Social Psychiatry & Psychiatric Epidemiology 38(6):305-10.
Mortensen PB (2003) Mortality and physical illness in schizophrenia. In The epidemiology of schizophrenia, ed. RM Murray, Jones PB, Susser E, van Os J & Cannon M. Cambridge Univ Press.
Männistö S, Virtanen M, Mikkonen T & Pietinen P (1996) Reproducibility and validity of a food frequency questionnaire in a case-control study on breast cancer. J Clin Epidemiol 49(4):401-9.
National Heart, Lung, and Blood Institute (2001) Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: evidence report. Available at: http://www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf. Accessed in January 18, 2005
National Institute of Health (1998) Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults-the evidence report. Obes Res 6(supl 2):51S-209S
National Public Health Institute (1998) Finravinto: 1997 –tutkimus [The 1997 Dietary Survey of Finnish Adults]. Helsinki, National Public Health Institute.
New Mexico AIDS InfoNet. Normal Laboratory values. Available at: http://aidsinfonet.org/en/pdf/120.pdf. Accessed in December 30, 2004.
Newcomer JW, Haupt DW, Fucetola R, Melson AK, Schweiger JA, Cooper BP & Selke G (2002) Abnormalities in Glucose regulation During Antipsychotic Treatment of Schizophrenia. Arch Gen Psychiatry 59:337-345.
Newcomer JW (2004) Abnormalities of glucose metabolism associated with atypical antipsychotic drugs. J Clin Psychiatry 65:36-46.
Newman SC & Bland RC (1991) Mortality in a cohort of patients with schizophrenia: a record linkage study. Canadian Journal of Psychiatry 36(4):239-45.
Osser DN, Najarian DM & Dufresne RL (1999) Olanzapine increases weight and serum triglyseride levels. J Clin Psychiatry 60:767-770.

72
Paton C, Esop R, Young C & Taylor D (2004) Obesity, dyslipidemias and smoking in inpatient population treated with antipsychotic drugs. Acta Psychiatr Scand 110:299-305
Patten CA, Gillin JC, Golshan S, Wolter TD, Rapaport M & Kelsoe J (2001) Relationship of mood disturbance to cigarette smoking status among 252 patients with current mood disorder. J Clin Psychiatry 62:319-324.
Pietinen P, Hartman AM, Haapa E, Rasanen L, Haapakoski J, Palmgren J, Albanes D, Virtamo J & Huttunen JK (1988) Reproducibility and validity of dietary assessment instruments. I. A self-administered food use questionnaire with a portion size picture booklet. Am J Epidemiol 128(3):655-66.
Pigott TA, Carson WH, Saha AR, Torbeyns AF, Stock EG, Ingenito GG, Aripiprazole Study Group (2003) Aripiprazole for the prevention of relapse in stabilized patients with chronic schizophrenia: a placebo-controlled 26-week study. J Clin Psychiatry 64 (9):1048-1056
Poikolainen K (1983) Accuracy of hospital discharge data: five alcohol-related diseases. Drug Alcohol Depend 12:315-322
Rantakallio P (1969) Groups at risk in low birth weight infants and perinatal mortality. Acta Paediatrica Scandinavica 193:1-71.
Rantakallio P (1988) The longitudinal study of the Northern Finland birth cohort of 1966. Pediatr Perinat Epidemiol 2:59-88.
Rantakallio P, Jones P, Moring J & Von Wendt L (1997) Association between central nervous system infections during childhood and adult onset schizophrenia and other psychoses: a 28-year follw-up. Int Epidemiol 26:837-843.
Rantakallio P, Myhrman A & Koiranen M (1995) Juvenile offenders, with special reference to sex differences. Soc Psychiatry Psychiatr Epidemiol 30:113-120.
Reaven GM (1988) Role of insulin resistance in human disease. Diabetes 37:1595-1607. Ridker PM, Cushman M, Stampfer MJ, Tracy RP & Hennekens CH (1997) Inflammation, aspirin,
and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 336:973-979. Rimm EB, Williams P, Fosher K, Criqui M & Stampfer MJ (1999) Moderate alcohol intake and
lower risk of coronary heart disease: meta-analysis of effects on lipids and haemostatic factors. BMJ 319(7224):1523-8.
Ryan M, Collins P & Thakore J (2003) Impaired Fasting Glucose Tolerance in First-Episode, Drug-Naïve Patients With Schizophrenia. Am J Psychiatry 160:284-289.
Räsänen P, Tiihonen J, Isohanni M, Moring J & Koiranen M (1998) Juvenile mortality, mental disturbances and criminality: a prospective study of the Northern Finland 1966 Birth Cohort. Acta Psych Scand 97:5-9.
Sacks FM (2004) Metabolic syndrome: epidemiology and consequences. J Clin Psychiatry 65 Suppl 18:3-12.
Sakata T, Yoshimatsu H & Kurokawa M (1997) Hypothalamic neuronal histamine: implications of its homeostatic control of energy metabolism. Nutrition 13:403-411.
Sasaki J, Kumagae G, Sata T, Kuramitsu M & Akakawa K (1984) Decreased concentration of high density lipoprotein cholesterol in schizophrenic patients treated with phenothiazines. Atherosclerosis 51:163-9.
Sasaki J, Funakoshi M & Arakawa K (1985) Lipids and apolipoproteins in patients treated with major tranquilizers. Clin Pharmacol Ther 37:684-7.

73
Schwartz MW, Woods SC, Porte D Jr, Seeley RJ & Baskin DG (2000) Central nervous system and food intake. Nature 404:661-671
Sernyak MJ, Leslie DL, Alarcon RD, Losonczy MF & Rosenheck R (2002) Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 159:561-566.
Sheitman BB, Bird P, Binz W, Akinli L & Sanchez C (1999). Olanzapine-induced elevation of plasma triglyceride levels. Am J Psychiatry 156, 1471-1472
Simpson GM, Glick ID, Weiden PJ, Romano SJ & Siu CO (2004) Randomized, controlled, double-blind multicenter comparison of the efficacy and tolerability of ziprasidone and olanzapine in acutely ill inpatients with schizophrenia or schizoaffective disorder. Am J Psychiatry 161:1837-1847.
Sorri M & Järvelin MR (1998) Well-being and health. Background to the Northern Finland 1966 birth cohort research. Int J Circumpolar Health 57:82-83.
Spivak B, Roitman S, Vered Y, Mester R, Graff E, Talmon Y, Guy N, Gonen N & Weizman A (1998) Diminished suicidal and aggressive behavior, high plasma norepinephrine levels, and serum triglyceride levels in chronic neuroleptic-resistant schizophrenic patients maintained on clozapine. Clinical Neuropharmacology 21:245-250.
Spivak B, Laschtein C, Talmon Y, Guy N, Mester R, Feinberg I, Kotler M & Weizman A (1999) The impact of clozapine treatment on serum lipids in chronic schizophrenic patients. Clinical Neuropharmacology 22:98-101.
Stanton JM (1995) Weight gain associated with neuroleptic medication: A review. Sch Bulletin 21:463-472.
Suomen lihavuustutkijat ry:n asettama työryhmä (2002) Aikuisten lihavuus. Käypä hoito suositus. Duodecim 118 (10):1076-1088.
Suomen Sisätautilääkärien Yhdistys ry:n asettama työryhmä (2004) Dyslipidemiat. Käypä hoito-suositus. Duodecim 120 (14):1794-816.
Thakore JH, Vlahoos J & Martin A (2002) Increased visceral fat distribution in drug-naïve and drug-free patients with schizophrenia. International Journal of Obesity Related Metabolic Disorders 26:137-141.
Tornwall ME, Virtamo J, Haukka JK, Aro A, Albanes D & Huttunen JK (2000) Prospective study of diet, lifestyle, and intermittent claudication in male smokers. American Journal of Epidemiology. 151(9):892-901.
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2003) Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26:3160-3167.
The Expert Consensus Panel for Optimizing Pharmacologic Treatment of Psychotic Disorders (2003) Medication selection, dosing, and dose equivalence. J Clin Psychiatry 64(suppl 12):21-41
Vartiainen E, Laatikainen T, Tapanainen H, Salomaa V, Jousilahti P, Sundvall J, Salminen M, Männistö S & Valsta L (2003) Suomalaisten sydän- ja verisuonitautien riskitekijät FINRISKI-tutkimuksessa 1982-2002. Suomen Lääkärilehti 58:4099-106.
Vreeland B, Minsky S, Menza M, Rigassio Radler D, Roemheld-Hamm B & Stern R (2003) A program for managing weight gain associated with atypical antipsychotics. Psychiatric Services 54(8):1155-1157.

74
Wen F & Tan J (2003) Effects of phenothiazine drugs on serum levels of apoplipoproteins and lipoproteins in schizophrenic subjects. Acta Pharmacol Sin 24 (10):1001-1005
Werneke U, Taylor D, Sanders TAB & Wessely S (2003) Behavioural management of antipsychotic-induced weight gain: a review. Acta Psychiatr Scand 108:252-259.
Wiltfang J, Schenk-Dapra B, Stiens G, Bleich S, Bandelow B, Müller P, Niedmann PD, Armstrong VW & Rüther E (2001) Clozapine-associated elevation of plasma cholinesterase. Eur Arch Psychiatry Clin Neurosci 251:269-271
Wirshing DA, Wirshing WC, Kysar L, Berisford MA, Goldstein D, Pashdag J, Mintz J & Marder SR (1999) Novel antipsychotics: comparison of weight gain liabilities. J Clin Psychiatry 62:347-349.
Wirshing DA, Boyd JA, Meng LR, Ballon JS, Marder SR & Wirshing WC (2002) The effects of novel antipsychotics on glucose and lipid levels. J Clin Psychiatry 63:856-865
Word Health Organization (1993) The ICD-10 Classification of mental and Behavioural Disorders. Diagnostic Criteria for Research. Geneva. Word Health Organization.
Yamada J, Sugimoto Y & Ujikawa M (1999) The serotonin precursor 5-hydroxy-tryptophan elevates serum leptin levels in mice. Eur J Pharmacol 383:49-51.