-
Case #114 yo white maleReferred after hypercholesterolemia
detected on routine screening because of fathers
hypercholesterolemiaTotal cholesterol 290 mg/dl, repeat 286
mg/dlTriglycerides 108 mg/dl, HDL cholesterol 55 mg/dl, LDL
cholesterol 209 mg/dlOtherwise well/No current medicationsPhysical
exam, BP WNL, 50th percentile for Ht/WtNo xanthelasma, cutaneous
xanthomata, or Achilles tendon thickening
-
Case #1ActivitySoccer, swimming, bikingDietFamily already
attempting to reduce dietary fat and cholesterol after learning of
elevated cholesterol in patient and fatherSocialNo
tobacco/alcohol/substance abuseBoth parents come with patient to
clinic, seem very supportive
-
Case #1Dietary assessment3-day dietary recall to determine
average daily intakeTotal calories: 2000 kcal/dayComposition as %
of total caloriesProtein: 22%Fat: 28%Saturated: 6%Monounsaturated:
14%Polyunsaturated: 8%Carbohydrate: 49%Cholesterol content: 221
g/dayFiber: 31 g/day
-
Case #1
-
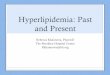
Xanthelasma Palpebrarum
-
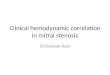
Xanthomata Tuberosa
-
Case #211 yo white maleReferred after hypercholesterolemia
detected after father was found to have hypercholestrolemia and
recent myocardial infarctionTotal cholesterol 254 mg/dl, repeat 250
mg/dlTriglycerides 102 mg/dl, HDL cholesterol 53 mg/dl, LDL
cholesterol 181 mg/dlOtherwise well/No current medicationsPhysical
exam, BP WNL, 50th percentile for Ht/WtNo xanthelasma, cutaneous
xanthomata, or Achilles tendon thickening
-
Case #2ActivityComputer games, TVBikingDietSome meals at home,
but often fast food, snacksNo effort yet to alter dietSocialNo
tobacco/alcohol/substance abuseParents are separated, lives with
mother, who works two jobs
-
Case #2Dietary assessment3-day dietary recall to determine
average daily intakeTotal calories: 2000 kcal/dayComposition as %
of total caloriesProtein: 16%Fat: 37%Saturated: 17%Monounsaturated:
15%Polyunsaturated: 5%Carbohydrate: 47%Cholesterol content: 373
g/dayFiber: 13 g/day
-
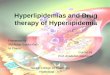
Case #249 yoMI59 yo hypertension66 yohealthy62 yo healthy36 yoCH
299MI 6 mos ago34 yoCH 159healthy34 yoMI6 yohealthyCH 2499
yohealthyCH 25511 yohealthyCH 250
-
Risk Factors for Atherosclerotic Heart
DiseaseHypercholesterolemiaSmokingHypertensionDiabetesSedentary
lifestyleMale SexFamily history of CHDAge (male > 45 yoa, female
> 55 yoa)
-
Evidence Relating Diet, Serum Cholesterol Level, and Coronary
Heart Disease
Animal studiesGenetic disorders, such as familial
hypercholesterolemia with elevated serum LDL cholesterol, are
associated with premature atherosclerosisEpidemiologic
studiesClinical trialsAutopsy studies
-
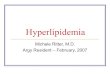
Dietary Saturated Fat and Cholesterol Intake and Serum Total
Cholesterol in Boys Aged 7-9 Years in Six Countries
-
Serum Cholesterol in Boys and Middle-Aged Men and CHD Mortality
Rates in Middle-Aged Men in Industrialized Countries
-
Coronary Primary Prevention Trial (CPPT)Hypercholesterolemic,
middle-aged menTreated with cholestyramine19% reduction in fatal
and/or non-fatal MI over 7 yearsA 25% reduction in serum
cholesterol level resulted in a 50% reduction in CHD risk
-
Controlled Angiographic Trials of Cholesterol LoweringSeveral
studies to date in adultsRegression of lesions in 16-47% with large
decreases in serum LDL cholesterol levels (34-48% reduction) for
2-5 yearsMain benefit may be slowing of progression of
atherosclerotic lesions
-
Why Intervene in ChildrenRole of hypercholesterolemia in
atherosclerosis well established in adultsChildren with elevated
cholesterol are more likely to have family members with elevated
levels and come from families with premature
atherosclerosisTrackingChildren with elevated serum cholesterol
levels are likely to have hypercholesterolemia later in lifeAutopsy
studies
-
Autopsy StudiesU.S. soldiers in Korean War (Enos et al,
1955)Gross coronary disease in 77% of subjects studiedMean age 22
yearsConfirmed in studies from Viet Nam WarHolman, 1961; Strong and
McGill, 1962; Stary, 1989Aortic fatty streaks are extensive in
childhoodCoronary fatty streaks appear in adolescenceFibrous
plaques appear in the second decade with progression into the
second decadeBogalusa StudyPDAY Study
-
Bogalusa StudyNEJM 338:1650, 1998N=93, 2-39 yoa
-
Pathobiological Determinants of Atherosclerosis in Youth
(PDAY)Multicenter post-mortem study in 1079 males, 364 females,
15-34 years of ageViolent deathArteries graded for atherosclerotic
lesions in aorta and right coronary arterySerum lipoproteins
measuredSerum thiocyanate measured as an index of smoking
Arterioscler Thromb Vasc Biol 17:95, 1997
-
PDAY ResultsExtent of surface area with fatty streaks and raised
lesions increased with age in all vesselsSerum VLDL plus LDL
cholesterol positively correlated with extent of fatty streaks and
raised lesions in all vesselsSerum HDL cholesterol negatively
correlated with extent of fatty streaks and raised lesions in all
vesselsSmoking associated with more extensive fatty streaks and
raised lesions in aorta
-
Pediatric Screening StrategiesScreen no one. Treat everyone with
diet.Screen only those children with a positive family history of
premature atherosclerotic disease or known hyperlipidemia.Screen
all children.
-
National Cholesterol Education Program (NCEP) Recommendations
for Pediatric Cholesterol ScreeningScreen after 2 years of ageAll
children with first degree relative with symptoms or diagnosis of
atherosclerotic disease, hyperlipidemia (serum cholesterol > 240
mg/dl), or sudden cardiac death before 55 years of age
-
Percentage of Children Aged 0-19 Years Who Would Be Screened,
and Percentage of Those with LDL Cholesterol 130 mg/dl Who Would Be
Identified, If the Presence of CV Disease or Various Levels of
Elevated Total Cholesterol in at Least One Parent Is Used to Select
Children for ScreeningThe Lipid Research Clinics Prevalence Study
(N=1042)
-
What to MeasureTotal cholesterol TriglyceridesHDL
cholesterolCalculate LDL cholesterolLDL cholesterol=total
cholesterol-HDL cholesterol-triglycerides/5Not accurate if
triglycerides > 400 mg/dlSome commercial labs now measure LDL
cholesterol directlyFasting not necessary for cholesterol
measurement alone, but overnight fast is required for profile
-
Classification of Total and LDL Cholesterol Levels in Children
and Adolescents
-
What to do After ScreeningIf total cholesterol > 95th %tile
(200 mg/dl), repeat with full profileIf confirmed, rule out
secondary causesScreen family membersStart Phase I diet and risk
factor reduction/preventionFollow-up and consider Phase II diet to
reduce LDL cholesterol to below 95th percentile
-
Borderline Cases70th-90th percentile (170-199 mg/dl)Repeat, if
average of two still borderline, get complete analysisIf LDL
cholesterol is borderline, start phase I diet and risk factor
reduction/preventionRecheck in 1 year
-
Abnormalities not detected by a simple cholesterol
measurementHypertriglyceridemiaHypoalphalipoproteinemia (low
HDL)Elevated apolipoprotein B level with normal LDL-C (excess
number of small LDL particles) Elevated lipoprotein(a)
levelElevated homocysteine level
-
Secondary Causes of
HyperlipidemiaEndocrineHypothyroidismDiabetes mellitusGlycogen
storage diseasePregnancyRenal DiseaseNephrotic syndromeObstructive
liver diseaseDrugsCorticosteroids, isotretinoin, thiazides,
anticonvulsants, b-blockers, anabolic steroids, oral
contraceptives
-
Familial Aggregation of HyperlipidemiaMonogenicHeterozygous
familial hypercholesterolemiaMutations in LDL receptor90% will have
CHD by 65 yoa4% of all cases of premature CHDFamilial Combined
HyperlipidemiaExpression variable (cholesterol and/or triglyceride
elevation) and may be delayed11% of all cases of premature
CHDPolygenicAccounts for majority of cases of premature
CHDExpression of a number of genes contributing to
hypercholesterolemia and atherosclerosis combined with
environmental factors
-
Dietary Fat in Children and Adolescents in the United StatesAge
1-19 years-14% of total calories from saturated fatAge 1-11
years-35% of total calories from fatAge 12-19 years-36% of total
calories from fat
-
Phase I DietNo more than 30% of total calories from fatLess than
10% of total calories from saturated fatLess than 300 mg of
cholesterol/dayTotal caloric intake appropriate for normal growth
and ideal body weight
-
Phase II DietNo more than 30% of total calories from fatLess
than 7% of total calories from saturated fatLess than 200 mg of
cholesterol/dayTotal caloric intake appropriate for normal growth
and ideal body weight
-
Criteria for Drug TherapyIn Children and Adolescents10 years of
age or olderAdequate trial of dietary therapy (6 mos-1 yr)LDL
cholesterol level 190 mg/dlLDL cholesterol level 160 mg/dl
andPositive family history of premature CVDor2 or more CVD risk
factors persisting after vigorousefforts to control or eliminate
these factors
-
Goals of Drug Therapyin Children and AdolescentsAcceptable-LDL
cholesterol level < 130 mg/dlIdeal-LDL cholesterol level <
110 mg/dlMonitor 6 weeks after starting therapy, then every 3
months until maximal effect, then every 6 monthsMonitor compliance,
lipids, growth, and appearance of side effects
-
Bile Acid SequestrantsCholestyramine (Questran), Colestipol
(Colestid)Only class of drugs approved for use in children to treat
hyperlipidemiaBind bile acids and enhance fecal elimination,
up-regulate hepatic bile acid synthesis from cholesterol, and
thereby up-regulate hepatic LDL receptorsWill often increase serum
triglyceride levels in mixed hyperlipidemiasNot absorbed, side
effects mainly constipation, bloatingCan lower fat-soluble vitamin
and folate levels, but usually not important clinicallyGritty,
sandy consistency; compliance a real problem
-
NCEP Treatment Guidelinesfor LDL-C Levels for Adults
Definite atherosclerotic disease
Two or more other risk factors
Initiation
level
(mg/dl)
Goal
(mg/dl)
No
No
> 190
< 160
No
Yes
> 160
< 130
Yes
Yes or No
> 130
-
HMG CoA Reductase InhibitorsStatinsCerivastatin
(BaycolR)Fluvastatin (LescolR)Atorvastatin (LipitorR)Lovastatin
(MevacorR)Pravastatin (PravacholR)Simvastatin (ZocorR)Decrease
hepatic cholesterol synthesis resulting in increased hepatic LDL
receptors with increased clearance of plasma LDL particles
-
HMG CoA Reductase InhibitorsDecrease serum LDL cholesterol
levelsModest increases in serum HDL-C levelsThe more potent
statins, atorvastatin, cerivastatin, and fluvastatin, also
significantly decrease triglyceride levels, possibly serving as
effective monotherapy in mixed hyperlipidemias
-
HMG CoA Reductase InhibitorsAdverse EffectsMyalgias, myopathy,
rhabdomyolysisRisk of rhabdomyolysis and acute renal failure
especially high with combined therapy with fibric acid derivatives,
niacin, cyclosporine, erythromycin, and azole antifungals
Transaminase elevationFetal toxicity
-
NiacinNiaspanR (extended release tablets)If equivalent dose of
crystalline niacin is substituted, toxicity will result, and
fulminant liver failure has been reportedDecreases total
cholesterol, LDL-C, and triglyceridesIncreases HDL-CEscalating dose
titration to minimize side effects, particularly flushing
-
NiacinAdverse EffectsFlushingUsually transient and improves with
duration of therapyASA or NSAID prior to dosing may minimizeAvoid
ingestion of alcohol or hot drinks around time of dosingIf
discontinued for an extended period, must escalate and titrate
dosing again
-
NiacinAdverse EffectsTransaminase elevationRare cases of
rhabdomyolysis with concomitant HMG CoA reductase inhibitorsGlucose
intoleranceUric acid elevationMonitor anticoagulant therapyUse with
caution in unstable angina/recovering MI, especially with
concomitant vasoactive drugs
-
Fibric Acid DerivativesClofibrate (AtromidR), gemfibrozil
(LopidR), fenofibrate (TricorR)Decrease triglycerides, increase
HDL-C levelsSerum triglycerides > 1000 mg/dl associated with
significant risk of pancreatitisNot to be used to treat low HDL-C
as only lipid abnormalityIncreased incidence of non-coronary and
age-adjusted all-cause mortality in studies (WHO)
-
Fibric Acid DerivativesAdverse EffectsMyalgias, myopathy,
rhabdomyolysisRisk of rhabdomyolysis and acute renal failure
especially high with combined therapy with statinsCholelithiasis
Transaminase elevation and Hgb/WBC depressionNeed to reduce
anticoagulant doseIncreased risk of liver and testicular
malignancyFetal toxicity
-
Family Approach to Treating Hyperlipidemia and Reducing
Cardiovascular Risk Affected family members generally have same
lipid disorderTeam Approach-Specialists from pediatrics, adult
medicine, and nutritionPrograms are designed to fit into the family
routine and alter eating habits and physical activityFamilies
develop an internal support structure which improves compliance
Note that this individual was referred for evaluation and
treatment after hypercholesterolemia was detected on a screening
test because of the fathers hypercholesterolemia. Later in this
seminar, we will discuss indications for cholesterol screening in
children and adolescents. Note that this patient had no physicial
findings of hypercholesterolemia, such as xanthelasma, cutaneous
xanthomata, or Achilles tendon thickening.Note that this family has
already taken the initiative to reduce dietary fat and cholesterol
in their diet after learning of the hypercholesterolemia in the
patient and his father.Notice that this patient has already
modified his dietary fat intake to a desirable level. Also, his
cholesterol and fiber intake are in the desirable range.Examination
of the patients pedigree demonstrates that the hypercholesterolemia
appears to be inherited on the patients fathers side of the family.
Notice that the paternal grandfather died at 53 yoa with a
myocardial infarction. The patients father, although healthy, has
an elevated cholesterol at 299 mg/dl. Finally, notice that the
patient has two female siblings who are healthy but have not had
their cholesterol measured. This pattern of inheritance would be
consistent with familial hypercholesterolemia, which is due to
mutations in the LDL receptor.The individual in this slide has
xanthelasma palpebrarum. These are cholesterol deposits in the skin
in the inner canthus of the eyes. This finding is rarely seen in
children and adolescents, but is more often seen in older adults
with long- standing hypercholesterolemia. This slide shows
xanthomata tuberosa on the elbows. Again, such a finding would be
extremely rare in children and adolescents, but is sometimes seen
in older individuals with hyperlipidemia. Notice that this patient
was referred after hypercholesterolemia was detected on screening
after the father was found to have not only hypercholesterolemia,
but had also had a recent myocardial infarction. Notice that this
family has not made any effort so far to improve their dietary
habits and frequently ingest fast food and other high-calorie,
high-fat snacks. The fact that the parents are separated with the
patient living with the mother, who works two jobs, probably
contributes to the difficulty in making dietary changes.Notice that
this patient ingests too high a percentage of total calories as fat
with too high a proportion of saturated fat. Also, the cholesterol
intake is excessive.Examination of this patients pedigree shows
that the hypercholesterolemia is inherited from the fathers side of
the family. Notice that the paternal grandfather died of a
myocardial infarction at 49 yoa. Also note that the father has
hypercholesterolemia and has had a recent myocardial infarction.
This patient has two healthy younger sisters. Note that both have
been screened and both have hypercholesterolemia. This pattern of
inheritance would be consistent with familial hypercholesterolemia,
due to mutations in the LDL receptor gene.Remember that
hypercholesterolemia is only one of several risk factors for
atherosclerotic cardiovascular disease. Pediatricians are in a
unique position to intervene to prevent many of these risk factors
later in life.Numerous animal studies have demonstrated that when
animal models are made hypercholesterolemic, they readily develop
atherosclerosis. Genetic disorders, such as familial
hypercholesterolemia and others, are clearly associated with
atherosclerosis and coronary heart disease. There have been a
number of epidemiologic studies associating diet with serum
cholesterol levels and coronary heart disease. We will discuss some
of these. Both primary and secondary intervention clinical trials
in adults with hyperlipidemia have clearly demonstrated a
beneficial effect of treatment of hyperlipidemia on serum
cholesterol levels and coronary heart disease. Finally, autopsy
studies have demonstrated that atherosclerosis has its beginnings
early in life and is clearly related to serum lipid levels and
family history of early atherosclerotic disease.This slide shows
that on an international scale, as dietary intake of saturated fat
and cholesterol increases, so does the serum cholesterol level in
children.Note that, as the serum cholesterol level in both boys and
men increases, so does the CHD mortality in middle-aged men in
several industrialized countries. Notice that the CHD mortality is
particularly high in Hungary and Poland. This is probably due to
other genetic and environmental factors impacting on the
development of atherosclerosis. Dr. Gerald Berenson has conducted a
large-scale population study for a number of years on a biracial
cohort of children in Bogalusa, LA. His studies have yielded unique
and important information on cardiovascular risk factors in
children and adolescents. Autopsy studies on the enrolled subjects
are an important part of his ongoing research. In this recent paper
in the New England Journal of Medicine, you can see as the number
of risk factors increases, the percent surface involvement with
both fatty streaks, the early lesions of atherosclerosis, and
mature fibrous plagues increases in both the aorta and coronary
arteries of young individuals. There are three possible approaches
to screening for hypercholesterolemia in children. One strategy is
to screen no one and treat everyone with diet. Certainly, this is
an important population-based approach that is advocated by the
American Heart Association and other agencies. Another approach is
to screen only those children with a positive family history of
premature atherosclerotic disease or known hyperlipidemia. This
approach would ensure that those individuals with a familial
hyperlipidemia, who may require more intensive therapy for their
disorder, would be identified. The third possible approach would be
to screen all children regardless of family history. This is the
approach advocated for adults. It is also an approach taken by many
pediatricians for screening children. Several studies have shown
that relying on family history will frequently miss individuals
with hyperlipidemia. This is often due to a fragmented family
structure, as well as the inability of many parents to recall or
have knowledge of illness in other family members. However, we do
not know the true risk of premature cardiovascular disease in
individuals with hypercholesterolemia who do not have a true
positive family history of premature atherosclerotic disease. The
NCEP, as well as the American Heart Association and the American
Academy of Pediatrics, have recommended that cholesterol screening
be undertaken after two years of age and in all children with a
first degree relative with symptoms or diagnosis of atherosclerotic
disease, hyperlipidemia with a serum cholesterol >240 mg/dl or
sudden cardiac death before 55 years of age.These data represent
the rationale for screening those children who have family members
with a serum cholesterol level >240 mg/dl. At this cholesterol
level in the parent, only about 25% of children would be screened
with a sensitivity of identification of those children with an
elevated LDL cholesterol being about 40%. This cut-off represents a
compromise between a higher sensitivity and the fact that to obtain
a higher sensitivity, an excessive number of children would have to
be screened.Note that single gene defects account for only about
15% of all cases of premature coronary heart disease. The other
cases are accounted for by polygenic disorders in which expression
of a number of genes contributing to hypercholesterolemia and
atherosclerosis interact with environmental factors to cause
hyperlipidemia and premature coronary heart disease.Th institution
of a Phase I diet in children does require caution. There have been
case reports of younger children presenting with failure to thrive
due to overzealous dietary restriction by the parents. Any
interventional diet should provide a total caloric intake
appropriate for normal growth and development and maintenance of
ideal body weight in children. Also, vitamin and micronutrient
intake should be adequate.The Phase II diet is more restrictive
than the Phase I diet, and even greater attention should be paid to
ensuring adequate total caloric intake in children.The family
approach to treating hyperlipidemia and reducing cardiovascular
risk represents the best approach and addresses changes in, not
only the diet, but the lifestyle of all family members, both
hyperlipidemic and unaffected. This is the optimum approach, but
does require trained personnel and resources that may not be
available in many institutions. An important point in the treatment
of hypercholesterolemia in children is the fact that, since drug
therapy is not recommended under the age of 10, dietary therapy and
increased activity and exercise represent the mainstay of
treatment. It is very important not to let parents have unrealistic
expectations with regard to what these interventions can achieve
with the serum cholesterol level. Under the best conditions, there
may be only a 10 or 15% reduction in the serum cholesterol level,
even though the family is following all of your recommendations.
This is particularly true in the monogenic disorders. It is
important to let the family know that this is what you expect at
the present time and that, when their child is older, there is the
option of drug therapy which will likely lower the lipid levels to
the normal range.