Embed Size (px)
Citation preview


PRIMARY HYPERHIDROSISPRIMARY HYPERHIDROSIS Disease or AnxietyDisease or Anxiety
N. I. PERINPANAYAGAM M.D, FRCS,N. I. PERINPANAYAGAM M.D, FRCS, FACSFACS
Professor of NeurosurgeryProfessor of Neurosurgery
NYU Medical CenterNYU Medical Center
New York, NYNew York, NY

PRIMARY PRIMARY HYPERHIDROSISHYPERHIDROSIS
Diagnosis of Primary Diagnosis of Primary HHHH -- Start in the Start in the
11stst or 2or 2ndnd decades of life & should be decades of life & should be
Bilaterally SymmetricalBilaterally Symmetrical
Occurs in 2.8% of the US populationOccurs in 2.8% of the US population
Typically affects the hands, Typically affects the hands, axillaeaxillae, feet , feet
& less commonly the face (facial & less commonly the face (facial
flushing)flushing)

INHERITANCEINHERITANCE
Primary HH is reported to be inherited Primary HH is reported to be inherited
as an Autosomal dominant gene, with as an Autosomal dominant gene, with
incomplete penetranceincomplete penetrance

PRIMARY HHPRIMARY HH
Has Psychological, Social, Economic & Has Psychological, Social, Economic &
Occupational implicationsOccupational implications
Most patients present in their teens and Most patients present in their teens and
twentiestwenties
Majority of pts. are on AntiMajority of pts. are on Anti--Anxiolytic Anxiolytic
drugsdrugs

TYPICAL PRESENTATIONTYPICAL PRESENTATION
PalmarPalmar, , AxillaryAxillary & plantar & plantar HHHH
PalmarPalmar HHHH onlyonly
AxillaryAxillary HHHH only, with or without only, with or without
BromhidrosisBromhidrosis
Facial Facial HHHH / Gustatory sweating with or / Gustatory sweating with or
without facial flushingwithout facial flushing
Plantar Plantar HHHH

DIAGNOSISDIAGNOSIS
Primary Primary vsvs Secondary Secondary HHHH
Endocrine workEndocrine work--up up –– Hyperthyroidism, Hyperthyroidism, HyperpituitarismHyperpituitarism, Dumping syndrome, , Dumping syndrome, Alcohol & drug withdrawal, Alcohol & drug withdrawal, menopause, Diabetes, febrile illnesses, menopause, Diabetes, febrile illnesses, paraplegia, stroke, anxiety etcparaplegia, stroke, anxiety etc
Objectively quantify degree/severity of Objectively quantify degree/severity of HHHH & the impact on ADL& the impact on ADL
Family historyFamily history

PATIENTS WITH PRIMARY HHPATIENTS WITH PRIMARY HH
Excessive sweating independent of Excessive sweating independent of
ambient temperature, worse with ambient temperature, worse with
anxiety!anxiety!
Excessive hand sweating leaves Excessive hand sweating leaves
puddles of sweat, avoid shaking handspuddles of sweat, avoid shaking hands
AxillaryAxillary sweaters change shirts 3sweaters change shirts 3--4 4
times/day, wear only darker clothestimes/day, wear only darker clothes
Plantar sweaters cannot wear sandals Plantar sweaters cannot wear sandals
or slippers, wear thick sox & closed or slippers, wear thick sox & closed
shoesshoes

NONNON--SURGICAL TREATMENTS FOR SURGICAL TREATMENTS FOR
PRIMARY HHPRIMARY HH
Antiperspirants (Aluminum Chloride Antiperspirants (Aluminum Chloride ––
DrysolDrysol))
AnticholinergicsAnticholinergics –– ((RobinulRobinul))
IontophoresisIontophoresis
Therapies based on BioTherapies based on Bio--feedbackfeedback
BotulinumBotulinum toxin “A” Injectiontoxin “A” Injection

IONTOPHORESIS (Drionic & Fischer)IONTOPHORESIS (Drionic & Fischer)
Immersing hands or feet in tap water Immersing hands or feet in tap water
through which a 15through which a 15--20ma direct current 20ma direct current
is passedis passed
Iontophoresis to deliver Iontophoresis to deliver
anticholinergicsanticholinergics
RecomRecom--20mts on days 1,2,4,7,10,15,22 20mts on days 1,2,4,7,10,15,22
& maintenance sessions every 4 wks& maintenance sessions every 4 wks
Side effects burning, tingling, skin Side effects burning, tingling, skin
irritation, erythemairritation, erythema

BOTULINUM TOXIN INJECTIONSBOTULINUM TOXIN INJECTIONS
IntraIntra--dermal botox blocks the release of dermal botox blocks the release of AchAch
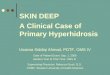
The area to be treated is outlined using The area to be treated is outlined using the “starchthe “starch--iodine test” the area is iodine test” the area is marked out into 1.5cm squares and marked out into 1.5cm squares and 2units of Botox is injected 2units of Botox is injected intradermally to each square intradermally to each square
(max dose 100units)(max dose 100units)
Works best for axilla and less well in Works best for axilla and less well in the hands and feet the hands and feet

MEDICAL MANAGEMENTMEDICAL MANAGEMENT
AntiperspirantsAntiperspirants –– 11stst line of Rx line of Rx --Palmar, Palmar, Plantar, Axillary HH (DrysolPlantar, Axillary HH (Drysol-- Aluminum Aluminum based)based)
IontophoresisIontophoresis –– nonnon--responsive to responsive to above Palmar & Plantarabove Palmar & Plantar
Anticholinergics Anticholinergics –– Robinul (1mg tid) Robinul (1mg tid) palmar, plantar, axillary ( 1palmar, plantar, axillary ( 1stst line in line in whole body HH & facial HH)whole body HH & facial HH)
Botox InjectionsBotox Injections –– Axillary HH not Axillary HH not responsive to 1 & 2 (not recom. In responsive to 1 & 2 (not recom. In palmar palmar –– muscle wasting & hand muscle wasting & hand weakness)weakness)

STARCH IODINE TEST SHOWING STARCH IODINE TEST SHOWING
LOCATION OF EXCESSIVE SWEATINGLOCATION OF EXCESSIVE SWEATING

SURGICAL TREATMENT OF SURGICAL TREATMENT OF
PRIMARY HHPRIMARY HH
Excision of Excision of ApocrineApocrine glands glands ––AxillaAxilla
(liposuction)(liposuction)
RadioRadio--frequency frequency lesioninglesioning of the of the
Sympathetic ganglia (Imprecise)Sympathetic ganglia (Imprecise)
Endoscopic Thoracic Endoscopic Thoracic SympathectomySympathectomy

Isolates the sympathetic supply to the Isolates the sympathetic supply to the
sweat glandssweat glands
Immediately stops sweating, hands after Immediately stops sweating, hands after
sympathectomysympathectomy slightly warmer & pinkslightly warmer & pink
Approaches Approaches ––
SupraSupra--clavicularclavicular; Trans; Trans--axillaryaxillary
PosteroPostero--lateral thoracic (midline lateral thoracic (midline
approach)approach)
Endoscopic Thoracic Endoscopic Thoracic SympathectomySympathectomy
THORACIC SYMPATHECTOMY FOR THORACIC SYMPATHECTOMY FOR
HHHH

INTERNATIONAL NOMENCLATURE FOR INTERNATIONAL NOMENCLATURE FOR
SYMPATHECTOMY SURGERY(ISSS)SYMPATHECTOMY SURGERY(ISSS)
Notation of level or levels where Notation of level or levels where sympathetic chain isolated sympathetic chain isolated
Rib basedRib based -- R2R2, , R3R3, , R4R4, , R5R5
Ganglion basedGanglion based –– G2G2 ((R2R2--3) 3) G3G3((R3R3--4), 4), G4G4((R4R4--5), 5), G5G5((R5R5--6)6)
Old terminology Old terminology –– SympathicotomySympathicotomy / / T2T2, , T3T3, , T4T4, , T5T5 SympathectomySympathectomy. .
T2T2 –– ((R2R3R2R3//G2G2), ), T3T3 –– ((R3,R4R3,R4//G3G3),),
T4T4--((R4,R5R4,R5//G4G4), ), T5T5 –– ((R5,R6R5,R6//G5G5))

INDICATIONS FOR ENDOSCOPIC INDICATIONS FOR ENDOSCOPIC
THORACIC SYMPATHECTOMY(ETS)THORACIC SYMPATHECTOMY(ETS)
Severe Palmar with Mod. Axillary, & Severe Palmar with Mod. Axillary, &
Plantar Hyperhidrosis (failed medical Plantar Hyperhidrosis (failed medical
Rx)Rx)
Isolated AxillaryIsolated Axillary
Facial Flushing or RednessFacial Flushing or Redness
Reflex Sympathetic Dystrophy (CRPS)Reflex Sympathetic Dystrophy (CRPS)
Raynaud’s SyndromeRaynaud’s Syndrome
Idiopathic cardiac arrythmiasIdiopathic cardiac arrythmias--childrenchildren

BILATERAL ENDOSCOPIC THORACIC BILATERAL ENDOSCOPIC THORACIC
SYMPATHECTOMYSYMPATHECTOMY--ETSETS

DIVISION OF THE TRUNK AT R3,R4 DIVISION OF THE TRUNK AT R3,R4
ISOLATES THE 3ISOLATES THE 3rdrd GANGLIONGANGLION

CLINICAL MATERIALS & METHODSCLINICAL MATERIALS & METHODS
Retrospective review of 185 patients for Retrospective review of 185 patients for
a total of 370 sympathectomies.a total of 370 sympathectomies.
138 patients were available for follow138 patients were available for follow--
up up
(very mobile young Pt. population)(very mobile young Pt. population)
Chwajol M, Barrenechea IJ, Chakraborty S, Ichiba T, Lesser JB, Connery
CP, Perin NI, Impact of symptomatic improvement, recurrence and
compensatory hyperhidrosis on patient satisfaction after endoscopic
thoracic sympathectomy. Neurosurgery. 2008; 64:511-518.

RESULTS RESULTS -- 11
ETS for HH ETS for HH -- 182pts, 182pts,
ETS for facial Flushing ETS for facial Flushing -- 3pts.3pts.
Avg. time from ETS to questionnaire Avg. time from ETS to questionnaire --
1.3yrs1.3yrs
Of the 138 patients, 81 females (59%) & Of the 138 patients, 81 females (59%) &
57 males(41%)57 males(41%)
Age range 10 Age range 10 -- 67yrs. (mean 28, SD 8.9)67yrs. (mean 28, SD 8.9)

RESULTS WITH ETS FOR HHRESULTS WITH ETS FOR HH
98% reduction of sweating in Palmar 98% reduction of sweating in Palmar
HHHH
80% Reduction in Axillary HH80% Reduction in Axillary HH
60% Reduction in Plantar HH 60% Reduction in Plantar HH
Facial Flushing / Facial sweating Facial Flushing / Facial sweating
inconsistent responseinconsistent response
Recurrence 1Recurrence 1--2% (Higher in patients 2% (Higher in patients
treated for Axillary HH)treated for Axillary HH)

COMPENSATORY COMPENSATORY HYPERHIDROSISHYPERHIDROSIS
Major source of dissatisfaction after Major source of dissatisfaction after ETS for HHETS for HH
Occurrence Occurrence -- All Pts. have some degree All Pts. have some degree of compensatory HH following ETS, of compensatory HH following ETS, especially during exercise and hot especially during exercise and hot weatherweather
However Intractable Compensatory HH, However Intractable Compensatory HH, occurs in less than 5% of patientsoccurs in less than 5% of patients
Incidence of the severe Intractable CHH Incidence of the severe Intractable CHH has decreased with going to lower has decreased with going to lower levels in the chain (R3,R4levels in the chain (R3,R4--3G,R4,R53G,R4,R5--4G)4G)

OCCURRENCE OF COMPENSATORY HHOCCURRENCE OF COMPENSATORY HH
Almost all Pts. experienced some Almost all Pts. experienced some
degree of degree of CHHCHH during exercise & hot during exercise & hot
weather(130 of 138 = 94%)weather(130 of 138 = 94%)
CHHCHH occurred mostly in the back, lower occurred mostly in the back, lower
chest, abdomen & thighschest, abdomen & thighs
18 had one body area affected, 41 had 18 had one body area affected, 41 had
two areas, 35 three areas & 36 had four two areas, 35 three areas & 36 had four
areas affectedareas affected

SEVERITY OF COMPENSATORY HH & SEVERITY OF COMPENSATORY HH &
POSSIBLE PREDISPOSITIONPOSSIBLE PREDISPOSITION
AgeAge of the patientof the patient--Tendency older ptsTendency older pts
PrePre--operative operative BMIBMI--Tends higher with Tends higher with
higher BMIhigher BMI
# of levels# of levels of the sympathetic chain of the sympathetic chain
/ganglion divided/ganglion divided-- Tends higher with more Tends higher with more
levelslevels
Occurrence of Compensatory Occurrence of Compensatory HHHH related related
to to upper versus lower ganglionupper versus lower ganglion isolationisolation
Shown to reduce severe Shown to reduce severe CHHCHH ( ( T2T2 to to T3T3 & &
T4T4))

CURRENT PROTOCOL FOR CURRENT PROTOCOL FOR
SYMPATHECTOMYSYMPATHECTOMY IN IN HHHH
Presently all patients with Presently all patients with PalmarPalmar HHHH
receive a receive a T3T3 Ganglion isolation Ganglion isolation
((R3,R4R3,R4//3G3G))
Patients with Patients with PalmarPalmar & & AxillaryAxillary HHHH ––
T3GT3G & & T4GT4G ((R3R3--R4R4//3G3G, , R4R4--R5R5//4G4G))
Patients with facial Patients with facial HHHH & Facial & Facial
Flushing Flushing –– T2GT2G ((R2R2--R3R3//2G2G))

SATISFACTION RATES REPORTED SATISFACTION RATES REPORTED
ON THE QUESTIONNAIREON THE QUESTIONNAIRE
Very Satisfied 88 pts (64%)Very Satisfied 88 pts (64%)
Somewhat Satisfied 36 pts (26%)Somewhat Satisfied 36 pts (26%)
Somewhat Unsatisfied 9 pts (7%)Somewhat Unsatisfied 9 pts (7%)
Regretted having the surgery Regretted having the surgery 5pts5pts (3%)(3%)
Satisfaction rates highest in patients with Satisfaction rates highest in patients with severe severe palmarpalmar HHHH, and lowest in patients , and lowest in patients with isolated severe with isolated severe AxillaryAxillary HHHH
Results in Facial flushing & facial sweating Results in Facial flushing & facial sweating inconsistantinconsistant
Some improvement in Plantar Some improvement in Plantar HHHH (60%)(60%)

REVERSIBILITYREVERSIBILITY
Cutting or Clipping of the Sympathetic Cutting or Clipping of the Sympathetic chainchain
Possible to remove the clips in very Possible to remove the clips in very severe Compensatory severe Compensatory HHHH to revert to to revert to original state original state –– Inconclusive evidence Inconclusive evidence of reversalof reversal
Nerve Grafting for reversal ( Nerve Grafting for reversal ( suralsural vsvs IntercostalIntercostal nerve for grafting)nerve for grafting)--
Latif MJ, Afthinos JN , Connery CP, Perin NI, Bhora FY, Chwajol M, Todd GJ, Belsley SJ,
Robotic intercostal nerve graft for reversal of thoracic sympathectomy: a large animal feasibility model. Int J MedRobotics Comput Assist Surg. 2008; 4:258-226.

ROBOTIC INTERCOSTAL NERVE GRAFTROBOTIC INTERCOSTAL NERVE GRAFT
IRB to perform IRB to perform -- Robotic Intercostal Robotic Intercostal
nerve to sympathetic trunk grafts, nerve to sympathetic trunk grafts,
to reverse Intractable to reverse Intractable
compensatory sweating.compensatory sweating.

CONCLUSION CONCLUSION
Sympathectomy for intractable Palmar Sympathectomy for intractable Palmar HH is a very effective treatmentHH is a very effective treatment
There was a 98% reduction of hand There was a 98% reduction of hand sweating, an 80% reduction of Axillary sweating, an 80% reduction of Axillary sweating & a 60% reduction of plantar sweating & a 60% reduction of plantar sweating after upper Thor.ETSsweating after upper Thor.ETS
94% of patients in our series developed 94% of patients in our series developed some degree of CHH. There was a some degree of CHH. There was a statistically significant association statistically significant association between advancing age & CHH(p=0.02), between advancing age & CHH(p=0.02), Higher BMI showed a trend towards Higher BMI showed a trend towards increased CHH (p=0.14)increased CHH (p=0.14)

CONCLUSION CONCLUSION
Higher satisfaction rates were noted in Higher satisfaction rates were noted in Pts. treated for Palmar (100%) even Pts. treated for Palmar (100%) even with asso. CHH vs. Axillary HH(73%). with asso. CHH vs. Axillary HH(73%). Overall satisfaction rate in both groups Overall satisfaction rate in both groups was 92% at one year.was 92% at one year.
With sectioning of the Sympathetic With sectioning of the Sympathetic trunk from T2G to T3G & T4G for trunk from T2G to T3G & T4G for palmar HH &, T4G,T5G for axillary HH palmar HH &, T4G,T5G for axillary HH has significantly reduced the incidence has significantly reduced the incidence of severe CHHof severe CHH