Embed Size (px)
Citation preview

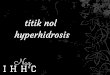
Figure e-1 Anisocoria with unilateral hyperhidrosis ipsilateral to the larger pupil involving forehead (A) and chest (B).

Appendix e-1 Further discussion regarding mechanism of anisocoria In the case presented, we propose that the mechanism is a primary unilateral, alternating, sympathetic overactivity leading to a compensatory contralateral sympathetic underactivity, rather than the more commonly seen primary sympathetic underactivity seen in Horner’s syndrome. It is reasonable to ask why the features seen in this patient could not be explained by alternating, transient Horner’s syndrome due to damage to the sympathetic tracts caused by his injury. In response to this question, we recognise that the assessment of pupils relies on a comparison between the two sides and so it can be difficult to provide incontestable proof about the absolute, as opposed to relative, over/normal/under-activity of each side. However, in this particular case, we can use several features to provide an insight the complex pathophysiology. Firstly, any explanation needs to account for the dynamic, alternating nature of the pupillary dysfunction, with no abnormality of the pupils identifiable between episodes. Secondly, the mechanism needs to explain how the episodes of anisocoria coincide with other features of autonomic dysreflexia in which there is evidence of unilateral eccrine sympathetic overactivity ipsilateral to the larger pupil. It is certainly possible that damage to the sympathetic tracts bilaterally may be a factor in this patient’s condition. However, there are several reasons against his condition being purely the result of a bilateral incomplete Horner’s syndrome. Firstly, we could find no evidence of sympathetic tract dysfunction between episodes. Secondly, this explanation would be inconsistent with the cocaine eye drop test, which is the established gold standard test for the pharmacological diagnosis of Horner’s syndrome. Whilst apraclonidine is reportedly as sensitive,e1 there are theoretical concerns that it may not be reliable in all circumstances.e2 Thirdly, it remains unclear how the occurrence of autonomic dysreflexia would transiently unmask these putative incomplete sympathetic lesions on alternate sides. The paper by Cragg et al. hypothesizes that this may occur due to an asymmetrically-distributed rise in intramedullary pressure during the episode of dysreflexia-induced hypertension selectively compromising sympathetic output.1 This is not an unreasonable explanation for an isolated, unilateral event but it is harder to believe this may occur recurrently, on alternate sides, and in a way that the side affected is related to the side of a noxious stimulus. It seems to us that a more plausible explanation is that the excessive sympathetic activity above the level of the lesion, that is a well-established feature of autonomic dysreflexia, may simply also involve the output to the sympathetic pupillary pathway. In this patient who experiences a unilateral form of autonomic dysreflexia, the sympathetic pupillary pathway may be stimulated unilaterally, resulting in a dilated pupil ipsilateral to the side of the flushing or sweating. Whilst the cocaine test confirmed that there was intact sympathetic innervation to both pupils, the apraclonidine test, somewhat confusingly, indicated there was a denervation hypersensitivity response, more pronounced in the miotic pupil, which we propose is due to a partial compensatory decrease in sympathetic tone on the contralateral side.

References
e-1. Freedman KA, Brown SM. Topical apraclonidine in the diagnosis of suspected Horner syndrome. J Neuroophthalmol. 2005;25(2):83-5.
e-2 Kardon R. Are we ready to replace cocaine with apraclonidine in the pharmacologic diagnosis of Horner syndrome? J Neuroophthalmol. 2005;25(2):69-70.
Table e-1 The action, rationale and interpretation of the pharmacological eye drop testing
used in this case
Cocaine
Action Cocaine acts by blocking the reuptake of norepinephrine (NE) that has been released into the sympathetic nerve junctions of the iris dilator muscle.
Diagnostic Use Used as the gold standard pharmacological test for Horner’s syndrome.
Findings Normal pupil: Blockade of noradrenaline update excess NE acting on iris
dilator mydriasis Horner’s pupil: Interruption to the sympathetic pathway results in a lack of
NE release no effect on pupil size
Apraclonidine
Action Apraclonidine is an α‐adrenoreceptor agonist.
Diagnostic Use Used as an alternative pharmacological test for Horner’s test. This agent is generally more easily available and less costly than cocaine.
Findings Normal pupil: Weak α1 adrenergic properties mild pupillary dilatation
Horner’s pupil: Loss of sympathetic innervation increased iris dilator α1‐
receptors hypersensitivity of Horner’s pupil to apraclonidine dilation of Horner’s pupil more than the normal side
Pilo
carpine
Action Pilocarpine is a muscarinic agonist.
Diagnostic Use Used as a parasympathetomimetic agent at the dose of 0.125% in the diagnosis of Adie’s tonic pupil (also used at higher dose to distinguish between parasympathetic antagonist exposure and 3rd nerve palsy)
Findings Normal pupil: Unreactive to 0.125% pilocarpine
Adie’s pupil: Parasympathetic denervation hypersensitivity to
pilocarpine pupillary constriction