Embed Size (px)
Citation preview

©2005 AWHONN
Hyperbilirubinemia in the Hyperbilirubinemia in the Neonate: Risk Assessment, Neonate: Risk Assessment, Screening and ManagementScreening and Management
Second EditionSecond Edition

©2005 AWHONN
ObjectivesObjectives
Summarize the mechanisms of bilirubin production and clearanceSummarize the mechanisms of bilirubin production and clearance
Describe a systematic process to assess and monitor neonatal Describe a systematic process to assess and monitor neonatal hyperbilirubinemiahyperbilirubinemia
Identify infants at risk for severe hyperbilirubinemiaIdentify infants at risk for severe hyperbilirubinemia
Identify prevention strategies for atIdentify prevention strategies for at--risk infantsrisk infants
Describe the recommended treatment modalities for severe Describe the recommended treatment modalities for severe hyperbilirubinemiahyperbilirubinemia
Summarize the current consensus guidelines for early interventioSummarize the current consensus guidelines for early intervention, treatment, n, treatment, and followand follow--up of neonates at risk for severe hyperbilirubinemiaup of neonates at risk for severe hyperbilirubinemia
Identify resources for staff and family education related to neoIdentify resources for staff and family education related to neonatal jaundice natal jaundice and hyperbilirubinemiaand hyperbilirubinemia

©2005 AWHONN
HyperbilirubinemiaHyperbilirubinemia
©2005 AWHONN
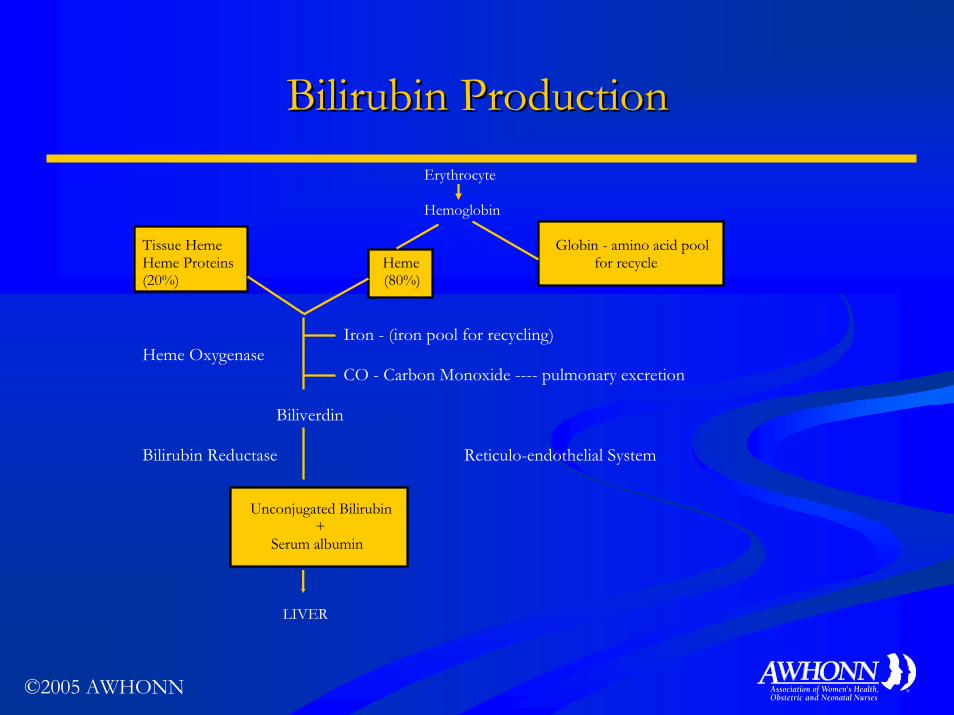
Bilirubin ProductionBilirubin Production Erythrocyte
Hemoglobin Tissue Heme Globin - amino acid pool Heme Proteins Heme for recycle (20%) (80%) Iron - (iron pool for recycling) Heme Oxygenase
CO - Carbon Monoxide ---- pulmonary excretion Biliverdin Bilirubin Reductase Reticulo-endothelial System Unconjugated Bilirubin + Serum albumin
LIVER

©2005 AWHONN
Types of BilirubinTypes of Bilirubin
Conjugated Conjugated -- directdirectWaterWater--solublesoluble
Easily excreted in urine Easily excreted in urine and stooland stool
Less toxic formLess toxic form
Requires ORequires O22 and glucoseand glucose
UnconjugatedUnconjugated -- indirectindirectFat or nonFat or non--water water soluble soluble
Potentially more toxic Potentially more toxic
Bound vs. unbound to Bound vs. unbound to albuminalbumin
Clinical management decisions are based on total serum bilirubin levels (by heel-stick sampling).

©2005 AWHONN
Bilirubin ClearanceBilirubin ClearanceUnconjugated Bilirubin
Liver Bilirubin glucuronide (conjugated bilirubin) β-glucuronidase Unconjugated Bilirubin Enterohepatic Circulation Bilirubin in Stools Gastro-intestinal tract

©2005 AWHONN
Development of Severe HyperbilirubinemiaDevelopment of Severe Hyperbilirubinemia
Increase in Increase in bilirubinbilirubin productionproductionSuch as Rh, ABO incompatibility, G6PD deficiency, Such as Rh, ABO incompatibility, G6PD deficiency, septicemia, extravascular blood, polycythemiasepticemia, extravascular blood, polycythemia
Decrease in Decrease in bilirubinbilirubin excretion excretion Bowel obstructions, hereditary defects, Bowel obstructions, hereditary defects, hypothyroidismhypothyroidism
Combination of both Combination of both Seen in prematurity, infectionSeen in prematurity, infection, G6PD deficiency, G6PD deficiency

©2005 AWHONN
Increases in Bilirubin Production: Increases in Bilirubin Production: HemolysisHemolysis
Genetic factorsGenetic factors
G6PD deficiencyG6PD deficiency
Erythrocyte enzymatic Erythrocyte enzymatic defectsdefects
Antibody mediatedAntibody mediated
Rh/ABO incompatibilityRh/ABO incompatibility
Acquired hemolytic Acquired hemolytic disordersdisorders
InfectionInfection
Drugs Drugs
Additional causeAdditional cause
PolycythemiaPolycythemia
Maternal diabetesMaternal diabetes
Extravasation of bloodExtravasation of blood

©2005 AWHONN
Decrease in Bilirubin ExcretionDecrease in Bilirubin Excretion
Increased Increased enterohepaticenterohepatic circulationcirculationBowel obstructionsBowel obstructions
Maternal liver diseaseMaternal liver disease
Hereditary defect Hereditary defect CriglerCrigler--Najjar, LuceyNajjar, Lucey--DriscollDriscoll
HypothyroidismHypothyroidism
HypopituitarismHypopituitarism

©2005 AWHONN
Combination of Combination of ↑↑ Production & Production & ↓↓ ExcretionExcretion
PrematurityPrematurity
InfectionInfectionBacterial sepsis, viral, protozoalBacterial sepsis, viral, protozoal
G6PD deficiencyG6PD deficiency

©2005 AWHONN
Major Risk Factors for Severe Major Risk Factors for Severe HyperbilirubinemiaHyperbilirubinemia
PrePre--discharge TSB/TcB in the highdischarge TSB/TcB in the high--risk zonerisk zone
Jaundice observed in the first 24 hoursJaundice observed in the first 24 hours
Blood group incompatibility, other known hemolytic disease Blood group incompatibility, other known hemolytic disease
Gestational age 35Gestational age 35--36 weeks36 weeks
Previous sibling received phototherapyPrevious sibling received phototherapy
Exclusive breastfeedingExclusive breastfeeding
Bruising/Bruising/cephalohematomacephalohematoma
Asian raceAsian race

©2005 AWHONN
Risk Factors for Risk Factors for Severe Severe HyperbilirubinemiaHyperbilirubinemia ((concon’’tt))
Minor risk factorsMinor risk factors
PrePre--discharge TSB/TcB in the highdischarge TSB/TcB in the high--intermediate risk zoneintermediate risk zoneGestational age 37Gestational age 37--38 weeks38 weeksJaundice observed before dischargeJaundice observed before dischargeMale genderMale genderMaternal age Maternal age >>25 years25 years
Decreased riskDecreased risk
TSB/TcB in the lowTSB/TcB in the low--risk zonerisk zoneGestational age Gestational age >>41 weeks41 weeksExclusive bottle feedingExclusive bottle feedingBlack raceBlack raceDischarged from hospital after 72 hoursDischarged from hospital after 72 hours

©2005 AWHONN
BreastfeedingBreastfeeding

©2005 AWHONN
Causes of Lactation FailureCauses of Lactation Failure
Lack of clinicianLack of clinician--initiated educationinitiated education
Lack of on site certified consultantsLack of on site certified consultants
Lack of documentation of infant latchingLack of documentation of infant latching
Inadequate measure of milk transferInadequate measure of milk transfer
Inappropriate followInappropriate follow--up and record of urine and stool pattern up and record of urine and stool pattern changeschanges
©2005 AWHONN
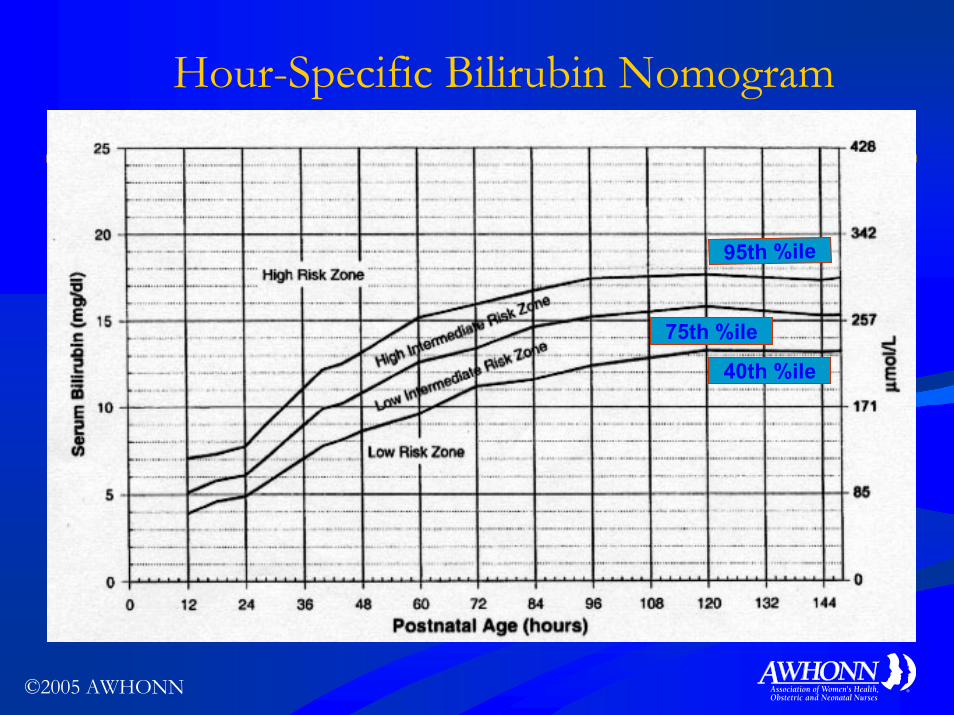
Hour-Specific Bilirubin Nomogram
95th %ile
75th %ile
40th %ile

©2005 AWHONN
Early Onset of Severe HyperbilirubinemiaEarly Onset of Severe Hyperbilirubinemia
Early OnsetEarly Onset
TSB/TcB values are >75TSB/TcB values are >75th th percentile prior to percentile prior to 72 hours of age72 hours of age
Acute/rapid rise in TSB/TcBAcute/rapid rise in TSB/TcB
↑↑ risk for potential adverse eventsrisk for potential adverse events
Frequent causes: ABO, Frequent causes: ABO, RhRh incompatibilityincompatibility

©2005 AWHONN
Late Onset Late Onset HyperbilirubinemiaHyperbilirubinemia
Late OnsetLate Onset
TSB/TcB values >95th percentile beyond TSB/TcB values >95th percentile beyond 72 hours of age72 hours of age
Frequent causes: BreastFrequent causes: Breast--fed infants with G6PD fed infants with G6PD deficiency, familial, or ethnic risk factorsdeficiency, familial, or ethnic risk factors
Need followNeed follow--up monitoring at the time of dischargeup monitoring at the time of discharge

©2005 AWHONN
Potential Neurotoxicity of BilirubinPotential Neurotoxicity of Bilirubin
Postnatal Age
Bilirubin levels* Why this level can be dangerous
Any age
Any jaundiced baby with any neurological signs suspicious for bilirubin induced neuro -dysfunction (BIND)
Any baby with signs suspicious for BIND must be assumed to have severe hype rbilirubinemia until proven otherwise
TSB >99.9 th percentile (correlates to TSB > 25 mg/dl)
These TSB levels may exceed the binding ability of serum albumin and the neur otoxicity risk increases exponentially
Over 72 hours
age
TSB >95 th and <99.9 th
percentile (correlates to TSB of 17 and 25 mg/dl)
Low levels of albumin (<3.4 g/dl) can be seen in term newborns and, more commonly near -term or bruised infants
TSB >95 th percentile and postnatal age
During the first 72 hours, the binding ability of albumin is compromised and lower TSB levels may be potentially neurotoxic
Less than 72 hours
age TSB >75 th percentile and a rate of rise > 0.20 mg/dl/hour
An increase in bilirubin load at > 1 mg per 5 hours or ~ 5 mg/day is likely to result in a TSB >95 th percentile and may reach neurotoxic levels

©2005 AWHONN
Risk of Bilirubin EntryRisk of Bilirubin Entry
These conditions These conditions ↑↑neurotoxicityneurotoxicity by:by:
↓↓ BilirubinBilirubin--albumin albumin bindingbinding
↓↓ Brain blood flowBrain blood flow
Disrupting the bloodDisrupting the blood--brain barrierbrain barrier
AsphyxiaAsphyxia
PrematurityPrematurityHypoalbuminemiaHypoalbuminemiaBilirubinBilirubin--displacing displacing drugsdrugsHyperosmolalityHyperosmolalityHypercarbiaHypercarbiaAcidosisAcidosisHypoxic injuryHypoxic injury

©2005 AWHONN
Clinical Progression of Clinical Progression of Bilirubin EncephalopathyBilirubin Encephalopathy
Clinical Evaluation
Non-specific, Subtle
Progressive Toxicity
Advanced Toxicity
Mental StatusSleepy
+ poor feedLethargy
+ irritabilitySemi-coma or
seizures
Muscle ToneSlight
Decrease
Hyper- or hypotonia
depending on arousal state orMild Nuchal
/Truncal arching
Markedlyincreased
(oposthotonus) or, decreased
tone or,bicycling
movements
Cry High-pitched Shrill Inconsolable

©2005 AWHONN
Reasons for ReReasons for Re--emergence of Kernicterusemergence of Kernicterus
Early dischargeEarly discharge
Lack of concern about Lack of concern about jaundicejaundice
OverOver--reliance on visual reliance on visual assessmentassessment
Birubin test considered as Birubin test considered as a healthcare costa healthcare cost
Limited experience with Limited experience with severe jaundicesevere jaundice
Clinicians were not Clinicians were not consistently using the AAP consistently using the AAP practice guidelines practice guidelines

©2005 AWHONN
Case Presentation, CalCase Presentation, Cal
BW: 2863gBW: 2863g
Gestation:Gestation: 37 wks37 wks
D.O.B.:D.O.B.: 3/23 @ 23523/23 @ 2352
Discharge: 36 hrs of ageDischarge: 36 hrs of age
Breastfeeding Breastfeeding
Blood typeBlood type--mom: O Rh+mom: O Rh+
Blood typeBlood type--infant: A Rh+ infant: A Rh+

©2005 AWHONN
Case Presentation, CalCase Presentation, Cal
Age 4 daysAge 4 days: very sleepy, poor : very sleepy, poor feeding, feeding, ““yellow to toes,yellow to toes,”” seen seen by MDby MD
7% wt loss, No TSB done7% wt loss, No TSB done
2 calls to MD overnight2 calls to MD overnight
Age 5 daysAge 5 days: seen in office and : seen in office and admitted for signs of admitted for signs of lethargy, poor feedinglethargy, poor feeding
TSB=34.6 mg/dlTSB=34.6 mg/dl
Double phototherapy X 3 daysDouble phototherapy X 3 days
No exchange transfusionNo exchange transfusion
©2005 AWHONN
JCAHO Sentinel Alert on KernicterusJCAHO Sentinel Alert on Kernicterus
11st st issued May of 2001issued May of 2001 to hospitals in the United to hospitals in the United StatesStates
Prompted by an increase in number of reported Prompted by an increase in number of reported casescasesCited risk factors, root causes, risk reduction Cited risk factors, root causes, risk reduction strategies, and followstrategies, and follow--up recommendationsup recommendations
ReRe--issued July 2004 to hospitals in the United issued July 2004 to hospitals in the United StatesStates
Recommended updated AAP guidelines be followed Recommended updated AAP guidelines be followed

©2005 AWHONN
Key Recommendations to Reduce Key Recommendations to Reduce Severe HyperbilirubinemiaSevere Hyperbilirubinemia
Promote & support Promote & support breastfeedingbreastfeedingEstablish institutional Establish institutional protocols to identify & protocols to identify & evaluate all infants evaluate all infants Obtain TSB/TcB levels on Obtain TSB/TcB levels on jaundiced infants in the 1st jaundiced infants in the 1st 24 hrs24 hrsVisual estimations can lead to Visual estimations can lead to errorserrorsUse age in hours to interpret Use age in hours to interpret TSB/TcB levelsTSB/TcB levels
Infants <38 weeks & Infants <38 weeks & breastfeeding are at higher risk breastfeeding are at higher risk Perform systematic risk Perform systematic risk assessment at time of dischargeassessment at time of dischargeGive written and verbal Give written and verbal information to parents about information to parents about jaundice jaundice Utilize phototherapy and Utilize phototherapy and exchange transfusion when exchange transfusion when indicated indicated Provide appropriate followProvide appropriate follow--up up based on risk assessmentbased on risk assessment

©2005 AWHONN
Assessment TechniquesAssessment Techniques
Visual Visual
Most widely used methodMost widely used method
Cephalocaudal Cephalocaudal progressionprogression
BUTBUT
Not reliableNot reliable
Not accurateNot accurate

©2005 AWHONN
Assessment TechniquesAssessment Techniques
Total Serum Bilirubin Levels (TSB)Total Serum Bilirubin Levels (TSB)
Primary test and monitoring methodPrimary test and monitoring method
Unrestricted ability to obtain the testUnrestricted ability to obtain the test
Universal bilirubin testingUniversal bilirubin testing
Evaluate by infantEvaluate by infant’’s age in hourss age in hours
©2005 AWHONN
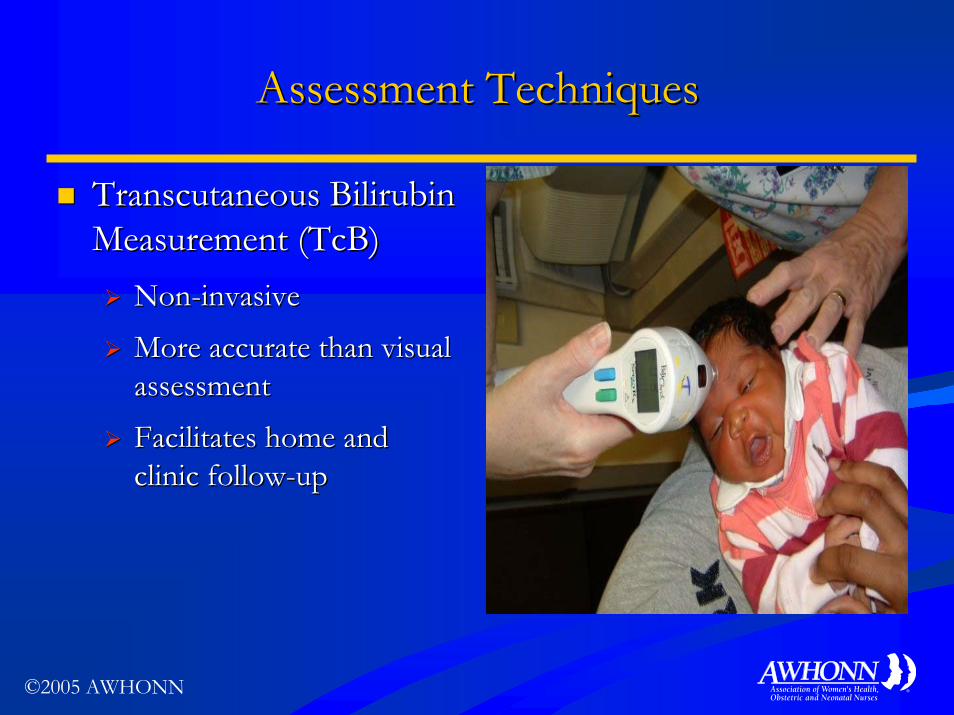
Assessment TechniquesAssessment Techniques
Transcutaneous Bilirubin Transcutaneous Bilirubin Measurement (TcB)Measurement (TcB)
NonNon--invasiveinvasive
More accurate than visual More accurate than visual assessmentassessment
Facilitates home and Facilitates home and clinic followclinic follow--upup

©2005 AWHONN
Assessment TechniquesAssessment Techniques
TSB monitoring remains the primary diagnostic TSB monitoring remains the primary diagnostic test to accurately identify bilirubin levels, and test to accurately identify bilirubin levels, and TSB levels must be determined prior to TSB levels must be determined prior to beginning any treatment.beginning any treatment.

©2005 AWHONN
Assessment TechniquesAssessment Techniques
EndEnd--Tidal Carbon Monoxide Measurement Tidal Carbon Monoxide Measurement ((ETCOcETCOc))
RapidRapid
NonNon--invasiveinvasive
Rules out hemolysis as a contributor to jaundiceRules out hemolysis as a contributor to jaundice
The only clinical test that provides information The only clinical test that provides information about the rates of about the rates of hemeheme catabolism and bilirubin catabolism and bilirubin productionproduction

©2005 AWHONN
Clinical Vigilance Can Clinical Vigilance Can Prevent the WorstPrevent the Worst
Consider these factors when Consider these factors when assessing for dischargeassessing for discharge
1.1. Visual assessment of Visual assessment of jaundice jaundice
2.2. Evaluation of clinical risk Evaluation of clinical risk factorsfactors
3.3. Universal TSB/TcB Universal TSB/TcB evaluationevaluation
4.4. HourHour--specific bilirubin specific bilirubin designation of riskdesignation of risk
5.5. Evaluation of hemolysis if Evaluation of hemolysis if TSB >75TSB >75thth percentilepercentile

©2005 AWHONN
Management TechniquesManagement TechniquesSupporting LactationSupporting Lactation
Prenatal breastfeeding educationPrenatal breastfeeding education
Supportive hospital routinesSupportive hospital routines
Evaluation of breastfeeding techniqueEvaluation of breastfeeding technique
Identification of lactation risk factorsIdentification of lactation risk factors
Intervention for breastfeeding problemsIntervention for breastfeeding problems
Early followEarly follow--up assessment of lactation and up assessment of lactation and infant weightinfant weight

©2005 AWHONN
Management TechniquesManagement TechniquesPhototherapyPhototherapy

©2005 AWHONN
Management TechniquesManagement TechniquesPhototherapyPhototherapy (con(con’’t)t)
Phototherapy units should allow for Phototherapy units should allow for maximum adsorption of bilirubinmaximum adsorption of bilirubin in a in a range fromrange from 420420--480 nm.480 nm.

©2005 AWHONN
Management TechniquesManagement TechniquesPhototherapy Phototherapy ((concon’’tt))
Adverse EffectsAdverse EffectsDehydration Dehydration
Lack of visualLack of visual--sensory input sensory input in animalsin animals
Watery diarrhea Watery diarrhea
Skin rashesSkin rashes
HyperthermiaHyperthermia
↓↓ maternalmaternal--infant infant interactioninteraction
SyndromesSyndromesBronze Baby Syndrome Bronze Baby Syndrome (in case of direct (in case of direct hyperbilirubinemia)hyperbilirubinemia)
Vulnerable Child SyndromeVulnerable Child Syndrome

©2005 AWHONN
Management TechniquesManagement TechniquesExchange TransfusionsExchange Transfusions
Absolute indications:Absolute indications:Signs of Acute Bilirubin Encephalopathy (intermediate or Signs of Acute Bilirubin Encephalopathy (intermediate or advanced)advanced)
Hazardous TSB levels >30 mg/dl (in infants with no risk Hazardous TSB levels >30 mg/dl (in infants with no risk factors) or >23 mg/dl (with higher risk factors)factors) or >23 mg/dl (with higher risk factors)
Failure of intensive phototherapy for infants with severe Failure of intensive phototherapy for infants with severe hyperbilirubinemia (substantial decline in bilirubin after hyperbilirubinemia (substantial decline in bilirubin after 33--4 hours, such as >2 mg/dl in 4 hours)4 hours, such as >2 mg/dl in 4 hours)
Onset of any clinical neurologic signs in infants with Onset of any clinical neurologic signs in infants with excessive hyperbilirubinemiaexcessive hyperbilirubinemia

©2005 AWHONN
Emerging Research: Emerging Research: Bilirubin as Natural AntioxidantBilirubin as Natural Antioxidant
Potent antioxidant when bound to albuminPotent antioxidant when bound to albumin
Protective component for the bodyProtective component for the body
May provide primary protection from ischemiaMay provide primary protection from ischemia--related injuries and retinopathy of prematurityrelated injuries and retinopathy of prematurity
Antioxidant effect not fully understoodAntioxidant effect not fully understood

©2005 AWHONN
Therapies Under InvestigationTherapies Under Investigation
Agent Agent Metabolic ProcessMetabolic Process MechanismMechanism
Tin protoporphyrin Tin protoporphyrin HemeHeme degradation degradation HemeHeme--oxygenaseoxygenaseinhibitorinhibitor
Zinc or TinZinc or Tin Alternate heme catabolism Alternate heme catabolism HemeHeme excretedexcretedmesoporphyrinmesoporphyrin in bile (currently in bile (currently
in US studies)in US studies)
Agar, Charcoal Agar, Charcoal ↓↓ EEnterohepatic nterohepatic Sequester Sequester bilirubin bilirubin circulation in circulation in bowel (used bowel (used outside the US)outside the US)

©2005 AWHONN
Therapies Under Investigation (Therapies Under Investigation (concon’’tt) )
Homeopathic Homeopathic Metabolic Process Metabolic Process MechanismMechanismAgentAgent
Bilirubin Bilirubin OxidaseOxidase ↓↓EEnterohepatic circulationnterohepatic circulation DegradeDegradebilirubinbilirubin in in gutgut
Herbal products Usually cathartics Herbal products Usually cathartics IncreaseIncreasestoolstoolexcretionexcretion

©2005 AWHONN
Follow-up Care MapRisk Assessment
Evaluation:Bili workup
Bili Follow-up 24hrs
Bili Follow-up 48hrs
Visual follow-up
95th %ile75th %ile
40th %ile

©2005 AWHONN
Use a System ApproachUse a System Approach
Prenatal educationPrenatal education through through post discharge evaluationpost discharge evaluation
InpatientInpatient
Evaluate jaundice with vital Evaluate jaundice with vital signssigns
Corroborate with TcB/TSBCorroborate with TcB/TSB
PeerPeer--review of cases with review of cases with TSB >25 mg/dlTSB >25 mg/dl
Post discharge followPost discharge follow--upup
RiskRisk--based and/or TSB/based and/or TSB/TcBTcB
Inpatient
PostDischargeFollow-Up
PrenatalEducation

©2005 AWHONN
Your Role as the Nurse IncludesYour Role as the Nurse Includes
Supporting and teaching breastfeeding Supporting and teaching breastfeeding
Identifying and monitoring jaundiceIdentifying and monitoring jaundice
Coordinating discharge planning for atCoordinating discharge planning for at--risk infantsrisk infants
Assuring proper treatmentAssuring proper treatment
Educating parentsEducating parents
Partnering with other healthcare professionals Partnering with other healthcare professionals through a multidisciplinary teamthrough a multidisciplinary team

©2005 AWHONN
Further Information Available FromFurther Information Available From
AWHONNAWHONNCDCCDCJCAHOJCAHOAAPAAPPICKPICKCochrane LibraryCochrane LibraryAHRQAHRQ
©2005 AWHONN
Make a Difference by Using Evidence in Make a Difference by Using Evidence in Your Nursing PracticeYour Nursing Practice





























