Embed Size (px)
Citation preview

HIY
SpfmwNonf
UTfecti
*
†A
0d
uman Milk and Clinical Outcomes in VLBWnfants: How Compelling Is the Evidence of Benefit?esenia Morales, MD,* and Richard J. Schanler, MD†,*
Significant benefits to infant host defense, sensory–neural development, gastrointestinalmaturation, and some aspects of nutritional status are observed when premature infantsare fed their mothers’ own milk. A reduction in infection-related morbidity in human milk-fedpremature infants has been reported in nearly a dozen descriptive, and a few quasi-randomized, studies in the past 25 years. Studies on neurodevelopmental outcomes havereported significantly positive effects for human milk intake on mental and motor develop-ment, intelligence quotient, and visual acuity compared with the feeding of formula. Humanmilk-fed infants also have decreased rates of re-hospitalization after discharge. It is unclearhow much human milk is needed to provide protection or at what postnatal age theprotective effects maximize. More data are warranted to elucidate these questions. Despitethe significant benefits of mothers’ own milk, nutritional adequacy may be a limiting factorin the infant weighing less than 1500 g at birth. The overall nutritional needs of these infantscan be supported with a nutrient supplement, or fortifier, added to the milk.Semin Perinatol 31:83-88 © 2007 Elsevier Inc. All rights reserved.
KEYWORDS human milk, premature infants, donor human milk, fortified human milk
fnbAhrtdsfvrmzmscehci(
ac
ignificant benefits to infant host defense, sensory–neuraldevelopment, gastrointestinal maturation, and some as-
ects of nutritional status are observed when premature in-ants are fed human milk.1 Nutritional adequacy of mother’silk, however, may be a limiting factor in the very low birtheight (VLBW) infant weighing less than 1500 g at birth.utritional needs are determined based on intrauterine ratesf growth and nutrient accretion.2 The overall nutritionaleeds of the VLBW infant are met if a nutrient supplement, orortifier, is added to the milk.
nfortified Human Milkhe nutritional adequacy of human milk for premature in-
ants may be limited for several reasons. The absolute nutri-nt content may be inadequate for their needs, such as cal-ium and phosphorus, which remain too low with respect tohe needs of the premature infant. In addition, the variabilityn nutrient content results in unpredictable nutrient intakes
Division of Neonatal–Perinatal Medicine, Schneider Children’s Hospital,North Shore-Long Island Jewish Health System, Manhasset, NY.
Department of Pediatrics, Albert Einstein College of Medicine, Bronx, NY.ddress reprint requests to Richard J. Schanler, MD, Neonatal–Perinatal
Medicine, North Shore University Hospital, 300 Community Drive,
oManhasset, NY 11030. E-mail: [email protected]146-0005/07/$-see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1053/j.semperi.2007.02.002
or an infant who cannot feed ad libitum. The variability inutrient composition is both inherent to milk and imposedy circumstances of collection, storage, and distribution.
large variation in the energy and protein contents ofuman milk brought to the neonatal nursery by the mother iseported.3 The most variable nutrient in human milk is fat,he content of which differs during lactation, throughout theay, from mother to mother, and within a single milk expres-ion.4,5 As human milk is not homogenized, on standing, theat content separates from the body of milk. Much of theariation in energy content of milk as used in the nursery is aesult of differences in and/or losses of fat in the unfortifiedilk.6,7 Although concentrations of protein, sodium, and
inc decline through lactation, the nutrient needs of the pre-ature infant remain higher than those of term infants until
ometime after term postmenstrual age. Therefore, the de-line in milk concentration precedes the reduction in nutri-nt needs and results in an inadequate nutrient supply fromuman milk for the premature infant. Technical issues asso-iated with collection, storage, and delivery of milk to thenfant also result in a decreased quantity of available nutrientseg, vitamin C, vitamin A, riboflavin).
Growth and nutritional status of premature infants duringnd after hospital stay are affected by the nutrient inadequa-ies of unfortified human milk.8-10 As growth rates in excess
f 15 g/kg/d are desired, unfortified human milk would not83

mbsompgccilwplathmgzh
eemsdtbtfia
HTmPiobobi
starhcp
ttobT
smc
ttuNmpcncmhbfsamh
EMTtmtviif
itpmgofcmwiitwfi
prcf
84 Y. Morales and R.J. Schanler
eet this target.11 Indices of protein nutritional status, eg,lood urea nitrogen, serum albumin, total protein, and tran-thyretin (prealbumin), are lower and continue to declinever time when premature infants are fed unfortified humanilk.12 As a consequence of the low intakes of calcium and
hosphorus, infants fed unfortified human milk have pro-ressive decreases in serum phosphorus, increases in serumalcium, and increases in serum alkaline phosphatase activityompared with infants fed preterm formula.13,14 Follow-upnvestigations of infants with extremely elevated serum alka-ine phosphatase activity at 18 months found an associationith linear growth, infants having the highest alkaline phos-hatase values in-hospital had as much as a 2 cm reduction in
inear growth.15 Evaluation of this cohort at 9 to 12 year ofge found that the elevated neonatal serum alkaline phospha-ase activity remained a significant predictor of attainedeight.16 These data suggest that long-term mineralizationight be affected by early neonatal diet. With respect to the
reater needs of the VLBW infant, the declining sodium andinc contents of mother’s milk may be associated with lateyponatremia and zinc deficiency.17,18
Human milk has not been rigorously studied in minimalnteral nutrition trials. The benefits observed for minimalnteral nutrition have been identified for infants fed humanilk or formula. However, full enteral feeding is achieved
ignificantly earlier with human milk than formula.19 In ad-ition, if human milk is used in early minimal enteral nutri-ion, infants receive more of their mothers’ milk, probablyecause mothers initiate and sustain lactation more readilyhan those whose infants are not receiving their milk in therst 2 weeks.20 Thus, although the data are limited, it seemsppropriate to use human milk in minimal enteral nutrition.
uman Milk Fortificationhe nutrient deficits that arise from feeding unfortified hu-an milk can be corrected with nutrient supplementation.1
rotein and energy supplementation are associated withmproved rates of weight gain, nitrogen balance, and indicesf protein nutritional status: blood urea nitrogen, serum al-umin, total protein, and transthyretin.12,21 The efficacy ofnly protein fortification of human milk was of short-termenefit resulting in increases in weight gain, and increments
n length and head circumference growth.22
Supplementation with both calcium and phosphorus re-ults in normalization of biochemical indices of mineral sta-us: serum calcium, phosphorus, and alkaline phosphatasectivity, and urinary excretion of calcium and phospho-us.13,23 Mineral supplementation of unfortified human milkas been associated with improved linear growth and in-reased bone mineralization during and beyond the neonataleriod.24
A systematic review that addressed multinutrient fortifica-ion of human milk included a meta-analysis of controlledrials of human milk fortification compared with the feedingf unfortified human milk.24 More than 600 infants withirth weights less than 1850 g were included in the analyses.
he addition of multinutrient fortifiers to human milk re- tulted in short-term improvements in weight gain, incre-ents in length and head circumference, and bone mineral
ontent during hospital stay.A theoretical concern with human milk fortification is that
he added nutrients may affect the intrinsic host defense sys-em of the milk. The Cochrane review of fortified versusnfortified human milk did not identify any differences inEC.24 One randomized trial of multi-nutrient fortified hu-an milk versus human milk supplemented only with phos-horus and vitamins in premature infants indicated no in-reases in the incidence of either confirmed infection orecrotizing enterocolitis.25 When the latter two events wereombined, however, the group fed fortified human milk hadore events than infants in the control group. The data,owever, were difficult to interpret because study infants inoth groups received more than 50% of their diet as pretermormula.26 Moreover, as indicated below, most contemporarytudies demonstrated protective effects of mother’s own milknd the milk studied was multi-nutrient fortified humanilk. Thus, the practice of human milk fortification mightave a marked effect on reducing the cost of medical care.
ffects of Humanilk on Host Defense
he relationship between diet and the incidence of infec-ion in premature infants demonstrates that the feeding ofother’s milk mitigates the high rate of infection common
o hospitalized premature infants. In a retrospective re-iew of medical records in a Washington DC neonatalntensive care unit, human milk-fed infants had a 26%ncidence of documented infection compared with 49% inormula-fed infants.27
A semirandomized trial in the U.K. reported that necrotiz-ng enterocolitis was reduced significantly by feeding prema-ure infants human milk, either exclusively or partially sup-lemented with either formula or pasteurized donor humanilk.28 That study identified the highest risk for NEC in the
roup of infants born before 28 weeks gestation. The receiptf human milk was associated with significant protectionrom NEC in infants more than 27 weeks gestation. Whenompared with exclusive human milk feeding (mother’s ownilk or donor human milk), the receipt of only formulaas associated with a 6.5-fold increase (95% confidence
nterval � 1.9 to 22, P � 0.001) in confirmed cases of NEC asdentified from surgical pathology or postmortem examina-ion. A significant threefold increase in NEC also was seenhen a diet of exclusive formula feeding was compared with
ormula used as a supplement to human milk (confidencenterval for confirmed cases 1.4 to 6.5, P � 0.005).
In a randomized comparison in a NICU in Mexico City,remature infants receiving human milk had markedly lowerates of NEC, diarrhea, and urinary tract infection and re-eived fewer days of antibiotic treatment than infants fedormula.29
The relationship between dose of human milk and protec-
ive effect was examined posthoc from data derived in a study
oimestpmtm1siapmommpta
iNhie8oa92oa(eIfrIs7iw
fsntmactdFfemafah
catntf
ENToptgdiwowsttm
T
NHNLLH
M
Human milk in VLBW infants 85
f two feeding strategies for premature infants: trophic feed-ng versus no feeding (4 versus 14 days) and tube-feeding
ethod, continuous versus intermittent bolus.19 The studynrolled infants born before 30 weeks gestation who weretratified in enrollment by diet, either mother’s milk or pre-erm formula. Differences between groups favored early tro-hic feeding at 4 days using the intermittent bolus feedingethod. However, for all measured outcomes, the diet was
he most important variable. Infants predominantly fed hu-an milk (averaged as more than 50 mL/kg/d, approximately
/3 of full milk feedings) had significantly less late-onsetepsis and NEC and shorter hospitalization compared withnfants fed preterm formula (Table 1). Late-onset sepsisnd/or NEC were of greater incidence in infants receivingreterm formula, but if infants received a combination ofother’s milk and preterm formula, they had the highest risk
f sepsis and/or NEC. The study identified a dose of humanilk that potentially might be protective. This dose ofother’s milk, �50 mL/kg/d, subsequently was shown to
rotect against late-onset sepsis in a 4-week study of prema-ure infants when compared with average daily doses of 1-24nd 25-49 mL/kg.30
Data from a multi-center study of extremely prematurenfants 22 to 27 weeks gestation weighing �1000 g at birth inorway are pertinent to understand the beneficial effects ofuman milk and early feeding.31 The study protocol was to
nitiate feedings of 1 to 2 mL in the first hours after birth, thenvery 2 to 3 hours, and advance by 0.5 to 1.0 mL every 6 tohours. More than 60% of the 462 infants received feedingsn day 1 and 92% by day 2. More than 2/3 of all infantschieved full enteral feeding by 2 weeks. Of the milk used,2% was mother’s own milk, 6% was donor human milk, and% was preterm formula. The investigators found that late-nset sepsis occurred in 20% of the study population and wasssociated with gestational age (negative), illness severitypositive), central venous catheter use (positive), and lack ofstablishment of full enteral feeding by 2 weeks (positive).ndeed, when adjusted for all the above factors, if full enteraleedings of mother’s milk was not achieved by 2 weeks, theelative risk of late-onset sepsis was 3.7 (95% CI 2.0 to 6.9).ndeed, if full enteral feeding was established by 2 weeks, theurvival free of late-onset sepsis was 90% compared with0% for those not achieving this milestone by 2 weeks. It is
mportant to emphasize that more than 90% of the infants
able 1 Effect of Dose of Mother’s Own Milk on Infection-Re
Human>50 mL/
o. infants 62uman milk intake (ml/kg/d) 96 �ecrotizing enterocolitis, n (%)* 1 (2ate-onset sepsis (LOS), n (%)** 19 (3OS and/or NEC, n (%)* 19 (3ospital stay (d)*** 73 �
ean � SD; *, P < 0.01; **, P � 0.07; ***, P < 0.05.
ere fed their mother’s milk. h
A reduction in infection-related morbidity in human milk-ed premature infants has been reported in nearly a dozentudies in the past 25 years.32 A critique of such reports findsumerous methodological issues that are compounded byhe inability to perform truly randomized trials in humanilk-fed premature infants. Many of the studies do not reportconsistent definition of human milk feeding, and there is noonsistent method used to quantify milk intake. The scien-ific validity of some studies is reduced when infants withiffering degrees of human milk intake are grouped together.urthermore, the inconsistent definitions of human milkeeding across studies may grossly underestimate the trueffect of human milk. Interpretation of results becomes evenore confusing when the type of human milk that is given
lso differs throughout studies (mother’s own, banked, fresh,rozen/thawed, fortified, unfortified). Some of the reportslso do not report the duration of human milk feeding norave they performed subgroup analyses.Lastly, there are difficulties in the interpretation of out-
omes; infection-related events are not uniformly definednd confounding factors inconsistently reported. Studies inhis area also are confounded by differences in socioeco-omic status, parental visiting, and other factors inherent inhe mother’s decision to provide milk for her premature in-ant.33,34
ffects oneurodevelopmental Outcome
he NICU diet may affect long-term neurodevelopmentalutcomes in premature infants. An 8-year follow up of 300remature infants (approximately 1.4 kg and 31 weeks ges-ation at birth) observed that when factors affecting intelli-ence quotient (social class, maternal education, infant gen-er, and duration of mechanical ventilation) were considered
n a regression model, the receipt of breastmilk in the NICUas associated with an 8-point advantage, slightly more thanne standard deviation of the mean.35 A cohort of adolescentsere followed since their NICU stay as premature infants and
ignificant cognitive and psychomotor benefits were ascribedo the feeding of human milk.36-38 In a large study of prema-ure infants 30 weeks gestation and birth weight approxi-ately 1.3 kg fed either human milk or preterm formula, a
Events and Hospital Stay19
Human Milkand Formula
PretermFormula
63 4220 � 15 016 (25) 6 (13)29 (46) 22 (48)35 (56) 25 (54)87 � 43 88 � 47
lated
Milkkg/d
23)1)1)19
uman milk diet was associated with significantly greater

samricHaiw
etdi2intciapapdhiomPiei
is
DTtwttrcfrbti
taass
ioftphlfmmm
2dpf
itacmtijdfiisfmN0rfdom
ic(lmb
T
GCLSO
R
86 Y. Morales and R.J. Schanler
cores in behavioral visual acuity at 2 to 6 months correctedge compared with preterm formula.39 The effect of humanilk on cognitive indices also was seen at 12 months cor-
ected age and, in infants with chronic lung disease, a signif-cant benefit of a human milk diet was observed in psy-homotor indices. These observations were adjusted forOME Inventory, maternal intelligence testing, smoking,
nd birth weight. This study also reported that infants receiv-ng the most human milk had fewer severe adverse events orere rehospitalized less after discharge.39
A large multi-center follow-up study of more than 1000xtremely low birth weight infants who had extensive nutri-ional data collected during their hospitalization was con-ucted to determine the relationship between human milk
ntake in-hospital and neurodevelopmental outcome at 18 to2 months of age.40 Neonatal birth weight, gestational age,
ntraventricular hemorrhage status, sepsis, bronchopulmo-ary dysplasia, and hospital stay were similar betweenhose never receiving (25% of cohort) and those who re-eived human milk (75% of cohort) during their hospital-zation. There were differences in socioeconomic vari-bles, race and ethnicity, educational attainment, andarity between groups. When adjusted for these variabless well as biological confounders, there were significantlyositive effects for human milk intake on mental and motorevelopment. The magnitude of the effect was greatest in theighest quintile (�80th percentile) group which averaged an
ntake of 110 ml/kg/day. The impact of feeding 100 mL/kg/df human milk was an increase in Bayley Mental Develop-ent Index (MDI) of 5 points (1/3 of an SD), an increase in
sychomotor Development Index of 6 points, and a decreasen rehospitalization rate by 6%.40 Others have reported thatven the 5-point difference on the MDI would have a signif-cantly meaningful effect on the outcome of ELBW infants.41
Thus, as long-term sensory-neural development is a signif-cant risk following premature birth, the use of mother’s milkhould be strongly encouraged in this population.
onor Human Milkhe benefits of mother’s own milk have prompted clinicians
o reconsider the use of donor human milk as an alternativehen mother’s own milk is not available. The concern about
ransmission of infectious agents through breastmilk led tohe decline in donor human milk banks and to the obligatoryequirement for pasteurization if donor milk is used.42 Theommon pasteurization process, Holder pasteurization, re-ers to heating milk at 62.5°C for 30 minutes.43 This processesults in a decrease in activity of many of the functionalioactive factors in the milk.44,45 There are scant data to de-ermine the efficacy of pasteurized donor milk in prematurenfants.
Small descriptive studies suggested that the nutrient con-ent of donor milk is lower in fat, calories, protein, sodium,nd calcium than formula, and the lower nutrient content isssociated with slower rate of growth and significantly lowercores on Brazelton examination for alertness and respon-
iveness to stimuli than similar infants fed formula.46 In an hnteresting experiment, investigators compared three groupsf premature infants assigned randomly to feedings of eitherormula, pasteurized donor mature term human milk, or pas-eurized preterm human milk fed sequentially from earlyostpartum.10 The group fed pasteurized donor mature termuman milk had the longest time to regain birth weight, and
ower rates of all growth parameters compared with infantsed formula or sequentially collected pasteurized preterm hu-an milk. Infants fed pasteurized donor mature term humanilk also had a significantly greater incidence of hyponatre-ia.10
A recent Cochrane review of studies conducted more than0 years ago concluded that feeding premature infants termonor milk did not significantly lower the risk of NEC com-ared with feeding formula (relative risk of NEC by feedingormula 2.5, 95% CI � 0.85 to 7.26).47
Most recently, a randomized trial of extremely prematurenfants (born before 30 weeks’ gestation) assigned randomlyo receive pasteurized donor human milk or preterm formulas supplements if their mothers’ own milk was unavailable,ompared morbidity of infants who received either donorilk or formula.34 No differences were found for any infec-
ion-related event (late-onset sepsis, meningitis, urinary tractnfection, necrotizing enterocolitis). The incidence of the ma-or outcome, combined late-onset sepsis and/or NEC, did notiffer between the groups fed pasteurized donor milk versusormula, 23/78 versus 20/88, respectively, P � 0.42. Thenfants receiving donor human milk also required a greaterntake of milk and more nutritional supplements, yet per-isted with a slower rate of weight gain than infants receivingormula. The infants who continued to receive their ownothers’ milk had fewer episodes of late-onset sepsis and/orEC (P � 0.034) and a shorter duration of hospital stay (P �.04) than those receiving donor milk or formula. Thus, thisandomized blinded trial in extremely premature infantsound that, as a substitute for mother’s own milk, pasteurizedonor human milk offered no observed short-term advantagever preterm formula. The data reiterated the benefit ofothers’ own milk for extremely premature infants.Although no single study found a significant reduction
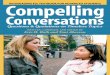
n the incidence of NEC when donor human milk wasompared with formula, the combined data are of interestTable 2). As all studies had relatively small sample size, theack of finding a difference in NEC between those fed donor
ilk or formula is not surprising.48 The studies were com-ined in a weighted analysis.34,48 The Breslow-Day test for
able 2 Studies of Donor Human Milk and NEC34,48
Donor Milk Formula
ross 1983 1/42 (2%) 3/29 (10%)ooper 1984 1/24 (4%) 3/15 (20%)ucas 1990 1/87 (1%) 4/80 (5%)chanler 2005 5/78 (6%) 10/88 (11%)verall 8/231 (3%) 20/212 (9%)
isk of NEC is reduced significantly with pasteurized donor milk0.35 (0.15; 0.81).
omogeneity of odds ratios was used to determine whether

ttHwNtntNIfNN
CTmpoFmtdttnssfbs
bu
ncjfwftbust
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
Human milk in VLBW infants 87
he data were consistent. Since this test was not significant,he common odds ratio was computed using the Mantel-aenszel estimate of the odds ratio. The combined odds ratioas 0.35 for donor milk (ie, donor milk is protective againstEC), and the associated 95% confidence interval was 0.15
o 0.81. However, it must be emphasized that the studies areot directly comparable, the number, birth weight, and ges-ational ages of the infant’s studied varied considerably, andEC was not included as an outcome in several of the studies.
n addition, only one of these studies included infants fedortified human milk and contemporary preterm formula.evertheless, this association suggests that larger studies ofEC in premature infants fed donor milk are warranted.
onclusionhere are significant host defense benefits from the feeding ofothers’ own milk for premature infants, even extremelyremature infants. It is unclear how much milk is protectiver at what postnatal age the protective effects maximize.urthermore, it is unclear why some premature infants fedother’s milk continue to have significant numbers of infec-
ion-related events while receiving this diet. Is this a result ofose of milk received or receipt of milk lacking certain pro-ective factors? A detailed composition analysis of milk ob-ained from women delivering before 30 weeks gestation iseeded to determine if the “immature” milk contains theame functional bioactive factors as more mature milk. It alsohould be recognized that there are interactions of multipleactors that affect the measured outcomes, and attempts muste made to control for confounders uniformly in subsequenttudies.
Sensory–neural development of premature infants mayenefit from mother’s milk, but more data are warranted tonderstand the mechanism for this association.Mother’s own milk is nutritionally inadequate to meet the
eeds of infants weighing less than 1500 g at birth, unless itontains multi-nutrient human milk fortifiers. Further ad-ustments in nutrients are warranted. Global human milkortifiers offer a wide range of nutrient contents, some ofhich do not meet recommended intakes for premature in-
ants. There are only scant nutritional data on recommenda-ions for the premature infants weighing 1500 to 2000 g atirth. This is a large group of premature infants who receivensupplemented human milk. Lastly, lactation strategieshould be sought that increase mother’s own milk produc-ion.
eferences1. Schanler RJ: The use of human milk for premature infants. Pediatr Clin
North Am 48:207-220, 20012. Ziegler EE, O’Donnell AM, Nelson SE, et al: Body composition of the
reference fetus. Growth 40:329-341, 19763. Polberger S: Quality of growth in preterm neonates fed individually
fortified human milk, in Battaglia FC, Pedraz C, Sawatzki G, et al (eds):Maternal and Extrauterine Nutritional Factors. Their Influence on Fetal
and Infant Growth. Madrid, Ediciones Ergon, S.A., 1996, pp 395-4034. Neville MC, Keller RP, Seacat J, et al: Studies on human lactation. I.Within-feed and between-breast variation in selected components ofhuman milk. Am J Clin Nutr 40:635-646, 1984
5. Valentine CJ, Hurst NM, Schanler RJ: Hindmilk improves weight gainin low-birth-weight infants fed human milk. J Pediatr GastroenterolNutr 18:474-477, 1994
6. Greer FR, McCormick A, Loker J: Changes in fat concentration ofhuman milk during delivery by intermittent bolus and continuousmechanical pump infusion. J Pediatr 105:745-749, 1984
7. Schanler RJ: Special methods in feeding the preterm infant, in TsangRC, Nichols BL (eds): Nutrition During Infancy. Philadelphia, PA, Han-ley & Belfus, 1988, pp 314-325
8. Atkinson SA, Bryan MH, Anderson GH: Human milk feeding in pre-mature infants: protein, fat and carbohydrate balances in the first twoweeks of life. J Pediatr 99:6l7-624, 1981
9. Atkinson SA, Radde IC, Anderson GH: Macromineral balances in pre-mature infants fed their own mothers’ milk or formula. J Pediatr 102:99-106, 1983
0. Gross SJ: Growth and biochemical response of preterm infants fedhuman milk or modified infant formula. N Engl J Med 308:237-241,1983
1. Ehrenkranz RA, Dusick AM, Vohr BR, et al: Growth in the neonatalintensive care unit influence neurodevelopmental and growth out-comes of extremely low birth weight infants. Pediatrics 117:1253-1261, 2006
2. Kashyap S, Schulze KF, Forsyth M, et al: Growth, nutrient retention,and metabolic response of low-birth-weight infants fed supplementedand unsupplemented preterm human milk. Am J Clin Nutr 52:254-262, 1990
3. Rowe JC, Wood DH, Rowe DW, et al: Nutritional hypophosphatemicrickets in a premature infant fed breast milk. N Engl J Med 300:293-296, 1979
4. Pettifor JM, Stein H, Herman A: Mineral homeostasis in very low birthweight infants fed either own mother’s milk or pooled pasteurizedpreterm milk. J Pediatr Gastroenterol Nutr 5:248-253, 1986
5. Lucas A, Brooke OG, Baker BA, et al: High alkaline phosphatase activityand growth in preterm neonates. Arch Dis Child 64:902-909, 1989
6. Fewtrell MS, Cole TJ, Bishop NJ, et al: Neonatal factors predictingchildhood height in preterm infants: evidence for a persisting effect ofearly metabolic bone disease? J Pediatr 137:668-673, 2000
7. Roy RN, Chance GW, Radde IC, et al: Late hyponatremia in very lowbirthweight infants. Pediatr Res 10:526-53l, 1976
8. Obladen M, Loui A, Kampmann W, et al: Zinc deficiency in rapidlygrowing preterm infants. Acta Paediatr 87:685-691, 1998
9. Schanler RJ, Shulman RJ, Lau C: Feeding strategies for premature in-fants: Beneficial outcomes of feeding fortified human milk vs pretermformula. Pediatrics 103:1150-1157, 1999
0. Schanler RJ, Shulman RJ, Lau C, et al: Feeding strategies for prematureinfants: randomized trial of gastrointestinal priming and tube-feedingmethod. Pediatrics 103:434-439, 1999
1. Polberger SKT, Axelsson IA, Raiha NCR: Growth of very low birthweight infants on varying amounts of human milk protein. Pediatr Res25:414-419, 1989
2. Kuschel CA, Harding JE: Protein supplementation of human milk forpromoting growth in preterm infants (Cochrane Review). The Co-chrane Library, 2001
3. Schanler RJ, Garza C: Improved mineral balance in very low birthweight infants fed fortified human milk. J Pediatr 112:452-456, 1987
4. Kuschel CA, Harding JE: Multicomponent fortified human milk forpromoting growth in preterm infants. The Cochrane Library, 2005
5. Lucas A, Fewtrell MS, Morley R, et al: Randomized outcome trial ofhuman milk fortification and developmental outcome in preterm in-fants. Am J Clin Nutr 64:142-151, 1996
6. Schanler RJ: Human milk fortification for premature infants. Am J ClinNutr 64:249-250, 1996
7. Hylander MA, Strobino DM, Dhanireddy R: Human milk feedings andinfection among very low birth weight infants. Pediatrics 102:e38,
1998
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
88 Y. Morales and R.J. Schanler
8. Lucas A, Cole TJ: Breast milk and neonatal necrotizing enterocolitis. Lan-cet 336:1519-1523, 1990
9. Contreras-Lemus J, Flores-Huerta S, Cisneros-Silva I, et al: Disminu-cion de la morbilidad en neonatos pretermino alimentados con leche desu propia madre. Biol Med Hosp Infant Mex 49:671-677, 1992
0. Furman L, Taylor G, Minich N, et al: The effect of maternal milk onneonatal morbidity of very low-birth-weight infants. Arch Pediatr Ado-lesc Med 157:66-71, 2003
1. Ronnestad A, Abrahamsen TG, Medbo S, et al: Late-onset septicemia ina Norwegian national cohort of extremely premature infants receivingvery early full human milk feeding. Pediatrics 115:e269-e276, 2005
2. de Silva A, Jones PW, Spenser SA: Does human milk reduce infectionrates in preterm infants? A systematic review. Arch Dis Child FetalNeonatal Ed 89:F509-F513, 2004
3. Lucas A, Cole TJ, Morley R, et al: Factors associated with maternalchoice to provide breastmilk for low birth weight infants. Arch DisChild 59:722-730, 1988
4. Schanler RJ, Lau C, Hurst NM, et al: Randomized trial of donor hu-man milk versus preterm formula as substitutes for mothers’ ownmilk in the feeding of extremely premature infants. Pediatrics 116:400-406, 2005
5. Lucas A, Morley R, Cole TJ, et al: Breast milk and subsequent intelli-gence quotient in children born preterm. Lancet 339:261-264, 1992
6. Horwood LJ, Fergusson DM: Breastfeeding and later cognitive andacademic outcomes. Pediatrics 101:E91-E97, 1998
7. Horwood LJ, Mogridge N, Darlow BA: Cognitive, educational, andbehavioral outcomes at 7 to 8 years in a national very low birthweightcohort. Arch Dis Child Fetal Neonatal 79:F12-F20, 1998
8. Horwood LJ, Darlow BA, Mogridge N: Breast milk feeding and cogni-tive ability at 7-8 years. Arch Dis Child Fetal Neonatal 84:F23-F27,
20019. O’Connor DL, Jacobs J, Hall R, et al: Growth and development ofpremature infants fed predominantly human milk, predominantly pre-mature infant formula, or a combination of human milk and prematureformula. J Pediatr Gastroenterol Nutr 37:437-446, 2003
0. Vohr BR, Poindexter BB, Dusick AM, et al: Beneficial effects of breastmilk in the neonatal intensive care unit on the developmental outcomeof extremely low birth weight infants at 18 months of age. Pediatrics118:e115-e123, 2006
1. Hack M, Flannery DJ, Schluchter M, et al: Outcomes in young adult-hood for very-low-birth-weight infants. N Engl J Med 346:149-157,2002
2. Wight NE: Donor human milk for preterm infants. J Perinatol 21:249-254, 2001
3. Human Milk Banking Association of North America: Guidelines for theEstablishment of a Donor Human Milk Bank. Raleigh, NC, HMBANA,2005
4. Lepri L, Del Bubba M, Maggini R, et al: Effect of pasteurization andstorage on some components of pooled human milk. J Chromatogr BBiomed Sci Appl 704:1-10, 1997
5. Koenig A, Diniz EMA, Barbarosa SFC, et al: Immunologic factors inhuman milk: the effects of gestational age and pasteurization. J HumLact 21:439-443, 2005
6. Tyson JE, Lasky RE, Mize CE, et al: Growth, metabolic response, anddevelopment in very-low-birth-weight infants fed banked human milkor enriched formula. I. Neonatal findings. J Pediatr 103:95-104, 1983
7. Henderson G, Anthony MY, McGuire W: Formula milk versus termhuman milk for feeding preterm or low birth weight infants (review).Cochrane Database Syst Rev 1-24, 2001
8. Boyd CA, Quigley MA, Brocklehurst P: Donor breast milk versus infantformula for preterm infants: a systematic review and meta-analysis.Arch Dis Child Fetal Neonatal Ed, published online 5 Apr 2006; doi:
10.1136/adc. 2005.089490