Embed Size (px)
Citation preview

How are we doing?
– Implementing Best
Practice
Tuula Rintala, RN, MSc PSPM
Quality Manager, KCH
Jacie Inspector, Collection Facility

KHP Transplant Programme – Brief summary
• KCH
– KCH BMT programme • First autograft 1986
• First allograft 1993
– 1000th transplant June 2008
– 1000th allogeneic stem cell infusion July 2012
• GSTT:
– 1975: BM transplant for a thalassaemia patient
– 1983: NHL transplant (Dept of Oncology)
– 500 transplants by 2005 - over 700 transplants by the
time programmes merged

KHP BMT Programme
• KHP (Kings Health Partners) BMT Programme – Merger completed October 2011
• Largest allogeneic transplant program in the
BMT consortium
– Largest MDS allograft program in the UK/Europe
– Largest Aplastic Anaemia Programme in the UK
• Anthony Nolan Trust collection centre
• JACIE, HTA, MHRA and CPA accredited

1. Unknowing variation in clinical practice and service delivery
2. Errors of commission and omission
3. Waste
4. Failure to implement new knowledge and technology
systematically and appropriately
5. Over-use and under-use – inappropriate care
6. Unsatisfactory patient experience
7. Poor quality clinical practice
8. Failure to manage uncertainty
8 most common problems in health care

What is Quality?
Moullin (2002)
– Quality leads to a service better meeting the patient’s
requirements, and increases patients confidence in
the service; staff is more empowered and higher job
satisfaction; better quality can reduce costs
MacKenzie (2005)
– Multidimensional & changeable concept
– ‘an acceptable compromise’
Donabedian (2005)
– reflection of values and goals current in healthcare and in the larger society

What is Quality?
• US Institute of Medicine: Six dimensions of
healthcare quality
– Safe
– Effective
– Patient-centred
– Timely
– Efficient
– Equitable

4 Pillars of Quality
Say
what
you
do
Do
What
you
Say
Prove
It
Improve
It
QUALITY
Ferlie & Shortell: Model for quality improvement
• Levels of Change
– Individual
– Group /Team
– Organisation
– Larger system /
environment
• Core properties
– Leadership
– Organisational culture
– Team /microsystems
development
– Information
Technology
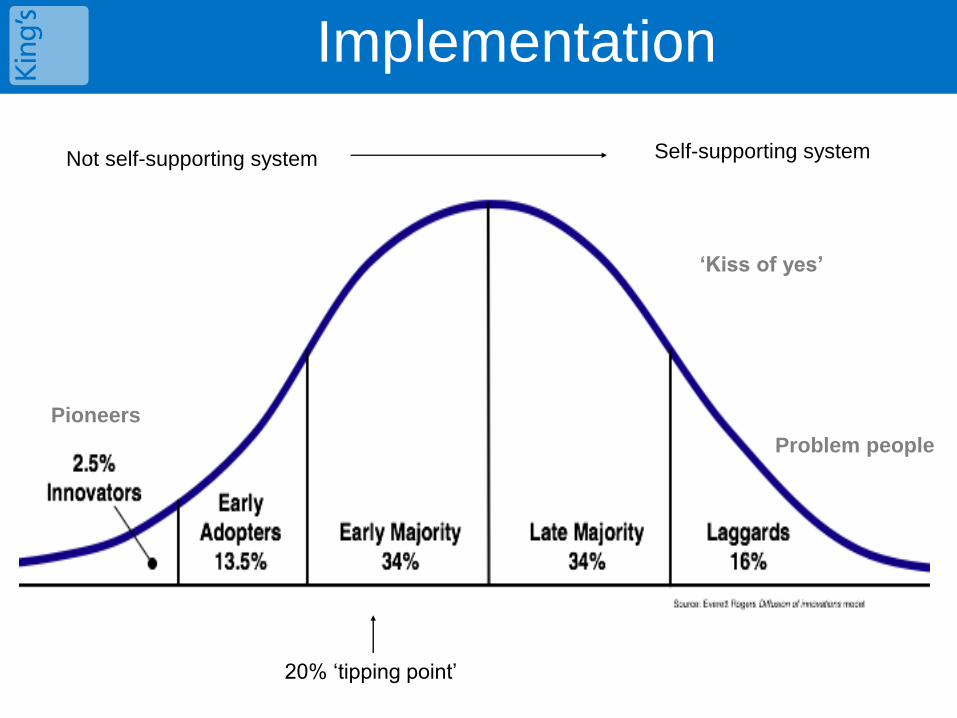
Implementation
20% ‘tipping point’
‘Kiss of yes’
Problem people
Self-supporting system Not self-supporting system
Pioneers

• Tacit knowledge –
• Held by an individual or shared by a community
• Explicit knowledge-
• Generalisable knowledge
Knowledge from research – evidence
Knowledge from the analysis of audit data – healthcare
statistics
Knowledge from the experience of clinicians and patients
Types of Knowledge

• Class 1 Randomised Controlled
Trials
• Class 2 Prospective, observational,
cohort, prevalence studies
• Class 3 Retrospective clinical,
database/registry, case
report study, expert opinion
• Challenges: Does not include qualitative methods
Traditional View of Evidence

Find the best evidence you can
Find appropriate evidence for your question
Traditional View of Evidence

Barriers to implementing EBP
• Work setting
• Authority to implement; lack of support from doctors & AHPs
• No data on what is already happening / what is being done / what
works
• Sharing the data with the wider team
• Research itself
• Relevance of research, presence of conflicting findings
• Presentation of research
• Readability of research, understanding statistics
• Person
• Ability to find and understand research
• Lack of time; engagement

Do we know
How We Are Doing?

• Collect Data
– Scorecards
– Surveys
– Audits
• Make collecting data easy
– Use & review data hospital collects & evaluates
– Share data
– Make sure everyone knows what the purpose of
collecting data is
• Engage all staff
– Make sure everyone knows what the purpose of
collecting data is
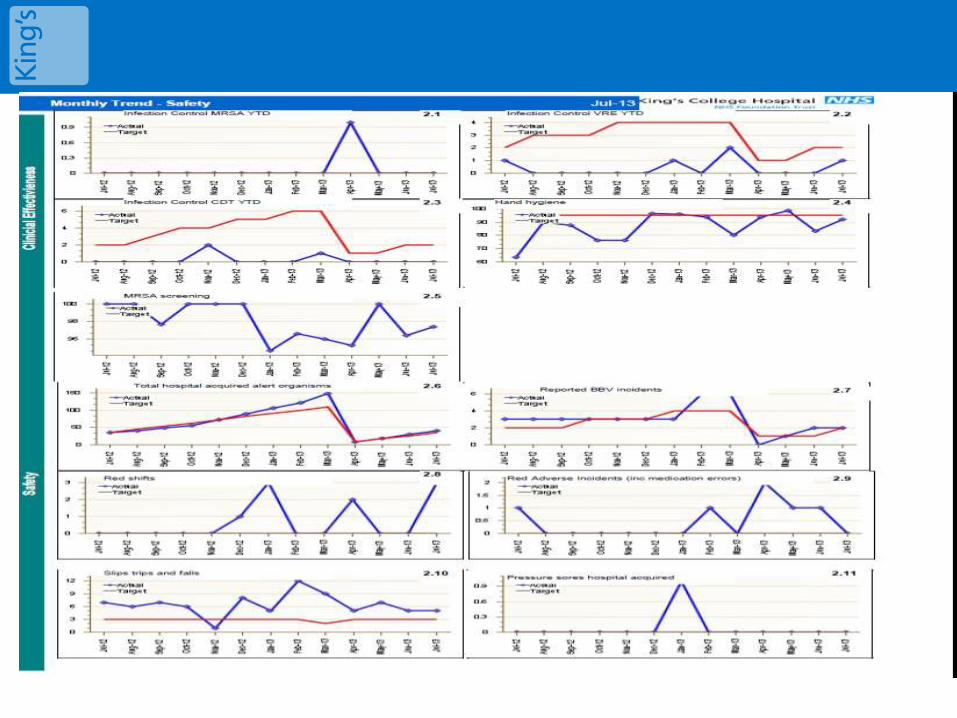
How do you know how you are doing?

Example: BMT Scorecard

How are we doing? –Ask your patients

How are we doing - Ask your customers
0
1
2
3
4
satisfaction
with turnaround
time
satisfaction
with turnaround
time for donor
searches
satisfaction
with
communication
about typing
not at all
not very
quite a bit
very much
don't know
Tissue Typing

0
2
4
6
8
satisfaction
with timing and
frequency of
clinic
appointments
not at all
not very
quite a bit
very much
don't know 0
2
4
6
8
ph
leb
oto
my
wa
itin
g t
ime
s
co
nti
nu
ity
co
mm
un
ica
tio
n
ph
arm
ac
y
pro
ce
du
res
an
d d
ay
un
it
ex
pe
rie
nc
e
not at all
not very
quite a bit
very much
don't know
0
2
4
6
8
10
satisfaction
with availability
of appropriate
staff for advice
our ability to
respond to
queries
accessibility of
beds to
transfer sick
patients
timeliness of
discharge post
bmt/
readmission
bmt co-
ordinators
not at all
not very
quite a bit
very much
don't know
Ask your customers (referring Hospitals)

Learn from Mistakes

What is reported?

Sources of Non-Compliances
(QPulse only; Datix AIs excluded)

Who reports your incidents ?

How can we do better ?
1. Measure what you are doing
– Learning through the process
– Measure over time
2. Understand the process
– Explains WHY the problem exists
– Tool for engaging staff
3. Improve reliability
– Helps to reduce waste in the process (time,
resource & reduces harm
– Consistent care
How can we do better ?
4. Demand, capacity and flow
– Understand the variation in the capacity
available
5. Engage all staff
– How the change is introduced, predicts the
success
– Engaging frontline staff is crucial
6. Involve patients
– Ask - ‘How do we know what constitutes
good care?’
– Patients may define quality differently from
clinicians & managers





![Bone marrow transplants for cancer (other than …...An autologous or allogeneic (ablative and non-myeloablative [mini-transplant]) hematopoietic stem cell transplantation, single](https://img.dokumen.tips/doc/110x75/5f0ea6807e708231d440431f/bone-marrow-transplants-for-cancer-other-than-an-autologous-or-allogeneic-ablative.jpg)
























