Embed Size (px)
Citation preview

HKDJJJJJ
122 Hong Kong Dent J Vol 2 No 2 December 2005
CASE REPORTHong Kong Dental Journal 2005;2:122-5
Introduction
Lichen planus (LP) is a common idiopathic mucocutaneousdisorder with oral lesions 1. It may involve oral, genital,and other mucosae, skin, and nails. Ocular, nasal, laryngeal,otic, esophageal, gastric, bladder, and anal involvementmay also be present. In addition to the common idiopathicLP, drug-induced LP was reported in the early twentiethcentury (as a consequence of arsenicals used in thetreatment of syphilis). It also became more common duringWorld War II among military personnel prescribing anti-malarial drugs 2. Drug-induced lichenoid reactions are rarecompared with other similar dermatoses but can manifestdue to a variety of drugs (Table) 3. Oral lesions are morecommon with drugs, such as angiotensin-convertingenzyme inhibitors and non-steroidal anti-inflammatorydrugs. Although less common, more frequently used drugs,
such as methyldopa and allopurinol, have been reportedto cause lichenoid reactions 4,5. Early diagnosis, withdrawaland/or replacement of the causative drug, and appropriatemanagement strategies are essential 6.
Case report
A 75-year-old Chinese woman was referred by her dentistto the Oral Diagnosis Clinic, Prince Philip Dental Hospital,Hong Kong in December 2002, with a history of painfululceration on the sides of her tongue, and bilateral cheekmucosae. The lesions had been present for over a monthand were accompanied by occasional dryness of themouth. The lesions and associated soreness started overthe left cheek and gradually appeared over the rightside with worsening of the pain and soreness. Impairedoral function, such as inability to wear her partial denture,dysarthria, dysphonia, dysphagia, and the resultantreduction in food intake and subsequent fall in bodyweight were also reported. Prior to referral, the patienthad visited her general medical practitioner and dentalpractitioner, neither of whom had been able to offer aspecific diagnosis or management except for a palliativesaline mouth rinse.
The patient’s medical history revealed diverticulosis,chronic bronchitis with bronchiectasis, pulmonarytuberculosis, and anxiety disorder with existing problems,such as hypothyroidism or myxedema, uncomplicatedhypertension, and gout. She was taking methyldopa
* Oral Medicine and Pathology, School of Dentistry and Oral Health,Griffith University, 16-30 High Street, Southport, Gold Coast, Australia
† Oral Diagnosis, Faculty of Dentistry, The University of Hong Kong,Hong Kong
‡ Paediatric Dentistry and Orthodontics, Faculty of Dentistry, TheUniversity of Hong Kong, Hong Kong
§ Oral Biosciences, Faculty of Dentistry, The University of Hong Kong,Hong Kong
Correspondence to:Dr. Raj G. NairSchool of Dentistry and Oral Health, Griffith University, Gold Coast,AustraliaTel : (61-7) 5678 0793Fax : (61-7) 5678 0708e-mail : [email protected]
Severe oral erosive lichen planus due tomethyldopa and allopurinol: a case report
Raj G. Nair *, BDS, MSc, PhD
Philip R. H. Newsome †, PhD, MBA, MRDRCS
Anut Itthagarun ‡, DDS, PDipDS, PhD
Lakshman P. Samaranayake §, DDS, MRCPath
ABSTRACT Oral lichen planus is a common condition with an unclear etiology although some common drugs havebeen implicated. We report on a 75-year-old Chinese woman with painful erosions and ulceration of the lateral tongue,gingivae, and buccal mucosa who had been taking methyldopa for several years and allopurinol for more than a month.Following the classic bilateral presentation, a provisional clinical diagnosis of oral erosive lichenoid planus was madeand drug therapy changed to metoprolol and paracetamol. Topical steroids, analgesic, and antiseptic mouth rinse wereprescribed. After 6 weeks, all lesions had resolved although a few Wickham’s striae remained. The patient’s oral functionwas restored and to date the lesions are in remission. It appears that proper identification of the causative drug togetherwith its immediate withdrawal and adjunctive topical therapy is an effective method for treating drug-induced lichenoidreactions.

Diagnosis and management of drug-induced oral lichen planus
Hong Kong Dent J Vol 2 No 2 December 2005 123
250 mg twice daily; allopurinol 100 mg once daily;thyroxine sodium 50 µg daily; and multivitamins. She waswidowed and living alone, a non-smoker, and consumedno alcohol or recreational drugs. She claimed to eat abalanced diet and was allergic to carbamazepine. Therewas no significant family history or similar problemreported by any of her immediate family.
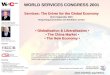
Physical examination revealed puffiness of the skinof both cheeks with mild erythema, warm to touch orpalpation, and a small healing ulcer (2-3 mm diameter)on the right upper lip laterally. The latter was said torecur frequently, especially during cooler months. Therewas no cervical lymphadenopathy and no other extraorallesions. Intraorally, desquamative gingivitis affectingthe anterior lower marginal gingivae, and both the buccalmucosae were present with white striae and multiplewhite plaques surrounding the margin of a large erosionand ulceration with irregular margins measuring about 2to 3 cm. Erythema and erosive lesions with irregular bordersmeasuring around 3 cm were found on the lateral bordersof the tongue extending from the posterior second or thirdto the tip of the tongue (Figures a and b). White Wickham’sstriae were also noted on the anterior two thirds of thedorsum of the tongue extending over 2 cm in diameter.Mild xerostomia (possibly due to methyldopa) wasnoticed with an unstimulated sialometry reading of 1.5 mLin 15 minutes (normal reading, ≥1.5 mL in 15 minutes).It was possible to induce saliva flow into the oral cavityby palpation of the salivary glands.
The initial presentation was pathognomonic for oralerosive LP presenting as a white reticular pattern,white plaques and erosions. After consultation withthe patient’s medical practitioner, methyldopa andallopurinol were discontinued and betamethasone0.5 mg tablets as mouth rinse 4 times a day and Difflam-Csolution mouth rinse (3M Pharmaceuticals Pty Ltd.,Thornleigh, Australia) containing benzydaminehydrochloride 0.15% with chlorhexidine gluconate 0.12%,3 to 4 times daily were prescribed. The lesion on the lipwas empirically diagnosed as recurrent herpes labialis dueto herpes simplex virus infection, for which acyclovir 5%cream 5 times daily was prescribed. A biopsy of the lesionwas not taken immediately due to the severity of the lesionon initial presentation. Upon request, the patient’s medicalpractitioner replaced methyldopa with metoprolol 50 mgtwice daily and discontinued allopurinol because her goutattacks were under control and could be effectivelymanaged with paracetamol on an as-required basis.
Six weeks later the patient presented with completeresolution of her erosive lesions with marked reduction inerythema (Figures c and d) and complete healing ofherpes labialis infection. Xerostomia was managed bydiscontinuation of the methyldopa, saliva substitute,Salivart (Gebauer, Cleveland, United States), and Difflamgel (3M Pharmaceuticals Pty Ltd.) for about a month andthe frequent sipping of water. There was also markedimprovement in mastication, swallowing, and speech, andshe was able to wear her denture.
Angiotensin-converting enzyme Ketoconazole Prazosininhibitors Labetalol ProcainamideAllopurinol Levamisole PropranololAmiphenazole Lincomycin PropylthiouracilAntimalarials Lithium Protease inhibitorsBarbiturates Lorazepam ProthionamideCaptopril Mepacrine QuinidineCarbamazepine Mercury (in amalgam) QuinineCarbimazole Metformin RifampicinChloral hydrate Methyldopa StreptomycinChloroquine Metronidazole SulphonamidesChlorpropamide Niridazole TetracyclineCinnarizine Non-steroidal anti-inflammatory drugs TocainideClofibrate Oral contraceptives TolbutamideColchicine Oxprenolol TriprolidineDapsone Para-aminosalicylateDipyridamole PenicillamineEthionamide Penicillins Vaccines:Flunarizine Phenindione Bacille Calmette-GuérinGaunoclor Phenothiazines CholeraGold Phenylbutazone Hepatitis BGriseofulvin PhenytoinHydroxychloroquine PiroxicamInterferon-α Practolol
Table List of reported drugs that may cause a lichenoid reaction 3

Nair et al
124 Hong Kong Dent J Vol 2 No 2 December 2005
The patient has regular follow-up and to date, almost10 months after withdrawal of the two drugs, the orallesions have not recurred except for faint and scantyWickham’s striae over the buccal mucosae. No xerostomiaor recurrence of herpes labialis has been noted either. Shehas been taking thyroxine sodium 50 µg once daily;hypertension remains controlled and she has had no newattacks of gout.
Discussion
A number of drugs can precipitate a range of orofacialproblems, predominantly oral ulceration and dryness ofthe mouth. Drug-induced lichenoid reactions, includingthose due to methyldopa and allopurinol, have beenreported (Table) 3-5. Drugs including non-steroidalanti-inflammatory agents and angiotensin-convertingenzyme inhibitors are the most common offenders 3.Nonetheless a host of other miscellaneous drugs, such asamiphenazole, some of the beta-blockers, carbamazepine,cinnarizine, cyanamide, f lunarizine, isoniazid,
ketoconazole, levopromazine, lithium, lorazepam,methopromazine, para-aminosalicylic acid, penicillamine,phenothiazines, pyrimethamine, quinidine, quinine,streptomycin, and thiazide diuretics have been observedto cause mucocutaneous LP or lichenoid reactions 1.Most are isolated case reports and at times multiple drugsare involved.
It has been proposed that drug-induced lichenoidreactions are usually unilateral and may be erosive and/or ulcerative in nature although this is not always the case.The oral manifestation may present as any of the LPvariants, such as white striae with reticular formation,atrophic, plaque-like, erosive or ulcerative types.
It has been suggested that histopathologically,drug-induced lichenoid reactions present with anincreased lymphocytic infiltrate with eosinophils andcolloid bodies. This differs to the idiopathic variant of LP 7.Circulating antibodies to epithelial components havebeen noted by some but not others 8. The exact
(a)
(c)
(b)
(d)
Figure Clinical photograph showing erosion, erythema, and Wickham’s striae presenting at the first visit: (a) left buccalmucosa and (b) left lateral tongue, and 6 weeks after withdrawal of causative drugs and palliative care: (c) left buccalmucosa and (d) left lateral tongue

Diagnosis and management of drug-induced oral lichen planus
Hong Kong Dent J Vol 2 No 2 December 2005 125
pathological mechanism of drug-induced lichenoidreactions remains unclear although an immunogeneticpredisposition has been postulated 9.
Methyldopa is a centrally acting anti-hypertensiveagent, known to be associated with orofacial complicationssuch as xerostomia, sialadenitis, Bell’s palsy, as well asgastro-intestinal disturbances and abnormal liver function.A window period of 5 months to almost 60 months hasbeen reported necessary for the development ofmethyldopa-induced lichenoid reactions, and drugwithdrawal leads to healing and lesion resolution aftera few months 4. In this patient different anti-hypertensiveagents had been prescribed for almost 20 years, includingmethyldopa. No oral lesions developed until allopurinolwas added to her drug regimen. The exact date andduration of methyldopa intake could not be verifiedbecause the patient could not recall or produce anyrecords of the specific drugs taken for hypertension in thepast. This suggests the initiating agent to be methyldopafurther synergized by the exacerbating effect ofallopurinol. Methyldopa was also likely the cause of hermouth dryness, especially when one considers thetransient nature of her xerostomia and the gradualimprovement of the condition that occurred once thedrug was withdrawn.
Allopurinol is an analog of hypoxanthine thatfunctions by interfering with an enzyme xanthineoxidase, that helps convert xanthine and hypoxanthineto uric acid. A wide variety of adverse reactions havebeen reported inducing hypersensitivity reactions,gastro-intestinal disturbances, bone marrow suppression,hepatic and renal impairment, and a variety of skinlesions. Allopurinol-induced oral ulcerative lichenoidreactions have also been reported 5,10. Such cases havebeen characterized by a short course of the disease,with rapid recovery and complete healing of ulcerationwith persistence of white reticular patterns afterdrug withdrawal and adjunct topical corticosteroidtherapy 5. These cases were similar to the patient reportedhere.
This report reaffirms the importance of awareness ofsuch lesions and conditions, especially when making adifferential diagnosis. For example, etiopathogenesisof Grinspan’s syndrome—a triad of hypertension, diabetesmellitus, and LP—has been suggested to be due to anti-hypertensive, anti-diabetic and other drugs and not a triadof diseases 11.
In this patient, substitution of metoprolol was welltolerated by the patient without any side-effects. Despitethis, beta-blockers, in particular propranolol, have beenreported to cause lichenoid reactions 12. This report alsohighlights the importance of monitoring commonly useddrugs for adverse effects. Drug-induced orofacialmanifestations are rarely mentioned as adverse effects,either in drug references or drug formularies.
Conclusion
This appears to be the first report in the English literatureof a methyldopa- and allopurinol-induced erosivelichenoid reaction in a Chinese female. Although bothmethyldopa and allopurinol have not usually beenconsidered to cause such a reaction, their use amongelderly patients in particular warrants close monitoring.This report also highlights the importance of identifyingthe offending drugs and withdrawing them, and thepalliative treatment options. Referral to a specialist is vital.
References
1. Scully C, el-Kom M. Lichen planus: review and update onpathogenesis. J Oral Pathol 1985;14:431-58.
2. Nisbet T. New cutaneous syndrome occurring in New Guinea andadjacent islands. Preliminary report. Arch Derm Syphilol 1945;52:221-5.
3. Scully C, Bagan JV. Adverse drug reactions in the orofacial region.Crit Rev Oral Biol Med 2004;15:221-39.
4. Brooks SL. Lichenoid reaction of oral mucosa and skin tomethyldopa. J Oral Med 1982;37:42-4.
5. Chau NY, Reade PC, Rich AM, Hay KD. Allopurinol-amplifiedlichenoid reactions of the oral mucosa. Oral Surg Oral Med OralPathol 1984;58:397-400.
6. Porter SR, Scully C. Adverse drug reactions in the mouth. ClinDermatol 2000;18:525-32.
7. Van den Haute V, Antoine JL, Lachapelle JM. Histopathologicaldiscriminant criteria between lichenoid drug eruption andidiopathic lichen planus: retrospective study on selected samples.Dermatologica 1989;179:10-3.
8. Ingafou M, Lodi G, Olsen I, Porter SR. Oral lichen planus is notassociated with IgG circulating antibodies to epithelialantigens. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84:175-8.
9. Powell FC, Rogers RS, Dickson ER, Moore SB. An associationbetween HLA DR1 and lichen planus. Br J Dermatol 1986;114:473-8.
10. Khoo BP, Leow YH. A review of inpatients with adverse drugreactions to allopurinol. Singapore Med J 2000;41:156-60.
11. Lamey PJ, Gibson J, Barclay SC, Miller S. Grinspan’s syndrome: adrug-induced phenomenon? Oral Surg Oral Med Oral Pathol 1990;70:184-5.
12. Massa MC, Jason SM, Gradini R, Welykyj S. Lichenoid drug eruptionsecondary to propranolol. Cutis 1991;48:41-3.