Embed Size (px)
Citation preview

HIV Medications – Where We’ve Been and Where We Are Headed
Dwayne Haught, MSN, ACRN
June 13, 2011

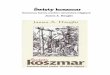
MMWR June 5, 1981
Pneumocystis carinii pneumonia(PCP)

A Month Later in July 1981
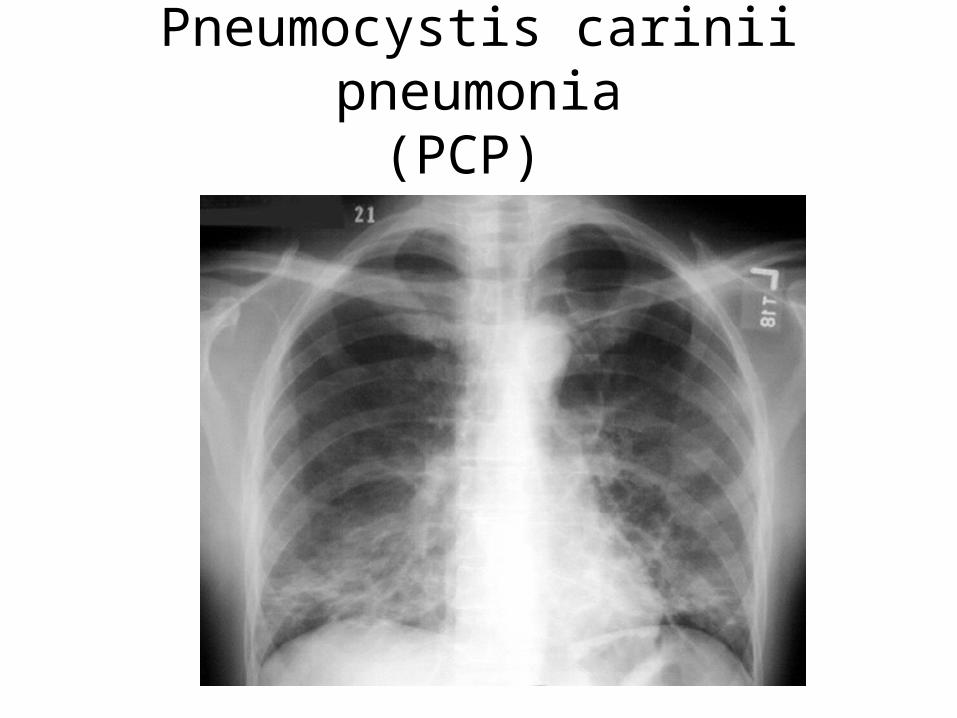
• MMWR reported that over the past 30 months, 26 young gay men had been dx with an aggressive skin malignancy, Kaposi’s Sarcoma (KS)
Kaposi’s Sarcoma

August 28, 1981 MMWR
• Reported an additional 70 cases of KS and PCP had been diagnosed
• By the end of the Summer 1981 the contours of a full-blown epidemic was already coming into view
• By the years end 150 adults and 9 children in the U. S. had died of the new immune-related illness

Initial Response
• A “gay disease”• Community and health
care workers critical of these “gay outsiders” feared that they would also become infected
• In just 2 years, HIV went from 5 gay men to a huge escalation of hundreds of cases

As public health moved slow and inefficiently “AIDS Hysteria” began to spread through the general public
Public fear over AIDS contaminated blood supply erupts in 1983
Huge Concern for Public Health

Ryan White
• Teenager, contracted HIV through contaminated clotting factor
• Fought to remain in public school
• Died in 1990 a few months before the federal Ryan White CARE Act would be implemented

HIV Discovered 1983
HIV Discovery
• Leads to an HIV test kit being developed that can be used to test HIV antibody development in people that are infected with the virus
• Also, now that the virus had been isolated it’s enzymes, replication process, structures, and genes could be studied for possible drug development
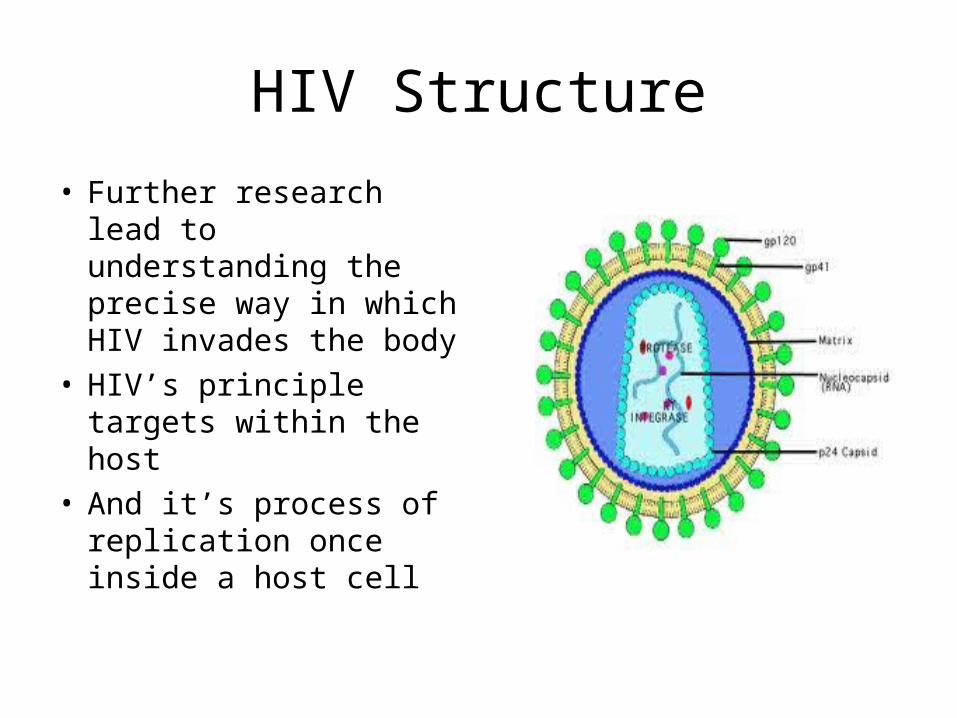
HIV Structure
• Further research lead to understanding the precise way in which HIV invades the body
• HIV’s principle targets within the host
• And it’s process of replication once inside a host cell

Helper T Cells (CD4s)
• HIV is attracted to the coating (CD4) on human Helper T Cells
• These cells are responsible for directing immune system responses to many disease causing organisms(Quarterback)
• Over time HIV depletes the reserve of T Helper cells and the body can no longer adequately fight off disease causing organisms

AZT Approved for HIV Treatment
• FDA approved 3/19/87
• Approved in record time
• Only 1 trial in humans instead of the standard 3
• Trial stopped after 19 weeks

AZT - Zidovudine
• Monotherapy – initially taken alone
• Inhibits viral enzyme “reverse transcriptase”
• Slows HIV replication but it is not a cure
• Great excitement about it’s approval in 1987

1987 – 1995Period of Monotherapy
• More drugs developed with similar actions like AZT
• Primarily taken as single therapy but occasionally 2 pills taken
• Therapeutic effects were not long lasting

Early HIV Medication Treatment
• Heavy pill burden – difficulty getting meds absorbed
• Dosing q 4-6 hours around the clock
• Toxicities and side effects – anemia and Peripheral Neuropathy
• Therapeutic effect of meds not long lasting

Significant Scientific Advances• Recognition of the
persistence of viral replication
• Billions of HIV particles being produced and destroyed daily
• Emergence of symptoms due to host’s immune system loosing the battle

Resistance
• Virus becomes less sensitive to anti-HIV medications
• HIV multiplies so rapidly that occasionally a small genetic mutation can occur
• The mutation can make HIV less sensitive to the effects of medications
• Resistance complicates and limits treatment options

Combination Therapy1995 to Today
• First Protease Inhibitor FDA Approved in 1995
• Began the period of Combination Therapy• Goals of Therapy
– Prolong life and improve quality of life– Suppress HIV levels below the limit of detection,
or as low as possible for as long as possible– Optimize and extend the use of current tx– Minimize toxicity and manage side effects

1995
• Dramatic effect on HIV related illnesses and death
• Highly Active Antiretroviral Therapy
• (HAART)• Reduced virus and
increased CD4s• Standard of care by
1997

Impact of Combination Therapy• Significant decline in death rates due to AIDS
since the mid 1990s as well as decreases in new AIDS dx and hospitalizations for AIDS-related complications
• Long term toxicities notably damage to vital organs such liver, kidneys, heart and metabolic toxicities
• Provide a window of opportunity for immune boosting or even curative treatments

Decline in AIDS Cases and AIDS Related Deaths

Today - 2011
From this. . . . . . . . . . To this. . . . . . . .

HIV Lifecycle

When to Start Treatment?• All with an AIDS-Defining illness or with a CD4
count <350
• Recommend with CD4 counts between 350 – 500
• All with HIV associated nephropathy; coinfection with Hep B and/or Hep C
• Pregnant women
• >500 CD4s National Panel divided – 50% treat – 50% optional
• www.aidsinfo.nih.gov

HIV Life Cycle

What Treatments Can We Expect to See in the Next 2
Years?

New and Innovative Therapy
• HIV Gene Therapy
• Study
• Results
• Implications

Resources
• AIDSinfonet.org
• http://hivinsite.ucsf.edu
• http://aactg.org
• Aidsmeds.com
• TheBody.com
• TheWellProject.com

There Still is No Cure For HIV






![3 Participant Round Robin 3rd Place Participant Round Robin ...[©Escape Sports, Inc.] ... Nolan Haught Edison Wesley Sarko Panthers BYE Nolan Haught BYE Nathan Boggs Cameron 525](https://img.dokumen.tips/doc/110x75/5aacdd867f8b9a8d678d6c97/3-participant-round-robin-3rd-participant-round-robin-escape-sports-inc-.jpg)