Embed Size (px)
Citation preview
lnt. J . Cancer: 11, 338-344 (1973)
HISTOLOGIC CHARACTERISTICS OF BREAST CANCER IN BOSTON AND TOKYO
Brian MACMAHON, Alan S. MORRISON, Lauren V. ACKERMAN, Raffaele LATTES, Herbert B. TAYLOR and Shu YUASA
Department of Epidemiology, Harvard School of Public Health, Boston, Massachusetts; Department of Pathology, Washington University, St. Louis, Missouri;
Department of Surgical Pathology, Columbia University, New York, N. Y.; Armed Forces Institute of Pathology, Washington, D. C., USA;
and Department of Epidemiology, National Institute of Public Health, Tokyo, Japan
Histologic slides from representative series of breast cancer patients in Boston, where the incidence rate of breast cancer is high, and in Tokyo, where the incidence rate is low, were reviewed by pathologists who did not know the city of origin of the material. Intraductal, medullary and colloid histologic types were relatively more frequent in Tokyo. Also more frequent in Tokyo were tumors with circumscribed margins and a high degree of cellular reaction. Tumors of small-cell or invasive ductal histologic type and tumors with a high degree of fibrosis were more frequent in Boston than in Tokyo.
A prominent characteristic of the epidemiology of breast cancer is international variation in incidence rates. One of the best-known features is that the age-standardized incidence rate is approximately six times higher in the United States than in Japan. There has been little study of whether differences in the histologic structure of breast cancer accompany these variations in incidence rate. As part of a recent international study, histologic slides were obtained from female breast cancer patients in Boston and Tokyo. The slides were assembled primarily for the purpose of establishing the diagnosis of cancer in women interviewed in an epidemiologic case-control study. Part of this histologic material has now been reviewed in greater detail, and in this report characteristics of the tumors in American and Japanese women are compared.
MATERIAL AND METHODS
The details of the parent case-control studies have been described previously (Salber et at.,
Received: October 20, 1972.
1969; Yuasa and MacMahon, 1970). As far as could be ascertained, the 758 breast cancer patients in Boston were all the female patients diagnosed in a geographically defined population between January, 1965, and December, 1966. The 861 breast cancer patients in Tokyo were all female patients first diagnosed in 25 of the largest hospitals in the city between April, 1965, and March, 1967. While the Tokyo patients probably represented only about half of the cases first diagnosed in the prefecture of Tokyo-to during the study period, there is no reason to believe that they were unrepresentative of cases in the area.
Pathologists in the participating hospitals furnished histologic slides to the study center for 709 (94%) of the patients in Boston and 757 (88%) of those in Tokyo. All the slides were examined by a single pathologist l, and on the basis of this diagnosis the specimens were divided into two groups: the invasive ductal tumors which constituted the majority of cases in
Dr. Harry Carter, Department of Pathology, New England Deaconess Hospital, conducted the first central review of histologic slides.
338

BREAST CANCER HISTOLOGY IN BOSTON AND TOKYO
both centers (group I), and all others (group 11). In instances in which more than one slide had been submitted, this pathologist also designated a single slide as exhibiting the histologic charac- teristics of that particular tumor. For this study, random samples of approximately 10% of the group I slides and 100% of group I1 slides were drawn. Sixty-four slides from Boston and two from Tokyo were received late and were not sampled. Of the slide numbers selected, 11 from Boston and three from Tokyo were found to be missing. The composition of the sample is shown in Table I. Of the slides submitted to reviewers, 52 American and 57 Japanese slides were from group I and 110 American and 148 Japanese slides were from group 11.
At the statistical center, the original slide numbers were masked, code numbers applied, and the slides circulated for review to each of three pathologists (L. V. A., R. L. and H. B. T.). Each pathologist was asked to classify each slide according to histologic type, tumor margin circumscription, degree of cellular reaction, and degree of fibrosis.
Twenty-six slides were excluded because on initial examination all three reviewers considered the slide to be of inadequate quality or classified the specimen as a metastasis, a sarcoma, or as not malignant. There were 28 slides for which there was disagreement between reviewers as to whether the lesion was primary carcinoma of the breast. For 20, the disagreement was on whether the lesion was malignant or benign, for 5 on the adequacy of the preparation, for 2 on the question of whether the malignancy observed was primary and for one on whether the lesion was a sarcoma. The three reviewers held a conference and, without knowledge of the center from which each slide came, arrived at a con- sensus diagnosis for each of these 28 slides. Nine of the 28 specimens were excluded-seven because the consensus was " not malignant " and two because of inadequacy of the preparation. The remaining 19 specimens were retained.
For the analyses to be presented, the histologic type was assigned by concordance of the diagnoses of at least two pathologists. For circumscription of the tumor margins, degree of cellular infiltration, and degree of fibrosis--each read as one of three grades by each reviewer-the slide was assigned the rounded average of the grades given by the three reviewers. In the few
instances in which there were only two observers and the two readings differed by one grade, half were assigned at random to each grade.
Statistical methods The method of selection of slides for review
involved double sampling. Results from the sample are extrapolated to the sampled popula- tion, and presented as differences between Boston and Tokyo with respect to estimates of the percentages of cases with a particular histologic characteristic in the original series. Variance estimates are computed as described by Cochran (1963). Ninety-five per cent confidence limits for
TABLE I
COMPOSITION OF SAMPLE A N D NUMBERS OF CASES EXCLUDED FROM ANALYSIS,
WITH REASONS FOR EXCLUSION
Boston Tokyo
Received in time to be sampled 645 755 Sampled for study 173 208 Missing 11 3
~
Submitted to reviewers 162 205
Excluded before conference : Poor preparation 4 6 Not malignant 2 8 Metastasis 2 2 Sarcoma 2 0
Not malignant 0 7 Poor preparation 2 0
Excluded at conference :
All exclusions 12 23
Number of specimens analysed 150 182
these differences are given, and a difference is considered statistically significant if this interval does not include zero. Whenever an empty cell occurred in a Table, one was added to each cell of the Table before calculating variances and confidence intervals. This procedure is adapted from a suggestion of Sheehe (1966).
In individual Tables, deviations from the total numbers of cases given in Table I are due to a characteristic being classified " unknown " by a majority of the reviewers.
339

MACMAHON ET AL.
FIGURE 1 .
small foci of calcification ( Atypical intraductal hyperplasia, with suggestive cribriform pattern and
350, W. U. Neg. 72-1449).
RESULTS
Agreement between reviewers
As shown in Table I, there were ten slides which all three reviewers considered to be not malignant. There were twenty additional slides in which there was disagreement as to whether malignancy was present or not. At conference, 13 of these 20 were considered malignant and 7 not.
The most frequent differences of opinion were on whether or not a particular intraductal or papillary lesion should be classified as benign or malignant. The obvious intraductal cancer is made up of very atypical cells lining a duct and incorporating areas of necrosis and calcification. The intraductal proliferative lesion illustrated in the photomicrograph (Fig. 1) shows cells which are not very atypical and there is little or no necrosis. Differences between pathologists in
340

BREAST CANCER HISTOLOGY IN BOSTON AND TOKYO
assigning a diagnosis to such a lesion depend largely on the individual pathologist’s experience and conception of the frequency with which this type of lesion progresses to or is associated with intraductal cancer.
In considering the relatively large proportion of slides diagnosed by these reviewers as not malignant, although classified as malignant by the original reviewer (17 out of 349 slides), it should be noted that: (1) the intraductal and papillary lesions, in which disagreement was most frequent, were assigned to group I1 and were therefore sampled with a frequency ten times that of the common infiltrating ductal tumors, and (2) for this study only one slide was reviewed for each patient, whereas in the original review all available material was examined.
Although not relevant to the issue of observer- agreement, it is of interest that 15 of the Japanese but only two of the Boston specimens were considered not malignant by these reviewers. If these specimens indeed represent controversial lesions of the intraductal type, this Boston-Tokyo difference complements the data to be presented on the greater frequency of intraductal lesions in the Japanese specimens.
Table I1 shows the extent of agreement between pathologists on the assignment of histologic type. Only slides not discussed at the reviewers’ conference are included in the Table. All three pathologists agreed on the histologic type of tumor in two-thirds of the slides, and in all of the remainder two of the reviewers agreed on a single diagnosis.
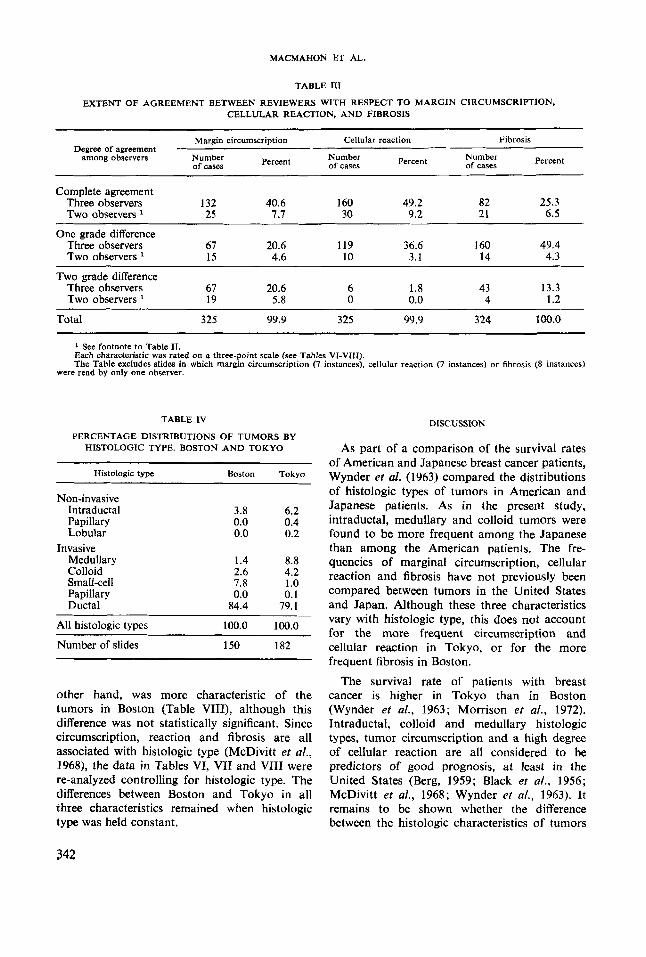
The extents to which the reviewers agreed on the assignment of values for tumor margin circumscription, cellular reaction and fibrosis are shown in Table 111. The best agreement was on cellular reaction. There was no more than a one-grade difference among the reviewers for 96% of the slides. Disagreement was greater for tumor margin circumscription and for fibrosis, but for each of these characteristics the reviewers differed by no more than one grade in more than two-thirds of the slides.
Diferences between Boston and Tokyo
The distributions by histologic type are compared in Table IV. Intraductal, medullary and colloid tumors were more frequent in Tokyo, and small-cell and invasive ductal tumors more frequent in Boston. Non-invasive papillary and
lobular tumors were rare, and are combined with intraductal tumors for the remainder of the analysis. The one invasive papillary tumor was grouped with the invasive ductal tumors.
The differences between Boston and Tokyo are examined in detail in Table V. Four questions are asked: 1. Does the proportion of intraductal tumors
differ between Boston and Tokyo? 2. Among invasive tumors, does the proportion
of medullary tumors differ between Boston and Tokyo?
3. Among the colloid, small-cell, and ductal tumors, does the proportion of colloid tumors differ between Boston and Tokyo?
4. Among the small-cell and ductal tumors, does the proportion of small-cell tumors differ between Boston and Tokyo?
TABLE I1
EXTENT OF AGREEMENT BETWEEN REVIEWERS
TYPE WITH RESPECT TO ASSIGNMENT OF HISTOLOGIC
Observers agreeing Percent
All observers agree Three observers 208 66.5 Two observers 5 1.6
One observer disagrees Three observers 100 31.9
- -~ ~
Total 313 100.0
Whenever a pathologist rated a slide “ unknown ” or did not classify a slide for a particular characteristic, he was not included as an observer.
Although intraductal and colloid tumors were more frequent in Tokyo than in Boston, the differences were relatively small and not statisti- cally significant. The substantial excess of medullary tumors in Tokyo does reach the 95% significance level. Although small-cell tumors were substantially more frequent in Boston, this difference does not quite reach conventional statistical significance.
Tumors with circumscription of the margin and tumors with moderate or severe cellular reaction were found significantly more frequently in Tokyo (Tables VI and VII). Fibrosis, on the
341
MACMAHON ET AL.
TABLE I11
EXTENT OF AGREEMENT BETWEEN REVIEWERS WITH RESPECT TO MARGIN CIRCUMSCRIPTION, CELLULAR REACTION, AND FIBROSIS
Margin circumscription Cellular reaction Fibrosis
among observers Number of cnses
Degree of agreement Percent Number
of cases Percent Number of cases Percent
-
Complete agreement Three observers 132 40.6 160 49.2 82 25.3 Two observers 25 I .7 30 9.2 21 6.5
One grade difference Three observers 67 20.6 119 36.6 160 49.4 Two observers 15 4.6 10 3.1 14 4.3
Two grade difference Three observers 67 20.6 6 1.8 43 13 .3 Two observers 19 5.8 0 0.0 4 1.2
Total 325 99.9 325 99.9 324 100.0
1 See footnote to Table 11. Each characteristic was rated on a three-point scale (see Tables VI-VIII). The Table excludes slides in which margin circumscription (7 instances), cellular reaction (7 instances) or fibrosis (8 instances)
were read by only one observer.
TABLE IV
PERCENTAGE DISTRIBUTIONS OF TUMORS BY HISTOLOGIC TYPE. BOSTON A N D TOKYO
Histologic type Boston Tokyo
Non-invasive Intraductal 3.8 6.2 Papillary 0.0 0.4 Lobular 0.0 0.2
Medullary 1.4 8.8 Colloid 2.6 4.2 Srnali-cell 7.8 I .o Papillary 0.0 0.1 Ductal 84.4 79.1
Invasive
All histologic types 100.0 100.0
Number of slides 150 182
other hand, was more characteristic of the tumors in Boston (Table VIII), although this difference was not statistically significant. Since circumscription, reaction and fibrosis are all associated with histologic type (McDivitt et a/., 1968), the data in Tables VI, VII and VIII were re-analyzed controlling for histologic type. The differences between Boston and Tokyo in all three characteristics remained when histologic type was held constant.
DLSCUSSION
As part of a comparison of the survival rates of American and Japanese breast cancer patients, Wynder et al. (1963) compared the distributions of histologic types of tumors in American and Japanese patients. As in the present study, intraductal, medullary and colloid tumors were found to be more frequent among the Japanese than among the American patients. The fre- quencies of marginal circumscription, cellular reaction and fibrosis have not previously been compared between tumors in the United States and Japan. Although these three characteristics vary with histologic type, this does not account for the more frequent circumscription and cellular reaction in Tokyo, or for the more frequent fibrosis in Boston.
The survival rate of patients with breast cancer is higher in Tokyo than in Boston (Wynder et al., 1963; Morrison er a/., 1972). Intraductal, colloid and medullary histologic types, tumor circumscription and a high degree of cellular reaction are all considered to be predictors of good prognosis, at least in the United States (Berg, 1959; Black et a[., 1956; McDivitt et al., 1968; Wynder et a/., 1963). It remains to be shown whether the difference between the histologic characteristics of tumors
342

BREAST CANCER HISTOLOGY IN BOSTON AND TOKYO
TABLE V
CONFIDENCE LIMITS OF THE DIFFERENCE BETWEEN BOSTON AND TOKYO WITH RESPECT TO FREQUENCY OF VARIOUS HISTOLOGIC TYPES OF TUMOR
95 % confidence limits Histologic type Boston Tokyo Difference for difference
% % Lower Upper
Intraductal tumors 3.8 6.8 -3.0 -8.7 2.7
Colloid tumors 2.7 5.0 -2.2 -7.5 3.0 Small-cell tumors * 8.5 1.3 7.2 -0.5 14.9
Medullary tumors 1.4 9.5 -8.1 - 16.0 -0.1
' Expressed as a percentage of all tumors.
* Expressed as a percentage of colloid, ductal and small-cell tumors. Expressed as a percentage of all invasive tumors.
Expressed as a percentage of ductal and small-cell tumors.
TABLE VI
PERCENTAGE DISTRIBUTIONS OF TUMORS BY DEGREE OF CIRCUMSCRIPTION OF TUMOR
MARGIN. BOSTON AND TOKYO
Circumscription of tumor margin Boston Tokyo
None Questionable Definite
74.0 49.0 24.1 35.5
1.9 15.6 ~.
Total 100.0 100.1
TABLE VIII
PERCENTAGE DISTRIBUTIONS OF TUMORS BY DEGREE OF FIBROSIS. BOSTON AND TOKYO
Fibrosis Boston Tokyo
None or minimal Moderate Severe
15.7 26.1 54.0 53.5 30.2 20.4
Total 99.9 100.0
Number of patients 149 175
Number of patients 150 175
% definite circumscription (Boston) minus % definite circumscription (Tokyo) = - 13.7%. 95 % confidence limits for difference = -22.2% to -5.1 %.
' % moderate and severe fibrosis (Boston) minus % moderate and severe fibrosis (Tokyo) = 10,3%. 95% confidence limits for difference: -1.1% to 21.8%.
TABLE VII
PERCENTAGE DISTRIBUTIONS OF TUMORS BY DEGREE OF CELLULAR REACTION.
BOSTON AND TOKYO
Cellular reaction Boston Tokyo
None or minimal 69.2 40.1 Moderate 28.0 43.1 Severe 2.9 16.9
Total 100.1 100.1 ~ ~
Number of patients 150 175
% moderate and severe reaction (Boston) minus % moderate and severe reaction (Tokyo) = -29.1 %. 95% confidence limits for difference: -44.2% to -13.9%.
in Japanese and American women can explain the high survival rate of the Japanese patients.
Also worthy of further study is the relationship of tumor histology to other known incidence risk factors such as age at first pregnancy and ovarian activity.
ACKNOWLEDGEMENTS
This study was supported by grants from the US National Cancer Institute (5 PO1 CA 06373 and 5 TO1 CA 05225)-and the World Health Organization. For the histologic preparations we are indebted to the pathologists in the hospitals listed in the publications describing the original studies (Salber et al,, 1969; Yuasa and MacMahon, 1970).
343

MACMAHON ET AL.
CARACTERISTIQUES HISTOLOGIQUES DU CANCER DU SElN A BOSTON ET A TOKYO
Des lames histologiques de shies reprksentatives de nialades atteintes de cancer du sein a Boston, ou le taux d’incidence de ce cancer est klevt, et ir Tokyo, ou Ie taux d’incidence est bas, ont ktk examinies par des pathologistes qui ne savaient pas de quelle ville provenait le matkriel. Les types histologiques intracanaliculaires, mkdullaires et colloides Ctaient relativement plus friquents 6 Tokyo, de mtme que les tumeurs bien dklimitkes et a fortes rkactions cellulaires. Les tumeurs a petites cellules ou les tumeurs canaliculaires invasives et les tumeurs accompagnkes d’une forte fibrose Ptaient plus frkquentes ir Boston.
REFERENCES
BERG, J. W., Inflammation and prognosis in breast cancer. A search for host resistance. Cancer, 12,
BLACK, M. M., SPEER, F. D., and OPLER, S. R., Structural representations of tumor-host relation- ships in mammary carcinoma. Biologic and prog- nostic significance. Amer. J . clin. Path., 26, 250-265 (1956).
COCHRAN, W. G., Sampling techniques, (2nd ed.), pp. 227-354, John Wiley and Sons, Inc., New York (1963).
MCDIVITT, R. W., STEWART, F. W., and BERG, J. W., Tumors of the breast, Atlas of tumor parhology, 2nd series, fascicle 2. Armed Forces Institute of Pathology, Washington, D.C. (1968).
MORRISON, A. S., LOWE, C. R., MACMAHON, B., WARRAM, J. H., JR., and YUASA, S., Survival of
714-720 (1959).
breast cancer patients related to incidence risk factors. Int. J . Cancer., 9, 470-416 (1972).
SALBER, E. J., TRICHOPOULOS, D., and MACMAHON,B., Lactation and reproductive histories of breast cancer patients in Boston, 1965-66. J . nat. Cancer Inst., 43, 1013-1024 (1969).
SHEEHE, P., Combination of log relative risk in retrospective studies of disease. Amer. J . pub/.
WYNDER, E. L., KAJITANI, T., KUNO, J., LUCAS, J. C., DEPALO, A., and FARROW, J., A comparison of survival rates between American and Japanese patients with breast cancer. Surg. Gynec. Obstet.,
YUASA, S., and MACMAHON, B., Lactation and reproductive histories of breast cancer patients in Tokyo, Japan. Bull. Wld Hlth Org., 42, 195-204 (1970).
Hlth, 56, 1745-1750 (1966).
117, 196-200 (1963).
344