Embed Size (px)
Citation preview
BRIEF COMMUNICATION
Collagenous colitis: Histologic progression, extraintestinal
features and lack of response to 5--ASA - A case report
FRANZJOSEF SCI lWEIGER, BSc, MO, FRCPC, FACG
ABSTRACT: Collagenous colitis is a clinicopathologic syndrome which presents as chronic, watery, nonbloody diarrhea. Colonic biopsies characteristically show a thick subepithelial collagen band. Barium enema and colonoscopy generally fail co establish the diagnosis. This case report provides evidence for histologic progression over time, pancolonic involvement and the presence of extraintestinal features of collagenous colitis. The reported patient showed no response to 5-aminosalicylic acid. Colonoscopic biopsies in cases of chronic diarrhea can save the patient repeated, uncomfortable and costly investigations. CanJ Gastroenterol 1990;4(1):19-22
Key Words: 5-aminosalicylic acid, Collagenous colitis, Chronic diarrhea, Extraintesnnal features
La colite du collagene: Evolution histologique progressive, manifestations extraintestinales et manque de reponse a 5-ASA
RESUME: La colite du collagene est un syndrome anatomocl inique caracterise par une diarrhee chronique aqueuse non sanglante. De maniere caracteristique, les biopsies coliques montren t une epaisse bride de collagene sous-epitheliale. l e lavement baryte et la colonoscopie ne parviennent generalement pas a etablir le diagnostic. le cas present montre une evolution histologique progressive, une atteinre pancolique et des manifestations exrraintestinales propres a la coli re du collagene. Le patient conceme n'a pas repondu a l'acide 5-aminosalicylique. Dans les cas de diarrhee chronique, le recours aux biopsies colonoscopiques peut epargner au patient des investigations repetees, desagreables et couteuses.
The Moncion Hospital , Moncion, New Brunswick Correspondence and reprints: Dr F Schweiger, I 00 Arden Street, Suite 405, Monct0n, New
Bnmswick EiC 4B7. Telephone (506)858-8441 Received f OT publication J rme 23, 1988. Accepted November 13, 1989
CAN J GASTROENTEROL VOL 4 NO 1 JANUARY/FEBRUARY 1990
THE CLINICOPATI IOLlX,IC ENTITY
of collagenous coliLis has hecome increasingly recognized since its first description l 3 year~ ago (1 ), with at least 50 cases rerortcd in the English literature.
A case of collagenous colitis is reported which nol only demonstrates the difficulty in diagnosis but also adds information with respect to mucosa] progression, rossible excraincest inal manifestations and treatment of th is condition.
CASE PRESENTATION A 71-year-old female presented with
a 16 year history of interm ittent diarrhea. The diarrhea was characterized by up to 15 loose to watery bowel movements per day, which often awakened her at night. It was preceded by bilateral lower abdominal cramps and associated with tenesmus. She denied the passage of blood but did notice mucus. These episodes occurred several times per year lasting up tO th ree to four weeks and were followed by more regular soft to loose bowel movements num-
19
SCHWEIGER
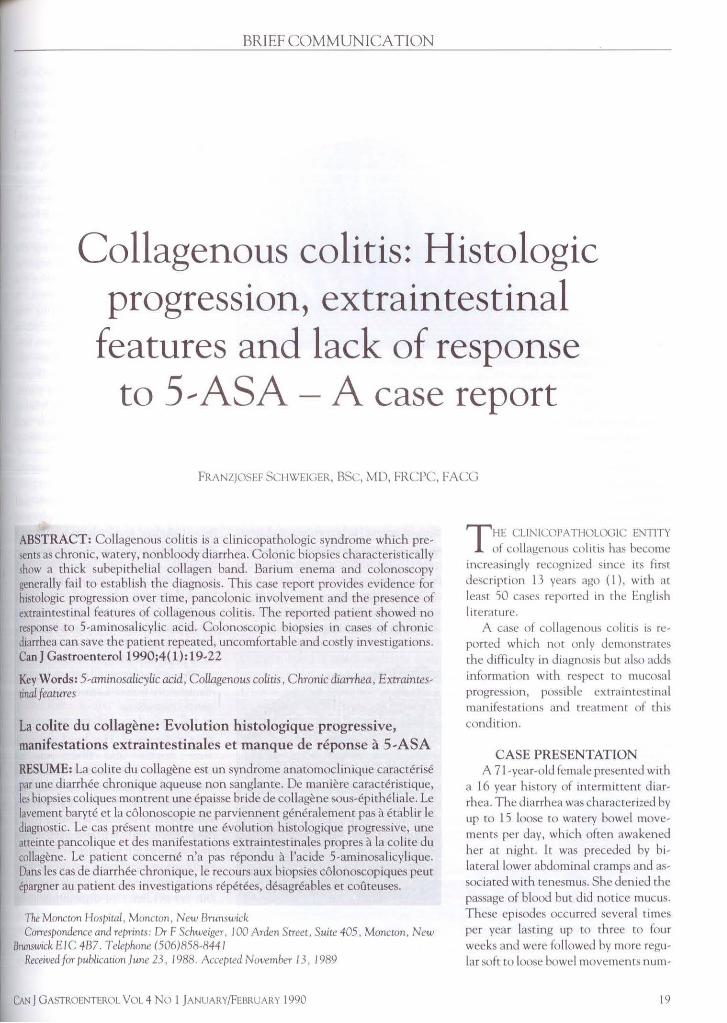
Figure 1) Rectal biopsy showing marked mononuclear inflammatory cell infiltration in che lamina propria with preservation of crypt architecture and normal goblet cells. ( Hematoxylin and eosin X 300)
bering two to three per day. Over the past year prior to admiss ion she began having more frequent bouts of diarrhea often leading to fecal incontinence. In addition , she complained of mild anorexia, nausea and severe heartburn that was relieved by H2 blocker therapy.
At age 56 she was found to have a slightly raised erythrocyte sed imentation rate, but stool cultures, sigmo idoscopy and barium x-rays of her upper and lower gastrointestina l tract were normal. An exploratory laparotomy revealed cho lelithiasis and her gallblad-
der was removed. A jejuna! biopsy was reported as normal.
At age 64 she was readmitted because of worsening diarrhea. She was found to have seronegative deforming arthritis involving the small joints of her hands and knees. Stool cultures, sigmoidoscopy, barium enema and liverspleen scan were negative and she was treated with a fibre-enriched die t and psyllium hydrophilic mucillo id .
One year later she required readmission to hospital because of persistence of her symptoms despite the admini-
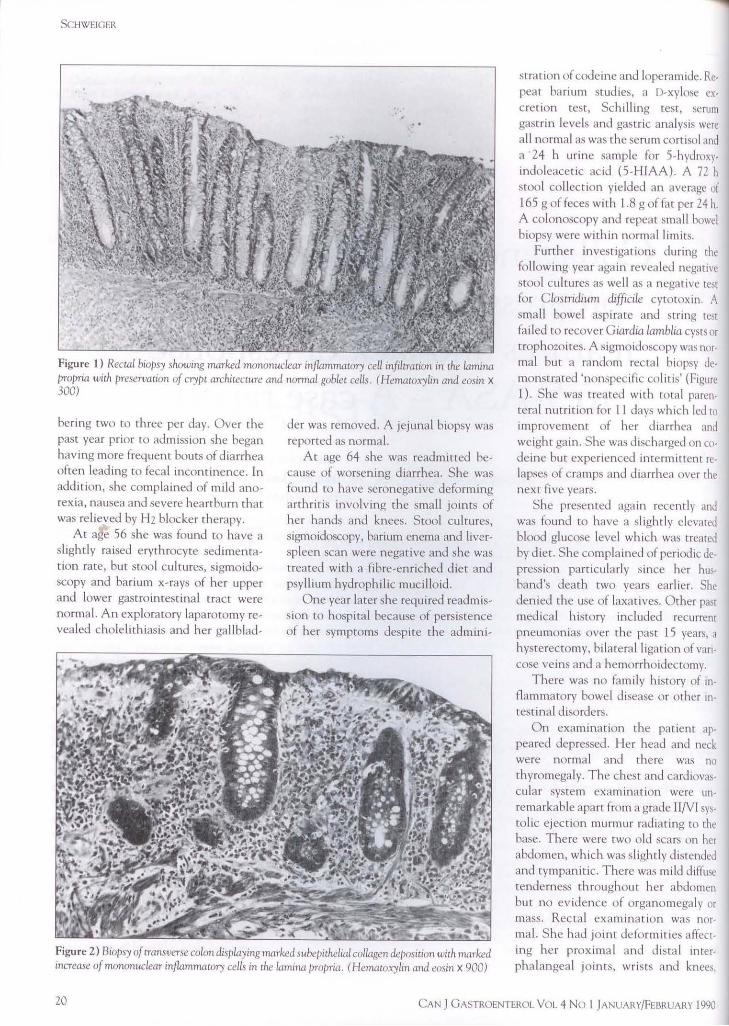
Figure 2) Biopsy of transverse colon displayinginarked subepithelial collagen de/JOsition with marked increase of mononuclear inflammatory cells in the lamina />ropria. ( Hematoxylin and eosin X 900)
stration of codeine and loperamide. Repeat ba rium studies, a D-xylose exc retion test, Schi ll ing test, serum gastrin levels and gastric analysis were a ll normal as was the scrum cortisol anJ a 24 h urine sample for 5-hydroxyindoleacetic ac id (5-HIAA). A 72 h stool collection yielded an average of 165 g of feces with l .8 g of fat per 24 h. A colonoscopy and repeat small bowel biopsy were within normal limits.
Further investigations during the following year again revealed negative stool cultures as well as a negative mt for Clostridium difficile cytotoxin. A small bowel aspirate and string test failed to recover Giardia lamblia cysts or t rophozoites. A sigmoidoscopy was normal but a random rectal biopsy demonstrated 'nonspec ific colit is' (Figure I). She was treated with total parenteral nutrition for l l Jays which led to
improvement of her diarrhea and weight ga in. She was d ischarged on codeine but experienced intermittent re· lapses of cramps and dia rrhea over the next five years.
She presented again recently anJ was found to have a slightly clcvateJ blood glucose level which was treated by diet. She compla ined of periodic depression particularly since her husband's death two years earl ier. She denied the use of laxfltives. Other past medical history included recurrent pneumonias over the past l 5 years, a hysterectomy, bi lateral ligation of varicose veins and a hemorrhoiJecromy.
There was no family h istory of inflammatory bowel disease or other intestinal disorders.
On examination the patient appeared depressed. I !er head and neck were normal and there was no thyromegaly. T he chest and cardiovascular system examination were unremarkable apart from a grade 11/Vl sy~tolic ejection murmur radiating to the base. There were two old scars on her abdomen, which was slightly distended and tympanitic. There was mi ld diffuse tenderness throughout her abdomen but no ev idence of organomegaly or mass. Rectal examina tio n was normal. S he had jo in t deformities affect· ing he r proxima l and dista l in terphalangeal joints, wrists and knee~,
20 CAN J 0ASTROENTEROL VOL 4 No I JANUARY/FEBRUARY l 990

but no acuvcly inflameJ joints were founJ. She haJ several patches of v1tiligo over her forearms.
Further investigations in hospital JcmonstrateJ a normal complete hlood count and erythrocyte scuimentation rate. Serum electrolytes, calcium anJ proteins were normal hut the fasting blood glucose and glycosylated hemoglobin were mildly clevateJ. A 72 h ,tool collection resulted in a stool wcightof225 g per 24 h and 14 g of fat per Jay while on a 100 g fa t containing diet. Stool electrolytes were potassium 99 mmol/L, sodium 61 mmol/L, chloride 68 mmol/L, with a stool osmolality of 468 mmol/L. The pH was 8 and sttX)l was negative for occult blood and reducing substances.
Upper endoscopy revealed grade ll ulcerative esophagitis and esophageal biopsy was consistent with this. Small bowel biopsy was normal. A colonoscopic examinauon was unremarkable but multiple biopsies obtained ar 10 cm intervals from cecum to rectum showed the presence of collagenous col itis in all specimens (Figure 2). The panenr was ,tarred on 5-aminosalicylic acid (5-ASA) , tlOO mg tid), a high fibre diet and psyllium mucilloid. Although she improved initially her diarrhea recurred after three weeks while on rbe medication and repeat biopsies showed no histologic improvement.
Subsequent therapy with sulfasa lazme and oral prednisone was poorly tolerated and <lid nor lead to symptomatic improvement. Currently, she is being treated with steroid enemas and she passes three m five scmiforrned bowel movements per day.
DISCUSSION Collagcnous colitis was fi rst de
scribed by Lindstr6m in 1976 (1) and has been the subject of recent reviews (2,3). This clinicoparhologic syndrome characteristically presents as a chronic watery diarrhea anJ colonic mucosa! biopsies reveal the presence of a linear subepithelial fibrous thickening and a chronic inflammaLOry infilLrate in the lamina propria. As in the patient described, radiologic and even colonoscopic findings may be entirely normal or nonspecifically abnormal and the diag-
no~,s 1s eventually m,1de only by mucosa! biopsy (2,4) .
The dbeasc appears w be most common 111 middle-aged co elderly women. The diarrhea is often intermittent, nonbkxxJy, and associated with ahdominal cramps. It is frequencly misd iagnosed as a manifestation of irritable bowel syndrome (5).1 lowever, the presence of nocturnal diarrhea, feca l incontinence and weight loss, should suggest an organic cause for diarrhea.
The patient in this case report suffered from a seronegative peripheral polyarthritis; its association with collagenous colitb has repeatedly been reported (6-8). In addition, the occurrence of glucose intolerance, Lhyroid disease and the finding of antinuclear ant1bodie::. m some patients with collagenous coli tis has been ci teJ as evidence for an autoimmune pathogenenc melharnsm (9). The presence of vitiligo has not been described previously.
The reported pat1enl in1t1ally had a rectal biopsy five years prior to the finding of a th ickened suhcpithelial collagen table 111 thesameanawm1c location. This initial biopsy revealed an active colitis consistent with the recently recognized emit)' of microscopic colitis (10). Hence, this case adds further support to the hypothesis that collagenous colitis and microscopic colitis are but Jifferent aspects of the same condition (9, 11 ,12). The pathogenesis of the fonnation of the collagen banJ 1s not completely understood, but likely requires rhe presence of chronic subepithelial inflammation ( 13 ). ln addition, the existence of a local abnonnaliry of collagen synthesis has been postulated (2).
T his case demomtrates the pancolonic distribution of collagenous col it is (3, 14) . Charactcmtica lly, jeiunal biopsie~ are normal except 111 rare cases in which celiac disease was found to be associated with collagenous or mic roscopic coli t is (12,14-17). However, there was no ev idence of small bowel villous atrophy in this pat ient and her mild steatorrhea remains unexplain ed.
The treatment response co various drugs is unpredictable and often disappo111ting ( 14). Both sulfasalazme and
CAN J GASIBOENTl:.ROL VOL 4 NO I jANUARY/FEBRL,ARY 1990
Collagenous colitis
corucnstermds have 111dl11 .. cd rembs1lm 111 ~evcral cases (2,9) but have heen ineffective in others ( 14 ). Anecdotal therapeutic success has been achieved with a number of mher compounds including mepau-inc ( 11), metro111dazole ( 18), and hbmuth subsa l1cylate ( 19). Sulfasalazine has been shown in several cases to lead not only to cl inical hut also h1smlog1c 1mprovemem seen 111 subsequent hiopsies (9,12). Wht'thcr this effect was brought ahout by the antimicrobial (su lfonamide) or ant1-1nflammatory (5-ASA) mrnety, however, is not clear. T his patient was treated with 5-ASA and Jespite a good therapeutic Jose and du rat 1011 of therapy there was no cl inical or hiswlngic response. Funhennore, su lfasalaz111e did not lead to 11nprovcment of di.irrhea. Rams ct al (2) proposed that rnllagcnous col1t b is an inflammatory disorJer, possibly of infectious origm, which 1s initia lly characterized by an acute mflammatory process which progresses over time and results 111 a gradual mcrcase llf collagen which may act as a diffusinn b.1mer, further contributing w diarrhea. Concc1vahly, neither anti-inflammatory nor ancimicmhial agents arc effective at this later stage of the disease.
Finally, th is t.ase report underlines the importance of colnnic hiopsies even in the absence of colonic find ings in patients w1tl1 unexplained chronic diarrhea. If pos1t 1ve, the diagnosis is established, and repeated, uncomfortable and costly mvcstigarions can he avoided.
ACKNOWLEDGEMENTS: The author ,1cknnwlcJgcs rhc help of Dr DA MalatJalian anJ Dr W Ying with rhc prcpamt1on of the phlltomicmgraphs.
REFERENCES I. LinJstriim CG. 'Collagenow, col1us'
with watery Jiarrhea - A new enrny? Pathol Eur 1976; 1 l:87-9.
2. Rams 11, Roger., Al, GhanJur-Mnaymneh L. Collagenous colms. Ann Intern Mc<l 1987; 106: I 08-13.
3. Covcrl1zza S, Ferr.ui A, Sccvola F, ct al. C lm1co-pacholog11.:a l features o(
collagenous colitis: C.isc report anJ literature revu:w. A m J G,1smientcml I 986;81: 1098-103.
21
SCIIWEIGER
4. Salt WB 11, Llaneza PP. Collagenous 1986;8:677-80. potentially reversible J1sorJer. J Clin col iris: A cause nf chronic diarrhea 9. Jcssurun J, Yardley Jl I, Giardicllo FM, Pacho! 1982; 35: 338-40. diagnosed only by biopsy nf n1lrmal ap- Hamilton SR, Bayless TM. Chronic 14. Kingh;:un JGC, Levison DA, Morson pearing colonic mucosa. Gastrointcst colitis with thickening of the suh- BC, Dawson AM. Collagcnou:, colitis. Endosc 1986;32:421-3. epithelial collagen layer (col lagenous Gut 1986;27:570-7.
5. G iardicllo FM, Bayless TM, Jessurun J, colitis): Hiscopathologic findings in 15 15. Hwang WS, Ke lly JK, Shaffer EA, Hamilton SR, Yardley JH. Collagenous patients. Hum Pathol 1987;18:839-48. Hershfield NB. Collagenous colitis: A colitis: Physiologic and histopathologic LO. Bo-Linn GW, Vendrell DD, Lee E, disease of pericryprnl fibmhlast sheath / studies in seven patients. Ann Intern Fordtrnn JS. An evaluation of the sig- J Pacho! L 986; 149:33-40. Med 1987;106:46-9. nificance of microscopic colitis in 16. Hamilton I, Sanders S, Hopwood D,
6. Erlendsson J, Fenger C, Meinicke J. patients with chronic diarrhea. J Clin Bouchier !AD. Collagenous col itis as-Arthritis and collagcnous colitis: Report Invest 1985;75:1559-69. soc iated with small intestinal villous of a case wirh concomitant chronic 11. Teglbjaerg PS, Thaysen EH, Jensen atrophy. Gut 1986;27: 1394-8. polyanhritis and collagenous colitis. I {H. Development of collagenous 17. Breen EG, Coughlan G, Connolly CE, Scand J Rheumatol 1983; 12:93-5. colitis in sequential biopsy specimens. Stevens FM, McCarthy CF. Coeliac
7. Farah DA, Mills PR, Lee FD, Mclay Gastroencerology l 984;87:703-9. proctitis. Scam! J Gastroenterol A, Russell RI. Collagennus colitis: Po~- 12. Sylwestrowicz T, Kelly JK, Hwang WS, 1987;22:47 l • 7. sible response to sulfasalazme and local Shaffer EA. Collagenous colitis and 18. Mogensen AM, Olsen JI l, GuJmand-steroid therapy. Gastrucnterology microscopic colitis: The watery diar- Hoyer E. Collagenous colitis. Acrn 1985;88:792-7. rhea-colitis syndrome. Am J Med Scand I 984;216:535-40.
8. Wiener MO. Collagenous colitis and Gastroenterol 1989;84: 763-8. 19. Girard DE, Keeffc EB. Therapy for col-pulmonary fibrosi,. Manifestations of a 13. Pieterse AS, Hecker R, Rowland R. lagenous colirb. Ann Intern Med single disea~c?J Clin Gastroenrerol Collagenous colitis: A distinctive and 1987;106:909.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com





























