Embed Size (px)
Citation preview

HIMSS Patient-Centered Payer Roundtable
October 10, 2012

2009 HIMSS Washington Office Pumpkin Decorating Contest Submission
2

Agenda Welcome Call to Order and Roll Call (David Fitzgerald, Shelley Price) 2-Minute Drills Healthcare M&A Activity Integrated Health Association Multi-Payer P4P Innovation Colorado Multi-Payer PCMH Pilot Topic discussion IHE (Integrating the Healthcare Enterprise): A solution for Payer- Provider Interoperability? An Introduction to the “Plumbing” (Mike Nusbaum, President MH Nusbaum & Associates Ltd.) Housekeeping (Shelley Price) Adjournment
3
Agenda Welcome Call to Order and Roll Call (David Fitzgerald, Shelley Price) 2-Minute Drills Healthcare M&A Activity Integrated Health Association Multi-Payer P4P Innovation Colorado Multi-Payer PCMH Pilot Topic discussion IHE (Integrating the Healthcare Enterprise): A solution for Payer- Provider Interoperability? An Introduction to the “Plumbing” (Mike Nusbaum, President MH Nusbaum & Associates Ltd.) Housekeeping (Shelley Price) Adjournment
4

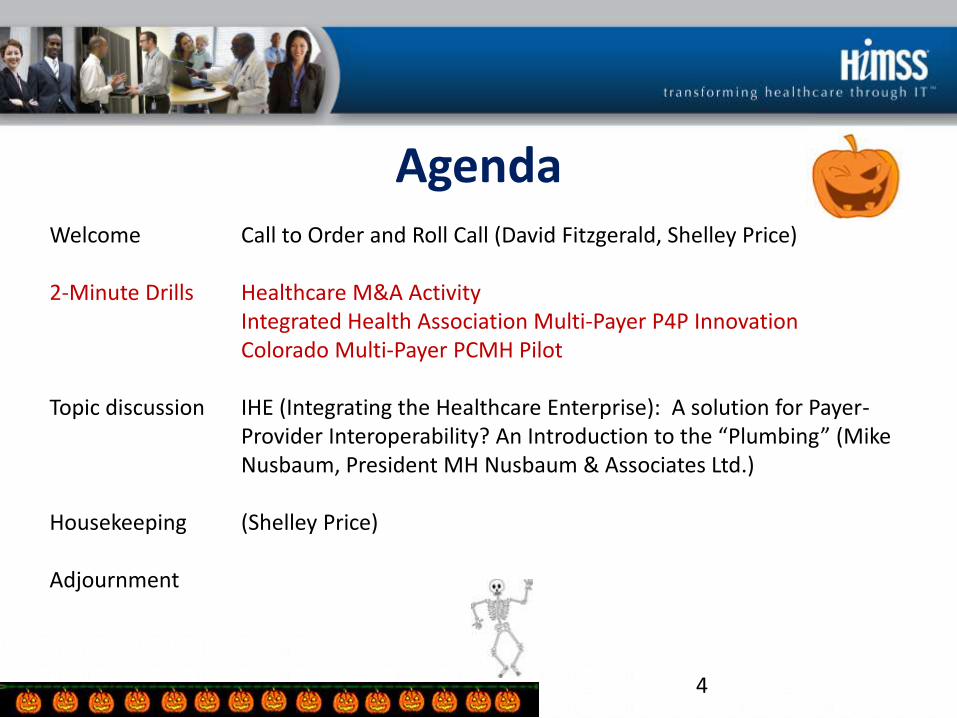
2 Minute Drill: Healthcare M&A Activity
5
• Healthcare investment is accelerating – Darn, another bubble missed
• Capital is so inexpensive, that acquisitions are often worth the SWAG to see if you get the right one – What the heck, buy 2, get 1 free!
• You can’t ACO without pervasive analytics – This may kill those IDNs without capital access, strong IT capabilities, or
comprehending leadership
– $500m year 1 HealthIT spend projection ($1m+ small / $4m+ large)
– Increasing sense of urgency; a VERY difficult train to catch once it leaves the station in your market

EMR Market Concentration Continues • Too many EMRs for the
market to sustain (600+)
• MU2 compliance will hurt a lot of them; MU3 compliance will be the death sentence for many, if not most
• Many hanging on just for the acquisition opportunity

M&A’s Keep Piling Up
• Lumpy’s bet – 2013 is the year of massive
EMR company M&A, failures and closures
• Good Read – http://www.theatlantic.com/
health/archive/2012/06/is-one-company-about-to-lock-up-the-electronic-medical-records-market/258473/
And coming soon to a theater near you….

Analytics Consolidation Seems Underway
• All the big boys staking their claim with an analytics solution that they use AND sell
• ACOs are going to drive “significant” analytics needs and purchases
• Tell your kid to give up on their sports management and get to studying biostatistics, actuarial, or pop health
And Then There’s…
• UPMC, Oracle, IBM, Informatica, dbMotion consortium
– 5yr, $100M investment
• Aetna, GNS Healthcare
– 35m lives available
• IBM Watson Project
– Beat Jeopardy; how hard is healthcare?
• Population Health
• Genomics
• Personalized Medicine
• Going to be some BIG winners and a heck of a lot of losers.
• Choose wisely, contract smartly, have a backup plan

Next Growth Wave?
• TeleHealth?
• Remote Monitoring?
• Genomic testing/counseling?
• Hospital consolidation and closure services?

Kim Harding
Florida Blue
Source: “2012 California Pay for Performance Program Updates.” Integrated Healthcare Association. February 2012.
*

*
*Core Competency: Standardization of health plan efficiency measures and payment methodologies
*A key collaborator with NCQA in identifying performance-based measures for incentive strategies
*Founded in 2001, the
California P4P program
is the oldest and
largest non-
governmental
physician incentive
program in the United
States

*
*Aetna
*Anthem Blue Cross
*Blue Shield of CA
*CIGNA
*Health Net
*Kaiser Permanente
*United Healthcare
*Western Health Advantage
*This represents approximately 10 million HMO/POS insured persons
* IHA is responsible for collecting data, deploying a common measure set, and reporting results for approximately 35,000 physicians in 221 physician groups

*Offer incentives to POs to eliminate waste and unnecessary utilization and deliver high quality care
* Savings generated contribute to lower cost trends and more competitive, value-based HMO product
* Available to all Providers, including full risk Providers; all health plans and Providers are encouraged to participate
* Providers that contribute to HMO price competitiveness and demonstrate quality should be rewarded
* Value Based P4P should not increase a health plan’s total cost trend
*Exclude the following data points:
*Mental health, chemical dependency, dental, vision, chiropractic, acupuncture
*P4P quality incentive payments
*Costs above $100K per member per Provider truncated
*

*
*Cardiovascular
*Diabetes
*Maternity
*Musculoskeletal
*Prevention
*Respiratory
*Prevention and Risk
Factors
*Care Processes
*Appropriateness of Care
*Utilization
*Cost and Efficiency
*Patient Experience
*Outcomes

*
Goal of Total Cost of Care Measures
* Total amount paid to any provider (including facilities) to care for all members of a Physician Organization (PO) for a year
* Risk adjusted for age, gender, and health status
* Geographic pricing differences accounted for
* PO results for each contracted health plan, and aggregated across all contracted health plans
Challenges of Implementation
* Assigning conclusive accountability for hospital costs
* Setting appropriate trend targets
* Implementation of a Quality composite score
* Integrating appropriate resource use for shared savings and utilization metrics
* Creating a cost neutral design

2 Minute Drill: Colorado Multi-Payer PCMH Pilot
• Many payer/provider initiatives to transform delivery system underway, multi-payer programs probably most important for true delivery system transformation
• “Colorado Patient-Centered Medical Home Pilot Met Numerous Obstacles, Yet Saw Results Such As Reduced Hospital Admissions” Marjie G. Harbrecht & Lisa M. Latts (Health Affairs, September 2012 31:9, pages 2010-2017)
• Pilot phase (May 2009-April 2012) involved six insurers, sixteen FP/IM practices, 100,000 patients – United HealthCare, Anthem/Wellpoint, Aetna, Cigna, Humana, Cover Colorado
(state’s high risk pool carrier)
– Most physician practices were small, independent (more typical for state)

Data Elements
• All participating plans agreed in principle to provide practices with data on patient use of services and identify patients in need of care management
• Practices believed data was critical to their ability to contain costs
• Most plans unable to follow through – Some plans not convinced practices needed granular data
– Others unable to follow through • Inconsistent formats
• Covered different intervals
• Lack of common definitions
• Limited actual cost data
– Practices needed to devote scarce resources to reviewing multiple web-sites
– Some practices interpreted lack of follow through as lack of plan commitment to program
• Some practices also struggled to extract data from their EHRs – “Meaningful Use” requirement challenges
– Registry functions not as robust as needed
Subsequent Blog Post & Informal Survey Of Health Plan Medical Directors— “What Might Have Been
Responsible For Health Plan Data Challenges?”
• Failure to agree on sufficiently detailed standards
• Limited resources in plan IT departments vs. multiple needed (e.g. ICD-10)
• Lack of CMS involvement
• Lack of central “data aggregator”
• Competitive issues
Agenda Welcome Call to Order and Roll Call (David Fitzgerald, Shelley Price) 2-Minute Drills Healthcare M&A Activity Integrated Health Association Multi-Payer P4P Innovation Colorado Multi-Payer PCMH Pilot Topic discussion IHE (Integrating the Healthcare Enterprise): A solution for Payer- Provider Interoperability? An Introduction to the “Plumbing” (Mike Nusbaum, President MH Nusbaum & Associates Ltd.) Housekeeping (Shelley Price) Adjournment
21

IHE (Integrating the Healthcare Enterprise):
A solution for Payer-Provider Interoperability? An Introduction to the “Plumbing”
Mike Nusbaum, BASc, MHSA, FHIMSS President
MH Nusbaum & Associates Ltd.
Today’s Agenda…
• Introduce IHE, it’s products & processes
• How can IHE serve the Payer community?
• Opportunities…
• Q&A
23

The Case for Standards
24

Why do we need IHE?
• IHE Profiles address real-world problems • IHE Profiles make standards
implementable • Compliance to IHE Profiles maximizes
opportunity for plug-compatible interoperability
• IHE can accelerate adoption and implementation of standards
• The IHE Process ensures rigor and robustness: • reliance on established standards • extensive engagement with stakeholders, incl.
public comment • profile maintenance • conformance testing in a real-world environment • attestation (not yet certification)
25 25

Base Standards eHealth Projects
Interoperability:
Highest Cause of Health IT project failures
IHTSDO
IETF
26

Profile
Development
Base Standards eHealth Projects
From a problem to a solution
Profiling Organizations Have
Emerged
IHTSDO
IETF
Specific Extensions
27
Standards:
Necessary… but not sufficient Standards are
• Foundational - to interoperability and communications
• Broad - varying interpretations and implementations
• Narrow - may not consider relationships between standards domains
• Plentiful - often redundant or disjointed
• Focused - standards implementation guides focus only on a single standard
IHE provides a standard process for
implementing multiple standards 28

Connecting Standards to Care
• Healthcare professionals work with industry
• Coordinate implementation of standards to meet clinical and administrative needs
• Clinicians and HIT professionals identify the key interoperability problems they face
• Providers and industry work together to develop and make available standards-based solutions
• Implementers follow common guidelines in purchasing and integrating effective systems
IHE: A forum for agreeing on how to implement
standards and processes for making it happen 29

IHE:
A Framework for Interoperability
• A common technical framework for harmonizing and implementing multiple standards • Application-to-application • System-to-system • Setting-to-setting
• Enables seamless health information movement within and between enterprises, regions, nations
• Promotes unbiased selection and coordinated use of established healthcare and IT standards to address specific clinical needs
30

Is IHE a novel idea?
Has IHE been adopted?
31
• What are the alternatives ?
• Ignore the issue
• Pick key standards, and hope for the best
• Rely on robust standards harmonization
• ISO Health Informatics: TR28380 Global Standards Adoption – IHE Process, Profiles and Implementation
• Widespread adoption of IHE Profiles by National and Regional Projects around the world: USA, Canada, Europe, Asia
• Home Health: CONTINUA and IHE work together.
• 12 Country European epSOS Project (IHE-Europe hosting Industry Team).
31

32 32
IHE International Organizational Structure
Contributing & Participating
Vendors
Example Deployment Committees
IHE Europe
IHE North America
France
USA
Canada
IHE Asia-Oceania
Japan
Korea Australia
Netherlands
Spain Sweden UK Italy
Germany
Norway
China
Austria
Professional Societies / Sponsors
IHE International Board
Global Development Domains
Radiology
Cardiology
IT
Infrastructure
Patient Care
Coordination
Patient Care
Devices
Laboratory
Pathology
Eye Care Radiation
Oncology
Public Health, Quality
and Research
Pharmacy
Endoscopy Dentistry
32 32

33
15 Years of Steady Evolution 1998 – 2012
The IHE Development Domains
Pathology since 2006
Radiation Oncology since 2004
Radiology since 1998
Cardiology since 2004
Patient Care Devices since 2005
Patient Care Coordination since 2004
Eye Care since 2006
Quality Research & Public Health
since 2006
Laboratory since 2004
(Healthcare) IT Infrastructure
since 2003
Endoscopy since 2010
Dentistry since 2010
Pharmacy since 2009
33

34
France
Local Deployment
National Extensions
Promotional & Live Demonstration Events
Funding
USA
Germany
Italy
Japan UK
Canada
Korea
Taiwan
Norway
Netherlands
Spain China
Austria
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
09
Pragmatic global standards harmonization + best practices sharing
20
08
Australia International Participation in IHE
34

IHE Sponsors
Professional societies: Healthcare Information Management Systems Society (HIMSS)
American College of Physicians (ACP),
American College of Emergency Physicians (ACEP)
American College of Obstetricians and Gynecologists (ACOG)
Many other American Professional Societies (ACCE), (AAO), (ASTRO), etc.
British Institute of Radiology (BIR), British Computer Society (BCS)
German Radiology Society (DRG) …ASIP (IT France), SFIL (laboratory), French National Project (DMP), European Society of Cardiology
Radiological Society of North America (RSNA)
JAHIS (IT Japan), JIRA, JRS,…
And many more
Government Agencies: French National Project (ASIP-Santé)
Dutch National Project (NICTIZ)
Austrian National Project (ELGA)
Canada Health Infoway (CHI)
Regional projects (Italy, USA, Japan) and many more…..
35

Document Use Case Requirements
Identify available standards (e.g. HL7, DICOM,
IETF, OASIS)
Develop technical specifications
Testing at Connectathons
Timely access to information
Easy to integrate products
RFPs with IHE reqts
IHE Standards Adoption Process
36
IHE Demonstrations

What is a Connectathon?
• Cross-vendor, live, supervised, structured testing event
• All participating vendors’ products tested together in the same place/time
• Experts from each vendor available for immediate problem resolution… fixes are done in minutes, not months!!
• Each vendor tests with multiple trading partners (actual product to actual product)
• Testing of real-world clinical scenarios using IHE Integration Profiles
37

IHE Product Registry
• A website to search IHE Integration Statements published by vendors
• Helps users find products that match their needs
• Product Registry maintains a database of actors/profiles in vendors’ integration statements
• Product Registry points to Integration Statement on vendor’s web site
38

39
Registering
IHE Integration Statements

Product Registry Usage
40
• Approximately 410 Integration Statements in the database
• Over 100 companies registered
• Average 280 visits per month
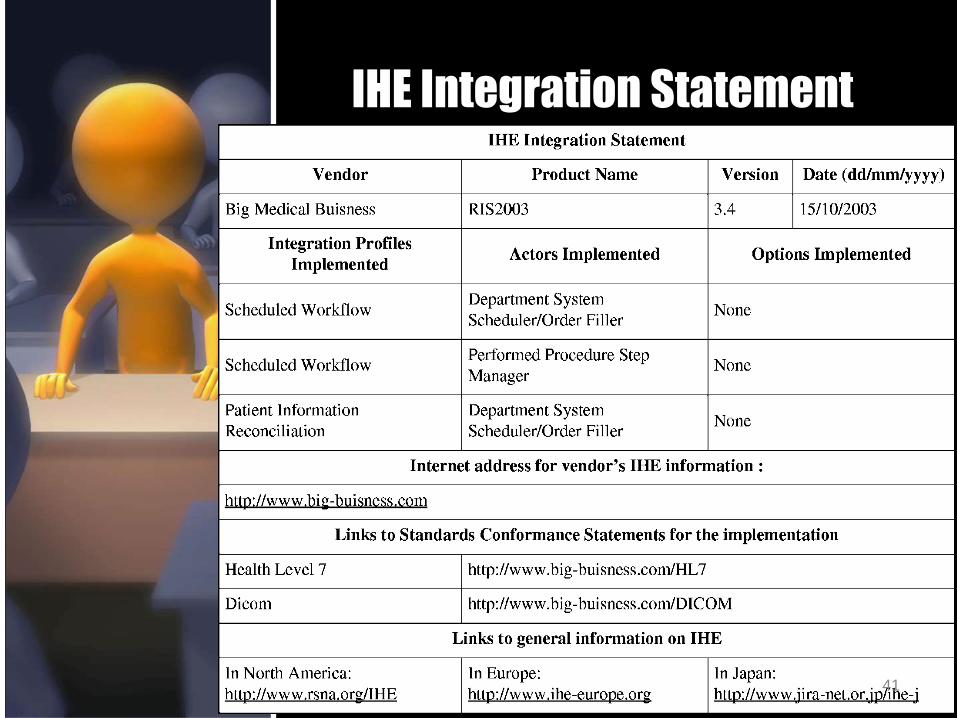
IHE Integration Statement
41

Product Registry Links
42
• IHE Integration Statement template http://tinyurl.com/62ymvtc
• Link to Product Registry : http://product-registry.ihe.net
• Documentation : http://gazelle.ihe.net/content/product-registry
• Support http://gazelle.ihe.net/jira/PR

HIMSS Interoperability Showcase
43

Where in the World is XDS and CDA
Link
44

Of interest to payers…
• XD* family of IT infrastructure profiles
• XDS, XDR, XDM, XDS-SD
• XCA
• Content profiles that leverage the XD* family
• XDS-MS, XD-LAB, XDS-I
• CDA (C-CDA) harmonized templates that carry clinical data exchanged amongst healthcare stakeholders
45

Opportunities
• Is there an interest in setting up a domain to address payer needs?
• International or US-realm?
• Implications
• Approach
• Next steps
46

Thank you!!! Questions?
Find out more at ihe.net 47

Agenda Welcome Call to Order and Roll Call (David Fitzgerald, Shelley Price) 2-Minute Drills Healthcare M&A Activity Integrated Health Association Multi-Payer P4P Innovation Colorado Multi-Payer PCMH Pilot Topic discussion IHE (Integrating the Healthcare Enterprise): A solution for Payer- Provider Interoperability? An Introduction to the “Plumbing” (Mike Nusbaum, President MH Nusbaum & Associates Ltd.) Housekeeping (Shelley Price) Adjournment
48
Housekeeping • We want to hear from you!
• Roundtable member survey coming soon
• What do you see are Key Areas? Trends? Coming down the pipeline?
• Ideas for speakers and topics
• 2-minute drills – want to present one?
• Get involved
• Join the Speakers Team. Join the Communications Team. Write for the HIMSS Payer Insider.
• HIMSS.org 2.0
49
Housekeeping
• 2012 mHealth Summit -- Connecting the Mobile Health Ecosystem
– When: December 3-5, 2012
– Where: Washington, DC.
– Focus: “The 2012 mHealth Summit will deliver new sponsors, partners and strategic
affiliates; expanded exhibit hall showcasing more than 400 exhibitors; new healthcare delivery track; new global health track; mHIMSS Hospital Mobile Survey results; and keynotes from industry luminaries. Overall, the 2012 mHealth Summit will offer attendees a comprehensive representation of the mobile technologies in healthcare looking at implementation and impact of its benefits and new opportunities. “
– Info at: http://www.mhealthsummit.org/
50

• Resources:
– HIMSS Calendar of Events:
– http://www.himss.org/ASP/confCalendarHome.asp
– Webinars and Audio Conferences
– http://www.himss.org/ASP/confCalendarHome.asp?cetid=200
51
Wrap-up

Wrap-up • Web page
– Payer Topics and Tools page!
– http://www.himss.org/ASP/topics_payers_healthplans.asp
– .
– http://www.healthcarepayernews.com/himss-payer-insider
• Next meeting
– 3rd Thursday of the month from 4-5pm EST
• Thursday, November 15, 2012
52

FY13 Leadership and Contact Information Chairperson: David Fitzgerald Enterprise Systems Architect Manager Aetna [email protected] Vice Chairperson: Gary Austin Principal & Co-Founder, TranzformHealth [email protected] HIMSS Staff Liaison: Shelley Price Nancy Devlin Director, Payer and Life Sciences Sr Assoc., Payer and Life Sciences HIMSS HIMSS [email protected] [email protected] 53