Embed Size (px)
Citation preview
ORIGINAL ARTICLE
High Prevalence of Coxa Vara in Patients With SevereOsteogenesis Imperfecta
Mehdi Aarabi, MD, Frank Rauch, MD, Reggie C. Hamdy, MD, and Francxois Fassier, MD, FRCSC
Abstract: The purpose of this study was to determine the incidence
and clinical presentation of coxa vara in 283 patients with osteo-
genesis imperfecta (OI). The charts and x-rays of 150 girls and
133 boys with OI were reviewed. The patients were classified accord-
ing to the Sillence classification modified by Glorieux: 94 type I,
90 type IV, 67 type III, 18 type V, 10 type VI, and 4 type VII. The
mean age was 9.4 years (range 0.3–23.3). Twenty-nine patients
(10.2%) had coxa vara (23 left and 20 right). Fifty-five percent of
them were type III, 24% type IV, 13.8% type VI, and 3.4% each of
types Vand VII. The incidence of coxa vara was 6% in type V, 8% in
type IV, 24% in type III, 25% in type VII, and 40% in type VI (P ,
0.001 for difference between types I, III, and IV). The mean neck–
shaft angle was 99 degrees (range 80–110 degrees), the average head–
shaft angle was 104 degrees (range 90–120 degrees), and the mean
Hilgenreiner–epiphyseal angle was 68 degrees (range 40–90 degrees).
Twenty-five patients (36 hips) had previous femoral rodding before
diagnosis and seven hips (all type III) had no history of rodding.
Abduction and internal rotation of the hip joints were restricted in all
patients with this deformity. All children with coxa vara had a
Trendelenburg gait. In conclusion, coxa vara in OI is not rare, espe-
cially in severe forms of the disease. Regular clinical and radiologic
follow-up is indicated in children with previous femoral rodding and in
severely affected children, particularly those with OI type III.
Key Words: coxa vara, osteogenesis imperfecta
(J Pediatr Orthop 2006;26:24–28)
Osteogenesis imperfecta (OI) is a genetic disorder thatcauses increased bone fragility and low bone mass. The
most commonly used classification distinguishes four clinicaltypes.1 Patients with OI type I have a mild phenotype withnormal or near-normal height and typically blue sclera. Type IIis lethal in the perinatal period. Type III is the most severe formin children surviving the neonatal period. These patients haveextremely short stature, with limb and spinal deformities sec-ondary to multiple fractures. Patients with mild to moderatebone deformities and variable short stature are classified as OI
type IV. In most cases, the disease can be linked to the presenceof mutations in one of the two genes that code for collagentype I.2 This traditional classification comprising four OI typeshas recently been expanded by the addition of OI types V toVII.3–5 These newly characterized OI types can be distin-guished from the other forms of the disease on the basis ofclinical appearance, bone histology findings, and the lack ofcollagen type I mutations.6–8 The hallmark of all forms of OI isbone fragility. The incidence of fractures can be high, es-pecially in the lower extremities, often leading to bowing offemoral and tibial diaphyses. Acetabular protrusion is alsocommon, affecting the majority of OI type III patients.9 A lesswell recognized feature of OI is coxa vara (CV), which in ourexperience is not rare in the more severely affected patients.CV has been defined as any decrease in the femoral neck–shaftangle to below 110 degrees (Fig. 1).6,10 The femoral neck–shaft normally is about 150 degrees at birth, 126 degrees inadults, and 120 degrees in the elderly.7,11 At present, there islittle information about the morbidity that CV may cause in OIpatients. The aim of this report was to evaluate CV in a largepopulation of children with OI and its associated clinicalfeatures.
METHODSThis was a retrospective evaluation of all children with
OI examined at the Shriners Hospital for Children in Montrealbetween October 1999 and October 2003. The diagnosis of OIwas based on clinical findings, as described by Sillence et al.1
All patients in whom anteroposterior radiographs of at leastone hip had been performed were included in the study, and thelast available x-ray was assessed for the present study. A totalof 283 patients fulfilled these criteria (150 girls, 133 boys).The patients were classified according to the Sillence clas-sification, as expanded by Glorieux.2 The diagnostic distribu-tion of the patients is shown in Table 1. Mean age at the time ofanalysis was 9.4 (range 0.3–23.3) years. One hundred seventy-eight patients had received medical therapy with intravenouspamidronate before the radiographic study.2 In 273 patientsradiographs from both hips were available. In 10 patients onlyone side had undergone radiographic examination. Thus,a total of 556 hips could be assessed.
Radiologic MeasurementsFigure 1 is an example of coxa vara in OI patients. All
measurements were performed on standard anteroposteriorradiographs of the hip (Figs. 2 and 3). The femoral neck–shaftangle was measured as the intersection of a line drawn through
From Shriners Hospital for Children, Division of Orthopaedics, McGillUniversity, Montreal, Quebec, Canada.
Study conducted at Shriners Hospital for Children, Montreal, Canada.None of the authors received financial support for the study.Reprints: Francxois Fassier, MD, FRCSC, Chief of Staff, Shriners Hospital
for Children, 1529 Cedar Avenue, Montreal, Quebec, Canada H3G 1A6(e-mail: [email protected]).
Copyright � 2006 by Lippincott Williams & Wilkins
24 J Pediatr Orthop � Volume 26, Number 1, January/February 2006
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

the shaft of the femur with another line passing through thelong axis of the femoral neck. The Hilgenreiner–epiphysealangle was determined according to Beals’ modification of themethod originally described by Weinstein et al.6,12 The normalvalue of the Hilgenreiner–epiphyseal angle is 16 degrees
(range 0–25 degrees).6 We also measured the head–shaftangle, the angle between the longitudinal axis of the femoralshaft and a line perpendicular to the largest diameter of thefemoral head.6 The lateral radiographs were also assessed inthe patients with CV to evaluate femoral bowing and toidentify false CV (Fig. 4). The ratio between tibia and femurlength was evaluated in patients with CV in whom anteropos-terior radiographs of the entire extremity (femurs and tibias onthe same film) were available (n = 29). Results were comparedwith reference data published by Robinow.13
Statistical AnalysisThe statistical difference of the CV between the femurs
that had been previously rodded and the femurs with no rod-ding procedure was evaluated by the chi-square test.
RESULTSCV was present in 29 of the 283 OI patients (10.2%).
The highest prevalence of CV was found in OI types III, VI,and VII, whereas no case was found among the 94 patientswith OI type I (see Table 1). Fifteen patients with CV hadunilateral involvement, and in 14 patients both hips wereaffected. Thus, 43 of the 556 evaluated hips (7.7%) wereaffected with CV (23 left and 20 right hips). In addition, fourcases of false coxa vara were identified; these were associatedwith anterolateral angulation in the proximal third of thefemur. On the other hand, 28 femurs had bowing in theproximal third without either false or true coxa vara. In 41 ofthe 43 cases of true CV, the deformity was located in the baseor in the middle of the femoral neck. The trochanteric regionwas affected in the remaining two hips. The neck–shaft angleof the affected hips averaged 99 degrees (range 80–110 degrees)and the mean Hilgenreiner–epiphyseal angle was 68 degrees(range 40–90 degrees). The head–shaft angle averaged104 degrees (range 78–120 degrees). Intramedullary roddinghad been performed in 25 of the 29 patients (83%) and in36 of the 43 femurs (84%) with CV. Thus, only four patients(all OI type III) with seven affected femora had no rod-ding procedures. In contrast, intramedullary rodding hadbeen performed in only 140 of 513 femurs (27%) that werenot affected by CV (P = 0.007 for the difference in prevalenceof rods between femurs with and without CV). The tibia-to-femur length ratio was above the reference range in 24 of the29 lower limbs with CV (83%) that could be evaluated.Intramedullary rodding procedures had previously beenperformed in 21 of these 24 femurs.
In 21 patients with 33 affected hips, we could retrieveinformation on the functional clinical status at the time pointconsidered in the present study. In 24 hips (72%), flexionand external rotation were full. In 31 hips (93%), more than90 degrees of flexion was possible. Eleven hips (33%) had noextension, and 15 hips (45%) had varying degrees of flexioncontracture. Twenty-one hips (63%) had normal external ro-tation, and in 7 hips (21%) the range of external rotation wasabove normal. The average abduction in the 33 hips was21 degrees. In 10 hips (30%), abduction was less than10 degrees. In 9 hips (27%) it was between 11 and 20 degrees,in 11 hips (33%) between 20 and 30 degrees, and in 2 hips
FIGURE 1. Anteroposterior x-ray of hip and femur in a childwith OI showing true CV. The child also had an elongating nailfor correction of femoral bowing. Multiple growth-arrest linesare seen in the distal femur.
q 2006 Lippincott Williams & Wilkins 25
J Pediatr Orthop � Volume 26, Number 1, January/February 2006 Coxa Vara in Osteogenesis Imperfecta
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

(6%) more than 30 degrees. In 17 hips (51%) internal rotationwas absent or very limited. Six hips (18%) had 5 to 10 degreesof internal rotation, 2 hips (6%) 15 degrees, and one hip (3%)more than 15 degrees. Seven hips (21%) had varying degreesof external rotation contracture. Most patients with CV hada Trendelenburg gait.
DISCUSSIONIn the present study we observed a high prevalence of
CV in patients with severe forms of OI but an absence of thisdeformity in patients with OI type I. Thus, CV clearly wasassociated with the severity of bone fragility in OI. Assessmentof CV in severe OI is not always simple, as the radiologicpicture is often complicated by bowing of the femoral dia-physis. As previously described by the senior author (F.F.),14
a curvature in the proximal third of the femoral shaft candecrease the distance between the femoral head and shaft,mimicking the pattern of CV on anteroposterior radiographs,even if the neck–shaft angle is normal. In the present study weavoided this pitfall by also evaluating lateral radiographs of thefemur. If CV is suspected in the presence of anterior bowing ofthe proximal third of the femur, a radiograph of the hip inextension should be obtained. In this manner false CV can beidentified (see Fig. 4).
The pathogenesis of CV in OI is unclear. Generallyspeaking, CV in children could be classified as developmental,congenital, dysplastic, or traumatic.12 Many of these factorsmay have contributed to the development of CV in our patients.In developmental CV, there is an intrinsic defect in cartilagematuration and bone formation involving the proximal femoralphysis and femoral neck.12 Its pathognomonic radiologic signis a triangular metaphyseal fragment in the medial side of thefemoral neck.6,15 Such fragments were seen in both hips of oneof our patients with OI type III. In dysplastic CV, the deformityusually affects the trochanteric area; this was found in two ofour patients.12,16 However, the large majority of our patientshad CV secondary to deformity in the base of the femoralneck. It appears plausible that many of these cases could beclassified as traumatic CV and may have been caused bymalunion of a fracture or repeated subclinical fractures of thefemoral neck. The majority of patients with CV had undergonefemoral rodding procedures. It is possible that the bio-mechanical effects of femoral rods contributed to the
TABLE 1. Diagnostic Distribution of the Study Population and Results of Radiologic Evaluation
OIType
No. ofPts. Examined
No. of Patients With CV(% of all patients with same type)
No. of HipsExamined
No. of Hips With CV(% of hips of patients with same type)
I 94 0 (0%) 185 0 (0%)
III 67 16 (24%) 131 26 (20%)
IV 90 7 (8%) 178 8 (4%)
V 18 1 (6%) 36 1 (3%)
VI 10 4 (40%) 18 6 (33%)
VII 4 1 (25%) 8 2 (25%)
Total 283 29 556 43
FIGURE 2. A, Anteroposterior x-ray of the pelvis and both hips ina child with type III OI showing severe CV with decreased femoralneck–shaft angle. B, Drawing of the femoral neck–shaft angle.
26 q 2006 Lippincott Williams & Wilkins
Aarabi et al J Pediatr Orthop � Volume 26, Number 1, January/February 2006
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
development of CV. However, the statistical associationbetween femoral rodding and CV does not necessarily provea causal link. Our observation may simply reflect the fact thatthe more severely affected OI patients are more prone todevelop CV and at the same time are more likely to requirerodding. Nevertheless, it may be prudent to closely evaluatesuch patients for the development of CV. Although CV isusually defined on the basis of the femoral neck–shaftangle,10,17 Weinstein et al suggested measuring the head–shaftangle to evaluate the varus angulation of the femoral neck.6
According to these authors, the head–shaft angle is morereproducible than the neck–shaft angle and more indicative ofthe actual deformity. We found that the mean neck–shaft anglewas lower than the head–shaft angle in our patients, probablybecause there was no defect in the femoral neck in CVand the
location of the deformity was mostly around the base of thefemoral neck. The addition of the head–shaft angle to the listof measured indices therefore did not provide much clinicallyuseful information.
As CV has been described in association withrhizomelia (shortness of the upper leg relative to the lowerleg) in some cases of OI,5 we assessed our CV cases forrhizomelia as well. In 24 lower limb x-rays that we reviewed,we found rhizomelia in all of them. Because more than 85% ofthe femurs (21/24) had already been corrected surgically androdded, and most femurs are osteotomized, this could be aninterpretation for this finding. We indeed found short femurs ina considerable proportion of cases. However, the large ma-jority of these femurs had undergone intramedullary roddingto correct bowing deformity. It therefore appears most likely
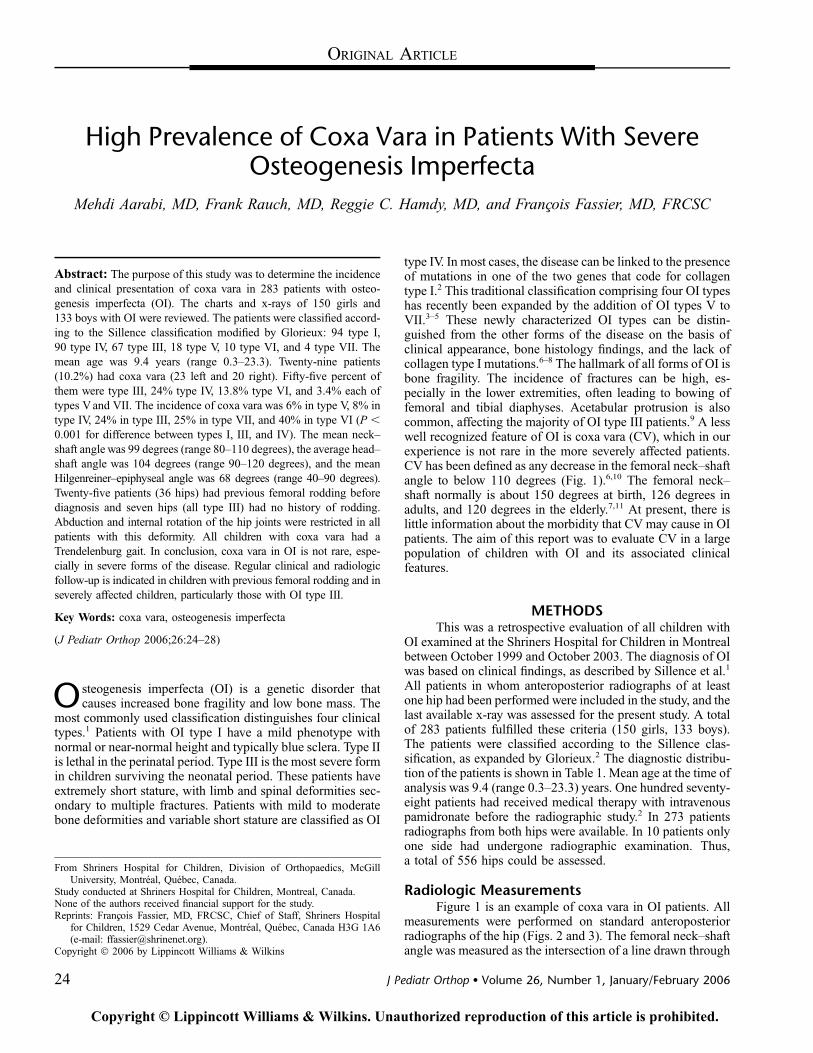
FIGURE 3. A, Anteroposterior x-ray ofthe pelvis and both hips in a child withtype III OI showing severe CV withincreased Hilgenreiner–epiphyseal an-gle. B, Drawing of the Hilgenreiner–epiphyseal angle.
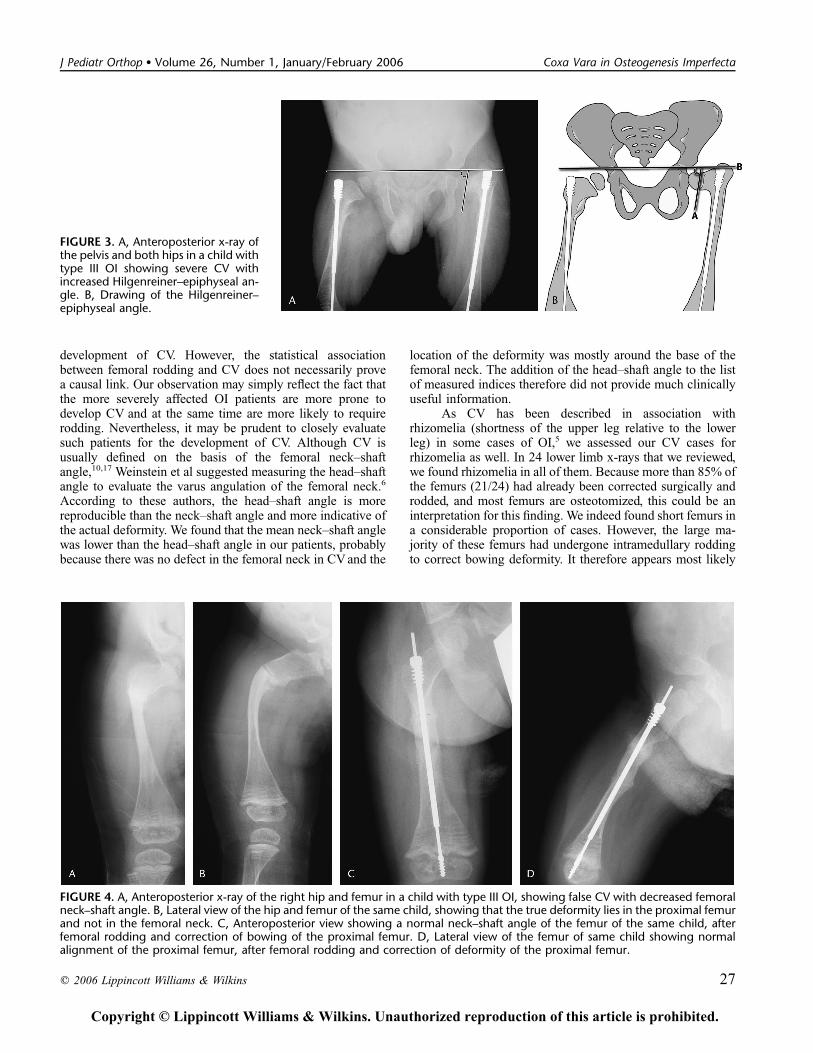
FIGURE 4. A, Anteroposterior x-ray of the right hip and femur in a child with type III OI, showing false CV with decreased femoralneck–shaft angle. B, Lateral view of the hip and femur of the same child, showing that the true deformity lies in the proximal femurand not in the femoral neck. C, Anteroposterior view showing a normal neck–shaft angle of the femur of the same child, afterfemoral rodding and correction of bowing of the proximal femur. D, Lateral view of the femur of same child showing normalalignment of the proximal femur, after femoral rodding and correction of deformity of the proximal femur.
q 2006 Lippincott Williams & Wilkins 27
J Pediatr Orthop � Volume 26, Number 1, January/February 2006 Coxa Vara in Osteogenesis Imperfecta
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

that short femurs were due to bony resections during rod-ding surgery rather than being caused by developmentalabnormalities.
As to the clinical consequences of CV, it is well knownthat a decrease in the neck–shaft angle will shorten the leverarm of the abductor mechanism and thereby cause abductorinsufficiency with a positive Trendelenburg sign.8,18 This waspresent in most of our patients. In addition, the range ofmotion of the hip in all of our patients was limited in abductionand internal rotation, as has also been reported in non-OIpatients with CV.6,11,19
All but the most mildly affected patients in the presentcohort had received bisphosphonates at some point. In theabsence of an untreated control group, we therefore cannotjudge the effect of bisphosphonates on hip development. Thelong-term effects of bisphosphonates on hip developmentremain to be addressed in the future. Thus, our data cannot beused to make recommendations about medical treatment mea-sures that could prevent such a deformity.
In conclusion, we observed a high incidence of CV inchildren and adolescents with severe forms of OI, particularlyOI type III. We believe that the presence of CV may aggravatethe functional status of these children, which is already impairedby bone fragility and multiple deformities. A high index ofsuspicion should be maintained in children with severe OI andregular radiologic follow-up is warranted. It is plausible that themost severely affected patients may benefit from surgicalcorrection, but it is probably not possible to unequivocallydemonstrate the functional benefit of such interventions ina single-center study such as the present one. Rather, the currentstudy attempts to set the scene for future intervention trials.
ACKNOWLEDGMENTSThe authors thank Mr. Denis Alves and Ms. Guylaine
Bedard in the audiovisual department. We are also grateful toMs. Paula Wall and Ms. Josee Perron for their secretarial help.
REFERENCES1. Sillence DO, Senn A, Danks DM. Genetic heterogeneity in osteogenesis
imperfecta. J Med Genet. 1979;16:101–116.2. Rauch F, Glorieux FH. Osteogenesis imperfecta. Lancet. 2004;363:1377–
1385.3. Glorieux FH, Rauch F, Plotkin H, et al. Type V osteogenesis imperfecta:
a new form of brittle bone disease. J Bone Miner Res. 2000;15:1650–1658.
4. Glorieux FH, Ward LM, Rauch F, et al. Osteogenesis imperfecta type VI:a form of brittle bone disease with a mineralization defect. J Bone MinerRes. 2002;17:30–38.
5. Ward LM, Rauch F, Travers R, et al. Osteogenesis imperfecta type VII: anautosomal recessive form of brittle bone disease. Bone. 2002;31:12–18.
6. Weinstein JN, Kuo KN, Millar EA. Congenital coxa vara. A retrospectivereview. J Pediatr Orthop. 1984;4:70–77.
7. Duthie RB, ed.Mercer’s Orthopedic Surgery, 7th ed. Baltimore: Williams& Wilkins, 1973.
8. Tauber C, Ganel A, Horoszowski H, et al. Distal transfer of the greatertrochanter in cox vara. Acta Orthop Scand. 1980;51:661–666.
9. Violas P, Fassier F, Hamdy R, et al. Acetabular protrusion in osteogenesisimperfecta. J Pediatr Orthop. 2002;22:622–625.
10. Carroll K, Coleman S, Stevens PM. Coxa vara: surgical outcomes ofvalgus osteotomies. J Pediatr Orthop. 1997;17:220–224.
11. Pavlov H, Goldman AB, Freiberger RH. Infantile coxa vara. Radiology.1980;135:631–640.
12. Beals RK. Coxa vara in childhood: evaluation and management. J AmAcad Orthop Surg. 1998;6:93–99.
13. Robinow M, Chumlea WC. Standards for limb bone length ratios inchildren. Radiology. 1982;143:433–436.
14. Fassier F, Glorieux F. Osteogenese imparfaite de l’enfant; Cahiersd’enseignement de la SOFCOT. Conferences d’enseignement 1999, p. 241.
15. Currarino G, Birch JG, Herring JA. Developmental coxa vara associatedwith spondylometaphyseal dysplasia (DCV/SMD): ‘‘SMD-corner fracturetype’’ (DCV/SMD-CF) demonstrated in most reported cases. PediatrRadiol. 2000;30:14–24.
16. Langer LO Jr, Brill PW, Ozonoff MB, et al. Spondylometaphysealdysplasia, corner fracture type: a heritable condition associated with coxavara. Radiology. 1990;175:761–766.
17. Burns KA, Stevens PM. Coxa vara: another option for fixation. J PediatrOrthop B. 2001;10:304–310.
18. Tachdijian MO. Developmental coxa vara. In: Tachdijian MO, ed.Pediatric Orthopedics. Philadelphia: WB Saunders, 1990:584–588.
19. Desai SS, Johnson LO. Long-term results of valgus osteotomy forcongenital coxa vara. Clin Orthop. 1993;294:204–210.
28 q 2006 Lippincott Williams & Wilkins
Aarabi et al J Pediatr Orthop � Volume 26, Number 1, January/February 2006
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.















![Tachdjian's Pediatric Orthopaedics [Chapter 18] · Congenital Coxa Vara Incidence, 765 Heredity, 765 Clinical Features, 765 Radiographic Findings, 766 Congenital coxa vara is a developmental](https://img.dokumen.tips/doc/110x75/5ba3689909d3f21e368b5a0e/tachdjians-pediatric-orthopaedics-chapter-18-congenital-coxa-vara-incidence.jpg)