Embed Size (px)
Citation preview

7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 1/17
Congenital Hip Dislocation
Introduction-
Hip dysplasia developmental dysplasia of the hip (DDH) or congenitaldysplasia of the hip (CDH) is a
congenital or acquired deformation or misalignment of the hip joint.Congenital dislocation of hip is a
condition present since birth in which thehead of the femur is detached from the acetabulum or can be
moved in andout of the acetabulum easily.Some children are born with a hip problem called congenital hipdislocation(dysplasia). he condition is usually diagnosed as soon as a baby is born.!ost of the time" it
affects the left hip in first#born children" girls" and babiesborn in the breech position.
Causes-
Se$ (females are more affected than males)Statistics show that the %ative &merican population has a high
incidence of hip dislocation.'nfants born by caesarian and breech position births.stborn infantsHormonal
changes within the mother duringpregnancyther musculos*eletal disorders of intrauterine malpositioning
or crowdingsuch as metatarsus adductus andtorticol lis ligohydramniosHip dysplasia can be associated
with underlying neuromuscular disorders"such as cerebral palsy" myelomeningocele" arthrogryposis" and
+arsensyndrome" although these are not usually considered DDH,amily History (positive in up to one third
of cases)
• ne affected sibling- / ris*b.
• ne affected parent- 0/ ris*
• ne affected sibling and one affected parent- 1/
Types of Congenital Hip Dislocation
. Classic congenital Hip Dislocation0. Congenital &bduction Contracture of the Hip
1. eratologic Congenital Hip Dislocationa.
a. Severe" prenatal fi$ed dislocation
b. &ssociated with genetic and neuromuscular disorders
Symptoms
'n congenital dislocation" the earliest sign may be a 2clic*ing3 sound when thenewborn4s legs are pushed
apart. 'f the condition goes undetected at thenewborn stage" eventually the affected leg will loo* shorter than
the other one"s*in folds in the thighs will appear uneven" and the child will have lessfle$ibility on the
affected side. 5hen he starts to wal*" he4ll probably limp" wal*on his toes" or 2waddle3 li*e a duc*.+egs of
different lengths.hip clic*6neven thigh s*in folds.+ess mobility or fle$ibility on one side.'n children whohave begun to wal*" limping" toe wal*ing and awaddling 7duc*#li*e7 gait are also signs.&n*le
fracturesbuttoc*s folds also may not be symmetrical with more creases on thedislocated sideHip pain
commonly manifests as *nee or anterior thigh pain
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 2/17
Diagnosis
& careful physical e$amination of a newborn usually detects hip dislocation. 'nolder infants and children"
hip $#rays can confirm the diagnosis.&rthrograms are dynamic studies" performed by injecting dye into
thehip joint and then e$amining the patient with aid of fluoroscopy" usually withthe patient under
anesthesia.& careful physical e$amination of a newborn usually detects hip dislocation. 'nolder infants and
children" hip $#rays can confirm the diagnosis.'maging
A. Dynamic Hip Ultrasound (infant aged 1-6 monts)
. Diagnostic for congenital Hip Dislocation
0. 8valuates for sublu$ation and reducibility
1. High false positive rate 9 wee*s
!. Hip "#ay
. %ot diagnostic for dislocation until : months
. ,emoral head not calcified under age ;# months
0. Diagnostic for &cetabular Dysplasiaa. &bnormal acetabular fossa will be seen
C. $%aluated &it reference lines dra&n o%er A' "-#ay
. Hilgenreiner<s +inea. Hori=ontal line through triradiate cartilages
0. >er*in<s +inea. ?ertical line along each lateral acetabulum
1. Shenton<s +ine
a. ,emoral nec* medial border
b. Superior border of obturator foramen
edical anagement-
A. anagement indicated for ip insta)ility )eyond * days
!. Step 1+ 'a%li, Harness
. 'ndicated as first#line if age 9 months
0. Start with harness trial for 1#; wee*s
1. Splints hips in fle$ed and abducted position
;. +ong#term effect- @A/ (B/ if fran* dislocation)
A. 6ltrasound should demonstrate reduction at 1 wee*s
a. educed- Continue harness for : wee*s
b. %ot educed- Eo to Step 0
C. Step + Closed #eduction and Casting )y rtopedics
. 'ndicationsa. %o reduction with >avli* Harness in 1#; wee*sb. Children over age months
0. &ttempted closed reduction under arthrogram
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 3/17
1. Hip Spica Casting for 0 wee*s
;. >ositioning confirmed by post#op !' or C
D. Step /+ Surgical pen reduction
. 'ndicated in refractory cases
0. equires multi#step procedure
a. endon lengthening
b. Clearing tissues obstructing relocation
c. ightening hip capsule
d. steotomy if performed after age B month
1. Complicated by re#dislocation" osteonecrosis
0ursing anagement
F >lacing rolled cotton diapers or a pillow between the thighs" thereby*eeping the *nees in a frog li*e
position
F ! e$ercise to unaffected issue
F 'mmobili=ation of hips in less than # degrees abduction per hip
F !eticulous s*in care around the immobili=ed tissues
F ,or patients who have splints" remind parents to maintain good diaper areacare- change diapers frequently
and wash area and apply an ointment suchas & and D oint*ment" vaseline r Desitin at each diaper change
since this canlead to severe diaper rash
F each parents to swaddle the baby tightly because this action is comforting.
F ,or older patients encourage a balanced diet" foods that promote healingsuch as protein rich foods and as
well as vit c rich foods
F !aintain proper positioning and alignment to limit further injury
F &ccompanying soft tissue injuries are treated by 'C8 therapy-
# rest
'# ice
C#compression bandage
8# elevation with or without immobili=ation
F Stimulation of affected area by isometric and isotonic e$ercises also helpspromote healing
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 4/17
Clu) foot ( Talipes $uino%arus2
Definition 3
Clubfoot also *nown as alipes 8quinovarus is a congenital deformity of foot characteri=ed by abduction offoot" inversion of the sub#taller joint and plantar fle$ion of the an*le joint.
alipes deformity is a disorder of an*le and foot. 't comes from the +atin wordstalus meaning an*le and pes
meaning foot.
Incidence 3
Commonly called clubfoot" it is a congenital anomaly occurring at appro$imately to 0 in every live
births.
!ale#female incidence ratio is 0-.Gilateral deformity involvement accounts 1/#A/ of cases.
T&o Types of Clu)foot 3
. >seudo#talipes #deformity that has developed because of the intrauterine position (metatarsus adductus)foot loo*s to be turned in but can be brought into a straight position by manipulation
0. rue talipes I conegenital talipes equinovarus
Types of True Talipes 3
. 8quinus (plantarfle$ion)0. Calcaneus (Dorsifle$ion)
1. ?arus (foot turns inward)
;. ?algus (foot turns outward)
$tiology-
alipes is a +atin word from the words-
• talus wJc means an*le
• pes wJc means foot
Congenital clubfoot is also reffered to as 2idiophatic3 clubfoot" meaning that the condition arises
spontaneously from an un*nown cause
'atopysiology-
he e$act cause of this deformity is un*nown. Gut suggestions or ypoteses of its disease process are the
following-
• Eenetic factor
• &bnormal tendon insertion
&nomalous tendons may affect the alignment of the foot.
• etracting fibrosis (myofibrosis)
Collagen found in all ligaments and tendons are coiled and could be stretched with the e$ception of&chilles tendon (made up of tightly coiled collagen and cannot be stretched).
hic*ening and scarring of fibrous tissue could cause the twisted foot appearance.
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 5/17
• %eurogenic factors
• 'nnervation changes during the prenatal period could be due to the presence of neurologic events or
disorder such as" spina bifida. Studies show that 1A/ of children with clubfoot have neurologic
impairment.
•
ligohydramnios,luid lea* during the prenatal period could cause restriction of fetal movements thereby"
predisposing to a deformed foot. Developmental arrest of fetal development .Disruption of themedial rotation of the fetal foot could result to a clubfoot condition.
• Diminished ?ascular Circulation
Disruption of the branches of the vascular supply of the lower e$tremity could contribute to
misalignment of the foot.
anagement-
Diagnostic $%aluation-
'ysical $4amination-
• wisted foot appearance should be assessed and gently manipulated. 'f the straightened foot does
not move to a normal position" true clubfoot is present.
adiography
• 6se of $#rays is definitive diagnosis for clubfoot as it determines abnormal bone anatomy and
assesses the treatment efficiency.
Categories of treatment+
. ,or mild cases- manipulation" cast and splint application (nonsurgical management)
0. ,or severe cases- surgery
0onsurgical management-
'onseti etod I &pplies certain techniques to reduce and correct the deformity to promote normal foot
mobility and position. !ethods used are the following-. !anipulation # Slightly pivoting the bones and stretching the soft tissue
0. >lacement of above the *nee cast• ,requency of changing the cast is every A#K days to accommodate the rapid growth during the first
year of life.
• 'n most cases" severing of &chilles tendon (tenotomy) is done before the final cast is applied. he
reason for doing this is to loosen the foot. he procedure is usually done in a clinic where a local
anesthetic is used. & small cut (about 1 mm) is made above the heel of the foot to lengthen thetendon. &fter the procedure final casting is done.
• ,inal cast is removed after 0#1 wee*s when &chilles tendon is already healed.
• &fter the final cast is removed-
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 6/17
. Denis !ro&n Splints (shoes or boots attached to a bar) are used 01 hours each day for 1 months to
maintain the normal foot alignment. ,or the ne$t 0#; years the splint is fitted during naps and nighttime
only.
0. >assive foot e$ercises (full range#of#motion) are e$ecuted by the primary caregiver to further maintain the
position.>ost#tenotomy management
bserve for the following-
• Drainage on the cast
• ,oul smelling odor from inside the cast.
• Swelling" redness and irritation at the distal portion of the cast.
• High fever
'li=arov echnique I !ethod used for comple$ an*le#foot deformity. Ili5aro% frames" the circular structure placed around the limb" are used in this technique which are attached to metal pins and are inserted through
the bone. & frame is individually made for each patient and weighs appro$imately K lbs. >lacement of the
frame requires the administration of a general anesthetic and the procedure may last for several hours.
Surgical anagement-
'osteromedial #elease 3
he last option for a clubfoot is the release of all tight tendons and ligaments in the posterior and medial
parts of the foot. he structures are then put bac* together in a lengthened position.
endon ransplantDone at ;#K years of age when other corrective measures have been ineffective.
Complications 3
L #oc,er )ottom oot
?ertical talus results from a forceful manipulation causing bone brea*age. his then will give rise to a flat
foot.
L #ecurrent deformity
he corrected foot may return to its deformed state if the parents or primary caregiver fails to apply the
methods to further correct the position (e.g. passive foot e$ercises and Denis Grown splint).
0ursing Inter%entions 3
. btain a family and obstetric history for ris* factors.
0. &fter delivery" assess the an*le and foot for a true talipes deformity by straightening the foot. >seudo#
talipes can be realigned to a normal position.
1. ,or infants with cast assess for circulation" redness and swelling distal from the cast and foul odor.;. !onitor the infant4s temperature (for those who underwent tenotomy or surgery). ,ever is the first sign of
infection.
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 7/17
A. Cautiously evaluate crying. 'nfants cannot voice out pain. Crying may mean hunger" wet diapers"
abdominal pain or tingling sensation from a tight cast.. Meep the cast clean and dry by changing diapers frequently. 6se a damp cloth and dry cleansers in
wiping. 5ater and soap causes brea*down of cast particles.
K. >lace a pillow or padding under the casted area to prevent cast damage and prevent sores from heel
pressure.B. ,or children with traction" chec* and cleanse the pin sites frequently.
@. 8$plain to the parents the importance of passive foot e$ercises after the final cast is removed.
. !aintaining the aligned position after the cast application is essential to prevent reoccurrence.. &dminister analgesics as ordered for pain relief after a surgical correction.
0. &ssess coping mechanisms of family and resources available for long#term treatment.
$4ercise 3
8$ecution of passive foot e$ercises several times a day for several months to maintain the corrected foot
alignment.
%ever forcibly evert or pronate the foot during clubfoot casting. his can cause damage to the bones.
Treatment I
Cast application
>hysiotherapy
Surgery (last option)
Healt Teacing
Cast care-
,requently change the infant4s diaper to prevent soiling of the cast.
6se dry cleanser in wiping the cast.
ngoing Assessment#
&ssess the circulation of casted foot.
Diet 3
Greastfeeding for infants younger than ;# months.
,or older infants" introduction of solid foods must have the interval of A#K days.
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 8/17
Co4a 'lana
Introduction-
Co$a >lana (+eggICalvNI>erthes Disease) is a form of osteochondritis of the hip joint" where growthJlossof bone mass leads to some degree of collapse of the hip joint and to deformity of the ball of the femur and
sometimes the surface of the hip soc*et. 'ts characteri=ed by idiopathic avascular osteonecrosis of the capital
femoral epiphysis of the femoral head leading to an interruption of the blood supply of the head of the femur
close to the hip joint. he disease is typically found in young children" specifically boys aged ;#" and it
can lead to osteoarthritis in adults. he effects of the condition can sometimes continue into adulthood.
Definition-
+egg#Calve#>erthes Disease or Co$a >lana is a childhood disease that affects the head of the femur (the ball
of the thigh bone at the hip joint) resulting in inadequate supply of blood to the epiphysis.
Causes and #is, actors of 7egg-Cal%e-'ertes Disease or Co4a 'lana-
+egg#Calve#>erthes Disease or Co$a >lana is caused due to lac* of blood supply to the ball portion of the
joint of the hip that is the femoral head forcing the bone to become unstable and wea* and to brea* down
easily" which later on recovers very poorly. <hough the e$act cause of this decrease in blood flow to the
femoral head is still not *nown" some of the suspected causes of +egg#Calve#>erthes Disease may include-
&ge- +egg#Calve#>erthes Disease most commonly affects children in the age group of four to eight years.
Se$- Goys are five times more prone to +egg#Calve#>erthes Disease when compared to girls.
ace- +egg#Calve#>erthes Disease more commonly affects white children than blac* children.
,amily History- +egg#Calve#>erthes Disease is seen to run in families in few of the cases.
C7I0ICA7 I0DI08S-
+imping gait (pathognomonic sign)
!oderate to severe hip" *nee or groin pain" e$acerbated by hipJleg movement
&pparent shortening of the leg in area and length
+imitation of movements
Stiffness or pain in the thigh" *nee" hip and groin.
Eradual worsening of limping.
Decreased range of motion of the affected hip.
Stiffness in the affected hip.
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 9/17
he affected leg may loo* shorter than the healthy leg.
he affected leg may also become slightly thinner eventually due to the thinner thigh muscles
because of less usage when compared to thigh muscles in the healthy leg.
DIA80STIC T$ST-
& complete subjective and physical e$amination is performed to diagnose +egg#Calve#>erthes Disease. &
physician will move around the affected leg in order to e$amine the pain. & leg is also rotated in different
positions in order to chec* for reduced range of motion.
O#ays of the hip may suggest andJor verify the diagnosis.
& bone scan or !' may be useful in ma*ing the diagnosis in those cases where $#rays are inconclusive
!agnetic resonance imaging (!').
A0A8$$0T-
&nti#inflammatory medicine (such as ibuprofen) can relieve stiffness in the hip joint
he treatment for +egg#Calve#>erthes Disease or Co$a >lana usually concentrates on *eeping the femoral
head as round as possible in order to help the hip to function appropriately. he soc*et wor*s li*e a mold for
the fractured femoral head during the healing process. here are many treatment options available for
*eeping femoral head snug in the soc*et of the joint. he healing time varies with each patient depending
upon the severity of the affected bone. he treatment process usually ta*es couple of years or more.
'f the patient is less than seven years of age and the femoral head is still round in shape" then the helpfulnonsurgical treatments for +egg#Calve#>erthes Disease may include.
#est- Decreasing the amount of stress and weight on the affected bone helps in slowing down the damage
caused due to +egg#Calve#>erthes Disease. estricting heavy amount of physical activity and using crutches
may help in *eeping the weight off from the affected joint.
Traction+ 8pisodes of traction and bed rest are also helpful to treat severe pain.
Casting- &s it is important to *eep the femoral head in its soc*et" a special *ind of leg cast is also used in
order to *eep both the legs spread widely apart for about four to si$ wee*s of duration.
$4ercises- Stretching and strengthening e$ercises help in *eeping the hip more fle$ible. 8$ercises not only
help in improving range of motion and muscle strength" but also maintain the balance and coordination of
the joint.
Surgery- Surgery is performed only when nonsurgical treatments fail to wor* appropriately for +egg#Calve#
>erthes Disease. his usually happens in case of patients above seven years of age. his may also wor* for
children suffering with more severe bone deformities. Surgeries may include-
Contracture #elease- +egg#Calve#>erthes Disease and the periods of immobility during treatment can
shorten some of the nearby tendons and muscles" which can cause the hip to pull inward forming a
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 10/17
contracture. Surgery may be required to lengthen out these tissues and help restore normal fle$ibility of the
hip joint.
7oose !ody #emo%al- 'n few cases" the damage to the femoral head leads to loosing bits of bone or tearing
of cartilage flaps. Surgery may be required to remove these bits of tissues and help the hip joint to function
smoothly.
Hard&are Implants- Hardware implants are placed when leg casts fail to *eep the ball and soc*et incorrect position due to which changing ball and soc*et position becomes necessary. Hardware implants may
include plates" wires" and screws.
'ysical Terapy- >hysical therapy for +egg#Calve#>erthes Disease is important in speeding up the healing
process and obtaining optimal results. >hysical therapy also decreases the li*elihood of recurrences in the
future. >hysical therapy may include-
Point mobili=ation.
8$ercises to improve strength and fle$ibility.
&ctivity modification and training.
&ppropriate plan for return to activity.
Hydrotherapy.
$4ercises for 7egg-Cal%e-'ertes Disease or Co4a 'lana-
Geneficial e$ercises for +egg#Calve#>erthes Disease or Co$a >lana concentrate on internal rotation" e$ternal
rotation" abduction" adduction" fle$ion and e$tension of the hips. &bduction e$ercises move the leg away
from hip whereas adduction e$ercises are performed by bringing the hip closer to the midline of the body.
'nternal and medial rotation is performed by turning the toes in toward the center of the body and e$ternal or
lateral rotation is performed by moving the toes outward. ,le$ion is caused when *nees are bent toward the
hips whereas e$tension e$ercises helps in straightening the legs. hese e$ercises are also performed by lying
on a bed and e$ercise mat in order to *eep the weight off the hip joints. Swimming may prove to be a good
e$ercise as it not only strengthens the muscles" but also provides range of motion e$ercises while water
helps in supporting the body weight.
8$ercises" contact sports and activities that involve jumping or running or activities that place weight on the
hips should be strictly avoided as they may worsen the condition.
0U#SI08 A0A8$$0T-
ange of motion e$ercises can help maintain joint mobility.
'nstruct the patient and parents to maintain activities that promote !.
'nstruct patient to limit activity and avoid contact sports and high#impact running.
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 11/17
>rovide equipment to assist with mobility such as crutches" wheelchairs and wal*ers.
ST$8$0$SIS I'$#$CTA
Definition-
steogenesis imperfecta (')" also *nown as brittle bone disease or +obstein syndrome" is a congenital bone disorder characteri=ed by brittle bones that are prone to fracture
' may also present with shorter height" neurological features including communicating hydrocephalus
"basilar invagination" and sei=ures" blue sclerae" hearing loss" or other complications. he fractures
themselves can cause acute or chronic pain" reduced quality of life" and depression.
CAUS$S-
Grittle bone disease is caused by a genetic defect that affects the production and formation of type
collagen" a protein used to create bone. he defective gene is usually inherited" but in some cases the defect
occurs due to a spontaneous mutation.
Symptoms-
bone deformities
multiple bro*en bones
loose joints
short stature
wea* teeth
riangular shaped face
blue sclera
bowed legs and arms
*yphosis
scoliosis
early hearing loss
respiratory problems
heart defects
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 12/17
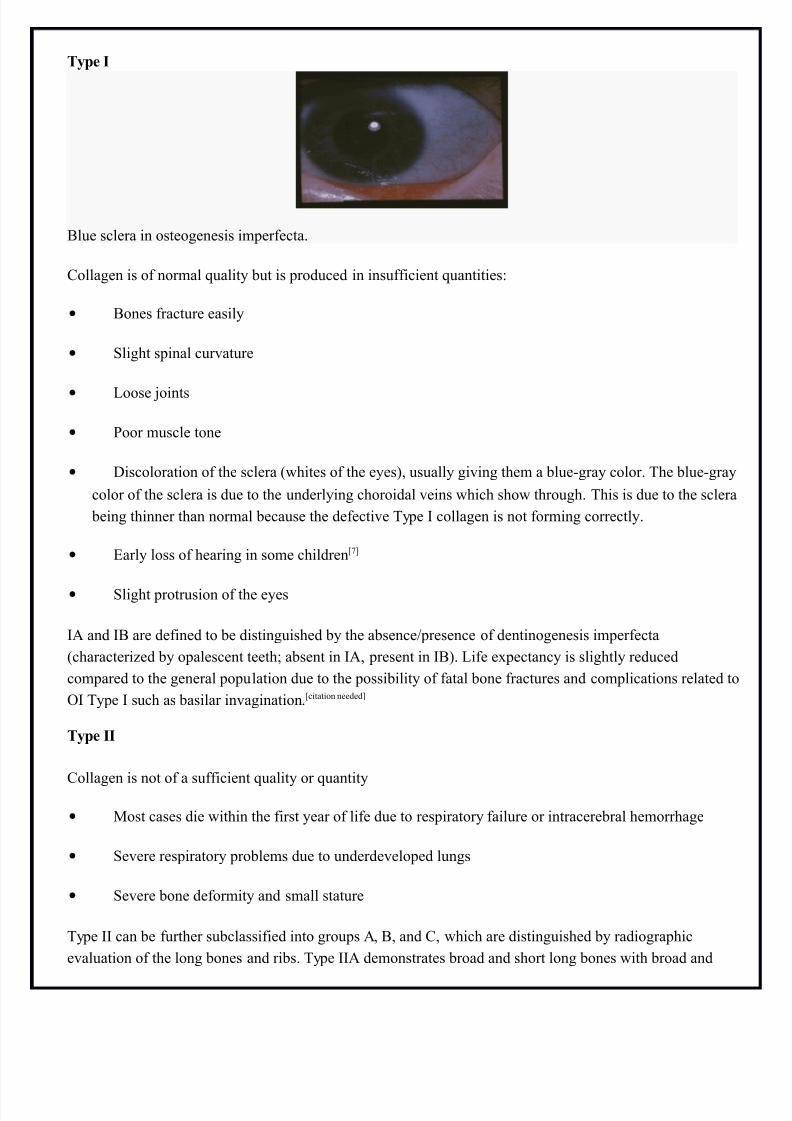
Type I
Glue sclera in osteogenesis imperfecta.
Collagen is of normal quality but is produced in insufficient quantities-
• Gones fracture easily
• Slight spinal curvature
• +oose joints
• >oor muscle tone
• Discoloration of the sclera (whites of the eyes)" usually giving them a blue#gray color. he blue#gray
color of the sclera is due to the underlying choroidal veins which show through. his is due to the sclera
being thinner than normal because the defective ype ' collagen is not forming correctly.
• 8arly loss of hearing in some childrenQKR
• Slight protrusion of the eyes
'& and 'G are defined to be distinguished by the absenceJpresence of dentinogenesis imperfecta
(characteri=ed by opalescent teeth absent in '&" present in 'G). +ife e$pectancy is slightly reduced
compared to the general population due to the possibility of fatal bone fractures and complications related to
' ype ' such as basilar invagination.Qcitation neededR
Type II
Collagen is not of a sufficient quality or quantity
• !ost cases die within the first year of life due to respiratory failure or intracerebral hemorrhage
• Severe respiratory problems due to underdeveloped lungs
• Severe bone deformity and small stature
ype '' can be further subclassified into groups &" G" and C" which are distinguished by radiographic
evaluation of the long bones and ribs. ype ''& demonstrates broad and short long bones with broad and
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 13/17
beaded ribs. ype ''G demonstrates broad and short long bones with thin ribs that have little or no beading.
ype ''C demonstrates thin and longer long bones with thin and beaded ribs.
Type III
Collagen improperly formed" enough collagen is made but it is defective
• Gones fracture easily" sometimes even before birth
• Gone deformity" often severe
• espiratory problems possible
• Short stature" spinal curvature and sometimes barrel#shaped rib cage
• riangular faceQBR
• +oose joints (double jointed)
• >oor muscle tone in arms and legs
• Discolouration of the sclera (the <whites< of the eyes are blue)
• 8arly loss of hearing possible
ype ''' is distinguished among the other classifications as being the 7progressive deforming7 type" wherein
a neonate presents with mild symptoms at birth and develops the aforementioned symptoms throughout life.+ifespans may be normal" albeit with severe physical handicapping.
Type I9
Collagen quantity is sufficient but is not of a high enough quality
• Gones fracture easily" especially before puberty
• Short stature" spinal curvature" and barrel#shaped rib cage
• Gone deformity is mild to moderate
• 8arly loss of hearing
Similar to ype '" ype '? can be further subclassified into types '?& and '?G characteri=ed by absence
('?&) or presence ('?G) of dentinogenesis imperfecta.
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 14/17
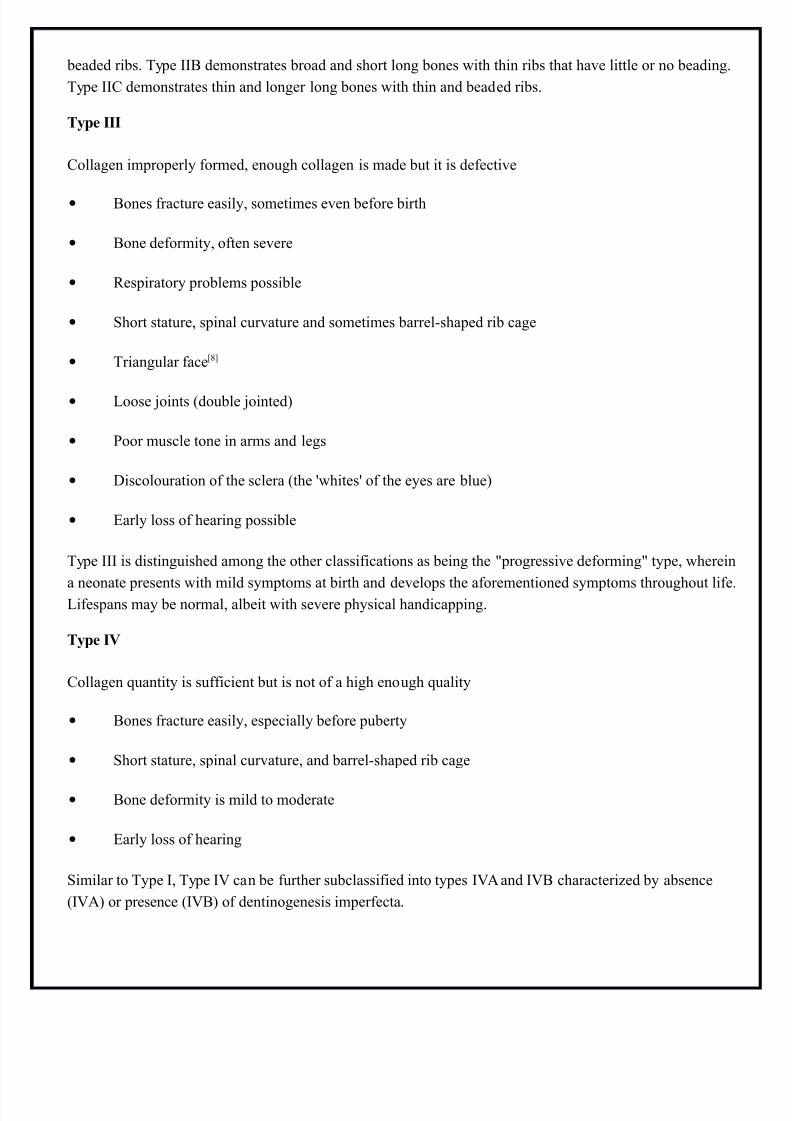
Type 9
' ype ? in an adult
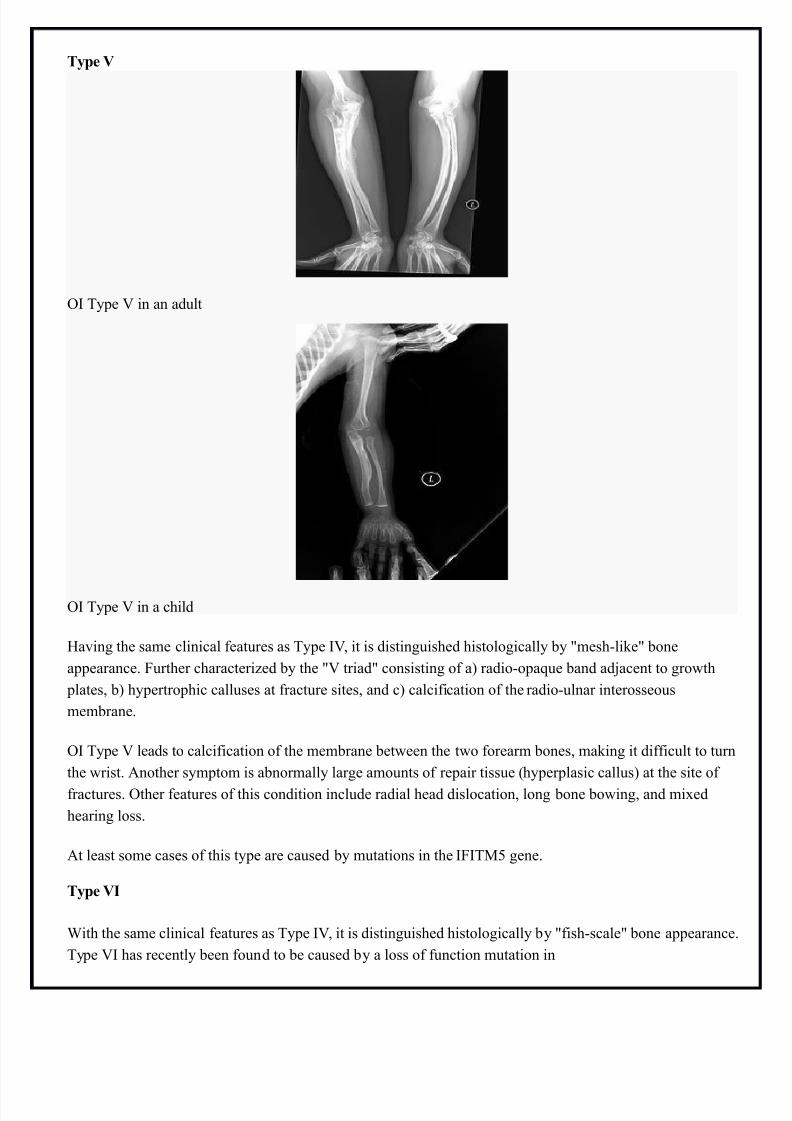
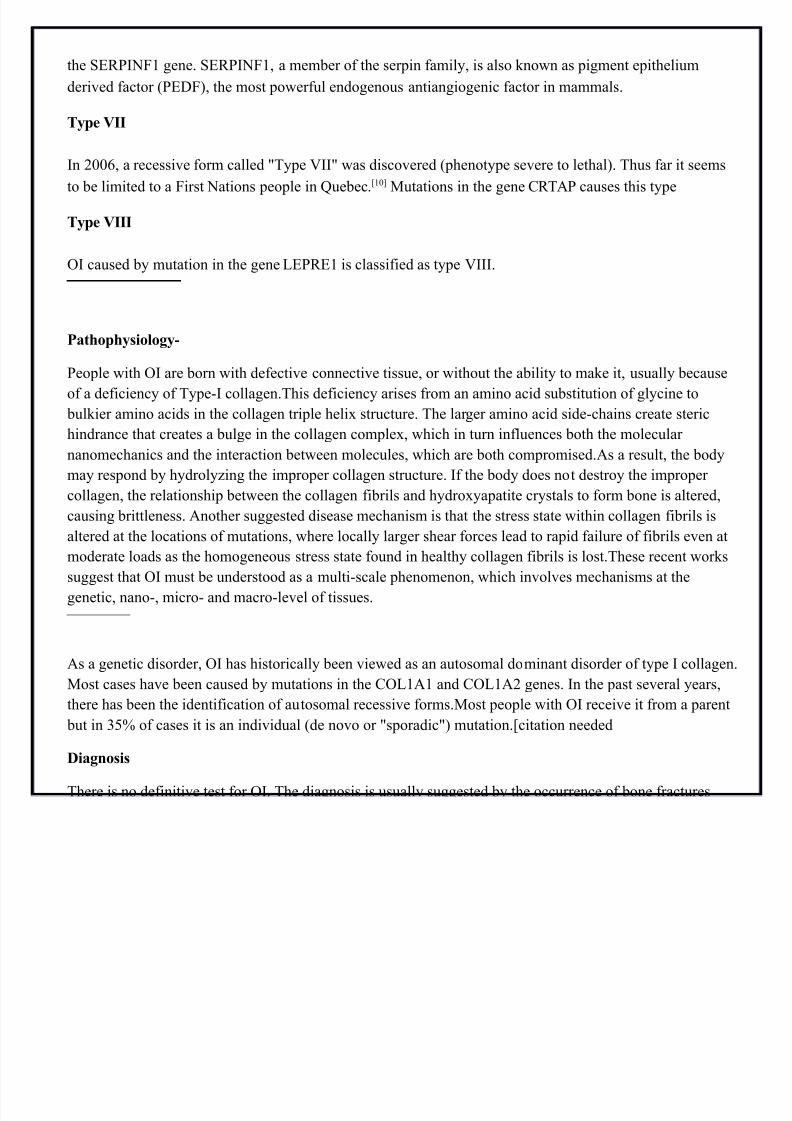
' ype ? in a child
Having the same clinical features as ype '?" it is distinguished histologically by 7mesh#li*e7 bone
appearance. ,urther characteri=ed by the 7? triad7 consisting of a) radio#opaque band adjacent to growth
plates" b) hypertrophic calluses at fracture sites" and c) calcification of the radio#ulnar interosseous
membrane.
' ype ? leads to calcification of the membrane between the two forearm bones" ma*ing it difficult to turn
the wrist. ¬her symptom is abnormally large amounts of repair tissue (hyperplasic callus) at the site of
fractures. ther features of this condition include radial head dislocation" long bone bowing" and mi$ed
hearing loss.
&t least some cases of this type are caused by mutations in the ','!A gene.
Type 9I
5ith the same clinical features as ype '?" it is distinguished histologically by 7fish#scale7 bone appearance.
ype ?' has recently been found to be caused by a loss of function mutation in
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 15/17
the S8>'%, gene. S8>'%," a member of the serpin family" is also *nown as pigment epithelium
derived factor (>8D,)" the most powerful endogenous antiangiogenic factor in mammals.
Type 9II
'n 0" a recessive form called 7ype ?''7 was discovered (phenotype severe to lethal). hus far it seems
to be limited to a ,irst %ations people in uebec.QR !utations in the gene C&> causes this type
Type 9III
' caused by mutation in the gene +8>8 is classified as type ?'''.
'atopysiology-
>eople with ' are born with defective connective tissue" or without the ability to ma*e it" usually because
of a deficiency of ype#' collagen.his deficiency arises from an amino acid substitution of glycine to bul*ier amino acids in the collagen triple heli$ structure. he larger amino acid side#chains create steric
hindrance that creates a bulge in the collagen comple$" which in turn influences both the molecular
nanomechanics and the interaction between molecules" which are both compromised.&s a result" the body
may respond by hydroly=ing the improper collagen structure. 'f the body does not destroy the improper
collagen" the relationship between the collagen fibrils and hydro$yapatite crystals to form bone is altered"
causing brittleness. ¬her suggested disease mechanism is that the stress state within collagen fibrils is
altered at the locations of mutations" where locally larger shear forces lead to rapid failure of fibrils even at
moderate loads as the homogeneous stress state found in healthy collagen fibrils is lost.hese recent wor*s
suggest that ' must be understood as a multi#scale phenomenon" which involves mechanisms at the
genetic" nano#" micro# and macro#level of tissues.
&s a genetic disorder" ' has historically been viewed as an autosomal dominant disorder of type ' collagen.
!ost cases have been caused by mutations in the C+& and C+&0 genes. 'n the past several years"
there has been the identification of autosomal recessive forms.!ost people with ' receive it from a parent
but in 1A/ of cases it is an individual (de novo or 7sporadic7) mutation.Qcitation needed
Diagnosis
here is no definitive test for '. he diagnosis is usually suggested by the occurrence of bone fractures
with little trauma and the presence of other clinical features. & s*in biopsy can be performed to determine
the structure and quantity of type ' collagen. D%& testing can confirm the diagnosis" however" it cannot
e$clude it because not all mutations causing ' are *nown andJor tested for. ' type '' is often diagnosed by
ultrasound during pregnancy" where already multiple fractures and other characteristic features may be
present. elative to control" ' cortical bone shows increased porosity" canal diameter" and connectivity in
micro#computed tomography.QR
7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 16/17
&n important differential diagnosis of ' is child abuse" as both may present with multiple fractures in
various stages of healing. Differentiating them can be difficult" especially when no other characteristic
features of ' are present. ther differential diagnoses include ric*ets" osteomalacia" and other rare s*eletal
syndromes.
Treatment
here is no cure for '. reatment is aimed at increasing overall bone strength to prevent fracture andmaintain mobility. Gisphosphonates can increase bone mass" and reduce bone pain and fracture. 'n severe
cases" bones are surgically corrected" and rods are placed inside the bones" particularly to enable infants to
learn to wal*.
Gone infections are treated as and when they occur with the appropriate antibiotics and antiseptics.
Gisphosphonates
'n @@B" a clinical trial demonstrated the effectiveness of intravenous pamidronate" a bisphosphonate which
had previously been used in adults to treat osteoporosis. 'n severe '" pamidronate reduced bone pain"
prevented new vertebral fractures" reshaped previously fractured vertebral bodies" and reduced the number
of long#bone fractures.
<hough oral bisphosphonates are more convenient and cheaper" they are not absorbed as well" and
intravenous bisphosphonates are generally more effective" although this is under study. Some studies have
found oral and intravenous bisphosphonates" such as oral alendronate and intravenous pamidronate"
equivalent. 'n a trial of children with mild '" oral risedronate increased bone mineral densities" and reduced
nonvertebral fractures. However" it did not decrease new vertebral fractures
Surgery
!etal rods can be surgically inserted in the long bones to improve strength" a procedure developed by
Harold &. Sofield" !D" at Shriners Hospitals for Children in Chicago. During the late @;s" Sofield" Chief
of Staff at Shriners Hospitals in Chicago" wor*ed there with large numbers of children with ' and
e$perimented with various methods to strengthen the bones in these children. 'n @A@" with 8dward &.
!iller" !D" Sofield wrote a seminal article describing a solution that seemed radical at the time- the
placement of stainless steel rods into the intramedullary canals of the long bones to stabili=e and strengthen
them. His treatment proved e$tremely useful in the rehabilitation and prevention of fractures it was adoptedthroughout the world and still forms the basis for orthopedic treatment of '.
Spinal fusion can be performed to correct scoliosis" although the inherent bone fragility ma*es this operation
more comple$ in ' patients. Surgery for basilar impressions can be carried out if pressure being e$erted on
the spinal cord and brain stem is causing neurological problems.
'ysioterapy

7/26/2019 coxa plana.docx
http://slidepdf.com/reader/full/coxa-planadocx 17/17
>hysiotherapy is used to strengthen muscles and improve motility in a gentle manner" while minimi=ing the
ris* of fracture. his often involves hydrotherapy and the use of support cushions to improve posture.
'ndividuals are encouraged to change positions regularly throughout the day to balance the muscles being
used and the bones under pressure.
Children often develop a fear of trying new ways of moving due to movement being associated with pain.his can ma*e physiotherapy difficult to administer to young children.
'ysical aids-
5ith adaptive equipment such as crutches" wheelchairs" splints" grabbing arms" or modifications to the
home" many individuals with ' can obtain a significant degree of autonomy.