Embed Size (px)
Citation preview

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Healthcare:Identifying Opportunities for
Intervention Prior to OverdoseMichele K. Bohm, MPH, Health Scientist, Centers for Disease Control and Prevention
Lindsey Bridwell, MPH, CHES, Evaluation Fellow, Opioid Overdose Health Systems Team, Centers for Disease Control and Prevention
Alexander Y. Walley, MD, MSc, Associate Professor of Medicine,Boston University School of Medicine
Third-Party Payer Track
Moderator: Amy G. Griffin, JD, Corporate Counsel, Kentucky Employers’ Mutual Insurance
ALTERED FROM LIVE PRESENTATION
#Rx Summit www.NationalRxDrugAbuseSummit.org
Disclosures
Lindsey Bridwell, MPH, CHES, Michele K. Bohm, MPH, Alexander Y. Walley, MD, MSc, and Amy G. Griffin, JD, have disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce healthcare goods and services.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Disclosures
All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
The following planners/managers have the following to disclose:- Kelly J. Clark, MD, MBA, FASAM, DFAPA –
Consulting fees: Braeburn, Indivior

#Rx Summit www.NationalRxDrugAbuseSummit.org
Learning Objectives
Explain how non-fatal drug overdose trends and healthcare utilization histories can inform prevention.
Describe differences in healthcare utilization patterns by insurance type for heroin overdose.
Identify strategies to support interventions at the point of care prior to the first heroin overdose.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Organization of Session
Heroin and Healthcare: What We Know
Heroin Overdose Trends, Healthcare Utilization, and Diagnoses Prior to Overdose
Heroin and Healthcare: Clinical Perspectives
.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Healthcare: What We Know
Lindsey Bridwell, MPH, CHES®
Evaluation FellowCenters for Disease Control and Prevention

#Rx Summit www.NationalRxDrugAbuseSummit.org
Topics
Role of Heroin in the Opioid Overdose Epidemic Heroin and Challenges for Prevention Other Adverse Health Outcomes
- Infectious Disease- Neonatal Abstinence Syndrome
Healthcare Access and Use by Payer Health Status and Comorbidities Gaps in Science
#Rx Summit www.NationalRxDrugAbuseSummit.org
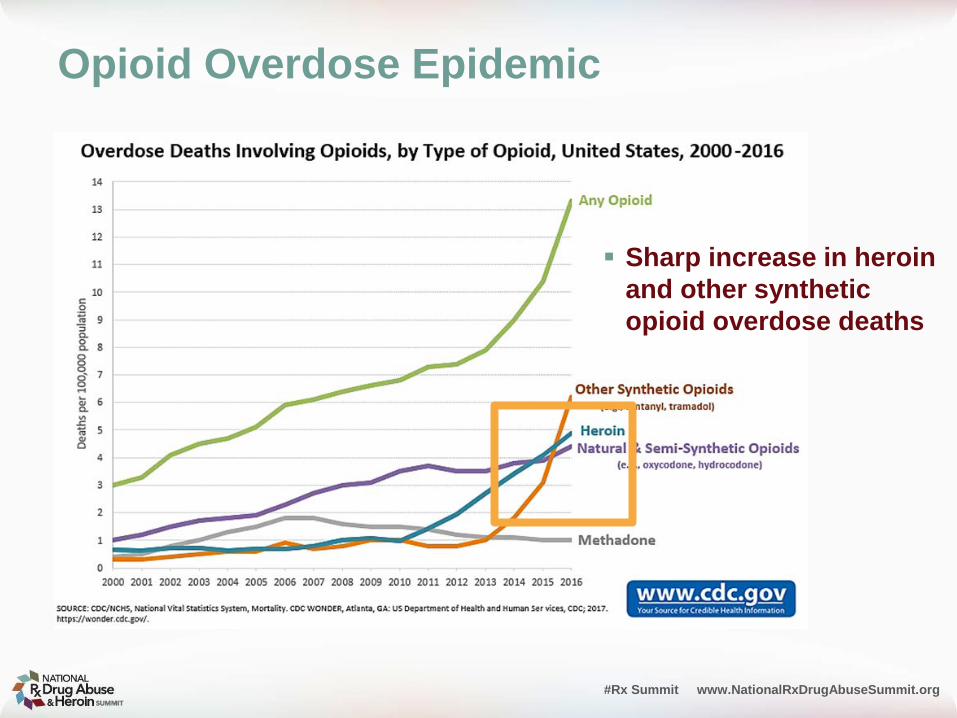
Opioid Overdose Epidemic
Sharp increase in heroin and other synthetic opioid overdose deaths

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Challenges for Prevention
Polysubstance Use
Rx OPIOIDS

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Challenges for Prevention
Average annual rates of heroin use per 1,000 people and the percent increase for 2002–2004 and 2011–2013
National Survey on Drug Use and Health, 2002-2013.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Challenges for Prevention
Past Year Heroin Use Disorder by Age Group, 2002-2016
2016 National Survey on Drug Use and Health
18-25 year olds have the highest prevalence of heroin use disorder
Year

#Rx Summit www.NationalRxDrugAbuseSummit.org
Adverse Health Outcomes Infectious Disease
* Rate = the number of reported cases of acute hepatitis C per 100,000 population

#Rx Summit www.NationalRxDrugAbuseSummit.org
Adverse Health Outcomes Neonatal Abstinence Syndrome (NAS)
Incidence 1.5 per 1000 hospital
births --1999 6 per 1000 hospital births
– 2013 300% increase
Cost --$1.5 Billion – 2012 Medicaid financially
responsible for 80%
Neonatal abstinence syndrome (NAS) incidence rates — 25 states, 2012–2013
Ko JY, Patrick SW, Tong VT, Patel R, Lind JN, Barfield WD. Incidence of Neonatal Abstinence Syndrome — 28 States, 1999–2013. MMWR Morb Mortal Wkly Rep 2016;65:799–802.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Healthcare Access and Use How Does Healthcare Access Vary by Payer for
Adults in the General Population?
Medicaid and CHIP Payment and Access Commission (2014). Revisiting Emergency Department Use in Medicaid. MACfacts-Key Findings on Medicaid and CHIP.
#Rx Summit www.NationalRxDrugAbuseSummit.org
Healthcare Access and Use
Affordable Care Act (ACA) and People With Substance Use Disorders
- Pre-ACA, slightly higher prevalence of substance use disorders among uninsured individuals who would be eligible for expanded Medicaid in 2014 [compared to traditional Medicaid beneficiaries].¹
- Among people with HUD, the prevalence of uninsured persons declined from 40 per 100 to 28 per 100 (OR= 0.59; CI= 0.39 – 0.89) largely due to Medicaid expansion – but there was no increase in treatment.²
1. Busch, S. H., Meara, E., Huskamp, H. A., & Barry, C. L. (2013). Characteristics of adults with substance use disorders expected to be eligible for Medicaid under the ACA. Psychiatr Serv, 64(6), 520-526. doi:10.1176/appi.ps.201200011
2. Feder KA, Mojtabai R, Krawczyk N, et.al. “Trends in insurance coverage and treatment among persons with opioid use disorders following the Affordable Care Act.” Drug Alcohol Depend. 2017 Aug 9;179:271-274.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Health Status and Comorbidities
Medicaid and CHIP Payment and Access Commission (MACPAC). 2012b. Section B: Access to care for non-elderly adults. In Report to the Congress on Medicaid and CHIP. June 2012. Washington, DC: MACPAC.
In general, Medicaid enrollees have a higher prevalence of comorbidities and poorer health status compared to enrollees with Employee Sponsored Insurance (ESI) and the uninsured.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Gap in the Science ap in the Literature and Science Characteristics and trends of non-fatal heroin
overdose by payer
Do not know…•Patterns of healthcare utilization prior to overdose
•Diagnoses preceding overdose•Prescription opioid use prior to overdose

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin Overdose Trends, Healthcare Utilization, and Diagnoses
Prior to Overdose for Medicaid and Commercial Enrollees,
2010-2014
Michele K. BohmCenters for Disease Control and Prevention
April 3, 2018

#Rx Summit www.NationalRxDrugAbuseSummit.org
Overview
Study Objective Background Data Source and Measures Results Implications
.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Study Objective
Characterize non-fatal heroin overdose (OD) trends among the insured, including healthcare utilization preceding overdose and prior use of prescription opioids, benzodiazepines and buprenorphine in order to inform prevention strategies for the population at risk of heroin OD.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Background

Project POINT-Indiana
“We’re now treating a heroin patient in the ED much as we would treat a heart attack or
stroke patient.” Dr. Charles Miramonti
Local Syringe Services Programs

#Rx Summit www.NationalRxDrugAbuseSummit.org
Health Insurance Coverage U.S. Population
Employer-sponsoredInsurance
Medicaid

#Rx Summit www.NationalRxDrugAbuseSummit.org
Q: Who Pays for Heroin ED Visits and Hospitalizations?
A: 50% Medicaid and Private Insurance
National Inpatient Sample (NIS) and National Emergency Department Sample (NEDS), Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality.
Medicaid26%
Private Insurance
19%Medicare
6%
Uninsured45%
Other4%
2013 ED VISITS HEROIN OVERDOSE
Medicaid30%
Private Insurance
20%Medicare
9%
Uninsured35%
Other6%
2013 HOSPITAL DISCHARGESHEROIN OVERDOSE

#Rx Summit www.NationalRxDrugAbuseSummit.org
Data Source and MeasuresData Source and Measures

#Rx Summit www.NationalRxDrugAbuseSummit.org
Data SourceMarketScan® Medicaid & Commercial Claims
Convenience Sample but strength in size of databases- Commercially-insured: >25% of all U.S. employer-sponsored
healthcare beneficiaries- Medicaid-insured patients: 10-13 de-identified states
Full continuum of care- Inpatient, outpatient, ED, retail pharmacy- ICD-9-CM, CPT, NDC
Analyzed data 2010-2014- Ages 15-64 years

#Rx Summit www.NationalRxDrugAbuseSummit.org
Measures OVERDOSE
- Heroin OD rates by year, payer, gender, age• ICD-9-CM 965.01 (poisoning by heroin) and E850.0
(accidental)- Opioid (other than heroin) OD rates by year and payer
COMORBIDITIES AND HEALTHCARE PRIOR TO OVERDOSE- Non-heroin OD or buprenorphine RX- Any healthcare utilization by setting--office, ED, inpatient (6
months)- Comorbidities per HCUP Clinical Classifications for
diagnoses (6 months)
PRESCRIPTIONS- Opioids, benzodiazepines, buprenorphine (1, 3, 6 months
prior to OD)

#Rx Summit www.NationalRxDrugAbuseSummit.org
Results

#Rx Summit www.NationalRxDrugAbuseSummit.org
Key FindingsHeroin OD Rates, 2010-2014
Gender: Generally higher among males
Age: Distribution varied by payer
Increases: Greatest for females
By 2012, rates among commercial enrollees 15-24 years=Overall rates in Medicaid population
Truven Health Analytics MarketScan®--United States, 2010-2014

#Rx Summit www.NationalRxDrugAbuseSummit.org
Limitations of Study
Continuously enrolled more likely to have chronic conditions ACA Medicaid expansion
- SUD higher among uninsured, expanded Medicaid-eligible - Excluded all new-to-Medicaid enrollees=conservative rates
Variability in coding Not nationally-representative/generalizable to entire U.S.
population. Claims do not capture: Heroin OD without transport to facility,
fatal OD, uninsured, prescriptions paid out-of-pocket

#Rx Summit www.NationalRxDrugAbuseSummit.org
Summary of Results Nonfatal heroin overdose trends, 2010-2014, reflect heroin use
and OD mortality1-2
Commercially-insured account for increasing burden from heroin OD
Multiple medical and mental healthcare needs among insured who overdose on heroin. - Higher opioid prescribing reflects painful comorbidities in
Medicaid - High benzo prescribing and co-prescribing with opioids
reflects mental health issues (2016 FDA Warning on combined use)
Insured patients with impending heroin overdose were not lost to follow-up.
1. Hedegaard, H., Chen, L. H., & Warner, M. (2015). Drug-poisoning deaths involving heroin: United States, 2000-2013. NCHS Data Brief(190), 1-8. 2. Jones, C. M., Logan, J., Gladden, R. M., & Bohm, M. K. (2015). Vital Signs: Demographic and Substance Use Trends Among Heroin Users - United States, 2002-2013. MMWR Morb Mortal Wkly Rep, 64(26), 719-725.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Implications

#Rx Summit www.NationalRxDrugAbuseSummit.org
Young Commercially-Insured Heroin OD rates in line with overall Medicaid population
- Dependents of primary insured3
- Emerging cohort? Office-based settings High OD rates in young commercially-insured, BUT opioid
prescribing lower in commercially-insured - Young people more likely obtain Rx opioids from
friends/family1
- Individuals entering treatment now more frequently reporting heroin as their opioid of initiation as opposed to prescription opioids.2
1. Lipari, R. N., & Hughes, A (2017). How people obtain the prescription pain relievers they misuse. The CBHSQ Report: January 12, 2017. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, Rockville, MD.2. Cicero, T. J., Ellis, M. S., & Kasper, Z. A. (2017). Increased use of heroin as an initiating opioid of abuse. Addict Behav, 74, 63-66. doi:10.1016/j.addbeh.2017.05.0303. The authors analyzed the MarketScan data and found that most enrollees aged 15 to 24 years were dependents of the primary insured member.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Beyond Opioid OD PreventionTreat impending OD as you would a
patient at risk for heart attack.
Opioid Misuse
Neonatal Abstinence Syndrome
Infectious Complications
CDC Guideline for Prescribing Opioids for Chronic Pain
Prescription Drug Monitoring Program (PDMP)
Medication Assisted Treatment (MAT)
Overdose Education and Naloxone Distribution (OEND)
No need to wait for heroin OD to intervene!

Federal funds can support COMPREHENSIVE Syringe Services Programs in certain jurisdictions.
SSPs prevent overdoses by distributing naloxone and teaching people who inject drugs to avoid and reverse overdose.
Third Party Payers: Note that SSPs save healthcare dollars by preventing infectious complications which are expensive to treat.
People who inject drugs should be tested for HIV, viral hepatitis and STDs, and vaccinated against hepatitis B if not immune.

#Rx Summit www.NationalRxDrugAbuseSummit.org
Neonatal Abstinence Syndrome In addition to MAT, ensure
access to family planning and preconception care for womenwho use opioids. - Among women with OUD, 86%
of pregnancies are unintended.1
- CDC recommends healthcare providers support family planning services: preconception services, pregnancy intention screening, and contraceptive counseling.2
1. Heil SH, Jones HE, Arria A, et al. Unintended pregnancy in opioid-abusing women. J Subst Abuse Treat 2011;40:199–202. 2. Gavin L, Moskosky S, Carter M, et al. Providing quality family planning services: recommendations of CDC and the U.S. Office of Population Affairs. MMWR Recomm Rep 2014;63(No. RR-4).3. https://www.drugabuse.gov/related-topics/trends-statistics/infographics/dramatic-increases-in-maternal-opioid-use-neonatal-abstinence-syndrome
3

#Rx Summit www.NationalRxDrugAbuseSummit.org
Opportunities for Pre-Overdose Interventions
Healthcare utilization patterns prior to first heroin overdose signal opportunities for pre-overdose interventions tailored to where patients access care (not necessarily ED).
Analyze more recent, granular data (third-party payer, ACO, etc.) to inform initiatives and innovate.
Integrate care with systematic coordination of medical (pain), social, and psychological health:- Judicious prescribing per CDC Guidelines- PDMP- MAT- Naloxone- Screen and treat HCV, HIV, other infections- SSP- Family planning- Reproductive health- Mental health

#Rx Summit www.NationalRxDrugAbuseSummit.org
Acknowledgments
Lindsey BridwellKun ZhangJon Zibbell
Questions or comments: [email protected]

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Healthcare: Clinical Perspectives
Alexander Y. Walley, MD, MSc
Associate Professor of Medicine and Director of Addiction Medicine Fellowship
Clinical Addiction Research and Education Unit, Boston Medical Center/ Boston University School of Medicine
Medical DirectorOpioid Overdose Prevention Pilot Program, Massachusetts
Department of Public Health

#Rx Summit www.NationalRxDrugAbuseSummit.org
Touchpoints: Identifying people at high risk for overdose and interact with systems before they overdose
People who present for opioid detoxification People have a non-fatal overdose People hospitalized for medical or mental health
conditions related to opioid use People with opioid use disorder who are
incarcerated People who are prescribed opioids for pain

#Rx Summit www.NationalRxDrugAbuseSummit.org
415.6%10.4%10.7%10.8%11.0%11.5%
12.4%12.5%12.8%13.4%
14.6%15.5%
17.1%20.4%20.6%
29.6%31.1%31.6%
33.8%38.8%
Other
Renal
Neurosurgery
Gyn
Heme / Onc
General Surgery
Cards CHF
Family Medicine
Hospitalist
Internal Medicine
Adult discharges with billed substance use code during visitPercentage of annual discharges
Source: Internal BMC admission / billing data; May 2014-June 2015.
▪ Across all adult discharges, 17.5% had a primary or secondary substance use code billed during their hospitalization
▪ Likely undercounts true demand, as substance use is not always coded when it is not primary

#Rx Summit www.NationalRxDrugAbuseSummit.org
0%10%20%30%40%50%60%70%80%90%
100%
-12 -9 -6 -3 0 3 6 9 12
% re
ceiv
ing
med
icatio
n
Months from index overdose
Buprenorphine
Methadone
Naltrexone
Larochelle et al. Presented at CPDD and AMERSA 2017 - Under review

#Rx Summit www.NationalRxDrugAbuseSummit.org
0%
2%
4%
6%
8%
10%
-12 -9 -6 -3 0 3 6 9 12% re
ceiv
ing
med
icatio
n
Months from index overdose
Buprenorphine
Methadone
Naltrexone
Larochelle et al. Presented at CPDD and AMERSA 2017 - Under review
%Months Received (median [IQR])
Any MOUD 30%Buprenorphine 17% 4 [2,8]Methadone 12% 5 [2,9]Naltrexone 6% 1 [1,2]

#Rx Summit www.NationalRxDrugAbuseSummit.org
Opioid and benzodiazepine prescriptions before and after overdose
0%
5%
10%
15%
20%
-12 -9 -6 -3 0 3 6 9 12
% re
ceiv
ing
med
icatio
n
Months from index overdose
Rx OpioidBenzodiazepineAny MOUD
Presented at CPDD and AMERSA 2017 - Study under review
#Rx Summit www.NationalRxDrugAbuseSummit.org
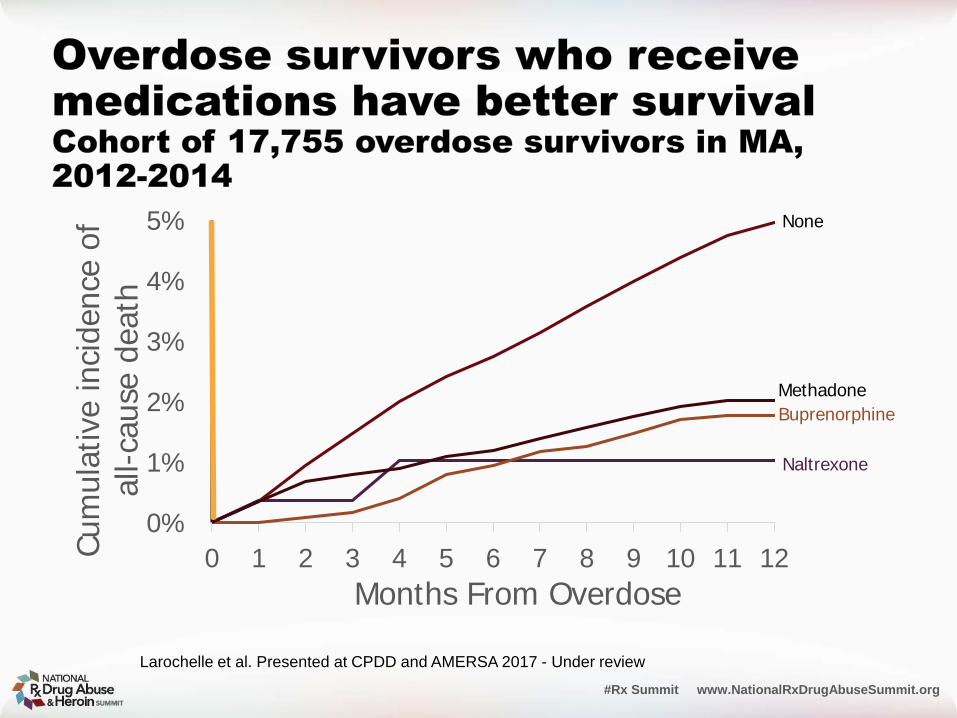
0%
1%
2%
3%
4%
5%
0 1 2 3 4 5 6 7 8 9 10 11 12Cum
ulat
ive in
ciden
ce o
f al
l-cau
se d
eath
Months From Overdose
Naltrexone
None
BuprenorphineMethadone
Larochelle et al. Presented at CPDD and AMERSA 2017 - Under review

#Rx Summit www.NationalRxDrugAbuseSummit.org
Morgan JR, Schackman BR, Leff JA, Linas BP, Walley AY. Injectable naltrexone, oral naltrexone, and buprenorphine utilization and discontinuation among individuals treated for opioid use disorder in a United States commercially insured population. JSAT. 2017 Jul 3.
2010-14 claims database of >200 million commercially insured in US 4-fold-increase in OUD dx
- 0.12% 0.48% BUT, proportion treated
decreased- 25% 16%

#Rx Summit www.NationalRxDrugAbuseSummit.org
Make MAT opt out, instead of opt in- Convert detox programs into MAT induction programs- Continue and initiate MAT for hospitalized/ED patients
with complications of OUD• Especially post-overdose
- Continue and initiate MAT for incarcerated people with OUD
Offer overdose prevention to everyone with risk and their networks- People who are prescribed opioids and benzos- Make overdose prevention part of addiction treatment- Medical and mental health patients who use opioids- Incarcerated
Intervention strategies at the point of care prior to the first heroin overdose
#Rx Summit www.NationalRxDrugAbuseSummit.org
A comprehensive public health response to address overdoses related to IMF 1. Fentanyl should be included on standard toxicology screens 2. Adapt existing harm reduction strategies, such as direct observation of anyone using
illicit opioids, and ensuring bystanders are equipped with naloxone3. Enhanced access and linkage to medication for opioid use disorders
“So, now what they [people selling illicit drugs] are doing is they’re cutting the heroin with the fentanyl to make it stronger. And the dope [heroin] is so strong with the fentanyl in it, that you get the whole dose of the fentanyl at once rather than being time-released [like the patch]. And that’s why people are dying—plain and simple. You know, they [people using illicit drugs] are doing the whole bag [of heroin mixed with fentanyl] and they don’t realize that they can’t handle it; their body can't handle it.” -- Overdose bystander

#Rx Summit www.NationalRxDrugAbuseSummit.org
Go further upstream! Engage people who do not touch systems and integrate
overdose prevention- Syringe service programs- Drug consumption spaces- Integrate HIV, HCV testing outreach with overdose
prevention- Housing First programs that integrate overdose
prevention- Post-overdose public health-public safety outreach- Pre-arrest treatment and harm reduction- Hot-spotting: Public health-public safety surveillance and
rapid response
Intervention strategies at the point of care prior to the first heroin overdose
#Rx Summit www.NationalRxDrugAbuseSummit.org
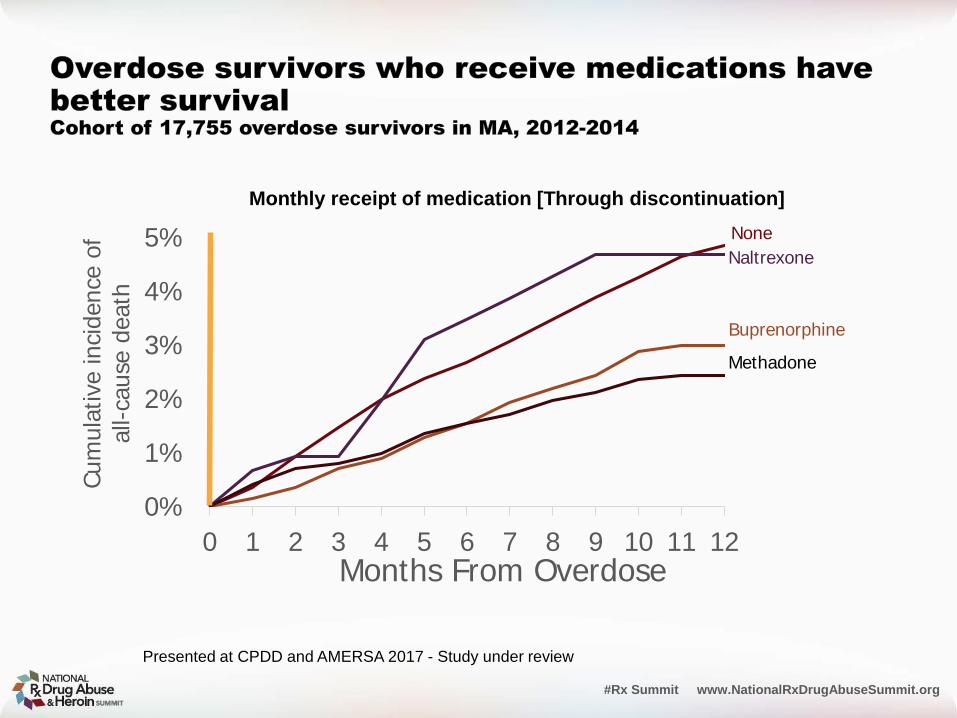
Monthly receipt of medication [Through discontinuation]
0%
1%
2%
3%
4%
5%
0 1 2 3 4 5 6 7 8 9 10 11 12
Cum
ulat
ive in
ciden
ce o
f al
l-cau
se d
eath
Months From Overdose
NaltrexoneNone
Buprenorphine
Methadone
Presented at CPDD and AMERSA 2017 - Study under review

#Rx Summit www.NationalRxDrugAbuseSummit.org
Heroin and Healthcare:Identifying Opportunities for
Intervention Prior to OverdoseMichele K. Bohm, MPH, Health Scientist, Centers for Disease Control and Prevention
Lindsey Bridwell, MPH, CHES, Evaluation Fellow, Opioid Overdose Health Systems Team, Centers for Disease Control and Prevention
Alexander Y. Walley, MD, MSc, Associate Professor of Medicine,Boston University School of Medicine
Third Party Payer Track
Moderator: Amy G. Griffin, JD, Corporate Counsel, Kentucky Employers’ Mutual Insurance

THANK YOU#RxSummit
www.NationalRxDrugAbuseSummit.org



![Heroin maintenance for chronic heroin-dependent individualsharmreductionactioncenter.org/HRAC_DOCUMENTS/ADDICTION AND... · [Intervention Review] Heroin maintenance for chronic heroin-dependent](https://img.dokumen.tips/doc/110x75/5b87383e7f8b9a1a248c3f66/heroin-maintenance-for-chronic-heroin-dependent-individualsharmr-and-intervention.jpg)


























