-
Advisor : dr. Sjaiful Bachri, SpB
Melissa L. Thenata
Fakultas Kedokteran Universitas Tarumanagara
-
Liver Structure
Largest gland in the body
(1.5 Kg)
Under the diaphragm, within
the rib cage in the upper
right quadrant of the
abdomen
-
Liver Structure
4 lobes: major (left and right),
minor (caudate and quadrate)
Ducts: common hepatic, cystic
from gall bladder, common bile
choledochus (join pancreatic
duct at hepatopancreatic
ampulla)
-
Liver Structure
Liver lobules hexagonal structures consisting of hepatocytes
Hepatocytes radiate outward from a central vein
At each of the six corners of a lobule is a portal triad
Liver sinusoids
-
Liver Structure
Hepatocytes produce bile
Bile flows through canals
called bile canaliculi to a
bile duct
Bile ducts leave the liver
via the common hepatic
duct
-
Liver Function
Regulating homeostasis of carbohydrate, lipid and amino
acid metabolism.
Storing nutrients such as glycogen, fats and vitamin B12, A
and K.
Producing and secreting plasma proteins and lipoproteins,
including clotting factors and acute phase proteins.
-
Liver Function
Synthesizing and secreting bile salts for lipid digestion.
Detoxifying and excreting bilirubin, other endogenous waste
products and exogenous metal ions, drugs and toxins
(xenobiotics).
Clearing toxins and infective agents from the portal venous
blood whilst maintain systemic immune tolerance to antigens
in the portal circulation.
-
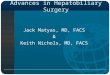
Gall Bladder Structure
Thin-walled green muscular sac
On the inferior surface of the liver
Stores bile that is not immediately needed for digestion
When the muscular wall of the gallbladder contracts bile is
expelled into the bile duct
-
Gall Bladder Structure
-
Gall Bladder Function
Stores 60 mL of bile, released when food containing fat
enters the digestive tract.
The bile, produced in the liver, emulsifies (breaks down)
fats
and neutralizes acids in partly digested food.
-
Biliary Atresia
Obliteration or discontinuity of the extrahepatic biliary
system,
resulting in obstruction to bile flow, in the first few weeks of
life.
Inflammatory process from an unknown cause affects the bile
duct
in the newborn infant.
Destruction of the extrahepatic bile ducts, causing
obstructive
jaundice and liver failure.
Kasai procedure, surgical correction of this abnormality before
8
weeks of age produces the best outcome.
-
Choledochal Cyst
Cystic dilatation of the intra- or extrahepatic ducts is a
rare
condition, usually presenting before the age of 16 years.
Symptoms : cholangitis, pancreatitis, stone formation and
jaundice.
Infants may occasionally present with an abdominal mass.
The cause of this condition is debated.
-
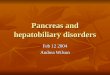
Choledochal Cyst
Cysts are classified according
to their site and shape,
although 80% are fusiform
abnormalities of the
extrahepatic bile duct. Type
II cysts are extremely rare.
-
Choledochal Cyst
Treated by surgical excision
of the cyst with the
formation of a roux-en-Y
anastomosis to the biliary
duct.
-
Hepatobiliary Trauma
The liver is the most commonly injured solid abdominal
organ,
despite its relative protected location.
Treatment of traumatic liver injuries is based on patient
physiology, mechanism and degree of injury, associated
abdominal and extra-abdominal injuries and local expertise.
-
Hepatobiliary Trauma
Liver Organ Injury Scale
Grade Description
I Hematoma Subcapsular,
-
Hepatobiliary Trauma
Liver Organ Injury Scale
Grade Description
IV Hematoma Parenchymal disruption involving 25% - 75% of
hepatic lobe or 1-3 Couinaud segments within a single lobe
V Laceration Parenchymal disruption involving >75% of hepatic
lobe >3 Couinaud segments within a single lobe
Vascular Juxtahepatic venous injuries; ie. Retrohepatic vena
cava/central major hepatic vein
VI Hepatic avulsion
-
Management of Hepatic Trauma
-
Gall Bladder Cancer
Highly aggressive malignancy, usually presents at an
advanced,
incurable stage, 5th most common gastrointestinal tumor
The median survival is less than 6 months after diagnosis
Women : Men = 2 6 : 1
The incidence steadily increases with age
Risk factor : obesity, a high-carbohydrate diet, smoking,
and
alcohol use
-
Gall Bladder Cancer
Gall bladder cancer arises in the setting of chronic
inflammation. In the vast majority of patients (>75%),
the
source of this chronic inflammation is cholesterol
gallstones.
10-25% is caused by calcification of the gallbladder
(porcelain
gallbladder)
Most common type of gallbladder cancer is adenocarcinoma.
Gallbladder cancer can spread by direct invasion through the
gallbladder wall into the liver or peritoneal cavity.
-
Gall Bladder Cancer
The symptoms of gallbladder cancer overlap with the
symptoms of gallstones and biliary colic. Abdominal pain may
be of a more diffuse and persistent nature than the classic
right upper quadrant pain of gallstone disease.
Jaundice, anorexia, and weight loss often indicate more
advanced disease.
-
Gall Bladder Cancer
Table 2. Summary of the Tumor-Node-Metastasis (TNM) Staging
System*
Stage Description
1
2
3
4A
4B
Mucosal or muscular invasion (T1N0M0)
Perimuscular-tissue invasion (T2N0M0)
Transmural invasion, liver invasion < 2 cm; lymph node
metastasis to
hepatoduodenal ligament (T3N0M0, T13 N1M0)
Liver invasion > 2 cm (T4N0M0, T4N1M0)
Distant nodal (outside porta hepatis) or hematogenous
metastasis
(TxN2M0, TxNxM1)
-
Gall Bladder Cancer
The work-up for right-upper-quadrant pain or biliary colic
generally starts with an ultrasound examination of the
gallbladder.
Laboratory tests should include liver function tests and
hematocrit. Advanced cases may demonstrate anemia and
elevated alkaline phosphatase and bilirubin.
Tumor markers, CEA and CA 19-9, may be of help and should
be considered if gallbladder cancer is suspected.
-
Gall Bladder Cancer
Further radiologic work-up such as CT-scan, MRI, or needle
biopsy are indicated if gallbladder cancer is suspected.
The most common and most effective treatment is surgical
removal of the gallbladder (cholecystectomy) with part of
liver
and lymph node dissection.
Chemotherapy has not shown significant activity in
gallbladder
carcinoma. Typically, 5-fluorouracil (5-FU) has been used
with
response rates of 10-24% in advanced disease.
-
Gall Bladder Cancer
Gemcitabine has shown activity in gallbladder cancer. There
is
an increased response rate with gemcitabine combination with
cisplatinum and capecitabine.
Currently, no clearly defined standard exists for
chemotherapy
in gallbladder cancer. Patients should be encouraged to
participate in clinical trials.
-
Cholangiocarcinoma
Cholangiocarcinomas are malignancies of the biliary duct
system
that may originate in the liver and extrahepatic bile ducts,
which
terminate at the ampulla of Vater.
The etiology of most bile duct cancers remains undetermined.
However, one of the most commonly recognized risk factors is
primary sclerosing cholangitis.
Cholangiocarcinoma arises from the intrahepatic or
extrahepatic
biliary epithelium. More than 90% are adenocarcinomas.
-
Cholangiocarcinoma
Cholangiocarcinomas tend to grow slowly and to infiltrate
the
walls of the ducts, dissecting along tissue planes.
Local extension occurs into the liver, porta hepatis, and
regional
lymph nodes of the celiac and pancreaticoduodenal chains.
Symptoms of cholangiocarcinoma include jaundice,
clay-colored
stools, bilirubinuria (dark urine), pruritus, weight loss,
and
abdominal pain.
-
Cholangiocarcinoma
The diagnosis and staging of cholangiocarcinoma require a
multimodality approach involving laboratory, radiologic,
endoscopic, and pathologic analysis.
The most studied serum tumor markers are the CA 19-9, is
currently the most commonly used tumor marker for
cholangiocarcinoma.
Surgical resection with curative intent is the treatment of
choice for extrahepatic cholangiocarcinoma.
-
Gallstones
Two major types of gallstones: cholesterol and
pigment stones. Cholesterol gallstones contain50%
cholesterol monohydrate. Pigment stones have 20%
cholesterol and are composed primarily of calcium
bilirubinate.
Predisposing factors include demographic/genetics,
obesity, weight loss, female sex hormones, age, ileal
disease, pregnancy, type IV hyperlipidemia, and
cirrhosis.
-
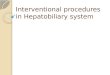
Gallstones
Many gallstones are
silent. Symptoms occur
when stones produce
inflammation or
obstruction of the cystic
or common bile ducts.
-
Gallstones
Major symptoms: (1) biliary colica severe steady ache in the
RUQ or epigastrium that begins suddenly; often occurs 3090
min after meals, lasts for several hours, and occasionally
radiates to the right scapula or back; (2) nausea, vomiting.
Physical exam may be normal or show epigastric or RUQ
tenderness.
Mild and transient elevations in bilirubin [85 mol/L (5
mg/dL)]
accompany biliary colic.
-
Gallstones
Only 10% of cholesterol gallstones are
radiopaque. USG is best diagnostic test.
Elective cholecystectomy should be
reserved for: (1) symptomatic patients;
(2) persons with previous complications
of cholelithiasis; and (3) presence of an
underlying condition predisposing to an
increased risk of complications (calcified
or porcelain gallbladder).
-
Gallstones
Patients with gallstones 3 cm or with an anomalous
gallbladder
containing stones should be considered for surgery.
Laparoscopic cholecystectomy is minimally invasive and is
the
procedure of choice for most patients undergoing elective
cholecystectomy.
Oral dissolution agents (ursodeoxycholic acid) partially or
completely dissolve small radiolucent stones in 50% of
selected
pts within 624 months.
-
Gallstones
Extracorporeal shockwave lithotripsy followed by medical
litholytic therapy is effective in selected patients with
solitary
radiolucent gallstones. Because of the frequency of stone
recurrence and the effectiveness of laparoscopic surgery,
the
role of oral dissolution therapy and lithotripsy has been
reduced to selected patients who are not candidates for
elective cholecystectomy.
-
Acute Cholecystitis
Acute inflammation of the gallbladder usually caused by
cystic
duct obstruction by an impacted stone.
90% calculous; 10% acalculous.
Acalculous cholecystitis associated with higher complication
rate
and associated with acute illness (i.e., burns, trauma,
major
surgery), fasting, hyperalimentation leading to gallbladder
stasis,
vasculitis, carcinoma of gallbladder or common bile duct,
some
gallbladder infections but in > 50% of cases an
underlying
explanation is not found.
-
Acute Cholecystitis
Signs and symptoms :
Attack of bilary colic (RUQ or epigastric pain), progressively
worsens
Nausea, vomiting, anorexia
Fever
Examination typically reveals RUQ tenderness
Palpable RUQ mass found in 20% of patients
Murphys sign is present when deep inspiration or cough
during
palpation of the RUQ produces increased pain or inspiratory
arrest.
-
Acute Cholecystitis
Laboratory : Mild leukocytosis; serum bilirubin, alkaline
phosphatase, and AST may be mildly elevated.
Imaging : Ultrasonography is useful for demonstrating
gallstones and occasionally a phlegmonous mass surrounding
the gallbladder. Radionuclide scans may identify cystic duct
obstruction.
-
Acute Cholecystitis
No oral intake, nasogastric suction, IV fluids and
electrolytes,
analgesia (meperidine or NSAIDS), and antibiotics
(ureidopenicillins, ampicillin sulbactam, third-generation
cephalosporins; anaerobic coverage should be added if
gangrenous or emphysematous cholecystitis is suspected;
consider combination with aminoglycosides in diabetic
patient
or others with signs of gram-negative sepsis).
-
Acute Cholecystitis
Acute symptoms will resolve in 70% of patient.
Optimal timing of surgery depends on patient stabilization
and
should be performed as soon as feasible.
Urgent cholecystectomy is appropriate in most patients with
a
suspected or confirmed complication.
Delayed surgery is reserved for patients with high risk of
emergent surgery and where the diagnosis is in doubt.
-
Chronic Cholecystitis
Chronic inflammation of the gallbladder; almost always
associated with gallstones. Results from repeated
acute/subacute cholecystitis or prolonged mechanical
irritation of gallbladder wall.
May be asymptomatic for years, may progress to symptomatic
gallbladder disease or to acute cholecystitis, or present
with
complications.
-
Chronic Cholecystitis
Laboratory tests are usually normal.
Ultrasonography preferred; usually shows gallstones within a
contracted gallbladder.
Surgery indicated if patient is symptomatic.
-
Liver Infections Pyogenic Abscess
Pyogenic or bacterial abscess may be caused by several
factors.
Infections may arise from the biliary tract, portal vein and
hepatic
artery or by direct extension.
Symptoms : pyrexia and rigours associated with right upper
quadrant pain, general malaise and anorexia.
Examination may reveal tender hepatomegaly. A pleural
effusion
may be present. Occasionally, hypotension and cardiovascular
collapse may be the presenting symptoms.
-
Liver Infections Pyogenic Abscess
Laboratory tests : hyperbilirubinemia, raised alkaline
phosphatase and transaminase levels, blood cultures are
frequently positive, leucocytosis.
USG / CT scan abdomen : to determine the size,
characteristics,
number and anatomical location of the liver abscesses.
Chest X-ray : elevated hemidiaphragm or a pleural effusion.
ERCP or a colonoscopy : to determine the cause of pyogenic
liver abscesses.
-
Liver Infections Pyogenic Abscess
Treatment :
Analgesics and attention to adequate nutrition and hydration
Antimicrobial therapy
Drainage of the abscess
Frequent clinical, biochemical, microbial and radiological
follow-up is required to assess progress and detect relapses
-
Liver Infections Amoebic Liver Abscess
Amoebic infestation is caused by the organism Entamoeba
histolytica.
Transmission is by passage of cysts in the stool, the cysts
then
being ingested orally as a result of poor hygienic
practices.
Risk factors include malnutrition, depressed immunity and
low
socioeconomic status.
Complications of amoebic abscess include rupture into the
peritoneal cavity or hollow viscus such as colon or stomach.
-
Liver Infections Amoebic Liver Abscess
The onset of the disease may be sudden or gradual.
The most common symptoms : right upper quadrant pain,
general malaise, weight loss, pyrexia and sweating.
Signs : tender hepatomegaly and, occasionally, jaundice.
Full blood examination : leukocytosis and eosinophilia.
Amoebic serology and stool cultures are usually positive.
The antibiotic of choice is metronidazole.
-
Benign Liver Tumors - Adenoma
Hepatocellular adenomas occur most commonly in women in
the third or fourth decades who take birth control pills.
The major concern is their tendency to rupture with massive
haemorrhage; therefore, this condition must be considered in
young women presenting with abdominal pain, signs of
hypovolaemic shock and features of haemoperitoneum.
After resuscitation, the treatment is resection of the
affected
liver segment.
-
Benign Liver Tumors Focal Nodular Hyperplasia
Focal nodular hyperplasia (FNH) is not a true neoplasm but
is
probably due to a fibrous reaction to vessel ingrowth.
It is most common in young women.
It appears as a nodular firm vascular mass.
There may be symptoms of right upper quadrant pain.
No specific treatment is required and the main purpose of
management is to distinguish the lesion from neoplasms.
-
Hepatocellular Cancer (Hepatoma)
Worldwides most common tumor.
Male : female = 4 : 1; tumor usually develops in cirrhotic
liver
in persons in fifth or sixth decade.
High incidence in Asia and Africa is related to etiologic
relationship between this cancer and hepatitis B and C
infections.
-
Hepatocellular Cancer (Hepatoma)
Aflatoxin exposure contributes to etiology and leaves a
molecular
signature, a mutation in codon 249 of the gene for p53.
Surgical resection or liver transplantation is therapeutic
option but
rarely successful.
Hepatitis B vaccine prevents the disease. Interferon may
prevent
liver cancer in persons with chronic active hepatitis C disease
and
possibly in those with hepatitis B.
Ribivarin / interferon (IFN) is most effective treatment of
chronic
hepatitis C.