Embed Size (px)
Citation preview

Hepatic CirrhosisHepatic Cirrhosis
(肝硬化)(肝硬化)
Yu BaopingYu Baoping

IntroductionIntroduction
CIRRHOSISCIRRHOSIS Term was 1st coined by Laennec in 1826Term was 1st coined by Laennec in 1826 Many definitions but common theme is injury, repair, reMany definitions but common theme is injury, repair, re
generation and scarringgeneration and scarring NOT a localized process; involves entire liverNOT a localized process; involves entire liver Primary histologic features:Primary histologic features:
1.1. Marked fibrosisMarked fibrosis2.2. Destruction of vascular & biliary elementsDestruction of vascular & biliary elements3.3. RegenerationRegeneration4.4. Nodule formationNodule formation

DefinitionDefinition
Cirrhosis is a pathological diagnosis. It is Cirrhosis is a pathological diagnosis. It is characterized by widespread fibrosis with characterized by widespread fibrosis with nodular regeneration. Its presence implies nodular regeneration. Its presence implies previous or continuing hepatic cell damageprevious or continuing hepatic cell damage



Aetiology Aetiology andand Pathogenesis Pathogenesis

Etiologic classification of cirrhosisEtiologic classification of cirrhosis
AlcoholAlcohol ( (>70%)>70%) Chronic infectionsChronic infections
hepatitis Chepatitis C, B, B, B, B++DD
brucellosis, syphilisbrucellosis, syphilis Chr. biliary obstructionChr. biliary obstruction
PBC, PSC, stricture,PBC, PSC, stricture,
sstonestones,, cystic fibrosis, cystic fibrosis, cong. cong.b. atresia,b. atresia, ~~cystscysts
AutoimmuneAutoimmune
CardiovascularCardiovascular
heart failure, pericarditis,heart failure, pericarditis,
Budd-Chiary-syBudd-Chiary-sy Metabolic/genetic errorsMetabolic/genetic errors
Fe, Cu, αFe, Cu, α11-AT, lipids, -AT, lipids, Drugs and chemicalsDrugs and chemicals NASHNASH CryptogenicCryptogenic CombinedCombined

Pathogenesis:Pathogenesis: Diffuse liver injury leading to necrosis.Diffuse liver injury leading to necrosis.
(Alcohol, virus, drugs, toxins, genetic etc.)(Alcohol, virus, drugs, toxins, genetic etc.) Chronic inflammation & healing Chronic inflammation & healing (hepatitis).(hepatitis). Bridging fibrosis – loss of architecture.Bridging fibrosis – loss of architecture. Regeneration Regeneration nodules. nodules. Obstruction to blood flow & shunts.Obstruction to blood flow & shunts. Portal hypertension Portal hypertension spleen, varices spleen, varices Liver failure – Debilitation, Jaundice, Ascitis, edema, bleediLiver failure – Debilitation, Jaundice, Ascitis, edema, bleedi
ng, jaundice.ng, jaundice. Hormone imbalance – spider nevi, testes atrophy etc..Hormone imbalance – spider nevi, testes atrophy etc..
Pathology Pathology and and PathophysiologyPathophysiology

Pathology Pathology (( liverliver ))

Classification of CirrhosisClassification of Cirrhosis
WHO divided cirrhosis into 3 categories baseWHO divided cirrhosis into 3 categories based on morphological characteristics of the hepad on morphological characteristics of the hepatic nodulestic nodules
1.1. MicronodularMicronodular
2.2. MacronodularMacronodular
3.3. MixedMixed

Micronodular CirrhosisMicronodular Cirrhosis
Nodules are <3 mm in diameterNodules are <3 mm in diameter Relatively uniform in sizeRelatively uniform in size Distributed throughout the liverDistributed throughout the liver Rarely contain portal tracts or efferent veinsRarely contain portal tracts or efferent veins Liver is of uniform size or mildly enlargedLiver is of uniform size or mildly enlarged Reflect relatively early diseaseReflect relatively early disease

Micronodular cirrhosis

Macronodular & Mixed CirrhosisMacronodular & Mixed Cirrhosis
Nodules are >3 mm in diameter and vary considerably Nodules are >3 mm in diameter and vary considerably in sizein size
Usually contain portal tracts and efferent veinsUsually contain portal tracts and efferent veins Liver is usually normal or reduced in sizeLiver is usually normal or reduced in size Mixed pattern if both type of nodules are present in Mixed pattern if both type of nodules are present in
equal proportionsequal proportions

Macronodular cirrhosis

CirrhosisCirrhosis
Fibrosis
Regenerating Nodule

Pathology Pathology (( splenomegalysplenomegaly
))

Pathology Pathology (( others )) gastrointestinal tract
varicose veins ,, hemorrhage , congestion
Kidney
glomerulonephritis
Endocrine muscular atrophy , degeneration ( testis , ovary , thyroid , adrenal cortex )

Cirrhosis: PathophysiologyCirrhosis: Pathophysiology
Primary event is injury to hepatocellular elemenPrimary event is injury to hepatocellular elementsts
Triggering inflammatory response with cytokine Triggering inflammatory response with cytokine release-toxic substancesrelease-toxic substances
Destruction of hepatocytes, bile duct cells, vascDestruction of hepatocytes, bile duct cells, vascular endothelial cellsular endothelial cells
Repair thru cellular proliferation and regeneratioRepair thru cellular proliferation and regenerationn
Formation of fibrous scarFormation of fibrous scar

Cirrhosis: PathophysiologyCirrhosis: Pathophysiology
Stellate cell is activated in response to injury anStellate cell is activated in response to injury and lead to expression of fibril-forming collagend lead to expression of fibril-forming collagen
Above process is also influenced by Kupffer cellAbove process is also influenced by Kupffer cells which activate stellate cells by eliciting producs which activate stellate cells by eliciting production of cytokinestion of cytokines
Sinusoidal fenestrations are obliterated becausSinusoidal fenestrations are obliterated because of collagene of collagen

Cirrhosis: PathophysiologyCirrhosis: Pathophysiology
Prevents normal flow of nutrients to hepatocytePrevents normal flow of nutrients to hepatocytes and increases vascular resistances and increases vascular resistance
Initially, fibrosis may be reversible if inciting eveInitially, fibrosis may be reversible if inciting events are removednts are removed
With sustained injury, process of fibrosis becomWith sustained injury, process of fibrosis becomes irreversible and leads to cirrhosis es irreversible and leads to cirrhosis

PathophysiologyPathophysiologyProtal hypertensionProtal hypertension
AscitesAscites
endocrineendocrine
respiratory systemrespiratory system hepatic hydrothoraxhepatic hydrothorax
hepatopulmonary syndromehepatopulmonary syndrome
the urinary system : hepatorenal syndrom, HRSthe urinary system : hepatorenal syndrom, HRS
hematological systemhematological system
nervous system : HEnervous system : HE

Portal Hypertension (PH)Portal Hypertension (PH)
Portal vein pressure above the normal range of Portal vein pressure above the normal range of 5 to 8 mm Hg5 to 8 mm Hg
Portal vein - Hepatic vein pressure gradient grePortal vein - Hepatic vein pressure gradient greater than 5 mm Hg (>12 clinically significant)ater than 5 mm Hg (>12 clinically significant)
Represents an increase of the hydrostatic pressRepresents an increase of the hydrostatic pressure within the portal vein or its tributariesure within the portal vein or its tributaries

Pathophysiology of PHPathophysiology of PH
Cirrhosis results in scarring (perisinusoidal deposition of Cirrhosis results in scarring (perisinusoidal deposition of collagen)collagen)
Scarring narrows and compresses hepatic sinusoids Scarring narrows and compresses hepatic sinusoids (fibrosis)(fibrosis)
Portal vein thrombosis, or hepatic venous obstruction Portal vein thrombosis, or hepatic venous obstruction also cause PH by increasing the resistance to portal also cause PH by increasing the resistance to portal blood flowblood flow
Progressive increase in resistance to portal venous Progressive increase in resistance to portal venous blood flow results in PHblood flow results in PH
Pathophysiology of PHPathophysiology of PH
As pressure increases, blood flow decreases and the As pressure increases, blood flow decreases and the pressure in the portal system is transmitted to its pressure in the portal system is transmitted to its branchesbranches
Results in dilation of venous tributariesResults in dilation of venous tributaries Increased blood flow through collaterals and Increased blood flow through collaterals and
subsequently increased venous return cause an subsequently increased venous return cause an increase in cardiac output and total blood volume and a increase in cardiac output and total blood volume and a decrease in systemic vascular resistancedecrease in systemic vascular resistance
With progression of disease, blood pressure usually With progression of disease, blood pressure usually fallsfalls

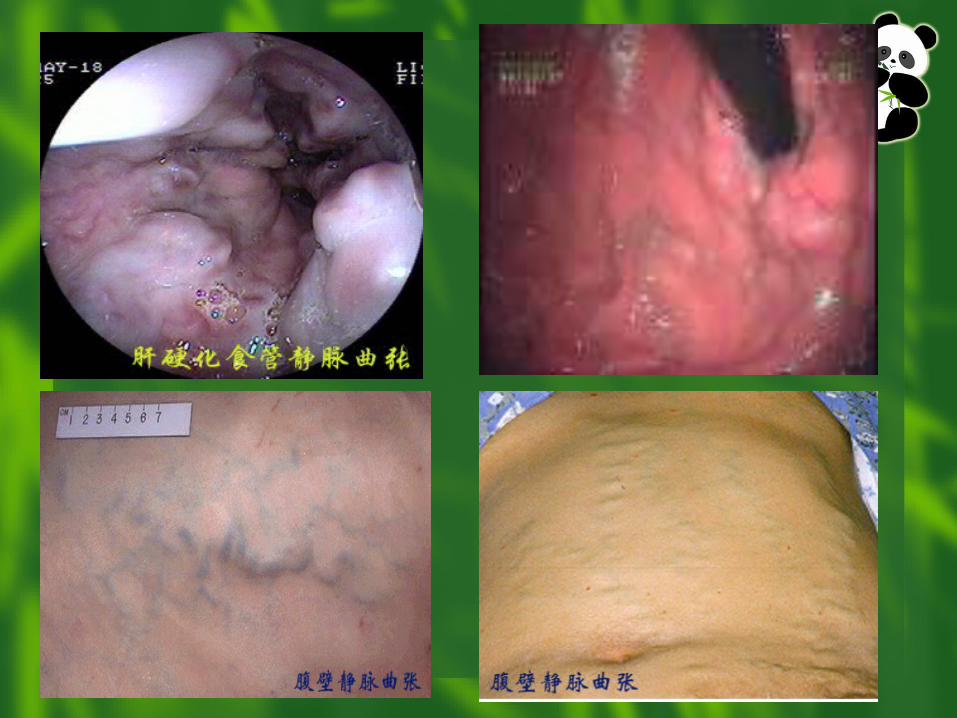
Portal Vein CollateralsPortal Vein Collaterals
Coronary vein and short gastric veins -> veins of the Coronary vein and short gastric veins -> veins of the lesser curve of the stomach and the esophagus, lesser curve of the stomach and the esophagus, leading to the formation of varicesleading to the formation of varices
Inferior mesenteric vein -> rectal branches which, when Inferior mesenteric vein -> rectal branches which, when distended, form hemorrhoidsdistended, form hemorrhoids
Umbilical vein ->epigastric venous system around the Umbilical vein ->epigastric venous system around the umbilicus (caput medusae)umbilicus (caput medusae)
Retroperitoneal collaterals ->gastrointestinal veins Retroperitoneal collaterals ->gastrointestinal veins through the bare areas of the liverthrough the bare areas of the liver


AscitesAscites Sodium and water retention occur due to renin-angioteSodium and water retention occur due to renin-angiote
nsin release secondary to arterial vasodilatation, causensin release secondary to arterial vasodilatation, caused by vasoactive substances such as nitric oxided by vasoactive substances such as nitric oxide
Portal hypertension per se causes fluid to accumulate iPortal hypertension per se causes fluid to accumulate in the peritoneal cavity due to increased hydrostatic pren the peritoneal cavity due to increased hydrostatic pressure, hence further reduces intravascular volume and ssure, hence further reduces intravascular volume and stimulates sodium and water retention via aldosterone.stimulates sodium and water retention via aldosterone.
Low albumin in plasmaLow albumin in plasma

Clinical presentationClinical presentation

Clinical presentationClinical presentation
There may be no abnormal clinical oThere may be no abnormal clinical or biochemical features of liver diseasr biochemical features of liver disease in initial timese in initial times
Features of hepatocellular failure, poFeatures of hepatocellular failure, portal hypertension, or both may appertal hypertension, or both may appear in advanced times.ar in advanced times.

CirrhosisCirrhosisClinical Clinical
FeaturesFeatures

Symptoms of advanced cirrhosisSymptoms of advanced cirrhosis Fatique, weaknessFatique, weakness Nausea, vomiting and Nausea, vomiting and
loss of appetiteloss of appetite Weight loss, muscle Weight loss, muscle
wastingwasting Jaundice, dark urineJaundice, dark urine Spider naevi, caput Spider naevi, caput
MedusaeMedusae Bloody, black stools Bloody, black stools
or unusually light-or unusually light-colored stoolscolored stools
Vomiting of bloodVomiting of blood
Abdominal swellingAbdominal swelling Swollen feet or legs Swollen feet or legs Liver Liver palmspalms GynecomastiaGynecomastia Loss of sex driveLoss of sex drive Menstrual changes in Menstrual changes in
women women Generalized itchingGeneralized itching Sleep disturbances, Sleep disturbances,
confusion,desorientatconfusion,desorientation,ion,tremor, asterixistremor, asterixis

Clinical FeaturesClinical Features
Hepatocellular failure.Hepatocellular failure. Malnutrition, low albumin & clotting factors, Malnutrition, low albumin & clotting factors,
bleeding.bleeding. Hepatic encephalopathy.Hepatic encephalopathy.
Portal hypertension.Portal hypertension. Ascites, Porta systemic shunts, varices, Ascites, Porta systemic shunts, varices,
splenomegaly.splenomegaly.
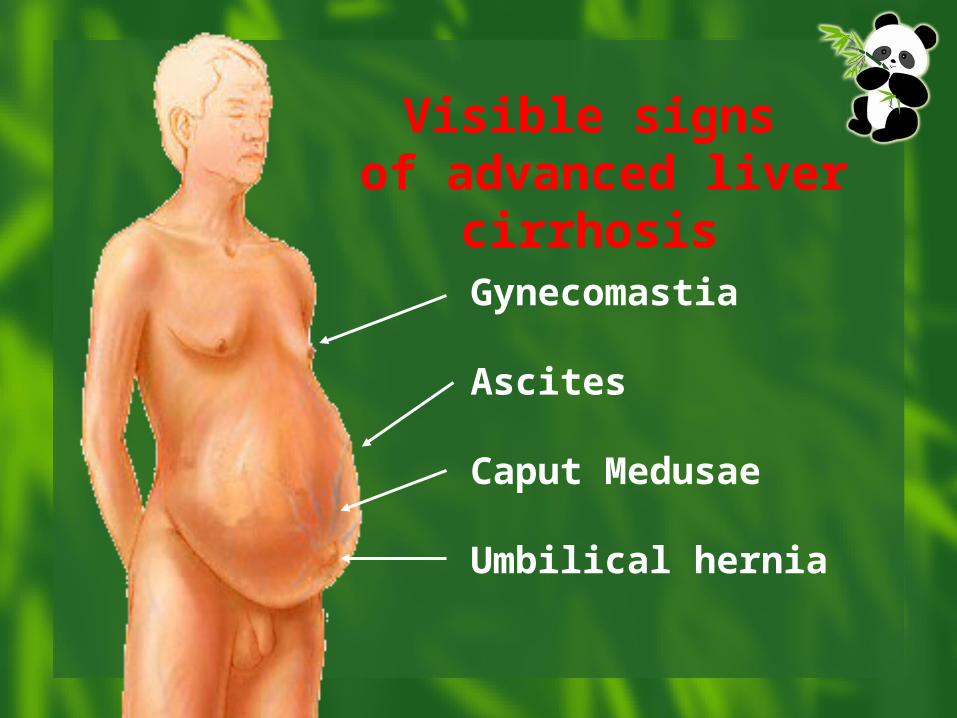
Gynecomastia
Ascites
Caput Medusae
Umbilical hernia
Visible signs of advanced liver
cirrhosis



ComplicationsComplications

ComplicationsComplications
Upper gastrointestinal hemorrhageUpper gastrointestinal hemorrhage Hepatic encephalopathyHepatic encephalopathy InfectionInfection Hepatorenal syndromeHepatorenal syndrome Hepatopulmonary SyndromeHepatopulmonary Syndrome Primary carcinoma of the liverPrimary carcinoma of the liver Disturbance of Disturbance of electrolyteelectrolyte and acid-base and acid-base
balancebalance

Laboratory tests Laboratory tests and investigations and investigations

laboratory tests and investigations
Blood-RTBlood-RT anaemiaanaemia ;; hyperspleniahypersplenia:WBC :WBC ,, PltPlt Urine-RTUrine-RT
urine bilirubinurine bilirubin ,, urobilinogenurobilinogen ;; sometimsometimes es albumenalbumen ,, haematuriahaematuria
Stool-RTStool-RT melenamelena

laboratory tests and investigations
liver function tests Compensation normal or abnormal slightly Decompensation transaminase transaminase : : ALT AST ALT AST cholesterolcholesterol albumin and globulinalbumin and globulin prothrombin timeprothrombin time bilirubinbilirubin P P, and so onⅢP P, and so onⅢQuantitation- liver function tests IGG

laboratory tests and investigations
Biochemistry can be surprisingly normal but some Biochemistry can be surprisingly normal but some abnormality will often be present with slightly raisabnormality will often be present with slightly raised transaminases and alkaline phosphatases. In seed transaminases and alkaline phosphatases. In severe cases, all live enzymes will be abnormal. Low vere cases, all live enzymes will be abnormal. Low sodium and albumin are also seen. sodium and albumin are also seen.
Coagulopathy is a very sensitive indicator of liver Coagulopathy is a very sensitive indicator of liver dysfunction and is reflected in the prolonged prothdysfunction and is reflected in the prolonged prothrombin time.rombin time.

laboratory tests and investigations
immunologic function test
AFP
virus hepatitis markers
antinuclear antibody, ANA non-specificity
antismooth muscle antibody autoantibody
anti-mitochondrial antibody

laboratory tests and investigations
Imaging examinationImaging examination Barium mealBarium meal
CT or MRICT or MRI
Ultrasound Ultrasound demonstrates fatty change, size, and demonstrates fatty change, size, and
fibrosis as well as hepatocellular carcinomafibrosis as well as hepatocellular carcinoma

laboratory tests and investigations

laboratory tests and investigations
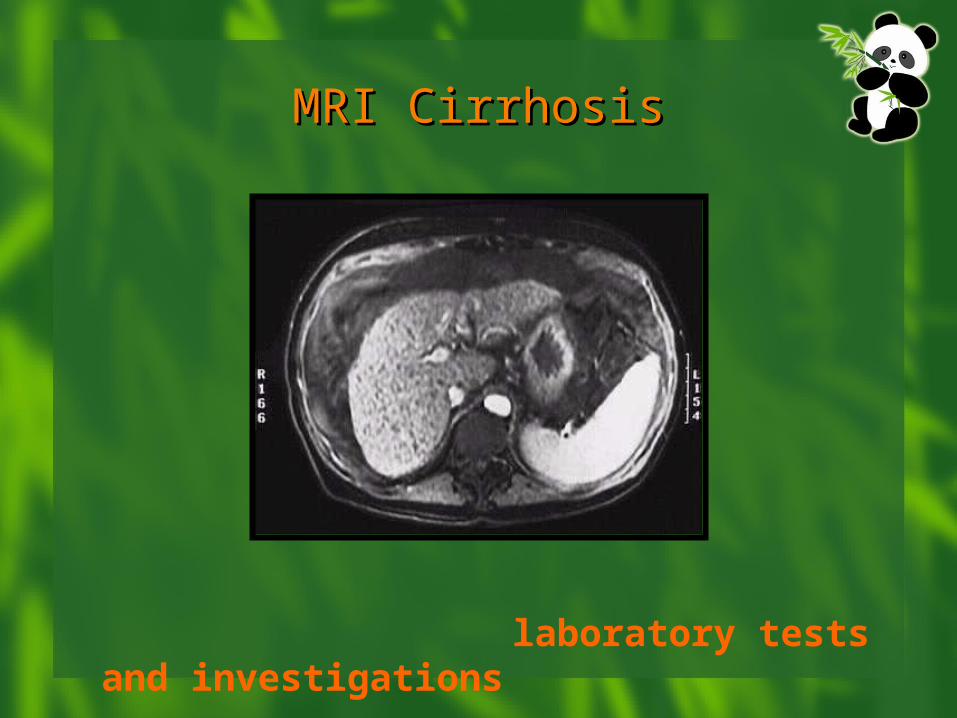
MRI CirrhosisMRI Cirrhosis
laboratory tests and investigations

laboratory tests and investigations
Special testSpecial test Endoscope Biopsy Laparoscope Hydroperitoneum test Measure the Pressure of Portal Vein


Diagnosis and Diagnosis and differential differential
diagnosisdiagnosis

Diagnosis of liver cirrhosisDiagnosis of liver cirrhosis
The gold standard: liver biopsy histologyThe gold standard: liver biopsy histology
Diffuse, chronic liver diseaseDiffuse, chronic liver disease
(hystory, physical, laboratory and US finding(hystory, physical, laboratory and US finding
s) s)
with evidences of portal hypertensionwith evidences of portal hypertension
(oesophageal varices on gastroscopy; dilate(oesophageal varices on gastroscopy; dilate
d portal vein and its branches by US)d portal vein and its branches by US)

Child-Pugh’s classificationChild-Pugh’s classification
CategoriesCategoriesClassification PointsClassification Points
11 22 33
EncephalopathyEncephalopathy NoneNone Grade I & IIGrade I & II Grade III & IVGrade III & IV
AscitesAscites AbsentAbsent Slight-moderateSlight-moderate TenseTense
Bilirubin (mg/dl)Bilirubin (mg/dl) <2 (4)<2 (4) 2-3 (4-10)2-3 (4-10) >3 (>10)>3 (>10)
Albumin (g/dl)Albumin (g/dl) >3.5>3.5 2.8-3.52.8-3.5 <2.8<2.8
Prothrombin TimeProthrombin Time 1-41-4 4-64-6 >6>6
Grade A: 5-6 Grade B: 7-9 Grade C: 10-15

Differential diagnosis
Liver diseasesLiver diseases chronic hepatitischronic hepatitis ;; primary carcinoma of the liverprimary carcinoma of the liver ;; scsc
histosomiasishistosomiasis ;; clonorchiasis sinensisclonorchiasis sinensis ;; hepatic hydatihepatic hydatidosisdosis ;; hemopathyhemopathy
Ascites and abdomen enlargedAscites and abdomen enlarged tuberculous peritonitistuberculous peritonitis ;; constrictive pericardiumconstrictive pericardium ; ; cc
hronic glomerulonephritishronic glomerulonephritis ;; ovarian cystsovarian cysts ComplicationsComplications Upper gastrointestinal hemorrhageUpper gastrointestinal hemorrhage ;; InfectionInfection ;; HepHep
atic encephalopathyatic encephalopathy ;; Hepatorenal syndromeHepatorenal syndrome ;; HepatHepatopulmonary Syndromeopulmonary Syndrome ; ; Primary carcinoma of the Primary carcinoma of the liverliver

TTreatmentreatment

Treatment of liver cirrhosisTreatment of liver cirrhosis
Removal of the etiological factorsRemoval of the etiological factors
can stop or delay further progressioncan stop or delay further progression
may lead to regressionmay lead to regression
may reduce complicationsmay reduce complications
Prevention and treatment and of coPrevention and treatment and of co
mplicationsmplications

Cirrhotic ascites Cirrhotic ascites RestRest Diet TreatmentTreatment::
bed rest, salt restriction, bed rest, salt restriction, Water immersion Water immersion diuretics:diuretics: spironolactone, furosemide; under spironolactone, furosemide; under
regular check-up (body wt, electrolyites, renal function)regular check-up (body wt, electrolyites, renal function)
Refractory ascites:Refractory ascites: large-volume paracentesislarge-volume paracentesis
TIPSTIPS peritoneovenous shuntingperitoneovenous shunting

ComplicationsComplications Spontaneos bacterial peritonitis (SBP): Spontaneos bacterial peritonitis (SBP): fever, sepsis, hyfever, sepsis, hy
potension, fast deteoriation of liver function, azotaemia, enpotension, fast deteoriation of liver function, azotaemia, encephalopathy, deathcephalopathy, deathDg.:Dg.: PMN count in the ascites > 250/μl; culture PMN count in the ascites > 250/μl; culture
Th.:Th.: antibiotics; antibiotics; paracentesisparacentesis Hepatorenal syndrome: Hepatorenal syndrome: renal failure with severe liver diserenal failure with severe liver dise
ase without an intrinsic abnormality of the kidneyase without an intrinsic abnormality of the kidneyCause: reduction in RBF, GFR (vasoconstrictors!)Cause: reduction in RBF, GFR (vasoconstrictors!)Dg.:Dg.: urine Na < urine Na < 10 mM, oliguria without volume depletion 10 mM, oliguria without volume depletion Th.:Th.: prevention of hypovolemia, hypotension prevention of hypovolemia, hypotensionterlipressin;terlipressin; TIPSTIPS
Prognosis:Prognosis: lethal if the liver disease is untreatable lethal if the liver disease is untreatable

Bleeding oesophageal and gasBleeding oesophageal and gastric varicestric varices
Features:Features: hematemesis, melena, shockhematemesis, melena, shock
Dg. and treatment:Dg. and treatment: stabilizing BP, replacing fstabilizing BP, replacing f
luid and blood, somatostatinluid and blood, somatostatin
endoscopic sclerotherapyendoscopic sclerotherapy or ligation or ligation
or balloon tamponade; or balloon tamponade;
eradication of varices; TIPS, P-C shuntingeradication of varices; TIPS, P-C shunting
Prevention:Prevention: propranolol propranolol
Liver transplantationLiver transplantation

PrognosisPrognosis
Liver transplantationLiver transplantation PrognosisPrognosis


"With ordinary talent and "With ordinary talent and extraordinary perseverance, all extraordinary perseverance, all things are attainable."things are attainable."- Thomas E. Buxton
"Achievement is connected "Achievement is connected
with action…..!”with action…..!”- Conrad Hilton