Embed Size (px)
Citation preview

Heparin Coating and Cardiotomy Suction
in
Cardiopulmonary Bypass
Staffan Svenmarker
Department of Surgical and Perioperative Science
Umeå University, Umeå, Sweden
2003


Umeå University Medical Dissertations
New Series No. 855 - ISSN 0346-6612 – ISBN 91-7305-523-9
From the Department of Surgical and Perioperative Science
Umeå University, Umeå, Sweden
Heparin Coating and Cardiotomy Suction
in
Cardiopulmonary Bypass
Staffan Svenmarker
Fakultetsopponent: Professor Jarle Vaage
Department of Surgery, Ullevål University Hospital
University of Oslo, Norway
Umeå 2003

Copyright � 2003 Staffan Svenmarker
ISBN 91-7305-523-9
Printed by Print & Media Umeå University, Sweden

��������������� ����������������������������
����������������������������
���������� ���������!���"�
#���������!���� ��������
��$!����������������"�
%�� ����������������!���"�
&������' �����������������!������
��������������'"�
�
� (��������������


Table of Contents
Abstract 7
Abbreviations 8
List of papers 9
Introduction
Historical aspects of cardiopulmonary bypass 11 Introductory remarks to cardiopulmonary bypass 12 The systemic inflammatory response syndrome 14 Cardiopulmonary bypass and clinical outcome 17 The role of heparin coating 17 The role of cardiotomy suction 19 Cardiopulmonary bypass and the brain 20 Memory dysfunction 22 The protein S100 23
Aim of the investigations 27
Material & Methods
Characteristics of population 28 General clinical management 30 Conduct of cardiopulmonary bypass 30 General assessments and measurements 31 Statistics 34
Results
HCC and general clinical outcome 35 HCC and renal function 37 Effects of different types of HCC 37 Effect of HCC and PSB-retransfusion on release of protein S100B 37 Effect of HCC and retransfusion of PSB on memory function 38 Recycling of PSB: effects of free plasma haemoglobin 40 Recycling of PSB: general inflammatory effects 40
General Discussion 42
Conclusions 50
Acknowledgements 51
Populärvetenskaplig sammanfattning på svenska 52
References 54


Abstract
7
Heparin Coating and Cardiotomy Suction in Cardiopulmonary Bypass
Staffan Svenmarker Department of Surgical and Perioperative Science, Umeå University, Umeå Sweden.
Abstract The present thesis addresses various means of reducing inflammatory responses associated with cardiopulmonary bypass (CPB) and retransfusion of pericardial suction blood (PSB) during cardiac surgery.
Four (I-IV) prospective randomised controlled clinical trials comprising 475 patients were performed in the following areas: effects of heparin coating on measures of clinical outcome and memory function (I, II), inflammatory reactions in PSB and its systemic effects after retransfusion using cardiotomy suction or cell salvage (III) and effects of retransfusion of PSB on memory function and release patterns of protein S100B (IV).
The use of heparin coated CPB-circuits was associated with a decrease of postoperative blood loss (I, II), transfusion requirements (II), shorter stay in hospital (I) decreased postoperative ventilator time (I), lower incidences of atrial fibrillation (II) and neurological deviations (I), reduction in releases of protein S100B (I, II) and lower postoperative creatinine elevation (I, II).
PSB contained high concentrations of cytokines, complements, myeloperoxidase, free plasma haemoglobin and protein S100B (III, IV). Retransfusion using cardiotomy suction increased the systemic concentrations of free plasma haemoglobin and protein S100B, whereas retransfusion using cell salvage caused no detectable systemic effects (III, IV). CPB was associated with a small but significant release of protein S100B, despite elimination of PSB-contained protein S100B using cell salvage (IV).
Subtle signs of impaired memory function were identified that were not associated with the use of heparin coated CPB-circuits (I, II) or retransfusion of PSB (IV).
Key words: cardiopulmonary bypass, oxygenators, heparin, S100 proteins, blood loss, haemostasis, memory, outcome and process assessment.

Abbreviations
8
Abbreviations
ACT Activated Clotting Time BCI Brain Cell Injury BMI Body Mass Index CABG Coronary Artery Bypass Grafting CBAS Carmeda BioActive Surface CNS Central Nervous System CPB Cardiopulmonary Bypass CR Cardiotomy Reservoir CRP C Reactive Protein CS Cell Saver CT Computerised Tomography ECG Electrocardiogram ELISA Enzyme-Linked Immunosorbent Assay HCC Heparin Coated Circuits IL Interleukin LOS Length of Stay in Hospital MAC Membrane Attack Complex MAP Mean Arterial Pressure MODS Multi Organ Dysfunction Syndrome MPO Myeloperoxidase OFF-PUMP Cardiac surgery without heart-lung machine PHb Plasma Haemoglobin PMN Polymorphonuclear PSB Pericardial Suction Blood SCADs Small Capillary Arterial Dilatations SD Standard Deviation SEM Standard Error of the Mean SIRS Systemic Inflammatory Response Syndrome TCC Terminal Complement Complex TNF Tumour Necrosis Factor

Original Papers
9
This thesis is based on the following papers referred to by their Roman
numerals:
I. Svenmarker S, Sandström E, Karlsson T, Jansson E, Häggmark S,
Lindholm R, Appelblad M, Åberg, T. Clinical effects of the
heparin coated surface in cardiopulmonary bypass. Eur J
Cardiothorac Surg 1997; 11(5): 957-964.
II. Svenmarker S, Sandström E, Karlsson T, Häggmark S, Jansson E,
Appelblad M, Lindholm R, Åberg, T. Neurological and general
outcome in low-risk coronary artery bypass patients using heparin
coated circuits. Eur J Cardiothorac Surg 2001; 19(1): 47-53.
III. Svenmarker S, Engström KG. The inflammatory response to
recycled pericardial suction blood and the influence of cell saving.
Scand Cardiovasc J 2003; 37(3): 158-164.
IV. Svenmarker S, Engström KG, Karlsson T, Jansson E, Lindholm
R, Åberg, T. Influence of pericardial suction blood retransfusion
on memory function and release of protein S100B. Submitted.
Reprints of original papers were made with approval from the publisher.

10

Introduction
11
Introduction
Historical Aspects of Cardiopulmonary Bypass
The invention of the heart-lung machine is attributed to John Gibbon, Jr. His wife, Mary Gibbon was the first perfusionist. Dr. Gibbon invented the heart-lung machine in his laboratory at the Bullfinch Building of the Massachusetts General Hospital in the 1930’s. Originally, it was designed to serve as life support during Trendelenburg operations and pulmonary embolectomy - at that time associated with nearly 100% mortality. In 1953, the heart-lung machine was introduced in cardiac surgery, when Gibbon successfully closed an atrial septum defect in an 18-year-old woman [1].
Clarence Crafoord performed the second heart operation ever with the aid of a heart-lung machine in Sweden 1954 [2]. Inge Rygg and Erik Kyvsgaard developed a new type of integrated soft-shell bubble oxygenator in Denmark in 1956 [3]. The main body of work for the evolution of extracorporeal circulation during the 1950’s took place at the Mayo Clinic by John Kirklin and by C. Walton Lillehei at the University of Minnesota [4-6].
Kirklin performed a series of cardiac interventions using a modified Gibbon heart-lung machine with promising results [4]. However, the equipment was complex and difficult to operate and maintain. C. Walton Lillehei had at the time introduced the bubble oxygenator [5]. The device represented a tremendous step towards simplicity, making the process of extracorporeal circulation more accessible. From 1955 to 1966, C. Walton Lillehei operated on more than 2500 patients with the help of bubble oxygenators [6]. The first disposable bubble oxygenator with integrated heat exchanger came in 1955 by DeWall and colleagues [7].
Today, bubble oxygenators have been replaced by membrane oxygenation, which first was described by Wilhelm Kolf [8] in 1956 and introduced clinically by Frank Gerbode [9] and Arnold J. Lande [10] in 1966.
Despite nearly half a century since the introduction of cardiopulmonary bypass (CPB) in cardiac surgery we are still confronted with similar challenges to those which occupied the pioneers. Gibbon was aware of the importance and possible deleterious effects of the contact between blood and the foreign environment represented by the extracorporeal circuit.

Introduction
12
“The surface contact with blood should be inert, friendly, one might say, to the blood passing along, and this passage of blood should provide the patient with adequate circulation of undamaged properly oxygenated blood and a means for its release of carbon dioxide” [11].
The present thesis addresses a related issue to describe ways of how to modulate the blood-to-surface interaction, as well as effects generated by the use of cardiotomy suction.
Introductory Remarks to Cardiopulmonary Bypass
Despite recent trends in cardiac surgery to avoid CPB in attempts to simplify and to reduce complications [12], CPB will play a major role for several cardiac surgical interventions for years to come. Therefore, further refinement and improvement of the extracorporeal technique remains an important field of research.
According to the Society of Thoracic Surgeons National Database, 20% or 22.000 low-risk patients develop postoperative complications after cardiac surgery [13]. Multiorgan failure occurs in 11% of cases, which increases the risks of other morbidity and mortality. In our own experience, more than 40% of cardiac surgical patients deviate in some respect from a completely normal postoperative course [14].
Since cardiac surgery is a multidisciplinary intervention, it is difficult to isolate to what extent CPB contributes to the development of organ dysfunction and poor patient outcome. The situation is further complicated by the varied and profound effects CPB may have on normal physiology. Safety and quality aspects of clinical perfusion routines should also be considered [15] (Figure 1).

Introduction
13
Figure 1. Physiological and procedure related aspects of cardiac surgery and cardiopulmonary bypass.
�����������
�� ���
� ������ ������ ���
���
������������� ��
������������� �� �
������ ����������
� ��������������������
��������������� ���
���� � �������
���! "�� � �����
# ��$��������� ���
� ��%������
�������������� ���������
� ������$������ ���
� �������� ��
"�� ��� ��
���������������
��������
� ��� ���������
�����&���
� �����"������������

Introduction
14
The Systemic Inflammatory Response Syndrome
Contact of blood with foreign surfaces during CPB triggers a global defence reaction affecting essentially every cell within the body, usually denoted in the literature as the systemic inflammatory response syndrome (SIRS) [16-18]. This response is characterised as being non-specific and of varying intensity, but may in a low percentage of cases lead to severe organ dysfunction, death or limit long time survival [19]. SIRS is governed by a complex interplay of cellular and humoral proinflammatory and antiinflammatory responses. Imbalance or a proinflammatory turnover may affect normal postoperative recovery and clinical outcome [20-22].
The general intensive care diagnosis of SIRS [23] requires the presence of two or more of the following criteria:
• Body temperature > 38˚C or < 36˚C • Heart rate > 90 beats/minute • Respiratory rate > 20 breaths/minute or PaCO2 < 4.3 kPa • Leukocyte count > 12 000 or < 4 000 (*109) or 10% immature forms
During cardiac surgery SIRS may also develop as a consequence of reperfusion injury after aortic cross clamping [24] or hypoperfusion of the gut leading to endotoxemia [25]. A schematic overview of SIRS in conjunction with CPB is presented in Figure 2.
Cardiopulmonary Bypass
Initiating Factors
• Contact activation • Ischemia & Reperfusion • Endotoxemia
Immune System Activation
• Complement • Cytokines • Coagulation & Fibrinolysis • Endothelium • Cellular Immune System
Figure 2. An overview of responses attributed to the use of cardiopulmonary bypass and the development of the systemic inflammatory response syndrome [26].

Introduction
15
Complement activation
One of the most important immunologic reactions related to the development of SIRS is complement activation. Complement is comprised of a group of more than 30 proteins activated through three different pathways. It serves as a primitive recognition system capable of self/nonself descrimination [24, 27]. The ‘classical’ pathway is initiated by complement factor C1 binding to antigen-antibody complexes. The ‘alternative’ pathway is initiated by complement C3b binding to various activating surfaces or bacteria. The third pathway is initiated by binding to lectin. All three pathways converge trough a central C3 convertase step, followed by a cascade action and self-assembly of the membrane attack complex C5b-C9 (MAC). The MAC is responsible for cell lysis, whereby the cell membrane is penetrated or attacked in an attempt to eradicate the invader [27].
Complement activation leads to generation of the anaphylatoxins C3a and C5a [24]. Their action initiates the release of histamine and leukotrienes from mast cells and basophiles. Effects of anaphylatoxins during CPB are observed in part as vasodilatation and increased vascular permeability [27]. C5a acts as a chemotactic and activating agent for neutrophils, leading both to their recruitment and release of lysosomal enzymes, reactive oxygen species and other inflammatory mediators [24].
CPB activates primarily the ‘alternate’ pathway [28], while protamine, or the heparin-protamine complex is a trigger of the classical pathway [29]. During the postoperative period a second delayed complement activation is observed, mediated by C reactive protein (CRP) [30]. The degree of complement activation during CPB is probably of clinical significance. Pulmonary function correlates with activation of the ‘classical’ pathway by protamine-heparin complexes and C4d activity with postoperative arrhythmia [30]. Furthermore, C3a activity or activation predicts occurrence of cardiac, pulmonary, renal and haemostatic dysfunction [22]. Modulation of the terminal complement complex is reported to affect cardiac function, blood loss and cognitive deficits [31].
Cytokines
Cytokines are a group of proteins produced by different cells, most notably cells of the immune system, either as a response to an immune stimulus or as an intercellular signal. Cytokines have a multitude of different biological effects and are important both in the innate and in the adaptive immune response [32].

Introduction
16
It is well recognised that use of CPB induces syntheses of proinflammatory cytokines [18, 33]. Among most widely recognised are tumour necrosis factor alpha (TNF-α), interleukins IL-1, IL-6 and IL-8. This proinflammatory activity is concomitantly counterbalanced by a similar antiinflammatory cytokine response, typical by for instance increases of IL-10, IL-1ra and TNFsr-1 and TNFsr-2 [33]. The specific role of an imbalance in cytokine control and possible interferences with normal organ function and clinical prognosis remains to be resolved [34].
Coagulation and fibrinolysis
Activation of coagulation and fibrinolysis represents two important processes in the systemic inflammatory response induced by CPB. The magnitude of activation is determined by many factors, including other branches of the inflammatory syndrome [17, 35-37]. The coagulation cascade is traditionally divided into the ‘intrinsic’ and ‘extrinsic’ pathways converging into a common pathway from which thrombin is generated. In a final step, thrombin converts fibrinogen to an insoluble fibrin clot [38]. The ‘intrinsic’ pathway is initiated by the blood-foreign surface contact, mediated via the Hageman factor XII. The ‘extrinsic’ pathway is predominately triggered by tissue factor VIIa. The relative importance of these two pathways in terms of coagulation activity during CPB is of great concern. In patients with congenital factor XII deficiency, thrombin is nonetheless produced, strongly engaging the ‘extrinsic’ pathway of coagulation during CPB [39]. In theory this requires expression and activation of tissue factor and VIIa [36]. The surgical trauma [36] and use of cardiotomy suction [40, 41] are probably the main mechanisms to this reaction.
Procoagulant activity and its restriction, mediated by anticoagulant mechanisms in the ideal case coexist in a delicate balance. CPB represents a threat to this balance evidenced by its procoagulant activity, which requires administration of anticoagulant drugs. CPB also stimulates fibrinolysis contributing to postoperative coagulopathy [38]. Disturbances to normal coagulation function may in the wider perspective lead to deposition of fibrin in end organs, contributing to the multiorgan dysfunction syndrome (MODS) and possible death [35].
The endothelium
The endothelium is no longer regarded as a static barrier [42]. On the contrary, it represents an active participant of many vital body functions, one being the inflammatory process. Its activity is apparent by control of vascular tone, permeability, coagulation processes, interactions with leukocytes and platelets through expression of surface proteins and

Introduction
17
secretion of soluble mediators [43]. Endothelial cell adhesion molecule expression mediates the interaction between the neutrophil and endothelial cell, resulting in neutrophil adhesion, activation and degranulation [44]. This neutrophil activity further damages the endothelium, causing diffuse capillary leak and oedema formation [42].
The cellular immune response
The interaction between neutrophils and the endothelium is an essential part of the inflammatory process, which leads to endothelial damage [43]. In the initial phase, neutrophils are converted into a “rolling state”, mediated by expression of adhesion molecules. P- and E-selectin are found on the endothelium and L-selectin on the neutrophils. A related mechanism of adhesion of platelets is mediated by the P-selectin. This is succeeded by a tight adhesive link of neutrophils to the endothelium governed by integrin molecules, whereupon the neutrophils eventually are transmigrating out of the circulation [43]. At this stage neutrophils degranulate and undergo a respiratory burst releasing cytotoxic proteases such as elastase and myeloperoxidase [45, 46]. These enzymes can lead to damage of the surrounding tissue [47]. CPB is associated with increased concentrations of both neutrophils and leukocyte adhesion molecules, which persists 24 h after surgery [48]. The clinical significance of leukocytes in the inflammatory response to CPB is verified by pulmonary sequestration of neutrophils, which can compromise normal lung function [47]. Influences on cardiac and renal function have also been demonstrated [45].
Cardiopulmonary Bypass and Clinical Outcome
SIRS is closely related to the development of organ dysfunction [18]. Use of CPB may significantly contribute to a systemic inflammatory response and development of postoperative dysfunction of major organs [49]. Ameliorating CPB-related initiation of SIRS during cardiac surgery should contribute to improvement of general clinical outcome after CPB [50]. We have chosen to investigate some aspects of CPB activation of systemic inflammation, with the goal of decreasing this type of post-bass morbidity.
The Role of Heparin Coating
Coating of artificial surfaces with heparin is designed to improve biocompatibility by mimicking the native constituents of heparan sulphate in endothelial cells [38]. Two different heparin coated surfaces (HCC) have been employed in this thesis: the Carmeda Bioactive Surface (CBAS) (Medtronic Foundation, Minneapolis, MN, USA) and Duraflo heparin coating (Jostra AG, Hirrlingen, Germany). The CBAS

Introduction
18
technology utilises a covalent bonding of heparin by end-point immobilisation to the artificial surface isolated via a duplicate layer of polyalkylenamine [51]. The antithrombin-binding sequence of the heparin molecule is thereby made available [52]. The Duraflo heparin coating is based on an ionic bond of heparin-benzalkonium-chloride complex adhered to the foreign surface [53]. The ionic bonding technique is known to be less stable and heparin may leach from the surface into the circulation [54]. Both types of heparin coatings have documented inhibitory effects on coagulation and other branches of inflammatory processes associated with CPB. However, indifferences in degree of biological activity have been demonstrated [55], with no significant connections to patient outcome [54].
More recent findings suggest that the biocompatibility properties of HCC are attributed to quantification of adsorbed plasma proteins occurring on the initial contact with blood [56]. Differentiation of the protein layer determines the unique qualities of a specific artificial surface, not only limited to thrombogenetic characteristics, but also from a global inflammatory response perspective.
The reduced thrombogenicity produced by HCC was initially believed to decrease or even exclude the need for systemic anticoagulation [51, 57]. However, to completely exclude the need for systemic heparin seems unrealistic, since coagulation is also triggered by the surgical trauma and use of cardiotomy suction [41]. The optimal heparin level for anticoagulation during CPB is still a matter open for discussion [35]. Combining HCC with reduced systemic heparin doses for routine coronary bypass grafting has proven to be safe based on an extended experience from a limited number of centres applying the technique [58, 59].
Despite all theoretical and proven advantages of HCC on humoral and cellular responses it has been difficult to identify a clear link with improved clinical outcome. The reason for this may have methodological causes as well as suboptimal study design [60]. Measurement of clinical outcome [61] is typically based on observations related to time as length of stay in intensive care or hospital. Blood loss and transfusion requirements are two other common parameters used to define clinical outcome. A problem with all these measures has been the researcher’s ambition to generalise from changes in these parameters with the use of HCC. Data reflecting clinical outcome are prone to be influenced by departmental routines, which in a study design are difficult to control. In large-scale multicenter investigations [62] this has apparently turned out to be a methodological problem [60]. To prove the

Introduction
19
significance of HCC to change clinical outcome may be difficult and therefore necessitates an optimal study design with sufficient power.
The Role of Cardiotomy Suction
The use of cardiotomy suction during CPB may be life saving in the case of major bleeding. However, in routine coronary artery surgery with a low risk of bleeding, the indication for cardiotomy suction is primarily to return relatively small volumes of blood from the surgical field. A defoaming chamber enables separation of air from blood by modulation of surface tension. Screen filtration (20-40 µm) removes debris before the pericardial suction blood (PSB) is re-administered into the systemic circulation. This relatively simple ‘cleaning’ process is employed to avoid macro-embolic debris being expelled into the arterial circulation and to ensure safe intraoperative autologous retransfusion during CPB. The method represents the standard procedure at most cardiac centres. We now know that the technique is associated with a number of limitations, several of which may have detrimental consequences for the patient.
Exposure to negative pressure and the interface with air are the two major determinates of haemolysis generated by cardiotomy suction systems [63]. Several methods of reducing haemolysis have been proposed [64], without receiving widespread use. Platelet activation and dysfunction is still another side effect, increasing the risk of postoperative bleeding [65].
More important are the demonstrated effects cardiotomy suction may have upon the normal functions of the brain. Blood travelling trough the filter of a cardiotomy reservoir contains debris of different origin [64]. The fat component especially seems to be important for the development of small capillary arterial dilatations (SCADs) identified in the brain among post mortem patients exposed to CPB [66]. These malformations are between 10-70 µm in sizes consisting of acellular fatty material and prevalent only during a limited time after the exposure to CPB [67]. Experimental data suggest that cardiotomy suction is a major cause for the development of SCADs. Retransfusion of PSB in dogs has been shown to systematically generate SCADs [68]. Means to remove fat are limited to specially designed filters [69] and the use of cell saver techniques [70]. New methods are being developed, but are not yet clinically established [71].
Analysis of PSB during clinical conditions verifies the content of fat [70, 72]. Appelblad and Engström have shown that fat contamination may seriously impair capillary blood flow conditions during in vitro

Introduction
20
measurements [72]. The in vivo implications of these findings are not yet defined. Organ dysfunction after CPB is generally acknowledged [18]. The impact of fat contamination in this context is of prime interest and deserves further attention, especially with reference to the functions of the brain.
Triggering mechanisms of inflammatory responses during CPB include apart from foreign surface interactions the effects of PSB recycling [41]. Most importantly, this concerns activation of the coagulation cascade via the extrinsic pathway and tissue factor VIIa [40]. Boisclair et al. showed already in 1993 how formation of thrombin correlates with factor IX and not with factor XII [36], which indicates significant tissue activation of coagulation during CPB. This, combined with observed subnormal heparin concentrations in pericardial blood [41], further emphasises the coagulation aspect of cardiotomy suction.
The most rational approach to avoid side effects of cardiotomy suction would simply be to exclude its use. Alternatively, other means of PSB retransfusion can be considered. Aldea and co-workers have shown that excluding cardiotomy suction may lower activation of coagulation, polymorphonuclear neutrophils (PMN) and platelets [59]. Cell saver devices are first choice alternatives for PSB recycling during CPB. The method has been reported to efficiently remove major parts of fat contained in PSB, evident both from clinical [70] and experimental data [73].
Consequences of PSB recycling are at present not fully elucidated. We know that PSB contains elements of inflammation [59, 74], most significantly activation of the coagulation [41]. Information on the balance of activation between different branches of inflammation is lacking, especially the involvements of cytokines and PMN neutrophils. The ultimate challenge is to establish risks associated with retransfusion of PSB, especially with reference to the brain and the appearance of cognitive disturbances [75].
Cardiopulmonary Bypass and the Brain
Thirty years ago Branthwaite [76] and Åberg [77] described how cardiac surgery using CPB is associated with a range of side effects altering normal functions of the brain. Despite refinements in surgical techniques, cerebral consequences following cardiac surgery still occur [75, 78-82]. The most frightened threat is a major focal injury with devastating consequences for the patient. Frank stroke is reported to occur in 1-3% [80, 81], while the prevalence of cognitive dysfunction is significantly higher and ranges from 4% to 80% depending on definition [75, 82, 83]. Plausible explanatory mechanisms focus on

Introduction
21
microembolism and hypoperfusion [75, 81, 84]. The incidence of brain injury has decreased over time in spite of a marked increase of complexity in the case-mix and severity of comorbidity of patients.
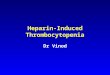
The risk of a focal cerebral injury coincides with degree of calcification of the aorta [85, 86], making surgical manipulation of the area potentially dangerous (Figure 3). Cognitive changes are related to the miroembolic load arising from the CPB-circuit [79, 87] and the surgical field [88].
0
5
10
15
20
25
30
35
32 57 62 67 71 75
Age [years]
%
Intermediat
Severe
Figure 3. Prevalence and degree of calcification in ascending aorta related to age based on subjective intraoperative palpation in 5863 coronary artery bypass surgical patients at the Heart Centre of Umeå University Hospital, Sweden. Registration period 1995-2002.
Circulatory effects of CPB are numerous; one consequence may be a compromise in cerebral perfusion [80]. Cerebral blood flow during CPB is primarily controlled by a calculated pump flow and the body’s autoregulatory mechanisms for vascular tone [89]. These very basic fundaments for blood flow control may in extreme situations not suffice to meet the actual demand [80]. One also needs to consider influences of pH control strategies [80], temperature management [90] and the complex interaction of different inflammatory cascade systems [91]. All of the given examples may in theory cause a mismatch situation leading to hyper- or hypoperfusion of the brain. Precise prevalence or severity of these changes has not been reported to date.
In explaining cognitive disturbances after CPB, the impact of SIRS has been proposed as an important factor [80]. To what extent SIRS contributes to the development of cognitive dysfunction needs to be clarified in more detail [91, 92].

Introduction
22
Consequences of neurologic adverse events
A state of focal cerebral injury or cognitive disability after cardiac surgery is a detrimental situation for the patient. It also contributes to a significant healthcare cost for the community. Mortality rates among patients with focal injury increase 10 fold and transfer to chronic care facilities are 5 times higher compared to patients without adverse cerebral outcome [81].
Joint efforts are therefore needed to improve surgery and perfusion techniques. One reasonable approach from the perfusion perspective would focus on completely elimination of emboli coming from the extracorporeal circuit and making the interface between blood and foreign surfaces physiologically inert or adaptive to avoid inflammatory reactions.
Memory Dysfunction
Although postoperative neurocognitive impairment is complex and not unique to cardiac surgery, it seems to be more frequent and more severe after operations using CPB [75, 93]. For some patients these changes may persist at six months [75] and also correlate with changes in measures of quality of life [94]. To minimise impairments related to CPB seems therefore to be a matter of high priority.
Cognitive function embraces a number of different domains of, which learning, language comprehension, psychomotor speed, figural memory, attention and concentration are of special concern [84]. The busy university hospital setting usually restricts the possibility of a comprehensive cognitive examination, especially during the immediate postoperative period. This requires a selection of an appropriate assessment battery amenable to these limitations. Such tests have been proposed and also adopted by many research groups [84]. However, controversy still exists as to the composition of an optimal test battery [95]. In our case, cognitive assessment consisted of three tests of explicit and implicit memory. Memory dysfunction is a very commonly reported type of cognitive dysfunction after cardiac surgery [75, 81, 96].
The lack of consensus on frequency and extent of cognitive impairment reported in the literature deserves comment [75, 82, 83]. A major problem is the variety of tests employed to measure cognitive function [97]. Tests are designed to cover specific domains of cognition using different techniques, which is why test results must be evaluated individually [84]. For instance, Mahanna demonstrated how the incidence of cognitive decline varies from 1.1% to 34% 6 weeks after cardiac surgery, depending on interpretation of test results [95]. Apart

Introduction
23
from inter-test variability, researchers use different thresholds for defining cognitive decline. Some researchers have based their conclusions on statistically significant differences based on raw scores; others set the cut-off to 20% between two test intervals and still other alternatives include cut-offs based on the standard deviation (SD) or constructed indices [98]. The statistical approach to data further adds to the complexity of interpretation [97, 98].
To validate cognitive decline, it is necessary to use at least two separate test occasions, which are typically performed pre- and postoperatively. Some test batteries employ the same test for both occasions, leading to false improvements or learning effects [99]. Basic reliability requirements are not fulfilled in these situations. Ways to avoid these drawbacks include using separate tests validated by a reference group [98]. Apart from improved reliability, the technique enables evaluation of the patient’s individual cognitive function relative to norms of the reference group. Relative performance is typically reported in standard units. Z-scores represent one alternative based on the normal distribution, with a mean of zero and standard deviation of 1. A Z-score of zero should be interpreted as normal performance compared to reference. Units of Z-scores away from zero denote degree of deviation from the normal: either improvement or impairment, depending on direction.
The Protein S100
The protein S100 was discovered by More in 1965 and named S100 due to its 100% solubility in ammonium sulphate at neutral pH [100]. This protein purified from bovine brain was later identified as two different, but closely related proteins (S100B and S100A1) [101]. It is found in astrocytes and in populations of oligodendrocytes within the central nervous system (CNS) [102], but also in Schwann cells of the peripheral nervous system [103]. One typical characteristic of the S100 family is the property of binding Ca2+ [101], but also Zn2+ and Cu2+ [104]. The molecular weight varies from 9 to 14 kDa [105].
Thirteen different forms of S100A (S100A1-S100A13) are found in humans, with their gene locus on chromosome 1 [102]. Most S100 proteins exist as homodimers within cells in which two monomers are joined by non-covalent bonds. Some S100 proteins form heterodimers [106]. The homodimer of S100B (S100BB) forms a very stable linkage and appear mainly within cells [107]. The dimer structure of the S100 protein enables each monomer to accommodate a target protein via Ca2+ cross-linking, whereby the S100 protein exerts its controlling functions [106].

Introduction
24
Extracellular functions of the S100 protein
S100B is secreted into the extracellular space by astrocytes [108], adipocytes [109] and pituritary folliculostellate cells [110]. Information is sparse regarding the functional mechanisms behind secretion from pituitary and adipose cells. S100B secreted from glial cells exerts trophic or toxic effects, depending on concentration. At low concentrations, neurite outgrowth [111] and survival [112] are enhanced, indicating that S100B has an important impact on both nerve development and nerve regeneration. High concentrations of S100B are seen in patients with Down’s syndrome [113] and Alzheimer’s disease [114], and this has been used as a diagnostic tool. Other situations when high serum levels of S100B concentrations have been associated with disease are head injury [115], cardiac surgery [116], stroke [117] and Creutzfeldt-Jakob disease [118].
S100 inflammation and cognitive function
S100 members are supposed to have a regulatory role in inflammation with actions both inside and outside cells. S100A8 and S100A9 have close connections to inflammations processes localised to neutrophils, macrophages and endothelial cells [119]. Extracellular S100B has been implicated in modulation of learning and memory [120]. The interplay between cognition and S100 is to date not well understood. However, it has been demonstrated that overexpression of S100B in transgenic mice impairs the ability to solve spatial tasks and temporal exploratory patterns [121]. Overexpression of S100B in neurons may also be linked to secretion of the proinflammatory cytokine IL-6, which may have implications in certain neuropathological changes [122].
Distribution and elimination of protein S100B
The protein S100B is mainly located to the brain, but may be found in other organs at a lower concentration [123]. Apart from the concentration of S100B in individual organs, organ weight and blood supply also influence degree of possible secretion into the extracellular space.
The S100B protein is mainly eliminated by renal metabolism [124]. Half-life of S100B was originally thought to be 113 minutes [125], but new findings suggest a half-life of 25 minutes [126].
The S100 protein assay
Two assays for S100B analysis have been described, both supplied by Sangtec® Medical AB, Sweden. The first assay used a two-site immunoradiometric assay (IRMA) with a sensitivity of 0.2 µg/L [127],

Introduction
25
followed by the new immunoluminometric methodology (LIA) [128] with improved sensitivity at 0.02 µg/L. Both types of assays use the same antibodies (SMST 12, SMSK 25, SMSK 28) for detection of the S100B protein. The emitted radiation (IRMA) and light signal (LIA) are measured and these are directly proportional to the S100B concentration of a blood sample.
The S100B subunit is not a single protein. It represents any of all possible S100 dimers that contain at least one beta monomer subunit [129]. The commercial immunoassay is sensitive for any occurring beta-subunit regardless of specific configuration. Beta-units appearing as homodimers and heterodimers are collectively recognised, which is why summed concentrations of S100BB and S100A1-B are reported. This limitation does not seem to interfere with its specificity of detecting brain injury [130].
Use of protein S100 as a diagnostic marker
The protein S100B is a useful marker to assist the clinician in diagnosing pathology involving the central nervous system [115, 131, 132] and malignant melanoma [133]. Computerised tomography (CT) verified head injury is associated with increased levels of S100B, whereas absence of S100B elevation predicts a normal CT-scan finding [131]. Stroke after cardiac surgery confirmed by magnetic resonance imaging induce migration of S100B to serum in concentrations correlating to the size of focal injury [132]. S100B can be used in early prognostic evaluation of short-term outcome after cardiac arrest; S100B in excess of 0.2 µg/L indicates lethal outcome [115].
S100B in Cardiac Surgery
Sellman and colleagues introduced S100B as a marker of cerebral damage in conjunction with cardiac surgery in 1992 based on samples from cerebrospinal fluid [134]. In 1995, Johnsson and associates demonstrated the use of serum samples for S100B analysis [135]. In ensuing publications, S100B has been used to identify cerebral disturbances after cardiac surgery and CPB [125, 136-139]. Associations were detected between release of S100B and duration of CPB [137, 138], deep circulatory arrest [140] and aortic cross clamp time [141]. Furthermore, occurrence of arterial emboli [141] and increased patient age [138, 141] was also found to coincide with serum concentration of S100B.
Limitations of S100B in cardiac surgery
New findings have suggested that S100B released during cardiac surgery using CPB may originate from sources other than the brain

Introduction
26
[136, 142, 143]. The group of Westaby found that S100B was only minimally released if CPB was omitted and only in patients with clear cerebral symptoms [144]. It has now been established that the major source of S100B generating pathological serum concentrations during CPB is shed blood and autotransfusion [130, 136]. CPB itself generates negligible amounts of S100B in serum [93, 136, 145]. S100B may also be found in fat, marrow and muscle tissue in high concentrations, which may contribute serum levels [130]. Outside the realm of cardiac surgery, pathological concentrations of S100B have been identified in trauma patients with no apparent injury to the brain [143]. Based on several independent observations, S100B appears to lack specificity for detection of brain cell injury (BCI) in cardiac surgery, irrespective of cardiotomy suction usage. The future role of S100B in cardiac surgery as brain cell injury marker seems uncertain.
Important considerations regarding S100B in the present thesis
In the start of preparation of the components for this thesis, S100B was regarded as a marker of BCI [127, 134, 135]. When the first findings of the non-specificity of S100B in the setting of cardiac surgery were published in 1999 [136, 142], we changed focus as regards S100B in order to critically assess its use.

Aim of Investigations
27
Aim of the Investigations
• To investigate the effect of heparin coated circuits on clinical outcome
• To investigate the relation of systemic inflammatory response and pericardial suction blood
• To investigate the effect of heparin coated circuits and retransfusion of pericardial suction blood on the appearance of postoperative memory disturbances
• To assess the value of protein S100B as a brain cell injury marker in the setting of cardiac surgery

Material & Methods
28
Material and Methods
Characteristics of the population
This thesis is based on a population of patients admitted to the Umeå University Hospital for elective first-time coronary artery bypass grafting (CABG). Inclusion criteria were good left ventricular function, normal coagulation parameters and no signs of neuropsychological illness. Age limits were 75 (I, II) and 70 years (III, IV), respectively. Ethical approval was obtained from the Ethical Committee at Umeå University. 56 59 100 100 100
16 17 30 30 Figure 4. A schematic presentation of included studies (I-IV) in this thesis. Total number of investigated subjects (n=475) organised in a two-arm model: Heparin coated circuits (HCC) (n=415) and pericardial suction blood (PSB) (n=60).
CBAS-Carmeda BioActive Surface, CR-Cardiotomy Reservoir and CS-Cell Saver.
HCC (415)
I (115) II (300)
CBAS Control CBAS Duraflo Control
PSB (60)
III (33) IV (60)
CR CS CR CS

Material & Methods
29
Table 1. Description of patient population
Study I (n=115) Study II (n=300)
CBAS Control CBAS Duraflo Control
Age years 64.0 ± 0.9 64.0 ± 1.0 61.3 ± 0.7 61.9 ± 0.8 61.0 ± 0.8
Male gender % 83 77 88 83 81
Weight kg 79.6 ± 1.4 78.2 ± 1.5 82.7 ± 1.2 82.8 ± 1.2 84.1 ± 1.5
Height cm 172 ± 1 172 ± 1 174 ± 1 172 ± 1 173 ± 1
Hypertension % 47 32 43 52 46
Diabetes % 12 14 12 13 16
Pump time min 95.9 ± 3.2 94.4 ± 4.1 75.8 ± 2.3 77.2 ± 2.5 78.8 ± 3.3
Clamp time min 56.6 ± 2.3 59.5 ± 0.8 40.9 ± 1.6 41.9 ± 1.5 42.8 ± 2.2
Temperature °C 32.5 ± 0.1 32.7 ± 0.1 33.8 ± 0.1 33.9 ± 0.1 33.9 ± 0.1
Study III (n=33) Study IV (n=60)
CR CS CR CS
Age years 56.4 ± 1.5 60.2 ± 1.5 58.7 ± 1 60.3 ± 1
EuroSCORE 1 (0-3) 0 (0-3) 1 (0-3) 0 (0-3)
BMI 28.4 ± 1.1 28.4 ± 0.8 27.5 ± 0.7 27.7 ± 0.6
Pump time min 69.7 ± 5.3 70.2 ± 5.8 69 ± 3.9 67 ± 4.1
Clamp time min 34.6 ± 2.9 37.5 ± 4.3 35 ± 2.3 36 ± 2.9
Temperature °C 34.5 ± 0.2 34.3 ± 0.1 34.3 ± 0.1 34.2 ± 0.1
CBAS-Carmeda BioActive Surface, CR-Cardiotomy Reservoir and CS-Cell Saver.

Material & Methods
30
Informed consent was obtained from all participating patients. Randomisation to type of CPB-circuit was performed preoperatively. Investigators were blinded to type of circuitry during postoperative data collection. Overview of thesis is presented in Table 1 and Figure 4.
General clinical management
Patients were premedicated with flunitrazepam and morphine-scopolamine. Intraoperative monitoring included radial arterial and central venous pressures, pulse oximetry and ECG. Anaesthesia was induced and maintained with propofol, midazolam, fentanyl and isoflurane, using pancuronium-bromide as muscle relaxant. Mechanical ventilation was controlled to normocapnia, extubation was performed upon normal postoperative recovery: when patients were alert, breathing spontaneously and had no circulatory instability. Inotropic treatment, administration of fluids and blood products followed departmental routines.
Surgical technique for coronary bypass grafting was performed according to generally accepted methods including the use of the left internal mammary artery and by placement of proximal venous grafts anastomosis behind a side-biting clamp. Intermittent antegrade St Thomas’s crystalloid cardioplegia was used for myocardial protection.
Our department collects a registry of deviations defined by norms of postoperative recovery [14]. Information extracted from this registry was used for evaluation of clinical end-points.
Conduct of cardiopulmonary bypass
CPB was controlled to maintain the mixed venous oxygen saturation greater than 70% and mean arterial pressure (MAP) more than 50 mmHg using a roller pump set to non-pulsatile flow mode. Rectal body temperature was targeted to 32 °C (I, II) and 34 °C (III, IV), respectively. α-stat acid-base regulation was implemented.
Anticoagulation
Heparin sodium was administered and the effect controlled by measuring the activated clotting time (ACT). ACT level was set to >480 seconds or >250 seconds when combined with HCC (I, II). Heparin and protamine dose requirements were calculated using the Hepcon Hemostasis Management System (Medtronic Inc. Minneapolis, MN USA) (I, II). In study III and IV, standard doses of heparin (350 IU/kg) and protamine were used.

Material & Methods
31
CPB circuit
All circuits were primed with Ringer’s acetate, mannitol and heparin sodium.
In study I and II, circuitry included components coated with heparin or non-coated equivalents: membrane oxygenator, PVC tubing, arterial line filter and closed venous reservoir. Two different heparin coatings were employed: CBAS (I, II) [51] with covalent end-point attachment and Duraflo (II) [53] an ionic bond of heparin to the artificial surface.
In study III and IV, the membrane oxygenator and reservoirs were coated with phosphorylcholine [146]. The circuits were otherwise comprised of components without surface modification.
General assessments and measurements
Study I
- To study the effects of CBAS heparin coated circuits compared to conventional uncoated control circuits. The endpoints were clinical outcome, memory disturbances and cerebral trauma assessed by protein S100B.
Study II
- To study the effects of two different heparin coatings: CBAS and Duraflo compared to conventional uncoated control circuits. The endpoints were clinical outcome, memory disturbances and cerebral trauma assessed by protein S100B.
Study III
- To study the inflammatory profile of PSB and the systemic reaction upon retransfusion.
Study IV
- To study influence of PSB retransfusion on memory function and release patterns of protein S100B.
Clinical outcome
Clinical outcome was defined by length of stay in hospital and intensive care, ventilator time, postoperative blood loss, blood transfusion requirements and the incidence of postoperative deviations.
Renal function was used as a crude marker of HCC’s effect on organs and was determined by the perioperative change of creatinine.

Material & Methods
32
Tests of memory function
Memory function was assessed on the day before surgery and at discharge from hospital. A standardised battery [147] of explicit and implicit memory tasks was administered using a laptop computer [148].
Implicit memory was defined as the degree of priming [149] or perceptual learning using one test [150]. Explicit memory was based on two tests of recognition and defined by the ability to discriminate between hits and false alarms. Results as to explicit memory were analysed in accordance with signal detection theory and expressed as d-prime values [151].
In study IV, memory scores were standardised to Z-scores [152] referring to normative test scores obtained from a reference group of healthy controls.
In study II, effects of HCC on memory function were also evaluated by six specific questions of memory before and 4 months after surgery. The questionnaire was directed to both the patient and spouse.
Protein S100B
In studies I and II, the serum concentration of protein S100B was determined before surgery, at termination of CPB (I) or 60 minutes of CPB (II), 7 h post CPB, and on the morning of postoperative day 1-2 (I).
In study IV, the serum concentration of protein S100B was determined before surgery, on the release of the aortic cross clamp, in PSB before retransfusion, in systemic circulation after PSB retransfusion, at termination of CPB, 5 h post CPB and on the morning of the first postoperative day.
The concentration of protein S100B was analysed in serum by using IRMA (I) and LIA-mat (II, IV) assays from Sangtec AB, Bromma, Sweden. Sensitivity of the assays was 0.2 µg/L and 0.02 µg/L respectively.
Pericardial suction blood
PSB was stored in the cardiotomy reservoir during CPB. Retransfusion of PSB was performed using two methods: either as a bolus directly from the cardiotomy reservoir upon weaning from bypass (CR-group) or using a cell saver (autoLog, Medtronic Ltd, Minneapolis, MN, USA) returning the red cell fraction after completed CPB (CS-group).
PSB was analysed with respect to contents of inflammatory markers and free plasma haemoglobin (pHb). The contribution of PSB to the general

Material & Methods
33
inflammatory response during surgery and CPB was examined by measuring the systemic concentration of inflammatory markers before and after retransfusion. Sampling intervals are given in Table 2.
Table 2. Sampling intervals study III
Sample Procedure
1 Before CPB
2 Release of aortic cross clamp
3 Before retransfusion of PSB, ~10 min to weaning from CPB
4 After retransfusion of PSB, at weaning from CPB
5 5h post CPB
6 Postoperative Day 1
Sampling intervals (1-6) refer to the systemic concentration of inflammatory markers including pHb. Systemic response of PSB retransfusion was determined for samples 4 through 6. PSB was analysed using the same battery of markers.
Inflammatory markers
The following markers were included for measurement of the inflammatory reaction in PSB and in systemic circulation during and after CPB. Cytokines: interleukin 6 (IL-6), interleukin 8 (IL-8) and tumour necrosis factor alpha (TNF-α). Complements: C3a and terminal complement complex TCC (SC5b-9). Polymorphonuclear (PMN) neutrophils: myeloperoxidase (MPO).
All these markers were analysed using standard immunoassay techniques (ELISA).

Material & Methods
34
Statistics
Results were presented as means ± standard error of the mean (SEM), if not otherwise stated. Analysis of differences between groups based on approximately normally distributed samples was analysed using the Student’s t-test. Samples severely skewed were analysed using an appropriate non-parametric test. When comparing differences between more than two groups, ANOVA was implemented combined with an appropriate post-hoc test. For analysis of measurements of the same individuals repeated over time, ANOVA for repeated measurements was used to validate main effects, interactions and inter-group differences.
Categorical data were typically tabulated and differences between cell frequencies were tested with the Chi-square test or Fisher’s exact test, whatever appropriate. Associations between non-normally distributed data was analysed with Spearman’s Rho. A P-value less than 0.05 was regarded as statistically significant.

Results
35
Results
HCC and general clinical outcome
Two patients died during the study period in the hospital. Cause of death was rupture of abdominal aortic aneurysm (I) and acute postoperative cerebral infarction (II).
The effects of HCC with respect to general clinical outcome are summarised in Figure 5. In brief, possible benefits of HCC included shorter LOS and shorter time to extubation (I). Also, lower postoperative blood loss (I, II) and fewer blood transfusions were noted (II). Results were generally, but not entirely, similar between studies (I, II).
The overall incidence of postoperative deviations among HCC-patients was not different from control patients (I, II). On the categorical level, patients using HCC had a lower incidence of neurological deviations in study I, but not in study II. Also, the occurrence of postoperative arrhythmias, most notably atrial fibrillation was lower in the HCC group (II). A summary of results is shown in Table 3.
Table 3. Overview of deviations from a normal postoperative course
Study 1 Study II
Deviation CBAS Control P-value CBAS Duraflo Control P-value
Overall 41 56 0.11 41 30 42 0.15
Arrhythmia 23 29 0.49 22 13 27 0.04
Coagulation 2 3 0.58 0 2 5 0.07
Infection 4 10 0.16 5 2 5 0.50
Neurology 2 15 0.01 5 4 6 0.94
Re-do 2 3 0.58 3 0 2 0.38
Respiration 11 10 0.92 5 4 2 0.64
Incident rates in percent (%). P-values denote χ2-tests based on frequencies of observed deviations.

Results
36
Figure 5. HCC and general clinical outcome ����� ������
&'
(
)
*(
*)
�%�� ������� �%�� ������� ����������
�
�
��+ $ ���
(*(,(-(
�%�� ������� �%�� ������� �������
�
� �� ���./��%�����
(
)
*(
*)
�%�� ������� �%�� ������� �������
�
���
����������0���� �1 �
(
,((
2((
3((
1((
*(((
�%�� ������� �%�� ������� �������
��
�
���44
� �� ��� ��������������������
(
*(
,(
-(
2(
)(
�%�� ������� �%�� ������� �������
5
����
Descriptors of clinical outcome and the influence of heparin coated circuits (HCC). Notation for statistical significance: Duraflo versus Control (* P<0.05, ** P<0.01), Duraflo versus CBAS (## P<0.01).

Results
37
HCC and renal function
The creatinine level increased significantly postoperatively as a sign of relative renal impairment (I, II). Use of HCC was shown to ameliorate the renal stress evident by significantly (P<0.01) lowering the perioperative creatinine elevation in both study I and II (Figure 6).
Figure 6. Heparin coated circuits and renal function ����� ������
(
)
*(
*)
,(
,)
�%�� ������� �%�� ������� �������
6���7�
88
88 88
Effects of heparin coated circuits on renal function as determined by the perioperative change of the creatinine level. Notation for statistical significance: ** P<0.01 versus control.
Effects of different types of HCC
Clinical outcome was very similar between patients using Duraflo and CBAS heparin coated circuits. No differences were identified for the incidence of postoperative deviations (P=0.14), atrial fibrillation (P=0.14), length of intensive care (P=0.84), time to extubation (P=0.75), length of stay in hospital (P=0.31), transfusion requirements (P=0.37) or renal function (P=0.96). Chest drain volume was however significantly lower in the Duraflo group 8 hours postoperatively: 464 ± 18 ml compared to 554 ± 22 ml in the CBAS-group (P=0.005).
Effects of HCC and PSB-retransfusion on release of protein S100B
CPB was associated with a significant (P<0.001) increase in systemic concentration of protein S100B (I, II, IV). Use of HCC appeared to reduce (P<0.01) the release of protein S100B (I), but could not be confirmed by study II (P=0.289).

Results
38
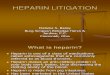
PSB contained substantial amounts of protein S100B (18 ± 1.7 µg/L) (IV). Retransfusion of PSB induced a profound increase of the systemic S100B concentration from 0.24 ± 0.001 µg/L to 1.42 ± 0.19 µg/L (IV). Protein S100B was effectively eliminated from the PSB after cell salvage processing (IV) (Figure 7).
Figure 7. Release of protein S100B during CPB and effects of PSB
(9(
(9,
(92
(93
(91
*9(
*9,
*92
*93
���
�� ���
�����
� ����� �
���
"������
��� ���� )���� � ��*
: 7&
�
�"
888
444
Retransfusion of pericardial suction blood (PSB) during CPB direct from the cardiotomy reservoir (CR) or after processing using a cell saver (CS) technique. Systemic concentration of protein S100B after retransfusion from CR (***) P<0.001 and on the first postoperative day compared with pre-surgery (###) P<0.001.
Effects of HCC and retransfusion of PSB on memory function
Use of CPB and exposure to cardiac surgery were associated with significant postoperative memory deficits, both within the domains of explicit (I, II) and implicit (IV) memory. Prevention of memory disturbances by means of HCC (I, II) or cell salvage processing of PSB (IV) proved to be non-effective (Figure 8).
Patient self-assessment of memory function 4 months after surgery revealed significant impairment of memory (II). Based on 6 specific questions of memory, patients reported the overall performance had decreased from 17.4 ± 0.1 to 14.7 ± 0.1 (P=0.001). However, these findings were not verified by the spouse (17.4 ± 0.1 – 17.6 ± 0.2) (P=0.801). Patients in the HCC-groups showed better memory scores (17.6 ± 0.4) than control group patients (14.3 ± 0.3) (P=0.021).

Results
39
Figure 8. Memory results
���� ��
(9,
(9,)
(9-
(9-)
(92
"��� �������������������
*9)
*91
,9*
,92
,9;
-
�<
=��$# �"��� ������
-
-9)
2
29)
)
)9)
3
�<
4
Perioperative memory results (I) showing the influence of heparin coated circuits during CPB. Versus preoperative score (#) P<0.05. CBAS (�) Control (�).
"��� �������������������
*9)
*91
,9*
,92
,9;
-
�<
���� ��
(9,
(9,)
(9-
(9-)
(92
=��$# �"��� ������
-
-9)
2
29)
)
)9)
3
�< 44
Perioperative memory results (II) showing the influence of two different heparin coated circuits during CPB. Versus preoperative score (# #) P<0.01. CBAS (�) Duraflo (�) Control (�).
$*9)
$*
$(9)
(
(9)
*
*9)
>
�
�"444
���� �� "��� ������������������� =��$# �" ��� ������
Perioperative memory results (IV) showing the influence of different retransfusion methods during CPB: cell saver (CS) technique and cardiotomy reservoir (CR). Versus preoperative memory score (# # #) P<0.001.

Results
40
Recycling of PSB: effects of free plasma haemoglobin (III)
The concentration of pHb in PSB was very high (3385 ± 457 mg/L). Direct recycling of PSB from the cardiotomy reservoir increased the systemic concentration of pHb from 41.4 ± 9.7 mg/L to 360.4 ± 42 mg/L (P<0.001). No systemic concentrations of pHb were measurable, however, if a cell salvage device was used to process the PSB before recycling (Figure 9).
Figure 9. Free plasma haemoglobin
(
*((
,((
-((
2((
���
���
�����
���� �
� �
���
.��
���
)�����
���
� ��* � �
� 7&
(
*(((
,(((
-(((
2(((
)(((
� 7&
888 ♥♥♥
♠♠♠
888
8
P-value refers to the inter-group difference (ANOVA). Difference at specific time points: (*** P<0.001, * P<0.05). Contrasts: Pre-CPB vs. End-CPB (♥♥♥ P<0.001) and Day 1 vs. End-CPB (♠♠♠ P<0.001) Cell Saver-group (�) Cardiotomy Reservoir-group (�).
Recycling of PSB: general inflammatory effects (III)
Surgery and CPB induced a significant systemic inflammatory response evident by markers of cytokines, complements and PMN granulocytes. The concentration of inflammatory markers was generally found to peak at termination of CPB, with the exception of IL-6, which continued to rise into the postoperative phase. TNF-α remained slightly elevated above preoperative levels throughout the perioperative period (Figure 10).
The collected volume of PSB (621 ± 54 ml) proved to represent a significant source of inflammation. The concentration of cytokines (IL-6, IL-8, TNF-α), MPO and complements (C3a) were significantly higher than what was found in the systemic circulation. Recycling of
�?(@((*

Results
41
PSB, directly from the cardiotomy reservoir or after cell saver processing gave no momentary systemic effects (Figure 10).
Figure 10. Inflammatory effects of PSB recycling IL-6 IL-8
(
*((
,((
-((
2((
������ �����
���� �
� �
���
.��
���
)�����
���
� ��* � �
� 7�
�
88
♥♥♥
♠♠♠
(
*((
,((
-((
2((
)((
3((
;((
������ �����
���� �
� �
���
.��
���
)�����
���
� ��* � �
� 7�
�
888
♥♥♥
TNF-α MPO
(
)
*(
*)
,(
������ �����
���� �
� �
���
.����� )�����
���
� ��* � �
� 7�
�
8
(
)(
*((
*)(
,((
,)(
���
���
�����
���� �
� �
���
.��
���
)�����
���
� ��* � �
� 7�
� ♥ ♥♥
♠♠♠
888
C3a TCC (SC5b-9)
(
)((
*(((
*)((
,(((
,)((
-(((
-)((
������ �����
���� �
� �
���
.��
���
)�����
���
� ��* � �
� 7�
�
88♥♥♥
AAA
(
*
,
-
2
)
������ �����
���� �
� �
���
.����� )�����
���
� ��* � �
� 7�
�
♥♥♥
♠♠♠
P-values refer to the inter-group difference (ANOVA). Contrasts: Pre-CPB vs. End-CPB (♥♥♥ P<0.001) and Day 1 vs. End-CPB (♠♠♠ P<0.001). Group identifiers: CS-group (�) CR-group (�).
�B(@--) �B(@1*)
�B(@2)- �B(@*C,
�B(@;,* �B(@,-C

General Discussion
42
General discussion
Cardiopulmonary bypass evokes a systemic inflammatory response syndrome [16, 50] that may impair normal organ function and contribute to postoperative morbidity [49, 153]. Use of HCC and alternative methods of PSB management offers two alternatives of reducing the inflammatory insult induced by CPB.
Perspectives on cardiopulmonary bypass
The EURO-score risk score [154] defines risk factors associated with cardiac surgery. The compiled information on 19030 patients did not find CPB to be a specific predictor of mortality [155]. Preliminary results from off-pump surgery indicate that CPB does not increase the risk of short-term adverse outcome [156]. Do differences in outcomes between on-pump and off-pump surgery exclude extracorporeal circulation as a specific risk factor? Probably not. This merely reflects the magnitude of complexity and difficulty in making appropriate interpretation of results in clinical research.
The general pattern of postoperative deviations [14] observed among cardiac patients is attributed to a wide range of preoperative risk-factors [154, 155]. The most important is probably the effect of old age [154]. Advanced age is closely related to degenerative processes of vital organs including cardiac and cerebral functions [80, 81, 85, 157]. Apart from the patient’s preoperative status as one crucial predictor of outcome [155], we also have to consider the impact of different therapeutic strategies. CPB represents one of those, though, the most important is probably the surgical treatment itself determined by surgical skill and smooth teamwork, but also the influence of anaesthetic and intensive care management, together with nursing competence and hospital organisational structure. The conditions for clinical research present a true challenge. Small effects due to different CPB-related strategies may be difficult to identify and relate to outcome.
Heparin coated circuits and clinical outcome
Our experience in using HCC (I, II) to reduce inflammatory responses [50, 58, 59, 158, 159] during CPB points to several possible clinical benefits. HCC appear to decrease both postoperative blood loss (I, II) and need for homologous blood transfusions (II). Moreover, a direct organ protective effect can be anticipated as demonstrated by the improved renal function (I, II). Analysis of postoperative deviations from the normal postoperative course revealed no overall outcome

General Discussion
43
effects of HCC (I, II). However, on a categorical level, HCC was associated with lower incidences of atrial fibrillation (II) and neurological deviations (I).
The blood saving effects of HCC (I, II) may in theory be attributed to the heparin surface per se or to the combined effect with systemically reduced heparin concentration. Heparin bound to the artificial surface is known to effectively blunt the initial contact activation of the intrinsic pathway governed by Hageman’s factor XII [160]. In addition, surgery initiates a concomitant major stimulus of the external pathway of the coagulation cascade through tissue factor VII, which only can be inhibited by systemically administered heparin [36]. The balance of internal and external activation of coagulation is of principal interest and determines to what extent HCC may reduce postoperative bleeding.
Heparin coated circuits and reduced systemic anticoagulation
CPB performed according to generally accepted anticoagulation protocols verified by ACT-levels of 480 seconds [161] is associated with a significant production of thrombin [37] suggesting a still ongoing activation of coagulation. The relative contribution of thrombin is less from the CPB-circuit than from the surgical trauma [36]. Use of HCC reduces only thrombin production mediated by the surface induced coagulation activity [162] and may explain why HCC in some cases have failed to lower the overall thrombin production [163, 164] as well as postoperative bleeding [20, 62, 165]. To appreciate stipulated benefits of HCC, limitations of extrinsic influences on coagulation are needed, which means restrictions of cardiotomy suction and retransfusion of PSB [40, 41, 59].
The group of Aldea [59] demonstrated recently the significance of thrombin derived from PSB and cardiotomy suction. Despite normal anticoagulation at ACT 480 seconds, use of cardiotomy suction was associated with significantly higher thrombin levels during CPB, than lowering the ACT-level to 250 seconds and use of HCC, if cardiotomy suction was excluded.
To what extent cardiotomy suction in our investigations may have masked these effects of HCC remains uncertain, since no analysis of coagulation parameters were performed. Plausible negative effects on coagulation were most likely minor, since a clear blood saving effect could be demonstrated (I, II). Øvrum et al. showed in a similar setting to ours that cardiotomy suction may be combined with HCC to achieve reductions in blood loss [166].

General Discussion
44
Intentionally lowering the systemic concentration of heparin to one third of the normal or to an ACT-level of 250 seconds (I, II) may seem dubious. Safety aspects have been raised [167, 168] and the methodology has not received universal acceptance. A few centres have adopted the low-dose regime on a routine basis and report in accordance with our experience (I, II) excellent clinical results without any complications, with respect to the management of coagulation [58, 169].
Controversies and possibilities of heparin coated circuits
The theoretical basis for using HCC to improve clinical outcome is based on its inherent ability to reduce inflammatory responses [50, 158, 159, 166]. Unfortunately, we do not know the level at which biological response modifiers are effective to safeguard normal organ functions [34]. In the complex setting of cardiac surgery it has so far been difficult to clearly show to what extent HCC may protect vital organs and in a wider perspective to alter clinical outcome [21, 62, 159, 164, 170]. Videm et al. [21] identified a significant reduction of complement and granulocyte activation among high-risk patients exposed to HCC, without being able to relate these effects to a reduction of postoperative complications. In a European multicenter study comprising 805 low-risk patients there were no clear effects shown with respect to clinical end-points and HCC usage [62]. Our own findings (I, II) in a well-controlled situation indicate that benefits of HCC from broad clinical viewpoints are probably small, but still present. The overall incidence of postoperative deviations was similar among HCC and control patients. HCC’s ability to reduce atrial fibrillation (II) agrees with previous findings [20, 171] and may be due to an antiinflammatory effect [171]. The reported lower rate of neurological deviations (I) was most likely due to a relative overrepresentation in the control group due to chance (I). Symptoms of dysphasia, pareses, impaired vision and balance & co-ordination disturbances would normally not be mediated by variations in inflammatory impulses. An etiology based on embolic events would seem more probable [81]. We were able to trace a significant improvement in renal function based on the postoperative elevation of the creatinine level, which was clearly lower among patients exposed to HCC (I, II). It is likely that a reduction of the inflammatory responses may explain this reaction. HCC are known to dampen production of cytokines [172], complements [55, 173] and PMN neutrophils [55, 174]. To isolate the exact mechanism was not possible with the implemented study design. Consequences of kidney dysfunction may be severe and are associated with prolonged intensive and hospital stay [175], which is why the isolated discovery of improved kidney function may be important (I, II). Interpretation of time and resource related outcome-

General Discussion
45
measures is restricted by influences of organisational routines. Findings of shortened hospital stay (I) and need for postoperative mechanical ventilation (I) should therefore be interpreted with caution, especially since inter-study (I→II) reproducibility was not accomplished.
Reasons for existing controversy [158] regarding effects of HCC during clinical CPB may have methodological implications [60]. Assumptions reflecting the efficacy of HCC are based on a range of different study designs and inference of results and outcome becomes cumbersome. An internal meta-analysis of HCC usage at our institution gave the following results [176]: the overall incidence of postoperative deviation was significantly lowered promoting smoothness of postoperative care (Figure 11). Moreover, favourable results were found with respect to length of stay in hospital, time to extubate, less postoperative coagulation disturbance, less blood- and haemoglobin loss accompanied with fewer blood transfusions. Benefits of HCC with regards to improved renal function were confirmed (I, II) and were in concordance with findings of Ranucci et al. [22].
05
101520253035404550
Heparin Coated Circuits Control Circuits
%
Figure 11. Influence of HCC on the incidence of postoperative deviations. Difference between groups: P=0.035.
Heparin coated circuits and neurological outcome
Occurrence of devastating neurological complications [81] and development of cognitive dysfunction [82] depict two major limitations of current cardiac surgical techniques. Recognition of the problem has prompted researchers to identify risk factors [177-179] and promote changes for improvements, with focus both on surgical and CPB-related aspects. Arterial-line filtration [77], alpha-stat management [180], temperature control [90] and strict regulation of systemic blood pressure [181] are some of the measures already implemented.

General Discussion
46
Inflammatory reactions during CPB are suspected to affect normal organ functions [18, 42, 49]. To what extent these impinge on cerebral functions is not clear [182]. Appearance of transient and generalised cerebral oedema post surgery may have at least in part an inflammatory genesis [91, 183]. Protease inhibitors have been shown to protect the brain from adverse reactions [184]. Use of HCC offers another form of protection against inflammatory reactions affecting the brain. To our knowledge, there exists to date only one published study in which this hypothesis has been tested [92]: outcome gave indications of a causal relationship between cognitive disturbance and use of HCC.
Heparin coated circuits and memory
Based on a large sample of patients admitted for routine coronary artery surgery, we found that HCC gave no protection against development of postoperative memory deficits (I, II). Identified deficits were moderate and only one out of three tests indicated a significant decline of memory performance (I, II). Interpretation of these results would suggest that surgery and CPB generate relatively mild effects upon memory performance. Secondly, since the identified deficits of explicit memory were insensitive to the exposure of HCC it would suggest processes other then inflammation as primary causative mechanisms.
Pericardial suction blood and memory
It is intriguing that elimination of PSB during CPB by use of cell salvage gave no effects on memory performance (IV). Explicit memory remained within normal range, both before and after surgery. Implicit memory performance deteriorated after surgery, however, unrelated to retransfusion of PSB (IV). Reasons for this reaction remain unclear. The volume of PSB retransfused was low (~600 ml), which may have limited the load of emboli to the brain. PSB-composition was analysed with respect to inflammatory markers (III), but not with respect to other components (IV). Despite the rather high concentrations of inflammatory markers in PSB, the elevation of the systemic concentration after PSB-retransfusion was generally insignificant, with the exception of free plasma haemoglobin and protein S100B (III). It seems therefore unlikely that the inflammatory reaction of re-administering PSB to the systemic circulation had any effects upon the brain. One would also assume that other potentially deleterious ingredients of PSB also were in insufficient concentrations to impair memory.

General Discussion
47
Cognitive dysfunction: methodological implications and current status
The observed rate of cognitive disturbances after cardiac surgery is gradually decreasing. The generally accepted high incidences of brain injury reported by Åberg in 1974 [77] and Shaw in 1986 ranged up to 78% [185] and are no longer current for today’s clinical practice. In a recent review by van Dijk the mean rate of cognitive disturbance was reported at 22.5% [82]. Accepted norms of cognitive decline after cardiac surgery are lacking, which may explain why incident rates vary considerably [84, 95, 97]. Interpretation of cognitive test scores in terms of clinical significance or impact on quality of life should also be considered [94].
One of the few publications referring neuropsychological outcome to a non-surgical matched control group was recently published by Selnes and collaborates [186]. In the late follow-up at 3 months and 1 year after surgery no differences were identified compared to control subjects. Authors conclude that early decline of cognitive function after surgery is transient and reversible [186], which diverges from previous understanding of a close connection between early and late outcome as proclaimed by the group of Newman et al. [75]. Some authors are even questioning if use of cardiopulmonary bypass still is the cause to cognitive dysfunction [187]. Emerging experience from off-pump surgery [188, 189] and angioplasty [96, 190] would support this provocative argument. Cognitive status seems to differ very little between CPB-patients compared to off-pump and angioplasty patient-groups. The procedure of CPB in its current status is by no means perfect, but there is reason to believe that the impact on cognitive disturbances is less than once believed.
We have no explanation to the still existing memory deficits encountered in our studies (I, II, IV). Since exclusion of cardiotomy suction (IV) and incorporation of HCC (I, II) were ineffective, other causes and strategies of prevention should be considered. To refine the interpretation of our memory results (I, II), data were in a recent publication from our group re-analysed and transformed into Z-scores [139]. It was revealed that 39.5% of the patients demonstrated a decline of explicit memory function exceeding 1 SD. Together with the verified implicit memory dysfunction identified in study IV, our data suggest that short term memory disturbances are still prevalent after cardiac surgery.
This thesis is limited by not having a long-term follow-up of intraoperative memory results using the same battery of tests. As a compromise solution a questionnaire was sent out 4 months after the

General Discussion
48
operation to obtain some insight concerning the post-hospital period (II). Results revealed sustained memory impairments as reported by the patients, though the spouses did not confirm these alterations. Use of questionnaires may be criticised as being less powerful to capture subtle memory deficits than performing the ordinary test battery. Nonetheless, subjective self-rating has been shown to correlate with results obtained from objective computer-based systems [191]. When resources are limited, the option of employing questionnaires may therefore be attractive. Two recent reports based on self-rating confirm our findings that decline of cognition and memory may persist after the surgical intervention. The disparity between ratings of memory performance between spouse and patients is of interest (II) and would suggest that the patient’s ratings were the more sensitive. In contrast there are the findings of Bergh et al., who report similar ratings from both patient and spouse [96].
The protein S100B
The protein S100B was believed for a long time to be the ideal marker of brain cell injury after cardiac surgery. This was the situation when the first trials of this thesis were conducted (I, II). After the detection of the protein S100B outside of the CNS, especially in shed blood used for autotransfusion during cardiac surgery [136, 142], most researchers have re-evaluated the usefulness of S100B as a reliable marker for monitoring of injuries to the brain [192].
The initial findings of HCC’s ability to decrease the release of protein S100B during CPB seemed promising and were at that time believed to represent decreased brain injury (I, II). We were later able to confirm the findings of Jönsson [136] and Anderson [142] that protein S100B is not brain specific (IV).
Protein S100B may be effectively removed from PSB by use of cell salvage (IV). The remaining release of S100B seen during CPB can then resemble the amounts associated with off-pump surgery [142]. It is not known exactly what triggers that smaller, but still significant release of S100B (IV). S100B may have arisen from a cerebral source; though, no correlations were identified between S100B concentrations at any time point versus memory performance (IV). Absorption of protein S100B from traumatised non-cerebral tissue during the surgical procedure may be one plausible explanation [130].
Closing remarks
More than ten years of experience of HCC [193] based on numerous clinical investigations [20, 22, 55, 59, 165, 166, 169, 194-197] now

General Discussion
49
suggests that important clinical benefits are achieved by HCC usage. HCC as an integral part of the extracorporeal circulation technology seems warranted, based on our own findings [176, 198, 199] and in concordance with others.
Measures of inflammatory markers in the systemic circulation and indices of memory function would suggest that use of cardiotomy suction for PSB-salvage is safe (III, IV). However, any reasonable means to avoid exposing patients to inflammatory mediators and other potentially harmful constituents of PSB should be explored.

Conclusions
50
Conclusions
• Use of heparin coated circuits is associated with improved clinical outcomes with respect to hospital stay, renal function, postoperative complications, blood loss and blood transfusions.
• Pericardial suction blood contains significant concentrations of proinflammatory cytokines, neutrophils, complements, protein S100B and free plasma haemoglobin.
• Cardiac surgery with use of cardiopulmonary bypass is associated with postoperative memory disturbances that were found to be unrelated to the use of heparin coated circuits and cardiotomy suction.
• Retransfusion of pericardial suction blood using cardiotomy suction increases the systemic concentrations of protein S100B and free plasma haemoglobin.
• Protein S100B is unsuitable as a marker of cerebral injury in conjunction with cardiac surgery due to its high presence in pericardial suction blood.

Acknowledgements
51
Acknowledgements
I would like to express my sincere gratitude to Torkel Åberg. He provided me the time and facilities to enable a rewarding research process. He has my greatest respect for his mentorship and wisdom for which I will remain ever thankful.
Thomas Karlsson knows everything there is to know about memory. He has my thanks for truly supporting my research activities over the years and for giving me comfort and encouragement when I needed it the most.
Gunnar Engström opened doors that I did not know existed. Research all of a sudden had a new dimension. His way of ‘lateral thinking’ will eventually lead to something big.
Perhaps, the most important of all is the perfusionist group: Sören Häggmark, Erica Jansson, Ronny Lindholm, Micael Appelblad and Lena Lindholm. Without their everyday support, research would have been a nightmare. Many thanks for never giving up and for always being my friends.
Erik Sandström, co-author and friend, willingly introduced me into the field of protein S100.
Berith Lundström provided excellent and professional technical assistance and laboratory skill.
I would also like to express my gratitude to all friends in the operating theatre and the wards for so loyally supporting my research.
Apart from all support at work, doing research would have been impossible without the understanding and love from my family. Thank you Barbro, Pontus, Anna and Magnus.

Populärvetenskaplig sammanfattning på svenska
52
Populärvetenskaplig sammanfattning på svenska
Hjärtkirurgiska ingrepp kräver ofta att hjärtats och lungornas funktion tillfälligt måste upprätthållas av en hjärt-lungmaskin. Behandlingen ger upphov till en rad biverkningar. Vårt immunförsvar reagerar när blodet når kontakt med främmande material i hjärt-lungmaskinen genom att utlösa en kedja av inflammatoriska reaktioner. Ett liknade mönster ses även när blod tillvaratas från operationsområdet och återförs via hjärt-lungmaskinen till patientens cirkulation.
I vissa fall kan inflammationsreaktioner påverka normal organfunktion och förlänga och komplicera det postoperativa förloppet. En påverkan av hjärnans funktioner kan inte uteslutas.
Att applicera heparin på hjärt-lungmaskinens kontaktytor är ett sätt att efterlikna kroppens egna blodkärl. Heparinytan minskar den inflammatoriska reaktionen och gör blodets passage genom hjärt-lungmaskinen mer fysiologisk. En ytterligare inflammationshämmande åtgärd är att återtransfundera kirurgisk blödning med en blodåtervinningsmaskin. Här avskiljs blodplasma med innehåll av inflammationsprodukter och endast de röda blodkropparna återförs till patienten.
Avhandlingen baseras på fyra (I-IV) kliniska studier omfattande sammanlagt 475 patienter. Samtliga patienter genomgick kranskärlskirurgi med användande av hjärt-lungmaskin.
Effekter av inflammationshämmande åtgärder bedömdes utifrån allmänna kliniska parametrar, koncentrationsförändringar av inflammationsmarkörer, samt påverkan av njurarnas och hjärnans funktioner. Kreatinin användes som markör för njurfunktion och protein S100B för att bedöma graden av eventuell hjärnskada. Dessutom utfördes minnestest.
Följande resultat erhölls: användning av hepariniserade ytor minskade blödning (I, II) och transfusionsbehov (II). Sjukhusvistelse (I) och tid för andningsstöd efter operationen (I) förkortades. Vidare observerades färre hjärtrytmrubbningar (II) och neurologiska avvikelser (I), samt lägre frisättning av protein S100B (I, II) och kreatinin (I, II).
Trots höga halter av olika inflammationsmarkörer i blodet från operationsområdet gav direkt återtransfusion via hjärt-lungmaskinen ingen tydlig inflammationspåverkan, undantag var S100B och fritt plasma hemoglobin. Återtransfusion med blodåtervinningsmaskin gav ingen påvisbar inflammationsreaktion alls (III, IV).

Populärvetenskaplig sammanfattning på svenska
53
Användande av hjärt-lungmaskin var förknippat med en frisättning av protein S100B, trots att S100B från blod i brösthålan eliminerats (IV). Denna frisättning torde inte indikera hjärnskada.
Subtila minnesstörningar kunde konstateras, vilka inte kunde relateras till frisättning av S100B (IV), användandet av heparinbehandlade ytor (I, II) eller återtransfusion av blod (IV). S100B är olämplig som markör av hjärnskada, då S100B finns i höga koncentrationer utanför hjärnan.

References
54
References
1. Gibbon JHJ. Application of a mechanical heart and lung apparatus to cardiac surgery. Minn Med 1954;37:171-85.
2. Crafoord C, Norberg B, Senning A. Clinical studies in extracorporeal circulation with a heart-lung machine. Acta Chir Scand 1957;112:200.
3. Rygg IH, Kyvsgaard E. A disposable polyethylene oxygenator system applied in the heart/lung machine. Acta Chir Scand 1956;112:433-7.
4. Kirklin JW, DuShane JW, Patrick RT. Intracardiac surgery with the aid of a mechanical pump oxygenator system (Gibbon type): report of eight cases. Proc Mayo Clin 1955;30:201-6.
5. Lillehei CW, DeWall RA, Read RC. Direct vision intracardiac surgery in man using a simple, disposiable artificial oxygenator. Dis Chest 1956;29:1-8.
6. Lillehei CW, Varco RL, Ferlic RM et al. Results in the first 2,500 patients undergoing open-heart surgery at the University of Minnesota Medical Center. Surgery 1967;62(4):819-32.
7. DeWall RA, Bentley DJ, Hirose M et al. A temperature controlling (omnithermic) disposable bubble oxygenator for total body perfusion. Dis Chest 1966;49(2):207-11.
8. Kolff WJ, Effler DB, Groves LJ. Disposable membrane oxygenator (heart-lung machine) and its use in experimental surgery. Cleve Clin Q 1956;23:69-97.
9. Osborn JJ, Bramson ML, Main FB et al. Clinical experience with a disposable membrane oxygenator. Bull Soc Int Chir 1966;25(4):346-53.
10. Lande AJ, Dos SJ, Carlson RG. A new membrane oxygenator-dialyzer. Surg Clin North Am 1967;47:1461-70.
11. Shumacker HB. Birth of an idea and the development of cardiopulmonary bypass. In: Gravlee G, David RF, Kurusz M, Utley JR eds. Cardiopulmonary Bypass Principles and Practice. Philadelphia: Lippincott Williams &Wilkins, 2000 : 22-34.
12. Puskas JD, Williams WH, Duke PG et al. Off-pump coronary artery bypass grafting provides complete revascularization with reduced myocardial injury, transfusion requirements, and length

References
55
of stay: A prospective randomized comparison of two hundred unselected patients undergoing off-pump versus conventional coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003;125(4):797-808.
13. Grover FL. The Society of Thoracic Surgeons National Database: current status and future directions. Ann Thorac Surg 1999;68(2):367-73.
14. Åberg T, Svenmarker S, Hohner P et al. Routine registration of deviations from the norm in cardiac surgery: a potent clinical research tool and quality assurance measure. Eur J Cardiothorac Surg 1997;11(1):10-2.
15. Svenmarker S, Häggmark S, Jansson E et al. Quality assurance in clinical perfusion. Eur J Cardiothorac Surg 1998;14:409-14.
16. Kirklin JK, Westaby S, Blackstone EH et al. Complement and the damaging effects of cardiopulmonary bypass. J Thorac Cardiovasc Surg 1983;86(6):845-57.
17. Edmunds Jr LH. Blood-surface interactions during cardiopulmonary bypass. J Card Surg 1993;8(3):404-10.
18. Asimakopoulos G. Systemic inflammation and cardiac surgery: an update. Perfusion 2001;16(5):353-60.
19. Quartin AA. Magnitude and duration of the effect of sepsis on survival. Department of Veterans Affairs Systemic Sepsis Cooperative Studies Group. JAMA 1997;277(13):1058-63.
20. Baufreton C, Le Besnerais P, Jansen P et al. Clinical outcome after coronary surgery with heparin-coated extracorporeal circuits for cardiopulmonary bypass. Perfusion 1996;11(6):437-43.
21. Videm V, Mollnes TE, Fosse E et al. Heparin-coated cardiopulmonary bypass equipment. I. Biocompatibility markers and development of complications in a high-risk population. J Thorac Cardiovasc Surg 1999;117(4):794-802.
22. Ranucci M, Mazzucco A, Pessotto R et al. Heparin-coated circuits for high-risk patients: a multicenter, prospective, randomized trial. Ann Thorac Surg 1999;67(4):994-1000.
23. Bone RC. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992;101(6):1644-55.

References
56
24. Monsinjon T, Richard V, Fontaine M. Complement and its implications in cardiac ischemia/reperfusion: strategies to inhibit complement. Fundam Clin Pharmacol 2001;15(5):293-306.
25. Andersen LW, Landow L, Baek L et al. Association between gastric intramucosal pH and splanchnic endotoxin, antibody to endotoxin, and tumor necrosis factor-alpha concentrations in patients undergoing cardiopulmonary bypass. Crit Care Med 1993;21(2):210-7.
26. Laffey JG, Boylan JF, Cheng DC. The systemic inflammatory response to cardiac surgery: implications for the anesthesiologist. Anesthesiology 2002;97(1):215-52.
27. Hornick P, Taylor KM. Immune and inflammatory responses after caridopulmonary bypass. In: Gravlee GP, David RF, Kurusz M, Utely JR eds. Cardiopulmonary bypass principles and practice. Philadelphia: Lippincott Williams & Wilkins, 2000 : 303-17.
28. Videm V, Mollnes TE, Bergh K et al. Heparin-coated cardiopulmonary bypass equipment. II. Mechanisms for reduced complement activation in vivo. J Thorac Cardiovasc Surg 1999;117(4):803-9.
29. Bruins P, te Velthuis H, Eerenberg-Belmer AJ et al. Heparin-protamine complexes and C-reactive protein induce activation of the classical complement pathway: studies in patients undergoing cardiac surgery and in vitro. Thromb Haemost 2000;84(2):237-43.
30. Bruins P, te Velthuis H, Yazdanbakhsh AP et al. Activation of the complement system during and after cardiopulmonary bypass surgery: postsurgery activation involves C-reactive protein and is associated with postoperative arrhythmia. Circulation 1997;96(10):3542-8.
31. Fitch JC, Rollins S, Matis L et al. Pharmacology and biological efficacy of a recombinant, humanized, single-chain antibody C5 complement inhibitor in patients undergoing coronary artery bypass graft surgery with cardiopulmonary bypass. Circulation 1999;100(25):2499-506.
32. Kelso A. Cytokines: principles and prospects. Immunol Cell Biol 1998;76(4):300-17.
33. McBride WT, Armstrong MA, Crockard AD et al. Cytokine balance and immunosuppressive changes at cardiac surgery: contrasting response between patients and isolated CPB circuits. Br J Anaesth 1995;75(6):724-33.

References
57
34. Antonelli M. Sepsis and septic shock: pro-inflammatory or anti-inflammatory state? J Chemother 1999;11(6):536-40.
35. Brister SJ, Ofosu FA, Buchanan MR. Thrombin generation during cardiac surgery: is heparin the ideal anticoagulant? Thromb Haemost 1993;70(2):259-62.
36. Boisclair MD, Lane DA, Philippou H et al. Mechanisms of thrombin generation during surgery and cardiopulmonary bypass. Blood 1993;82(11):3350-7.
37. Koster A, Fischer T, Praus M et al. Hemostatic activation and inflammatory response during cardiopulmonary bypass: impact of heparin management. Anesthesiology 2002;97(4):837-41.
38. Shore-Lesserson L, Gravlee GP. Anticoagulation for Cardiopulmonary Bypass. In: Gravlee GP, Davis RF, Kurusz M, Utley JR eds. Cardiopulmonary Bypass Priniciples and Practice. Philadelphia: Lippincott Williams & Wilkins, 2000 : 435-72.
39. Burman JF, Chung HI, Lane DA et al. Role of factor XII in thrombin generation and fibrinolysis during cardiopulmonary bypass. Lancet 1994;344(8931):1192-3.
40. Chung JH, Gikakis N, Rao AK et al. Pericardial blood activates the extrinsic coagulation pathway during clinical cardiopulmonary bypass. Circulation 1996;93(11):2014-8.
41. Tabuchi N, de Haan J, Boonstra PW et al. Activation of fibrinolysis in the pericardial cavity during cardiopulmonary bypass. J Thorac Cardiovasc Surg 1993;106(5):828-33.
42. Boyle EM, Pohlman TH, Johnson MC et al. Endothelial cell injury in cardiovascular surgery: the systemic inflammatory response. Ann Thorac Surg 1997;63(1):277-84.
43. Elliott MJ, Finn AH. Interaction between neutrophils and endothelium. Ann Thorac Surg 1993;56(6):1503-8.
44. Moen O, Hogasen K, Fosse E et al. Attenuation of changes in leukocyte surface markers and complement activation with heparin-coated cardiopulmonary bypass. Ann Thorac Surg 1997;63(1):105-11.
45. Nilsson L, Tydén H, Johansson O et al. Bubble and membrane oxygenators--comparison of postoperative organ dysfunction with special reference to inflammatory activity. Scand J Thorac Cardiovasc Surg 1990;24(1):59-64.

References
58
46. Faymonville ME, Pincemail J, Duchateau J et al. Myeloperoxidase and elastase as markers of leukocyte activation during cardiopulmonary bypass in humans. J Thorac Cardiovasc Surg 1991;102(2):309-17.
47. Tonz M, Mihaljevic T, von Segesser LK et al. Acute lung injury during cardiopulmonary bypass. Are the neutrophils responsible? Chest 1995;108(6):1551-6.
48. Williams HJ, Rebuck N, Elliott MJ et al. Changes in leucocyte counts and soluble intercellular adhesion molecule-1 and E-selectin during cardiopulmonary bypass in children. Perfusion 1998;13(5):322-7.
49. Holmes JH, Connolly NC, Paull DL et al. Magnitude of the inflammatory response to cardiopulmonary bypass and its relation to adverse clinical outcomes. Inflamm Res 2002;51(12):579-86.
50. Wan S, LeClerc JL, Vincent JL. Inflammatory response to cardiopulmonary bypass: mechanisms involved and possible therapeutic strategies. Chest 1997;112(3):676-92.
51. Larm O, Larsson R, Olsson P. A new non-thrombogenic surface prepared by selective covalent binding of heparin via a modified reducing terminal residue. Biomater Med Devices Artif Organs 1983;11(2-3):161-73.
52. Olsson P, Sanchez J, Mollnes TE et al. On the blood compatibility of end-point immobilized heparin. J Biomater Sci Polym Ed 2000;11(11):1261-73.
53. Toomasian JM, Hsu LC, Hirschl RB et al. Evaluation of Duraflo II heparin coating in prolonged extracorporeal membrane oxygenation. ASAIO Trans 1988;34(3):410-4.
54. Ovrum E, Tangen G, Oystese R et al. Comparison of two heparin-coated extracorporeal circuits with reduced systemic anticoagulation in routine coronary artery bypass operations. J Thorac Cardiovasc Surg 2001;121(2):324-30.
55. Ovrum E, Mollnes TE, Fosse E et al. Complement and granulocyte activation in two different types of heparinized extracorporeal circuits. J Thorac Cardiovasc Surg 1995;110(6):1623-32.
56. Weber N, Wendel HP, Ziemer G. Quality assessment of heparin coatings by their binding capacities of coagulation and complement enzymes. J Biomater Appl 2000;15(1):8-22.

References
59
57. von Segesser LK, Weiss BM, Garcia E et al. Reduction and elimination of systemic heparinization during cardiopulmonary bypass. J Thorac Cardiovasc Surg 1992;103(4):790-8.
58. Ovrum E, Brosstad F, Am Holen E et al. Complete heparin-coated (CBAS) cardiopulmonary bypass and reduced systemic heparin dose; effects on coagulation and fibrinolysis. Eur J Cardiothorac Surg 1996;10(6):449-55.
59. Aldea GS, Soltow LO, Chandler WL et al. Limitation of thrombin generation, platelet activation, and inflammation by elimination of cardiotomy suction in patients undergoing coronary artery bypass grafting treated with heparin-bonded circuits. J Thorac Cardiovasc Surg 2002;123(4):742-55.
60. Westaby S. Commentary on clinical evaluation of Duraflow II heparin treated extracorporeal circulation circuits. Eur J Cardiothorac Surg 1997;11:624-5.
61. Silber JH, Rosenbaum PR, Schwartz JS et al. Evaluation of the complication rate as a measure of quality of care in coronary artery bypass graft surgery. JAMA 1995;274(4):317-23.
62. Wildevuur CR, Jansen PG, Bezemer PD et al. Clinical evaluation of Duraflo II heparin treated extracorporeal circulation circuits (2nd version). The European Working Group on heparin coated extracorporeal circulation circuits. Eur J Cardiothorac Surg 1997;11(4):616-23.
63. Mulholland JW, Massey W, Shelton JC. Investigation and quantification of the blood trauma caused by the combined dynamic forces experienced during cardiopulmonary bypass. Perfusion 2000;15(6):485-94.
64. Wright G, Sanderson JM. Cellular aggregation and trauma in cardiotomy suction systems. Thorax 1979;34(5):621-8.
65. Boonstra PW, van Imhoff GW, Eysman L et al. Reduced platelet activation and improved hemostasis after controlled cardiotomy suction during clinical membrane oxygenator perfusions. J Thorac Cardiovasc Surg 1985;89(6):900-6.
66. Moody DM, Bell MA, Challa VR et al. Brain microemboli during cardiac surgery or aortography. Ann Neurol 1990;28(4):477-86.
67. Moody DM, Brown WR, Challa VR et al. Brain microemboli associated with cardiopulmonary bypass: a histologic and

References
60
magnetic resonance imaging study. Ann Thorac Surg 1995;59(5):1304-7.
68. Brooker RF, Brown WR, Moody DM et al. Cardiotomy suction: a major source of brain lipid emboli during cardiopulmonary bypass. Ann Thorac Surg 1998;65(6):1651-5.
69. Kaza AK, Cope JT, Fiser SM et al. Elimination of fat microemboli during cardiopulmonary bypass. Ann Thorac Surg 2003;75(2):555-9.
70. Jewell AE, Akowuah EF, Suvarna SK et al. A prospective randomised comparison of cardiotomy suction and cell saver for recycling shed blood during cardiac surgery. Eur J Cardiothorac Surg 2003;23(4):633-6.
71. Engström KG, Appelblad M. Fat reduction in pericardial suction blood by spontaneous density separation: an experimental model on human liquid fat versus soya oil. Perfusion 2003;18(1):39-45.
72. Appelblad M, Engström G. Fat contamination of pericardial suction blood and its influence on in vitro capillary-pore flow properties in patients undergoing routine coronary artery bypass grafting. J Thorac Cardiovasc Surg 2002;124(2):377-86.
73. Kincaid EH, Jones TJ, Stump DA et al. Processing scavenged blood with a cell saver reduces cerebral lipid microembolization. Ann Thorac Surg 2000;70(4):1296-300.
74. Reents W, Babin-Ebell J, Misoph MR et al. Influence of different autotransfusion devices on the quality of salvaged blood. Ann Thorac Surg 1999;68(1):58-62.
75. Newman MF, Kirchner JL, Phillips-Bute B et al. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med 2001;344(6):395-402.
76. Branthwaite MA. Neurological damage related to open-heart surgery. Thorax 1972;27:748-53.
77. Åberg T. Effect of open heart surgery on intellectual function. Scand J Thorac Cardiovasc Surg Suppl 1974;15:1-63.
78. Åberg T, Ronquist G, Tyden H et al. Adverse effects on the brain in cardiac operations as assessed by biochemical, psychometric, and radiologic methods. J Thorac Cardiovasc Surg 1984;87(1):99-105.

References
61
79. Fearn SJ, Pole R, Wesnes K et al. Cerebral injury during cardiopulmonary bypass: emboli impair memory. J Thorac Cardiovasc Surg 2001;121(6):1150-60.
80. Murkin JM. Etiology and incidence of brain dysfunction after cardiac surgery. J Cardiothorac Vasc Anesth 1999;13(4 SUPPL 1):12-7.
81. Roach GW, Kanchuger M, Mangano CM et al. Adverse cerebral outcomes after coronary bypass surgery. Multicenter Study of Perioperative Ischemia Research Group and the Ischemia Research and Education Foundation Investigators. N Engl J Med 1996;335(25):1857-63.
82. van Dijk D, Keizer AM, Diephuis JC et al. Neurocognitive dysfunction after coronary artery bypass surgery: a systematic review. J Thorac Cardiovasc Surg 2000;120(4):632-9.
83. Shaw PJ, Bates D, Cartlidge NE et al. An analysis of factors predisposing to neurological injury in patients undergoing coronary bypass operations. Q J Med 1989;72(267):633-46.
84. Murkin JM, Newman SP, Stump DA et al. Statement of consensus on assessment of neurobehavioral outcomes after cardiac surgery. Ann Thorac Surg 1995;59(5):1289-95.
85. Davila-Roman VG, Barzilai B, Wareing TH et al. Atherosclerosis of the ascending aorta. Prevalence and role as an independent predictor of cerebrovascular events in cardiac patients. Stroke 1994;25(10):2010-6.
86. van der Linden J, Hadjinikolaou L, Bergman P et al. Postoperative stroke in cardiac surgery is related to the location and extent of atherosclerotic disease in the ascending aorta. J Am Coll Cardiol 2001;38(1):131-5.
87. Brown WR, Moody DM, Challa VR et al. Longer duration of cardiopulmonary bypass is associated with greater numbers of cerebral microemboli. Stroke 2000;31(3):707-13.
88. van der Linden J, Casimir-Ahn H. When do cerebral emboli appear during open heart operations? A transcranial Doppler study. Ann Thorac Surg 1991;51(2):237-41.
89. Newman MF, Croughwell ND, Blumenthal JA et al. Effect of aging on cerebral autoregulation during cardiopulmonary bypass. Association with postoperative cognitive dysfunction. Circulation 1994;90(5 PT 2):II243-9.

References
62
90. Grigore AM, Grocott HP, Mathew JP et al. The rewarming rate and increased peak temperature alter neurocognitive outcome after cardiac surgery. Anesth Analg 2002;94(1):4-10.
91. Anderson RE, Li TQ, Hindmarsh T et al. Increased extracellular brain water after coronary artery bypass grafting is avoided by off-pump surgery. J Cardiothorac Vasc Anesth 1999;13(6):698-702.
92. Heyer EJ, Lee KS, Manspeizer HE et al. Heparin-bonded cardiopulmonary bypass circuits reduce cognitive dysfunction. J Cardiothorac Vasc Anesth 2002;16(1):37-42.
93. Diegeler A, Hirsch R, Schneider F et al. Neuromonitoring and neurocognitive outcome in off-pump versus conventional coronary bypass operation. Ann Thorac Surg 2000;69(4):1162-6.
94. Newman MF, Grocott HP, Mathew JP et al. Report of the substudy assessing the impact of neurocognitive function on quality of life 5 years after cardiac surgery. Stroke 2001;32(12):2874-81.
95. Mahanna EP, Blumenthal JA, White WD et al. Defining neuropsychological dysfunction after coronary artery bypass grafting. Ann Thorac Surg 1996;61(5):1342-7.
96. Bergh C, Backstrom M, Jonsson H et al. In the eye of both patient and spouse: memory is poor 1 to 2 years after coronary bypass and angioplasty. Ann Thorac Surg 2002;74(3):689-93.
97. Blumenthal JA, Mahanna EP, Madden DJ et al. Methodological issues in the assessment of neuropsychologic function after cardiac surgery. Ann Thorac Surg 1995;59(5):1345-50.
98. Browne SM, Halligan PW, Wade DT et al. Cognitive performance after cardiac operation: implications of regression toward the mean. J Thorac Cardiovasc Surg 1999;117(3):481-5.
99. Bruggemans EF, Van de Vijver FJ, Huysmans HA. Assessment of cognitive deterioration in individual patients following cardiac surgery: correcting for measurement error and practice effects. J Clin Exp Neuropsychol 1997;19(4):543-59.
100. Moore BW. A soluble protein characteristic of the nervous system. Biochem Biophys Res Commun 1965;19(6):739-44.
101. Isobe T, Okuyama T. The amino-acid sequence of the alpha subunit in bovine brain S-100a protein. Eur J Biochem 1981;116(1):79-86.

References
63
102. Zimmer DB, Cornwall EH, Landar A et al. The S100 protein family: history, function, and expression. Brain Res Bull 1995;37(4):417-29.
103. Stefansson K, Wollmann RL, Moore BW. Distribution of S-100 protein outside the central nervous system. Brain Res 1982;234(2):309-17.
104. Schafer BW, Fritschy JM, Murmann P et al. Brain S100A5 is a novel calcium-, zinc-, and copper ion-binding protein of the EF-hand superfamily. J Biol Chem 2000;275(39):30623-30.
105. Donato R. Functional roles of S100 proteins, calcium-binding proteins of the EF-hand type. Biochim Biophys Acta 1999;1450(3):191-231.
106. Donato R. S100: a multigenic family of calcium-modulated proteins of the EF-hand type with intracellular and extracellular functional roles. Int J Biochem Cell Biol 2001;33(7):637-68.
107. Donato R. S100 proteins. Cell Calcium 1986;7:123-45.
108. Van Eldik LJ, Zimmer WE, Barger SW et al. Perturbation of the calmodulin system in transformed cells. Adv Exp Med Biol 1990;269:111-20.
109. Suzuki F, Kato K, Nakajima T. Regulation of nervous system-specific S-100 protein and enolase levels in adipose tissue by catecholamines. J Neurochem 1984;42(1):130-4.
110. Ishikawa H, Nogami H, Shirasawa N. Novel clonal strains from adult rat anterior pituitary producing S-100 protein. Nature 1983;303(5919):711-3.
111. Winningham-Major F, Staecker JL, Barger SW et al. Neurite extension and neuronal survival activities of recombinant S100 beta proteins that differ in the content and position of cysteine residues. J Cell Biol 1989;109(6 PT 1):3063-71.
112. Bhattacharyya A, Oppenheim RW, Prevette D et al. S100 is present in developing chicken neurons and Schwann cells and promotes motor neuron survival in vivo. J Neurobiol 1992;23(4):451-66.
113. Allore R, O'Hanion R, Price R et al. Gene encoding the beta subunit of S100 protein is on chromosome 21: implications for Down's syndrome. Science 1988;239:1311-3.

References
64
114. Marshak DR, Pesce SA, Stanley LC et al. Increased S100 beta neurotrophic activity in Alzheimer's disease temporal lobe. Neurobiol Aging 1992;13(1):1-7.
115. Rosen H, Rosengren L, Herlitz J et al. Increased serum levels of the S-100 protein are associated with hypoxic brain damage after cardiac arrest. Stroke 1998;29(2):473-7.
116. Kumar P, Dhital K, Hossein-Nia M et al. S-100 protein release in a range of cardiothoracic surgical procedures. J Thorac Cardiovasc Surg 1997;113(5):953-4.
117. Buttner T, Weyers S, Postert T et al. S-100 protein: serum marker of focal brain damage after ischemic territorial MCA infarction. Stroke 1997;28(10):1961-5.
118. Otto M, Wiltfang J, Schutz E et al. Diagnosis of Creutzfeldt-Jakob disease by measurement of S100 protein in serum: prospective case-control study. BMJ 1998;316(7131):577-82.
119. Kerkhoff C, Klempt M, Sorg C. Novel insights into structure and function of MRP8 (S100A8) and MRP14 (S100A9). Biochim Biophys Acta 1998;1448(2):200-11.
120. Gromov LA, Syrovatskaya LP, Ovinova GV. Functional role of the neurospecific S-100 protein in the processes of memory. Neurosci Behav Physiol 1992;22(1):25-9.
121. Gerlai R, Wojtowicz JM, Marks A et al. Overexpression of a calcium-binding protein, S100 beta, in astrocytes alters synaptic plasticity and impairs spatial learning in transgenic mice. Learn Mem 1995;2(1):26-39.
122. Li Y, Barger SW, Liu L et al. S100beta induction of the proinflammatory cytokine interleukin-6 in neurons. J Neurochem 2000;74(1):143-50.
123. Kato K, Kimura S. S100ao (alpha alpha) protein is mainly located in the heart and striated muscles. Biochim Biophys Acta 1985;842(2-3):146-50.
124. Ytrebo LM, Nedredal GI, Korvald C et al. Renal elimination of protein S-100beta in pigs with acute encephalopathy. Scand J Clin Lab Invest 2001;61(3):217-25.
125. Blomquist S, Johnsson P, Luhrs C et al. The appearance of S-100 protein in serum during and immediately after cardiopulmonary bypass surgery: a possible marker for cerebral injury. J Cardiothorac Vasc Anesth 1997;11(6):699-703.

References
65
126. Jönsson H, Johnsson P, Höglund P et al. Elimination of S100B and renal function after cardiac surgery. J Cardiothorac Vasc Anesth 2000;14(6):698-701.
127. Stigbrand T, Nyberg L, Ullen A et al. A new specific method for measuring S-100B in serum. Int J Biol Markers 2000;15(1):33-40.
128. Nyberg L, Bhattacharya R, Kroon R et al. S-100 protein to detect cerebral impairment after cardiac surgery - measuring serum levels using a new immunoluminometric assay (LIA). Book of abstracts: The Brain and Cardiac Surgery, Oxford, England 1966;.
129. Kligman D, Hilt DC. The S100 protein family. Trends Biochem Sci 1988;13(11):437-43.
130. Anderson RE, Hansson LO, Nilsson O et al. Increase in serum S100A1-B and S100BB during cardiac surgery arises from extracerebral sources. Ann Thorac Surg 2001;71(5):1512-7.
131. Ingebrigtsen T, Romner B, Marup-Jensen S et al. The clinical value of serum S-100 protein measurements in minor head injury: a Scandinavian multicentre study. Brain Inj 2000;14(12):1047-55.
132. Jönsson H, Johnsson P, Birch-Iensen M et al. S100B as a predictor of size and outcome of stroke after cardiac surgery. Ann Thorac Surg 2001;71(5):1433-7.
133. Schultz ES, Diepgen TL, Von Den Driesch P. Clinical and prognostic relevance of serum S-100 beta protein in malignant melanoma. Br J Dermatol 1998;138(3):426-30.
134. Sellman M, Ivert T, Ronquist G et al. Central nervous system damage during cardiac surgery assessed by 3 different biochemical markers in cerebrospinal fluid. Scand J Thorac Cardiovasc Surg 1992;26(1):39-45.
135. Johnsson P, Lundqvist C, Lindgren A et al. Cerebral complications after cardiac surgery assessed by S-100 and NSE levels in blood. J Cardiothorac Vasc Anesth 1995;9(6):694-9.
136. Jönsson H, Johnsson P, Alling C et al. S100beta after coronary artery surgery: release pattern, source of contamination, and relation to neuropsychological outcome. Ann Thorac Surg 1999;68(6):2202-8.

References
66
137. Jönsson H, Johnsson P, Alling C et al. Significance of serum S100 release after coronary artery bypass grafting. Ann Thorac Surg 1998;65(6):1639-44.
138. Kilminster S, Treasure T, McMillan T et al. Neuropsychological change and S-100 protein release in 130 unselected patients undergoing cardiac surgery. Stroke 1999;30(9):1869-74.
139. Svenmarker S, Sandström E, Karlsson T et al. Is there an association between release of protein S100B during cardiopulmonary bypass and memory disturbances? Scand Cardiovasc J 2002;36(2):117-22.
140. Astudillo R, Van der Linden J, Rådegran K et al. Elevated serum levels of S-100 after deep hypothermic arrest correlate with duration of circulatory arrest. Eur J Cardiothorac Surg 1996;10(12):1107-12.
141. Grocott HP, Croughwell ND, Amory DW et al. Cerebral emboli and serum S100beta during cardiac operations. Ann Thorac Surg 1998;65(6):1645-9.
142. Anderson RE, Hansson LO, Liska J et al. The effect of cardiotomy suction on the brain injury marker S100beta after cardiopulmonary bypass. Ann Thorac Surg 2000;69(3):847-50.
143. Anderson RE, Hansson LO, Nilsson O et al. High serum S100B levels for trauma patients without head injuries. Neurosurgery 2001;48(6):1255-8.
144. Westaby S, Johnsson P, Parry AJ et al. Serum S100 protein: a potential marker for cerebral events during cardiopulmonary bypass. Ann Thorac Surg 1996;61(1):88-92.
145. Anderson RE, Hansson LO, Vaage J. Release of S100B during coronary artery bypass grafting is reduced by off-pump surgery. Ann Thorac Surg 1999;67(6):1721-5.
146. De Somer F, Francois K, van Oeveren W et al. Phosphorylcholine coating of extracorporeal circuits provides natural protection against blood activation by the material surface. Eur J Cardiothorac Surg 2000;18(5):602-6.
147. Snodgrass JG, Vanderwart M. A standardized set of 260 pictures: norms for name agreement, image agreement, familiarity, and visual complexity. J Exp Psychol 1980;6(2):174-215.
148. Abboud HA. Macintosh computer software Silver Spring, Maryland: Cedrus Corporation. SuperLab 1994;.

References
67
149. Ochsner KN, Chiu CY, Schacter DL. Varieties of priming. Curr Opin Neurobiol 1994;4(2):189-94.
150. Schacter DL. Understanding implicit memory. A cognitive neuroscience approach. Am Psychol 1992;47(4):559-69.
151. Snodgrass JG, Corwin J. Pragmatics of measuring recognition memory: applications to dementia and amnesia. J Exp Psychol Gen 1988;117(1):34-50.
152. Keith JR, Puente AE, Malcolmson KL et al. Assessing postoperative cognitive change after cardiopulmonary bypass surgery. Neuropsychology 2002;16(3):411-21.
153. Rothenburger M, Soeparwata R, Deng MC et al. Prediction of clinical outcome after cardiac surgery: the role of cytokines, endotoxin, and anti-endotoxin core antibodies. Shock 2001;16 Suppl 1:44-50.
154. Nashef SA, Roques F, Michel P et al. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg 1999;16(1):9-13.
155. Roques F, Nashef SA, Michel P et al. Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19030 patients. Eur J Cardiothorac Surg 1999;15(6):816-22.
156. Hernandez F, Cohn WE, Baribeau YR et al. In-hospital outcomes of off-pump versus on-pump coronary artery bypass procedures: a multicenter experience. Ann Thorac Surg 2001;72(5):1528-33.
157. Vaage J, Jensen U, Ericsson A. Neurologic injury in cardiac surgery: aortic atherosclerosis emerges as the single most important risk factor. Scand Cardiovasc J 2000;34(6):550-7.
158. Hsu LC. Biocompatibility in cardiopulmonary bypass. J Cardiothorac Vasc Anesth 1997;11(3):376-82.
159. Wendel HP, Ziemer G. Coating-techniques to improve the hemocompatibility of artificial devices used for extracorporeal circulation. Eur J Cardiothorac Surg 1999;16(3):342-50.
160. Sanchez J, Elgue G, Riesenfeld J et al. Studies of adsorption, activation, and inhibition of factor XII on immobilized heparin. Thromb Res 1998;89(1):41-50.

References
68
161. Bull MH, Huse WM, Bull BS. Evaluation of tests used to monitor heparin therapy during extracorporeal circulation. Anesthesiology 1975;43(3):346-53.
162. te Velthuis H, Baufreton C, Jansen PG et al. Heparin coating of extracorporeal circuits inhibits contact activation during cardiac operations. J Thorac Cardiovasc Surg 1997;114(1):117-22.
163. Gorman RC, Ziats N, Rao AK et al. Surface-bound heparin fails to reduce thrombin formation during clinical cardiopulmonary bypass. J Thorac Cardiovasc Surg 1996;111(1):1-11.
164. Olsson C, Siegbahn A, Halden E et al. No benefit of reduced heparinization in thoracic aortic operation with heparin-coated bypass circuits. Ann Thorac Surg 2000;69(3):743-9.
165. Jansen PG, Baufreton C, Le Besnerais P et al. Heparin-coated circuits and aprotinin prime for coronary artery bypass grafting. Ann Thorac Surg 1996;61(5):1363-6.
166. Ovrum E, Åm Holen E, Tangen G et al. Completely heparinized cardiopulmonary bypass and reduced systemic heparin: Clinical and hemostatic effects. Ann Thorac Surg 1995;60:365-71.
167. von Segesser LK, Weiss BM, Pasic M et al. Risk and benefit of low systemic heparinization during open heart operations. Ann Thorac Surg 1994;58(2):391-7.
168. Kuitunen AH, Heikkilä LJ, Salmenperä MT. Cardiopulmonary bypass with heparin-coated circuits and reduced systemic anticoagulation. Ann Thorac Surg 1997;63(2):438-44.
169. Aldea GS, Lilly K, Gaudiani JM et al. Heparin-bonded circuits improve clinical outcomes in emergency coronary artery bypass grafting. J Card Surg 1997;12(6):389-97.
170. Levy M, Hartman AR. Heparin-coated bypass circuits in cardiopulmonary bypass: improved biocompatibility or not. Int J Cardiol 1996;53 Suppl:S81-7.
171. Ovrum E, Am Holen E, Tangen G et al. Heparinized cardiopulmonary bypass and full heparin dose marginally improve clinical performance. Ann Thorac Surg 1996;62(4):1128-33.
172. Harig F, Feyrer R, Mahmoud FO et al. Reducing the post-pump syndrome by using heparin-coated circuits, steroids, or aprotinin. Thorac Cardiovasc Surg 1999;47(2):111-8.

References
69
173. Fosse E, Thelin S, Svennevig JL et al. Duraflo II coating of cardiopulmonary bypass circuits reduces complement activation, but does not affect the release of granulocyte enzymes : a European multicentre study. Eur J Cardiothorac Surg 1997;11(2):320-7.
174. Ovrum E, Fosse E, Mollnes TE et al. Complete heparin-coated cardiopulmonary bypass and low heparin dose reduce complement and granulocyte activation. Eur J Cardiothorac Surg 1996;10(1):54-60.
175. Mangano CM. Renal dysfunction after myocardial revascularization: risk factors, adverse outcomes, and hospital resource utilization. The Multicenter Study of Perioperative Ischemia Research Group. Ann Intern Med 1998;128(3):194-203.
176. Svenmarker S, Häggmark S, Jansson E et al. Use of heparin-bonded circuits in cardiopulmonary bypass improves clinical outcome. Scand Cardiovasc J 2002;36(4):241-6.
177. Svenmarker S, Åberg T. Prediction of neurological complications in cardiac surgery: use of a multiple logistic regression model. Abstract book SATS-SCANSECT, Helsinki 1998;:65.
178. Newman MF, Croughwell ND, Blumenthal JA et al. Predictors of cognitive decline after cardiac operation. Ann Thorac Surg 1995;59(5):1326-30.
179. Puskas JD, Winston AD, Wright CE et al. Stroke after coronary artery operation: incidence, correlates, outcome, and cost. Ann Thorac Surg 2000;69(4):1053-6.
180. Patel RL, Turtle MR, Chambers DJ et al. Alpha-stat acid-base regulation during cardiopulmonary bypass improves neuropsychologic outcome in patients undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 1996;111(6):1267-79.
181. Gold JP, Charlson ME, Williams-Russo P et al. Improvement of outcomes after coronary artery bypass. A randomized trial comparing intraoperative high versus low mean arterial pressure. J Thorac Cardiovasc Surg 1995;110(5):1302-11.
182. Westaby S, Saatvedt K, White S et al. Is there a relationship between cognitive dysfunction and systemic inflammatory response after cardiopulmonary bypass? Ann Thorac Surg 2001;71(2):667-72.

References
70
183. Harris DN, Bailey SM, Smith PL et al. Brain swelling in first hour after coronary artery bypass surgery. Lancet 1993;342(8871):586-7.
184. Stump DA, Levy JH, Murkin JM. The relationship between reinfusion of shed blood and stroke in coronary artery bypass grafting patients. J Thorac Cardiovasc Surg 2000;70:1787.
185. Shaw PJ, Bates D, Cartlidge NE et al. Early intellectual dysfunction following coronary bypass surgery. Q J Med 1986;58(225):59-68.
186. Selnes OA, Grega MA, Borowicz LM et al. Cognitive changes with coronary artery disease: a prospective study of coronary artery bypass graft patients and nonsurgical controls. Ann Thorac Surg 2003;75(5):1377-84.
187. Taggart DP, Browne SM, Halligan PW et al. Is cardiopulmonary bypass still the cause of cognitive dysfunction after cardiac operations? J Thorac Cardiovasc Surg 1999;118(3):414-20.
188. Van Dijk D, Jansen EW, Hijman R et al. Cognitive outcome after off-pump and on-pump coronary artery bypass graft surgery: a randomized trial. JAMA 2002;287(11):1405-12.
189. Andrew MJ, Baker RA, Kneebone AC et al. Neuropsychological dysfunction after minimally invasive direct coronary artery bypass grafting. Ann Thorac Surg 1998;66(5):1611-7.
190. Hlatky MA, Bacon C, Boothroyd D et al. Cognitive function 5 years after randomization to coronary angioplasty or coronary artery bypass graft surgery. Circulation 1997;96(9 SUPPL):II-11-4.
191. Larrabee GJ, West RL, Crook TH. The association of memory complaint with computer-simulated everyday memory performance. J Clin Exp Neuropsychol 1991;13(4):466-78.
192. Vaage J, Anderson R. Biochemical markers of neurologic injury in cardiac surgery: the rise and fall of S100beta. J Thorac Cardiovasc Surg 2001;122(5):853-5.
193. Borowiec J, Thelin S, Bagge L et al. Heparin coated cardiopulmonary bypass circuits in coronary artery surgery - a clinical study. J Extra Corpor Technol 1990;:86-90.
194. Shapira OM, Aldea GS, Zelingher J et al. Enhanced blood conservation and improved clinical outcome after valve surgery

References
71
using heparin-bonded cardiopulmonary bypass circuits. J Card Surg 1996;11(5):307-17.
195. Aldea GS, O'Gara P, Shapira OM et al. Effect of anticoagulation protocol on outcome in patients undergoing CABG with heparin-bonded cardiopulmonary bypass circuits. Ann Thorac Surg 1998;65(2):425-33.
196. Jensen E, Andréasson S, Bengtsson A et al. Influence of two different perfusion systems on inflammatory response in pediatric heart surgery. Ann Thorac Surg 2003;75(3):919-25.
197. Hsu LC. Heparin-coated cardiopulmonary bypass circuits: current status. Perfusion 2001;16(5):417-28.
198. Svenmarker S, Sandström E, Karlsson T et al. Neurological and general outcome in low-risk coronary artery bypass patients using heparin coated circuits. Eur J Cardiothorac Surg 2001;19(1):47-53.
199. Svenmarker S, Sandström E, Karlsson T et al. Clinical effects of the heparin coated surface in cardiopulmonary bypass. Eur J Cardiothorac Surg 1997;11(5):957-64.

Umeå University Medical Dissertations
New Series No. 855 - ISSN 0346-6612 – ISBN 91-7305-523-9
Edited by the Dean of the Faculty of Medicine
Umeå University SE-901 87 Umeå, Sweden
www.umu.se