Embed Size (px)
DESCRIPTION
pathology lectures "hemostasis"for Dr.Raed Al-ani
Citation preview

Homeostasis

EDEMA
• Increased fluid in the interstitial tissue spaces
• Massive edema is called Anasarca.
• Fluid may also accumulate in body cavities
• These collections of fluid are referred to based on location as: – Hydrothorax, hydropericardium, hydroperitoneum (Ascites )

• maintained by opposing effects of vascular hydrostatic pressure and plasma colloid osmatic pressure

Homeostasis is maintained by the opposing effects of vascular hydrostatic pressure and plasma colloid osmotic pressure
Homeostasis is maintained by the opposing effects of vascular hydrostatic pressure and plasma colloid osmotic pressure
Fluid Homeostasis

Edema Development
PictureFig 2.2
Either increased vascular hydrostatic pressure or decreased plasma colloid osmotic pressure can lead to EDEMA
Either increased vascular hydrostatic pressure or decreased plasma colloid osmotic pressure can lead to EDEMA
Inflammatory mediators can alter vascular permeability causing local EDEMA
Inflammatory mediators can alter vascular permeability causing local EDEMA

Edema Fluid = TRANSUDATE
• A transudate is protein-poor (specific gravity <1.012)
• An exudate is protein-rich (specific gravity >1.020)

Pathophysiologic Categories of Edema
I.Increased Hydrostatic Pressure
II.Reduced Plasma Oncotic Pressure
III.Inflammation
IV.Other
I. Increased Hydrostatic Pressure

I. Increased Hydrostatic Pressure:• Generalized increases in venous pressure, with
resultant SYSTEMIC EDEMA, occur MOST COMMONLY in CONGESTIVE HEART FAILURE”
• Thus, Congestive Heart Failure is the most common cause of EDEMA due to Increased Hydrostatic Pressure
Types of disease causing Edema:A. Congestive Heart FailureB. Portal HypertensionC. Venous Thrombosis

Congestive Heart Failure
• The Pump is FAILING!!! (All the blood going in IS NOT going out!)
• Blood backs up, first into the lungs, • then into the venous circulation - increasing
Central Venous Pressure (CVP)• Increased CVP leads to increased capillary
pressure (Hydrostatic Pressure) leading to Edema

Congestive Heart Failure
Overall, there are TWO main effects...
1. Increased Central Venous Pressure
(we just talked about this one…)
2. Decreased Renal Perfusion

Congestive Heart FailureDecreased Renal Perfusion
• Decreased Cardiac Output
• Leads to decreased ARTERIAL blood volume
• Activates the Renal Defense Mechanisms:– Renin-Angiotensin-Aldosterone Axis
– Renal Vasoconstriction
– Increased Renal Anti-diuretic Hormone (ADH)

Congestive Heart FailureDecreased Renal Perfusion
• Decreased Renal Perfusion activates the Renal Defense Mechanisms:– Renin-Angiotensin-Aldosterone Axis
– Renal Vasoconstriction
– Increased Renal Anti-diuretic Hormone (ADH)

Congestive Heart FailureRenin-Angiotensin-Aldosterone Axis
Renin Aldosterone Renal Na reabsorption
Renal retention of Na + H2O
Plasma volume
Transudation EDEMA
Decreased Renal Perfusion

Congestive Heart FailureRenal Vasoconstriction
Renal Vasoconstriction
Glomerular Filtration Rate (GFR)
Tubular reabsorption of Na + H2O
Plasma volume
Transudation EDEMA
Decreased Renal Perfusion
Renal retention of Na + H2O

Congestive Heart FailureRenal Vasoconstriction
Anti-Diuretic Hormone (ADH)
Renal retention of H2O
Plasma volume
Transudation EDEMA
Decreased Renal Perfusion
Renal retention of Na + H2O

Congestive Heart Failure
CentralVenousPressure
Renal
Perfusion
Renin Renal Vasoconstriction
ADH


Portal Hypertension
• Portal Hypertension is “Increased resistance to portal blood flow”
• The most common cause of Portal Hypertension is CIRRHOSIS.
• Pathogenesis of Ascites is complex– Increased Portal Pressure (hydrostatic pressure) leads to increased
liver sinusoidal hypertension. Fluid moves into the Space of Disse then into lymphatics

Pathogenesis of Ascites is complex
• Cirrhosis leads to hypoalbuminemia sneaking into the next category
• And ultimately, there is decreased renal perfusion leading to secondary hyperaldosteronism (increased renin etc.)

Portal Hypertension
Sinusoidal Hypertension
Renal
Perfusion
Hepatic LymphOverwhelms
Thoracic DuctAldosterone
ASCITES
Cirrhosis
Serum
Albumin

Venous Thrombosis
• Impaired venous outflow increases hydrostatic pressure

Pathophysiologic Categories of Edema
I.Increased Hydrostatic Pressure
II.Reduced Plasma Oncotic Pressure
III.Inflammation
IV.Other

Reduced Plasma Osmotic Pressure
• Albumin is the serum protein MOST responsible for the maintenance of colloid osmotic pressure.
• A decrease in osmotic pressure can result from increased protein loss or decreased protein synthesis.
• Increased albumin Loss: Nephrotic Syndrome– Increased protein permeability of the glomerular basement
membrane• Reduced albumin synthesis
– Cirrhosis– Protein malnutrition

Pathophysiologic Categories of Edema
I.Increased Hydrostatic Pressure
II.Reduced Plasma Oncotic Pressure
III.Inflammation
IV.Other

Inflammation
• Both Acute and Chronic Inflammation are associated with EDEMA

Pathophysiologic Categories of Edema
I.Increased Hydrostatic Pressure
II.Reduced Plasma Oncotic Pressure
III.Inflammation
IV.Other
Lymphatic Obstruction

Lymphatic Obstruction
• Impaired lymphatic drainage with resultant lymphedema, usually localized– Usually due to INFLAMMATION or
NEOPLASTIC OBSTRUCTION– Inflammatory (Filariasis - A parasitic infection
affecting inguinal lymphatics resulting in elephantiasis

Picture of Elephantiasis

• Resection and/or radiation to auxiliary lymphatic can lead to arm edema
• Carcinoma of breast with obstruction of superficial lymphatic can lead to an unusual appearance of the breast - “peau d’orange” (orange peel)
Neoplastic

GENERALIZED EDEMA(Walker’s Law)
• HEART
• LIVER
• KIDNEY

EdemaMorphology
• Edema of the Subcutaneous Tissue is most easily detected Grossly (not microscopically)
• Push your finger into it and a depression remains

• Dependent Edema is a prominent feature of Congestive Heart Failure
• Facial edema is often the initial manifestation of Nephrotic Syndrome
EdemaMorphology

• Pulmonary Edema is most frequently seen in Congestive Heart Failure– May also be present in Renal
failure, Adult Respiratory Distress Syndrome (ARDS), Pulmonary Infections and Hypersensitivity Reactions.
• The Lungs are typically 2-3 times normal weight
• Cross sectioning causes an outpouring of frothy, sometimes blood-tinged fluid

Normal Pulmonary Edema

Edema of the Brain :• Trauma, Abscess, Neoplasm, Infection (Encephalitis), etc.• The big problem is: There is no place for the fluid to go!!! The skull is
the limit.• Herniation into the foramen ovale will kill
Subcutaneous Edema : Annoying but Points to Underlying Disease
– However, it can impair wound healing or clearance of Infection.
Pulmonary Edema :• May cause death by interfering with Oxygen and Carbon Dioxide
exchange• Creates a favorable environment for infection
“Culture Media”

Hyperemia and Congestion
• Hyperemia : is an active process resulting from augmented tissue inflow due to arteriolar dilation (e.g. acute inflammation).
• Congestion is a passive process resulting from impaired outflows from a tissue (e.g. cardiac failure or venous obstruction)

Hyperemia in PneumoniaHyperemia
Infection(Pneumonia)

Hemorrhage
• extravasation of blood due to rupture of blood vessels– Rupture of a large vessel: Trauma, Atherosclerosis, Inflammatory or
Neoplastic Erosion– Rupture of small vessels: hemorrhagic diathesis.
• May be external, into a body cavity or into a tissue• hematoma: accumulation of blood enclosed or confined within
tissue• petechiae: minute hemorrhages into skin or lining surface

Hemorrhage• Purpura (slightly larger hemorrhages than petechia)• Ecchymoses (over 1-2 cm subcutaneous hematoma aka ‘bruise’).• Accumulation of blood in a body cavity:
– Hemothorax– Hemopericardium– Hemoperitoneum– Hemarthrosis
• The RBC’s in a hemorrhage are broken down:– hemoglobin (red) bilirubin (blue-green) hemosiderin (golden-brown)– That’s why bruises change color as they resolve

Clinical Effects of Hemorrhage
• <20% blood loss, little health effect in otherwise healthy individuals– But suppose you have heart or lung disease - could
decrease critical oxygen carrying capacity and ‘heart attack’

Clinical Effects of Hemorrhage
• >20% blood loss, hemorrhagic shock
• Bleeding into the brainstem is fatal while same blood loss from a finger cut is trivial
• Chronic recurrent bleeding can lead iron deficiency anemia!

Anemia from Blood Loss
• This may be the only hint of Occult Cancer– Carcinoma of the Colon
– Gastric Carcinoma (less common)

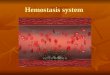
Hemostasis & Thrombosis
• Hemostasis is the normal, rapid formation of a localized “plug” at the site of vascular injury
• Thrombosis is the pathologic formation of a blood clot within the non-interrupted vascular system in a living person

Hemostasis
• Normal - blood is flowing and not clotting
• Injury - blood is clotting and not flowing
• This works due to a daily interaction between the vascular wall, platelets and the coagulation cascade

Thrombosis
• Abnormal activation of the normal hemostatic process
• Thrombosis is Pathologic

Hemostasis• after initial injury, there is a brief period of
arteriolar vasoconstriction (neurogenic reflex augmented by local factors such as endothelin)

Vasoconstriction A transient effect

Hemostasis
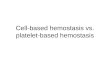
• Endothelial injury exposes the blood to the extracellular matrix (ECM)– The ECM is highly thrombogenic
– Platelets adhere, flatten and then activate
– To form hemostatic plug (primary hemostasis)


summary
Adhere
FlattenActivate
Recruit
HemostaticPlug
vWF = von Willebrand Factor

Secondary Hemostasis
• Tissue factor together with platelet factors activate the coagulation cascade with fibrin deposition. Thrombin activation induces further platelet recruitment and granule release (secondary hemostasis)

Secondary Hemostasis
• Polymerized fibrin and platelet aggregates to form permanent plug

Secondary Hemostasis Pic

Anti-thrombotic Regulation

Components of Normal Hemostasis
• Endothelium
• Platelets
• Coagulation Cascade

Endothelium
• Anti-thrombotic and Procoagulant Properties– Anti-thrombotic - Anti-platelet, anti-coagulant and
fibrinolytic effects
– Procoagulant - Tissue Factor, vWF attachment

Figure 4-5 pro- anti coag effects of endothelium

Endothelial Anti-platelet Effects
• Physical Barrier– prevent platelet contact with ECM;
• Endothelial production of prostacyclin and nitric oxide inhibits platelet adhesion to normal endothelium

Endothelial Anticoagulant Effects
• Mediated by membrane-associated, heparin-like molecules and thrombomodulin and anti-thrombin III

Endothelial Fibrinolytic Effects
• Synthesize tissue type plasminogen activation
(t-PA) promoting fibrinolytic activity

Pro-thrombotic Properties- Normal endothelium produces : von Willebrand factor (vWF) facilitates adhesion of platelets to ECM
- Tissue Factor secretion by endothelium is induced by cytokines or bacterial endotoxin – Tissue Factor activates the extrinsic clotting pathway.
- Endothelial cells secrete plasminogen activator inhibitors (PAIs) which depress fibrinolysis thus promoting thrombosis

Platelets
• When circulating are (membrane-bound smooth discs)• They contain two specific types of granules: alpha granules and delta granules.1- Alpha: contain fibrinogen, fibronectin, factors V and
VIII, platelet factor 4, platelet-derived growth factor (PDGF), and transforming growth factor ß (TGF- ß) .
2- Delata: contain adenine nucleotides (ADP and ATP), ionized calcium, histamine, serotonin and epinephrine

Platelet Activation
• On contact with ECM, platelets undergo:(1) Adhesion and shape change
(2) Secretion (release reaction)
(3) Aggregation

Platelet Adhesion
• Adhesion to ECM is mediated largely via interactions with vWF which acts as a bridge between platelet surface receptors and exposed collagen.

Platelet Secretion• Both granules Explode soon after adhesion
• Calcium and ADP: potent mediators of coagulation and platelet aggregation

Platelet Aggregation
• ADP and thromboxane A2 (TXA2) stimulate further platelet adhesion
• This sets up an autocatalytic reaction leading to an enlarging platelet mass(the primary hemostatic plug)
• This is a ‘reversible’ collection of platelets

Platelet Aggregation
• With activation of the coagulation cascade, thrombin is generated, causing further aggregation then platelet contraction constituting the secondary hemostatic plug
• This is an ‘irreversible’ fusion of platelets

Prostaglandin Balancing Act
• PG12 (endothelium)
– vasodilator
– inhibits platelet aggregation
• TXA2 (platelets)
– vasoconstriction
– Stimulates platelet aggregation

Clinical Use of ASPIRIN in Cardiac Patients
• Inhibits TXA2 Synthesis by platelets
• Benefits Patients at risk for Coronary Artery Thrombosis

“New” Coagulation
CascadeFactor XII Tissue Factor
X
Prothrombin
Fibrinogen
Fibrin
Thrombin
Activates Activates
Activates Activates
Xa

Coagulation Cascade • Conversion of Pro-Factors to Activated Factors , ending in the
formation of Thrombin, Thrombin converts Fibrinogen to Fibrin, Fibrin is critical for hemostasis.
• Each reaction is the result of the assembly of:– Enzyme (activated) coagulation factor– Substrate (pro-enzyme form of a coagulation factor)– Co-Factor (reaction accelerator).
• Occurs on a phospholipid substrate – Such as on the surface of activated platelets– Held together by calcium ions
• This helps to Localize the thrombus– To sites of platelet aggregation

Fig 4-7 Thrombosis on a phospholipid
surface

Thrombosis

Pathogenesis Of Thrombosis
Virchow’s triad– endothelial injury
– stasis or turbulence of blood flow
– blood hypercoagulability


Endothelial Injury
• exposure of subendothelial collagen and other platelet activators
• adherence of platelets
• release of tissue factor
• local depletion of postacyclin (prostaglandin) and plasminogen activator (PA)

ALTERATIONS IN NORMAL BLOOD FLOW
• turbulence of blood flow (arterial and cardiac thrombosis); stasis of blood flow (venous thrombosis)
• disrupt laminar flow and brings platelet in contact with endothelium
• prevent dilution of activated clotting factors

ALTERATIONS IN NORMAL BLOOD FLOW
• Retard the inflow of clotting factor inhibitors and permit thrombi build-up
• Promote endothelial cell activation
• Aneurysms, mitral valve stenosis, hyperviscosity syndromes (e.g. polycythemia)

HYPERCOAGULABILITY
• any alterations of the coagulation pathways that predispose to thrombosis
• primary (genetic) or secondary (acquired) disorders

HYPERCOAGULABILITY (cont’d)
• mutation of factor V gene with functional deficiency of protein C, and other anticoagulants (protein S, antithrombin III). Patient will have venous thrombosis and recurrent thromboembolism
• smoking, obesity, lupus anticoagulant with lupus erythematosis (arterial and venous thrombosis)

ARTERIAL THROMBI
• usually begin at site of endothelial injury and grow in a retrograde direction from point of attachment
• typically are firmly adherent to the injured arterial wall (atherosclerotic plaque) and are gray-white and friable (mesh of platelets, fibrins, RBC, and leukocytes)

Arterial thrombi
• Usually begin at site of endothelial injury and grow along flow of blood
• Typically are firmly adherent to the injured arterial wall (atherosclerotic plaque)

Clinical Settings for Cardiac/arterial Thombus Formation
• Myocardial Infarction (MI)
• Rheumatic Heart Disease
• Atherosclerosis



Morphology of Thrombi
• Arterial Thrombi Are Usually Occlusive
• Venous Thrombi Are Almost Always Occlusive– 85-90% of Venous Thrombi Form in Lower
Extremities• Walker’s Law :-)

VENOUS THROMBOSIS (PHLEBOTHROMBOSIS)
• Superficial venous thrombi, usually occur in saphenous system, may cause local congestion, swelling, and pain; rarely embolize
• Deep thrombi, usually in large leg veins at or above knee joint (e.g. popliteal, femoral, and iliac veins); cause edema of foot and ankle; may embolize

• Characteristically occur at site of stasis and extend in the direction of blood flow (towards heart); contains more enmeshed erythrocytes (red)

• Superficial Veins of the Lower Extremities– Cause Pain, Swelling - Rarely with emobolization– Associated With Varicosities
• Varicose Veins - Abnormally Dilated, Tortuous Veins
– Increased Risk of Infections– Increased Risk of Varicose Ulcers.
• Thrombi in Deep Veins (Femoral, Iliac) More Likely to show emobolization
• About 50% Are Asymptomatic (Formation of Collaterals)
• May Produce Edema, Pain and Tenderness

Clinical Settings for Venous Thrombus Formation
• Cardiac Failure (CHF)• Trauma• Surgery• Burns.• 3rd Term Pregnancy and Postpartum• Cancer
– Migratory Thrombophlebitis (Trousseau’s Syndrome)
• Bed Rest• Immobilization

Valvular Thrombi
• Infective Endocarditis
• Non-bacterial Thrombotic Endocarditis
• Verrucous Endocarditis (Libman-sacks)– Lupus Related

FATE OF THROMBOSIS
• Propagation and obstruction
• Embolization
• Dissolution
• Organization and recanalization


Dissolution of Thrombi
• Recent Thrombi Can Undergo Total Lysis
• After the First 2-3 h, Thrombi won’t undergo Lysis– Thus the Use of TPa Is Only Effective in the First 1-
3 Hours

Organization/Recanalization
• Granulation Tissue Followed by Capillary Channel Formation or may heal so totally As to Leave Only a Small Fibrous ‘Lump’ As Evidence of a Previous Thrombus

Disseminated Intravascular Coagulation (DIC)
• Sudden Widespread Fibrin Deposition in Microcirculation• Rapid Consumption of Platelets and Coagulation Proteins• Secondary Massive Fibrinolysis, all the little thrombi
dissolve• Clotting Disorder Turns Into a Bleeding Disaster

EMBOLISM
• An embolus is a detached intravascular solid, liquid or gaseous mass that is carried by the blood to a site distant from its point of origin
• 99% are dislodged thrombus
• potential consequence: ischemic necrosis (infarction)

PULMONARY THROMBOEMBOLISM
• Generally originates from deep leg veins
• Usually pass through the right heart into pulmonary vasculature and may occlude main pulmonary artery, across the bifurcation (saddle embolus) or pass into the smaller, branching arterioles; multiple emboli may occur


Paradoxical Embolism
• An embolus pass through an interarterial or intraventricular defect to gain access to the systemic circulation( from vein to artery)
• Most pulmonary emboli (60-80%) are clinically silent because of small size

PULMONARY THROMBOEMBOLISM
• When 60% or more of the pulmonary circulation is obstructed, sudden death may occur as caused by right heart failure .
• Embolic obstruction of medium-sized arteries may result in hemorrhage without infarction because of intact bronchial circulation (unless bronchial circulation is compromised - left heart failure).
• multiple pulmonary emboli over time may cause pulmonary hypertension and right heart failure

SYSTEMIC THROMBOEMBOLISM
• emboli traveling within the arterial circulation
• 80% arise from intracardiac mural thrombi, others from ulcerated atherosclerotic plaques, aortic aneurysm, or from fragmentation of valvular vegetation
• major sites are lower extremities (75%), brain (10%), intestines and kidneys

FAT EMBOLISM SYNDROME
• characterized by pulmonary insufficiency, neurologic symptoms, anemia, and thrombocytopenia. 10% of cases are fatal
• typically are caused by microscopic fat globules derived from long bone fractures (fatty marrow), or rarely from soft tissue trauma and burns

AIR EMBOLISM
• gas bubbles within the circulation can obstruct vascular flow to cause distal ischemic injury
• air may enter circulation in chest wall injury or in individuals exposed to sudden atmospheric pressure changes (decompression sickness)

AIR EMBOLISM (cont’d)
• Caisson Disease: chronic form of decompression sickness in which persistent of gas emboli in the bones (heads of femora, tibia, and humera) leads to multiple foci of ischemic necrosis

Amniotic Fluid Embolism
• Torn placental membrane - amniotic fluid release
• Rupture of uterine veins
• Infusion of amniotic fluid into maternal venous circulation

Amniotic Fluid Embolism
• Lungs show squamous cells, lanugo hair, fat from vernix caseosa
• Pulmonary edema, diffuse alveolar damage
• DIC

Amniotic Fluid Embolism
• Present with dyspnea, cyanosis, shock, seizures and coma
• Mortality of 80%– Walker’s Law :-)

Embolism
• Potential Consequences– Ischemic Necrosis (Infarction)
– Though Pulmonary Emboli Are Common and Important, Secondary Pulmonary Infarction Is Not Common
– Lung Is Protected by a Dual Blood Supply
– The Brain Is Not So Protected and Gets Infarcts (Stroke) LIQUEFACTIVE NECROSIS

INFARCTION
• An infarct is an area of ischemic necrosis caused by occlusion of either the arterial supply or venous drainage in a particular tissue
• nearly 90% of all infarcts result from thrombotic or embolic events in arterial vasculatures

• Venous infarcts are more likely in organs with a single venous outflow channel (testis, ovary)
• All infarcts tend to be wedge-shaped, with the occluded vessel at the apex

RED INFARCTSOccur:
– with venous occlusions (e.g. ovarian torsion)
– in loose (spongy) tissues (e.g. lung) that allow blood to collect in the infarcted zone
– in tissues with dual circulations (e.g. lung and small intestines)
– in tissues that were previously congested
– when the occluded site is re-perfused


WHITE OR PALE INFARCTS
• occur with arterial occlusions in solid organs (e.g. heart, spleen, kidney) where the solidity of the tissue limits the amount of hemorrhage into the ischemic area

FACTORS THAT INFLUENCE DEVELOPMENT OF AN
INFARCT
• nature of the vascular supply (dual arterial supply?)
• rate of development of occlusion
• vulnerability of the tissue to hypoxia
• oxygen content of blood

SHOCK
• Constitutes systemic hypoperfusion due to reduction either in cardiac output or in the effective circulating blood volume. The end results are hypotension, followed by impaired tissue perfusion and cellular hypoxia
• Three main categories: cardiogenic, hypovolemic, and septic
• Others: neurogenic shock and anaphylactic shock

CARDIOGENIC SHOCK
• Results from myocardial failure (infarction), ventricular arrhythmia, extrinsic compression [cardiac tamponade, or outflow obstruction pulmonary embolism)]

HYPOVOLEMIC SHOCK
• Results from loss of blood or plasma volume (hemorrhage, fluid loss from severe burns or trauma)


SEPTIC SHOCK
• Caused by systemic microbial infection, most often by gram-negative infection (endotoxic shock) but can also occur with gram-positive and fungal infections

PATHOGENESIS OFSEPTIC SHOCK
• Endotoxic shock: endotoxins are bacterial wall lipopolysaccharides (LPS) which consists of a toxic fatty acid (lipid A) core and a complex polyssacharide cost (including O antigen)

PATHOGENESIS OFSEPTIC SHOCK (cont’d)
• LPS TNF (macrophages) 1L-1 1L6/1L8
• systemic vasodilation (hypotension), diminished cardiac contractility, endothelial injury and activation (alveolar capillary damage), activation of coagulation system


ANAPHYLATIC SHOCK
• IgE mediated hypersensitivity response associated with systemic vasodilatation and increased vascular permeability

NEUROGENIC SHOCK
• Occur in esthetic accident or spinal cord injury with loss of vascular tone and peripheral pool of blood

STAGES OF SHOCK
1- Initial non-progressive stage: compensatory reflex, perfusion of vital organs maintained
2- Progressive stage: characterized by tissue hypoperfusion and onset of circulatory and metabolic imbalance
3- Irreversible stage: tissue and organ damage