Embed Size (px)
Citation preview

Tina Postrel, SPT
UCF DPT c/o 2015
Stroke Prognosis, in general
Classifications of strokes
Prognosis◦ Ischemic stroke
Early prognosis
Late prognosis
◦ Hemorrhagic stroke Early prognosis
Define Vasospasm
Late prognosis
EBP
Rehab principles
Summary

The greatest amount of recovery occurs in the first 7-14 days◦ Swelling subsides
◦ Impairments may resolve spontaneously
◦ “Reversible ischemic neurological deficit”
Residual neurological impairments, may lead to permanent disability…
14% of persons who survive an initial
stoke or TIA will experience another
one within 1 year
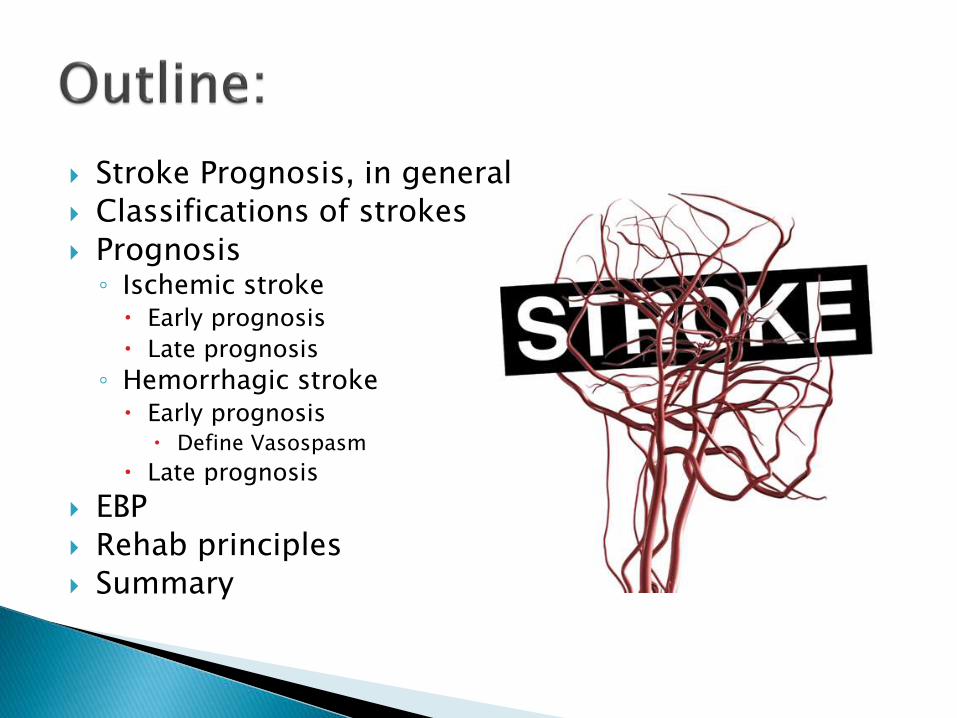
By specific vascular
territory or region:
•Artery: MCA,
ACA, PCA
•Lobe: Frontal,
temporal,
occipital, etc.
By management:
•Minor/major
stroke
•Young stroke
•Deteriorating
Stroke
By Etiology:
•Thrombosis
(Ischemic)
•Embolus
(Ischemic)
•Hemorrhage
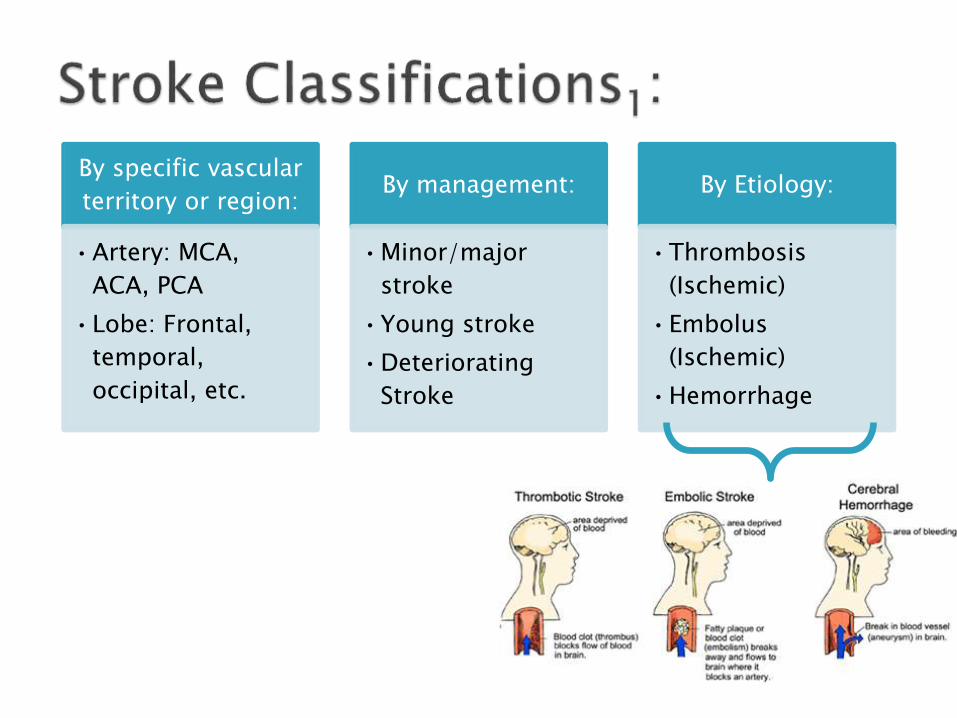
Early Prognosis: Late Prognosis:
Hemorrhagic Stroke POOR GOOD
Ischemic Stroke FAIR FAIR
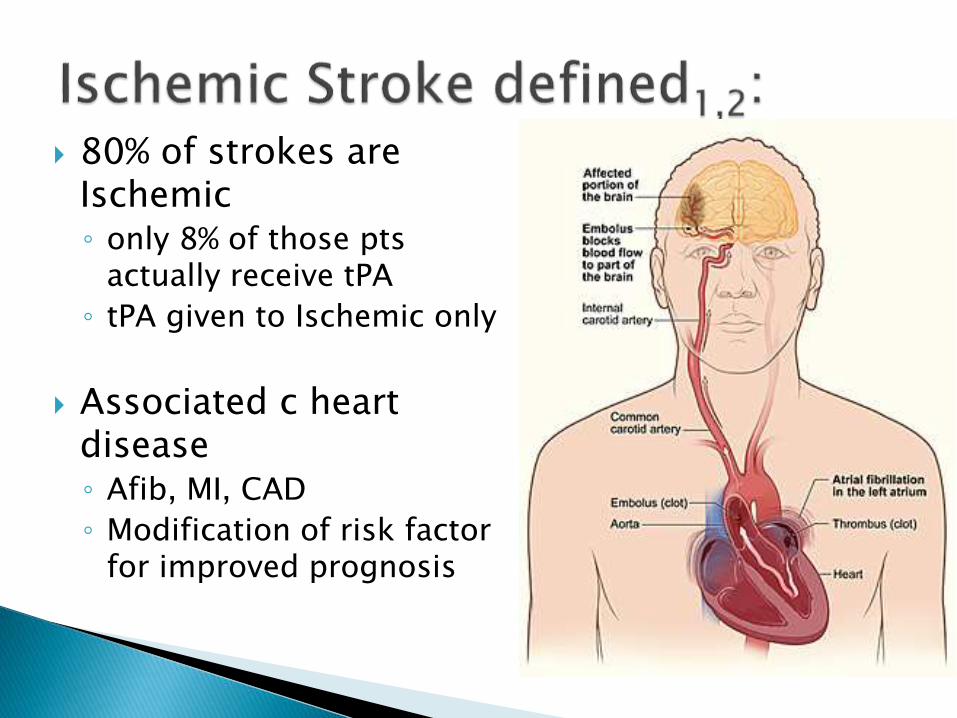
80% of strokes are Ischemic◦ only 8% of those pts
actually receive tPA
◦ tPA given to Ischemic only
Associated c heart disease◦ Afib, MI, CAD
◦ Modification of risk factor for improved prognosis
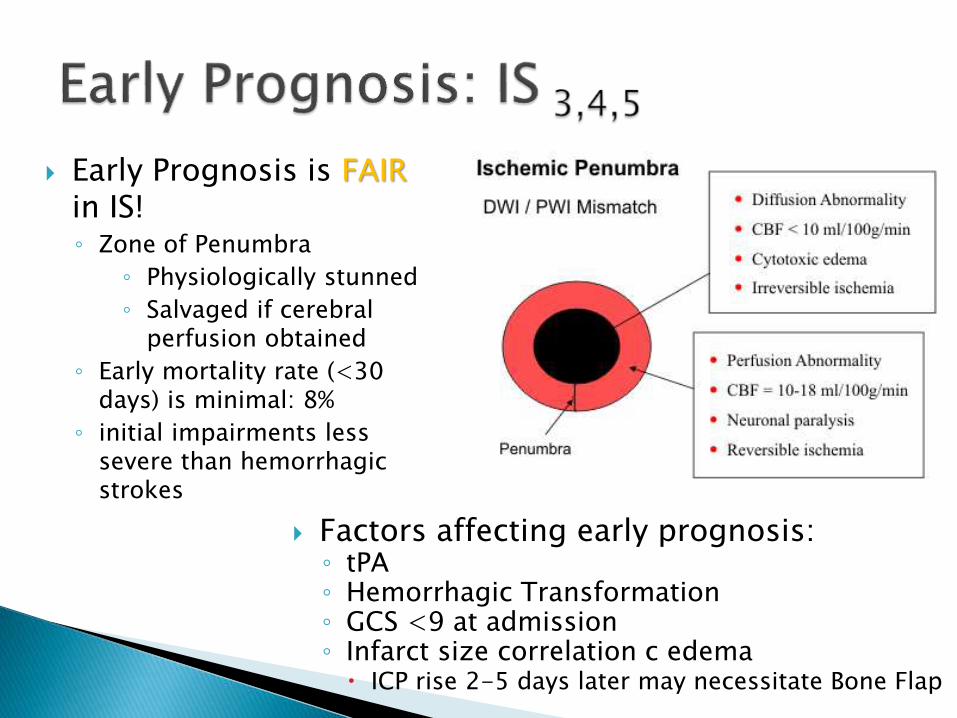
Factors affecting early prognosis:◦ tPA◦ Hemorrhagic Transformation ◦ GCS <9 at admission◦ Infarct size correlation c edema
ICP rise 2-5 days later may necessitate Bone Flap
Early Prognosis is FAIRin IS!◦ Zone of Penumbra
◦ Physiologically stunned
◦ Salvaged if cerebral perfusion obtained
◦ Early mortality rate (<30 days) is minimal: 8%
◦ initial impairments less severe than hemorrhagic strokes

Late Prognosis is FAIR in IS!◦ Lower rate of functional return
Slower, more gradual rate of functional return when compared to hemorrhagic strokes
Factors affecting late prognosis:◦ GCS <9 at admission
◦ Comorbidities: Afib, DM
◦ PLOF
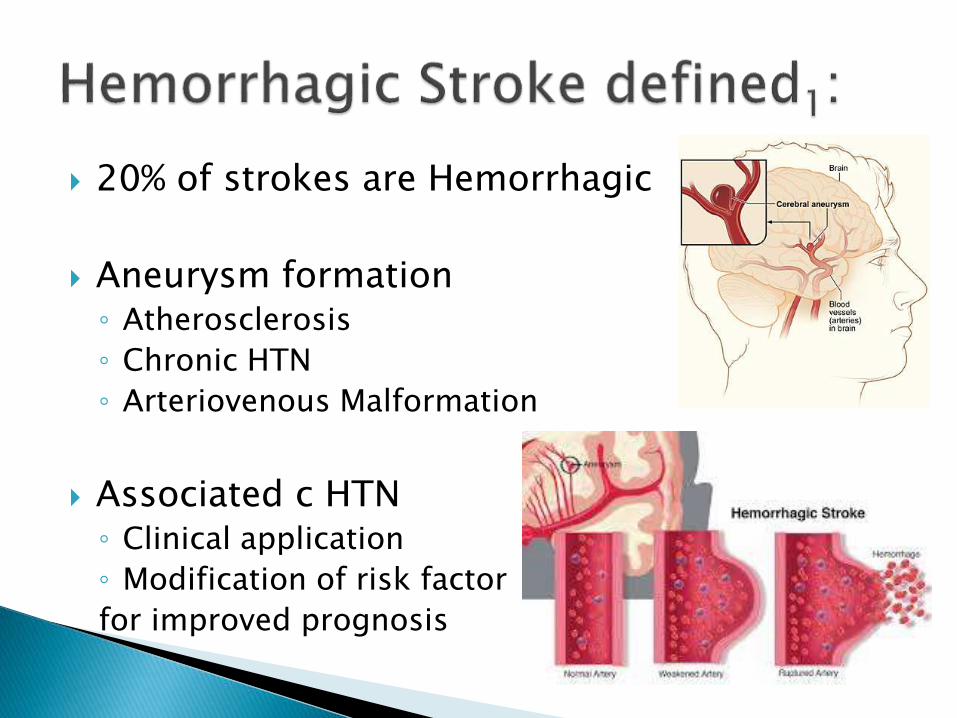
20% of strokes are Hemorrhagic
Aneurysm formation◦ Atherosclerosis
◦ Chronic HTN
◦ Arteriovenous Malformation
Associated c HTN◦ Clinical application
◦ Modification of risk factor
for improved prognosis
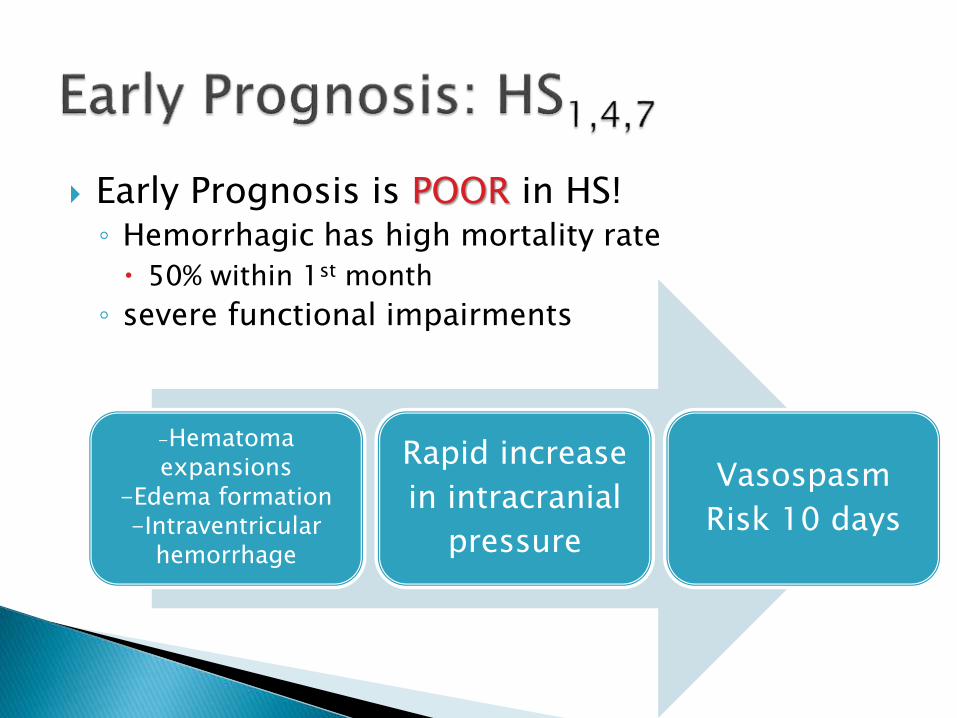
Early Prognosis is POOR in HS!◦ Hemorrhagic has high mortality rate
50% within 1st month
◦ severe functional impairments
-Hematoma expansions
-Edema formation-Intraventricular
hemorrhage
Rapid increase
in intracranial
pressure
Vasospasm
Risk 10 days
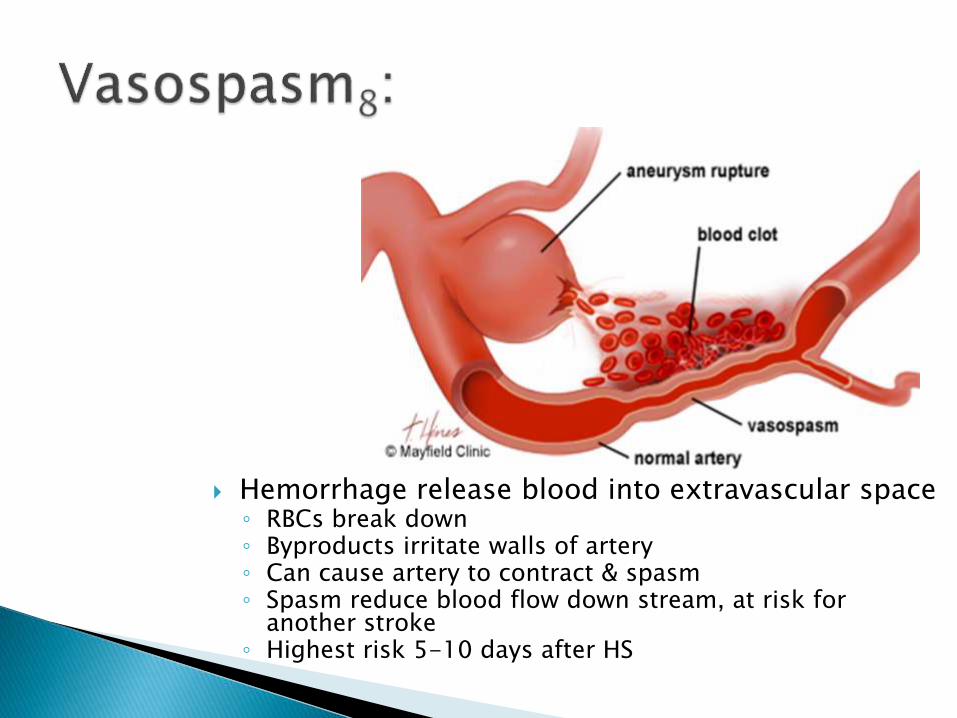
Hemorrhage release blood into extravascular space◦ RBCs break down◦ Byproducts irritate walls of artery◦ Can cause artery to contract & spasm◦ Spasm reduce blood flow down stream, at risk for
another stroke◦ Highest risk 5-10 days after HS
Late Prognosis is GOOD in HS!
Hematoma
resolves
Brain
compression
reduces
Neurological
function
recovers
Partially or
wholly return
to function!
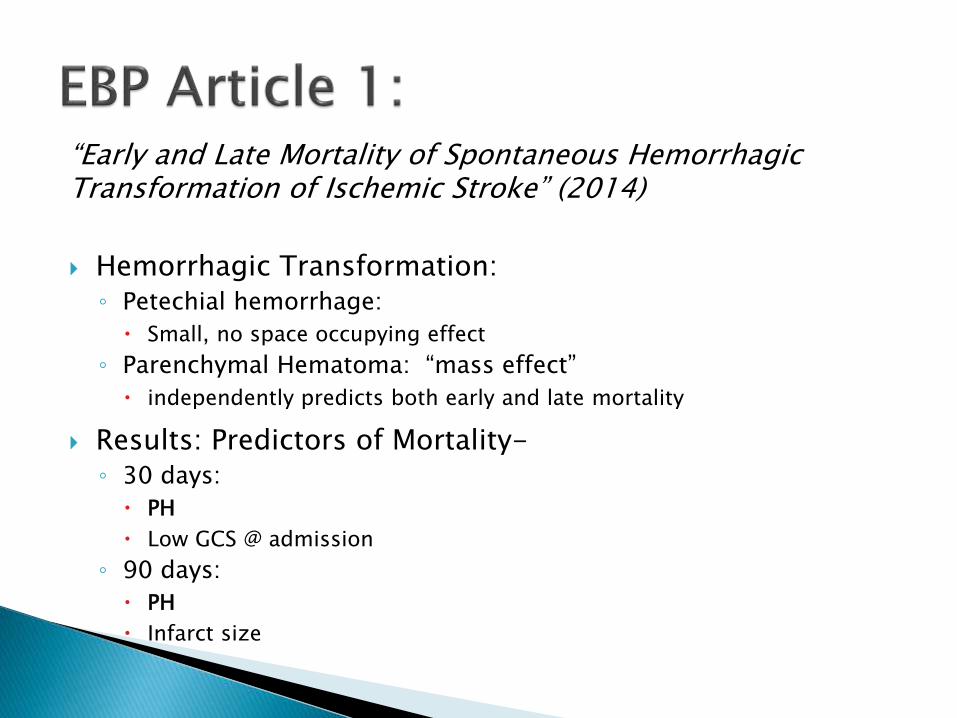
“Early and Late Mortality of Spontaneous Hemorrhagic Transformation of Ischemic Stroke” (2014)
Hemorrhagic Transformation: ◦ Petechial hemorrhage:
Small, no space occupying effect
◦ Parenchymal Hematoma: “mass effect”
independently predicts both early and late mortality
Results: Predictors of Mortality-◦ 30 days:
PH
Low GCS @ admission
◦ 90 days:
PH
Infarct size

“Functional Outcome of Ischemic and Hemorrhagic Stroke Patients After Inpatient Rehabilitation” (2003)
Intervention: ◦ Inpatient Rehab: 60 mins, 2xday, 5 days per week
Results: ICH had a better rehab prognosis at D/C than ischemic strokes◦ Higher Canadian Neurologic Scale
◦ Higher Rivermead Mobility Index scores
◦ Higher Barthel Index scores (2.5x greater than ischemic strokes)
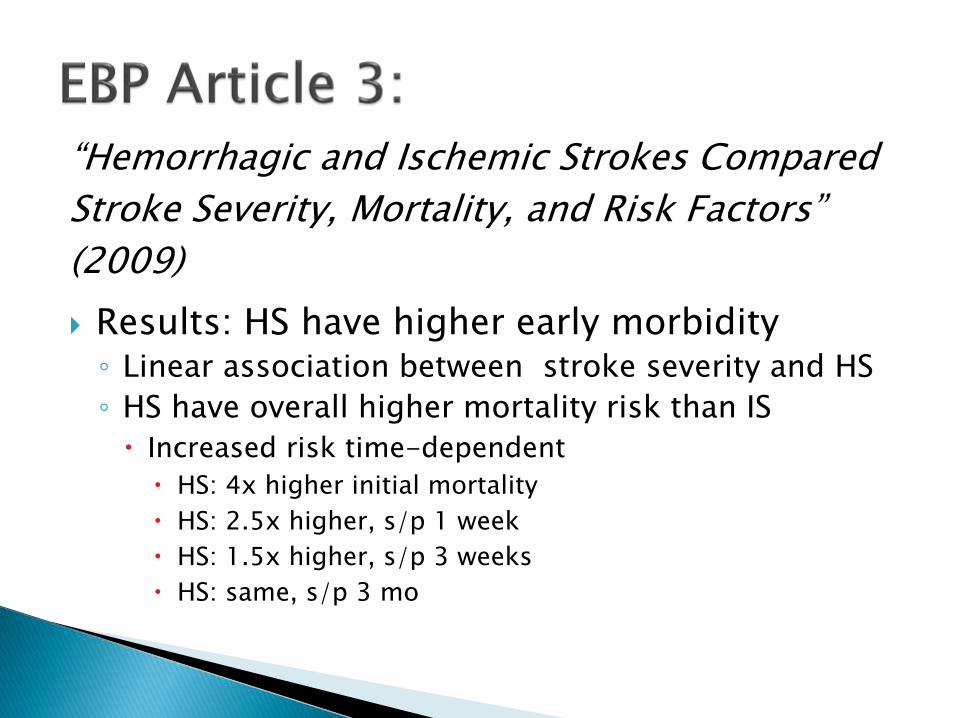
“Hemorrhagic and Ischemic Strokes Compared
Stroke Severity, Mortality, and Risk Factors”
(2009)
Results: HS have higher early morbidity◦ Linear association between stroke severity and HS
◦ HS have overall higher mortality risk than IS
Increased risk time-dependent
HS: 4x higher initial mortality
HS: 2.5x higher, s/p 1 week
HS: 1.5x higher, s/p 3 weeks
HS: same, s/p 3 mo
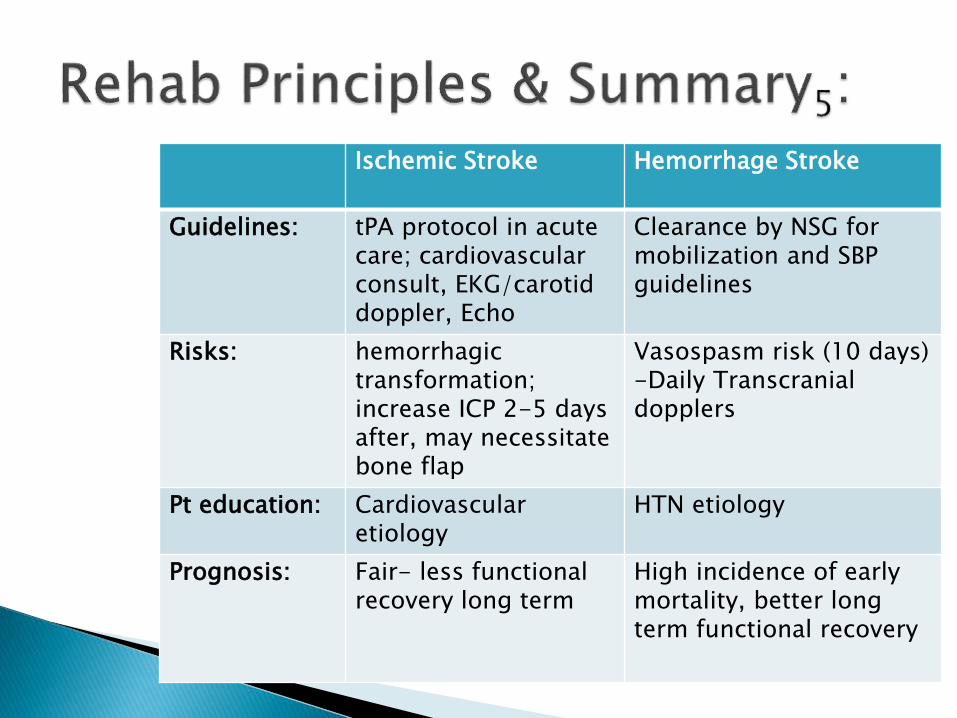
Ischemic Stroke Hemorrhage Stroke
Guidelines: tPA protocol in acute care; cardiovascularconsult, EKG/carotid doppler, Echo
Clearance by NSG for mobilization and SBP guidelines
Risks: hemorrhagic transformation; increase ICP 2-5 days after, may necessitate bone flap
Vasospasm risk (10 days)-Daily Transcranial dopplers
Pt education: Cardiovascular etiology
HTN etiology
Prognosis: Fair- less functional recovery long term
High incidence of early mortality, better long term functional recovery
1) O'Sullivan S, Schmitz T. Physical Rehabilitation: Assessment And Treatment. 5Th Ed. Philadelphia;: F.A. Davis; 2001. Available from: SPORTDiscus, Ipswich, MA.
2) Persson M, Fhager A, Elam M, et al. Microwave-based stroke diagnosis making global pre-hospital thrombolytic treatment possible. IEEE Transactions On Bio-Medical Engineering. June 12, 2014;Available from: MEDLINE, Ipswich, MA.
3) D'Amelio M, Terruso V, Aridon P, et al. Early and Late Mortality of Spontaneous Hemorrhagic Transformation of Ischemic Stroke. Journal Of Stroke & Cerebrovascular Diseases. 2014;23(4):649-654.
4) Schepers V, Ketelaar M, Visser-Meily A, de Groot V, Twisk J, Lindeman E. Functional recovery differs between ischaemic and haemorrhagic stroke patients. Journal Of Rehabilitation Medicine (Stiftelsen Rehabiliteringsinformation) [serial online]. June 2008;40(6):487-489.
5) Kollmar R, Schwab S. Ischaemic stroke: acute management, intensive care, and future perspectives. BJA: The British Journal Of Anaesthesia [serial online]. July 2007;99(1):95-101.
6) Wei J, Heeley E, ChinaQUEST I, et al. Comparison of Recovery Patterns and Prognostic Indicators for Ischemic and Hemorrhagic Stroke in China The ChinaQUEST (QUality Evaluation of Stroke Care and Treatment) Registry Study. Stroke [serial online]. n.d.;41(9):1877-1883.
7) Paolucci S, Antonucci G, Pratesi L, et al. Functional outcome of ischemic and hemorrhagic stroke patients after inpatient rehabilitation: a matched comparison. Stroke (00392499). December 2003;34(12):2861-2865.
8) Mayfield Clinic & Spine Institute: Subarachnoid Hemorrhage & Vasospasm. http://www.mayfieldclinic.com/PDF/PE-SAH.pdf Published February 2013. Accessed July 19, 2014.
9) Andersen K, Olsen T, Dehlendorff C, Kammersgaard L. Hemorrhagic and Ischemic Strokes Compared Stroke Severity, Mortality, and Risk Factors. Stroke. 2009.;40(6):2068-2072.




















![Hemorrhagic Stroke Size by Optimization of - cureus.com · hemorrhagic stroke, and are associated with a higher mortality risk than ischemic strokes [3-4]. An IPH can lead to secondary](https://img.dokumen.tips/doc/110x75/5e0958916e06c4432d031ac7/hemorrhagic-stroke-size-by-optimization-of-hemorrhagic-stroke-and-are-associated.jpg)