Embed Size (px)
Citation preview

Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock
in the in the in the in the InjuriedInjuriedInjuriedInjuried PatientPatientPatientPatient
Hasanul Arifin
Departemen Anestesiologi dan Reanimasi
Fakultas Kedokteran USU
CaO2
• Oxygen Bound (HbO2)
• Oxygen dissolved (plasma)
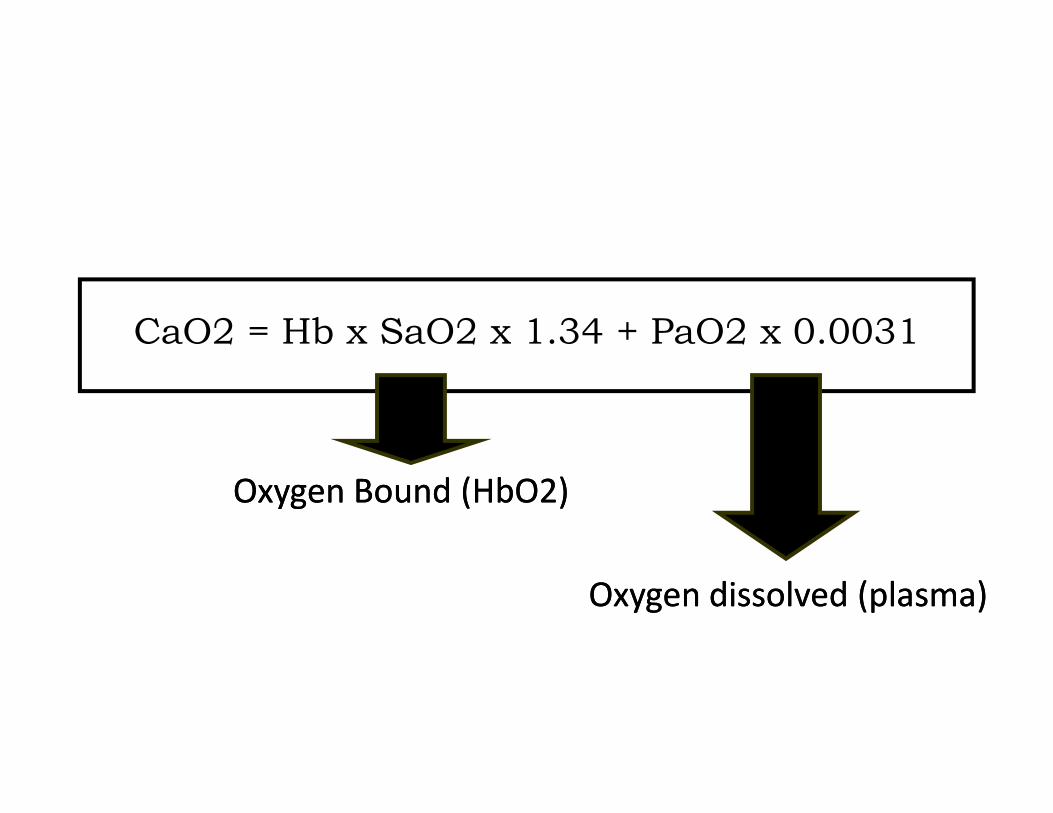
CaO2 = Hb x SaO2 x 1.34 + PaO2 x 0.0031
Oxygen Bound (HbO2)Oxygen Bound (HbO2)
Oxygen dissolved (plasma)Oxygen dissolved (plasma)

26/08/2010 4

26/08/2010 5

26/08/2010 6
Initial Management of Initial Management of Initial Management of Initial Management of
Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock Hemorrhagic Shock

Pasien Trauma
(dianggap menderita shock hypovolemia)
Hentikan Perdarahan, Ganti
Kehilangan Volume
Physical Examination
( ABCDE)
• Airway & Breathing• Keep the airway clear
• Ventilasi & Oksigenasi• Ventilasi & Oksigenasi
• Beri O2 ���� SpO2 96-98%
• Circulation ( kontrol perdarahan)• Penekanan
• PASG (Pneumatic Anti shock Garment)
• Operatip
Physical Examination
( ABCDE)
• Disability (neurologi)
• Brain perfusion
• GCS
• Respon pupil• Respon pupil
• Exposure
• Head to Too
• Cegah hypothermia ( penghangatan internal,
eksternal)
Tindakan lain
• Dekompressi ( Maag dilatation)
• Maag dilatasi ���� vagal stimulation ���� bradikardia,
hypotensi
• Risiko aspirasi
• Insersi NGT no besar untuk dekompressi, suction aktif
• Urinary Catheter
• Hematuria?
• Jumlah urine ���� renal perfusion

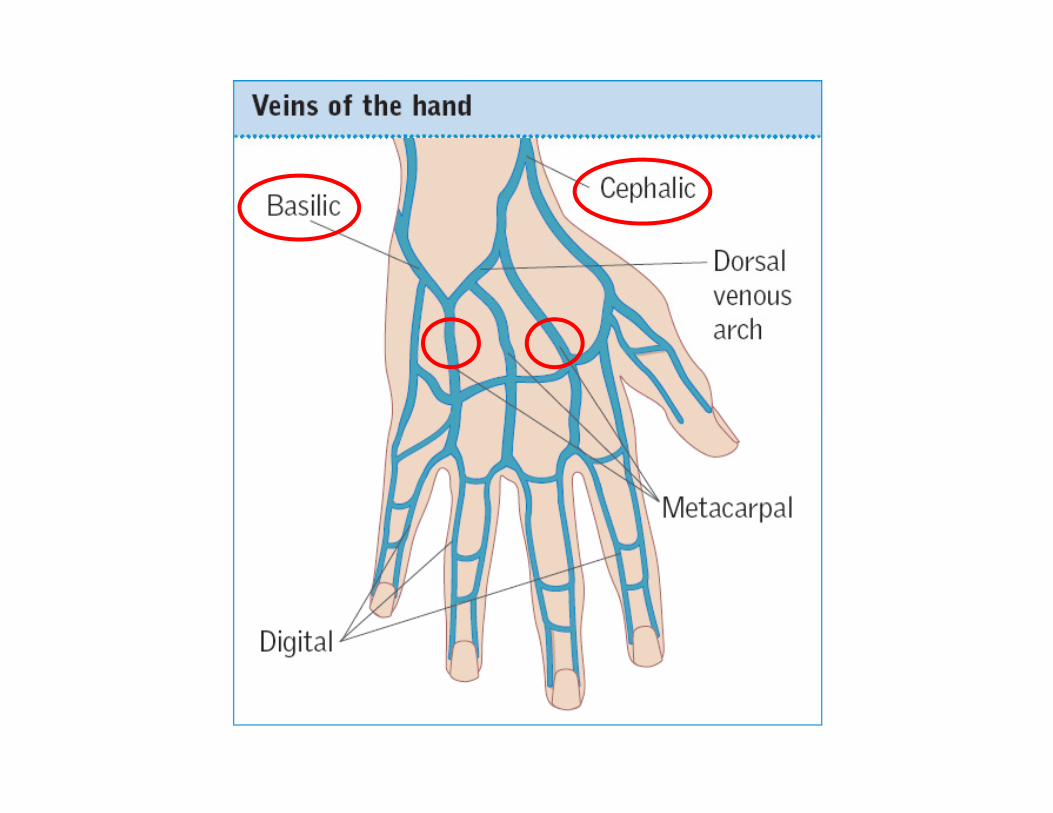
iv. line
• 2 (dua) iv catheter no. besar (16G, 18G)
• Vena lengan bawah
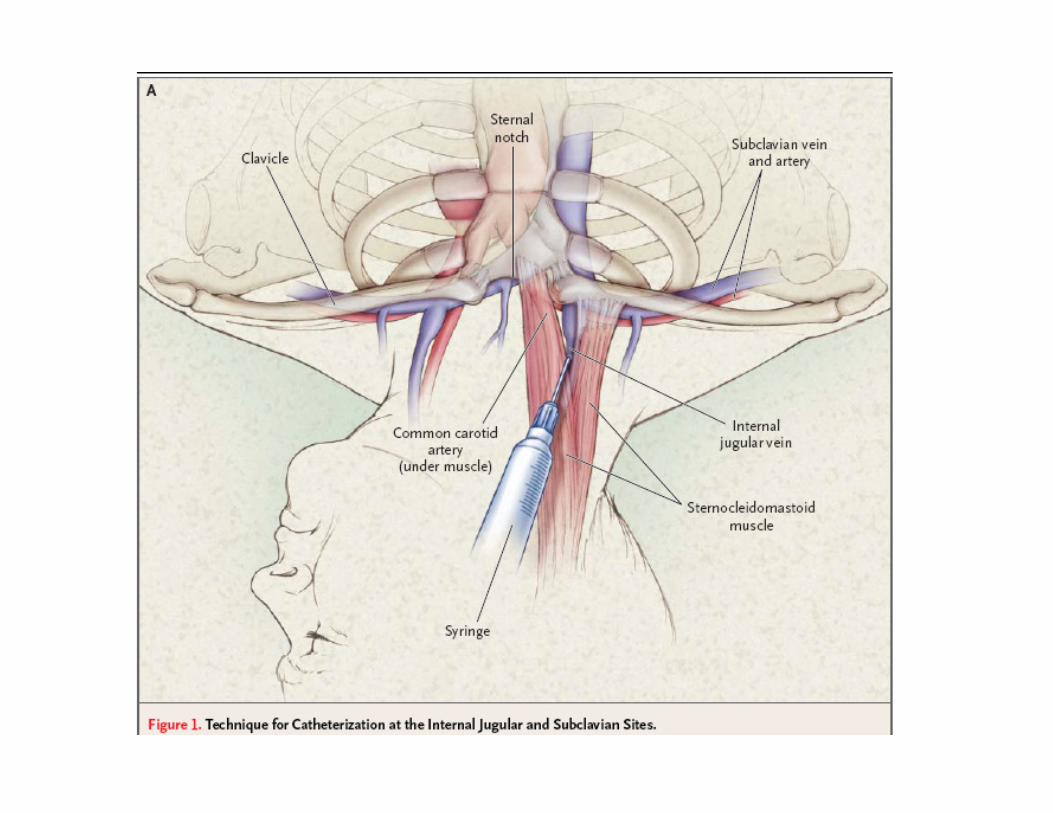
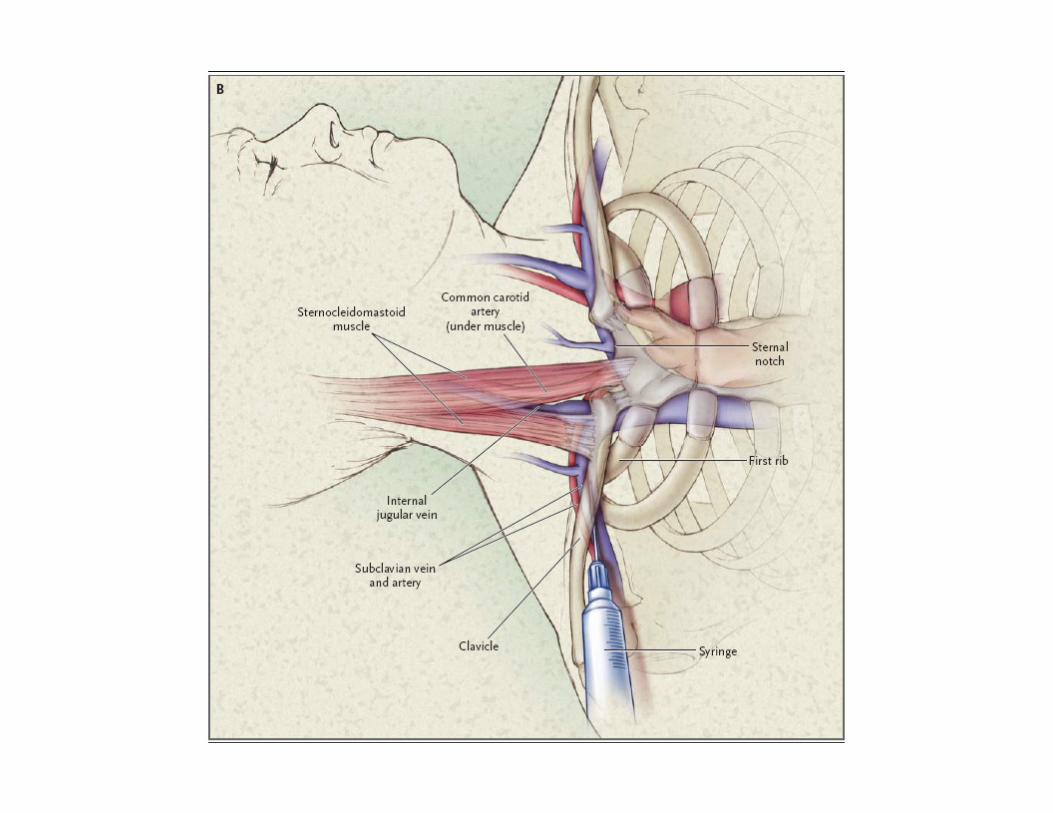
• Kalau kesulitan, akses vena besar :
�Dilakukan oleh tenaga yang
� v. subclavia
� v. jugularis interna
� v. femoralis
� Sekalian ambil contoh darah (laboratorium)
Dilakukan oleh tenaga yang
terlatih, jangan sampai
menimbulkan komplikasi
( peneumothorax,
hematothorax, arterial
puncture )

Vein Selection
• Both upper limbs should be inspected to
identify possible veins for cannulation.
• Potential veins can then be palpated to assess
their condition.their condition.
• An ideal vein is ‘soft and bouncy’ when
palpated.
• Veins that are tender, thrombosed or hard
should be avoided


Device selection
• It is important to select the correct vascular
access device for the patient’s specific clinical
situation
• PUR (polyurethane), modern, softer, cause
less intimal damage and are kink resistant less intimal damage and are kink resistant
which reduces the incidence of cannula failure
• PVC, Teflon, older materials are more rigid,
higher incidence of thrombophlebitis.

equipment
• Infusion standart
• Fluid (RL, NaCl, etc)
• Infusion tubing
• The following equipment for cannulation should be
assembled and placed on a clean tray:assembled and placed on a clean tray:
• cannula, antiseptic, sterile gauze, sterile saline flush,
single or multiway adapter (primed with sterile saline)
with integral ‘needle-less’ device, sterile moisture-
permeable transparent dressing, tape, and a small
sharps’ container.
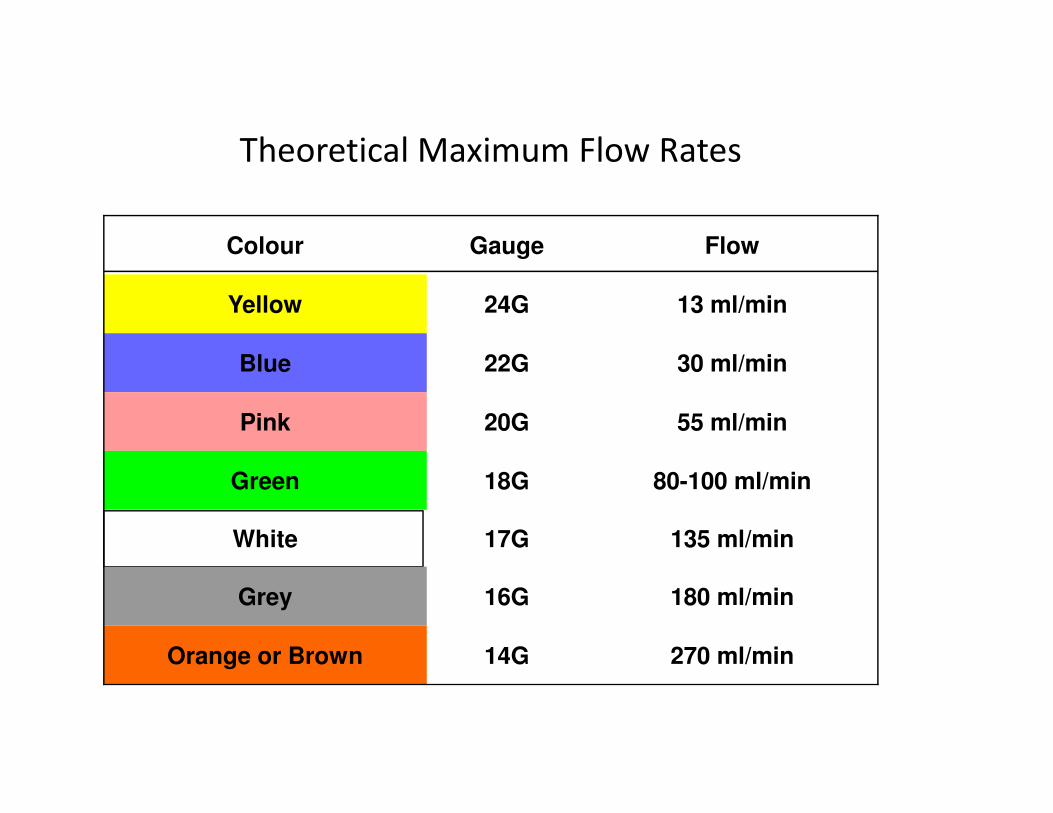
Theoretical Maximum Flow Rates
Colour Gauge Flow
Yellow 24G 13 ml/min
Blue 22G 30 ml/min
Pink 20G 55 ml/min
Green 18G 80-100 ml/min
White 17G 135 ml/min
Grey 16G 180 ml/min
Orange or Brown 14G 270 ml/min

26/08/2010 21

Class IClass I Class IIClass II Class IIIClass III Class IVClass IV
BloodBlood--Loss[ml]Loss[ml] -->750>750 750750--15001500 15001500--20002000 >2000>2000
BloodBlood--loss [%BV]loss [%BV] -->15%>15% 1515--30%30% 3030--40%40% >40%>40%
PulsePulse--Rate [x/min.]Rate [x/min.] <100<100 >100>100 >120>120 >140>140
BloodBlood--PressurePressure NormalNormal NormalNormal DecreasedDecreased DecreasedDecreased
Estimated Fluid and Blood Losses Based on Estimated Fluid and Blood Losses Based on
Patient’s Initial PresentationPatient’s Initial Presentation
26/08/2010 22
PulsePulse--PressurePressure N or N or increasedincreased
DecreasedDecreased DecreasedDecreased DecreasedDecreased
Respiratory RateRespiratory Rate 1414--2020 2020--3030 3030--3535 >35>35
Urine outUrine out--put put [ml/hour][ml/hour]
>30>30 2020--3030 55--1515 NegligibleNegligible
Mental status/CNSMental status/CNS Slightly Slightly anxiousanxious
Midly Midly anxiousanxious
Anxious Anxious and and confusedconfused
Confused Confused and and lethargiclethargic
EEBV BV = 70 ml/kg= 70 ml/kg
Kegunaan Klinis
Tabel Prakiraan Kehilangan Darah• Dengan menyesuaikan tanda dan gejala dari penderita pada
tabel, dapat diperkirakan berapa kehilangan darah yang sdhterjadi.
• Kemudian kita dapat memperhitungkan berapa jumlah cairanyang harus diberikan untuk resusitasi
• Bila post resisitasi belum ada tanda perbaikan, maka• Bila post resisitasi belum ada tanda perbaikan, makakemungkinan :
– Ongoing loss
– Prakiraan ada kesalahan (BB tidak sesuai, kurang jeli menilai tanda dangejala
– Ada tambahan kehilangan cairan lain selain perdarahan
– Shock bukan ok. perdarahan

Initial Fluid Therapy
• Tujuan :
• mengisi intravaskular dalam waktu singkat � preload � mekanisme
hemodinamik
• Cairan :
• Kristalloid• Kristalloid• Ringer Lactat
• Ringer Asetat
• NaCl 0.9%
• Rule : 3 for 1 (1000 mL perdarahan ganti 3000 mL)
• Kolloid ���� rule 1 : 1 ( 500 mL perdarahan ganti 500 mL)

TOTAL BODY WATER : 60% TOTAL BODY WEIGHTTOTAL BODY WATER : 60% TOTAL BODY WEIGHT
36 L36 L60 kg60 kg
Physiologic principles of Physiologic principles of
fluid managementfluid management
26/08/2010 25
ISF
9L9L
ISFISF IVFIVF ICFICF
3L3L 24 L24 L
Hasanul, 2002Hasanul, 2002

PhysiologyPhysiologydefinitiondefinition
•• CrystalloidCrystalloid is the term commonly is the term commonly
applied to solutions that do not applied to solutions that do not
contain any highcontain any high--molecularmolecular--weight weight
compounds and thus have an compounds and thus have an oncoticoncoticcompounds and thus have an compounds and thus have an oncoticoncotic
pressure of zeropressure of zero
•• ColloidColloid is the term used to denote is the term used to denote
solutions that have an solutions that have an oncoticoncotic
pressure similar to that of plasma.pressure similar to that of plasma.
Jenis cairan yang beredar :Jenis cairan yang beredar :
•• KristalloidKristalloid ( D5W, RL, RA, NaCl )( D5W, RL, RA, NaCl )
•• Kolloid Kolloid ( Albumin, HES, Expafusin, ( Albumin, HES, Expafusin,
Gelatine)Gelatine)
26/08/2010 27
Gelatine)Gelatine)
•• Cairan NutrisiCairan Nutrisi ( Intrafusin, Ivelip, ( Intrafusin, Ivelip,
Triofusin)Triofusin)
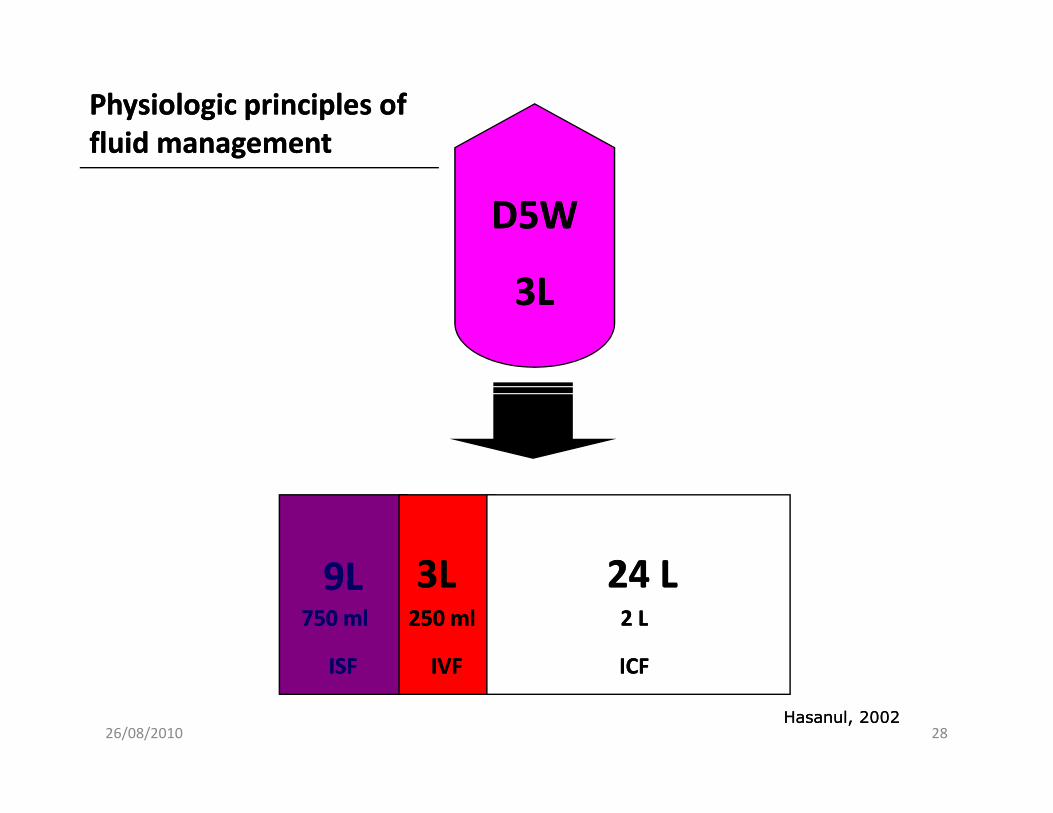
D5WD5W
3L3L
Physiologic principles of Physiologic principles of
fluid managementfluid management
26/08/2010 28
ISF
9L9L
ISFISF IVFIVF ICFICF
3L3L 24 L24 L750 ml750 ml 250 ml250 ml 2 L2 L
Hasanul, 2002Hasanul, 2002
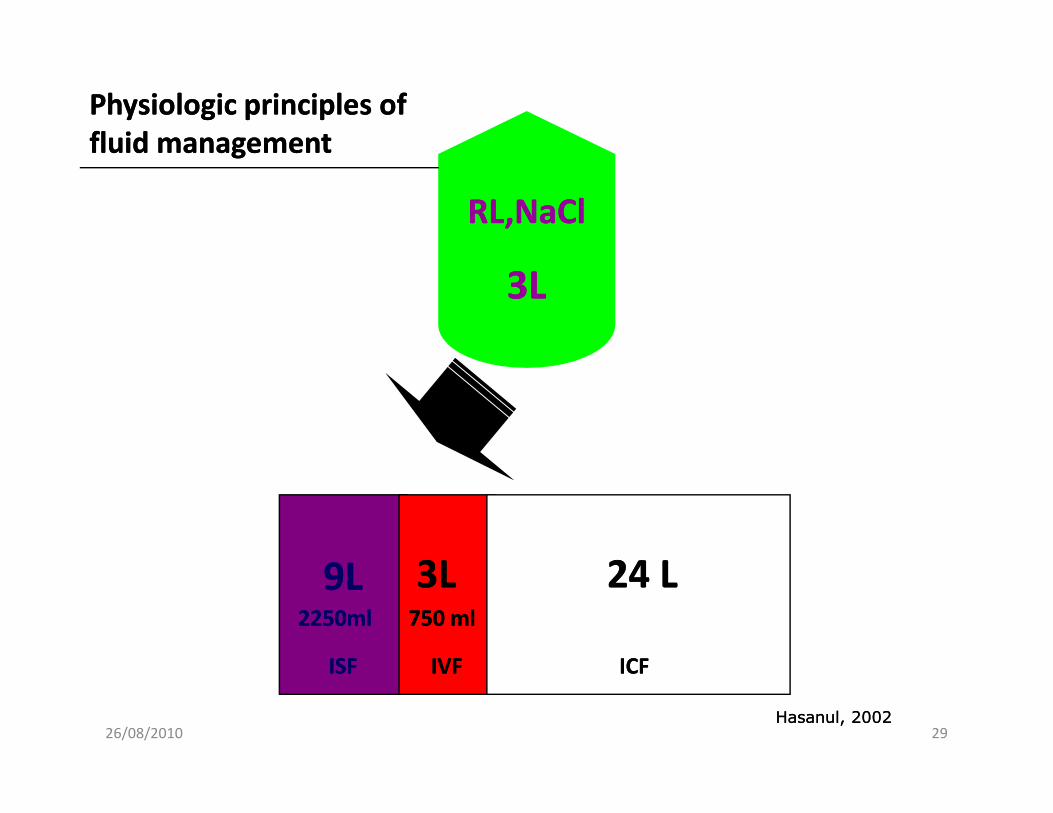
RL,NaClRL,NaCl
3L3L
Physiologic principles of Physiologic principles of
fluid managementfluid management
26/08/2010 29
ISF
9L9L
ISFISF IVFIVF ICFICF
3L3L 24 L24 L2250ml2250ml 750 ml750 ml
Hasanul, 2002Hasanul, 2002

AlbuminAlbumin--
5%5%
1 L1 L
Physiologic principles of Physiologic principles of
fluid managementfluid management
26/08/2010 30
ISF
9L9L
ISFISF IVFIVF ICFICF
3L3L 24 L24 L1L1L
Hasanul, 2002Hasanul, 2002
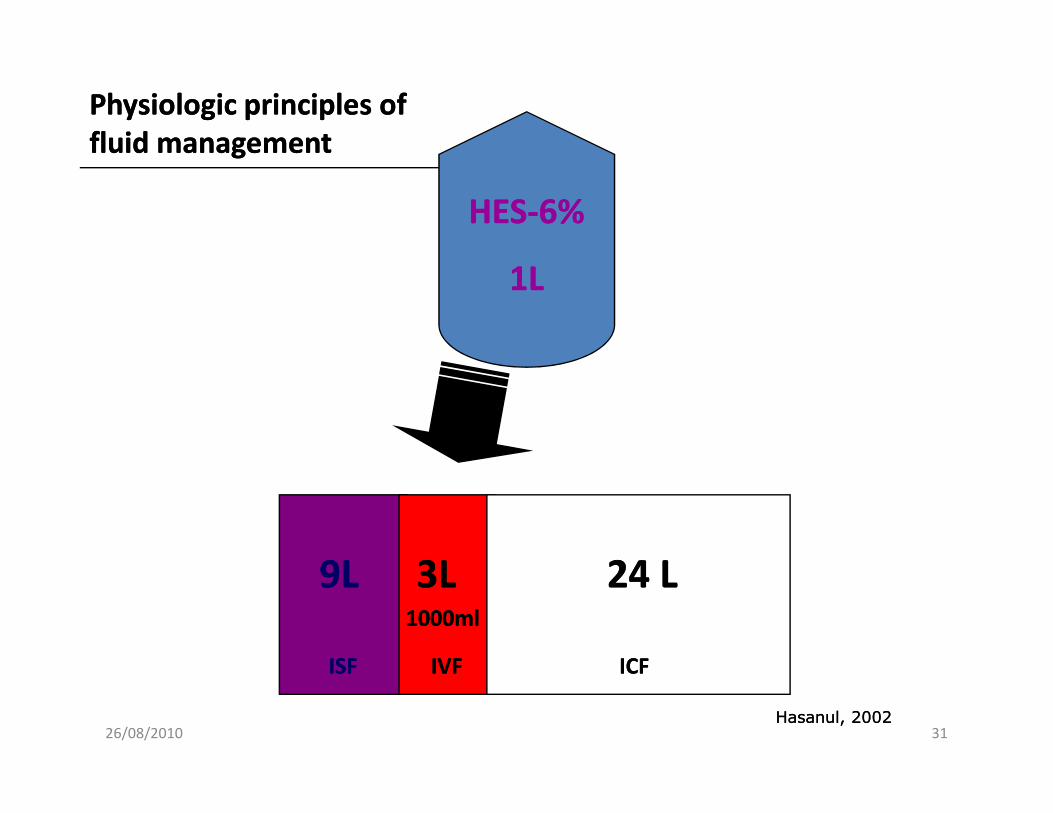
HESHES--6%6%
1L1L
Physiologic principles of Physiologic principles of
fluid managementfluid management
26/08/2010 31
ISFISFISF IVFIVF ICFICF
3L3L 24 L24 L1000ml1000ml
Hasanul, 2002Hasanul, 2002
9L9L
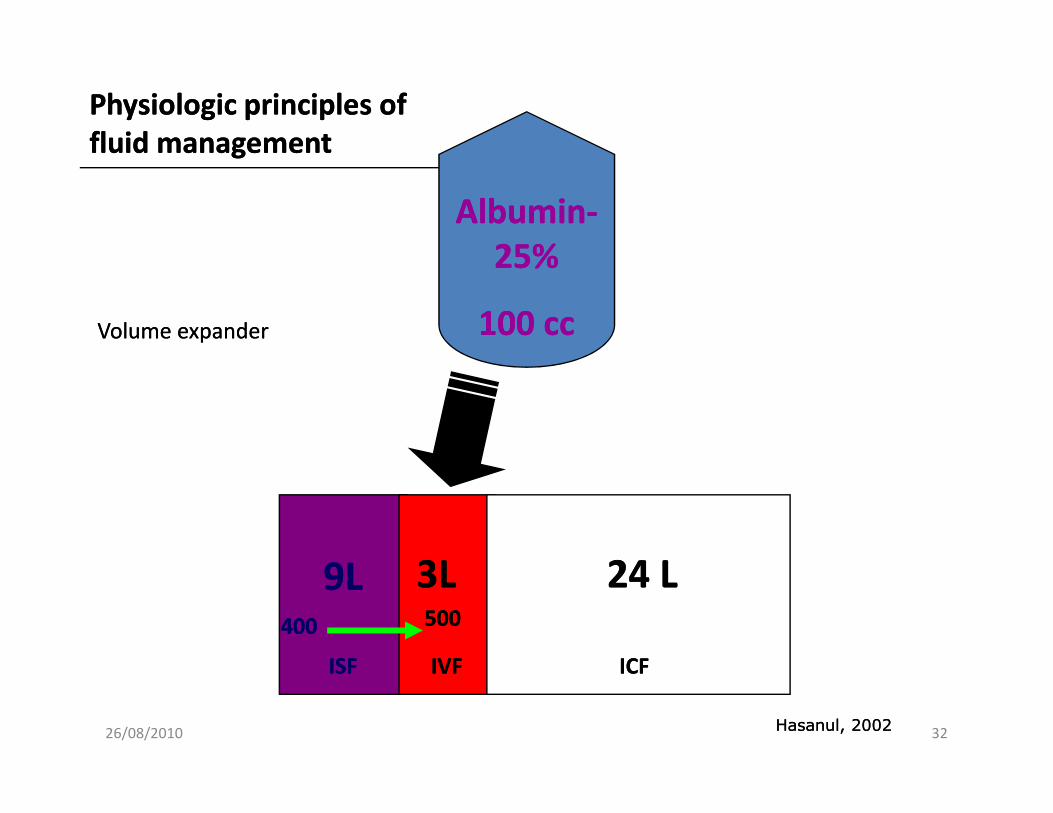
AlbuminAlbumin--
25%25%
100 cc100 cc
Physiologic principles of Physiologic principles of
fluid managementfluid management
Volume expanderVolume expander
26/08/2010 32
ISF
9L9L
ISFISF IVFIVF ICFICF
3L3L 24 L24 L500500
Hasanul, 2002Hasanul, 2002
400400

HaemacelHaemacel
1L1L
Physiologic principles of Physiologic principles of
fluid managementfluid management
26/08/2010 33
ISFISFISF IVFIVF ICFICF
3L3L 24 L24 L700ml700ml
Hasanul, 2002Hasanul, 2002
9L9L300ml300ml
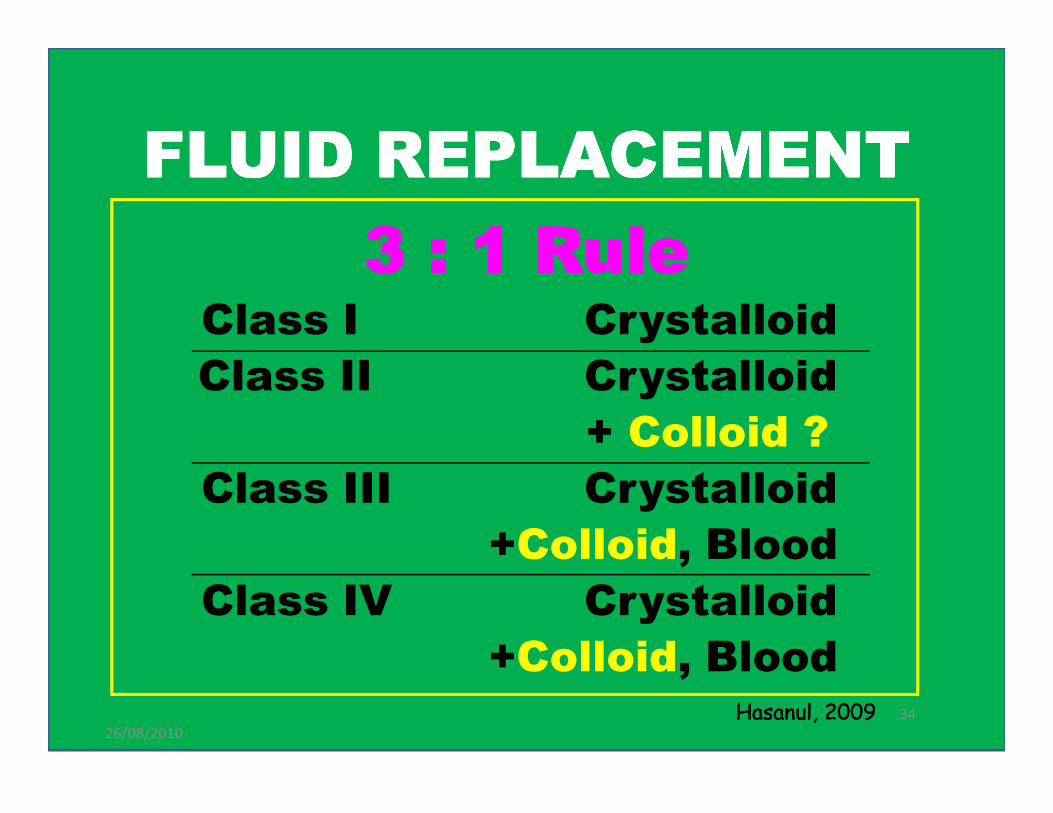
FLUID REPLACEMENTFLUID REPLACEMENTFLUID REPLACEMENTFLUID REPLACEMENT
3 : 1 Rule3 : 1 Rule3 : 1 Rule3 : 1 Rule3 : 1 Rule3 : 1 Rule3 : 1 Rule3 : 1 RuleClass I Crystalloid
Class II Crystalloid
+ Colloid ?
26/08/2010
34
+ Colloid ?
Class III Crystalloid
+Colloid, Blood
Class IV Crystalloid
+Colloid, BloodHasanulHasanul, , 20092009
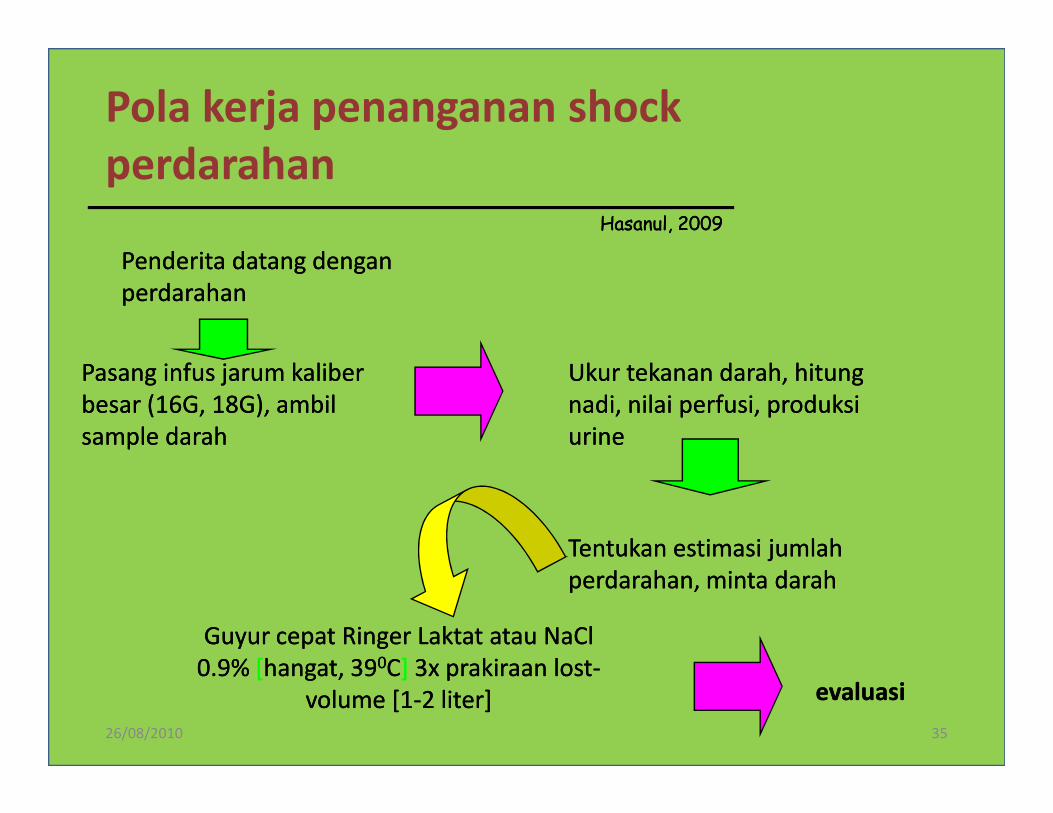
Pola kerja penanganan shock
perdarahan
Penderita datang dengan Penderita datang dengan
perdarahanperdarahan
Pasang infus jarum kaliber Pasang infus jarum kaliber
besar (16G, 18G), ambil besar (16G, 18G), ambil
Ukur tekanan darah, hitung Ukur tekanan darah, hitung
nadi, nilai perfusi, produksi nadi, nilai perfusi, produksi
HasanulHasanul, , 20092009
26/08/2010 35
besar (16G, 18G), ambil besar (16G, 18G), ambil
sample darahsample darah
nadi, nilai perfusi, produksi nadi, nilai perfusi, produksi
urineurine
Tentukan estimasi jumlah Tentukan estimasi jumlah
perdarahan, minta darahperdarahan, minta darah
Guyur cepat Ringer Laktat atau NaCl Guyur cepat Ringer Laktat atau NaCl
0.9%0.9% [[hangat, 39hangat, 3900CC] ] 3x prakiraan lost3x prakiraan lost--
volume [1volume [1--2 liter]2 liter] evaluasievaluasi
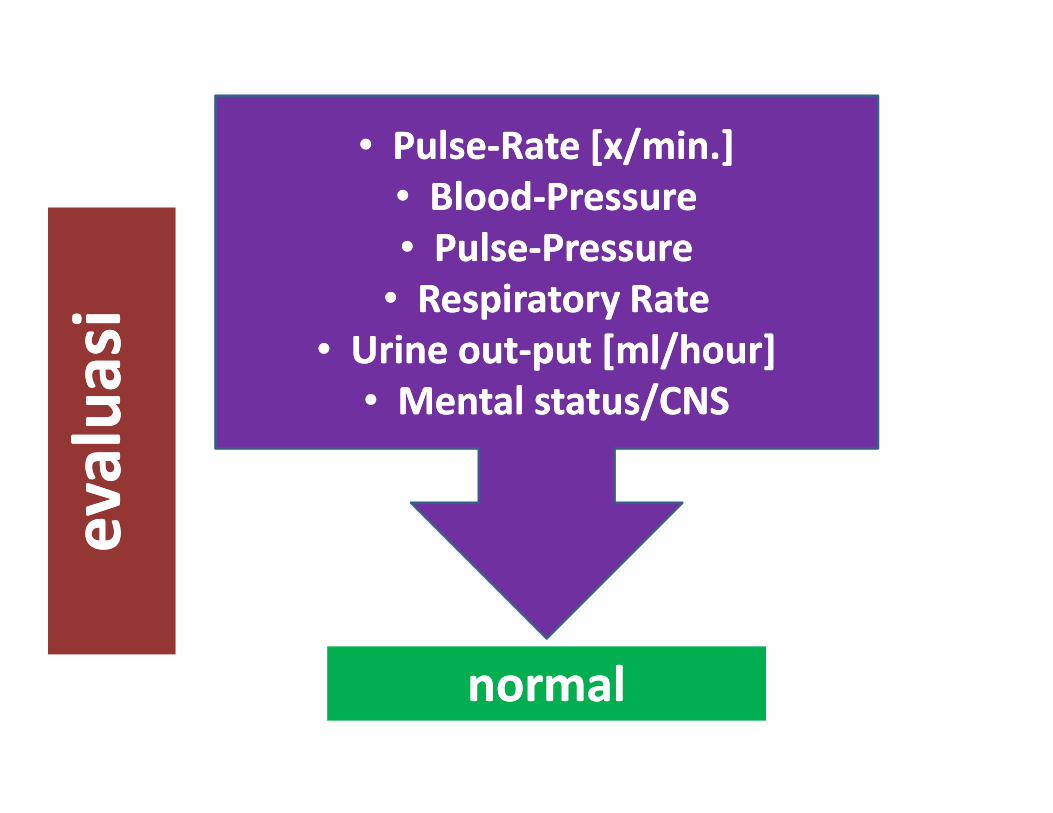
•• PulsePulse--Rate [x/min.]Rate [x/min.]
•• BloodBlood--PressurePressure
•• PulsePulse--PressurePressure
•• Respiratory RateRespiratory Rate
•• Urine outUrine out--put [ml/hour]put [ml/hour]
•• Mental status/CNSMental status/CNS
ev
alu
asi
ev
alu
asi
•• Mental status/CNSMental status/CNS
normalnormal
ev
alu
asi
ev
alu
asi

Thank you for listeningThank you for listeningThank you for listeningThank you for listeningThank you for listeningThank you for listeningThank you for listeningThank you for listening
and to be continuedand to be continuedand to be continuedand to be continuedand to be continuedand to be continuedand to be continuedand to be continued
8/26/2010 37
and to be continuedand to be continuedand to be continuedand to be continuedand to be continuedand to be continuedand to be continuedand to be continued


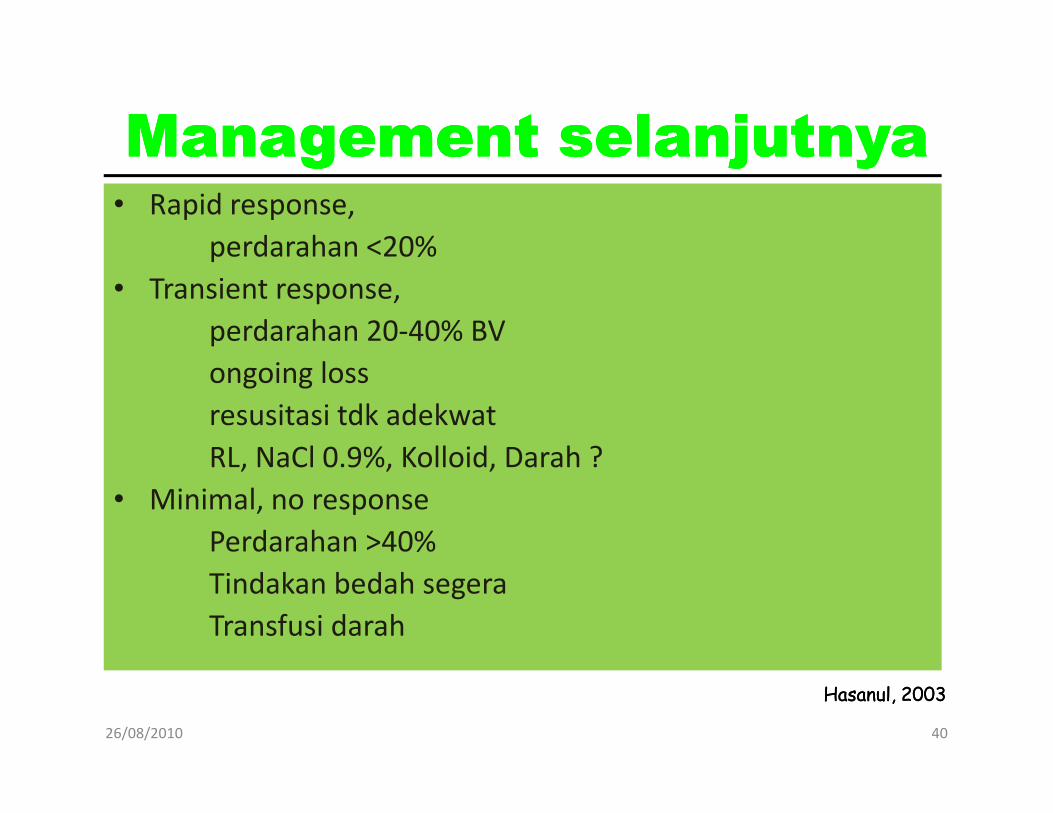
ManagementManagementManagementManagement selanjutnyaselanjutnyaselanjutnyaselanjutnya• Rapid response,
perdarahan <20%
• Transient response,
perdarahan 20-40% BV
ongoing loss
resusitasi tdk adekwat
26/08/2010 40
resusitasi tdk adekwat
RL, NaCl 0.9%, Kolloid, Darah ?
• Minimal, no response
Perdarahan >40%
Tindakan bedah segera
Transfusi darah
Hasanul, 2003Hasanul, 2003
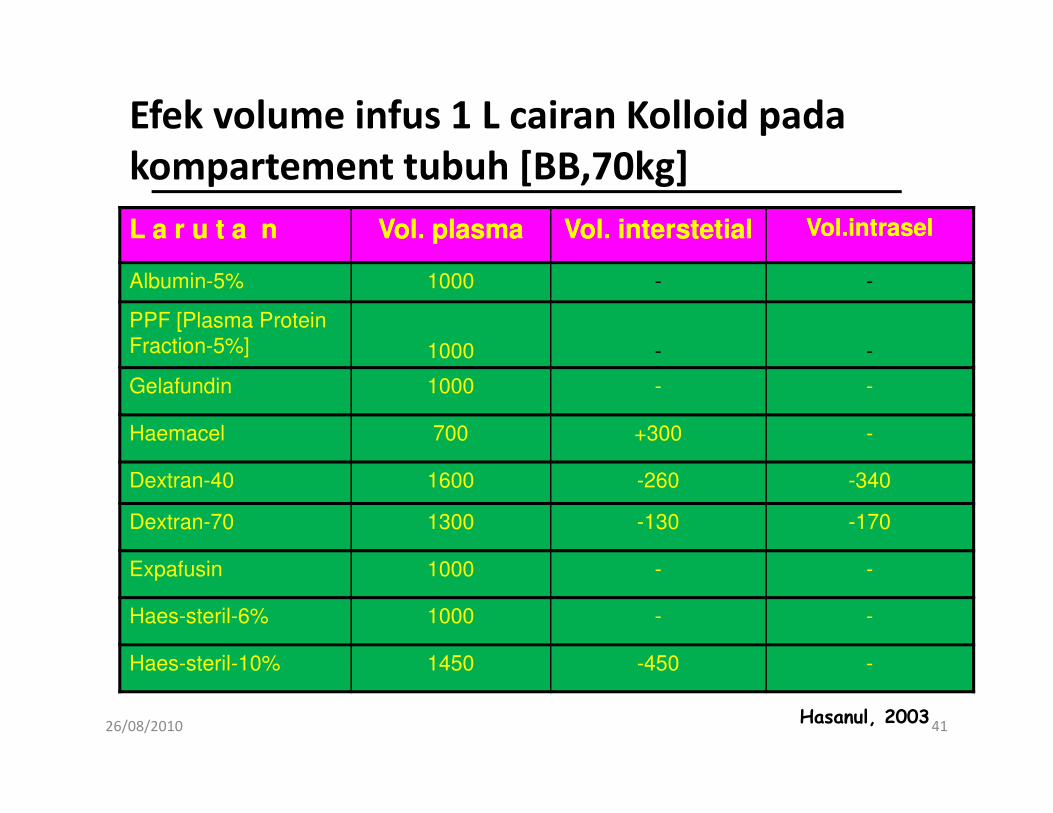
Efek volume infus 1 L cairan Kolloid pada
kompartement tubuh [BB,70kg]
L a r u t a nL a r u t a n Vol. plasmaVol. plasma Vol. interstetialVol. interstetial Vol.intraselVol.intrasel
Albumin-5% 1000 - -
PPF [Plasma Protein
Fraction-5%] 1000 - -
Gelafundin 1000 - -
26/08/2010 41
Haemacel 700 +300 -
Dextran-40 1600 -260 -340
Dextran-70 1300 -130 -170
Expafusin 1000 - -
Haes-steril-6% 1000 - -
Haes-steril-10% 1450 -450 -
Hasanul, 2003
TRANSIENT RESPONSE,TRANSIENT RESPONSE,
DARAH BELUM DATANG,DARAH BELUM DATANG,
KOLLOIDKOLLOID
26/08/2010 42
KOLLOIDKOLLOID
1:11:1
Transfusion, indications
• Indications for transfusion in normovolemic
anemia,
– VO2 < normal range (indicating an oxygen debt)
26/08/2010 43
– VO2 < normal range (indicating an oxygen debt)
– Blood lactate > 4 mmol/L
– O2ER > 0.5

TransfusiTransfusiTransfusiTransfusiTransfusiTransfusiTransfusiTransfusi,,,,,,,,
Target 7 Target 7 -- 9g%9g%
Rule of Rule of -- 55
26/08/2010 44
ml Wholeml Whole--Blood = 5 x delta Blood = 5 x delta HbHb x BB x BB
contoh:
BB 60 kg, Hb 6g%, WB yang dibutuhkan = 5 x 3 x 60
= 900 ml
= 4 bag [unit]
HasanulHasanul, , 20092009
Why does hypothermia happen?
26/08/2010 45
Hypothermia
� Casualties who are hypovolemic quickly
become hypothermic.
� Body temperatures below 91° F causes the
vicious triad.
26/08/2010 46
vicious triad.
– Hypothermia
– Acidosis
– Coagulopathy


![pediatric trauma.ppt2-rev-1.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000130-emergency-medicine/e… · Cancer 12.1% Homicide 11.6% Heart disease Leading causes of death among](https://img.dokumen.tips/doc/110x75/5f36ed0903449e7b3b25c8f5/pediatric-read-onlyocwusuacidcoursedownload1110000130-emergency-medicinee.jpg)


![EM-K 24.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000130-emergency... · © ACS 11 Blunt Trauma • A direct blow, eg, contact with the lower rim of the steering wheel •](https://img.dokumen.tips/doc/110x75/5e4cbe981f3dec559d49f06f/em-k-24ppt-read-onlyocwusuacidcoursedownload1110000130-emergency-.jpg)






















