-
Key Opinion Leaders Call- PLX-R18Hematological Programs
& Acute Radiation SyndromeSeptember 16, 2019
-
This presentation contains express or implied forward-looking
statements within the Private Securities Litigation Reform Act of
1995 and other U.S. Federalsecurities laws. For example, we are
using forward-looking statements when we discuss the expected
timing of obtaining regulatory approval for our variouspatient
trials and clinical data readout, proposed trials that may occur in
the future, the timing and implementation of our collaborations
with various partnersand the execution of definitive agreements
relating to such collaborations and the potential benefits and
impact our products could have on improving patienthealth care.
These forward-looking statements and their implications are based
on the current expectations of our management only, and are subject
to anumber of factors and uncertainties that could cause actual
results to differ materially from those described in the
forward-looking statements. The followingfactors, among others,
could cause actual results to differ materially from those
described in the forward-looking statements: changes in technology
and marketrequirements; we may encounter delays or obstacles in
launching and/or successfully completing our clinical trials; our
products may not be approved byregulatory agencies, our technology
may not be validated as we progress further and our methods may not
be accepted by the scientific community; we may beunable to retain
or attract key employees whose knowledge is essential to the
development of our products; unforeseen scientific difficulties may
develop withour process; our products may wind up being more
expensive than we anticipate; results in the laboratory may not
translate to equally good results in real clinicalsettings; results
of preclinical studies may not correlate with the results of human
clinical trials; our patents may not be sufficient; our products
may harmrecipients; changes in legislation; inability to timely
develop and introduce new technologies, products and applications;
loss of market share and pressure onpricing resulting from
competition, which could cause our actual results or performance to
differ materially from those contemplated in such
forward-lookingstatements. Except as otherwise required by law, we
undertake no obligation to publicly release any revisions to these
forward-looking statements to reflectevents or circumstances after
the date hereof or to reflect the occurrence of unanticipated
events. For a more detailed description of the risks and
uncertaintiesaffecting us, reference is made to our reports filed
from time to time with the Securities and Exchange Commission
Forward looking Statement
2
-
• Acute Radiation Syndrome (ARS)- Studies conducted and funded
by U.S. government (NIH, DOD)- Data for studies conducted under the
FDA animal rule suggest the potential of PLX-R18 cells to
stimulate
the regeneration of damaged bone marrow to increase survival and
produce blood cells, critically needed for this very sick patient
population
- FDA has cleared Pluristem’s Investigational New Drug (IND)
application for PLX-R18 in the treatment of ARS in case of nuclear
events
- FDA Orphan Drug Designation
• Phase I - Incomplete Hematopoietic Recovery Following
Hematopoietic Cell Transplantation (HCT)
− N= 24− Open-label trial allows for interim data analysis−
Clinical sites in U.S and Israel− FDA Orphan Drug Designation
Hematological and ARS Programs
3
-
• Cell therapy company focused on Regenerative Medicine•
Off-the-shelf placenta-derived cell product candidates• Two ongoing
Phase III studies• Publicly listed in Nasdaq and TASE• Favorable
safety profile and efficacy data from hundreds
of patients treated worldwide
• Best-in-class cell manufacturing technology producinghighest
quality cell products at a commercial scale
• Strong IP portfolio (over 120 granted patents)• Full time
employees: 160
Pluristem Therapeutics
4
-
PLURISTEM in one slide
5
Placenta
Technology
Allogeneic off-the-shelf
Simple IM administration
Adaptive slow release secretion of cytokines
Long term regenerative effect
-
Indication ProductCandidate Location Pre-Clinical Phase I Phase
II Phase III Funding
Clinical Pipeline
FDA Animal Rule
Critical Limb Ischemia
Intermittent Claudication
Hip Fracture
Acute Radiation Syndrome*
PLX-PAD
PLX-PAD
PLX-PAD
PLX-R18
Graft Versus Host Disease PLX-PAD
Incomplete recovery following bone marrow transplantation*
PLX-R18
U.S., Europe Israel
U.S., Europe South Korea,
Israel
U.S., Europe Israel
U.S.
Israel
U.S., Israel
* FDA Orphan Drug Designation
-
Key Opinion Leaders CallHematological Programs
Jacob M. Rowe, MD
-
8
• Hematopoietic cell transplantation (HCT), is a standard
treatment in various malignant and non-malignant conditions
• Diseases commonly treated with HCT include multiple myeloma,
non-Hodgkins lymphoma, Hodgkinsdisease, acute myeloid leukemia,
aplastic anemia or thalassemia, as well as non-malignant
diseasesand autoimmune disorders
• Transplant patients require extensive care and monitoring, and
sometimes need intensive treatmentfor complications
• The current treatment for incomplete hematopoietic recovery
after transplantation includesadministration of factors stimulating
blood cell growth, such as granulocyte-colony stimulating
factor(G-CSF), granulocyte-macrophage colony-stimulating factor
(GM-CSF), and erythropoietin.
• A significant number of patients do not respond to current
treatment and may require frequenttransfusions, which expose them
to transfusion-related risks such as allo-sensitization and
infectionsthat are also associated with significant costs
Hematopoietic Cell Transplantation- Overview
-
Incomplete Hematopoietic Recovery Following HCT Phase I Study -
Overview
Design Phase I, Open Label Study
Study population Incomplete hematopoietic recovery persisting at
list 3 months following HCT
Countries U.S., IsraelSample size 24 patients
Doses tested for PLX-R18* 1m/kg (n=3), 2m/kg (n=6), 4m/kg
(n=15)
Administration IM injections, 2 treatments at 5 days
interval
Primary efficacy endpoint Safety
Main Secondary & exploratory endpoints
Change in platelets, hemoglobin and neutrophil level,
transfusion frequency/dependency, QoL
Follow Up length 52 Weeks
9
* Granted an FDA-Orphan drug designation
-
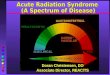
10
Incomplete Hematopoietic Recovery Following HCT Phase I Study –
Overview of 1st and 2nd Cohort
Incomplete hematopoietic recovery persisting at list 3 months
following HCTPlatelet ≤50,000/µL and/orHemoglobin ≤8 g/dL
and/or
Absolute neutrophil count ≤1,000/µL
-
11
0
20
40
60
80
100
120
140
160
-4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
42 44 46 48 50 52
Plat
elet
s (x1
0^3/
uL)
Weeks from treatment
Platelets
Median Cohort 1 Median Cohort 2
PLX 1st PLX 2nd
140-400 x10^3/uL
Platelets 6 months follow up• Median increase of platelets in
cohort 1 and cohort 2 was 130% and 170% respectively • A 65%
reduction in platelets transfusion was observed compared to last
month before
treatment in both cohorts
Incomplete Hematopoietic Recovery Following HCT Phase I Study –
Overview of 1st and 2nd Cohort
-
12
6
8
10
12
14
-4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
42 44 46 48 50 52
Hem
oglo
bin
(g/d
L)
Weeks from treatment
Hemoglobin
Median Cohort 1 Median Cohort 2
PLX 1st PLX 2nd
11.6-16.4 g/dL
Incomplete Hematopoietic Recovery Following HCT Phase I Study –
Overview of 1st and 2nd Cohort
Platelets 6 months follow up• Median increase in hemoglobin
levels in cohort 1 and cohort 2 was 34% and 36% respectively • A
68% reduction in RBC transfusion was observed compared to last
month before treatment
in both cohorts
-
13
0
1
2
3
4
-4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
42 44 46 48 50 52
Neu
trop
hils
(x10
^3/u
L)
Weeks from treatment
Neutrophils
Median Cohort 1 Median Cohort 2
PLX 1st PLX 2nd
1.96-7.23 x10^3/uL
Neutrophils 6 months follow up• A modest response in Neutrophil
level was seen in both cohorts
Incomplete Hematopoietic Recovery Following HCT Phase I Study –
Overview of 1st and 2nd Cohort
-
14
Recruitment for 1st and 2nd cohort was completed Following DSMB
approval 3rd cohort is now enrolling FDA Orphan drug designation
approval for incomplete hematopoietic recovery
Incomplete Hematopoietic Recovery Following HCT Phase I Study –
Study Status
• Primary endpoint- Safety data –No unexpected toxicities were
reported for PLX-R18IM administration of PLX-R18 cells was safe and
well tolerated
• Initial results shown in 1st and 2nd cohort, suggest PLX-R18
ability to stimulate the regeneration ofdamaged bone marrow to
produce platelets and red cells, critically needed for this very
sick patientpopulation and reduce their need of blood
transfusions
• The same trend seems to continue even at 9 months of
follow-up. Additional data is still collected• Cohort 3, targeting
dose of 4 million cells/kg, in now enrolling patients in U.S. and
Israel
-
PLX-R18 Potential Benefits for the Treatment of Hematological
Deficiencies
15
PLX-R18 may benefit additional bone marrow deficiency
syndromes
Benefits of PLX-R18• Multifactorial clinical effect, secretion
of range of cytokines in response to patient’s clinical condition•
Off the shelf approach, easy administration• Clinical grade, high
quality cells• Current clinical data suggest the potential of
PLX-R18 cells to stimulate the regeneration of damaged
bone marrow to produce blood cells, critically needed for this
very sick patient population and reducetheir need for blood
transfusions
-
Key Opinion Leaders CallRadiation Nuclear Medical
Countermeasures
Bert W. Maidment, Ph.D.
Executive ConsultantBWMaidment LLC
Overland Park, Kansas
DisclaimerThe views expressed in this presentation are my own
and are neither endorsed by nor do they
represent the opinions of the US Federal Government
-
Dr. Maidment was the former Assistant Director, Radiation
Nuclear Countermeasures Program at the National Institutes of
Health, National Institute of Allergy and Infectious Diseases,
Division of Allergy, Immunology, and Transplantation
(NIH/NIAID/DAIT) until retiring in 2016. He is now consulting for
the biomedical and pharmaceutical research and development
communities in academia and industry. His expertise spans from
basic biomedical research and development, product development, to
clinical development. He has experience building start-up
companies, industry divisions, and federal government programs. He
received his doctorate in Experimental Pathology from the State
University of New York at Buffalo, School of Medicine and
Biomedical Sciences and performed his research at the Roswell Park
Cancer Institute.
Bert W. Maidment, Ph.D.
-
Types of Radiation Exposure Radiological terrorist
events– RDD (Dirty Bombs)– RED– Food or Water
Contamination Nuclear detonation Accident
– Power Plant Release– Sealed radiological
sources
-
Health Impacts of Radiation Exposure
-
Radiation Countermeasure Needs
■Radionuclide Threats• Am-241• Co-60• Cs-137• I-131• Ir-192•
Po-210• Pu-238/239• Sr-90• U-235
■ Late Effects• Carcinogenesis• Cardiovascular Disease•
Cataractogenesis
■Acute Radiation Syndrome/Delayed Effects of Acute Radiation
Exposure (ARS/DEARE)
• Hematopoietic ARS: • Neutropenia• Thrombocytopenia• Anemia•
Lymphopenia
• GI ARS• CNS Injury• Cutaneous Injury• Lung Injury• Kidney
Injury• Combined Radiation Injury
■Biodosimetry Methods and Devices
-
Mechanisms of
Action―Anti-oxidants―Anti-inflammatories―Anti-apoptotics―Growth
factors and cytokines―Cell-based therapies―Others
Radionuclides―Blocking agents―Decorporation agents―Enhancement
of mucociliary clearance
Types of Radiation/Nuclear Medical Countermeasures
-
Neupogen®―Granulocyte Colony Stimulating Factor (GCSF)―
Increased NHP survival by ~39%―FDA approved March 2015
Neulasta®―Pegylated Granulocyte Colony Stimulating Factor
(peg-GCSF)― Increased NHP survival by ~42%―FDA approved November
2015
Leukine®―Granulocyte-Macrophage Colony Stimulating Factor
(GMCSF)―FDA approved March 2018
FDA Approved Radiation/Nuclear Medical Countermeasures
-
Radiation Countermeasure Gaps
■Acute Radiation Syndromes and Delayed Effects of Acute
Radiation Exposure
• Hematopoietic ARS: • Neutropenia• Thrombocytopenia• Anemia•
Lymphopenia
• GI ARS• CNS Injury• Cutaneous Injury• Lung Injury• Kidney
Injury• Combined Radiation Injury• Vascular Endothelial Cell
Injury
-
Radiation Countermeasure Characteristics
For Public Health Radiation Emergency Incident
• Safety (also in normal healthy subjects)• Efficacy• Mechanisms
of action well-understood• Civilian indication: administered 24
hours or more after exposure• Military indication: Pre-exposure
prophylaxis and post-exposure• Product approved for other medical
indications: • Ease of distribution (SNS or VMI), doctors familiar
with use • Ease of administration in mass casualty incident•
Stability and Storage• Demographic concerns: pediatric to elderly
populations
-
Pluristem’s PLX-R18 Advantages
- Cellular Product – putative apocrine mechanisms of action-
Ease of administration by intramuscular route and potential for
auto-
injector technology- Potentially administered by First
Responders, sparing health
professional resources during an emergency incident- Efficacy
shown in NHPs (FDA’s preferred animal model)- Non-clinical data
show increased neutrophil and platelet production- Potential for
efficacy in gastrointestinal, kidney and lung radiation
exposures- Clinical safety studies show product is
well-tolerated- Development for other medical indications- Maturity
of cGMP manufacture
-
Key Opinion Leaders CallAcute Radiation SyndromeArik Eisenkraft,
MD, MHA
-
27
PLX Cells Proposed Mechanism of Action
-
ARS Projects- Overview
Late Post Exposure
Department of Defense (DOD)Warfighter and Immediate Response
Department of Health and Human Services (DHHS)First Responders
and Hospitals
Armed Forces Radiobiology Research Institute
NIAID/NIH
Chronic Phase (Months-Years)Response
Phase
Exposure
Timeline
ResearchInstitutes &
Agencies
Governmental Departments
Initial Response (hours)
Clinical Syndrome
24h
Pre-exposure
Acute Phase (Days-Weeks)
DEARE (Months-Years)ARS (Hours-Weeks)
Early Post Exposure
-
Monitoring of survival, body weight, blood profile (CBC), BM
count, Plasma cytokines
C3H mice irradiation770 RAD Study Design
Bone histology at day 23
PLX-R18 Small Animal Studies Following the FDA Animal Rule
68% Survival Increase29
-
Placebo - 50%
20M/Kg - 67%
4/10M/Kg - 83/86%
Non irradiated and low radiation - 100%
Legend:
R : RadiatedR-ID: Low RadiationNR : Non-Radiated
R-00 : Not TreatedR-04 : 4 million cells per kgR-10 : 10 million
cells per kgR-20 : 20 million cells per kg
PLX-R18 Large Animal study Following the FDA Animal
RuleLD30/45
62 irradiated and non-irradiated Rhesus monkeys
Three cell doses:
• 4 M/cells/ Kg
• 10 M/cells/ Kg
• 20 M/cells/ Kg
Safety
Efficacy
35% Survival Increase(LD50)
30
-
Collaboration with Fukushima Medical UniversityEvaluating
PLX-R18 cells as a treatment for radiation damage to the GI and
BM
0
20
40
60
80
100
120
0 2 4 6 8 10 12 14
Surv
ival
(%)
Days after radiation exposure
w/o irradiation + Vehicle (n=3)
w/o irradiation + PLX-R18 (n=3)
PBI-BM40 (14Gy) + Vehicle (n=8)
PBI-BM40 (14Gy) + PLX-R18 (n=8)
TBI (11Gy) (n=3)
PLX 1st PLX 2nd
31
• 30% increase in survival rate and reduced weight loss•
Increased white blood cell and platelet counts • Preserve GI stem
cells activity and prevent severe damage to the
intestines
-
32
PLX-R18
Placebo
GT3
Saline
PLX-R18
Placebo
GT3
Saline
0 1 0 2 0 3 00
2 5
5 0
7 5
1 0 0
T im e p o s t- ir ra d ia t io n (d a y s )
Pe
rce
nt
su
rviv
al
74%
13%
S a l in e
G T 3
P la s m a -L y te
P L X -R 1 84%
100%
Log-rank test p < 0.0001Log-rank test p = 0.0003
PLX-R18 is Efficacious Upon Prophylactic Treatment (-24
hr)Relevant to first responders who are called to help and rescue
victims of an event
50-70% Survival Increase
-
Pluristem’s PLX-R18 Advantages• Cellular product with apocrine
MOA, potentially a multi-organ therapy for ARS: Non-clinical
(Mice/NHP) and clinical data show efficacy - increased neutrophil
and platelet production
Potential for efficacy in gastrointestinal, kidney and lung
radiation exposures
Clinical safety studies show product is well-tolerated
• Ease of administration by intramuscular route and no need for
tissue matching• Could be administered by various medical providers
including First Responders• Development for other medical
indications (BMT, hematological indications, mustard gas injury,
trauma…)• Maturity of cGMP manufacture (approved by regulators,
breakthrough production means)• Cryopreservation is an advantage
when deployment is needed in limited resources setting
33
-
Key Opinion Leaders CallPLX-R18
Yaky Yanay, CEO
-
PLX-R18 Product Development
35
Completion of the development and registration of
PLX-R18 for ARS, targeting government purchase contract
Completion of Phase I study
ARSPrograms
Hematological Programs
FDA- Agreed on the regulatory pathway NIH- Supporting additional
mechanism studies• DoD-Further small and large animal studies
in
relevant DoD models• BARDA- Government contract, submission
by
end of September Large animal study strategically designed
to show the superiority of our product in comparison to current
standard of care
Full contract
Recruitment for 1st and 2nd cohort was completed
Following DSMB approval 3rd cohort targeting dose of 4 million
cells/kg, in now enrolling patients in U.S. and Israel
• Expansion to additional hematological indications
-
[email protected] Israel +972-74-710-8600U.S.
+1-347-973-2098
www.Pluristem.com
36
Thank you
Slide Number 1Slide Number 2Slide Number 3Slide Number 4Slide
Number 5Slide Number 6Slide Number 7Hematopoietic Cell
Transplantation- OverviewIncomplete Hematopoietic Recovery
Following HCT Phase I Study - OverviewIncomplete Hematopoietic
Recovery Following HCT Phase I Study – Overview of 1st and 2nd
CohortIncomplete Hematopoietic Recovery Following HCT Phase I Study
– Overview of 1st and 2nd CohortIncomplete Hematopoietic Recovery
Following HCT Phase I Study – Overview of 1st and 2nd
CohortIncomplete Hematopoietic Recovery Following HCT Phase I Study
– Overview of 1st and 2nd CohortIncomplete Hematopoietic Recovery
Following HCT Phase I Study – Study StatusSlide Number 15Slide
Number 16Slide Number 17Slide Number 18Health Impacts of Radiation
ExposureRadiation Countermeasure NeedsSlide Number 21Slide Number
22Radiation Countermeasure GapsRadiation Countermeasure
CharacteristicsPluristem’s PLX-R18 AdvantagesSlide Number 26Slide
Number 27Slide Number 28PLX-R18 Small Animal Studies Following the
FDA Animal RulePLX-R18 Large Animal study Following the FDA Animal
RuleSlide Number 31Slide Number 32Pluristem’s PLX-R18
AdvantagesSlide Number 34PLX-R18 Product DevelopmentSlide Number
36



![CP.PHAR.295 Sargramostim (Leukine) · exposed to myelosuppressive doses of radiation (Hematopoietic Syndrome of Acute Radiation Syndrome [H-ARS]). Policy/Criteria : Provider must](https://img.dokumen.tips/doc/110x75/600f034e23039e08c74889d1/cpphar295-sargramostim-leukine-exposed-to-myelosuppressive-doses-of-radiation.jpg)