Embed Size (px)
Citation preview

HA
SAA
a
ARAA
KHVSAA
1
fas(is&cKlH
bfTau
MN
h0
Biological Psychology 105 (2015) 43–50
Contents lists available at ScienceDirect
Biological Psychology
jo ur nal home p age: www.elsev ier .com/ locate /b iopsycho
eart rate variability during adolescent and adult social interactions: meta-analysis
ara Shahrestani, Elizabeth M. Stewart, Daniel S. Quintana, Ian B. Hickie,dam J. Guastella ∗
utism Clinic for Translational Research, Brain and Mind Research Institute, University of Sydney, Australia
r t i c l e i n f o
rticle history:eceived 31 October 2013ccepted 24 December 2014vailable online 3 January 2015
eywords:eart rate variability
a b s t r a c t
Social interaction skill is important for psychological wellbeing, stress regulation, protection from disabil-ity and overall life satisfaction. Increase in activity of the vagus nerve, measured by heart rate variability(HRV), is associated with social interaction skill and decreased stress. In this meta-analysis we collatedstatistics from thirteen studies consisting of 787 participants who were participating in social interac-tions while HRV was simultaneously collected. Results revealed that while dyadic social interactionsdo not increase HRV generally from a baseline state, negative dyadic social interactions decrease HRV
agalocialdolescentdult
in a manner similar to the Trier Social Stress Task. Further, participants with psychopathology do notshow cardiac autonomic flexibility during social interactions as indicated by reductions under stress andincreases with subsequently positive social interactions. The role of age, gender and HRV index were alsoexamined as potential moderators of HRV. Implications for health and wellbeing resulting from exposureto negative social interactions are discussed.
. Introduction
Social interaction skill is central to well-being and healthyunctioning (Hari & Kujala, 2009; Ishii-Kuntz, 1990). These skillsre associated with many positive health outcomes, levels oftress and disease (Ono et al., 2011), disability, and life satisfactionNezlek, Richardson, Green, & Schatten-Jones, 2002). Some mentalllnesses are characterized by an inability to effectively regulateocial interactions (e.g., autism, schizophrenia) (Klin, Volkmar,
Sparrow, 1992), while social isolation and rejection increaseshronic stress (Blackhart, Eckel, & Tice, 2007; Bolger, Delongis,essler, & Schilling, 1989; Cacioppo & Hawkley, 2003) and is
inked to psychological and physical health problems (Cacioppo &awkley, 2003; House, 2001).
Social interactions require an individual to engage in dyadic-ased situations (Griffin & Gonzalez, 2003) and necessitate capacityor stress regulation during social tasks (Heinrichs & Gaab, 2007).
here has been growing interest in studying biological markersssociated with social interaction skill, with biological systemsnderlying social effectiveness proposed (Porges, 2007). Porges∗ Corresponding author at: Autism Clinic for Translational Research, Brain andind Research Institute, University of Sydney, 100 Mallett Street, Camperdown,SW 2050, Australia. Tel.: +61 2 351 0539; fax: +61 2 351 0855.
E-mail address: [email protected] (A.J. Guastella).
ttp://dx.doi.org/10.1016/j.biopsycho.2014.12.012301-0511/© 2014 Elsevier B.V. All rights reserved.
© 2014 Elsevier B.V. All rights reserved.
(2007), in particular, has described the activity of the myelinatedvagus in contributing to the control of facial muscles, middle ear,and laryngo-pharyngeal muscles, which are critical for under-standing social cues and responding effectively (through facialexpression or vocalization). Moreover, Porges (2003) has arguedthat the myelinated vagus can be differentially disrupted by stressto disable effective social interaction, through the activation of theadreno-cortical system. The role of the vagus in states of stress andsocial interaction or relaxation is referred to as Polyvagal theory(Porges, 2007).
The ability of the body to regulate autonomic activity in a dyadicinteraction, or stressful and challenging social contexts, has beendescribed as autonomic flexibility (Appelhans & Luecken, 2006;Friedman & Thayer, 1998). Autonomic flexibility refers to adaptivechanges in arousal, respiration, heart rate, and attention that arisefrom parasympathetic nervous system regulation, and is linked toincreases in vagal tone (Kok & Fredrickson, 2010). Thus, effectivesocial interaction may reflect both increased activity of the myelin-ated vagus, leading to flexible and responsive facial, vocal, andauditory systems in the social environment, and effective stressregulation with stressful social contexts, as indicated by a reducedadreno-cortical response. While Polyvagal theory is not without
critics (Grossman & Taylor, 2007), alternate models also highlightthe importance of the vagus nerve for social interaction. The Neu-rovisceral Integration Model, for instance, conceptualizes cardiacvariability as an index of autonomic nervous system regulation,
4 ical Ps
rTptsws
vtiaoop2snt
stLptelha2aTtsaobit2dH
HcmdGiwortawa2RG
i(ftts
4 S. Shahrestani et al. / Biolog
elated to attentional and affective control (Thayer & Lane, 2000).hese authors argue HRV may play a role in the organization ofhysiological resources to assist goal directed behavior, an impor-ant component of social interaction skill. Further, the authorsuggest the GABAergic, and other inhibitory pathways, associatedith the amygdala may play a role in regulating autonomic nervous
ystem outflow (Thayer & Lane, 2009).Heart rate variability (HRV) has been used to approximate
agus nerve outflow. It represents the beat-to-beat variation inhe duration of the R–R interval (heart period), reflecting complexnteractions between parasympathetic, sympathetic, mechanicalnd other factors on the pacemaker located at the sinoatrial nodef the heart (Billman, 2011). When individuals are in a relaxedr resting state, HRV is generally increased, reflecting greaterarasympathetic activity that facilitates social interaction (Porges,007). In contrast, when individuals are faced with challenging ortressful events, a reduction in vagal influence on the sino-atrialode inhibits parasympathetic nervous system activity, preparinghe person for a ‘flight or fight’ response (Porges, 2007).
Autonomic flexibility appears to be associated with refinedocial skills in dyadic interaction contexts and improved regula-ion in stressful or challenging social environments (Appelhans &uecken, 2006). For instance, when pairs of women discussed areviously seen upsetting film, those who regulated their emo-ions showed higher HRV than those who did not regulate theirmotions (Butler, Wilhelm, & Gross, 2006). Discussing a majorife event with a supportive friend has also been associated withigher HRV, whereas discussing with an ambivalent friend has beenssociated with lower HRV (Holt-Lunstad, Birmingham, & Light,008). Lower HRV was even associated with poorer recovery afternticipating a stressor (Waugh, Panage, Mendes, & Gotlib, 2010).hus, HRV appears to predict regulation of emotions in both posi-ive and supportive social interactions and stressful or challengingocial contexts. Furthermore, the valence of a dyadic social inter-ction task (i.e., positive or negative) may moderate the directionf HRV change during social interactions in a manner predictedy Polyvagal theory. In one study, negative appraisal by an exper-
menter was associated with decreased HRV, while an apology ledo HRV increasing back to baseline levels (Whited, Wheat, & Larkin,010). Similarly, the experience of failure in a stressful alarm testecreased HRV in adolescents, but reuniting with parents increasedRV (Willemen, Goossens, Koot, & Schuengel, 2008).
A number of other factors are known to potentially influenceRV including age, gender and respiration rate. Age can signifi-antly impact measurements of HRV (Antelmi et al., 2004) withiddle aged participants recovering from a marital disagreement
isplaying lower HRV than older participants (Smith et al., 2009).ender also appears to play a role in moderating HRV responses
n an index specific manner with one study showing that whileomen score higher on some indexes of HRV, men score higher on
thers (Antelmi et al., 2004). A study into the HRV responses of mar-ied couples during collaboration and disagreement tasks showedhat while some women displayed greater autonomic flexibilitycross tasks than men did, gender related differences increasedith age (Smith et al., 2009). Other factors that have demonstrated
n impact on HRV include respiration rate (Quintana & Heathers,014; Song & Lehrer, 2003), cognitive load (Thayer, Hansen, Saus-ose, & Johnsen, 2009) and posture (Lipsitz, Mietus, Moody, &oldberger, 1990).
In this meta-analysis, we assessed the impact of dyadic socialnteraction tasks on HRV. Based on Porges’ Polyvagal theoryPorges, 2003), we hypothesized that HRV responses would dif-
erentiate between states of social disengagement and stress andhose of relaxation (baseline) and social engagement. In addi-ion, we directly compared these results against a well-knownocial stress task that does not involve dyadic social interactionychology 105 (2015) 43–50
between participants, the Trier Social Stress Task (TSST). In theTSST, participants deliver a speech without feedback so, whilestressful, it does not involve reciprocated dyadic social interac-tion. Past research suggests the task results in decreases in HRVfrom baseline measures (Codispoti, Mazzetti, Baldaro, Tuozzi, &Trombini, 2001; Fagundes et al., 2011; Fagundes, Diamond, & Allen,2012; Mauss, Wilhelm, & Gross, 2003; Page-Gould, Mendes, &Major, 2010; Waugh et al., 2010). Inclusion of the TSST allowsus to determine whether negative reciprocated, dyadic socialinteractions decrease HRV to the extent of an established acutesocial stressor task. Finally, this meta-analysis will examine theinfluence of psychopathology on HRV responses during socialinteractions. Adults with schizophrenia (Bär et al., 2007) anxi-ety disorders (Alvares et al., 2013; Chalmers, Quintana, Abbott,& Kemp, 2014) major depressive disorders (Henje Blom, Olsson,Serlachius, Ericson, & Ingvar, 2010; Kemp et al., 2010), and alcoholdependence (Quintana, McGregor, Guastella, Malhi, & Kemp, 2013)show reduced HRV generally. Some researchers have argued thatHRV during social interactions may differ in individuals with psy-chopathology; specifically those associated with social dysfunction(Porges, 2003).
A number of moderator variables were included based onavailability of data in the current literature. These included psy-chopathology, age, gender and type of HRV index used. We didnot expect gender to play a role in determining cardiovascularresponses to social interaction with pooled indices as while someindices are higher in men others are higher in women (Antelmiet al., 2004) and may equate when pooled across type of HRV index.However, we hypothesized that there would be decreased reactiv-ity in older participants.
2. Methods
2.1. Criteria for considering studies for this review
All studies that evaluated HRV in social tasks in adolescents and adults wereincluded (excluding studies in children aged <12 years old). All studies examinedHRV as explicitly measured during performance of differing task types and comparedto a baseline measure.
2.2. Inclusion and exclusion criteria
Participants included in this review were either typically developing controlsor adolescents and adults characterized as having psychopathology (Smeekens,Didden, & Verhoeven, 2013; Willemen, Schuengel, & Koot, 2009) or trait markers ofsocial anxiety (Mauss et al., 2003). Tasks used to study social behavior in adolescentsand adults were similar in design, however, to ensure age effects did not confoundresults, we conducted moderator analyses where possible.
2.3. Types of tasks
Both dyadic tasks such as ‘cyberball’ and marital conflict discussion tasks aswell as non-interactive tasks, where participants were delivering a speech with nofeedback, were used (see Table 1 for specific tasks). All studies included involveda participant wearing a device that collected interbeat intervals during baselineperiods as well as during the social performance task.
2.3.1. Baseline tasksThe control condition used across studies requires participants to sit as still as
possible for a short period of generally 5–15 min (Hastings et al., 2008).
2.3.2. Trier social stress testThe Trier Social Stress test (TSST; Kirschbaum, Pirke, & Hellhammer, 1993) con-
sists of the active performance of a speech and mental arithmetic task, during whicha committee threatens the self-esteem of the participant. The committee pretendsto evaluate the participant’s performance, providing no signs of social support, lead-ing the participant to question the accuracy of their own behavior. The participantexperiences stress as a result of self-questioning and feelings of lack of control (Het,
Rohleder, Schoofs, Kirschbaum, & Wolf, 2009). We included the TSST as a compara-tor. While it is a social stress task, it does not involve any reciprocal dyadic interaction(Shahrestani, Stewart, Quintana, Hickie, & Guastella, 2014). Other examples of recip-rocal dyadic interaction tasks include those where only one experimenter is present,rather than a panel, and this experimenter interacts with the participant in order
S. Shahrestani et al. / Biological Psychology 105 (2015) 43–50 45
Table 1Summary of parameters used in studies that were included in the meta-analysis.
References Experimental task Population Psychopathology/healthy Task valence, effect size (g) Respirationrate mea-sured/controlled
Measures
Butleret al.(2006)
Pairs of womenwatched anupsetting film anddiscussed it.
190 female collegestudents with a mean ageof 20 years participated.
Participants assumed to behealthy. No exclusioncriteria specified in paper.
Neutral, 0.004Yes RSA
Positive, 0.108Negative, 0.062
Codispoti et al.(2001)
Public speakingtask
60 young women from acollege population with amean age of 23.9.
Participants were healthywith those reportingcentral nervous system,cardiovascular andgastrointestinal disordersbeing excluded.
Negative, −0.451 Yes RSA
D’Antonoet al.(2005)
Agreeable andquarrelsome roleplays
College men (N = 33) andwomen (N = 33) with amean age of 21.
Participants were healthy.Positive, (−0.186, −0.175,−0.179, −0.519) No RSA
Negative (−1.043, −0.677,−0.167, −0.335)
Fagundes et al.(2011)
Trier Social StressTask
84 women who hadcompleted treatment forbreast cancer wereincluded in this study.Mean age of participantswas 51.6 years.
Exclusion criteria includedprior history of cancer,more than 5 h a week ofvigorous exercise, highBMI, diabetes, pulmonarydisease, hypertension andliver or kidney failure.
Negative, −0.596 No RMSSD
Fagundes et al.(2012)
Trier Social StressTask
Sample consisted of 11014-year-old adolescents(54 boys and 56 girls). Atage 14 participantscompleted assessments.
Participants were healthyand were screened formajor psychiatric illness,endocrine andcardiovascular disorders orif they were takingmedications withendocrine orcardiovascular side effects.
Negative, −0.036 Yes RSA
Kemper andShaltout(2011)
Communication ofcompassion duringloving-kindnessmeditation.
5 subjects were all womenwith a mean age of 43.6years.
Subjects were healthyvolunteers.
Positive, 1.821 Yes HF HRV
Mauss et al.(2003)
Speech task 35 participants including18 high trait social anxiouswith an average age of 19.3years and 17 low traitsocially anxious with anaverage age of 19.0 yearswere selected.
Participants were selectedto be low versus highanxiety based on the SocialPhobia and AnxietyInventory.
Negative, −0.385 Yes RSA
Mulderet al.(2009)
Simulatedambulancedispatcher’s task(emphasis onadaptive support).
12 participants, two malesand ten females with amean age of 21.1 yearscompleted the study one.
Participants assumed to behealthy although nospecific exclusion criteria isprovided.
Negative, −0.506 No HF HRV
19 participants, five malesand fourteen females witha mean age of 22.3 yearscompleted study two.
Murray-Close(2011)
Experience ofexclusion
131 female emergingadults with a mean age of19.13.
Participants were assumedto be healthy and noexclusion criteriapertaining topsychopathology wereprovided.
Negative, −0.328 Yes RSA
Page-Gouldet al. (2010)
Trier Social StressTask
125 adults recruited from aprimarily universitycommunity. Half werecollege students. Overallthe mean age was 28.1years.
Participants were assumedto be healthy although nospecific exclusion criteria isprovided.
Negative, −0.197 No RSA
Smeekens et al.(2013)
Social SkillsPerformanceAssessment
16 male participants withautism spectrum disordersand a mean age of 23.46years participated. 19typically developing adultswith a mean age of 26.23years were also recruited.
Participants had adiagnosis of ASD or wereincluded in the non-ASDgroup. Exclusion criteriaincluded cardiac problems,respiratory problems, liveror kidney failure.
Neutral (0.238, 0.148) No SDNN
Tininenko et al.(2012)
Trier Social StressTask
74 undergraduate femaleparticipants were includedin this study with a meanage of 20.1 years.
None of the participantsendorsed having heart ratearrhythmia howeveraround 10% reportedhaving asthma.
Neutral, −0.644 Yes RSA

46 S. Shahrestani et al. / Biological Psychology 105 (2015) 43–50
Table 1 (Continued)
References Experimental task Population Psychopathology/healthy Task valence,effect size (g)
Respirationrate mea-sured/controlled
Measures
Waugh et al.(2010)
Speech task 61 individuals with a meanage of 33.6 years. 33 ofthese individuals werefemale.
Participants were assumedto be healthy – allparticipants were free ofcardiovascular disease andwere not taking anycardiovascular medication.
Negative,−0.027
Yes RSA
Willemen et al.(2008)
Alarm stress taskwith reunion withthe parent.
23 adolescents including13 boys with a mean age of12.8 in a clinical sampleand 10 boys with a mean
Both the clinical samplefrom the clinic of anacademic center for childand adolescent psychiatry
as uson-clie com
Positive, 0.099 Yes RSA
tiaTt
2
mapT
2
ftNa
2
oramndatqf(
tpata1
Sst
MpP22
2
2
eRP
age of 12.64 in thenon-clinical sample.
wnth
o deliver the subject matter of the speech (Mauss et al., 2003). In a separate mod-fication, participants are relaxed, give a public speech for four minutes and thenre coaxed into relaxation again (Codispoti et al., 2001). These tasks differ from theSST where the silence and lack of feedback from a panel of experimenters acts ashe central stressor employed in the task.
.3.3. Dyadic interactive tasks (all other)Remaining tasks were classified as interactive. That is, they involved two or
ore individuals partaking in an interaction in which they communicate with onenother. Types of tasks varied but included role play, discussion tasks, exclusionaradigms and support tasks (details of papers using each study is provided inable 1).
.3.4. Positive, negative and neutral tasksWe classified positive tasks as those that were designed to elicit positive affect
rom participants (e.g., agreement tasks between spouses), and negative tasks ashose that were designed to elicit negative affect or stress (e.g., disagreement tasks).eutral tasks were those that were not designed to elicit any particular valence offfect (e.g., discussing un-emotive content).
.4. Primary outcome measures
Respiratory sinus arrhythmia refers to characteristic changes in heart period,ccurring in the frequency corresponding to respiration, and thought to reflect vagalegulation of the cardiac system (Berntson et al., 1997). Time and frequency domainnalyses are two primary approaches to measuring HRV. Time domain analysiseasures the changes in heart rate over time, or the intervals between successive
ormal cardiac cycles (Sztajzel, 2004). HRV can also be measured by frequency-omain analysis, which produces a decomposition of the total variance ‘power’ of
continuous series of beats. One common mode of spectral analysis is fast Fourierransform analysis, which characterizes the power of oscillations within certain fre-uency bands (Sztajzel, 2004). Two or three main bands are often used; very lowrequency (VLF) 0.003–0.04 Hz, low frequency (LF) 0.04–0.15 Hz, and high frequencyHF) 0.15–0.4 Hz.
RSA may also be quantified by portioning in the frequency band, characterized byhe respiration rate of an individual and separated from other slower rhythmic com-onents. A third method, uses a complex detrending procedure applied to both timend frequency domain approaches, that eliminates complex aperiodic trends in theime series and separates RSA from other frequency components. Most importantly,ll three of these methods are highly correlated (Grossman, Van Beek, & Wientjes,990).
One included study utilized RMSSD (Fagundes et al., 2011) and another usedDNN as the main index (Smeekens et al., 2013). All other studies either reportedome measure of HF or RSA. A moderator analysis was conducted in order to explorehe potential moderating effect of HRV measure used.
Two studies used the Polar heart rate monitor system (D’Antono, Moskowitz,iners, & Archambault, 2005; Fagundes et al., 2011) while others used a bioam-
lifier system (Butler et al., 2006; Codispoti et al., 2001; Fagundes et al., 2012;age-Gould et al., 2010; Tininenko, Measelle, Ablow, & High, 2012; Waugh et al.,010) or ambulatory monitoring systems (Kemper & Shaltout, 2011; Willemen et al.,008).
.5. Search methods for identification of studies
.5.1. Initial searchThe initial search was conducted on 31st of January 2013. The search strat-
gy followed guidelines outlined in the Preferred Reporting Items for Systematiceviews and Meta-Analyses (PRISMA) (Moher, Liberati, Tetzlaff, Altman, & TheRISMA Group, 2009) statement.
ed, and anical sample frommunity.
Electronic databases including PsycINFO, PubMed/MEDLINE and EMBASE weresearched using combinations of the following terms: social, dyadic, interaction, syn-chrony, heart rate variability, respiratory sinus arrhythmia or vagal. Databases weresearched using the following search script: (Social[All Fields] OR Dyadic[All Fields]OR (“Interaction”[Journal] OR “interaction”[All Fields]) OR Synchrony[All Fields])AND (((“heart rate”[MeSH Terms] OR (“heart”[All Fields] AND “rate”[All Fields]) OR“heart rate”[All Fields]) AND variability[All Fields]) OR (respiratory[All Fields] AND(“arrhythmia, sinus”[MeSH Terms] OR (“arrhythmia”[All Fields] AND “sinus”[AllFields]) OR “sinus arrhythmia”[All Fields] OR (“sinus”[All Fields] AND “arrhyth-mia”[All Fields]))) OR vagal[All Fields]). In addition to these electronic searches, eachreport’s citation list was examined for additional studies. Reference lists of relevantreview papers identified in the literature search were also examined for relevantreferences.
2.5.2. Data collectionThe search strategy involved screening titles and abstracts for duplicates and
identifying ineligible studies. Relevant statistics were then extracted from the eligi-ble studies in the form of means and standard deviations, and at times F or t values(Mauss et al., 2003; Mulder, Dijksterhuis, Stuiver, & de Waard, 2009; Page-Gouldet al., 2010). Information pertaining to individual studies is presented in Table 1.
2.6. Study characteristics
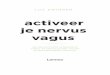
14 articles met our inclusion criteria from a total of 5948 studies (see Fig. 1,outlining the number of papers included and excluded at each stage of the meta-analysis). These included fourteen independent studies comprising 822 researchparticipants. The average number of participants per study was 58.71. All studiesemployed a baseline condition. Six studies employed a non-interactive paradigm(Codispoti et al., 2001; Fagundes et al., 2011, 2012; Mauss et al., 2003; Page-Gouldet al., 2010; Waugh et al., 2010) and all other studies employed an interactiveparadigm.
2.7. Statistical analyses
The Comprehensive Meta-Analysis (CMA; Borenstein, Hedges, Higgins, &Rothstein, 2005) program was used to transform results of individual studies intothe common effect size of Hedges’ g. Hedges’ g is a measure of the standardizeddifference between intervention and control condition that corrects for biases asso-ciated with small sample sizes and can be interpreted in the same way as Cohen’sd, whereby 0.2 represents a small effect, 0.5, a medium effect and 0.8, a large effect(Cohen, 1988).
To determine whether any evidence of publication bias was present, weinspected Egger’s regression intercept (Egger, Davey Smith, Schneider, & Minder,1997) and the corresponding p value. If bias was present we calculated the clas-sic fail safe N statistic. This technique determines whether there is a significantrisk of bias, and provides information about how many studies would be needed tooverturn obtained results.
A single overall meta-analysis was conducted to acquire an effect size for HRVduring social interaction relative to baseline. Following this, moderator analyseswere conducted to isolate the possible role of dyadic versus stress task, valence ofdyadic task, psychopathology diagnosis, gender, age and index of HRV and combi-nations of these moderators with valence, in the obtained result.
3. Results
Initially, we examined whether dyadic social interaction tasksand stress induction tasks differentially impacted HRV. It was foundthat dyadic interaction tasks (g = −0.201 p = 0.032, 95% CI −0.385,

S. Shahrestani et al. / Biological Psychology 105 (2015) 43–50 47
papers
−−rd
tdtatCt0iF
hlTfottg
trii−d−a
Fig. 1. Consort diagram outlining number of
0.017) and stress tasks (g = −0.277, p = 0.003, 95% CI −0.458,0.095) significantly reduced HRV overall. Inspection of Egger’s
egression intercept indicated that there was no significant evi-ence of publication bias present in this sample (p = 0.324).
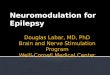
Using moderator analyses we further classified social interac-ion tasks as being dyadic positive tasks, dyadic negative tasks andyadic neutral tasks. The number of individual study effect sizeshat were used in the calculation of overall effect of positive, neg-tive and neutral tasks were 13, 7 and 4 respectively. We foundhat dyadic negative tasks reduced HRV (g = −0.356, p = 0.001, 95%I −0.562, −0.150). Positive dyadic tasks, however, did not appearo increase HRV significantly (g = 0.002, p = 0.992, 95% CI −0.354,.358). Analysis also revealed that dyadic neutral tasks had no
mpact on HRV (g = −0.116, p = 0.622, 95% CI −0.578, 0.345, seeig. 2).
Given the negative dyadic and stress based tasks appeared toave similar effects on HRV, for the remaining analysis we col-
apsed these groups together into a single ‘negative’ effect group.his allowed us to conduct moderator analyses based on valenceor the remaining variables. For the following analysis of the rolef psychopathology, age, gender and HRV index, we have furtheredhe analysis by separating statistics into positive, negative and neu-ral categories, to avoid the possibility of effects being masked. Onlyroupings including two or more studies are reported here.
We compared participants who were typically developingo those who were diagnosed with psychopathology, in HRVesponses, during social interactions. Participants who were typ-cally developing had significant differences in HRV during socialnteraction relative to baseline (g = −0.254, p < 0.001, 95% CI −0.392,
0.115). However, participants with diagnosis of psychopathologyid not show significant differences (g = −0.146, p = 0.629, 95% CI0.740, 0.447). In order to ensure valence played no role in thisnalysis we further separated groups by valence. These analysesincluded at each stage of the meta-analysis.
revealed that healthy participants showed decreases in HRV dur-ing negative tasks (g = −0.274, p = 0.002, 95% CI −0.448, −0.099) butnot during neutral (g = −0.206, p = 0.439, 95% CI −0.729, 0.316) orpositive tasks (g = −0.151, p = 0.315, 95% CI −0.446, 0.144).
Next we compared males and females in HRV responses tosocial interactions. Male participants (g = −0.185, p = 0.264, 95% CI−0.511, 0.140) did not show differences relative to baseline, whilefemale (g = −0.279, p = 0.003, 95% CI −0.464, −0.094) showed sig-nificant effects. Again we separated statistics by valence withineach gender, to ensure this was not a confounding factor. Thisanalysis revealed that both females (g = −0.380, p < 0.001, 95% CI−0.521, −0.239) and males (g = −0.487, p = 0.007, 95% CI −0.809,−0.125) responded to negative social environments. However, nei-ther females (g = 0.145, p = 0.681, 95% CI −0.548, 0.839) nor males(g = −0.058, p = 0.763, 95% CI −0.434, 0.318) showed changes inHRV from baseline in response to positive interactions. No changesfrom baseline were shown during neutral interactions for females(g = −0.340, p = 0.292, 95% CI −0.974, 0.293) or males (g = 0.190,p = 0.418, 95% CI −0.269, 0.649).
In examining the role of age in determining HRV, we found thatwhile individuals in their teens (g = −0.204, p = 0.046, 95% CI −0.406,−0.003) and those in their twenties showed significant decreasesin HRV during social interactions (g = −0.245, p = 0.002, 95% CI−0.399, −0.092), those thirty or older experienced no changesin HRV (g = −0.127, p = 0.624, 95% CI −0.634, 0.380). When wemoderated further by valence we found that individuals in theirteens (g = −0.348, p = 0.001, 95% CI −0.544, −0.152) and twenties(g = −0.307, p = 0.005, 95% CI −0.523, −0.092) experienced signif-icant HRV changes during negative social tasks. However, those
in the older category did not (g = −0.279, p = 0.068, 95% CI −0.579,0.021). Individuals in their twenties showed non-significantresponses to both positive and neutral interactions and no othergroupings were possible due to lack of statistics in groupings.
48 S. Shahrestani et al. / Biological Psychology 105 (2015) 43–50
asks a
sidbdw9−nwn
4
atrssarattmitmpsfeasvH
Fig. 2. Effect size and standard error for valence during dyadic t
Finally, we assessed whether the index of HRV used to mea-ure social interaction could be differentially sensitive. RSA as anndex of HRV differed from HF as an index of HRV. It was found thaturing social interactions RSA changed significantly relative toaseline (g = −0.270, p < 0.001, 95% CI −0.403, −0.136) however HFid not (g = −0.061, p = 0.769, 95% CI −0.472, 0.349). When valenceas factored in, it was revealed that both RSA (g = −0.296, p = 0.001,
5% CI −0.463, −0.129) and HF (g = −0.204, p = 0.039, 95% CI −0.398,0.010) successfully indexed changes in HRV from baseline duringegative tasks. RSA in tasks that were positive or neutral, however,as not significantly different to baseline and other groupings wereot possible.
. Discussion
This meta-analysis assessed the influence of social interactionnd stress on HRV in adolescents and adults. Overall, we foundhat dyadic social interactions reduced HRV. As predicted, thiseduction was moderated by the valence of the social task. Dyadicocial interactions that were negative reduced HRV, with effectize indicative of a small-to-medium effect. Dyadic interactions of
positive or neutral valence, however, did not alter HRV from aelaxed-state baseline. We then compared the effect of a knownnd well-established social stressor task, the TSST. Results showedhe TSST reduced HRV and this reduction was similar in magni-ude to a negative social interaction task. We examined potential
oderators of these effects on HRV. While typical control partic-pants showed changes in parasympathetic outflow during socialasks relative to baseline, those with psychopathology did not. This
ay suggest dysregulation of HRV in response to social tasks inarticipants with social dysfunction disorders. Participant genderhowed no discernible influence on results with both males andemales responding to negative, but not positive, social tasks. Asxpected, HRV flexibility appeared to reduce with age. Finally, we
ddressed conjecture around the HRV index that provides optimalensitivity to detect changes during social interaction tasks. Oncealence was accounted for, both RSA and HF indexed decreases inRV during negative social tasks.nd Trier Social Stress Task. Error bars represent standard error.
Negatively valenced social interactions impact on HRV in amanner that is comparable to the TSST – a well-known stressbased performance task. Reductions in HRV may represent a lossof autonomic flexibility and an increase in sympathetic activitysignaling the stress response (Porges, 2003). Negative social inter-actions have also been associated with increased cortisol levelsin other studies (Heffner et al., 2006; Saxbe, Repetti, & Nishina,2008). Independent measures of cortisol or sympathetic activitycould confirm whether decreases in HRV may reflect an increase insympathetic nervous system activity. Chronic negative social inter-actions significantly predict depressive symptoms (Okabayashi,Liang, Krause, Akiyama, & Sugisawa, 2004). They are also a strongpredictor of psychological distress as a result of financial strainand traumatic events (Lincoln, Chatters, & Taylor, 2010). Futureresearch is therefore required to determine whether HRV responsemay provide a useful marker in the context of repeated and ongo-ing negative social interactions to predict longer-term health andphysiological dysregulation. Interestingly, HRV did not change dur-ing positive social interactions, relative to baseline. However, theresponse of HRV to positive social tasks subsequent to a negativeor stressful social task may have additional importance as a markerof flexibility and effective social interaction skill.
As expected, the TSST caused significant decreases in HRV rel-ative to baseline, which may reflect a decrease in vagal influenceunder stress. Porges’ Polyvagal theory suggests that reductions invagal tone are associated with sympathetic activation in order tosupport the fight-flight response (Porges, 2003). The complex rela-tionship between sympathetic activation and HPA activation hasbeen discussed elsewhere (Dienstber, 1989). Results could alsobe interpreted in terms of the Neurovisceral Integration modelsuggesting that the environmental demands of both negativesocial interactions and stressful tasks lead to a reduction in auto-nomic nervous system regulation and neurovisceral integrationbetween the central autonomic network and anterior executiveregion.
One of the main findings was that HRV changes during socialinteraction may provide a useful index for psychopathology. Inour meta-analysis, studies included participants with high traitsocial anxiety at risk of diagnosis (Mauss et al., 2003) and autism

cal Ps
(acOp
saHiHww
wtnitaio(stipsbata
A
tNGM
R
A
A
A
B
B
B
B
B
B
B
C
S. Shahrestani et al. / Biologi
Smeekens et al., 2013). Future studies in other diagnostic groupsre now required. One study has, for example, shown that in thease of mania RSA could be elevated rather than depressed (Gruber,veis, Keltner, & Johnson, 2008) and HRV responses of manicatients during a social interaction task remain unclear.
Findings from this meta-analysis reveal that women and menhow similar HRV responses during social interactions, as moder-ted by valence. That is, both men and women showed decreases inRV during negative social interactions and no change during pos-
tive or neutral ones. Other studies have, however, suggested thatRV responses differ by type of index (HF and rMSSD) in men andomen (Antelmi et al., 2004). Moderating by both index and genderas not possible due to the limited number of eligible studies.
We classified participants into groups based on whether theyere teenagers, young adults or older adults. Past research shows
hat while there is a general decrease in HRV as individuals age, sig-ificant differences from the twenties to the thirties are apparent
n common indexes of HRV such as SDNN (Yukishita et al., 2010). Inhis meta-analysis we found that this decrease could be observeds reduced autonomic responsivity to negative social interactionsn older participants. This may reflect improvements in the choicef coping strategies arising from experience in social interactionCharles & Carstensen, 2004). Results also reveal that RSA and HFuccessfully indexed HRV change during negative social interac-ions. Both these indexes appear to be sensitive and applicable tondexing HRV in negative social settings. Future studies could com-are the sensitivity of different indexes of HRV in multiple socialettings. In conclusion, the results of this study show that HRV maye a useful biomarker differentiating between positive and neg-tive social interactions in adolescents and adults. Furthermore,he data suggest that negative social interactions may have similarutonomic effects as established social stressors.
cknowledgments
We would like to acknowledge Gail Alvares for her kind assis-ance in the preparation of this manuscript and the support ofHMRC grant APP1043664 and a career development fellowship touastella APP1061922). Quintana is now at the Institute of Clinicaledicine, University of Oslo, Oslo, Norway.
eferences
lvares, G. A., Quintana, D. S., Kemp, A. H., Van Zwieten, A., Balleine, B. W., Hickie, I.B., et al. (2013). Reduced heart rate variability in social anxiety disorder: Asso-ciations with gender and symptom severity. PLOS ONE, 8(7), e70468.
ntelmi, I., De Paula, R. S., Shinzato, A. R., Peres, C. A., Mansur, A. J., & Grupi, C. J.(2004). Influence of age, gender, body mass index, and functional capacity onheart rate variability in a cohort of subjects without heart disease. AmericanJournal of Cardiology, 93(3), 381–385.
ppelhans, B. M., & Luecken, L. J. (2006). Heart rate variability as an index of regulatedemotional responding. Review of General Psychology, 10(3), 229–240.
är, K. J., Boettger, M. K., Koschke, M., Schulz, S., Chokka, P., Yeragani, V. K.,et al. (2007). Non-linear complexity measures of heart rate variability in acuteschizophrenia. Clinical Neurophysiology, 118(9), 2009–2015.
erntson, G. G., Bigger, J. T., Eckber, D. L., Grossman, P., Kaufmann, P. G., Malik, M.,et al. (1997). Heart rate variability: Origins, methods and interpretative caveats.Psychophysiology, 34(6), 623–648.
illman, G. E. (2011). Heart rate variability – A historical perspective. Frontiers inPhysiology, 2(1), 2–86.
lackhart, G. C., Eckel, L. A., & Tice, D. M. (2007). Salivary cortisol in response to acutesocial rejection and acceptance by peers. Biological Psychology, 75(3), 267–276.
olger, N., Delongis, A., Kessler, R. C., & Schilling, E. A. (1989). Effects of daily stresson negative mood. Journal of Personality and Social Psychology, 57(5), 808–818.
orenstein, M., Hedges, L., Higgins, J., & Rothstein, H. (2005). Comprehensive meta-analysis (version 2) (software). Englewood, NJ: Biostat.
utler, E. A., Wilhelm, F. H., & Gross, J. J. (2006). Respiratory sinus arrhythmia, emo-tion, and emotion regulation during social interaction. Psychophysiology, 43(6),612–622.
acioppo, J. T., & Hawkley, L. C. (2003). Social isolation and health, with an emphasison underlying mechanisms. Perspectives in Biology and Medicine, 46(3), S39–S52.
ychology 105 (2015) 43–50 49
Chalmers, J., Quintana, D. S., Abbott, M. J., & Kemp, A. H. (2014). Anxiety disordersare associated with reduced heart rate variability: A meta-analysis. Frontiers inPsychiatry, 5(80), eCollection 2014.
Charles, S. T., & Carstensen, L. L. (2004). A life span view of emotional functioning inadulthood and old age. Advances in Cell Aging and Gerontology, 15(1), 133–162.
Codispoti, M., Mazzetti, M., Baldaro, B., Tuozzi, G., & Trombini, G. (2001). Effect ofpublic speaking on gastric myoelectrical reactivity and parasympathetic cardiaccontrol. Stress and Health, 17(5), 291–296.
Cohen, J. D. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ:Lawrence Earlbaum Associates.
D’Antono, B., Moskowitz, D. S., Miners, C., & Archambault, J. (2005). Gender and com-munal trait differences in the relations among social behaviour, affect arousal,and cardiac autonomic control. Journal of Behavioral Medicine, 28(3), 267–279.
Dienstber, R. A. (1989). Arousal and physiological toughness: Implications for mentaland physical health. Psychological Review, 96(1), 84–100.
Egger, M., Davey Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysisdetected by a simple, graphical test. British Medical Journal (Clinical ResearchEdition), 315(7109), 629–634.
Fagundes, C. P., Diamond, L. M., & Allen, K. P. (2012). Adolescent attachment insecu-rity and parasympathetic functioning predict future loss adjustment. Personality& Social Psychology Bulletin, 38(6), 821–832.
Fagundes, C. P., Murray, D. M., Hwang, B. S., Gouin, J. P., Thayer, J. F., Sollers, J. J., et al.(2011). Sympathetic and parasympathetic activity in cancer-related fatigue:More evidence for a physiological substrate in cancer survivors. Psychoneuroen-docrinology, 36(8), 1137–1147.
Friedman, B. H., & Thayer, J. F. (1998). Anxiety and autonomic flexibility: A cardio-vascular approach. Biological Psychology, 49(3), 303–323.
Grossman, P., & Taylor, E. W. (2007). Toward understanding respiratory sinusarrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral func-tions. Biological Psychology, 74(2), 263–285.
Grossman, P., Van Beek, J., & Wientjes, C. (1990). A comparison of three quantificationmethods for estimation of respiratory sinus arrhythmia. Psychophysiology, 27(6),702–714.
Griffin, D., & Gonzalez, R. (2003). Models of dyadic social interaction. PhilosophicalTransactions of the Royal Society of London, Series B, 358(1431), 573–581.
Gruber, J., Oveis, C., Keltner, D., & Johnson, S. J. (2008). Risk for mania and positiveemotional responding: Too much of a good thing? Emotion, 8(1), 23–33.
Hari, R., & Kujala, M. (2009). Brain basis of human social interaction: From conceptsto brain imaging. Physiological Reviews, 89(1), 453–479.
Hastings, P. D., Nuselovici, J. N., Utendale, W. T., Coutya, J., McShane, K. E., &Sullivan, C. (2008). Applying the polyvagal theory to children’s emotional regu-lation: Social context, socialization and adjustment. Biological Psychology, 79(3),299–306.
Heffner, K. L., Loving, T. J., Kiecolt-Glaser, J. K., Himawan, L. K., Glaser, R., & Malarkey,W. B. (2006). Older spouses’ cortisol responses to marital conflict: Associationswith demand/withdraw communication patterns. Journal of Behavioral Medicine,29(4), 317–325.
Heinrichs, M., & Gaab, J. (2007). Neuroendocrine mechanisms of stress and socialinteraction: Implications for mental disorders. Current Opinion in Psychiatry,20(2), 158–162.
Henje Blom, E., Olsson, E. M., Serlachius, E., Ericson, M., & Ingvar, M. (2010). Heartrate variability (HRV) in adolescent females with anxiety disorders and majordepressive disorder. Acta Paediatrica, 99(4), 604–611.
Het, S., Rohleder, N., Schoofs, D., Kirschbaum, C., & Wolf, O. T. (2009). Neuroendocrineand psychometric evaluation of a placebo version of the ‘Trier Social Stress Test.’.Psychoneuroendocrinology, 34(7), 1075–1086.
Holt-Lunstad, J., Birmingham, W. A., & Light, K. C. (2008). Influence of a “warmtouch” support enhancement intervention among married couples on ambu-latory blood pressure, oxytocin, alpha amylase, and cortisol. PsychosomaticMedicine, 70(9), 976–985.
House, J. S. (2001). Social isolation kills, but how and why? Psychosomatic Medicine,63(2), 273–274.
Ishii-Kuntz, M. (1990). Social interaction and psychological well-being: Compari-son across stages of adulthood. The International Journal of Aging and HumanDevelopment, 30(1), 15–36.
Kemp, A. H., Quintana, D. S., Gray, M. A., Felmingham, K. L., Brown, K., & Gatt, J. M.(2010). Impact of depression and antidepressant treatment on heart rate vari-ability: A review and meta-analysis. Biological Psychiatry, 67(11), 1067–1074.
Kemper, K. J., & Shaltout, H. A. (2011). Non-verbal communication of compas-sion: Measuring psychophysiologic effects. BMC Complementary and AlternativeMedicine, 11(1), 132–140.
Kirschbaum, C., Pirke, K., & Hellhammer, D. H. (1993). The “Trier Social Stress Test” –A tool for investigating psychobiological stress responses in a laboratory setting.Neuropsychobiology, 28(1–2), 76–81.
Klin, A., Volkmar, F. R., & Sparrow, S. S. (1992). Autistic social dysfunction: Somelimitations of the theory of mind hypothesis. Journal of Child Psychology andPsychiatry, 33(5), 861–876.
Kok, B. E., & Fredrickson, B. L. (2010). Upward spirals of the heart: Autonomic flexi-bility, as indexed by vagal tone, reciprocally and prospectively predicts positiveemotions and social connectedness. Biological Psychology, 83(3), 432–436.
Lincoln, K. D., Chatters, L. M., & Taylor, R. J. (2010). Psychologial distress among black
and white americans: Differential effects of social support, negative interactionand personal control. Journal of Health and Social Behavior, 44(3), 390–407.Lipsitz, L. A., Mietus, J., Moody, G. B., & Goldberger, A. L. (1990). Spectral character-istics of heart rate variability before and during postural tilt. Relations to agingand risk of syncope. Circulation, 81(6), 1803–1810.

5 ical Ps
M
M
M
M
N
O
O
P
P
P
Q
Q
S
S
0 S. Shahrestani et al. / Biolog
auss, I. B., Wilhelm, F. H., & Gross, J. J. (2003). Autonomic recovery and habituationin social anxiety. Psychophysiology, 40(4), 648–653.
oher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group. (2009). Pre-ferred reporting items for systematic reviews and meta-anayses: The PRISMAstatement. PLoS Medicine, 6(7), 1–6.
ulder, L. J. M., Dijksterhuis, C., Stuiver, A., & de Waard, D. (2009). Cardiovascularstate changes during performance of a simulated ambulance dispatchers’ task:Potential use for adaptive support. Applied Ergonomics, 40(6), 965–977.
urray-Close, D. (2011). Autonomic reactivity and romantic relational aggressionamong female emerging adults: Moderating roles of social and cognitive risk.International Journal of Psychophysiology, 80(1), 28–35.
ezlek, J. B., Richardson, D. S., Green, L. R., & Schatten-Jones, E. C. (2002). Psycholog-ical well-being and day-to-day social interaction among older adults. PersonalRelationships, 9(1), 57–71.
kabayashi, H., Liang, J., Krause, N., Akiyama, H., & Sugisawa, H. (2004). Mentalhealth among older adults in Japan: Do sources of social support and negativeinteraction make a difference? Social Science & Medicine, 59(11), 2259–2270.
no, E., Nozawa, T., Ogata, T., Motohashi, M., Higo, N., Kobayashi, T., et al. (2011).Relationship between social interaction and mental health. In 2011 IEEE/SICEInternational Symposium on System Integration (SII) (pp. 246–249).
age-Gould, E., Mendes, W. B., & Major, B. (2010). Intergroup contact facilitatesphysiological recovery following stressful intergroup interactions. Journal ofExperimental Social Psychology, 46(5), 854–858.
orges, S. W. (2003). The polyvagal theory: Phylogenetic contributions to socialbehavior. Physiology & Behavior, 79(3), 503–513.
orges, S. W. (2007). The polyvagal perspective. Biological Psychology, 74(2),116–143.
uintana, D. S., & Heathers, J. (2014). Considerations in the assessment of heart ratevariability in biobehavioral research. Frontiers in Psychology, 5(805), 1–10.
uintana, D. S., McGregor, I. S., Guastella, A. J., Malhi, G. S., & Kemp, A. H. (2013). Ameta-analysis on the impact of alcohol dependence on short-term resting-stateheart rate variability: Implications for cardiovascular risk. Alcoholism: Clinicaland Experimental Research, 37(S1), E23–E29.
axbe, D. E., Repetti, R. L., & Nishina, A. (2008). Marital satisfaction, recovery fromwork, and diurnal cortisol among men and women. Health Psychology, 27(1),
15–25.hahrestani, S., Stewart, E. M., Quintana, D. S., HIckie, I. B., & Guastella, A. J. (2014).Heart rate variability during social interactions in children with and withoutpsychopathology: a meta-analysis. Journal of Child Psychology and Psychiatry,55(9), 981–989.
ychology 105 (2015) 43–50
Smeekens, I., Didden, R., & Verhoeven, E. W. M. (2013). Exploring the relationship ofautonomic and endocrine activity with social functioning in adults with autismspectrum disorders. Journal of Autism and Developmental Disorders, 1–11.
Smith, T. W., Uchino, B. N., Berg, C. A., Florsheim, P., Pearce, G., Hawkins, M., et al.(2009). Conflict and collaboration in middle-aged and older couples: II. Car-diovascular reactivity during marital interaction. Psychology and Aging, 24(2),274–286.
Song, H., & Lehrer, P. M. (2003). The effects of specific respiratory rates on heart rateand heart rate variability. Applied Psychophysiology Biofeedback, 28(1), 13–23.
Sztajzel, J. (2004). Heart rate variability: A noninvasive electrocardiographic methodto measure the autonomic nervous system. Swiss Medical Weekly, 134(35–36),514–522.
Thayer, J. F., Hansen, A. L., Saus-Rose, E., & Johnsen, B. H. (2009). Heart rate variabil-ity, prefrontal neural function, and cognitive performance: The neurovisceralintegration perspective on self-regulation, adaptation, and health. Annals ofBehavioral Medicine, 37(2), 141–153.
Thayer, J. F., & Lane, R. D. (2000). A model of neurovisceral integration in emotionalregulation and dysregulation. Journal of Affective Disorders, 61(3), 201–216.
Thayer, J. F., & Lane, R. D. (2009). Claude Bernard and the heart–brain connection:Further elaboration of a model of neurovisceral integration. Neuroscience andBiobehavioral Reviews, 33(1), 81–88.
Tininenko, J. R., Measelle, J. R., Ablow, J. C., & High, R. (2012). Respiratory controlwhen measuring respiratory sinus arrhythmia during a talking task. BiologicalPsychology, 89(3), 562–569.
Waugh, C. E., Panage, S., Mendes, W. B., & Gotlib, I. H. (2010). Cardiovascularand affective recovery from anticipatory threat. Biological Psychology, 84(2),169–175.
Whited, M. C., Wheat, A. L., & Larkin, K. T. (2010). The influence of forgiveness andapology on cardiovascular reactivity and recovery in response to mental stress.Journal of Behavioral Medicine, 33(4), 293–304.
Willemen, A. M., Goossens, F. A., Koot, H. M., & Schuengel, C. (2008). Physiologicalreactivity to stress and parental support: Comparison of clinical and non-clinicaladolescents. Clinical Psychology & Psychotherapy, 351(1), 340–351.
Willemen, A. M., Schuengel, C., & Koot, H. M. (2009). Physiological regulation of stressin referred adolescents: The role of the parent–adolescent relationship. Journal
of Child Psychology and Psychiatry, 50(4), 482–490.Yukishita, T., Lee, K., Kim, S., Yumoto, Y., Kobayashi, A., Shirasawa, T., et al. (2010).Age and sex-dependent alterations in heart rate variability: Profiling the char-acteristics of men and women in their 30s. Journal of Anti-Aging Medicine, 7(8),94–99.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具