Embed Size (px)
Citation preview

Heart FailureHeart Failure
Current ConceptsCurrent Concepts
Howard M. Weinberg, D.O. Howard M. Weinberg, D.O. F.A.C.CF.A.C.C..
Cardiac ArchitectureCardiac Architecture
UltrastructureUltrastructure
11. 75% total volume of the heart is made up of . 75% total volume of the heart is made up of cardiomyocytecardiomyocyte
2. Contractile proteins lie within the cardiomyocyte2. Contractile proteins lie within the cardiomyocyteA. Ventricular and atrial myocytesA. Ventricular and atrial myocytesB. Myofibrils form myocytes(contractile B. Myofibrils form myocytes(contractile
elements)elements)C. Myofibers are groups of C. Myofibers are groups of
myocytes.myocytes.



Contractile ProteinsContractile Proteins
1.1. Actin and MyosinActin and Myosin
2.2. Calcium interacts with Troponin CCalcium interacts with Troponin Crelieves the inhibition caused by relieves the inhibition caused by Troponin ITroponin I


Cardiac CycleCardiac Cycle
Three Phases:Three Phases:1) LV Contraction1) LV Contraction
2) LV Relaxation2) LV Relaxation
3) LV Filling3) LV Filling
The Cardiac CycleThe Cardiac CycleLV CONTRACTIONLV CONTRACTION
Isovolumic contraction(b)Isovolumic contraction(b) Maximal Ejection ©Maximal Ejection ©
LV RelaxationLV Relaxation
Start of relaxation andStart of relaxation and reduced ejection (d)reduced ejection (d) Isovolumic relaxation(e)Isovolumic relaxation(e) LV Filling: rapid phase (f) LV Filling: rapid phase (f) Slow LV Filling (g)Slow LV Filling (g) Atrial systole( a)Atrial systole( a)See Wiggers DiagramSee Wiggers Diagram


Frank-Starling Relationship
A.A. Preload: Load before contraction(venous Preload: Load before contraction(venous return) return)
B.B. Afterload: Load which the LV contracts Afterload: Load which the LV contracts against against

Starling CurveStarling Curve

HF DefinedHF Defined
““Heart failure is a complex clinical syndrome that Heart failure is a complex clinical syndrome that
can result from any structural can result from any structural
or functional cardiac disorder that impairs or functional cardiac disorder that impairs
the ability of the ventricle to fill with the ability of the ventricle to fill with
or eject blood with an increase in intracardiac or eject blood with an increase in intracardiac
chamber pressure”chamber pressure”
Hunt SA et al. Circulation. 2001;104:2996

Clinical Aspects of Heart FailureClinical Aspects of Heart Failure
Backward Heart FailureBackward Heart FailureLVEDP and LVEDV increaseLVEDP and LVEDV increaseLAP and LAV increase(atria contracts for LAP and LAV increase(atria contracts for
C.O.) C.O.) Venous and PCWP increaseVenous and PCWP increaseTransudation of fluid from capillary bed Transudation of fluid from capillary bed

Clinical Aspects of Heart FailureClinical Aspects of Heart Failure
Forward Heart FailureForward Heart FailureDecrease C.O.= decrease perfusion to vital Decrease C.O.= decrease perfusion to vital
organsorgans Increase Na and Water retentionIncrease Na and Water retention

Symptoms of Heart FailureSymptoms of Heart Failure
Exertional DyspneaExertional Dyspnea Orthopnea-Sx in the recumbent positionOrthopnea-Sx in the recumbent position Paroxysmal Nocturnal DyspneaParoxysmal Nocturnal Dyspnea
Theory: 1. Slow resorption of interstial Theory: 1. Slow resorption of interstial fluid fluid
2. Reduced adrenergic support 2. Reduced adrenergic support at nightat night
3. Normal nocturnal 3. Normal nocturnal depression of the respiratorydepression of the respiratory
center center

FraminghamFramingham Criteria for CHF Criteria for CHF

Cardiac vs Pulmonary DyspneaCardiac vs Pulmonary Dyspnea
Frequent coughingFrequent coughingCough productionCough productionFeverFeverDiaphoresisDiaphoresisResponse to TxResponse to Tx

Diastolic Heart FailureDiastolic Heart Failure
1.1. 1/3 of pts. have primary diastolic HF 1/3 of pts. have primary diastolic HF (normal or near normal LV function)(normal or near normal LV function)
2.2. 1/3 combined systolic and diastolic HF1/3 combined systolic and diastolic HF
3.3. Altered ventricular relaxation(inactivation Altered ventricular relaxation(inactivation of contraction)of contraction)
4.4. Alteration of ventricular fillingAlteration of ventricular filling
5.5. Some causes: myocardial ischemia, Some causes: myocardial ischemia, restrictive cardiomyopathy,pericardial restrictive cardiomyopathy,pericardial diseasedisease

Diastolic Heart FailureDiastolic Heart Failure
Impaired ability to accept blood and relax Impaired ability to accept blood and relax during diastoleduring diastole
Both types increase with age, African Both types increase with age, African AmericansAmericans
40-70% incidence more often female, 40-70% incidence more often female, obese, older HTN and less likely to have obese, older HTN and less likely to have CADCAD
Less symptomatic and lower morbidity and Less symptomatic and lower morbidity and mortalitymortality

High Output FailureHigh Output Failure
Usually occurs with some underlying heart Usually occurs with some underlying heart diseasedisease
Clinical conditions: Clinical conditions: AnemiaAnemia Systemic Ateriovenous Fistula-dialysis/traumaSystemic Ateriovenous Fistula-dialysis/trauma HyperthyroidismHyperthyroidism BeriberiBeriberi PagetsPagets Multiple myeloma/Pregnancy/Carcinoid/ renal diseaseMultiple myeloma/Pregnancy/Carcinoid/ renal disease Obesity/polycythemia veraObesity/polycythemia vera



Yancy CW, Strong M. Prim Care Spec Ed. 2002;6:15
High Risk: Hypertension, coronary artery disease, diabetes, family history of cardiomyopathy
Asymptomatic LVD: Previous MI, LV systolic dysfunction, asymptomatic valvular disease
Symptomatic HF: Known structuralheart disease, shortness of breath and
fatigue, reduced exercise tolerance
RefractoryEnd-Stage HF:
Marked symptomsat rest despite maximal
medical therapy
AA
BB
CC
DD
Disease Progression of HF: Disease Progression of HF: ACC/AHA HF StagesACC/AHA HF Stages

EpidemiologyEpidemiology
Only major Only major cardiovascular cardiovascular disorder increasing in disorder increasing in incidence and incidence and prevalenceprevalence
Leading cause of Leading cause of hospitalization in >65hospitalization in >65
1/3 hospitalized 1/3 hospitalized patients readmitted in patients readmitted in 90 days90 days
5% of all hospital 5% of all hospital admissionsadmissions


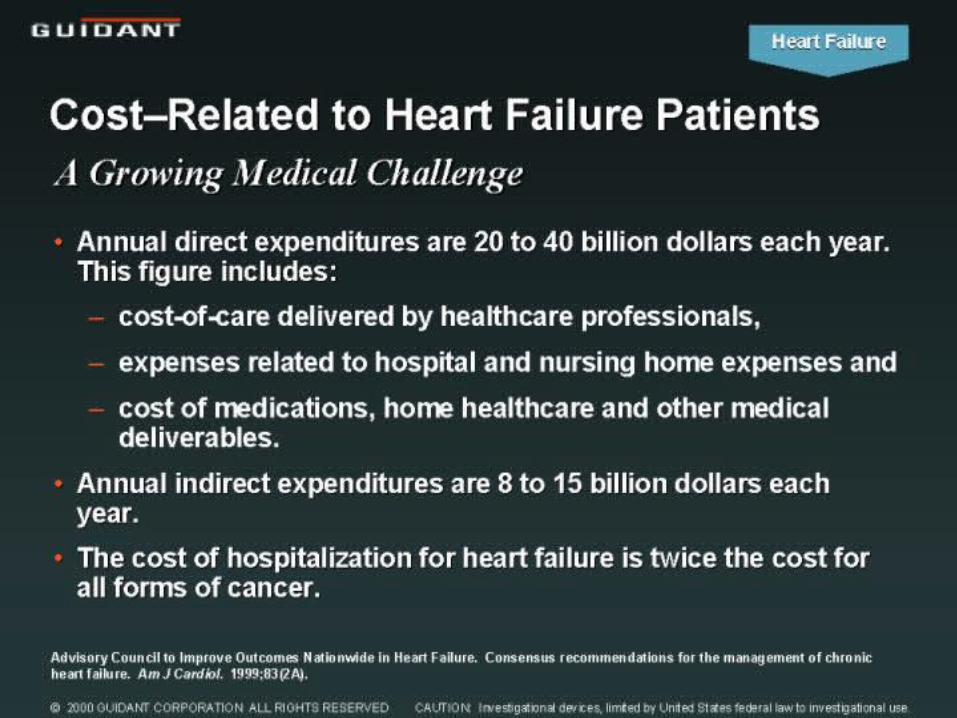
Heart Failure is a Major and Growing Public Health Problem in the U.S.
Approximately 5 million patients in this country have HF
Over 550,000 patients are diagnosed with HF for the first time each year
Primary reason for 12 to 15 million office visits and 6.5 million hospital days each year
In 2001, nearly 53,000 patients died of HF as a primary cause

Mortality/MorbidityMortality/Morbidity
Despite therapeutic Despite therapeutic advances, the 1 year advances, the 1 year mortality for NYHA mortality for NYHA class IV approaches class IV approaches 40%40%
Impaired Quality of Impaired Quality of life.life.
Psychological distressPsychological distress Reduced social Reduced social
functioningfunctioning 49% admitted after 49% admitted after
an emotional eventan emotional event



Prevalence of HF Increases Prevalence of HF Increases With AgeWith Age
US, 1988–1994AHA. Heart Disease and Stroke Statistics—2004 Update
0
2
4
6
8
10
20–24 25–34 35–44 45–54 55–64 65–74 75+
Age (yr)
Pop
ulat
ion
(%)
Males
Females


Number of Patients Number of Patients With HF IncreasingWith HF Increasing
1979–20011979–2001 Hospital discharges from HF rose 164% from Hospital discharges from HF rose 164% from
377,000 to 995,000377,000 to 995,000 Deaths increased 155%Deaths increased 155%
As US population ages, number of patients As US population ages, number of patients with HF expected to double in 30 yrwith HF expected to double in 30 yr
AHA. Heart Disease and Stroke Statistics—2004 UpdateMassie BM et al. Am Heart J. 1997;133:703
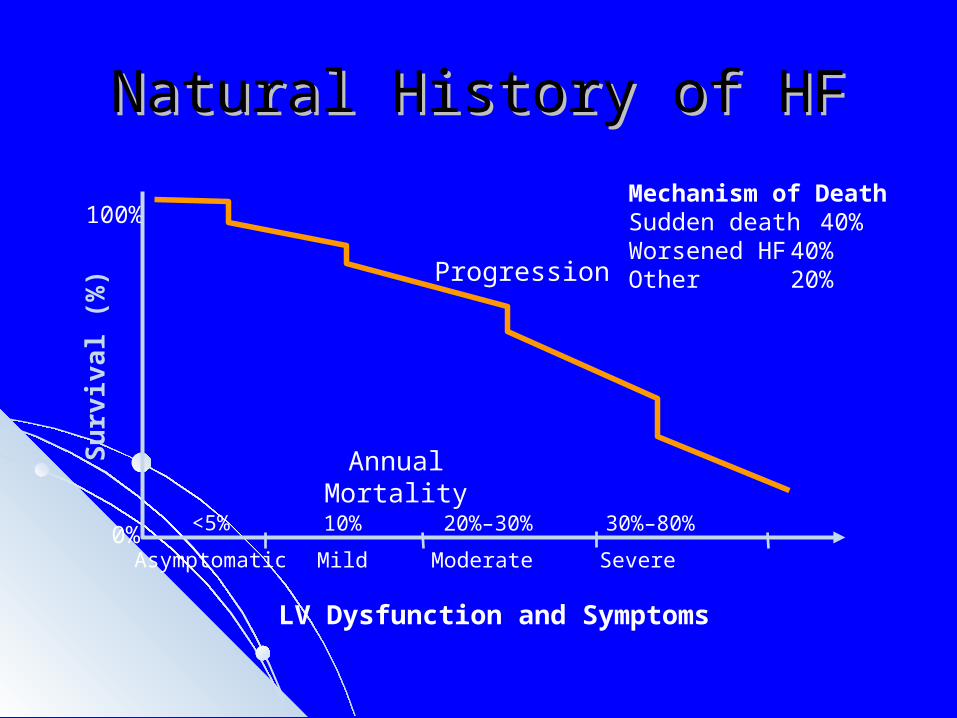
Natural History of HFNatural History of HFS
urv
iva
l (%
)
LV Dysfunction and Symptoms
Mechanism of DeathSudden death 40%Worsened HF 40%Other 20%Progression
Annual Mortality
0%
100%
Asymptomatic Mild Moderate Severe
<5% 10% 20%–30% 30%–80%

Treatment of Heart FailureTreatment of Heart Failure
Non-surgicalNon-surgicalSpecialty ClinicsSpecialty ClinicsLifestyle ModificationLifestyle ModificationPharmacologicalPharmacological
SurgicalSurgical

Contributing Factors to ADHFContributing Factors to ADHF
Cardiovascular FactorsCardiovascular Factors Superimposed ischemia or infarctionSuperimposed ischemia or infarction Uncontrolled hypertensionUncontrolled hypertension Unrecognized primary valvular diseaseUnrecognized primary valvular disease Worsening secondary mitral regurgitationWorsening secondary mitral regurgitation New onset or uncontrolled atrial fibrillationNew onset or uncontrolled atrial fibrillation Excessive tachycardia or bradycardiaExcessive tachycardia or bradycardia Pulmonary embolismPulmonary embolism
Stevenson LW et al. Am Heart J. 1998;135:293

Contributing Factors to ADHF Contributing Factors to ADHF cont'dcont'd
Systemic FactorsSystemic Factors Inappropriate medicationsInappropriate medications Superimposed infectionSuperimposed infection AnemiaAnemia Uncontrolled diabetesUncontrolled diabetes Thyroid dysfunctionThyroid dysfunction Electrolyte abnormalitiesElectrolyte abnormalities PregnancyPregnancy
Stevenson LW et al. Am Heart J. 1998;135:293
Contributing Factors to ADHF Contributing Factors to ADHF cont'dcont'd
Patient-Related FactorsPatient-Related Factors Medication nonadherenceMedication nonadherence Dietary indiscretionDietary indiscretion Alcohol consumptionAlcohol consumption Substance abuseSubstance abuse
Stevenson LW et al. Am Heart J. 1998;135:293



Proven Outcomes for HF Proven Outcomes for HF TherapiesTherapies
Improve SurvivalImprove Survival ACE inhibitorACE inhibitor ARBARB Beta blockerBeta blocker Aldosterone receptor Aldosterone receptor
antagonistantagonist Hydralazine/long-Hydralazine/long-
acting nitratesacting nitrates
Reduce HospitalizationReduce Hospitalization ACE inhibitorACE inhibitor ARBARB Beta blockerBeta blocker Aldosterone receptor Aldosterone receptor
antagonistantagonist Hydralazine/long-acting Hydralazine/long-acting
nitratesnitrates DigoxinDigoxin

Surgical/Interventional TherapySurgical/Interventional Therapy
Cardiac Resynchronization TherapyCardiac Resynchronization TherapyRevascularizationRevascularizationValue repair/replacementValue repair/replacementCardiomyoplastyCardiomyoplastyVentricular ReductionVentricular ReductionLeft Ventricular Assist DevicesLeft Ventricular Assist DevicesTransplantTransplant
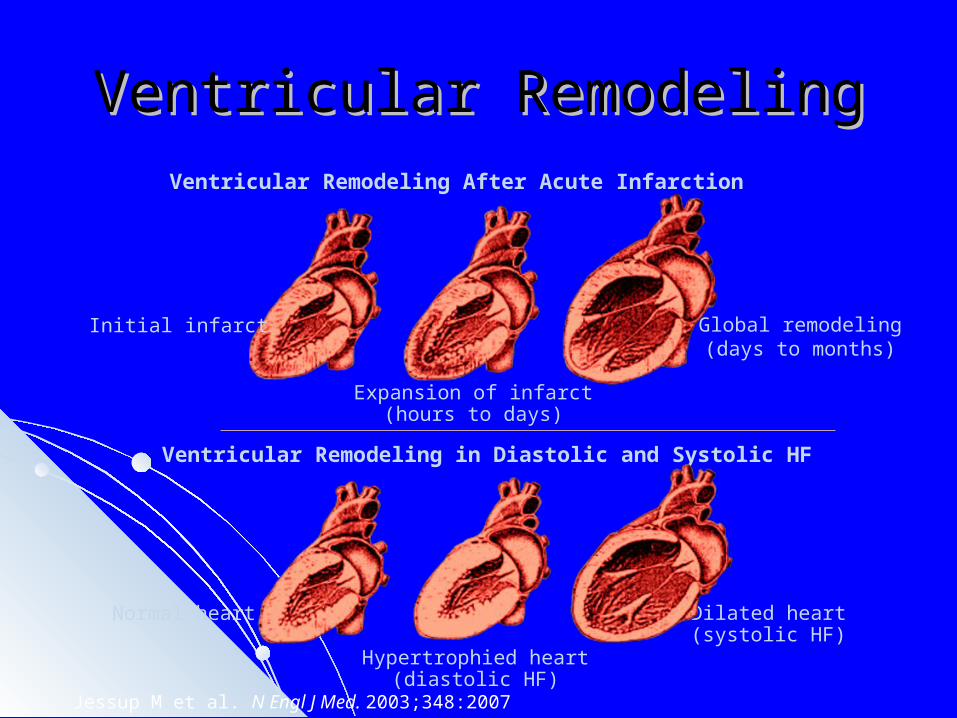
Ventricular RemodelingVentricular RemodelingVentricular Remodeling After Acute Infarction
Ventricular Remodeling in Diastolic and Systolic HF
Initial infarct
Expansion of infarct(hours to days)
Global remodeling(days to months)
Normal heart
Hypertrophied heart(diastolic HF)
Dilated heart(systolic HF)
Jessup M et al. N Engl J Med. 2003;348:2007

Yancy CW, Strong M. Prim Care Spec Ed. 2002;6:15
PLUS inotropes, transplant, ventricular assist device
Treat hypertension and lipids, smoking cessation, exercise, limit alcohol, ACE inhibitors in appropriate populations
PLUS ACE inhibitors, beta blockers in appropriate populations
PLUS ACE inhibitors, beta blockers, diuretics, digoxin, aldosterone receptor antagonists, dietary salt restriction
HF TherapyHF Therapy

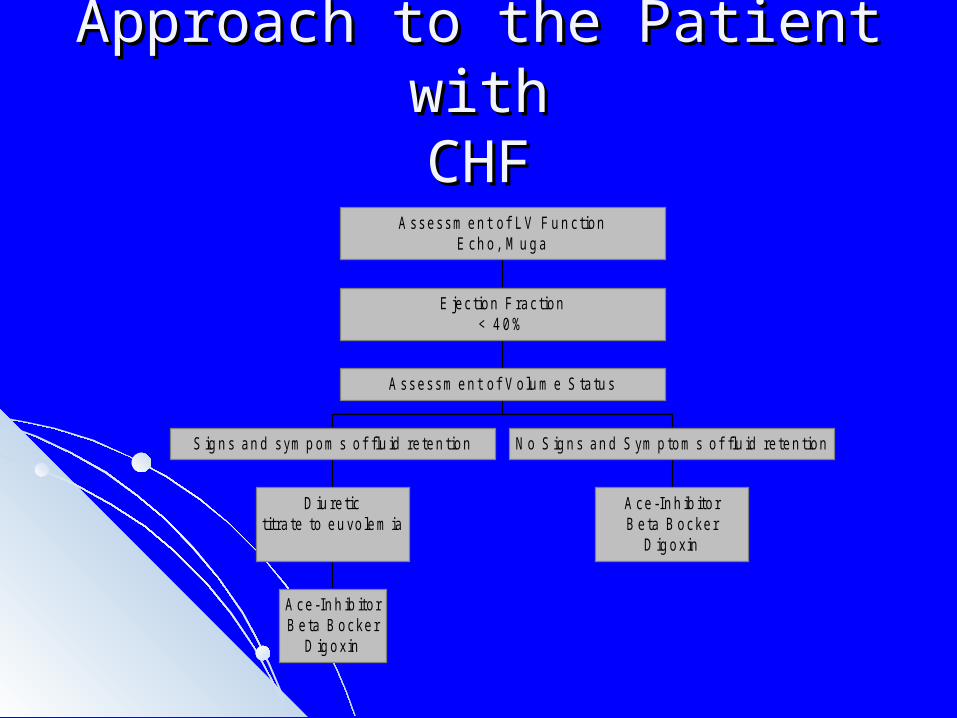
Approach to the Patient withApproach to the Patient withCHFCHF
A ce-In h ib ito rB e ta B ocker
D ig oxin
D iu re tict itra te to eu vo lem ia
S ig n s an d sym p om s o f flu id re ten tion
A ce-In h ib ito rB e ta B ocker
D ig oxin
N o S ig n s an d S ym p tom s o f flu id re ten tion
A ssessm en t o f V o lu m e S ta tu s
E jec tion F rac tion< 4 0 %
A ssessm en t o f L V F u n c tionE ch o , M u g a


Neurohormonal Activation Neurohormonal Activation in Heart Failurein Heart Failure
M orb id ity/M orta lityA rrh yth m ias
P u m p F a ilu re
L V R em od e lin gan d
p rog ress ive L V D ys fu n c tion
F ib ros is , ap op tos is , h yp ertrop h yce llu la r/m o lecu la r a lte ra tion s ,
m yotoxic ity
H eart F a ilu re S ym tom sD ysp n ea
F atig u e ,E d em aC h es t C on g es tion
P erip h era l vasocon s tric tionH em od yn am ic a lte ra tion s
A c tiva tion o f R A S an d S N S
L V D ys fu n c tionIn c rease w a ll s tress
M yocard ia l In ju ry(C A D ,H TN ,C M P )
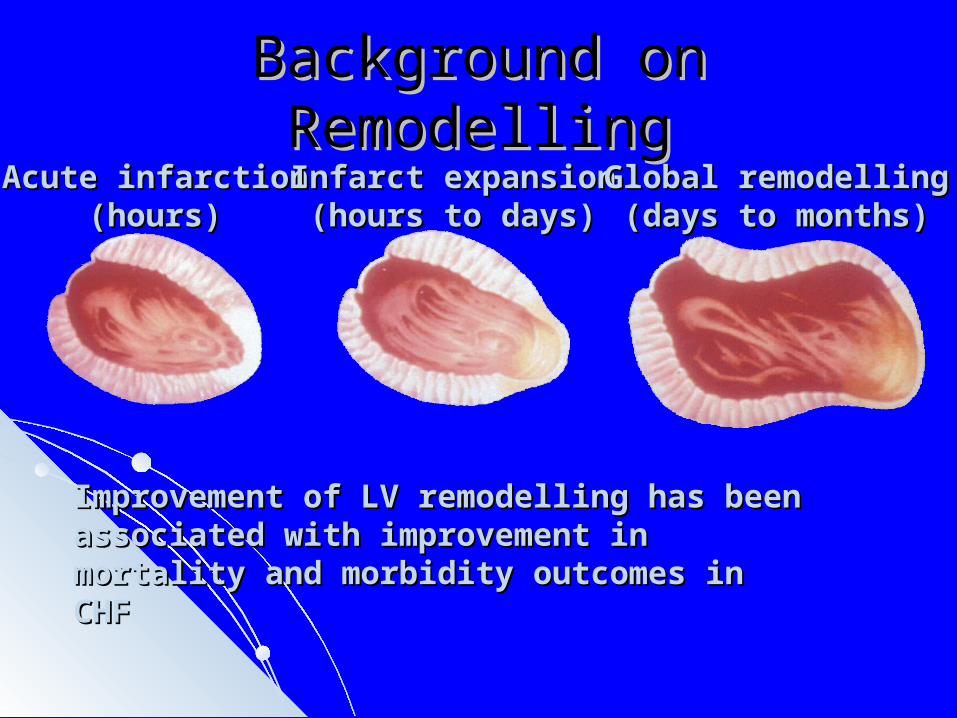
Background on RemodellingBackground on RemodellingAcute infarctionAcute infarction
(hours)(hours)Infarct expansionInfarct expansion(hours to days)(hours to days)
Global remodellingGlobal remodelling(days to months)(days to months)
Improvement of LV remodelling has been Improvement of LV remodelling has been associated with improvement in mortality and associated with improvement in mortality and morbidity outcomes in CHFmorbidity outcomes in CHF




B-Adrenergic Receptor BlockersB-Adrenergic Receptor Blockers
Improve survivalImprove survival Improve ejection fractionImprove ejection fractionRemodelingRemodelingQuality of lifeQuality of lifeReduce SCDReduce SCD Inhibiting adverse effects of the Inhibiting adverse effects of the
sympathetic nervous systemsympathetic nervous systemDiminish RAAS activationDiminish RAAS activation



All-Cause Mortality: MERIT-HFAll-Cause Mortality: MERIT-HF
MERIT-HF Study Group. Lancet. 1999;353:2001
P=0.0082 (adjusted)P=0.00009 (nominal)
PlaceboMetoprolol CR/XL
0
5
10
15
20
0 3 6 9 12 15 18 21
Follow-up (mo)
Cu
mu
lati
ve M
ort
alit
y (
%)

Cumulative Mortality in Patients Cumulative Mortality in Patients With Severe HF: With Severe HF: COPERNICUSCOPERNICUS
Packer M et al. N Engl J Med. 2001;344:1651
PlaceboPlacebo 11331133 937937 703703 580580 446446 286286 183183 114114CarvedilolCarvedilol 11561156 947947 733733 620620 479479 321321 208208 142142
No. of Patients at Risk
Carvedilol(n = 1156)
Placebo(n = 1133)
0
60
80
90
100
0
Months
Su
rviv
al (
% o
f P
ati
ents
)
3 6 9 12 15 18 21
70
P=0.0014 (adjusted)P=0.00013 (unadjusted)

Angiotensin-Converting InhibitorsAngiotensin-Converting Inhibitors
Decrease conversion of angiotensin I-IIDecrease conversion of angiotensin I-II Improve survivalImprove survivalDecrease rate of hospitalizationDecrease rate of hospitalization Improve symptomsImprove symptoms Inhibit neurohormonal activationInhibit neurohormonal activationReverse remodelingReverse remodelingDecrease incidence of SCD?Decrease incidence of SCD?


Cumulative Mortality in Patients Cumulative Mortality in Patients With Symptomatic HF: SOLVD With Symptomatic HF: SOLVD
P=0.0036 for comparison between groups by log-rank testSOLVD Investigators. N Engl J Med. 1991;325:293
Enalapril(n = 1285)
(n = 1284)Placebo
P=0.0036
0
10
20
30
40
50
0 6 12 18 24 30 36 42 48
Months
Mo
rtal
ity
(%)
PlaceboPlacebo 12841284 11591159 10851085 10051005 939939 819819 669669 487487 299299EnalaprilEnalapril 12851285 11951195 11271127 10691069 10101010 891891 697697 526526 333333
No. of Patients at Risk


DIGOXIN
NEUROHORMONAL EFFECTSDIGOXIN
NEUROHORMONAL EFFECTS
Plasma Noradrenaline
Peripheral nervous system activity
RAAS activity
Vagal tone
Normalizes arterial baroreceptors
Plasma Noradrenaline
Peripheral nervous system activity
RAAS activity
Vagal tone
Normalizes arterial baroreceptors

%WORSENING
OF CHF
%WORSENING
OF CHFp = 0.001p = 0.001DIGOXIN: 0.125 - 0.5 mg /d
(0.7 - 2.0 ng/ml)EF < 35%Class I-III (digoxin+diuretic+ACEI)Also significantly decreased exercisetime and LVEF.
DIGOXIN: 0.125 - 0.5 mg /d (0.7 - 2.0 ng/ml)EF < 35%Class I-III (digoxin+diuretic+ACEI)Also significantly decreased exercisetime and LVEF.
DIGOXIN EFFECT ON CHF PROGRESSION
DIGOXIN EFFECT ON CHF PROGRESSION
RADIANCEN Engl J Med 1993;329:1RADIANCEN Engl J Med 1993;329:1
Placebo n=93DIGOXIN Withdrawal
Placebo n=93DIGOXIN Withdrawal
DIGOXIN n=85DIGOXIN n=85
3030
1010
00
2020
1001008080202000 4040 6060DaysDays

All-Cause Mortality: DigoxinAll-Cause Mortality: Digoxin
DIG Investigation Group. N Engl J Med 1997;336:525
P=0.80
Placebo
Digoxin
0
10
20
30
40
50
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Mo
rtal
ity
Fro
m A
ny
Cau
se (
%)
Months
PlaceboPlacebo 34033403 32393239 31053105 29762976 28682868 27582758 26522652 25512551 22052205 18811881 15061506 11681168 734734 339339DigoxinDigoxin 33973397 32693269 31443144 30193019 28822882 27592759 26442644 25312531 21842184 18401840 14751475 11561156 737737 335335
No. of Patients at Risk

ARB in Heart FailureARB in Heart Failure(meta-analysis(meta-analysis))
17 Trials, 12,469pts (JACC Feb 2002)17 Trials, 12,469pts (JACC Feb 2002) No superiority of ARBs in reducing all-cause No superiority of ARBs in reducing all-cause
mortality or hospitalizations for heart failuremortality or hospitalizations for heart failure Poss. benefit with combination ace inhibitionPoss. benefit with combination ace inhibition Beneficial for pts intolerant to ace inhibitionBeneficial for pts intolerant to ace inhibition

ALDOSTERONEALDOSTERONE
Retention Na+
Retention H2O
Excretion K+
Excretion Mg2+
Retention Na+
Retention H2O
Excretion K+
Excretion Mg2+
Collagen
deposition
Fibrosis - myocardium
- vessels
SpironolactoneSpironolactone
Edema Edema
Arrhythmias Arrhythmias
Competitive antagonist of thealdosterone receptor(myocardium, arterial walls, kidney)
Competitive antagonist of thealdosterone receptor(myocardium, arterial walls, kidney)
ALDOSTERONE INHIBITORSALDOSTERONE INHIBITORS

RALES: All-Cause MortalityRALES: All-Cause Mortality1.00
0.95
0.90
0.85
0.80
0.75
0.70
0.65
0.60
0.55
0.50
0.45
0 3 6 9 12 15 18 21 24 27 30 33 36
Risk Reduction 30%95% Cl (18%-40%)P<0.001
Spironolactone+ standard therapy
Standard therapy(ACE inhibitor + loopdiuretic ± digoxin)
Probability of survival
MonthsPitt B, Zannad F, Remme WJ, et al. N Engl J Med, 1999;341:709-717.

00
2020
4040
6060
8080
>4 cm/m>4 cm/m22 <4 cm/m<4 cm/m22 LV IndexLV Index
2-Y
ear
Mo
rtal
ity
(%)
2-Y
ear
Mo
rtal
ity
(%) P = 0.004P = 0.004
Lee TH et al. Am J Cardiol 1993Lee TH et al. Am J Cardiol 1993
Relation Between LV Size Relation Between LV Size and Outcome in CHFand Outcome in CHF
M-mode echocardiography was performed on 382 M-mode echocardiography was performed on 382 patients with class III or IV HF (mean LVEF=20%)patients with class III or IV HF (mean LVEF=20%)
LV End-Diastolic DimensionLV End-Diastolic Dimension
Estimated Body Surface AreaEstimated Body Surface Area==

Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
Cardiac resynchronization therapy (CRT) has Cardiac resynchronization therapy (CRT) has emerged as a promising new treatment for heart emerged as a promising new treatment for heart failure patients with intraventricular conduction failure patients with intraventricular conduction delays or ventricular dysynchronydelays or ventricular dysynchrony
Studies of CRT have demonstrated improvement Studies of CRT have demonstrated improvement in patient symptoms and exercise capacity, in patient symptoms and exercise capacity, quality of life, NYHA class(69% vs. 34% at 6 quality of life, NYHA class(69% vs. 34% at 6 mnths).mnths).

Ventricular DysynchronyVentricular Dysynchrony
Abnormal ventricular conduction resulting Abnormal ventricular conduction resulting in a mechanical delayin a mechanical delayWide QRS (IVCD); typically LBBB Wide QRS (IVCD); typically LBBB
morphologymorphology
Poor systolic functionPoor systolic function
Impaired diastolic functionImpaired diastolic function

Abraham WT, et al. MIRACLE Trial Results; ACC 2001Abraham WT, et al. MIRACLE Trial Results; ACC 2001



ConclusionsConclusions
In NYHA Class III and IV systolic heart In NYHA Class III and IV systolic heart failure patients with intraventricular failure patients with intraventricular conduction delays, CRTconduction delays, CRT is safe and well toleratedis safe and well tolerated improves Quality of Life, functional class, and improves Quality of Life, functional class, and
exercise capacityexercise capacity improves cardiac structure and functionimproves cardiac structure and function improves heart failure composite responseimproves heart failure composite response

Thank You Thank You