Embed Size (px)
Citation preview
Health & Medical Health & Medical InformaticsInformatics
Northern IrelandNorthern Ireland
Paul McCullaghPaul McCullaghEmail:[email protected]:[email protected]
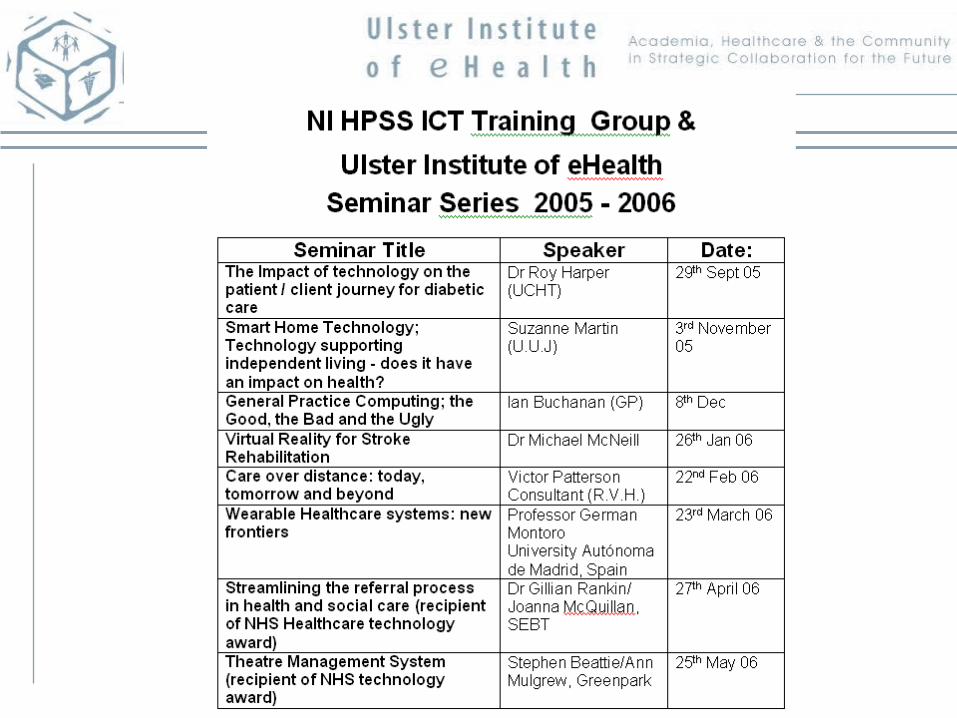
2525thth April 2006, BCS Health Informatics Forum April 2006, BCS Health Informatics Forum
Sectors
• Hospital Trusts– Clinicians, PAM, ICT
• Queen’s University of Belfast– Medicine
• University of Ulster– PAM
NI Regional Context
• Review of Public Administration
• Reconfiguration of Health Structures
• 4 Health Authorities 1 SHA
• 18 Trusts 5 Integrated Trusts
• Implications • Systems/information consolidation• standardisation


HEALTHCARE INFORMATICS RESEARCH GROUP at QUB
• Digital microscopy and machine vision in cancer diagnosis and prognosis
• Signal Processing and Compression in Medical Imaging
• Surgical Informatics • Information and Communications
Technology in Primary Care • Decision Support Systems in
Clinical Decision Making Telemedicine
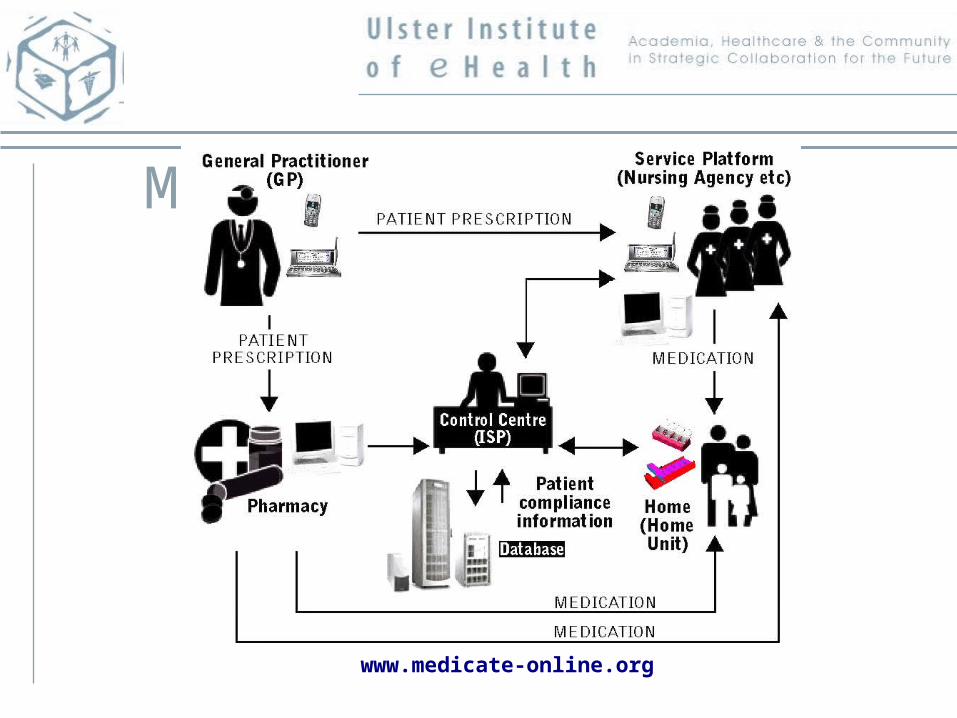
MEDICATE Solution
www.medicate-online.org
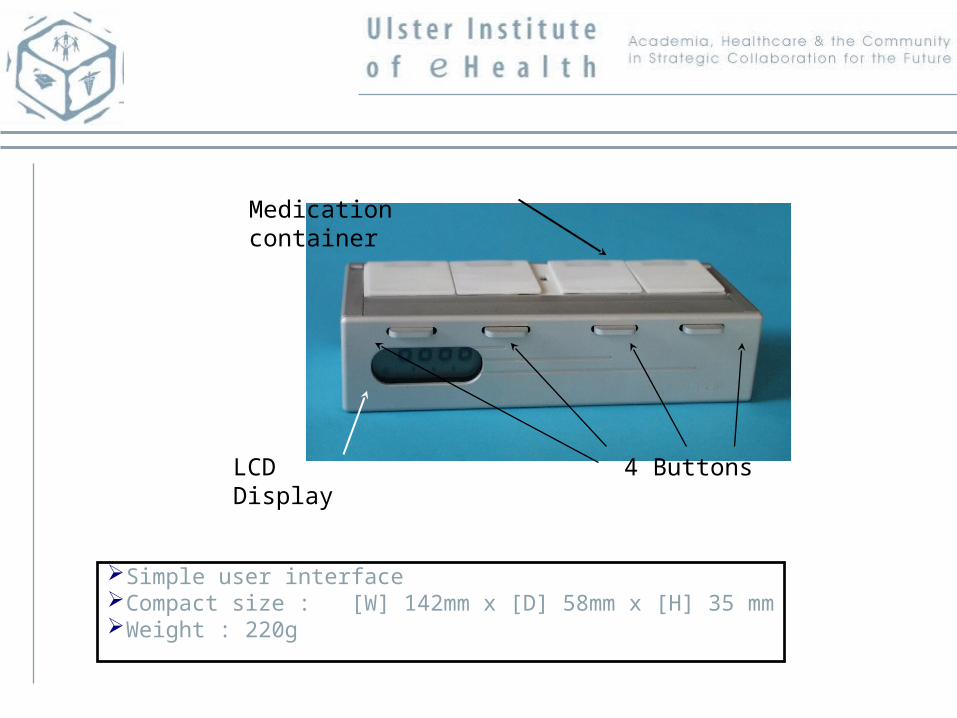
Simple user interface Compact size : [W] 142mm x [D] 58mm x [H] 35 mmWeight : 220g
4 Buttons
Medication container
LCD Display

Prescription Outputs
• Patient Empowerment• Patient Education &
Training• Patient ‘Experts’• Need Education and
Self-Management Training
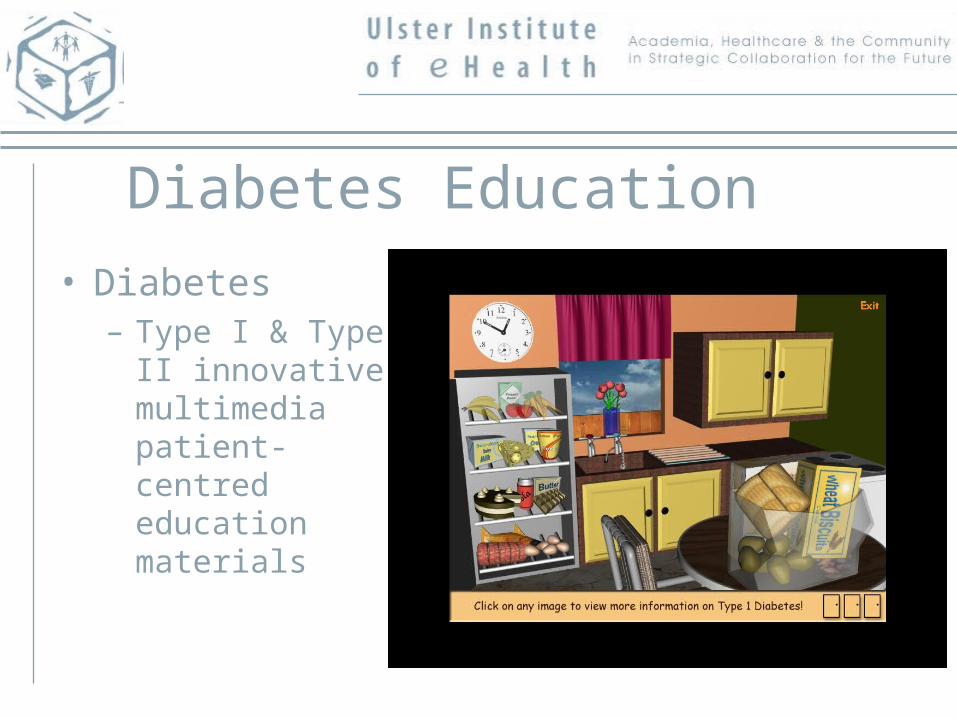
Diabetes Education
• Diabetes– Type I & Type II
innovative multimedia patient-centred education materials
DI@L-log
Gluconnect.com
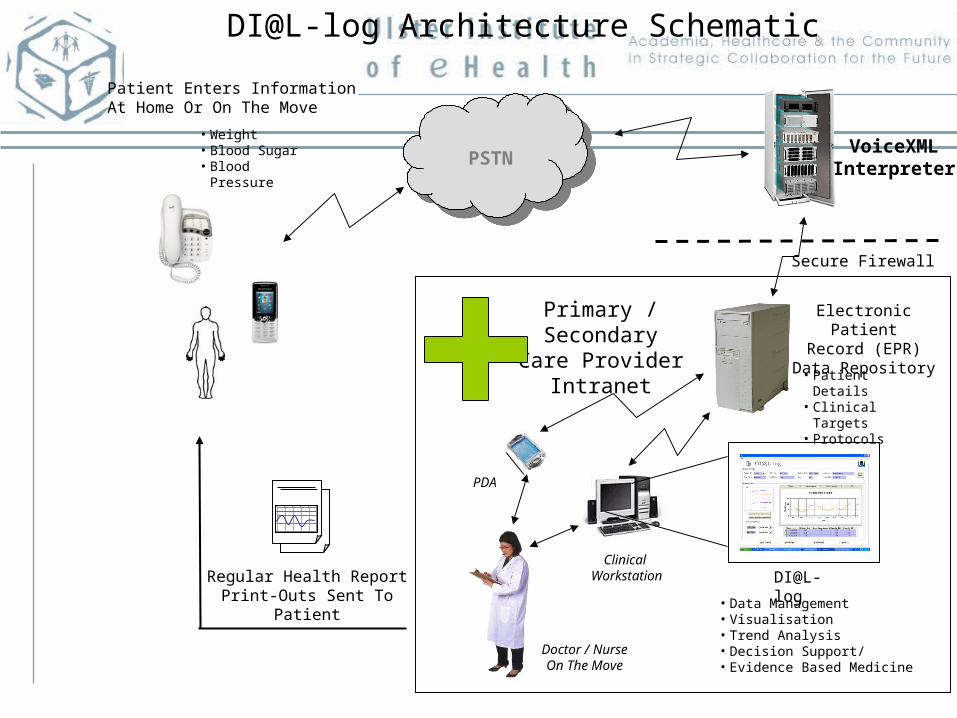
VoiceXMLInterpreter
Primary / SecondaryCare Provider
Intranet
Patient Enters InformationAt Home Or On The Move
Regular Health ReportPrint-Outs Sent To Patient
PSTN
Secure Firewall
Electronic PatientRecord (EPR)
Data Repository
• Data Management• Visualisation• Trend Analysis• Decision Support/• Evidence Based Medicine
PDA
Clinical Workstation
Doctor / NurseOn The Move
• Patient Details• Clinical Targets• Protocols
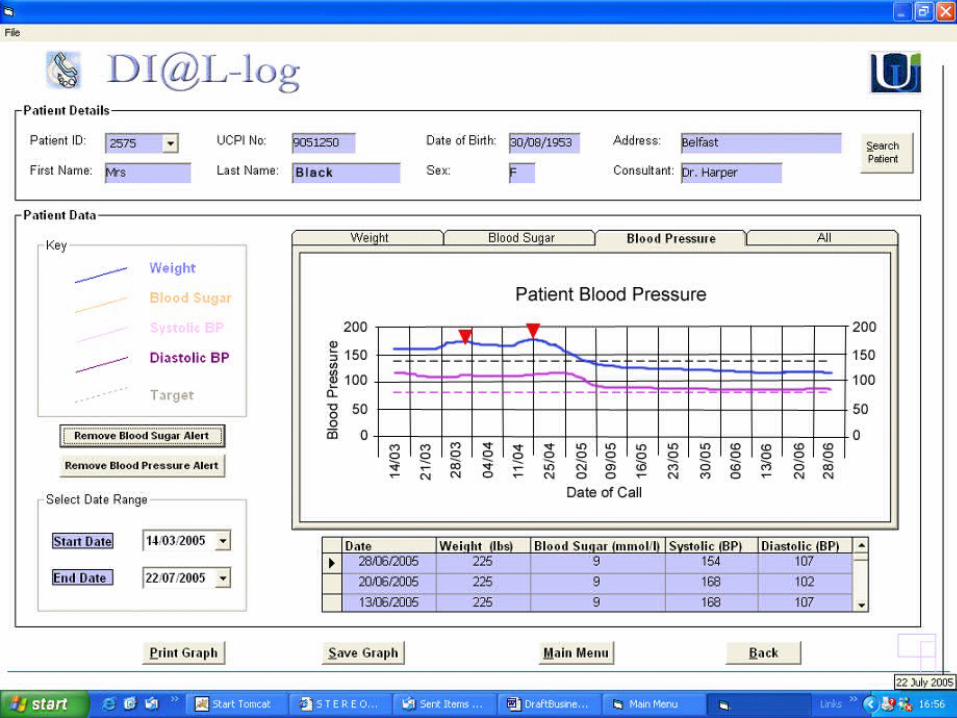
DI@L-log
• Weight • Blood Sugar• Blood Pressure
DI@L-log Architecture Schematic
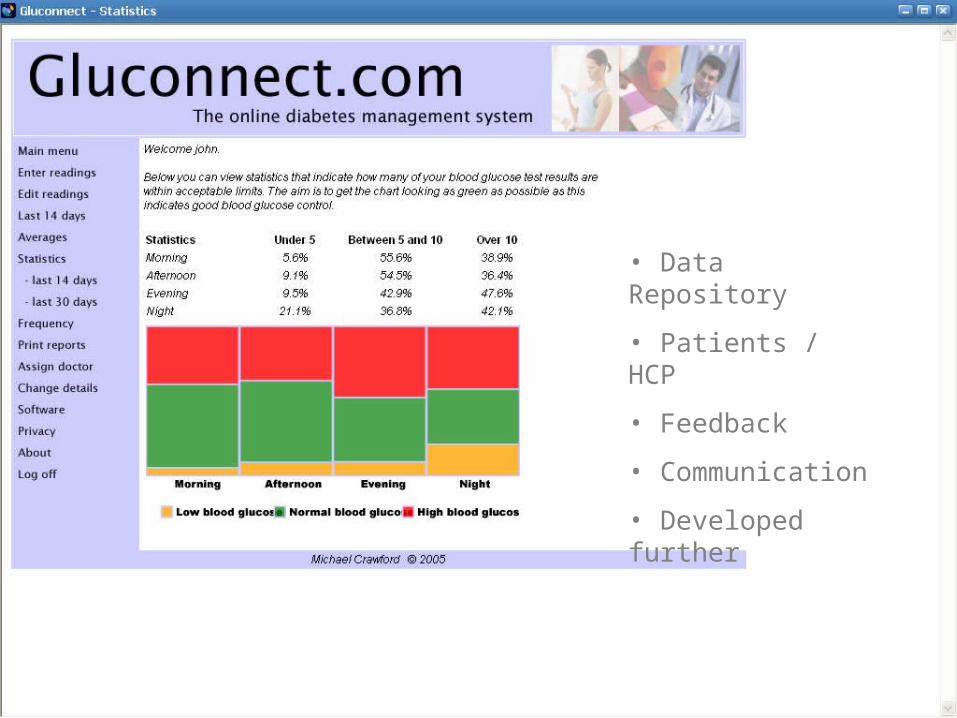
• Data Repository
• Patients / HCP
• Feedback
• Communication
• Developed further
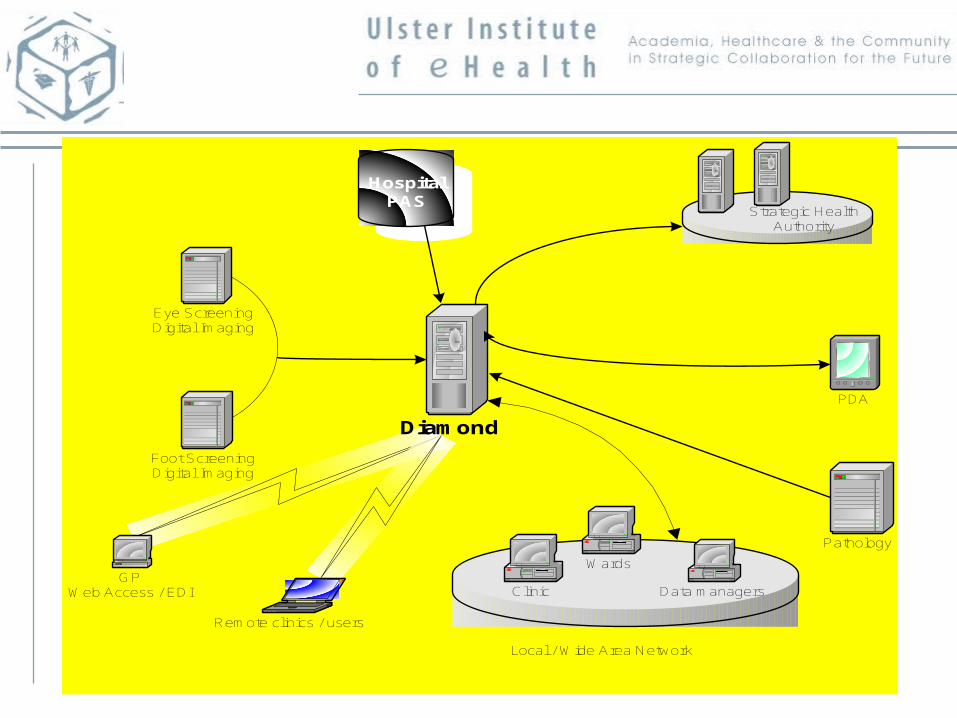
Electronic Patient Record (EPR)
Diamond
HospitalPAS
Remote clinics / users
Eye ScreeningDigital Imaging
Foot ScreeningDigital Imaging
Clinic
Wards
Local / Wide Area Network
Data managersGP
Web Access / EDI
Strategic HealthAuthority
PDA
Pathology
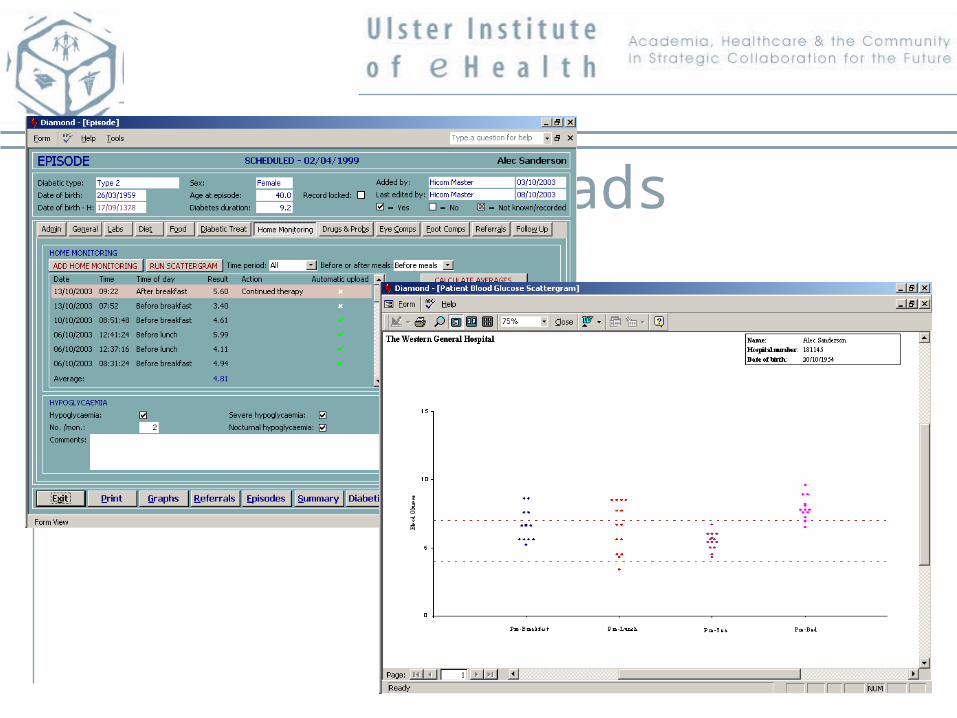
Meter Uploads
The Top 15 Features• Age and Diagnosis Duration
• Insulin Treatment, Smoking Status and Family History
• LabRBG, Diet Treatment and Tablet Treatment
• Complication Type and Drug Type
• LabCholesterol, LabMicroalbuminuria and LabTriglycerides
• BMI and Sex
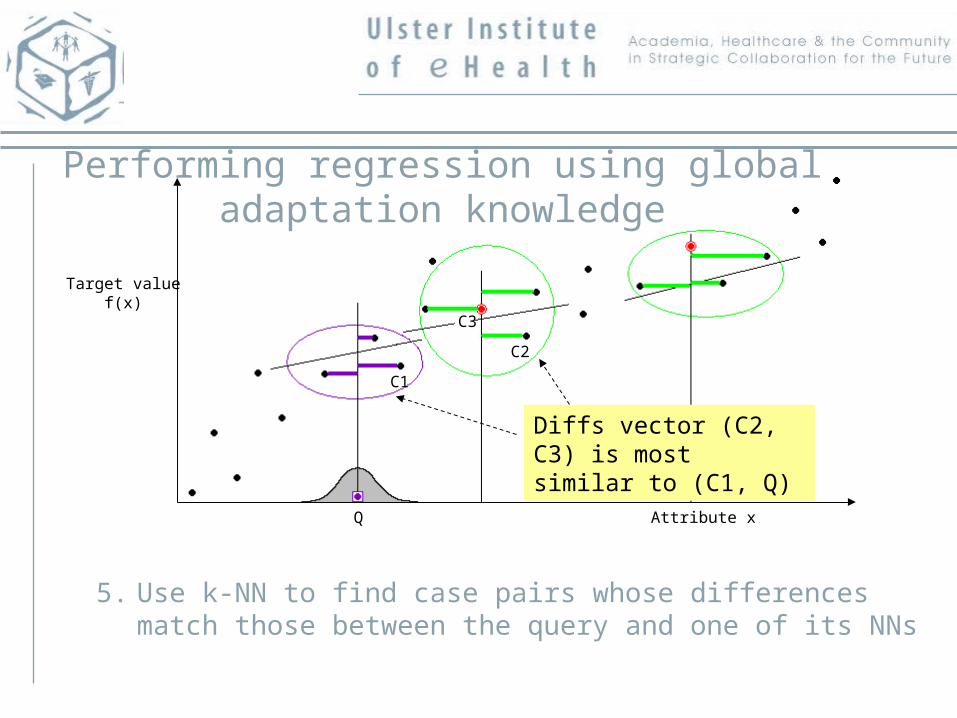
Performing regression using global adaptation knowledge
5. Use k-NN to find case pairs whose differences match those between the query and one of its NNs
C2
C1
Q
Diffs vector (C2, C3) is most similar to (C1, Q)
Target valuef(x)
Attribute x
C3
Healthcare Informatics Society of Ireland
Mr. Tom Holmes of IMS Maxims plc. presenting the prize for best paper to Ms. Ann Forde
The prevailing educational and health environment drives course development
• Fees (who pays for the education?), • Policy Drivers (from government, NHS), • Market (is there sufficient demand for more specialised
ICT graduates in HI?), • Graduate Output (will the graduate contribute?), • Bologna (harmonisation of course throughout Europe)
The nature of the course• The Scientific and Engineering Base of Course (is this sufficiently different from
Computer Science to warrant a new degree?), • Models & Philosophy (are they different from existing HI courses?), • Level of Course (is postgraduate the natural level for HI practitioners?), Audience
(existing workers or school leavers?), • Content / Relevance (core material which doesn’t change or the latest tools and
packages?), • Delivery Modes (Learning and Teaching: how flexible should delivery be?),• Progression (will student complete in time, given flexibility of delivery?)• Coherence of Subject (wide ranging or more depth in core discipline of computer
science), • Distinctiveness / Scope, Workplace Support, Teaching Expertise and Staffing Mix (is
this sufficient in one institution or do we need collaborative approach ?), • Educational Viability (will a practical course deliver proper education and knowledge)• Reflect Research (should the course reflect and use the latest HI research?)
The Healthcare Informatics occupation
• Mandatory (should HI professionals require a domain specific qualification?),
• Career Path (will a qualification enhance their career?)• Occupational Standards and Contractual Expectations (should
these reflect academic achievement?)• Knowledge and Skills Framework (is Otley the correct model, do we
need to refine or add to ducks and ponds?) • Graduate Characteristics (benefit to graduates and, benefits to
Employers), • General Health (Social / Community) Benefits (will a better educated
workforce in HI deliver this?), • Ethics
Collaboration between providers
• Ownership at University, Inter-disciplinarity (this may be a desirable way forward but requires good working relationships
• Tackling the digital divide by collaborating on course to third world countries might provide a way forward).
Acknowledgements
• Roy Harper• Chris Nugent• Juan Carlos Augusto• Maurice Mulvenna• Jonathan Wallace• Medical Informatics Recognised Research
Group


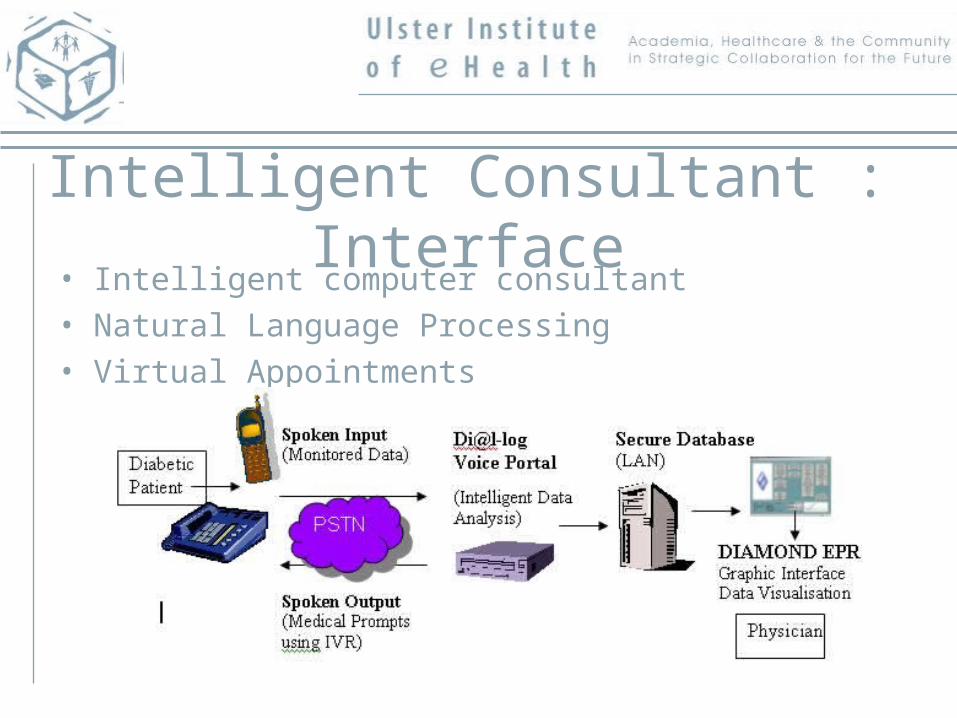
Intelligent Consultant : Interface• Intelligent computer consultant• Natural Language Processing• Virtual Appointments





























