Embed Size (px)
Citation preview

PART 2: THEMATIC ANALYSIS
HEALTH AND IMMUNIZATION SERVICES FOR THE
URBAN POOR IN EAST ASIA
Part 2 of Health and Immunization for the Urban Poor in East Asia:Thematic analysis of access barriers and opportunities in seven countries

UNICEF East Asia and Pacific Regional Office
19 Phra Atit Road Bangkok 10200 Thailand
Email: [email protected]/eapro
Cover image: © UNICEF EAPRO Health 2017

PART 2: THEMATIC ANALYSIS
HEALTH AND IMMUNIZATION SERVICES FOR THE
URBAN POOR IN EAST ASIA
Part 2 of Health and Immunization for the Urban Poor in East Asia:Thematic analysis of access barriers and opportunities in seven countries
UNICEF East Asia and Pacific Regional Office
FOREWORD
The East Asia and Pacific Region is undergoing significant social changes, fast growing economies, demographic transitions, and rapid urbanization. Rapid urbanization specifically has the potential to bring both opportunities and challenges to the development of its social systems.
Everyday in our region, families leave their rural homes, with dreams of a better life and future for their children, moving into cities, or places where urbanization is under way. In a rapidly changing world, children are the most vulnerable group in a society. Children need special care and protection
including adequate access to essential health, sanitation and social services.
The public health emergency of measles and diphtheria outbreaks in certain cities in our region is causing deaths and suffering to many children. This rings loud bells for the development community. The phenomenon of vaccine preventable disease outbreaks indicates an increased public health risk for urban populations. This may only be the tip of the iceberg. There are many other public health and development challenges for the urban poor that are affecting the well-being of millions of children and families. Among them are pneumonia and diarrhea.
Considering the important transition the East Asia and Pacific Region is undergoing, I am pleased to introduce our work on HEALTH AND IMMUNIZATION SERVICES FOR THE URBAN POOR IN EAST ASIA. The Summary Report and two detailed reports share existing evidence and analysis to examine how effectively health systems are responding to rapid urbanization in the region. They also map out policy and service gaps to close, and recommend strategies to reduce inequities of access to health care in urban settings. They clearly articulate the complexity of urban development systems. It shows the essential need for public and private sectors to work collaboratively to respond to the rapidly changing social conditions in the region.
UNICEF in East Asia and the Pacific is committed to protecting the rights of every child in the region, and leaving no one behind. We are also committed to working tirelessly and cooperatively with national and local governments, international partners and civil society agencies, to enhance social development systems to meet the needs of children and families. It also provides the opportunity to offer special support to those most suffering deprivation in what is a rapidly urbanizing region of the world.
We count on you to address the urgent need to tie down accountability for management and financing of health services for the urban poor.
Karin Hulshof UNICEF Regional Director, East Asia and the Pacific
CONTENTS
Acronyms and Abbreviations v
1. INTRODUCTION 1
2. MAIN THEMES 3
2.1 Social conditions of the urban poor in East Asia 3
2.2 Demographic trends in urban areas 4
2.3 Immunization coverage and vaccine-preventable diseases in urban areas 6
2.4 Evidence of vaccine-preventable disease outbreaks in urban areas in East Asia 8
2.5 Innovations in immunization operational strategy in urban areas in East Asia 8
2.6 Governance arrangements for immunization and urban health care in East Asia 12
3. DISCUSSION 15
3.1 Summary of main findings 15
3.2 Recommendations 16
4. CONCLUSIONS 21
References 22

iv l Health and Immunization Services for the Urban Poor in East Asia
LIST OF FIGURES AND TABLES
Figure 1 Number of people living in urban slums in six countries in East Asia, 2015 5
Figure 2 Percentage of population urbanized, 1995–2025 5
Figure 3 Urban DPT3 coverage for children aged 12-59 months by highest and lowest wealth quintile, six countries in East Asia, from most recent DHS/MICS 7
Figure 4 Urban DPT3 coverage for children aged 12-59 months by wealth quintile, Cambodia, DHS 2000–2014 7
Figure 5 Variables in municipal health governance 12
Table 1 Data on vaccine-preventable diseases in East Asia, 2012-2016 9
Table 2 Overview of urban strategies with comprehensive multi-year plans for immunization, six countries in East Asia 11
Health and Immunization Services for the Urban Poor in East Asia l v
ACRONYMS AND ABBREVIATIONS
ARMM Autonomous Region in Muslim MindanaoCHC commune health centrecMYP comprehensive multi-year plan (for immunization)CDC Centers for Disease Control and Prevention (United States) DHS Demographic and Health SurveyDOH Department of HealthDPT3 three doses of combined diphtheria/pertussis/tetanus vaccineEAPRO East Asia and Pacific Regional Office (UNICEF)EPI Expanded Programme on ImmunizationFGP family group practice (Indonesia)FHC family health centreHIV human immunodeficiency virusHPV human papilloma virusHSS health systems strengtheningJICA Japan International Cooperation AgencyLGU local government unitMICS Multi Indicator Cluster SurveyMMR measles, mumps and rubella vaccineMOH Ministry of HealthMCH maternal and child healthNCDs non-communicable diseasesNCR National Capital Region (the Philippines)NDOH National Department of Health (Papua New Guinea)NGO non-government organizationNIP national immunization programmeOPV oral poliomyelitis vaccine PATH Program for Appropriate Technology in HealthPHC primary health careREC Reaching Every CommunityRED Reaching Every DistrictREP Reaching Every PurokTB tuberculosisWPRO Western Pacific Regional Office of WHOUN United NationsUNICEF United Nations Children’s FundVDPV vaccine-derived polio virusVHV village health volunteerWHO World Health Organization

© UNICEF Cambodia 2017, Fani Llaurado
Health and Immunization Services for the Urban Poor in East Asia l 1
1. INTRODUCTION
This report aims to undertake a thematic analysis of a set of case studies on access by the urban poor to immunization and related health care services in selected countries of East Asia (Cambodia, Indonesia, Mongolia, Myanmar, Papua New Guinea, the Philippines,
and Viet Nam). Themes were then extracted from these seven country case studies to inform a wider view of current approaches, lessons learned, and potential policy and practice developments.
In all, six main themes were extracted from the case studies, and form the main headings to the sections that follow. The themes are:
1. Social conditions of the urban poor.
2. Demographic Trends in urban areas.
3. Immunization coverage and vaccine-preventable diseases in urban areas.
4. Evidence of vaccine-preventable disease outbreaks in urban areas.
5. Innovations in immunization operational strategy in urban areas.
6. Governance arrangements for urban health.
Although this report mainly focuses on immunization programming, the thematic analysis also explores the wider implications of the findings for health care for the urban poor more generally. This is illustrative of the fact that many of the policy and planning challenges confronted by immunization planners are not only relevant to the functioning of this programme, but can also apply to the implementation of other programmes such as maternal and child health (MCH) and communicable disease control programmes.
Before proceeding to a description and analysis of these themes, the report commences with a background to urbanization in East Asia, and a presentation of the main data sources and methods that inform this thematic analysis.
PART 2: THEMATIC ANALYSIS Health and Immunization Services for the Urban Poor in East Asia

© UNICEF EAPRO Health 2017
Health and Immunization Services for the Urban Poor in East Asia l 3
2. MAIN THEMES
2.1 Social conditions of the urban poor in East Asia
One of the main observations of this study is the extent to which the severity of the social conditions for the urban poor is ‘hidden’ by
administrative authority. In many of the countries, access to government services is regulated through systems of civil registration (Cambodia, Mongolia, Myanmar, the Philippines and Viet Nam). Although health systems are intended to provide services to all the population, lack of registration by urban migrants restricts the supply of adequate financing. It also may restrict demand, as lack of legal status may inhibit the very poor from accessing public services due to concerns regarding the cost of services for unregistered populations.1 In Mongolia and the Philippines, for example, social sector administrators and local authorities were requested to link up with the immunization strategy to expand the population’s access to services.2 In Viet Nam, lack of registration of new arrivals in Ho Chi Minh City has meant that there has been a chronic underestimate of the ‘real’ population in the catchment area, with surveys subsequently confirming low coverage amongst the urban poor.3 The question as to whether rural to urban poor migrants are being counted and included in health and local government registers is, therefore, a major issue to be addressed in urban health policy.
Compounding this problem of the hidden nature of the urban poor is the severity of the social conditions in which they reside. There are large agglomerations of poor who relocate to areas where there is limited public health infrastructure and services, such as in the peri-urban areas of Yangon and Phnom Penh. In Cambodia, the urban poor reside both in these peri-urban areas and in inner urban areas such as along railway tracks, in less accessible high-rise buildings and on public or privately owned lands.4 In Myanmar, there are very high concentrations of peri-urban poor, who have flooded into the city post political reform seeking improved economic opportunities.5 In Mongolia, the political and free-market reforms unleashed rapid rural to urban migrations, resulting in the relocation of dispersed traditional housing (ger) settlements in rural regions to very high concentrations of these settlements in the ‘ger districts’ of Ulaanbaatar.6 This rural style of living in the congested urban areas presents overwhelming public health infrastructure challenges relating to water, sanitation and access to public services.
4 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
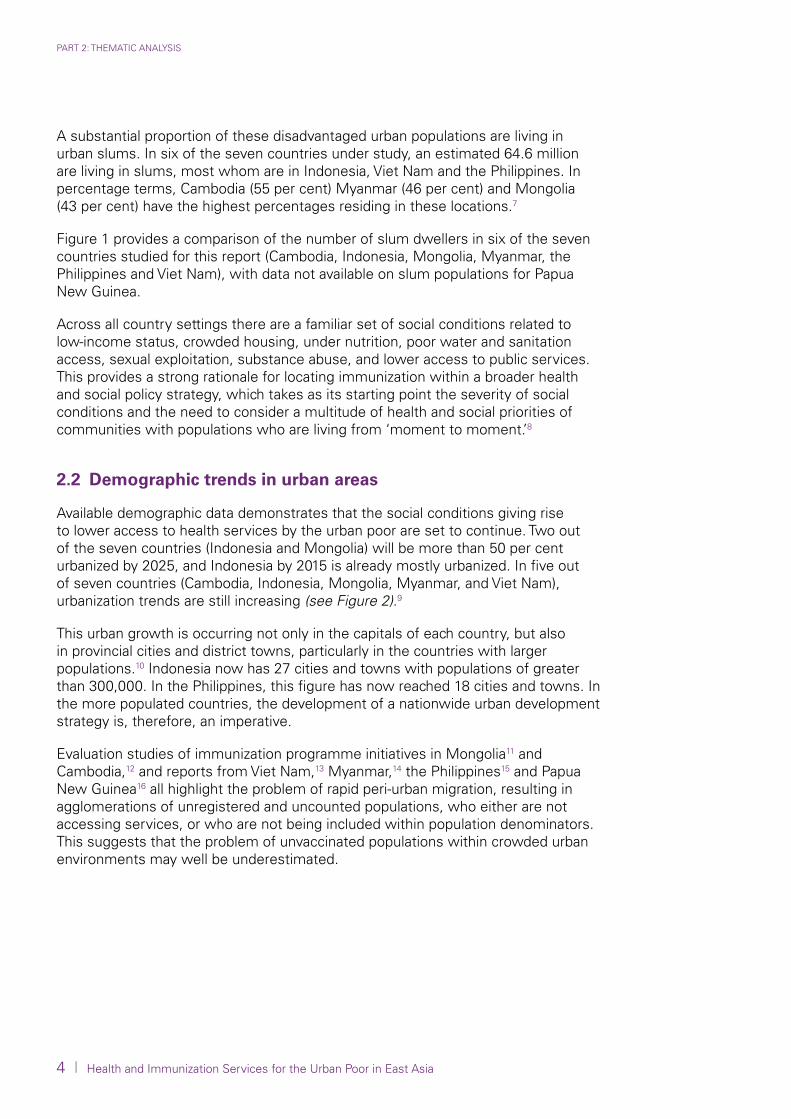
A substantial proportion of these disadvantaged urban populations are living in urban slums. In six of the seven countries under study, an estimated 64.6 million are living in slums, most whom are in Indonesia, Viet Nam and the Philippines. In percentage terms, Cambodia (55 per cent) Myanmar (46 per cent) and Mongolia (43 per cent) have the highest percentages residing in these locations.7
Figure 1 provides a comparison of the number of slum dwellers in six of the seven countries studied for this report (Cambodia, Indonesia, Mongolia, Myanmar, the Philippines and Viet Nam), with data not available on slum populations for Papua New Guinea.
Across all country settings there are a familiar set of social conditions related to low-income status, crowded housing, under nutrition, poor water and sanitation access, sexual exploitation, substance abuse, and lower access to public services. This provides a strong rationale for locating immunization within a broader health and social policy strategy, which takes as its starting point the severity of social conditions and the need to consider a multitude of health and social priorities of communities with populations who are living from ‘moment to moment.’8
2.2 Demographic trends in urban areas
Available demographic data demonstrates that the social conditions giving rise to lower access to health services by the urban poor are set to continue. Two out of the seven countries (Indonesia and Mongolia) will be more than 50 per cent urbanized by 2025, and Indonesia by 2015 is already mostly urbanized. In five out of seven countries (Cambodia, Indonesia, Mongolia, Myanmar, and Viet Nam), urbanization trends are still increasing (see Figure 2).9
This urban growth is occurring not only in the capitals of each country, but also in provincial cities and district towns, particularly in the countries with larger populations.10 Indonesia now has 27 cities and towns with populations of greater than 300,000. In the Philippines, this figure has now reached 18 cities and towns. In the more populated countries, the development of a nationwide urban development strategy is, therefore, an imperative.
Evaluation studies of immunization programme initiatives in Mongolia11 and Cambodia,12 and reports from Viet Nam,13 Myanmar,14 the Philippines15 and Papua New Guinea16 all highlight the problem of rapid peri-urban migration, resulting in agglomerations of unregistered and uncounted populations, who either are not accessing services, or who are not being included within population denominators. This suggests that the problem of unvaccinated populations within crowded urban environments may well be underestimated.
Health and Immunization Services for the Urban Poor in East Asia l 5
2. MAIN THEMES
Figure 1 Number of people living in urban slums in six countries in East Asia, 201517
Figure 2 Percentage of population urbanized, 1995–2025
1995 2005 2015 2025
Perc
enta
ge o
f po
pula
tion
that
is u
rban
ized
80
70
60
50
40
30
20
10
0
Mongolia
Indonesia
Philippines
Myanmar
Viet Nam
Cambodia
Papua New Guinea
Num
ber
of p
eopl
e liv
ing
in u
rban
slu
ms
(in m
illio
ns)
30
25
20
15
10
5
0
Mongolia Cambodia Myanmar Viet Nam Philippines Indonesia

6 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
2.3 Immunization coverage and vaccine-preventable diseases in urban areas
There is sufficient available data to confirm wide gaps in DPT3 coverage between wealth quintiles in urban setting (see Figure 3). In Cambodia, there was a gap of 12.1 per cent between the highest and lowest wealth quintiles in 2014, and 18.9 per cent gap between highest and lowest wealth quintiles in Indonesia in 2012. There was a 16.7 per cent gap between wealth quintiles in the Philippines in 2013, and an 11 per cent gap between wealth quintiles in Viet Nam in 2013. The latest DHS survey conducted in Myanmar in 2015 confirmed a 29.2 per cent gap in DPT3 coverage between the highest and lowest wealth quintiles.
Trend analysis from successive DHS data for children aged 12–59 months indicates some narrowing of inequities. In Cambodia, analysis on urban coverage over the last 14 years has demonstrated a narrowing of inequities between wealth quintiles, where coverage gaps between the highest and lowest wealth quintiles for DPT3 coverage for children aged 12-59 months have narrowed from 49 per cent in 2000 to 12.2 per cent in 2014.
In the two other countries where successive DHS data is available (Indonesia and the Philippines), gaps have also narrowed. Data from successive DHS surveys in Indonesia between 1997 and 2012 demonstrates that immunization coverage gaps between highest and lowest wealth quintiles for DPT3 coverage have narrowed over a 15-year period from a 26 per cent gap in 1997 to a 19 per cent gap in 2012. In the Philippines, the gap between highest and lowest quintiles for DPT3 coverage narrowed only slightly from 17.3 per cent in 1993 to 15.5 per cent in 2013.
From a public health and policy standpoint, it is important to observe that, even though overall inequities in coverage are narrowing, the absolute numbers of poor migrating to cities and residing in urban poor areas is also rapidly expanding, which potentially increases the pool of susceptible individuals to vaccine-preventable diseases (see further information on this in the next section). This supports the case for high levels of vigilance on the part of public health planners and policy makers in reducing the public health risk for vaccine-preventable and emerging diseases in the expanding urban poor communities of East Asia.

Health and Immunization Services for the Urban Poor in East Asia l 7
2. MAIN THEMES
Figure 3 Urban DPT3 coverage for children aged 12-59 months by highest and lowest wealth quintile, six countries in East Asia, from most recent DHS/MICS18
Figure 4 Urban DPT3 coverage for children aged 12-59 months by wealth quintile, Cambodia, DHS 2000–2014
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%Cambodia
(2014)
87.1%
99.3%
Mongolia(2013)
90.7%
95.1%
Philippines(2013)
77.3%
92.8%
Indonesia(2012)
65.1%
84.0%
Myanmar(2015)
58.8%
88.0%
Viet Nam(2013)
46.9%
58.4%
Lowest urban wealth quintileHighest urban wealth quintile
Perc
enta
ge o
f ur
ban
DP
T3 c
over
age
for
child
ren
aged
12-
59 m
onth
s
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%2000
31.8%
46.3%
61.7%
68.2%
80.8%
Lowest wealth quintile
Second wealth quintile
Third wealth quintile
Fourth wealth quintile
Highest wealth quintile
2005
58.6%
63.9%
65.2%
72.8%
90.1%
2010
81.4%
83.2%
88.9%
94.2%
95.7%
2014
87.1%
92.9%
93.4%
96.1%
99.3%
Perc
enta
ge o
f ur
ban
DP
T3 c
over
age
for
child
ren
aged
12-
59 m
onth
s

8 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
2.4 Evidence of vaccine-preventable disease outbreaks in urban areas in East Asia
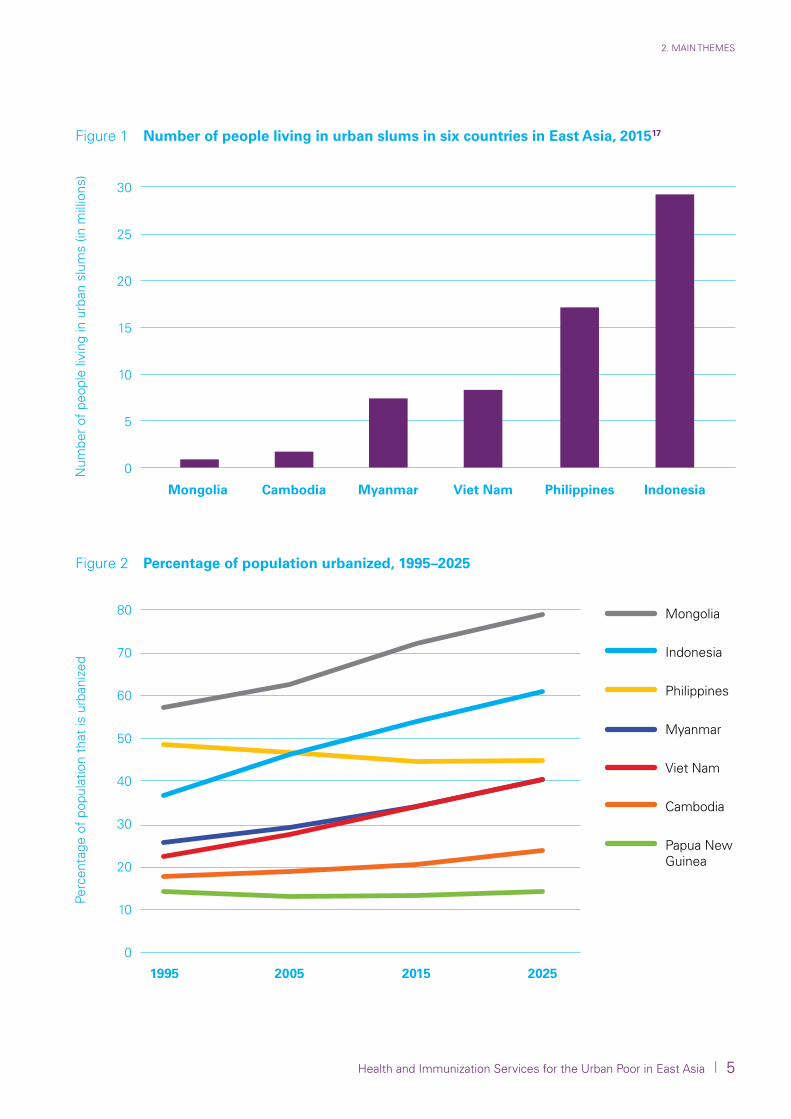
Recent vaccine disease outbreaks in Asia provide additional evidence to support the claim of significant immunity gaps in urban populations. In 2014 in the Philippines, there was a measles outbreak with highest caseloads in the National Capital Region.19 A diphtheria outbreak occurred in 2015, with 105 cases, of which one third were reported in one city hospital in Metro Manila.20 San Lazaro Hospital (SLH) in Manila has had, on average, at least one diphtheria death per month over the last seven years, with a case fatality rate greater than 50 per cent.21 In 2015 in Viet Nam, there was a nationwide measles outbreak, with 150 deaths reported at the National Hospital of Paediatrics in Hanoi.22 In Indonesia, there have been annual measles outbreaks in slums in North, East and West Jakarta districts, which comprised two thirds of annual confirmed measles cases.23 In Phnom Penh in 2005, a vaccine derived polio virus was detected in an urban poor area near the centre of the city, which resulted in the need for a subsequent national immunization campaign effort.24 And finally, in Mongolia in 2016, there was a measles outbreak nationally, with the outbreak first reported in Ulaanbaatar City and most cases reported from there. In all there were 23,000 cases and 105 fatalities.25 These findings point to significant immunity gaps for vaccine-preventable diseases in urban settings in East Asia, and align with earlier findings of lower immunization coverage in concentrated urban poor populations.
Table 1 summarizes evidence of vaccine-preventable disease outbreaks in East Asia in the last five years (2012-2016).
2.5 Innovations in immunization operational strategy in urban areas in East Asia
In Cambodia, Indonesia, Mongolia, Myanmar, the Philippines and Viet Nam, national programmes have been trialling approaches to urban immunization strategy. Cambodia, building on lessons learned from campaign methodology and a Reaching Every Community (REC) approach, developed a ‘high risk’ listing of villages across the country, which included urban poor locations.26 In Indonesia, a pilot project in Jakarta is trialling innovative communication, monitoring and management strategies in high-risk areas of Jakarta, with some promising coverage improvement reported.27 Mongolia developed a revitalized Reaching Every District (RED) strategy from 2010, focussing on high-risk identification, household visits to the urban poor, and social sector and civil society collaborations to expand access through improved civil registration. Several evaluations there have demonstrated the potential of the approach to improve immunization and other health service access for the urban poor.28 29 In Myanmar, a REC approach was designed in 2010, with a focus on mapping of high-risk areas, and an emphasis on analysis of risk in terms of social distance and not just physical distance.30
Health and Immunization Services for the Urban Poor in East Asia l 9
2. MAIN THEMES
In the Philippines, a ‘Reaching every Purok’ strategy (the purok is a subdivision of a barangay and is the smallest governance unit in the Philippines) has been devised, as a corollary to a wider nationwide Reaching Every Barangay approach. Main elements of the strategy include mapping of high-risk areas, identifying high-risk puroks through household card checks, developing a method for risk classification, working with community volunteers and local authorities to expand access to services through household visits.38 In Viet Nam, a National Immunization Review focussed on urban strategy development and highlighted major issues such as population tracking, waste management, public and private sector coordination, consistency in immunization scheduling, and financing by local governments as the main issues to be addressed in the upcoming cMYP.39
Except for the case of Mongolia, no in depth evaluations of the potential impact of these strategies has been documented. Although this may be attributable to the early stages of implementation, the fact that there is not adequate baseline or outcomes research indicates that current programme design is not being driven by research and evaluation efforts.
Location Year Disease outbreak and sources of data
Indonesia 2014 There have been annual measles outbreaks in slums in North, East and West Jakarta districts comprising two thirds of the annual confirmed measles cases31
Mongolia 2016 Measles outbreak nationally, with outbreak first reported in Ulaanbaatar City and most cases reported from there, 23,000 cases and 105 fatalities32
Myanmar 2012 Measles outbreak nationwide with immunization campaign activity in urban areas33
2016 Diphtheria outbreak in Yangon34
Papua New Guinea 2013 Measles outbreaks
2014 Measles outbreaks
Philippines 2014 Measles outbreak, with highest caseloads of measles in the National Capital Region35
2015 Diphtheria outbreak, 105 cases, with one third of cases reporting to San Lazaro Hospital in Metro Manila36
Viet Nam 2014 Measles outbreak, 150 deaths reported at the National Paediatric Hospital Hanoi37
Table 1 Data on vaccine-preventable diseases in East Asia, 2012-2016

10 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
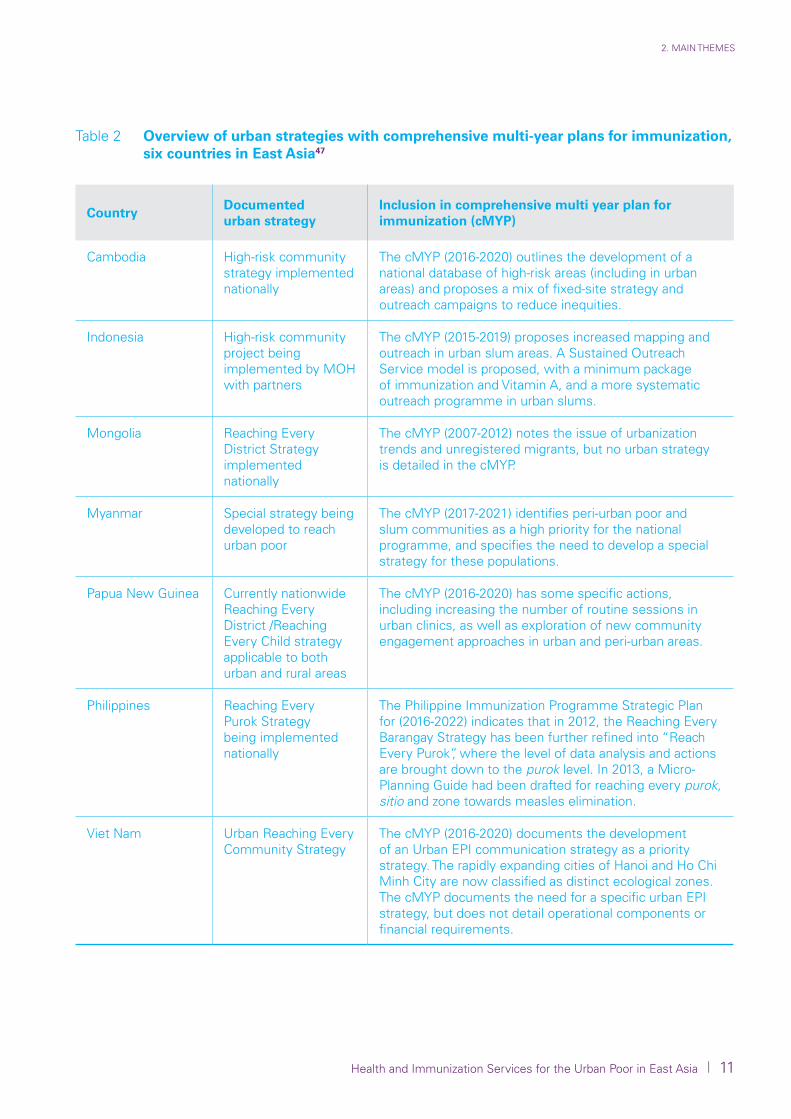
Although some countries have documented separate guidelines for urban strategy (Cambodia, the Philippines and Viet Nam), no country provides strategic or operational planning guidance of urban immunization within a multi-year plan for immunization (see Table 2).
Although project designs and financing have the potential to positively influence policies and plans, sustaining such project initiatives is reliant on their integration into national planning and budgeting systems. The Mongolia evaluations express in some detail the frustration in moving from a project to a system approach. Despite the development of the Ministerial Decree on Reaching Every District strategy, the strategy has still failed to be embedded in health system planning and budgeting functions, leaving the initiative highly exposed to the vagaries of project financing.40 Despite this managerial challenge, one in depth evaluation in Mongolia found that additional families can be reached through community-level mapping and follow up, provided additional resources can be mobilized to reach out to the most disadvantaged.41
In Cambodia, the nationwide REC approach is being financed through GAVI Health System Strengthening funds, leaving the question open as to how national and local governments will take up financing of the strategy post project completion.42 Despite this limitation, successive DHS over the last 15 years in Cambodia have seen a narrowing of gaps between lowest and highest wealth quintiles in urban areas.43
In Viet Nam, the clear evidence base and intent for strategy development is there, but the exact policy or procedural instrument by which to extract budgetary commitments for local governments in Hanoi and Ho Chi Minh City remains unclear.44 In the Philippines, advocacy meetings with local chief executives are proposed to accelerate the strategy, but how local governments are held accountable for financing and results requires more clarification and is currently under development.45 In Myanmar, the government has recently proposed significant decentralization reforms in line with the new constitution, but it remains the case that townships (the third administrative level in the Myanmar context) do not yet have operational budgets linked to health plans. In contrast, financing is ‘project based’ and strongly co-related to external financing.46
In summary, although there are promising innovations in operational strategy in urban immunization, there remain significant gaps in strategic policy and planning initiatives to tie down accountability and financing within policy or strategic planning documents, or in health system procedures.
Health and Immunization Services for the Urban Poor in East Asia l 11
2. MAIN THEMES
CountryDocumented urban strategy
Inclusion in comprehensive multi year plan for immunization (cMYP)
Cambodia High-risk community strategy implemented nationally
The cMYP (2016-2020) outlines the development of a national database of high-risk areas (including in urban areas) and proposes a mix of fixed-site strategy and outreach campaigns to reduce inequities.
Indonesia High-risk community project being implemented by MOH with partners
The cMYP (2015-2019) proposes increased mapping and outreach in urban slum areas. A Sustained Outreach Service model is proposed, with a minimum package of immunization and Vitamin A, and a more systematic outreach programme in urban slums.
Mongolia Reaching Every District Strategy implemented nationally
The cMYP (2007-2012) notes the issue of urbanization trends and unregistered migrants, but no urban strategy is detailed in the cMYP.
Myanmar Special strategy being developed to reach urban poor
The cMYP (2017-2021) identifies peri-urban poor and slum communities as a high priority for the national programme, and specifies the need to develop a special strategy for these populations.
Papua New Guinea Currently nationwide Reaching Every District /Reaching Every Child strategy applicable to both urban and rural areas
The cMYP (2016-2020) has some specific actions, including increasing the number of routine sessions in urban clinics, as well as exploration of new community engagement approaches in urban and peri-urban areas.
Philippines Reaching Every Purok Strategy being implemented nationally
The Philippine Immunization Programme Strategic Plan for (2016-2022) indicates that in 2012, the Reaching Every Barangay Strategy has been further refined into “Reach Every Purok”, where the level of data analysis and actions are brought down to the purok level. In 2013, a Micro-Planning Guide had been drafted for reaching every purok, sitio and zone towards measles elimination.
Viet Nam Urban Reaching Every Community Strategy
The cMYP (2016-2020) documents the development of an Urban EPI communication strategy as a priority strategy. The rapidly expanding cities of Hanoi and Ho Chi Minh City are now classified as distinct ecological zones. The cMYP documents the need for a specific urban EPI strategy, but does not detail operational components or financial requirements.
Table 2 Overview of urban strategies with comprehensive multi-year plans for immunization, six countries in East Asia47

12 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
2.6 Governance arrangements for immunization and urban health care in East Asia
In the 1970s and 1980s, the seven countries in the study commenced development of a primary health care (PHC) system based on a rural health model, with clear command and control structures, and administrative boundaries with defined population catchments, linked to primary care centres and village volunteers networked into a ‘social mobilization’ communication approach. This study demonstrates that urban health has evolved in a significantly more complex way, with governance and service delivery mechanisms dispersed across government, local government, civil society and private sector actors, with a completely different set of institutional and population dynamics. Figure 5 illustrates the diversity in management and provision of immunization services in the urban setting in Asia.
Figure 5 Variables in municipal health governance
National programmes
Urban populations,
migrants and mobile populations
Civil society agencies
Local government
Public sector providers
Private sector agencies
Social sector agencies
01
0206
0305
04
Health and Immunization Services for the Urban Poor in East Asia l 13
2. MAIN THEMES
Across the region, local government also have also proved to have critical roles in urban EPI. In Viet Nam, whilst the central government retains its financing functions for vaccines and cold chain equipment, the financing of operations rests with local government officials. In Myanmar, the Township Administrator (through the Township Health Committee) is responsible for ensuring the smooth operations of health services.48 Since 2004, the Government of Cambodia legislated an ‘Organic Law’, which defines the decentralized roles of local government in the provision of health care. A published plan for the development of the Municipality of Phnom Penh envisions the expansion of public health services as coming within its area of governance accountability.49
In the Philippines, services have been devolved to Local Government Units (LGUs) since 1993, with these LGUs providing most of the operational financing of PHC provision. In Mongolia, as part of its programme of health reform, performance contracts were established between family group practices, local government, and the Ministry of Health for provision of primary care. In both Indonesia and Papua New Guinea, the central government has the responsibility for policy and guidelines, supplementary immunization activities, procurement of vaccines and syringes, and technical assistance. But it is local government that has the responsibility for implementation in their area, and provides the budget for human resource recruitment and management, including for incentives, transportation and maintenance.50 Added into this governance and service delivery mix are the activities of non-government organizations (NGOs) and the private medical sector, that both have key roles in PHC in urban settings. Across the region, NGOs have been active in promoting access to primary care for the urban poor. Although the public sector remains the mainstay of immunization service provision, there is also growing evidence of increased availability of vaccines through a private sector model as illustrated by the cases of Cambodia51 and Viet Nam.52
Although these developments in devolution, and civil society and private sector development have also occurred in rural areas, it is urban areas that civil reforms and private sector development has the highest concentration of reform initiatives and resources. These complex institutional factors, along with high population concentration, growth and mobility, represent the more significant coordination and governance challenge as the region continues to urbanize.

© UNICEF EAPRO Health 2017
Health and Immunization Services for the Urban Poor in East Asia l 15
3. DISCUSSION
3.1 Summary of main findings
Despite important evidence gaps on immunization coverage in urban settings, there still remains sufficient evidence from surveys,
surveillance data, evaluations and analysis of planning documents to confirm that immunization in urban settings requires more urgent policy and planning attention.
This study has found that there are several factors working against efforts to ease social disadvantage and improve immunization access for the poor in urban areas, and which would need to be considered when developing an urban immunization strategy. There has been a rapid agglomeration of peri-urban poor, and a failure to keep pace with this growth through development of public health services infrastructure including PHC facilities, which is very evident on the periphery of such cities as Yangon, Phnom Penh and Ulaanbaatar. Despite evidence of rapid economic growth in most of these countries, there is also evidence for persisting or widening disparities between population groups in large population countries such as Indonesia.53 Disadvantage is also exacerbated by the fact that many of the poorest populations lack of civil registration status, which means that migrants are ‘hidden’ from administrative authorities, leading to unclear population denominators and limited entitlement by migrants to social sector support. This study has also found that there is a lack of health policy and planning models for urban health, and insufficient links between programme micro-planning and higher level urban master or development planning. These findings align with an international review of urban immunization coverage, which found that the main coverage concern is related to the pressure of rural to urban migration, and the related incapacity of local government infrastructure development to keep pace with this growth.54 It also aligns with The World Bank in its review of urbanization in South Asia, which found that issues of congestion, hidden populations and lack of responsiveness of public services were mostly attributable to problems with urban governance and finance.55
These management and operational shortcomings have resulted in coverage gaps and outbreaks of disease in urban areas across Asia in recent years. This is of concern given the harsh social conditions and associated high public-health risk for disease transmission in crowded slum environments. The overall public health and environmental conditions in which people live is reported by some analysts to increase intensity of disease transmission, severity of disease and efficacy of some vaccines.56 57 Despite these limitations, practical REC operational strategies in Mongolia and Cambodia, regardless of whether they are project related or not, have demonstrated the potential to reach more of the urban poor with immunization and other PHC services. Arguably such strategies will mitigate the risk of urban-based vaccine-preventable disease outbreaks in the future.

16 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
Despite these reported improvements in access, concerns remain as to whether such operational initiatives are reflected in higher-level health systems policy, planning and budgeting processes. A recent study on the implementation of the RED strategy in Africa found that the strategy often faded in its implementation rate and impact due to its dependence on external project funds.58 Increasingly, planners there are focussing more on linking immunization planning to a health system strengthening strategy, to improve the capability of the immunization system to leverage human resources and operational financing support through the wider health system. These findings resonate with the findings from an evaluation of the RED strategy in Mongolia, which demonstrated that lack of capability of health planners to link effectively to social sector planners and civil registration systems had led to lack of institutional support for the strategy and to a ‘stop start’ project culture.59 A recent evaluation of district evidence-based planning methodology in Bangladesh reached a similar conclusion, with coverage falling in some trial districts due to chronic shortages of human resources, supervision and operational finance, and inability of project planners to link the strategy to wider health sector planning and budgeting processes.60 These international cases illustrate that, although operational methods have become somewhat clearer and have demonstrated impacts in several countries, there are major gaps with strategic level thinking for urban health and immunization, that fails to consider the required governance, financing, and community engagement approaches to extend and sustain the strategy.
3.2 Recommendations
Given the pace of demographic trends, and the challenges and harshness of the social conditions of the urban poor in East Asia, and threat of ongoing disease outbreaks, development of urban immunization strategy should be an urgent concern of national planners and technical partners. There is sufficient evidence now to recommend a set of measures to activate the urban immunization strategy development and guide it on a sustainable pathway. These policy, planning and operational pathways include the following:
(a) Conduct baseline research on immunization and health access for the urban poor.
There are several options for such an approach, which could be conducted over a five-year period. The easiest way to facilitate this development may be to include urban health as a focus area in an EPI Review. This approach has been applied with some success in Cambodia and Viet Nam, and has facilitated development of urban strategies in these two countries. Alternate approaches could be to conduct baseline health systems and social research or health programme evaluations, as has been the case in Cambodia and Mongolia.
Health and Immunization Services for the Urban Poor in East Asia l 17
3. DISCUSSION
As part of these initial baseline studies, a ‘policy maker’ survey or mapping could be undertaken to better understand and describe the existing managerial and service delivery networks for health care in the urban setting.
Another important aspect of baseline studies are identifying the reasons and barriers behind low uptake of vaccination, including examination of social, cultural or political factors, and examination of levels of trust between service providers and communities.
(b) Redefine or review governance arrangements for urban health and immunization.
Governance arrangements for immunization and other health related services are urgently required to address the documented problems in urban settings of non-financed services, coverage gaps and prevention and control of disease outbreaks. Implementation strategies for review and refinement of urban health governance include the following:
(i) Clearer delegation of authority for urban health through development of regulatory or planning instruments including city master plans, national health or immunization policies, or health laws. In addition to development of these policy and planning instruments, consensus needs to be reached on the peak governance body or authority that accepts accountability for performance and outcomes for urban poor coverage and health. This will also involve clear delegation of authority for the operational aspects of service delivery in urban poor settings – including for financing and supervision, and other aspects of the immunization system in urban areas, such as waste management and cold chain maintenance.
(ii) Information and reporting networks will need to be clarified and defined, particularly given the pluralistic delivery system and widespread population movements in the urban setting. This networking of information extends to linking of health and local government registration systems, which has been identified in this report as a major barrier to access for the urban poor.
(iii) Modelling of PHC in the urban setting is an urgent policy and strategic focus for governments and international organizations. Technical assistance and policy-maker consultation is urgently required in order to achieve consensus on a model of municipal PHC that is best matched to the dynamic social and health conditions of urban settings in East Asia.
18 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
(c) Develop or revise urban immunization strategy, and link it to a wider urban health strategy.
Countries should develop an urban immunization strategy, which should be a standalone document, with a summary of key urban strategies and monitoring measures included in the multi-year plan for immunization. The main components of which should be:
(i) A situation analysis outlining the main gaps in service provision, and the legal and policy context for implementation.
(ii) An operational strategy to enhance coverage and programme performance (e.g. “Reaching Every Community Strategy”).
(iii) Definition of governance arrangements and standards for management of immunization in urban areas, with clear accountabilities for management (financing, service delivery, waste management, cold chain maintenance, surveillance and reporting) defined and agreed to by the main stakeholders.
(iv) A monitoring and evaluation strategy, with attention provided to monitoring of narrowing of inequities (see more below).
(d) Development of a monitoring and evaluation strategy on urban health and immunization.
Countries have developed effective strategies for monitoring and evaluation of urban health policies, that only require to be implemented more uniformly across the regions. The following strategies are recommended to develop monitoring and evaluation capacity for urban health:
(i) Demographic and Health Surveys, which disaggregate data by socio-economic exposure and location, are the definitive means by which countries track progress on reducing urban inequities.
(ii) Social research has been applied in Cambodia and Mongolia to characterize the needs of the urban poor, and recommend strategies to improve access. Formal evaluations, knowledge attitude and practice surveys, and network analyses are just some examples of social research.
(iii) National Immunization Reviews have been applied in both Cambodia and Viet Nam, focussing on inequities in Cambodia, and urban immunization in Viet Nam. In both countries, these reviews have facilitated movements toward a more urban approach.
(iv) Household checks of immunization status (potentially linked to documenting access to other MCH interventions) are a proven way to identify service gaps and needs, and have been applied successively in Cambodia, Mongolia and the Philippines. This model of household-level checking of immunization cards can be integrated into an operational strategy of ‘high risk’ or ‘reaching every district or community.’ It can also be a helpful way to track urban population movement and registration status.
Health and Immunization Services for the Urban Poor in East Asia l 19
3. DISCUSSION
(e) Support sustainability, explore links between health strategy (immunization as an entry point) and social policy.
The problem of unregistered status and lower access to health services exists in many of the countries, including Cambodia, Mongolia, Myanmar and Viet Nam. This finding provides a rationale for exploring stronger operational links between urban health sector strategy and social policy interventions. Examples of such an approach include the following:
(i) Health management and local government partnerships: There are opportunities for obtaining more accurate population estimates and improved health funding through more formal linkages of health and local government information, and management systems, particularly in relation to aligning health registration with birth and civil registration.
(ii) Linking health programmes to social safety nets: Equally, there may be opportunities to link to social programmes to supporting social safety nets, such as health financing schemes for the poor and conditional cash transfers where these systems exist.
(iii) Closer engagement of health programmes with education services: Given the expansion of national immunization programmes, the health sector could also explore closer linkages with the education sector, to improve immunization knowledge and access through the education system. UNICEF is well placed to explore such links, given this agency’s expanded roles in health, education, and child and social protection.

© UNICEF EAPRO Health 2017

Health and Immunization Services for the Urban Poor in East Asia l 21
4. CONCLUSIONS
This review has found that there are pockets of deep disadvantage in urban areas, with low immunization coverage frequently related to lower socio-economic status. These pockets of low coverage are resulting in widespread urban preventable-disease outbreaks
in Asia, and do not augur well for future containment of emerging diseases. The development of an urban health and immunization strategy is urgently required regionally and nationally to respond to the impacts of rapid demographic change, social transition and increased epidemiological risk.
It will be critical that policy makers tie down accountability for resourcing of the strategy, and include the approach within the planning and budgeting procedures of ministries of health and local governments. In the shorter term, international organizations and non-government organizations will need to redouble efforts to ensure operational technical guidance for reaching every community is documented and disseminated across the region. In the medium to long term, technical agencies and partner governments will need to focus on the development of municipal models of primary health care that have clear delegations of authority and shared networks of information. Given the governance and public health challenges, including expanding slum and peri-urban populations, reliance on external partners and charitable institutions is not a viable option in the long term for urban poor strategies. What is required is a scale up of known operational strategies through ministry and local government institutional arrangements, so that pro-poor health services become core priority business for urban planners.
22 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
REFERENCES
1 Lhamsuren, K, et al., ‘Taking action on the social determinants of health: improving health access for the urban poor in Mongolia’, International Journal for Equity in Health, vol. 11, no. 5, 20 March 2012, <www.equityhealthj.com/content/pdf/1475-9276-11-15.pdf>.
2 Ibid.3 Government of Vietnam, National Institute of Hygiene and Epidemiology, National EPI
Review 2015, NIHE and WHO Hanoi.4 United Nations Children’s Fund, Health Service Access Among Poor Communities in
Phnom Penh, UNICEF, 2009, <www.unicef.org/eapro/Health_Service_Access_Among_ Poor_Communities_Phnom_Penh_(Low.pdf>, accessed 16 October 2017.
5 Sheehy, Grace, et al., ‘Dynamics Shaping Access to Reproductive Health Services inPeri Urban Yangon, Myanmar: A Multi-Methods Study’, Global Journal of Health Science, vol. 8, no. 11, 2016.
6 Benedikte V. Lindskog, ‘Natural calamities and ‘the Big Migration’: Challenges to the Mongolian Health System in ‘the Age of the Market,’ Global Public Health, 2014, vol. 9, no. 8, 2014, pp. 880–893, <http://dx.doi.org/10.1080/17441692.2014.940361>, accessed 16 November 2016.
7 World Health Organization, Country Profiles on Urban Health, WHO Geneva, <www.who.int/kobe_centre/measuring/urban_health_observatory/uhprofiles/en/>, accessed 11 November 2016.
8 UNICEF Health Access Study in 4 Communities in Phnom Penh 2010, <www.unicef.org/eapro/Health_Service_Access_Among_Poor_Communities_Phnom_Penh_(Low.pdf>, accessed 11 November 2016.
9 UN Habitat, 2016 Statistical Annex of the Worlds Cities Report, <http://unhabitat.org/ urban-knowledge/global-urban-observatory-guo/>, accessed 11 November 2016.
10 Ibid.11 HERA REDS Strategy Evaluation Mongolia Final Report 2014, <www.unicef.org/
evaldatabase/files/2014_Mongolia_-_REDS_Strategy_Evaluation_Mongolia.pdf>, accessed 9 September 2016.
12 UNICEF, Health Access Study in 4 Communities in Phnom Penh, 2010. <www.unicef. org/eapro/Health_Service_Access_Among_Poor_Communities_Phnom_Penh_(Low.pdf>, accessed 11 November 2016.
13 Ministry of Health, National EPI Review Report Vietnam, NIHE and WHO Hanoi, 2015.14 Asia Pacific Observatory, Health Systems Review Myanmar 2013.15 UN Habitat, 2016 Urban population and urbanization by country, 1990–2050.16 Independent State of Papua New Guinea, National Urbanisation Policy 2010–2030, Office
of Urbanisation, May 2010.17 World Health Organization, Country Profiles on Urban Health, WHO Geneva, <www.who.
int/kobe_centre/measuring/urban_health_observatory/uhprofiles/en/>, accessed 11 November 2016
18 The DHS program, <http://dhsprogram.com>, accessed 14 December 2016.19 Dulce C. Elfa, ‘Strategy: Addressing Immunity Gaps in Urban Communities’, PowerPoint
presentation, DOH the Philippines Manila, 2016.20 WHO, Lessons learned from recent diphtheria cases, <www.wpro.who.int/philippines/
mediacentre/features/lessons_learned_diphtheria_cases/en>, accessed 30 August 2016.
Health and Immunization Services for the Urban Poor in East Asia l 23
REFERENCES
21 Department of Health, WHO, The Philippine Immunization Program Strategic Plan for 2016–2022, DOH Manila.
22 National Preventive Medicine Centre, Hanoi, National EPI Review 2015, Vietnam, p. 59.23 UNICEF Indonesia, May 2016 presentation on health programmes, UNICEF Jakarta.24 Soeung S, et al., The social determinants of health and health service access: An in depth
study in four poor communities in Phnom Penh Cambodia, International Journal for Equity in Health vol. 11(1): 46, August 2012 article (pdf available).
25 WHO, Measles outbreak in Mongolia – FAQs, 5 May 2016, <www.wpro.who.int mongolia/mediacentre/releases/20160505-measles-outbreak-faqs/en>, accessed 9 September 2016.
26 Ministry of Health Cambodia, Health System Strengthening Strategy, GAVI proposal 2015, Phnom Penh, <www.gavi.org/country/cambodia/documents>, accessed 3 November 2016.
27 UNICEF 2016, ‘Reaching Every Community to achieve full coverage with essential vaccinations, status update and action plan’, UNICEF, July 2016, Jakarta.
28 HERA REDS Strategy Evaluation Mongolia, Final Report 2014, <www.unicef.org evaldatabase/files/2014_Mongolia_-_REDS_Strategy_Evaluation_Mongolia.pdf>, accessed 9 September 2016.
29 UNICEF Mongolia, ‘Assessment of Reaching Every District Strategy’, UNICEF Ulaanbaatar. www.unicef.org/eapro/Mongolia_REDassessment_FINAL, accessed 9 September 2016.
30 Ministry of Health Myanmar, Reaching Every Community Guidelines 2010, UNICEF Yangon.
31 UNICEF Indonesia, May 2016, Presentation on Health Programmes, UNICEF Jakarta.32 WHO Measles outbreak in Mongolia – FAQs 5 May 2016, <www.wpro.who.int/mongolia/
mediacentre/releases/20160505-measles-outbreak-faqs/en>, accessed 9 September 2016.
33 IRIN Myanmar to immunize 6.4 million against measles, <www.irinnews.org photo/201203221156030186/some-64-million-children-will-be-vaccinated-against-measlesacross-Myanmar>, accessed 16 August 2016.
34 As reported in Myanmar Times, 10 June 2016, <www.mmtimes.com/national-news/yangon/20789-diphtheria-outbreak-claims-six-lives.html.
35 Dulce C. Elfa, ‘Strategy: Addressing Immunity Gaps in Urban Communities’, PowerPoint presentation, DOH the Philippines Manila, 2016.
36 WHO, Lessons learned from recent diphtheria cases, <www.wpro.who.int/philippines/mediacentre/features/lessons_learned_diphtheria_cases/en>, accessed 30 August 2016.
37 National Preventive Medicine Centre, Hanoi, National EPI Review 2015, Vietnam, p. 59.38 UNICEF, ‘Reducing Inequities in Urban Poor Immunization Programme’, Monitoring
Report, July–Sept 2016, UNICEF Manila.39 Government of Vietnam, National Institute of Hygiene and Epidemiology, National EPI
Review 2015, NIHE and WHO, Hanoi.40 HERA REDS, Strategy Evaluation Mongolia Final Report 2014, <www.unicef.org/
evaldatabase/files/2014_Mongolia_-_REDS_Strategy_Evaluation_Mongolia.pdf>, accessed 9 September 2016.
24 l Health and Immunization Services for the Urban Poor in East Asia
PART 2: THEMATIC ANALYSIS
41 Lhamsuren K, et al., Taking action on the social determinants of health: Improving health access for the urban poor in Mongolia, International Journal for Equity in Health, 2012, Vol. 11(15), 20 March 2012, <www.equityhealthj.com/content/pdf/1475-9276-11-15.pdf>, accessed 21 November 2016.
42 Ministry of Health Cambodia, Health System Strengthening Proposal 2015.43 For impact in Cambodia, refer to successive DHS <http://dhsprogram.com/what-we-do/
survey/survey-display-464.cfm>, accessed 23 November 2016.44 National Preventive Medicine Centre, Hanoi, National EPI Review 2015 Vietnam, p. 59.45 UNICEF, ‘Reducing Inequities in Urban Poor Immunization Programme’, Monitoring
Report, July–Sept 2016, UNICEF Manila.46 Tin N, Saw Lwin et al., ‘An Approach to Health System Strengthening in the Union of
Myanmar, Health Policy’, vol. 95(2010): pp. 95–10247 All Multi-Year Plans sourced from GAVI website <www.gavi.org/country>, accessed
14 December 2016.48 Myanmar Ministry of Health, National Immunisation Programme, Multi-Year Plan for
Immunization, 2012–2016.49 Municipality of Phnom Penh, City Development Strategy, 2005–2015.50 GAVI, Joint Appraisal 2015 Indonesia, GAVI, Geneva.51 Soeung S et al., Evaluation of Public Private Collaboration for Immunization in Cambodia,
Journal of Health, Population and Nutrition, vol. 26(0): 2008.52 Ministry of Health Vietnam, National EPI Review Report Vietnam, WHO and NIHE,
Hanoi, 2015.53 The World Bank, Indonesia’s Rising Divide, <http://documents.worldbank.org/curated/
en/885651468180231995/pdf/101668-WP-PUBLIC-Box394818BExecutive-Summary-Indonesias-Rising-Divide-English.pdf>, accessed 4 November 2016.
54 Awoh AB., Plugge E., Immunisation coverage in rural-urban migrant children in low and middle-income countries (LMICs): A systematic review and meta-analysis. Journal of Epidemiol Community Health, 2016 Mar, vol. 70(3), pp. 305-11, <https://www.ncbi.nlm.nih.gov/pubmed/26347277>.
55 Ellis P, Roberts R, Leveraging Urbanisation in South Asia, 2016, World Bank, Washington D.C.
56 J. Atkinson, J. Cheyne, Immunization in urban areas: Issues and strategies, Bulletin of the World Health Organization, 1994, vol. 72(2), pp. 183-194.
57 Victoria Jiang et al., Performance of rotavirus vaccines in developed and developing countries, 2010 July, vol. 6(7), pp. 532–542. doi: 10.4161/hv.6.7.11278 PMCID: PMC332251
58 UNICEF, Review of Pro Equity Planning Approaches in Africa, Draft Report, 2015.59 HERA REDS, Strategy Evaluation Mongolia Final Report 2014, <www.unicef.org/
evaldatabase/files/2014_Mongolia_-_REDS_Strategy_Evaluation_Mongolia.pdf>, accessed 9 September 2016.
60 John Grundy, Shukhrat Rakhimdjanov and Merina Adhikari, Policy opportunities and limitations of Evidence Based Planning for Immunisation: Lessons learnt from a field trial in Bangladesh, WHO South-East Asia, Journal of Public Health, September 2016,vol. 5(9), <http://apps.who.int/iris/bitstream/10665/249537/1/seajph2016v5n2.pdf#page=85>.




UNICEF East Asia and Pacific Regional Office
19 Phra Atit Road Bangkok 10200 Thailand
Email: [email protected]/eapro





























