Embed Size (px)
Citation preview

International Journal of Pediatric Otorhinolaryngology (2008) 72, 719—724
www.elsevier.com/locate/ijporl
CASE REPORT
Head and neck epithelioid sarcoma in a child:Diagnostic dilemma and anterolateral thigh freeflap reconstruction
Jayakar V. Nayak a, Lisa A. Teot b, Yatin Vyas c,Carl H. Snyderman a, Elizabeth H. Toh a, Frederic W.-B. Deleyiannis a,d,*
aUniversity of Pittsburgh, Department of Otolaryngology, University of Pittsburgh Medical Center,United StatesbUniversity of Pittsburgh, Department of Pathology, University of Pittsburgh Medical Center, United StatescUniversity of Pittsburgh, Department of Pediatric Oncology,University of Pittsburgh Medical Center, United StatesdUniversity of Pittsburgh, Department of Plastic Surgery, University of Pittsburgh Medical Center,6th Floor Scaife Hall, Pittsburgh, PA 15213, United States
Received 31 October 2007; accepted 22 January 2008Available online 17 March 2008
KEYWORDSEpithelioid sarcoma;Granuloma annulare;Free flapreconstruction;Anterolateral thighfree flap;Head and neck sarcoma
Summary The diagnostic dilemma is discussed of a child who presented witha granulomatous process of the external ear that was originally consideredgranuloma annulare and was later diagnosed as epithelioid sarcoma. We presentthe surgical treatment and the first report of reconstruction of a lateral skullbase and cheek defect with an anterolateral thigh (ALT) free flap in a pediatricpatient.# 2008 Elsevier Ireland Ltd. All rights reserved.
1. Case report
A 7-year-old boy presented with a 1-year history ofslow growing, painful, cutaneous nodules involvingthe left preauricular area at the site of a previousdog bite. A biopsy of the area 1-year prior to pre-senting in our clinic demonstrated pathology con-
* Corresponding author.E-mail address: [email protected]
(F.W.B. Deleyiannis).
0165-5876/$ — see front matter # 2008 Elsevier Ireland Ltd. All rigdoi:10.1016/j.ijporl.2008.01.032
sistent with granuloma annulare. Subsequent to theinitial biopsy, he had persistent symptoms of inter-mittent pain as well as continued progression of thecutaneous nodules and of soft tissue thickening ofthe external ear and preauricular skin.
On physical exam, the left pinna was slightlymore proptotic compared to the right ear, andhad an erythematous inflammatory process invol-ving the superior aspect of the auricle, conchal bowland external auditory meatus (Fig. 1A). There wasextension into the tragus and preauricular tissues.
hts reserved.
720 J.V. Nayak et al.
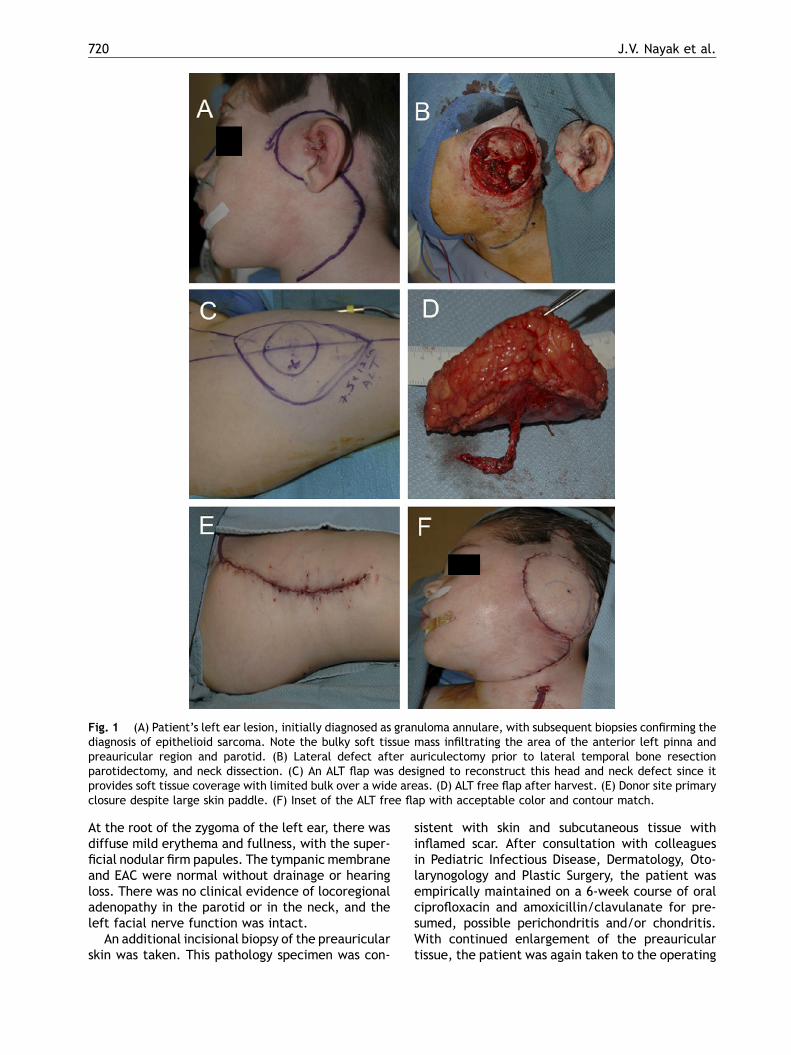
Fig. 1 (A) Patient’s left ear lesion, initially diagnosed as granuloma annulare, with subsequent biopsies confirming thediagnosis of epithelioid sarcoma. Note the bulky soft tissue mass infiltrating the area of the anterior left pinna andpreauricular region and parotid. (B) Lateral defect after auriculectomy prior to lateral temporal bone resectionparotidectomy, and neck dissection. (C) An ALT flap was designed to reconstruct this head and neck defect since itprovides soft tissue coverage with limited bulk over a wide areas. (D) ALT free flap after harvest. (E) Donor site primaryclosure despite large skin paddle. (F) Inset of the ALT free flap with acceptable color and contour match.
At the root of the zygoma of the left ear, there wasdiffuse mild erythema and fullness, with the super-ficial nodular firm papules. The tympanic membraneand EAC were normal without drainage or hearingloss. There was no clinical evidence of locoregionaladenopathy in the parotid or in the neck, and theleft facial nerve function was intact.
An additional incisional biopsy of the preauricularskin was taken. This pathology specimen was con-
sistent with skin and subcutaneous tissue withinflamed scar. After consultation with colleaguesin Pediatric Infectious Disease, Dermatology, Oto-larynogology and Plastic Surgery, the patient wasempirically maintained on a 6-week course of oralciprofloxacin and amoxicillin/clavulanate for pre-sumed, possible perichondritis and/or chondritis.With continued enlargement of the preauriculartissue, the patient was again taken to the operating

ALT flap reconstruction in a child after sarcoma excision 721
room for exploration and additional tissue sampling.Biopsies were diagnosed as epithelioid sarcoma.
Asdefinitive treatment, thepatient receiveda lefttotal auriculectomy, superficial parotidectomy withfacial nerve dissection and cheek skin excision, andselective neck dissection levels 1—3 (Fig. 1A and B).This was followed by a lateral temporal bone resec-tion with removal of the malleus, incus, temporalbone cortex and skin of the external auditory canal.This defect was thereafter reconstructed with a freeanterolateral thigh (ALT) flap (Fig. 1C—F) with a skinpaddle measuring 8 cm � 11 cm. The final pathologydemonstrated a tumor 3.5 cm in greatest dimension(T2) arising in the subcutaneous tissue of the anteriorauricle and preauricular area, without evidence ofangiolymphatic or perineural invasion. All surgicalmargins, lymph nodes, and bone specimens werenegative for malignancy. Presently the patient is 12months post-surgery without evidence of persistentor recurrent disease based on interval MRI and PET—CT imaging of the head and neck.
2. Discussion
This patient initially presented as a diagnosticdilemma. Given the initial phenotypic appearanceand pathologic findings of these lesions, this patientwas given a working diagnosis of granuloma annu-lare. Subcutaneous granuloma annulare lesions arecommonly found in children, with head and neckareas such as the scalp and forehead being thesecond most common sites of initial presentationafter the extremities [1]. The papules of granulomaannulare appear as smooth, firm, nonulceratedlesions, which upon biopsy are found to have pali-sading histiocytes admixed with lymphocytes sur-rounding a central bed of degenerated collagen[1,2]. Of note, however, lesions diagnosed as gran-uloma annulare in children are almost universallyasymptomatic and nontender, and noted only inci-dentally by parents of the affected patients. Thedifferential diagnosis of firm, subcutaneous papularlesions in the pediatric population includes benignprocesses such as erythema nodosum, rheumatoidand pseudorheumatoid nodules, dermoid cysts,infections and trauma, and malignant neoplasms[3]. Given the history and characteristics of thislesion on presentation and histologic examination,granuloma annulare is an understandable diagnosis,until persistence with symptoms warranted furtherinvestigation and tissue sampling.
Epithelioid sarcoma, sometimes referred toepithelioid sarcoma of Enzinger, was only formallydefined in 1970 [4]. This nonrhabdomyosarcoma softtissue sarcoma typically arises in teens and young
adults [5] and most commonly affects the distalextremities. It is rare in children under 10 yearsof age and the head and neck is involved in less than10% of cases.
Epithelioid sarcoma is divided into conventionaland proximal types. Proximal-type epithelioid sar-coma typically arises in axial locations in middle-aged adults, and is composed of large atypicalepithelioid or rhabdoid cells with prominentnucleoli arranged in sheets [4,6]. In contrast, con-ventional epithelioid sarcoma, as seen in thispatient, has nodular arrays of epithelioid and plumpspindle cells, often with central degeneration ornecrosis. The cells are often deceptively bland, withminimal cytologic atypia and pleomorphism, andperipheral lymphocytic infiltrates may be present,mimicking a chronic inflammatory process. Bothproximal-type and conventional epithelioid sarco-mas generally express cytokeratins, epithelial mem-brane antigen (EMA), and vimentin. CD34 is positivein over 50% of epithelioid sarcomas, and helps todistinguish this tumor from carcinomas. In contrast,S100 protein, desmin, CD31 and FLI-1 are usuallyabsent in epithelioid sarcomas [4]. This immuno-phenotype parallels that observed in our patientwhose tumor specimen was strongly positive forCD34, EMA, and vimentin (Fig. 2), and focally posi-tive for wide-spectrum cytokeratins, while negativefor CD31, desmin, S100 and p53 (data not shown).Loss of heterozygosity at chromosome 22q [7,8] andvarious other nonspecific cytogenetic abnormalitieshave been reported in epithelioid sarcoma. How-ever, to date, no consistent cytogenetic or molecu-lar genetic abnormalities have been identified inthis tumor.
In addition to a variety of malignant epithelioidtumors, the differential diagnosis for epithelioidsarcoma includes a variety of benign processes,including nodular fasciitis, necrotizing infectiousgranulomas, necrobiosis lipoidica, rheumatoidnodules and granuloma annulare, as reviewedrecently [4], helping to explain the initial diagnosisand treatment plan in this patient. Distinction fromthese benign entities is based on immunoreactivityfor the aforementionedmarkers, which are typicallyabsent in benign granulomatous processes, andabsence of staining for infectious agents such asacid-fast bacilli and fungal elements. As well, com-parative analysis of mitotic figures can also beperformed, although slowly growing malignant neo-plasms with infrequent atypical nuclei might still bemissed [9]. Indeed, on review, the original biopsyspecimens from this patient showed deceptivelybland nuclei not typically reminiscent of sarcomaand few mitotic figures, which helped to thwart thecorrect diagnosis. In contrast, the resection speci-

722 J.V. Nayak et al.
Fig. 2 Immunohistochemical staining pattern for epithelioid sarcoma. These sarcomas are notable for their expressionof CD34 (A), EMA (B), vimentin (C), and scattered cytokeratin (D). Standard monoclonal antibody staining protocols withimmunoperoxidase amplification was utilized. Each image was taken at 200� magnification.
men showed 5—10 mitotic figures/hpf and Ki-67staining in up to 20% of nuclei in the most cellularareas.
The primary treatment ladder for this diseaseconsists of surgical extirpation, and depending onthe institution and adequacy of resection, can alsobe followed with adjuvant radiation therapy (con-ventional and/or hyperfractionated) and multiplechemotherapeutic options (similar to those used forrhabdosarcoma) in children [5].
Prognosis in terms of 5- and 10-year survivalthresholds is 70% and 40%, respectively, with favor-able indicators including young age of diagnosis,female gender and small initial tumor size [4].However, a recent report from the Italian soft tissuesarcoma committee demonstrated an overall survi-val of 92% at 5 years and 87% at 10 years in theircohort of pediatric patients with various stages ofepithelioid sarcoma, with favorable indicatorsincluding distal extremity cancers and primaries<3 cm in size [5]. In Enzinger’s series of over 200patients, 77% of patients developed local recur-rence and 45% displayed locoregional metastases[7]. These discrepancies are probably explainedby the wide range of initial TNM site and stagedifferences of the patients included in each series.
Free flaps are often the ideal reconstructivemodality for parotidectomy and lateral skull basedefects with large cutaneous defects [10,11]. Themost common free flaps for skin reconstruction arethe ALT flap [12,13], scapular flap [14], the rectus
abdominis flap [15], and the radial forearm free flap(RFFF). The ALT flap has recently gained popularityin soft tissue reconstruction of the head and neck[13,16,17]. It is a perforator flap, derived from thedescending branch of the lateral circumflex femoralartery. Its advantages include a long pedicle with asuitable vessel diameter and the possibility of har-vesting the flap with thigh musculature (the vastuslateralis muscle, rectus femoris muscle, and/or thetensor fasciae lata) or as a sensate flap (by incor-porating the anterior branch of the lateral cuta-neous nerve of the thigh). Because of its distance tothe head and neck, its harvest can be performedsimultaneously with tumor extirpation. A skindefect of less than 9 cm in width can be closedprimarily without any reported evidence of com-partment syndrome to the extremities. Largerdefects require skin grafting. A distinct disadvan-tage is the thickness of the flap in overweightindividuals. However, the flap can be trimmed tothe subdermal fat level for use as a thinner flap(4 mm). The disadvantages of scapular and para-scapular flaps are that they require harvesting in thelateral position and that the skin on the back canalso be among the thickest in the body. With obesitythe latter flaps can also be quite thick. Probably thebiggest disadvantage of using the rectus abdominisflap is its bulky nature. However, for parotidectomydefects that involve a large loss of midface volume(i.e., after resection of check skin, parotid, lateralmandible, and muscles of mastication), the rectus

ALT flap reconstruction in a child after sarcoma excision 723
abdominis can be a useful option. Compared to anALT or scapular flap, a RFFF is thinner, and thus,reconstruction of a parotid and cutaneous defectwith a RFFF may still leave the patient with acontour depression at the site of the parotidectomy.Potential donor site morbidities, including tendonexposure, failure of skin graft take, and poorappearance, are other disadvantages.
The ALT has been used previously for reconstruc-tion of large temporal bone and parotidectomydefects [11,18], and a variety of flaps for free tissuetransfer have been previously successfullyemployed in children [19]. In a recent retrospectiveanalysis of the indications and morbidity of freeflaps in the pediatric population by the AAO-HNSMicrovascular Committee [20], head and neck sar-coma was the most common tumor requiring opera-tion and reconstruction, and the fibula was thecommonly utilized free flap donor site. Interest-ingly, of the 49 flaps employed in 47 patients, therewere no ALT free flaps reported. To our knowledge,this is the first publication that describes use of theALT free flap in a child with a skull base defect.Similar to prior publications [21] and to overallmorbidity outcomes [20], we found limited donorsite morbidity to the lower extremity following flapharvest. This child was involved in playing his usualsports activities within 1 month. Flap thicknessapproximated the cheek and lateral skull basedefect without being too thick or too thin.
Currently, the patient is doing very well. His freeflap underwent rapid healing without complication,and the lateral thigh donor site did not compromisethis patient’s activity level. He had a follow-upPET—CT scan at 3 and 8 months post-operatively,which showed no evidence of disease recurrence.
3. Conclusion
Given the unconventional history and circumstancethat is presented, this case helps to reinforce thecurrent need for multidisciplinary care in the assess-ment of the complex pediatric patient, and more-over, the principle of continually revisiting theinitial diagnosis if the patient is not improved fol-lowing active therapeutic measures. The ALT flapcan now be considered a viable and cosmeticallyfavorable free flap for reconstruction of large headand neck defects that arise in children.
Conflict of interest statement
The authors (J.V.N., L.T., Y.V., C.H.S., E.H.T. andF.W.-B.D.) attest that they each have no financial or
personal conflicts of interests to disclose regardingthis work.
References
[1] E.I. Felner, J.B. Steinberg, A.G. Weinberg, Subcutaneousgranuloma annulare: a review of 47 cases, Pediatrics 100(December (6)) (1997) 965—967.
[2] K.L. Grogg, A.G. Nascimento, Subcutaneous granulomaannulare in childhood: clinicopathologic features in 34cases, Pediatrics 107 (March (3)) (2001) E42.
[3] J.P. Whelan, A. Zembowicz, Case records of the Massachu-setts General Hospital. Case 19—2006. A 22-month-old boywith the rapid growth of subcutaneous nodules, N. Engl. J.Med. 354 (June 22 (25)) (2006) 2697—2704.
[4] C. Fisher, Epithelioid sarcoma of Enzinger, Adv. Anat. Pathol.13 (May (3)) (2006) 114—121.
[5] M. Casanova, A. Ferrari, P. Collini, G. Bisogno, R. Alaggio, G.Cecchetto, et al., Epithelioid sarcoma in children and ado-lescents: a report from the Italian Soft Tissue SarcomaCommittee, Cancer 106 (February 1 (3)) (2006) 708—717.
[6] E.A. Zevallos-Giampietri, C. Barrionuevo, Proximal-typeepithelioid sarcoma: report of two cases in the perineum:differential diagnosis and review of soft tissue tumors withepithelioid and/or rhabdoid features, Appl. Immunohisto-chem. Mol. Morphol. 13 (September (3)) (2005) 221—230.
[7] D.R. Chase, F.M. Enzinger, Epithelioid sarcoma. Diagnosis,prognostic indicators, and treatment, Am. J. Surg. Pathol. 9(April (4)) (1985) 241—263.
[8] M.M. Quezado, L.P. Middleton, B. Bryant, K. Lane, S.W.Weiss,M.J. Merino, Allelic loss on chromosome 22q in epithelioidsarcomas, Hum. Pathol. 29 (June (6)) (1998) 604—608.
[9] J.C. Cordoba, D.M. Parham, W.H. Meyer, E.C. Douglass, Anew cytogenetic finding in an epithelioid sarcoma, t(8;22)(q22; q11), Cancer Genet. Cytogenet. 72 (February(2)) (1994) 151—154.
[10] A. Afifi, F.W.-B. Deleyiannis, Reconstruction after excision ofcancer of the salivary glands, in: E.N. Myers, R.L. Ferris(Eds.), Salivary Gland Disorders, first ed., Springer, 2007, pp.435—462.
[11] J.J. Disa, V.M. Rodriguez, P.G. Cordeiro, Reconstruction oflateral skull base oncological defects: the role of free tissuetransfer, Ann. Plast. Surg. 41 (December (6)) (1998) 633—639.
[12] Y. Kimata, K. Uchiyama, S. Ebihara, T. Yoshizumi, M. Asai, M.Saikawa, et al., Versatility of the free anterolateral thighflap for reconstruction of head and neck defects, Arch.Otolaryngol. Head Neck Surg. 123 (December (12)) (1997)1325—1331.
[13] F.C. Wei, V. Jain, N. Celik, H.C. Chen, D.C. Chuang, C.H. Lin,Have we found an ideal soft-tissue flap? An experience with672 anterolateral thigh flaps, Plast. Reconstr. Surg. 109(June (7)) (2002) 2219—2226 (discussion 27—30).
[14] J. Upton, R.E. Albin, J.B. Mulliken, J.E. Murray, The use ofscapular and parascapular flaps for cheek reconstruction,Plast. Reconstr. Surg. 90 (December (6)) (1992) 959—971.
[15] F.W. Deleyiannis, C. Rogers, E. Lee, J. Russavage, B. Gast-man, J. Dunklebarger, et al., Reconstruction of the lateralmandibulectomy defect: management based on prognosisand location and volume of soft tissue resection, Laryngo-scope 116 (November (11)) (2006) 2071—2080.
[16] F. Demirkan, H.C. Chen, F.C. Wei, H.H. Chen, S.G. Jung, S.P.Hau, et al., The versatile anterolateral thigh flap: a muscu-locutaneous flap in disguise in head and neck reconstruction,Br. J. Plast. Surg. 53 (January (1)) (2000) 30—36.

724 J.V. Nayak et al.
[17] W.C. Huang, H.C. Chen, V. Jain, M. Kilda, Y.D. Lin, M.H.Cheng, et al., Reconstruction of through-and-through cheekdefects involving the oral commissure, using chimeric flapsfrom the thigh lateral femoral circumflex system, Plast.Reconstr. Surg. 109 (February (2)) (2002) 433-L441 (discus-sion 42—3).
[18] F. Demirkan, S. Unal, E. Arslan, O. Gurbuz, Versatileanterolateral thigh perforator flap: case of tailoredreconstruction for a large temporal and parotidectomydefect, J. Reconstr. Microsurg. 19 (May (4)) (2003)221—224.
[19] J.M. Serletti, V.A. Schingo Jr., M.A. Deuber, A.J. Carras, H.R.Herrera, V.F. Reale, Free tissue transfer in pediatricpatients, Ann. Plast. Surg. 36 (June (6)) (1996) 561—568.
[20] D.J. Arnold, M.K. Wax, Pediatric microvascular reconstruc-tion: a report from the Microvascular Committee, Otolar-yngol. Head Neck Surg. 136 (May (5)) (2007) 848—851.
[21] Y.R. Kuo, S.F. Jeng, M.H. Kuo, M.N. Huang, Y.T. Liu, Y.C.Chiang, et al., Free anterolateral thigh flap for extremityreconstruction: clinical experience and functional assess-ment of donor site, Plast. Reconstr. Surg. 107 (June (7))(2001) 1766—1771.
Available online at www.sciencedirect.com





























